
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pharmacol., 09 April 2025
Sec. Neuropharmacology
Volume 16 - 2025 | https://doi.org/10.3389/fphar.2025.1571699
 Raquel Piñar-Morales1,2*
Raquel Piñar-Morales1,2* Raquel Calle-Calle1Maria Carrasco-Garcia1Cristina Davila-Arias3
Raquel Calle-Calle1Maria Carrasco-Garcia1Cristina Davila-Arias3 Luisa Maria Villar-Guimerans4
Luisa Maria Villar-Guimerans4 Francisco J. Barrero Hernandez2,5
Francisco J. Barrero Hernandez2,5Progressive multifocal leukoencephalopathy (PML) results from the reactivation of John Cunningham virus JC virus and is a rare complication of anti-CD20 drug therapy. Neurofilament light chains increasingly serve as a marker of neuroaxonal damage in the follow-up of patients with multiple sclerosis (MS), but its role in the monitoring and detection of processes such as PML is yet to be defined. We report the case of a patient with MS who was treated with ocrelizumab and developed PML. Results: Serum neurofilament light chain (sNFL) levels were elevated at the diagnosis and progressively increased over his follow-up. Our results suggest that the monitoring of sNFL levels may be useful for the early diagnosis of PML in patients with MS.
Progressive multifocal leukoencephalopathy (PML) is a rare and often lethal disease caused by reactivation of the John Cunningham virus JC virus in immunocompromised patients (Schweitzer et al., 2023). JC virus is a highly ubiquitous polyomavirus that remains latent in a large proportion of healthy individuals (Bozic et al., 2014). It was first described in individuals with hematological diseases and then in people living with human immunodeficiency virus (HIV). It has recently been associated with the receipt of immunosuppressive drugs and with immune system deficiencies that favor virus reactivation (Cortese et al., 2021). One of the most frequently implicated drugs is natalizumab, which acts against alpha-4 integrin and is used in the treatment of multiple sclerosis (MS). PML has also been related to other disease-modifying therapies (DMTs) for MS, such as fingolimod or dimethyl fumarate. An association between PML and ocrelizumab (OCR) has only been described in two patients (Rindi et al., 2024). Neurofilaments light chain (NfL) are key indicators of axonal damage and hold great promise as biomarkers for monitoring patients with MS. In the case of patients with PML, their measurement has been reported in various publications, although their role in the early detection of PML remains to be defined. We report the case of a patient with progressive primary MS (PPMS) who was treated with OCR and developed PML. Since the diagnosis of PML and during follow-up, serum neurofilament light chain (sNfL) has been determined.
56-year-old right-handed male diagnosed with PPMS (2010 McDonald criteria) in 2013. He had a history of latent tuberculosis and pulmonary nodule lesion, with a pathological diagnosis of necrotizing granuloma and a positive PCR result for Mycobacterium tuberculosis, and he underwent a complete chemoprophylaxis cycle in 2017. At the PPMS diagnosis, the patient reported weakness and gait abnormality during the previous year, and examination revealed proximal and distal weakness of 4/5 in right lower limb alongside pyramidal syndrome with bilateral Babinski sign. Neuroimaging showed spatial dissemination of demyelinating lesions and IgG- and IgM-positive oligoclonal bands in the cerebrospinal fluid (CSF). The expanded disability status scale (EDSS) score at diagnosis was 3.5. The patient was treated with glatiramer acetate (GA) for transient improvement after corticosteroid bolus administration. Follow-up neuroimaging study in 2018 evidenced radiological activity, with the emergence of new lesions (Figure 1A). In February 2019, the GA regimen was interrupted to initiate treatment with OCR, which was well tolerated. At OCR treatment onset, his EDSS score was 6.5, Timed 25-foot Walk Test (T25FW) was 18.25 s, 9-hole peg test (9HPT) 21.7 s in dominant hand (D) and 24.73 s in non-dominant hand (ND), immunoglobulin IgG was 937 mg/dL (normal range 540–1882 mg/dL) and IgM 513 mg/dL (normal range 22–240 mg/dL). A slight initial improvement was followed by a gradually progressive deterioration. At follow-up examination in December 2022, the 9HTP result was 25.10 s in D and 27.20 s in ND, the EDSS score remained stable, and there was no significant change in T25FW score (16.9 s) or IgG value (989 mg/dL), while IgM levels had progressively decreased but remained within the normal range (44 mg/dL). He received OCR treatment for 4 years, with no infusion-related adverse effects and no onset of severe infection.
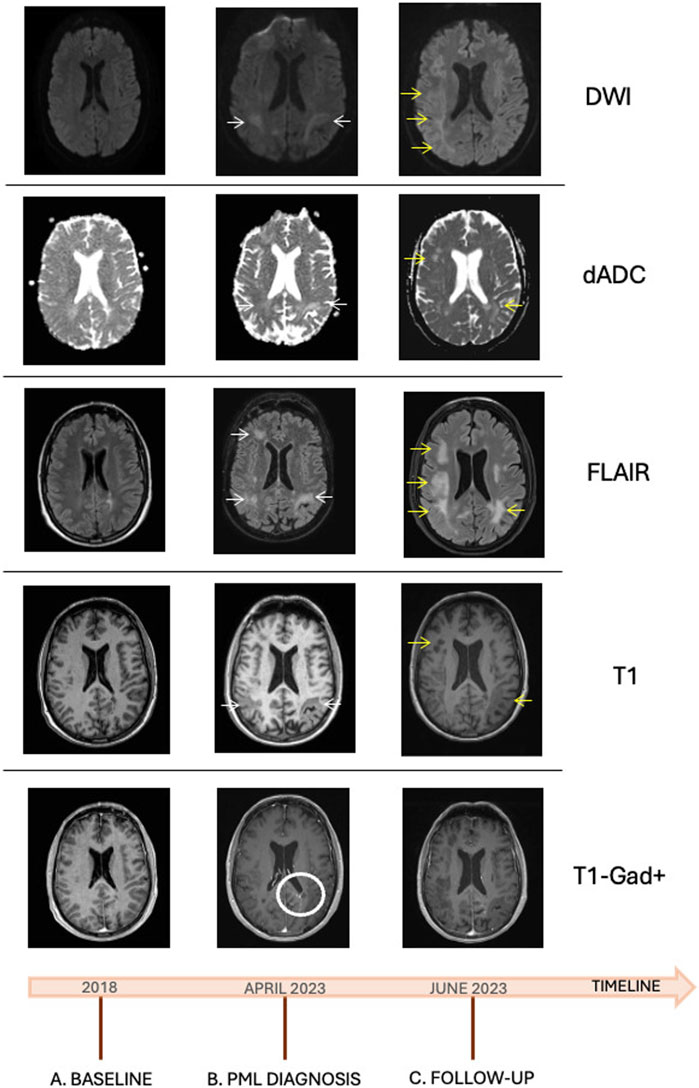
Figure 1. Neuroimaging study during follow up: (A) baseline MRI, 6 months before OCR treatment onset, observing hyperintense T2/FLAIR lesions with no contrast enhancement or diffusion restriction; (B) MRI performed upon PML diagnosis, observing subcortical lesions and lesions in both parietal and occipital lobes, T1 hypointense and FLAIR hyperintense (white arrows), with no expansive effect, contrast enhancement, or diffusion restriction. Contrast enhancement in the left parieto-temporal region related to a venous development anomaly, previously known (white circle) (C) Follow-up MRI after symptom worsening, observing an expansion of PML lesions (yellow arrows), with no contrast enhancement or diffusion restriction. dADC, Apparent diffusion coefficient ADC map; DWI, Diffusion-weighed imaging; FLAIR, fluid-attenuated inversion recovery; PML, progressive multifocal leukoencephalopathy; OCR, ocrelizumab; MRI, magnetic resonance imaging; T1-Gad+, T1 sequence with gadolinium.
In April 2023, he reported language problems over the previous 3 months, with confusion of phonemes and difficulty to find words, being able to understand what he read but unable to remember it immediately afterwards. The most recent OCR dose had been administered in December 2022. Examination revealed low-fluency spontaneous language with frequent blocks and some phonemic paraphasia. He understood simple orders but evidenced saturation with more complex orders, naming was preserved, and the result of the categorical verbal fluency test was six animals in 1 minute. He committed errors in reading with preserved writing. The cranial nerves were preserved. He had minimal distal weakness in right upper limb and paraparesis with right lower limb predominance. He had preserved symmetrical tactile sensitivity and algesia, and lower limb hypoesthesia.
Magnetic resonance imaging (MRI) (Figure 1B) showed multiple subcortical lesions and lesions in both parietal and occipital lobes, hypointense in T1 and hyperintense in T2/FLAIR, with no expansive effect, contrast uptake, or diffusion restriction. In addition, lesions were observed in the frontal lobe of the left hemisphere, which would explain the language impairment. Hyperintense supra- and infra-tentorial lesions in T2 were related to the presence of MS. Findings of no restriction in diffusion and no contrast uptake were compatible with PML. Blood count and immunoglobulin test results were within normal ranges, with IgA of 197 mg/dL (normal range, 70–400 mg/dL), IgG of 989 mg/dL (540–1882 mg/dL), and IgM of 45 (22–240 mg/dL). Lymphocyte counts were 1/μL for CD19 (normal range, 122–682/μL), 812/μL for CD4+ (540–1,660/μL), and 655/μL for CD8+ (270–930/μL). HIV serology was negative, and remaining proteinogram, serology, and autoimmunity results were negative or normal. Anti-aquaporin-4 antibodies (AbAQP4), anti-myelin oligodendrocyte antibodies (antiMOG Ab), anti-glial fibrillary acidic protein antibodies, and antineuronal antibodies were negative. CSF analysis showing no cellularity and 23.3 mg/dL proteins with 60 mg/dl glucose. Immunophenotyping in CSF showed low cellularity. Serum neurofilament light chain (sNfL) levels were 43.3 pg/mL. PCR studies in CSF were negative for viruses and bacteria, including toxoplasma. The determination of JC virus in CSF by PCR was performed at the Virgen de las Nieves Hospital in Granada with a positive result.
Given the clinical and radiological characteristics, along with the positivity of JC virus in the CSF, he was diagnosed with definitive PML. Treatment with mirtazapine 30 mg daily and mefloquine 250 mg twice a day, later once weekly, was administered as compassionate treatments due to the absence of approved options. The patient remained clinically stable for the first 3–4 weeks, with no radiological worsening, and his sNfL levels were also followed at weekly examinations (Figure 2). Mild motor worsening was recorded in June 2023, and the patient was again admitted to hospital. An MRI scan evidenced larger and more extensive lesions (Figure 1C), and he died after a few days of clinical deterioration with increasing language disorder and motor impairment.
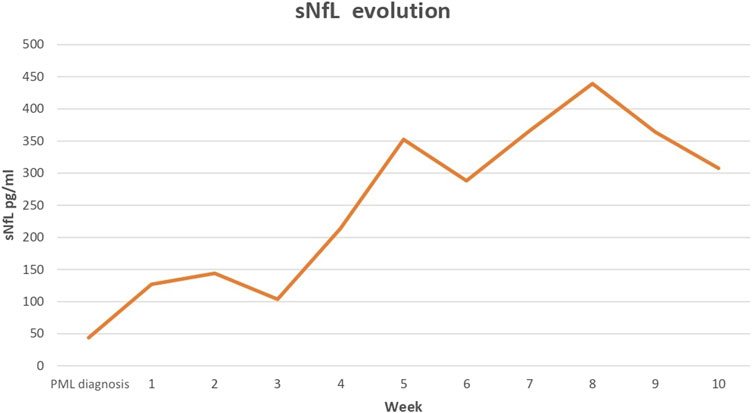
Figure 2. Time course of sNfL levels from PML diagnosis until death of patient. PML, progressive multifocal leukoencephalopathy; sNFL, serum neurofilament light chain.
The pathogenesis of PML has not yet been fully elucidated, and it is not known why this severe disease develops in certain patients. However, sustained immunosuppression plays a key role, given the high seroprevalence of JC virus in the general population. JC virus is ubiquitous and transmitted person-to-person or by contact with contaminated surfaces, food, or water (Cortese et al., 2021). The virus remains latent in kidneys, lymph nodes, and the brain, among other organs (Monaco et al., 1996). Chronic immunosuppression favors genetic changes that can foster neurotropism and brain damage by the virus (Cortese et al., 2021). In addition, virus clearance is hampered by the immunosuppression of lymphocytes, especially CD4+ and also CD8+ T lymphocytes, and by cytokine profile changes in the setting of immunosuppression (Bernard-Valnet et al., 2021).
PML has been described as a complication of anti-CD20 drug therapy since 2002, when it was first associated with rituximab treatment for patients with non-Hodgkin lymphoma (Bennett et al., 2021) (Calabrese et al., 2007). Most reported cases related to anti-CD20 drugs have involved patients receiving rituximab for MS, hematological neoplasms, or rheumatological diseases such as rheumatoid arthritis or sarcoidosis (Focosi et al., 2019). The mechanism by which these drugs favor virus reactivation and PML emergence is unknown but appears to involve factors related to the virus per se and to humoral and cellular immunity (Durali et al., 2015). It has been proposed that JC virus can remain as an intact virion after infecting B lymphocytes (BLs), which can therefore propagate and disseminate the virus in the central nervous system (CNS) (Chapagain and Nerurkar, 2010). Furthermore, JC virus DNA has been detected in peripheral BLs and BLs from PML-derived brain tissue (Major et al., 1990). Antibodies against VP1, the main protein of this virus, may play a neutralizing role and may be related to the number of activated plasmatic cells, although their protective effect remains unclear. In addition, given that BLs regulate T lymphocyte functionality via different pathways, BL depletion may alter homeostasis and facilitate virus persistence through a failure of effector T lymphocytes and inhibition of the inflammatory response (Durali et al., 2015).
JC virus reactivation with PML development is a highly infrequent complication of some DMTs in MS. To our best knowledge, we present only the third published case of PML associated with OCR in a patient not previously treated with another DMT. There have been reports of PML onset in seven patients who had previously received natalizumab or fingolimod (Sharma et al., 2022). The first reported case of a patient with PML treated with OCR and without prior DMT was a 78-year-old male who had received OCR for 2 years Lymphocyte test revealed grade 2 lymphopenia (780/μL), with a CD4+ count of 294/μL (normal range: 325–1,251/μL) and CD8+ count of 85/μL (90–775/μL). He was treated with pembrolizumab but did not survive (Patel et al., 2021). The second published case, a 56-year-old female with remittent-recurrent MS, previously treated with GA and later switched to OCR, which she received OCR for 4 years. She had 882 JC virus copies in CSF, grade 2 lymphopenia in peripheral blood (690/μL), and hypogammaglobulinemia, with IgG of 541 mg/dL (normal range: 700–1,600 mg/dL) and IgM of 24 mg/dL (40–230 mg/dL). She stabilized after treatment with pembrolizumab but was readmitted to hospital for an epileptic episode, where she died after failing to respond to anti-epileptic therapy (Puig-Casadevall et al., 2023).
NfL form part of the neuronal structure, are released into extracellular space upon cell damage or death and have therefore been proposed as markers of neuroaxonal damage (Khalil et al., 2024). NfL can be detected in CSF or serum and already serve as activity marker of MS in some centers, although their role in the follow-up of patients has yet to be established. The determination of NfL may permit the early detection of PML in at-risk patients, since increased sNfL levels have been observed up to 3 months before the diagnosis of PML in natalizumab and ozanimod-treated patients (Valentino et al., 2023; Quintanilla-Bordás et al., 2024). The study of sNfL levels may be useful to differentiate between cases of PML and relapses, given that levels in PML, which are 10-fold higher versus baseline (Dalla et al., 2019), are up to 8-fold higher than in relapses (Fissolo et al., 2021).
The present patient was diagnosed with PPMS and had received prolonged OCR treatment. Unlike the above two cases, there was no evidence of lymphopenia, no alteration in CD4+ or CD8+ T lymphocyte counts, and no reduction in immunoglobulin levels before or during the course of PML. In our prospective study of sNfL levels, these were above the normal range after PML onset. Although no data are available on pre-PML values, sNfL levels increased over the follow-up period alongside a clinical worsening and an increase in lesions on MRI scans.
This case reflects the complexity of DMT mechanisms, which can modify the immune system in ways that remain poorly understood. Clinicians should be alert to the possible onset of PML in patients receiving a DMT, even when lymphopenia is absent and immunoglobulin levels are normal. Early detection of PML may be facilitated by incorporating the determination of sNfL levels into routine clinical practice. CNS diseases other than MS, including PML, should be considered in the differential diagnosis when a rise in levels is not consistent with clinical symptoms.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical approval was not required for the studies involving humans because the ethical approval is not necessary in this case. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study and for publication this case report. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
RP-M: Conceptualization, Investigation, Project administration, Resources, Writing–original draft, Writing–review and editing. RC-C: Investigation, Resources, Writing–review and editing. MC-G: Investigation, Resources, Writing–review and editing. CD-A: Investigation, Resources, Writing–review and editing. LV-G: Resources, Validation, Writing–review and editing. FB: Visualization, Writing–review and editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
We thank the immunology department of the Ramon y Cajal University Hospital in Madrid, where the sNfL measurement was performed.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Bennett, C. L., Focosi, D., Socal, M. P., Bian, J. C., Nabhan, C., Hrushesky, W. J., et al. (2021). Progressive multifocal leukoencephalopathy in patients treated with rituximab: a 20-year review from the Southern Network on Adverse Reactions. Lancet Haematol. 8 (8), e593–e604. doi:10.1016/S2352-3026(21)00167-8
Bernard-Valnet, R., Koralnik, I. J., and Du Pasquier, R. (2021). Advances in treatment of progressive multifocal leukoencephalopathy. Ann. Neurol. 90 (6), 865–873. doi:10.1002/ana.26198
Bozic, C., Subramanyam, M., Richman, S., Plavina, T., Zhang, A., and Ticho, B. (2014). Anti-JC virus (JCV) antibody prevalence in the JCV Epidemiology in MS (JEMS) trial. Eur. J. Neurol. 21 (2), 299–304. doi:10.1111/ene.12304
Calabrese, L. H., Molloy, E. S., Huang, D., and Ransohoff, R. M. (2007). Progressive multifocal leukoencephalopathy in rheumatic diseases: evolving clinical and pathologic patterns of disease. Arthritis Rheum. 56 (7), 2116–2128. doi:10.1002/art.22657
Chapagain, M. L., and Nerurkar, V. R. (2010). Human polyomavirus JC (JCV) infection of human B lymphocytes: a possible mechanism for JCV transmigration across the blood-brain barrier. J. Infect. Dis. 202 (2), 184–191. doi:10.1086/653823
Cortese, I., Reich, D. S., and Nath, A. (2021). Progressive multifocal leukoencephalopathy and the spectrum of JC virus-related disease. Nat. Rev. Neurol. 17 (1), 37–51. doi:10.1038/s41582-020-00427-y
Dalla, C. G., Martinelli, V., Moiola, L., Sangalli, F., Colombo, B., Finardi, A., et al. (2019). Serum neurofilaments increase at progressive multifocal leukoencephalopathy onset in natalizumab-treated multiple sclerosis patients. Ann. Neurol. 85 (4), 606–610. doi:10.1002/ana.25437
Durali, D., de Goër de Herve, M. G., Gasnault, J., and Taoufik, Y. (2015). B cells and progressive multifocal leukoencephalopathy: search for the missing link. Front. Immunol. 6, 241. doi:10.3389/fimmu.2015.00241
Fissolo, N., Pignolet, B., Rio, J., Vermersch, P., Ruet, A., deSèze, J., et al. (2021). Serum neurofilament levels and PML risk in patients with multiple sclerosis treated with natalizumab. Neurol. Neuroimmunol. Neuroinflamm 8 (4), e1003. doi:10.1212/NXI.0000000000001003
Focosi, D., Tuccori, M., and Maggi, F. (2019). Progressive multifocal leukoencephalopathy and anti-CD20 monoclonal antibodies: what do we know after 20 years of rituximab. Rev. Med. Virol. 29 (6), e2077. doi:10.1002/rmv.2077
Khalil, M., Teunissen, C. E., Lehmann, S., Otto, M., Piehl, F., Ziemssen, T., et al. (2024). Neurofilaments as biomarkers in neurological disorders - towards clinical application. Nat. Rev. Neurol. 20 (5), 269–287. doi:10.1038/s41582-024-00955-x
Major, E. O., Amemiya, K., Elder, G., and Houff, S. A. (1990). Glial cells of the human developing brain and B cells of the immune system share a common DNA binding factor for recognition of the regulatory sequences of the human polyomavirus, JCV. JCV. J. Neurosci. Res. 27 (4), 461–471. doi:10.1002/jnr.490270405
Monaco, M. C., Atwood, W. J., Gravell, M., Tornatore, C. S., and Major, E. O. (1996). JC virus infection of hematopoietic progenitor cells, primary B lymphocytes, and tonsillar stromal cells: implications for viral latency. J. Virol. 70 (10), 7004–7012. doi:10.1128/JVI.70.10.7004-7012.1996
Patel, A., Sul, J., Gordon, M. L., Steinklein, J., Sanguinetti, S., Pramanik, B., et al. (2021). Progressive multifocal leukoencephalopathy in a patient with progressive multiple sclerosis treated with ocrelizumab monotherapy. JAMA Neurol. 78 (6), 736–740. doi:10.1001/jamaneurol.2021.0627
Puig-Casadevall, M., Álvarez-Bravo, G., Varela, A. Q., Robles-Cedeño, R., Sànchez Cirera, L., Miguela, A., et al. (2023). Progressive multifocal leukoencephalopathy in a patient with relapsing multiple sclerosis treated with ocrelizumab: a case report. Eur. J. Neurol. 30 (10), 3357–3361. doi:10.1111/ene.15988
Quintanilla-Bordás, C., Gorriz, D., Cubas-Núñez, L., Castillo-Villalba, J., Carreres-Polo, J., Casanova, B., et al. (2024). Elevation of serum neurofilament light-chain levels disclose possible occult progressive multifocal leukoencephalopathy and immune reconstitution syndrome in a patient receiving ozanimod: a case report. Front. Immunol. 15, 1465678. doi:10.3389/fimmu.2024.1465678
Rindi, L. V., Zaçe, D., Braccialarghe, N., Massa, B., Barchi, V., Iannazzo, R., et al. (2024). Drug-induced progressive multifocal leukoencephalopathy (PML): a systematic review and meta-analysis. Drug Saf. 47 (4), 333–354. doi:10.1007/s40264-023-01383-4
Schweitzer, F., Laurent, S., Cortese, I., Fink, G. R., Silling, S., Skripuletz, T., et al. (2023). Progressive multifocal leukoencephalopathy: pathogenesis, diagnostic tools, and potential biomarkers of response to therapy. Neurology 101 (16), 700–713. doi:10.1212/WNL.0000000000207622
Sharma, K., Tolaymat, S., Yu, H., Elkhooly, M., Jaiswal, S., Jena, A., et al. (2022). Progressive multifocal leukoencephalopathy in anti-CD20 and other monoclonal antibody (mAb) therapies used in multiple sclerosis: a review. J. Neurol. Sci. 443, 120459. doi:10.1016/j.jns.2022.120459
Keywords: John Cunningham virus, multiple sclerosis, neurofilament light chain, ocrelizumab, progressive multifocal leukoencephalopathy
Citation: Piñar-Morales R, Calle-Calle R, Carrasco-Garcia M, Davila-Arias C, Villar-Guimerans LM and Barrero Hernandez FJ (2025) Case Report: Neurofilament light chain in the follow up of progressive multifocal leukoencephalopathy in a patient with multiple sclerosis treated with ocrelizumab. Front. Pharmacol. 16:1571699. doi: 10.3389/fphar.2025.1571699
Received: 05 February 2025; Accepted: 24 March 2025;
Published: 09 April 2025.
Edited by:
Zubair Ahmed, University of Birmingham, United KingdomReviewed by:
Salvador Sierra, University of Michigan, United StatesCopyright © 2025 Piñar-Morales, Calle-Calle, Carrasco-Garcia, Davila-Arias, Villar-Guimerans and Barrero Hernandez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Piñar-Morales, cnBpbmFybW9yYWxlczAyQHVnci5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.