 Hua Luo
Hua Luo Shaohua Fan1†
Shaohua Fan1† Youfu He
Youfu He Jing Zhu
Jing Zhu Liwei Zhang
Liwei Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 06 March 2025
Sec. Experimental Pharmacology and Drug Discovery
Volume 16 - 2025 | https://doi.org/10.3389/fphar.2025.1534802
This article is part of the Research TopicAdvancing Glioma Treatment: Novel Drugs, Mechanisms of Resistance, and Therapeutic StrategiesView all 10 articles
Introduction: In gliomas, various oncogenic factors can lead to an imbalance between cell proliferation and apoptosis. Lomustine inhibits tumor cell growth by disrupting DNA replication and repair mechanisms. In contrast, temozolomide, an imidazole tetrazine compound, promotes cell apoptosis through DNA alkylation. The present study aimed to systematically analyze and compare the adverse drug reactions (ADRs) associated with lomustine and temozolomide, as reported in the World Health Organization (WHO) VigiAcess database.
Methods: Utilizing a retrospective descriptive analysis design, this study focused on two commercially available anti-glioma drugs. ADR reports pertaining to these medications were collected from the WHO-VigiAccess database. The data collection process involved gathering detailed information on various parameters, including age groups, gender, and geographical distribution of patients involved in the ADR reports. Additionally, the study examined the disease systems and symptoms reported alongside the adverse reactions, as recorded in the annual ADR summaries generated by the WHO. By calculating the proportion of adverse events reported for each drug, this investigation provided a comparative analysis of both the similarities and differences in the adverse reactions observed across the two anti-glioma drugs.
Results: At the time of the search, a total of 22,854 adverse events (AEs) associated with the two anti-glioma drugs were documented in the VigiAccess database. Lomustine exhibits a higher reporting rate concerning blood and lymphatic system disorders, gastrointestinal disorders, and hepatobiliary disorders. In contrast, Temozolomide has a higher reporting rate for general disorders and administration site conditions, nervous system disorders, and skin and subcutaneous tissue disorders. The top five types of AEs for anti-glioma drugs are as follows: general disorders and administration site conditions (8,825 cases, 38.61%), blood and lymphatic system disorders (7,369 cases, 32.24%), gastrointestinal disorders (5,614 cases, 24.56%), nervous system disorders (5,047 cases, 22.08%), and investigations (4,855 cases, 21.24%).
Conclusion: The present comparative observational study indicates that these inhibitors are associated with both common and specific adverse reactions, as documented in ADR reports. Clinicians should formulate individualized treatment plans that consider the adverse reactions linked to various drugs and the specific conditions of each patient, thereby promoting the rational use of these costly medications.
Glioma is the most prevalent primary intracranial tumor, accounting for approximately 30% of all brain and central nervous system tumors and 80% of all malignant brain tumors (Gusyatiner and Hegi, 2018; Xu et al., 2020). According to the current classification by the World Health Organization, gliomas are categorized into four histological grades, which can be further divided into low-grade (Grades I and II) and high-grade (Grades III and IV) tumors. Glioblastoma (GBM) is the most common high-grade glioma, constituting 45.2% of primary malignant brain tumors and central nervous system (CNS) tumors (Louis et al., 2021). GBM is an intractable disease, with a median survival of merely 15 months; only 5.5% of patients survive 5 years after diagnosis. In individuals aged 65 and older, the incidence rate has been shown to rise to 130 cases per million (Kanderi et al., 2024). The pathogenesis of glioma remains elusive; however, two identified risk factors include exposure to high doses of ionizing radiation and high-penetrance genetic mutations associated with rare syndromes. Additionally, carcinogenic factors such as nitrite-containing foods and viral or bacterial infections may also contribute to the development of glioma. The principal clinical manifestations of glioma include increased intracranial pressure, neurological and cognitive dysfunction, and epileptic seizures.
The highly aggressive nature of gliomas and their resistance to traditional treatments present significant challenges for patients. In gliomas, multiple oncogenic factors can create an imbalance between cell proliferation and apoptosis. Researchers are increasingly focusing on individualized treatment plans as their understanding of the biology of gliomas deepens. Among various treatment modalities, the chemotherapy drugs lomustine and temozolomide have garnered considerable attention due to their notable efficacy in glioma treatment. Lomustine is a nitrosourea and an oral alkylating agent. Upon entering the body, lomustine requires hepatic activation to form active intermediates that can modify purine bases in DNA. This modification inhibits DNA, RNA, and protein synthesis, ultimately inducing programmed cell death in rapidly dividing cells (National Institute of Diabetes and Digestive and Kidney Diseases, 2012; Guo et al., 2021). Temozolomide is an alkylating prodrug and a chemotherapeutic agent that can cross the blood-brain barrier. The brain tumor microenvironment is typically alkaline, rendering temozolomide unstable. Temozolomide spontaneously decomposes to form an active metabolite that methylates purine bases in DNA, thereby causing cellular damage and ultimately inducing apoptosis (Zhou et al., 2022; Zhang et al., 2012). Both drugs are extensively utilized in clinical practice for the radiotherapy treatment of tumors. Data from clinical trials have demonstrated that the combination of lomustine and temozolomide is more effective than either drug alone in patients with glioblastoma, resulting in prolonged average survival (Herrlinger et al., 2019). However, despite the achievements of lomustine and temozolomide in clinical settings, their adverse drug reactions (ADRs) (refer to adverse reactions that are directly induced by the drug) must not be overlooked. Adverse reactions not only affect the patient’s treatment experience but may also limit the dosage and efficacy of the drugs, potentially leading to treatment discontinuation. Therefore, a comprehensive and thorough analysis of the adverse reactions associated with these drugs is crucial for optimizing treatment regimens and enhancing treatment safety and tolerability. The existing literature primarily focuses on animal studies, mechanisms of action, and adverse events in small clinical trial samples of lomustine and temozolomide. However, no studies have yet analyzed the combined safety profile of lomustine and temozolomide using large-scale, real-world data. The present study aims to systematically analyze and compare the ADRs related to lomustine and temozolomide as reported in the World Health Organization (WHO) VigiAcess database, with the goal of identifying the antiglioma drug with the lowest risk for individualized use in clinical patients, thereby providing a valuable reference for clinical treatment.
Despite the thoroughness of pre-marketing clinical trials, the safety of these medications remains partially undefined based on data from pre-authorization studies, as these trials are conducted under controlled conditions that differ from everyday practice (Gagliardi et al., 2022). Lomustine and temozolomide, which have been commercially available for a significant period, serve a large patient demographic and have multiple applications. Therefore, it is particularly important and insightful to conduct safety research utilizing extensive data from real-world scenarios. Consequently, a more detailed characterization of ADRs linked to anti-glioma drugs is essential, leveraging spontaneous reports from pharmacovigilance databases. It is noteworthy that there is a lack of comparative studies examining the similarities and disparities in ADRs caused by these drugs. Since 2015, data archived in VigiBase has been made publicly accessible through VigiAccess (Watson et al., 2018; Habarugira and Figueras, 2021).
The VigiAccess database enables searches using the trade names of drugs, while also identifying the active ingredients and presenting the corresponding results of ADR reports. This research primarily examines two anti-glioma drugs used for treating glioma: lomustine and temozolomide. Clinicians frequently need to tailor treatment choices considering the potential risk of adverse events for each patient. To assess the occurrence of adverse reactions associated with these two drugs, we performed a descriptive study that analyzed spontaneously reported adverse reactions in the VigiAccess database and compared the rates of adverse reactions linked to these two medications.
Table 1 presents the general information regarding the two anti-glioma drugs available for clinical treatment in our study.
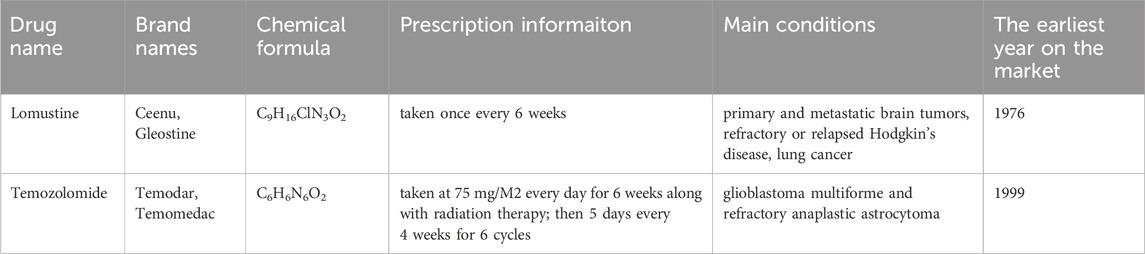
Table 1. General information of two anti-glioma drugs.
Lomustine is likely the second most widely used drug for glioma treatment, following temozolomide. Also known as CCNU (chloroethyl-cyclohexyl-nitrosourea), lomustine is an alkylating agent that belongs to the nitrosourea family. It functions as a monofunctional alkylating agent, capable of alkylating both DNA and RNA, and can induce cross-linking of DNA, thereby acting in both cell cycle-dependent and -independent manners. A significant lesion induced by lomustine is the formation of O6-chloroethylguanine, which can be reversed by O6-methylguanine DNA methyltransferase (MGMT) (Strobel et al., 2019). Additionally, lomustine may inhibit enzymatic functions through the carbamoylation of amino acids; however, the clinical significance of this activity remains unclear. As a lipid-soluble drug, lomustine effectively permeates the blood-brain barrier, making it a suitable candidate for the chemotherapy of intrinsic brain tumors (de Gooijer et al., 2018).
Temozolomide is an imidazole tetrazine prodrug that remains stable at acidic pH and undergoes spontaneous non-enzymatic hydrolysis at neutral or slightly alkaline pH. It can be administered both orally and intravenously. Following absorption, it is rapidly converted into the active compound 5-(3-methyltriazen-1-yl) imidazole-4-carboxamide (MTIC) through non-enzymatic pathways. MTIC subsequently reacts with water to yield 5-aminoimidazole-4-carboxylamine (AIC) and the highly reactive methyldiazonium cation. These methyldiazonium cations are notably reactive and can methylate the adenine and guanine bases in DNA, primarily at the O6 and N7 positions of guanine. The repair of O6-methylguanine (O6-MeG) is facilitated by MGMT (Lips and Kaina, 2001). When MGMT activity is diminished or absent, O6-MeG mispairs with thymine, thereby activating the DNA mismatch repair (MMR) pathway (Zhang et al., 2012; Strobel et al., 2019). This activation may lead to ineffective repair cycles, resulting in DNA chain breaks and ultimately cell apoptosis.
Despite challenges such as incomplete data, misinformation, delayed reporting, and regional concentration of reports, spontaneous reporting systems remain a valuable source for obtaining real-world data on drug and vaccine safety, comparing treatment regimens, and elucidating the underlying mechanisms of ADRs (Hazell and Shakir, 2006). The WHO-VigiAccess database was searched on 8 November 2024, to collect all documented adverse events following the introduction of two anti-glioma drugs. The access URL is https://www.vigiaccess.org. All pharmaceutical agents under study were identified using their generic names. Data collection encompassed various age ranges, genders, years of reporting, and geographic regions, as detailed by WHO-VigiAccess. Descriptive statistics were computed using Excel 2021.
WHO-VigiAccess serves as an open-access portal to the PIDM database, facilitating the retrieval of safety reports concerning medicinal products provided by the UMC. The evaluation relied on system organ class (SOC) and preferred terms (PTs) as defined by the Medical Dictionary for Regulatory Activities (MedDRA). Consequently, records for each drug were compiled, and all distinct adverse events (AEs) (refer to all adverse reactions that occur after taking a drug) identified at the MedDRA SOC and PT levels were specified to delineate the range of toxicities. The reporting terms utilized in MedDRA were gathered from various dictionaries, including the WHO Adverse Reaction Terminology (WHO-ART) and others (Sultana et al., 2020). In total, 27 items were categorized by SOC. This research focused on the PTs, which represent the extent of publicly available information in the VigiBase database through WHO-VigiAccess. To assess the results of the identified safety signals, we organized them using outcome codes, culminating in three critical categories: death, hospitalization, and major events, which encompass life-threatening occurrences, disabilities, and congenital anomalies.
Statistical Evaluation: A retrospective quantitative approach was adopted for this study. Descriptive analysis was conducted using Excel to assess the characteristics of victims who experienced adverse reactions from the two medications. The rate of ADR reporting for each medication was determined by dividing the number of ADR symptoms associated with that specific drug by the total number of ADR reports. The common ADRs linked to each medication were identified as the symptoms corresponding to the top 20 ADR report rates. Following this, the reported ADR symptoms for each drug were calculated, and a descriptive comparative analysis was performed. Frequencies and percentages were utilized to classify the descriptive variables.
The initial documentation of negative reactions to lomustine and temozolomide was recorded in the WHO-VigiAccess database in 1976 and 1997, respectively. As of 2024, the WHO has accumulated a total of 1,647 and 21,207 reports of ADRs for these two medications, resulting in an aggregate of 22,854 reports. Among these 22,854 ADR reports associated with the two anti-glioma drugs, as detailed in Table 1, there were 2,445 instances where the sex of the subjects was not specified. Notably, the number of ADR reports from men (10,100) was approximately equal to that of women (9,980), yielding a female-to-male ratio of nearly 1:1, which indicates a relatively balanced distribution. Excluding reports that lacked age information, the demographic groups with the highest rates of reported incidents were primarily those aged between 45 and 64 years. Furthermore, the majority of adverse events were reported from the Americas, accounting for 62.10% of the overall total. Table 2 provides additional details regarding the reporting years for each of the medications analyzed.
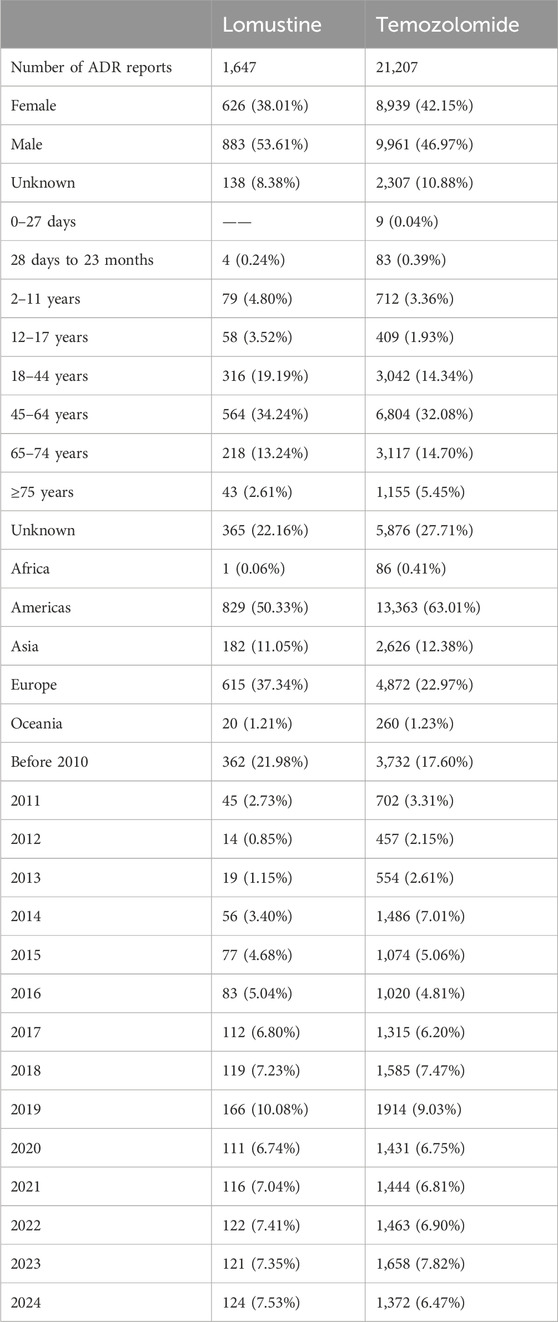
Table 2. Characteristics of ADR reports of two anti-glioma drugs.
Table 3 presents the reporting frequencies of 27 SOCs associated with two anti-glioma drugs. Lomustine exhibits a higher reporting rate for blood and lymphatic system disorders, gastrointestinal disorders, and hepatobiliary disorders. Conversely, Temozolomide shows a higher reporting rate for general disorders and administration site conditions, nervous system disorders, and skin and subcutaneous tissue disorders. Furthermore, the number of ADRs exceeding 10% within each SOC was eight for lomustine and nine for temozolomide.
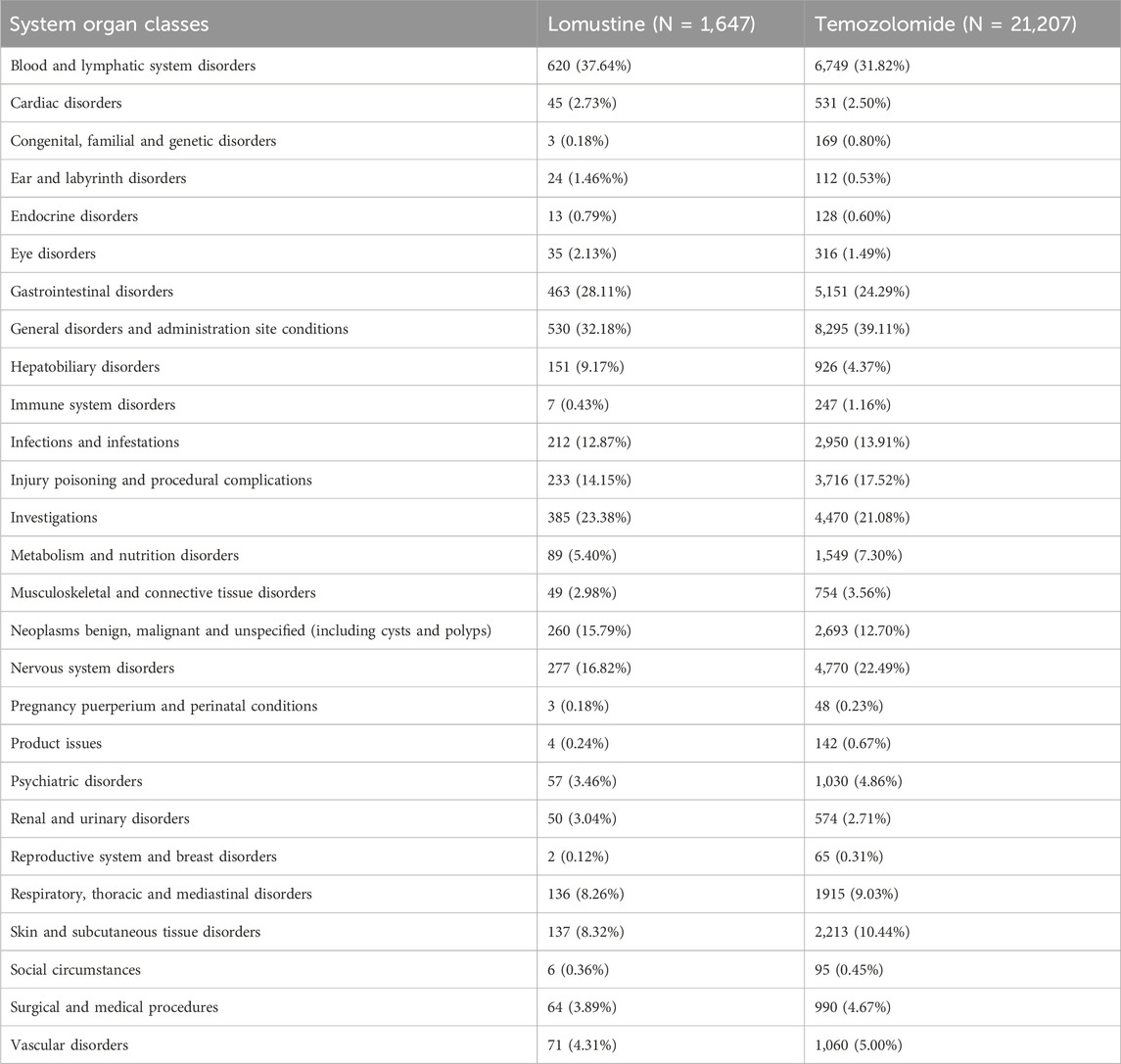
Table 3. ADR number and report rate of 27 SOCs of two anti-glioma drugs.
The five most common types of AEs related to anti-glioma drugs are as follows: general disorders and administration site conditions (8,825 cases, 38.61%), blood and lymphatic system disorders (7,369 cases, 32.24%), gastrointestinal disorders (5,614 cases, 24.56%), nervous system disorders (5,047 cases, 22.08%), and investigations (4,855 cases, 21.24%).
Table 4 presents the 20 most frequently reported ADRs associated with the two drugs. The manifestations listed are preferred terms categorized within the SOC. The commonly observed ADRs for both anti-glioma drugs include thrombocytopenia, vomiting, death, nausea, leukopenia, decreased platelet count, neutropenia, disease progression, seizures, fatigue, malignant neoplasm progression, pancytopenia, diarrhea, off-label use, pyrexia, use in unapproved indications, and drug ineffectiveness.
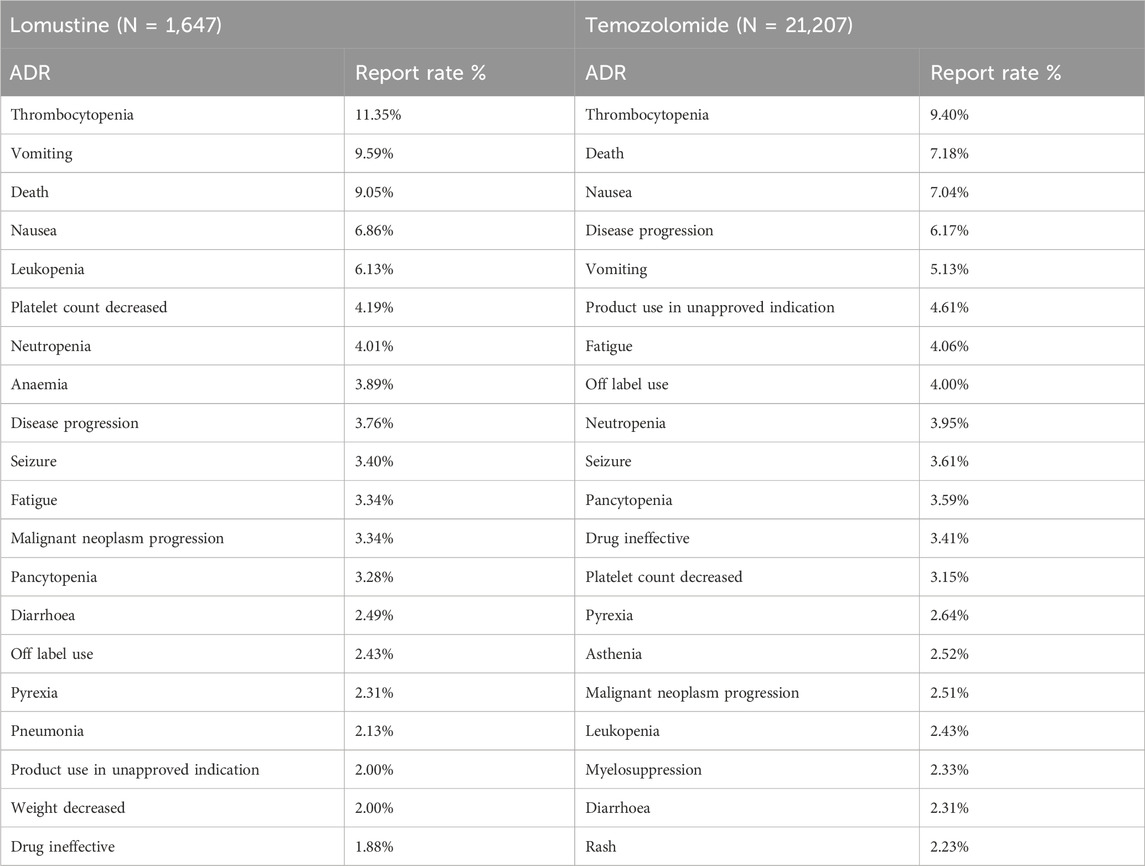
Table 4. Top 20 ADRs of two anti-glioma drugs.
Lomustine and temozolomide exhibit certain similarities in their adverse reactions. Both drugs significantly affect the hematological system and gastrointestinal tract, and they are associated with disease progression and mortality. However, notable differences exist in the incidence of specific adverse reactions: Lomustine is more likely to cause thrombocytopenia, while temozolomide is associated with a higher incidence of nausea and vomiting. Furthermore, off-label use and applications for unapproved indications were frequently noted in reports for both drugs, suggesting potential issues with appropriate use and the risks associated with their administration outside the approved scope.
Through WHO-VigiAccess, we can identify significant adverse events associated with anti-glioma drugs, including life-threatening occurrences, disabilities, and congenital malformations. The proportions of serious adverse reactions reported for lomustine and temozolomide were 9.96% and 8.34%, respectively (Figure 1).
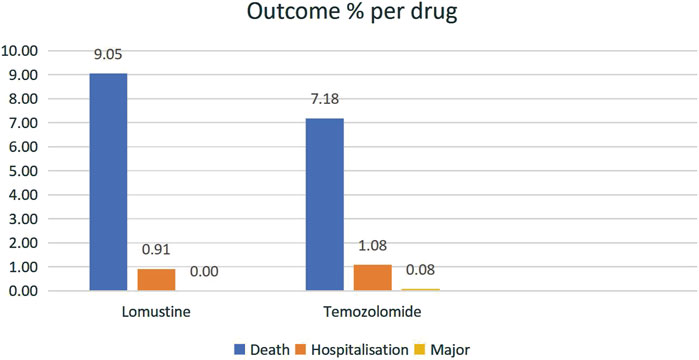
Figure 1. The proportions of serious adverse reactions reported for lomustine and temozolomide.
By examining the top 20 ADRs associated with each anti-glioma drug within the SOCs, a cumulative total of 214 identical signals was identified across the two anti-glioma drugs. All overlapping signals are detailed in Table 5. General disorders and administration site conditions emerged as the SOC with the largest number of adverse signals, with the five most frequently reported reactions being chills, no adverse event, treatment failure, asthenia, and condition aggravated. Following this, nervous system disorders ranked as the second most prevalent SOC, featuring the top five reactions of ataxia, cognitive disorder, cerebrovascular accident, speech disorder, and cerebral hemorrhage.
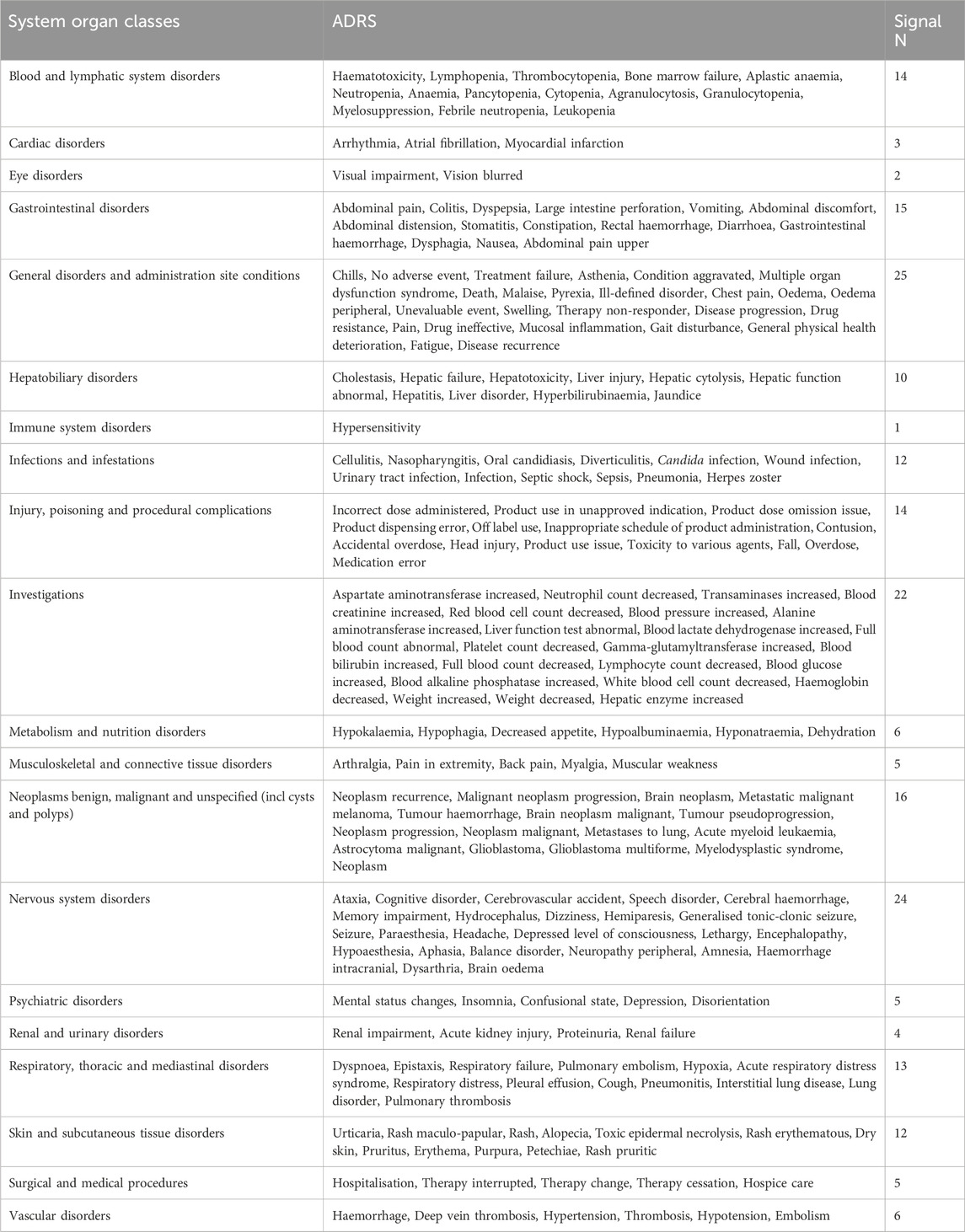
Table 5. Same ADRs between two anti-glioma drugs.
When comparing the top 20 ADRs reported by the two anti-glioma drugs, there are 25 differences at the PTs level (Table 6). Among these, the two drugs exhibit the highest number of infections and infestations, totaling 25. The top five adverse reactions reported by lomustine include mycobacterium chelonae infection, influenza, bacteraemia, oral fungal infection, and pseudomonas infection. In contrast, the top five adverse reactions reported by temozolomide are pneumocystis jirovecii infection, meningitis, herpes simplex encephalitis, neutropenic sepsis, and pneumocystis jirovecii pneumonia. Furthermore, regarding neoplasms—benign, malignant, and unspecified (including cysts and polyps)—lomustine reports the top five adverse reactions as non-Hodgkin’s lymphoma, basal cell carcinoma, acute myelomonocytic leukaemia, chronic myelomonocytic leukaemia, and myelofibrosis, while temozolomide reports its top five adverse reactions as metastases to the central nervous system, metastases to bone, tumour necrosis, malignant melanoma, and metastases to the liver.
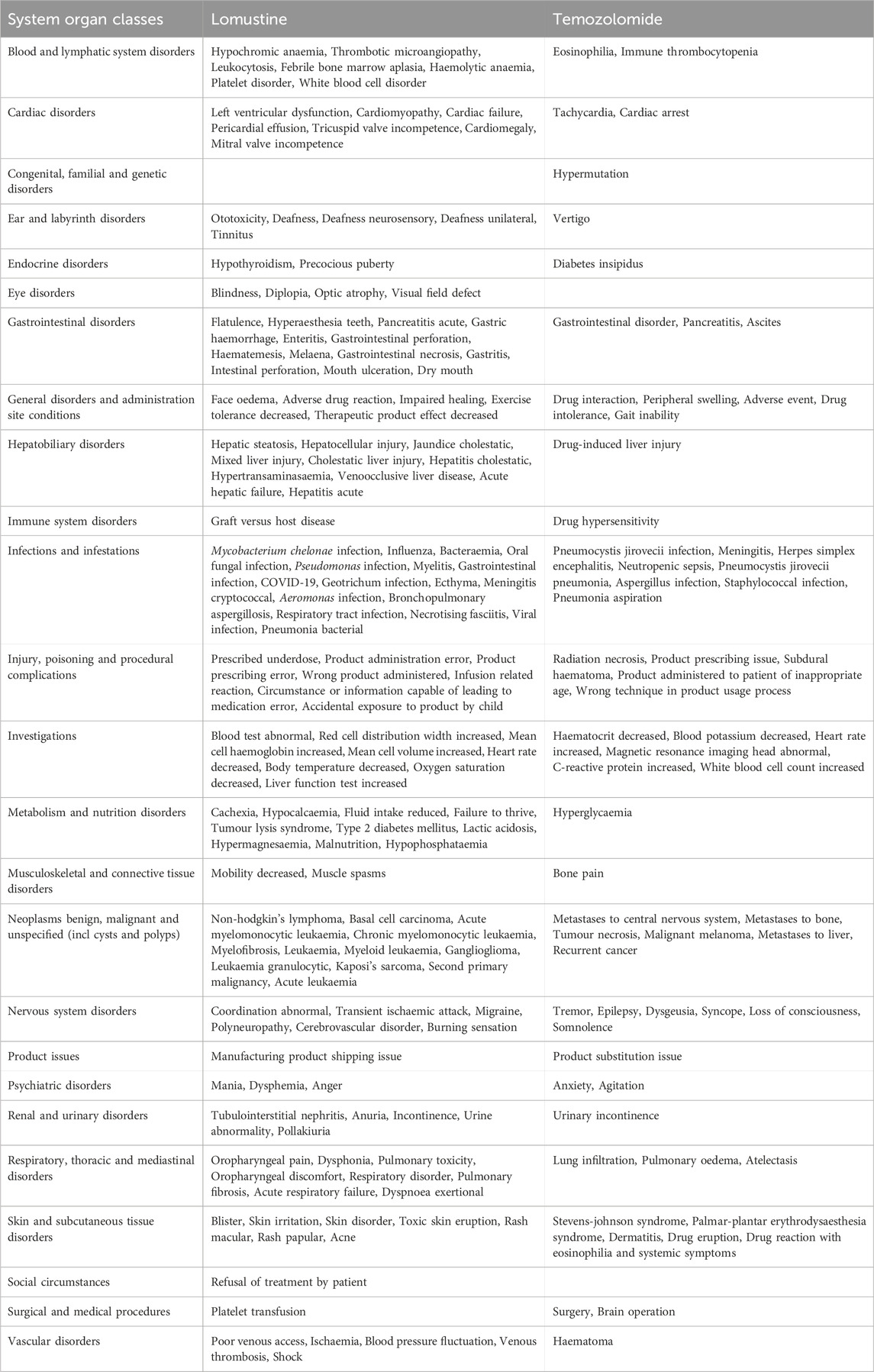
Table 6. Different ADRs bwtween two anti-glioma drugs.
The Spontaneous Reporting System (SRS) is widely employed in pharmacovigilance to assess the safety of suspected adverse events. Clinical trials are subject to limitations, including rigorous designs, stringent enrollment criteria, restricted sample sizes, and short follow-up durations, which may hinder the accurate reflection of real-world scenarios characterized by diverse patient demographics and comorbidities. Consequently, data derived from the SRS database can more effectively illustrate the safety of specific drugs in real-world settings and plays a crucial role in signal detection. Currently, research on the safety signals of numerous drugs primarily relies on three key databases: the EudraVigilance Data Analysis System (EVDAS), the Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS), and WHO-VigiBase® (Vogel et al., 2020). In 2015, the WHO introduced WHO-VigiAccess, which provides public access to the information contained in VigiBase®, the WHO’s global repository of reported potential adverse effects associated with medicinal products. Analyzing data from the WHO-VigiAccess database can reveal previously unknown associations between drugs and AEs, as well as validate some established clinical connections (Yamoah et al., 2022). This study aims to evaluate the post-market adverse events linked to two anti-glioma drugs using the WHO-VigiAccess database.
According to data from WHO-VigiAccess, 62.10% of adverse events related to these two anti-glioma drugs were reported from the Americas, followed by Europe, while Africa reported the lowest incidence of adverse events. Prior research has highlighted a significant issue regarding the low reporting rates of adverse events in both Africa and Oceania (Gidudu et al., 2020; Alawadhi et al., 2012). In South Africa, a shortage of medical understanding concerning biopharmaceuticals among healthcare workers, coupled with high costs and complicated procurement procedures, further exacerbates the challenges associated with the use of these medications (Gidudu et al., 2020; Martelli et al., 2017; Kvamme et al., 2020). The African region has been noted for having the lowest incidence of reported adverse events, which may be attributed to insufficient social mobilization, restricted access to adverse event reporting mechanisms, and low levels of information system coverage.
The number of ADR reports from men (10,100) was approximately equal to that of women (9,980), resulting in a female-to-male ratio of nearly 1:1, which indicates a relatively balanced distribution. When excluding reports lacking information on age, the demographic groups with the highest rates of reported incidents were primarily those aged between 45 and 64 years. An AE)with a reporting rate of 1% or greater is generally considered common (Chen et al., 2019). Major adverse events associated with anti-glioma drugs include life-threatening incidents, disabilities, and congenital malformations. The mortality rates for lomustine and temozolomide are 9.96% and 8.34%, respectively. Lomustine exhibits a higher reporting rate for blood and lymphatic system disorders, gastrointestinal disorders, and hepatobiliary disorders. Conversely, temozolomide has a higher reporting rate for general disorders and administration site conditions, as well as nervous system disorders and skin and subcutaneous tissue disorders. Through the VigiAccess database, we identified the top five adverse reactions related to lomustine: thrombocytopenia (11.35%), vomiting (9.59%), death (9.05%), nausea (6.86%), and leukopenia (6.13%). For temozolomide, the top five adverse reactions are thrombocytopenia (9.40%), death (7.18%), nausea (7.04%), disease progression (6.17%), and vomiting (5.13%). The frequently observed ADRs for both anti-glioma drugs include thrombocytopenia, vomiting, death, nausea, leukopenia, decreased platelet count, neutropenia, disease progression, seizures, fatigue, malignant neoplasm progression, pancytopenia, diarrhea, off-label use, pyrexia, product use in unapproved indications, and drug ineffectiveness.
Lomustine is an emetogenic chemotherapy drug that typically necessitates standard antiemetic precautions, which are generally effective. Thrombocytopenia is the primary toxic reaction associated with this treatment, often leading to dosage reductions, delays in chemotherapy cycles, or even cessation of therapy. Neutropenia and lymphopenia occur less frequently and are generally less severe. Despite this toxic profile, the development of myelodysplastic syndromes and leukemias as sequelae of lomustine chemotherapy is rare. This rarity is presumably due to the limited life expectancy of glioma patients, which decreases the likelihood of complications arising years after exposure to the drug (Czarnywojtek et al., 2023).
The adverse reactions associated with temozolomide are typically classified as NCI common toxicity criteria (CTC) grade 1 or 2 (mild to moderate) and are generally self-limiting. Nausea and vomiting can be effectively managed with antiemetics. The incidence of severe nausea and vomiting (CTC grade 3 or 4) has been reported at 10% and 6%, respectively (Matsuda et al., 2015; Bae et al., 2014). The primary dose-limiting toxicity of temozolomide is myelosuppression, which can occur at any dose but tends to be more pronounced at higher doses (Ortiz et al., 2021). Patients receiving higher doses have experienced adverse reactions such as severe and prolonged myelosuppression, infections, and, in some cases, death. Patients who experience an overdose should have their complete blood counts monitored and receive supportive care as necessary.
Undoubtedly, this study has certain limitations. Firstly, the voluntary nature of the spontaneous reporting system leads to issues such as irregular recording, incorrect reporting, delayed reporting, and incomplete data, all of which complicate data analysis and affect the results. For example, this study lacks data on gender, age, and region, and there is a notable absence of reports from Africa. Therefore, the conclusions and data presented here may not be generalizable to all populations. Secondly, the WHO-VigiAccess database contains cumulative data for drugs since their market introduction, but it does not provide annual ADR data. The 13-year difference in market introduction between the two drugs limits our ability to conduct a more in-depth analysis of the data. In addition, the relatively short life expectancy associated with glioma often precludes the opportunity to observe long-term complications that may arise after several years of drug treatment.
The WHO-VigiAccess database, which operates on a voluntary basis for adverse event reporting, presents several challenges that hinder its ability to provide a complete and thorough count of adverse events. The database may lack essential information regarding reported incidents, highlighting the need to enhance the transparency of reporting practices. By improving the clarity and accessibility of the data available to the public, stakeholders can engage in more effective screening for potential connections between pharmaceuticals and adverse reactions. This enhancement would also help mitigate misguidance that could arise from incomplete or unclear information. The reliance on a spontaneous reporting system carries significant inherent limitations, primarily due to various biases that can affect the reporting process. These biases include notoriety bias, where more well-known drugs receive disproportionate attention, selection bias, which skews the data towards certain demographics, and under-reporting, which typically results in substantial gaps in data collection (Faillie, 2019). In the context of the current study, it was noted that the missing data included adverse events that could not be specifically linked to certain genders or age groups, complicating the interpretation of the data. Additionally, the cumulative nature of the VigiAccess database presents challenges in isolating ADRs on a yearly basis. When medications are introduced to the market at different times, the volume of reported ADRs can vary significantly, complicating efforts to compare signal differences across all drug classes concurrently. Consequently, conducting further data mining becomes impractical. In this analysis, the focus was placed on aggregating the number of ADRs reported over recent years and correlating these with the number of PTs associated with various drugs. This approach was designed to mitigate the impact of the differing timelines of drug market introductions on the study’s outcomes. However, the findings are limited to relative comparisons involving only the two anti-glioma drugs examined in the study.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
HL: Writing–original draft, Writing–review and editing. SF: Writing–original draft, Writing–review and editing. LL: Writing–original draft, Writing–review and editing. YH: Investigation, Writing–original draft, Project administration, Software. JC: Writing–original draft, Writing–review and editing. CX: Writing–original draft, Writing–review and editing. JZ: Writing–original draft, Writing–review and editing. LZ: Writing–original draft, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Natural Science Foundation of China (82202738), Taizhou Social Development Science and Technology Project (23ywb09, 24ywb04, 22ywa06), and Traditional Chinese Medicine Science and Technology Project of Zhejiang Province (2024ZL194).
We are grateful to all individuals and organizations that have provided support for this research, including financial sponsors and technical assistance who participated in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alawadhi, A., Alawneh, K., and Alzahrani, Z. A. (2012). The effect of neutralizing antibodies on the sustainable efficacy of biologic therapies: what's in it for African and Middle Eastern rheumatologists. Clin. Rheumatol. 31 (9), 1281–1287. doi:10.1007/s10067-012-2040-2
Bae, S. H., Park, M. J., Lee, M. M., Kim, T. M., Lee, S. H., Cho, S. Y., et al. (2014). Toxicity profile of temozolomide in the treatment of 300 malignant glioma patients in Korea. J. Korean Med. Sci. 29 (7), 980–984. doi:10.3346/jkms.2014.29.7.980
Chen, C., Borrego, M. E., Roberts, M. H., and Raisch, D. W. (2019). Comparison of post-marketing surveillance approaches regarding infections related to tumor necrosis factor inhibitors (TNFi's) used in treatment of autoimmune diseases. Expert Opin. Drug Saf. 18 (8), 733–744. doi:10.1080/14740338.2019.1630063
Chen, R., Smith-Cohn, M., Cohen, A. L., and Colman, H. (2017). Glioma subclassifications and their clinical significance. Neurotherapeutics 14 (2), 284–297. doi:10.1007/s13311-017-0519-x
Czarnywojtek, A., Borowska, M., Dyrka, K., Van Gool, S., Sawicka-Gutaj, N., Moskal, J., et al. (2023). Glioblastoma multiforme: the latest diagnostics and treatment techniques. Pharmacology 108 (5), 423–431. doi:10.1159/000531319
de Gooijer, M. C., de Vries, N. A., Buckle, T., Buil, L. C. M., Beijnen, J. H., Boogerd, W., et al. (2018). Improved brain penetration and antitumor efficacy of temozolomide by inhibition of ABCB1 and ABCG2. Neoplasia 20 (7), 710–720. doi:10.1016/j.neo.2018.05.001
Faillie, J. L. (2019). Case-non-case studies: principle, methods, bias and interpretation. Therapie 74 (2), 225–232. doi:10.1016/j.therap.2019.01.006
Gagliardi, A., Iaquinta, F. S., Grembiale, R. D., De Sarro, C., Fabiano, A., Fraija, D., et al. (2022). Real-world safety profile of biologics used in rheumatology: a six-year observational pharmacovigilance study in the calabria region. Pharmaceutics 14 (11), 2328. doi:10.3390/pharmaceutics14112328
Gidudu, J. F., Shaum, A., Dodoo, A., Bosomprah, S., Bonsu, G., Amponsa-Achiano, K., et al. (2020). Barriers to healthcare workers reporting adverse events following immunization in four regions of Ghana. Vaccine 38 (5), 1009–1014. doi:10.1016/j.vaccine.2019.11.050
Guo, X., Sun, Z., Jiang, S., Jin, X., and Wang, H. (2021). Identification and validation of a two-gene metabolic signature for survival prediction in patients with kidney renal clear cell carcinoma. Aging (Albany NY) 13 (6), 8276–8289. doi:10.18632/aging.202636
Gusyatiner, O., and Hegi, M. E. (2018). Glioma epigenetics: from subclassification to novel treatment options. Semin. Cancer Biol. 51, 50–58. doi:10.1016/j.semcancer.2017.11.010
Habarugira, J. M. V., and Figueras, A. (2021). Pharmacovigilance network as an additional tool for the surveillance of antimicrobial resistance. Pharmacoepidemiol Drug Saf. 30 (8), 1123–1131. doi:10.1002/pds.5249
Hazell, L., and Shakir, S. A. (2006). Under-reporting of adverse drug reactions: a systematic review. Drug Saf. 29 (5), 385–396. doi:10.2165/00002018-200629050-00003
Herrlinger, U., Tzaridis, T., Mack, F., Steinbach, J. P., Schlegel, U., Sabel, M., et al. (2019). Lomustine-temozolomide combination therapy versus standard temozolomide therapy in patients with newly diagnosed glioblastoma with methylated MGMT promoter (CeTeG/NOA-09): a randomised, open-label, phase 3 trial. Lancet 393 (10172), 678–688. doi:10.1016/S0140-6736(18)31791-4
Kanderi, T., Munakomi, S., and Gupta, V. (2024). “Glioblastoma multiforme,” in StatPearls (St. Petersburg, FL: StatPearls Publishing).
Kvamme, M. K., Lie, E., Uhlig, T., Moger, T. A., Kvien, T. K., and Kristiansen, I. S. (2020). Cost-effectiveness of TNF inhibitors vs synthetic disease-modifying antirheumatic drugs in patients with rheumatoid arthritis: a Markov model study based on two longitudinal observational studies. Rheumatol. Oxf. 59 (4), 917. doi:10.1093/rheumatology/kez609
Lips, J., and Kaina, B. (2001). Repair of O(6)-methylguanine is not affected by thymine base pairing and the presence of MMR proteins. Mutat. Res. 487 (1-2), 59–66. doi:10.1016/s0921-8777(01)00105-7
Louis, D. N., Perry, A., Wesseling, P., Brat, D. J., Cree, I. A., Figarella-Branger, D., et al. (2021). The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol. 23 (8), 1231–1251. doi:10.1093/neuonc/noab106
Martelli, L., Olivera, P., Roblin, X., Attar, A., and Peyrin-Biroulet, L. (2017). Cost-effectiveness of drug monitoring of anti-TNF therapy in inflammatory bowel disease and rheumatoid arthritis: a systematic review. J. Gastroenterol. 52 (1), 19–25. doi:10.1007/s00535-016-1266-1
Matsuda, M., Yamamoto, T., Ishikawa, E., Nakai, K., Akutsu, H., Onuma, K., et al. (2015). Profile analysis of chemotherapy-induced nausea and vomiting in patients treated with concomitant temozolomide and radiotherapy: results of a prospective study. Neurol. Med. Chir. (Tokyo) 55 (9), 749–755. doi:10.2176/nmc.oa.2014-0413
National Institute of Diabetes and Digestive and Kidney Diseases (2012). Livertox: clinical and research information on drug-induced liver injury. Bethesda (MD): National Institute of Diabetes And Digestive and Kidney Diseases.
Ortiz, R., Perazzoli, G., Cabeza, L., Jiménez-Luna, C., Luque, R., Prados, J., et al. (2021). Temozolomide: an updated overview of resistance mechanisms, nanotechnology advances and clinical applications. Curr. Neuropharmacol. 19 (4), 513–537. doi:10.2174/1570159X18666200626204005
Strobel, H., Baisch, T., Fitzel, R., Schilberg, K., Siegelin, M. D., Karpel-Massler, G., et al. (2019). Temozolomide and other alkylating agents in glioblastoma therapy. Biomedicines 7 (3), 69. doi:10.3390/biomedicines7030069
Sultana, J., Scondotto, G., Cutroneo, P. M., Morgante, F., and Trifirò, G. (2020). Intravitreal anti-VEGF drugs and signals of dementia and Parkinson-like events: analysis of the VigiBase database of spontaneous reports. Front. Pharmacol. 11, 315. doi:10.3389/fphar.2020.00315
Vogel, U., van Stekelenborg, J., Dreyfus, B., Garg, A., Habib, M., Hosain, R., et al. (2020). Investigating overlap in signals from EVDAS, FAERS, and VigiBase®. Drug Saf. 43 (4), 351–362. doi:10.1007/s40264-019-00899-y
Watson, S., Chandler, R. E., Taavola, H., Härmark, L., Grundmark, B., Zekarias, A., et al. (2018). Safety concerns reported by patients identified in a collaborative signal detection workshop using VigiBase: results and reflections from lareb and uppsala monitoring centre. Drug Saf. 41 (2), 203–212. doi:10.1007/s40264-017-0594-2
Xu, S., Tang, L., Li, X., Fan, F., and Liu, Z. (2020). Immunotherapy for glioma: current management and future application. Cancer Lett. 476, 1–12. doi:10.1016/j.canlet.2020.02.002
Yamoah, P., Mensah, K. B., Attakorah, J., Padayachee, N., Oosthuizen, F., and Bangalee, V. (2022). Adverse events following immunization associated with coronavirus disease 2019 (COVID-19) vaccines: a descriptive analysis from VigiAccess. Hum. Vaccin Immunother. 18 (6), 2109365. doi:10.1080/21645515.2022.2109365
Zhang, J., Stevens, M. F., and Bradshaw, T. D. (2012). Temozolomide: mechanisms of action, repair and resistance. Curr. Mol. Pharmacol. 5 (1), 102–114. doi:10.2174/1874467211205010102
Keywords: glioma, adverse drug reactions, WHO-VigiAccess, lomustine, temozolomide
Citation: Luo H, Fan S, Liang L, He Y, Chen J, Xu C, Zhu J and Zhang L (2025) Adverse event profile of lomustine and temozolomide: a descriptive analysis from WHO-VigiAccess. Front. Pharmacol. 16:1534802. doi: 10.3389/fphar.2025.1534802
Received: 26 November 2024; Accepted: 17 February 2025;
Published: 06 March 2025.
Edited by:
Zhenyu Gong, Technical University of Munich, GermanyReviewed by:
Faisal Imam, King Saud University, Saudi ArabiaCopyright © 2025 Luo, Fan, Liang, He, Chen, Xu, Zhu and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Zhu, amluZy56aHVAbmp1Y20uZWR1LmNu; Liwei Zhang, bWVkemx3QHNpbmEuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.