 L. Gómez-Ganda1†C. J. Parramón-Teixidó1*†
L. Gómez-Ganda1†C. J. Parramón-Teixidó1*† G. Giralt-García2†C. Fernández-García3†Q. Ferrer-Menduiña2†
G. Giralt-García2†C. Fernández-García3†Q. Ferrer-Menduiña2† M. J. Cabañas-Poy1†
M. J. Cabañas-Poy1†- 1Pharmacy Department, Vall d’Hebron University Hospital, Barcelona, Spain
- 2Pediatric Cardiology Department, Vall d’Hebron University Hospital, Barcelona, Spain
- 3Neonatology Department, Vall d’Hebron University Hospital, Barcelona, Spain
Background: Although heart failure (HF) and supraventricular tachycardias (SVT) are associated with high morbidity and mortality in pediatrics, especially, in children under 6 months; the efficacy of available treatments is limited, requiring the use of off-label therapies. The aim of the study is to investigate the efficacy, dosage, and safety of off-label ivabradine in patients under 6 months of age with HF or SVT.
Methods: Retrospective observational study, which included patients under 6 months of age with HF or SVT who received ivabradine between January 2020 - May 2024. Demographic, clinical, and treatment-related variables were collected. Response variables were established according to indication, HF: heart rate (HR) and left ventricular ejection fraction (LVEF); SVT: HR.
Results: Thirteen patients (nine women) with a median age of 1.4 (1-4) months were included. Ivabradine was discontinued in five of the seven HF patients due to resolution of HF, control of HR, and improvement of LVEF. One patient discontinued ivabradine because of bradycardia. In the SVT group, four of the seven patients discontinued ivabradine after the resolution of tachyarrhythmia and improvement of HR. Two patients experienced bradycardia but did not require treatment discontinuation. HR reduction was statistically significant in both groups. In HF, the median initial ivabradine dose was 0.06 mg/kg/day and the maintenance dose was 0.2 mg/kg/day. In SVT, the initial and maintenance doses were 0.1 mg/kg/day and 0.24 mg/kg/day, respectively.
Conclusion: Ivabradine demonstrated favorable efficacy and safety results in patients under 6 months of age with HF or SVT.
Highlights
• First published study that reports the use of ivabradine in patients under 6 months of age with heart failure.
• Study with the largest cohort of patients under 6 months who have received ivabradine for a diagnosis of supraventricular tachycardia.
• Ivabradine improved clinical parameters with an appropriate safety profile in patients under 6 months with heart failure and supraventricular tachycardia, presenting an effective and safe therapeutic alternative.
• Reduction in heart rate in patients with heart failure and supraventricular tachycardia was statistically significant.
1 Introduction
Heart failure (HF) and cardiac arrhythmias are significant causes of morbidity and mortality in the pediatric population, particularly during the perinatal period (Bonnet et al., 2017; Marín-García, 2004).
1.1 Heart failure (HF)
Congenital heart diseases (CHD) represent the leading cause of HF in the pediatric population (Gómez-Guzmán et al., 2013). Approximately 90% of patients with CHD develop HF within the first year of life, with the highest incidence occurring during the first 6 months (SECPCC, 2015). The second most common cause of HF are primary cardiomyopathies, particularly dilated cardiomyopathy (DCM), which has a higher incidence and worse prognosis in patients under 1 year of age (Bonnet et al., 2017; Gómez-Guzmán et al., 2013).
Currently, the treatment of HF aims to alleviate symptoms, slow disease progression, and reduce associated mortality. To achieve this, therapies that improve cardiac function and decrease heart rate (HR) are necessary, as elevated HR values are sometimes associated with an increased risk of death (Bonnet et al., 2017). However, the heterogeneity of the condition and its low incidence make standardizing treatment in pediatrics challenging (Gómez-Guzmán et al., 2013). Guidelines recommend the use of diuretics, digoxin, angiotensin-converting enzyme inhibitors (ACEIs), aldosterone antagonists, and beta-blockers (Bonnet et al., 2017; SECPCC, 2015). Nonetheless, due to the lack of evidence and controlled clinical trials in pediatric patients, treatment recommendations are often extrapolated from adult data. Consequently, most drugs are not approved for pediatric use (Bonnet et al., 2017).
1.2 Supraventricular tachycardias (SVT)
Tachyarrhythmias, a subset of cardiac arrhythmias, are characterized by heart rates exceeding the normal limits for age, with supraventricular tachycardias (SVT) being the most common in pediatrics (SECPCC, 2015). The age distribution of pediatric SVT is bimodal, with peaks occurring in infants under 1 year and in children between seven and 12 years of age (SECPCC, 2015). SVT typically present in patients without structural heart disease, although it can also be associated with CHD or cardiomyopathies, as well as secondary to surgical interventions (SECPCC, 2015).
SVT include conditions such as junctional ectopic tachycardia (JET), focal atrial tachycardia (FAT), multifocal atrial tachycardia (MAT), and ectopic atrial tachycardia (EAT) (SECPCC, 2015).
The increase in HR is associated with greater myocardial oxygen demand and impaired diastolic perfusion. Therefore, the treatment aims to achieve adequate HR control to meet myocardial oxygen demands and prevent potential complications (Younis et al., 2021). This treatment involves the administration of antiarrhythmic agents such as amiodarone, digoxin, and flecainide; however, a lack of response and resistance to these therapies is commonly observed (Younis et al., 2021; Michel et al., 2020).
1.3 Ivabradine in the pediatric population
Given the lack of effective therapeutic alternatives for treating HF, as well as the frequent resistance to conventional therapies in the case of SVT in pediatric patients, the use of oral ivabradine has been proposed for both conditions.
Currently, ivabradine is approved by the European Medicines Agency (EMA) as an antiarrhythmic agent exclusively for adult patients (EMA, 2024). However, while the U.S. Food and Drug Administration (FDA) initially approved ivabradine for use only in adult patients, it later extended its indication to pediatric patients for the treatment of stable symptomatic HF due to DCM from 6 months of age (Bonnet et al., 2017; FDA, 2024).
Ivabradine has also been used off-label for HR control in pediatric patients with various SVT, such as JET, FAT, MAT, and EAT, demonstrating efficacy and good tolerability (Younis et al., 2021; Kumar et al., 2019; Kumar et al., 2017; Tolani et al., 2024; Dieks et al., 2016). However, the experience with ivabradine in these indications is limited and primarily based on case reports or case series, particularly in patients under 6 months of age, for whom no dosing recommendations have been established.
Thus, data on the efficacy, safety, and dosing of ivabradine in patients younger than 6 months remain very limited. Nevertheless, HF caused by CHD or DCM, as well as SVT, have a higher incidence in this population. This highlights an urgent need for further research on its use in this age group.
The present study aims to evaluate the efficacy and safety of off-label ivabradine use in patients under 6 months of age and to describe the dosing regimens employed.
2 Materials and methods
2.1 Study design and patient selection
Retrospective observational study conducted at a national referral center for both pediatric cardiology and neonatology. The study included all pediatric patients who initiated ivabradine treatment before 6 months of age between January 2020 and May 2024.
Prior to starting ivabradine therapy, as per the hospital’s standard practice, parents or legal guardians were informed about the off-label use of the drug and its potential side effects.
2.2 Data collection
The study was reviewed and approved by the center’s Research Ethics Committee for medicinal products [EOM(AMI)054/2024 (6325)]. After obtaining approval, patients who had received ivabradine treatment within the first 6 months of life during the study period were identified and selected through the electronic prescribing system. The following parameters were collected in an anonymized database (Microsoft Excel® 2016) from the electronic medical records: demographic and clinical variables, indication for ivabradine treatment, variables related to ivabradine use, clinical parameters at the start and end of treatment, and adverse effects.
Patients were classified into two groups based on the indication for ivabradine to evaluate treatment response according to associated clinical variables: i) symptomatic HF: HR and left ventricular ejection fraction (LVEF), and ii) SVT: HR. LVEF was determined via echocardiography using the Teichholz and Simpson methods. The final treatment values of these variables correspond to those recorded at the time of discontinuation or, for patients still receiving therapy, to the latest values measured before the study’s conclusion.
2.3 Compounded formulation of ivabradine
Since ivabradine in Europe is only approved for adult patients, it is commercially available only in tablet form at doses defined for this population, complicating its administration in pediatric patients, especially in those under 6 months of age who require lower doses. Although ivabradine is not classified as a hazardous drug by the U.S. National Institute for Occupational Safety and Health (NIOSH), it could be considered hazardous due to its teratogenic potential, and safety precautions are recommended during its handling (National Institute for Occupational Safety and Health NIOSH, 2020).
To ensure accurate dosing and increase safety during handling, the Pharmacy Department decided to prepare individualized ivabradine capsules for each patient, starting from the commercially available tablet form, using lactose as the excipient.
2.4 Statistical analysis of results
A descriptive statistical analysis was conducted for the demographic and clinical variables of the patients. The results are presented as mean (standard deviation), median (interquartile range), absolute frequencies, and percentages, depending on the nature and distribution of the data.
To evaluate treatment response, the reduction in HR was calculated in both groups, and in the symptomatic HF group, the change in LVEF was also determined. Normality of the variables was assessed graphically and through Skewness/Kurtosis and Shapiro-Wilk tests. If the normality assumption was met, the paired Student’s t-test was used; otherwise, the Wilcoxon signed-rank test was applied. Statistical analysis was performed using StataCorp. 2019 (Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC).
3 Results
During the study period, 13 patients under 6 months of age (nine women) initiated treatment with ivabradine, with a median age of 1.4 (1 - 4) months. Table 1 details the patients diagnosed with symptomatic HF, while Table 2 presents those diagnosed with SVT. Patient 7 is listed in both groups, as she initially received ivabradine for sinus tachycardia and, after completing that treatment, was later diagnosed with severe diastolic dysfunction and resumed ivabradine therapy. Individualized ivabradine capsules were prepared by the Pharmacy Department for all patients included in the study.
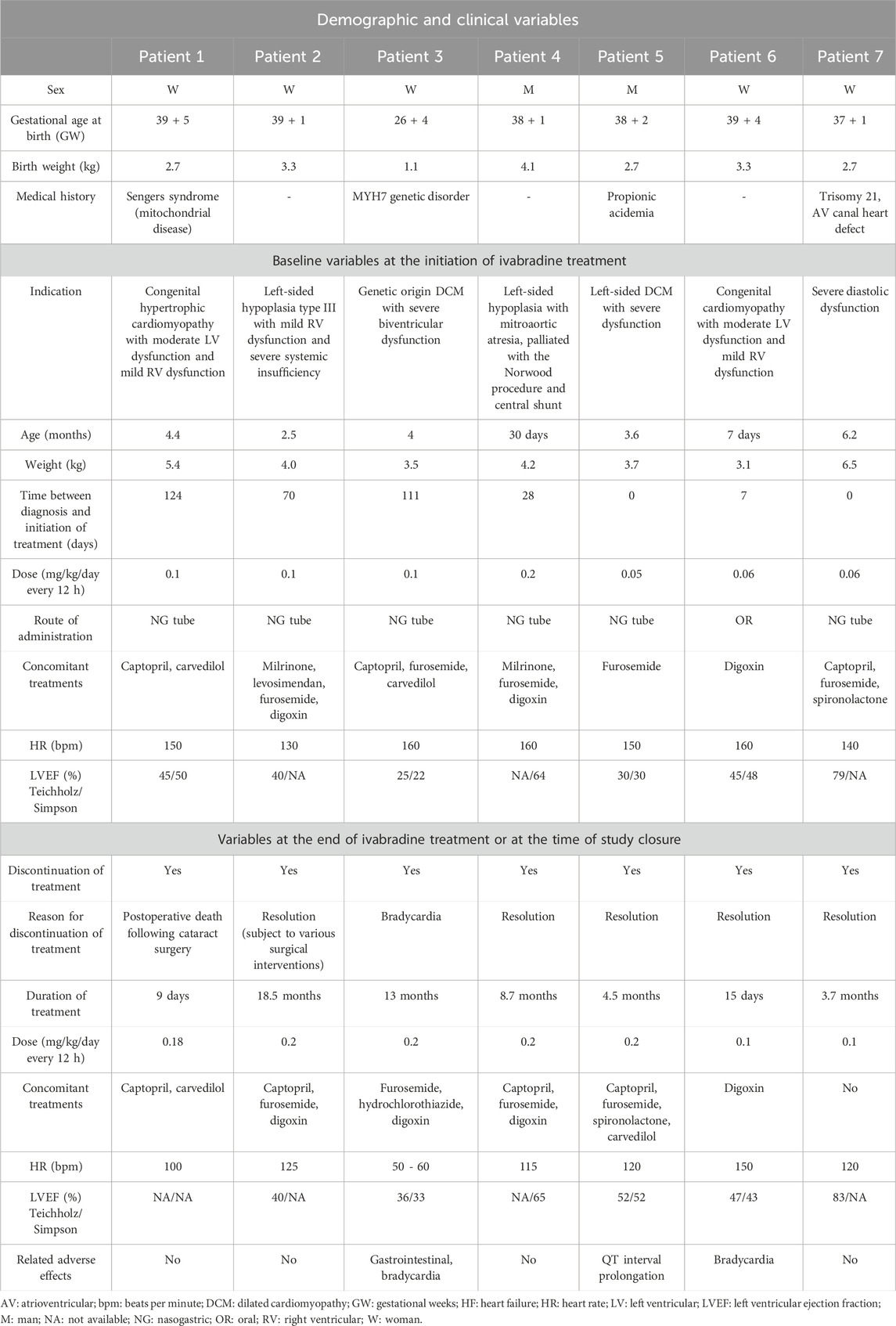
Table 1. Patients who received treatment with ivabradine for a diagnosis of symptomatic HF.
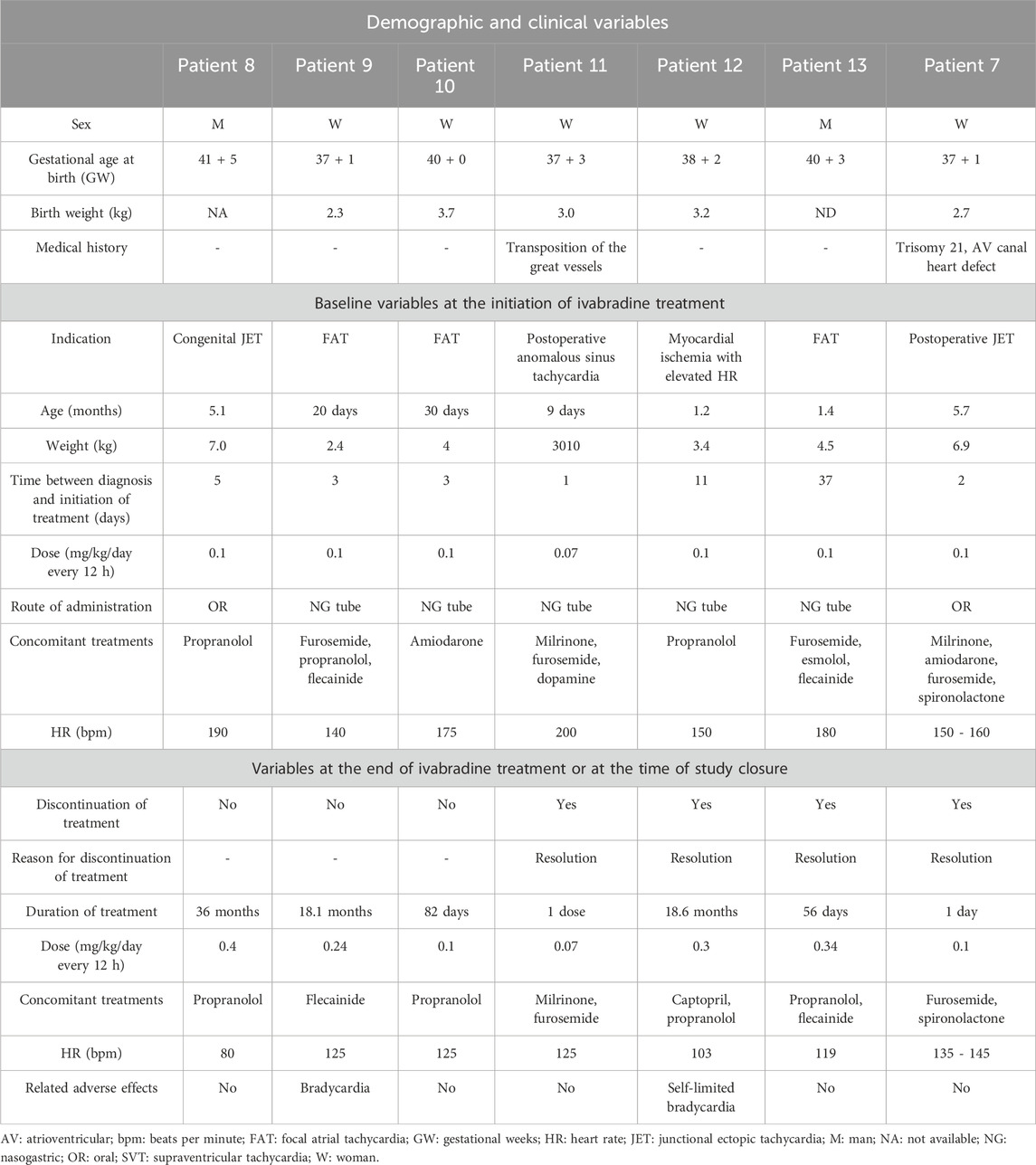
Table 2. Patients who received ivabradine treatment for a diagnosis of SVT.
Table 3 presents the descriptive statistics and statistical analysis of the demographic and clinical variables of patients classified by diagnosis, as well as the results before and after ivabradine treatment.
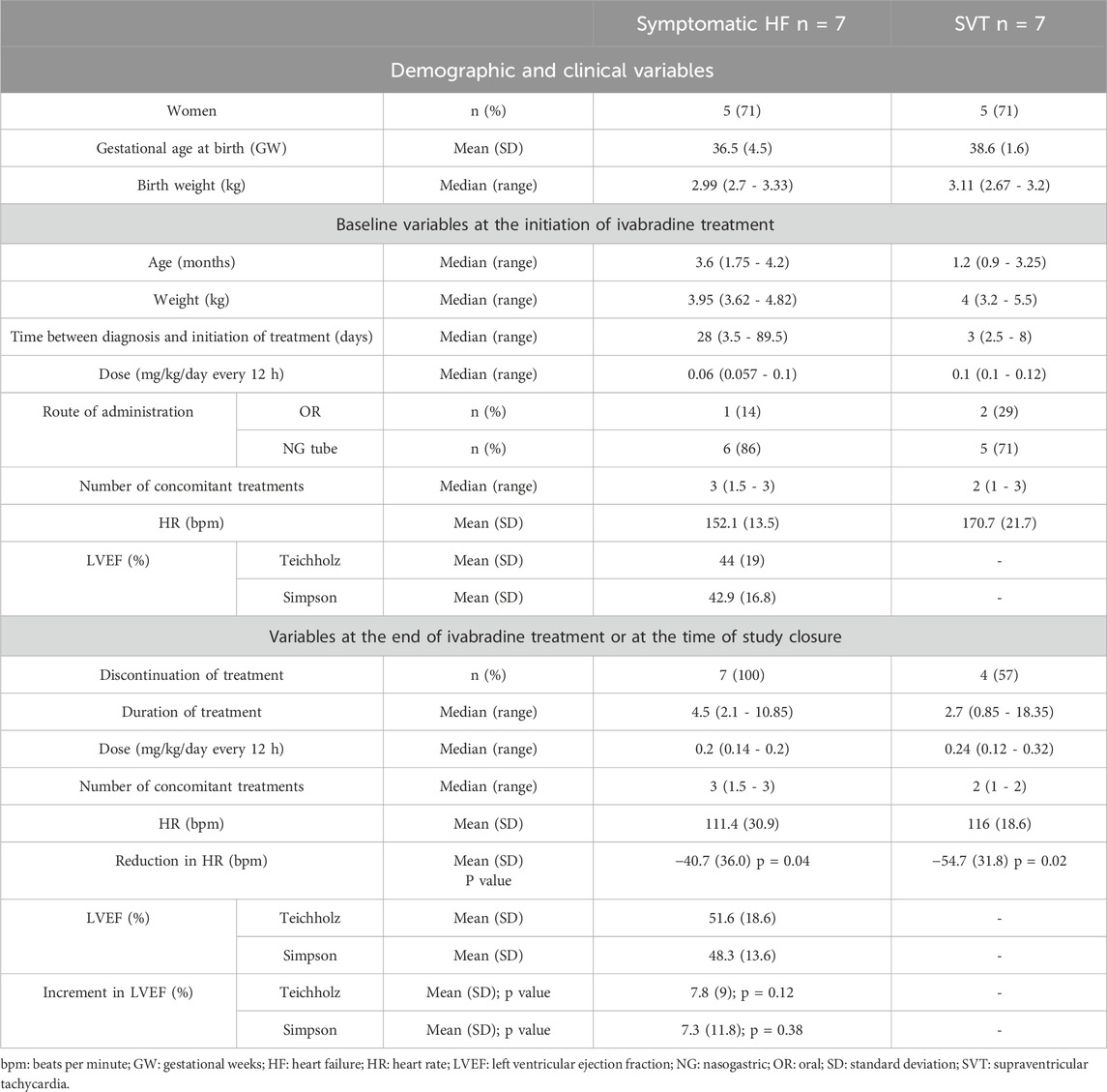
Table 3. Descriptive statistics and analysis of demographic and clinical variables of patients by diagnosis.
None of the patients in the symptomatic HF group continued on ivabradine therapy. In five of the seven patients (71.4%), treatment was discontinued following resolution of dysfunction, with adequate HR control observed in all of them (mean reduction of 41 beats per minute (bpm)) and an improvement in LVEF (mean increase of 7%–8%). Treatment was only discontinued in one patient due to adverse effects (bradycardia). For patients with SVT, treatment was discontinued in four of the seven patients (57.1%) following resolution of the tachyarrhythmia and improvement in HR (mean reduction of 55 bpm), and no discontinuation was required due to adverse effects, although two patients experienced bradycardia during treatment, with one case being self-limiting. In both groups, the reduction in HR was statistically significant.
Regarding the dosing of ivabradine for symptomatic HF, the median starting dose was 0.06 (0.057 - 0.1) mg/kg/day and the maintenance dose was 0.2 (0.14 - 0.2) mg/kg/day. In the case of SVT, the doses were 0.1 (0.1 - 0.12) mg/kg/day for the starting dose and 0.24 (0.12 - 0.32) mg/kg/day for the maintenance dose. The median duration of treatment for patients with symptomatic HF was 4.5 (2.1 - 10.9) months, while for patients with SVT, it was 2.7 (0.9 - 18.35) months.
4 Discussion
Certain cardiac conditions, such as HF and SVT, are associated with high morbidity and mortality in the pediatric population, particularly in patients under 6 months and 1 year of age (Bonnet et al., 2017; Marín-García, 2004). Despite the severity of these conditions, treatment evidence is limited due to a lack of studies in pediatrics. This results in restricted pharmacological options and, at times, inadequate disease management due to poor response or resistance to conventional treatments. Consequently, there is a need for the use of off-label therapies and/or those with limited evidence, such as ivabradine.
The mechanism of action of ivabradine is based on the selective and specific inhibition of the cardiac pacemaker current (If), which controls spontaneous diastolic depolarization in the sinus node and regulates HR; this results in a dose-dependent reduction in HR and myocardial oxygen consumption (EMA, 2024). Because its cardiac effects are specific to the sinus node, ivabradine exhibits negative inotropic activity, which may present a safer alternative in patients with decompensated systolic HF, compared to beta-blockers (Younis et al., 2021; EMA, 2024). Adverse effects are dose-dependent and arise from its mechanism of action, with frequent side effects including luminous phenomena (phosphenes), bradycardia, atrial fibrillation, headaches, dizziness, blurred vision, and hypotension. Gastrointestinal adverse effects and QT interval prolongation have also been observed (EMA, 2024).
However, evidence on the use of ivabradine off-label in the pediatric population is limited and primarily based on case reports or series, particularly in patients younger than 6 months. This poses a significant challenge, as higher prevalence, morbidity, and mortality rates have been reported in this age group.
In this context, the authors find it relevant to share our experience with ivabradine use in patients under 6 months of age to enhance the current evidence regarding its efficacy, safety, and dosing. This also aims to assist other healthcare professionals in its application. To date, this represents the largest published cohort of patients under 6 months receiving ivabradine treatment.
4.1 Ivabradine in HF
The only published clinical trial of ivabradine in pediatric patients was conducted by Bonnet et al. (2017); this study included pediatric patients aged 6 months and older with DCM and chronic symptomatic HF. Patients under 6 months of age were excluded due to potential inadequate tolerability with the concomitant administration of two antiarrhythmic drugs. Ivabradine was shown to significantly improve HR, cardiac function, LVEF, and patient quality of life, with an acceptable safety profile. The overall reduction in HR was 21%, and in the subgroup of patients aged six to 12 months, it was 25%. Patients exhibited an increase in LVEF of 11.4% at 6 months of treatment and 13.5% at 12 months. In our cohort of patients with symptomatic HF, a statistically significant reduction in HR was observed, along with an improvement in cardiac function, although the increase in LVEF was smaller. Bradycardia was reported in 11% of patients in the clinical trial, a value comparable to that observed in our cohort (n = 1, 14%).
Most patients in the trial received ivabradine in combination with other pharmacological therapies, including ACEIs, diuretics, beta-blockers, and digoxin. In the present study, all patients started ivabradine in conjunction with other treatments, and only in one case was it possible to discontinue these additional therapies by the end of the ivabradine treatment.
Due to the high interindividual variability observed in treatment response, Bonnet et al. (2017) emphasized the importance of appropriate dose titration. In the subgroup of patients aged six to 12 months (n = 10), an initial dose of 0.02 mg/kg/day every 12 h was established, with dose escalation up to a maximum dose of 0.2 mg/kg/day. In our cohort, the median initial dose used (0.06 mg/kg/day every 12 h) was higher than that reported in the trial, while the maintenance dose was similar (0.2 mg/kg/day every 12 h).
In the literature review conducted, no published cases or series of cases regarding the use of ivabradine in patients under 6 months of age with a diagnosis of HF were found. Therefore, this study is the first to report on the use of ivabradine in this population, making it essential for the authors to share the obtained results. The study demonstrates favorable outcomes regarding the efficacy and safety of ivabradine in this cohort. Additionally, the dosing guidelines used may provide valuable guidance for other healthcare professionals in its application.
4.2 Ivabradine in SVT
The use of ivabradine in pediatric patients with SVT is not well-defined, and current experience is based on case reports and series. The observed results are promising, especially in patients refractory to conventional antiarrhythmics, allowing for complete reversion to sinus rhythm with an acceptable safety profile (Younis et al., 2021; Tolani et al., 2024). Most cases involve patients aged 1 year and older, with evidence for patients under 6 months (Michel et al., 2020; Kumar et al., 2017; Bohora et al., 2011; Janson et al., 2019; Gul et al., 2023; Dasgupta and Johnsrude, 2023), being even more limited. Table 4 summarizes publications that include patients under 6 months of age who have received ivabradine treatment for various types of SVT.
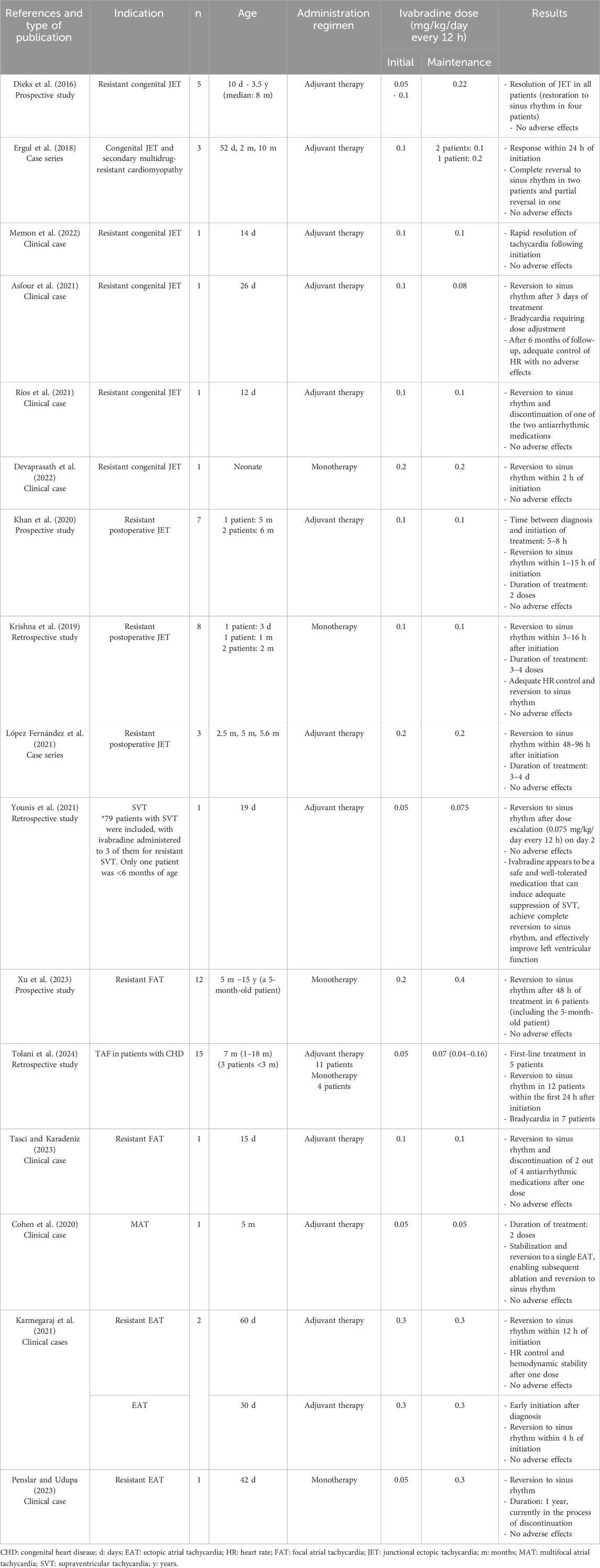
Table 4. Publications including patients under 6 months of age who have received ivabradine treatment for a diagnosis of any type of SVT.
JET is considered an uncommon SVT, which can be congenital (congenital JET) or post-surgical (post-surgical JET), with the latter being more common (Younis et al., 2021; Kumar et al., 2019; Dieks et al., 2016). Despite its lower incidence, congenital JET is associated with severe cardiovascular complications and high morbidity and mortality, particularly in patients under 6 months of age with elevated heart rates, who have a worse prognosis (Younis et al., 2021; Dieks et al., 2016). To achieve adequate HR control, the administration of at least two antiarrhythmic drugs is typically required, with amiodarone being the treatment of choice (Dieks et al., 2016). However, the lack of efficacy of conventional treatments has led to the use of off-label medications such as ivabradine, which, although its experience is limited, has shown favorable results (Younis et al., 2021). Current studies conclude that ivabradine is an effective therapeutic option with a good safety profile for managing resistant congenital JET, providing adequate HR control and complete reversion to sinus rhythm (Dieks et al., 2016; Ergul et al., 2018; Ríos et al., 2021; Devaprasath et al., 2022; López Fernández et al., 2021). Additionally, it may reduce the need for combinations of more than two antiarrhythmic drugs and invasive treatments (Ríos et al., 2021). While ivabradine is often administered in combination with other antiarrhythmic agents, it has also demonstrated adequate efficacy as monotherapy (Devaprasath et al., 2022). Some authors suggest that early initiation of treatment following diagnosis may be related to the positive response (Dieks et al., 2016).
Post-surgical JET is the most common post-surgical arrhythmia that causes hemodynamic instability, and it is associated with significant morbidity and mortality (Kumar et al., 2019). One of the risk factors for its development is young age (Kumar et al., 2019). Its treatment typically involves intravenous pharmacotherapy with agents such as amiodarone and flecainide (Kumar et al., 2019). Similar to congenital JET, ivabradine has shown promising results in terms of efficacy and safety for the treatment of post-surgical JET, both as an adjunctive therapy and as monotherapy, with a notable rapid onset of action (Kumar et al., 2019; Khan et al., 2020; Krishna et al., 2019; López Fernández et al., 2021). In this case, studies also recommend early initiation of treatment (Michel et al., 2020; López Fernández et al., 2021).
In cases of FAT, MAT, or EAT that are refractory to conventional treatments, off-label use of ivabradine has also yielded results similar to those observed with JET; so, ivabradine may be an effective and safe therapeutic option, either in conjunction with other antiarrhythmic agents or as monotherapy. Additionally, there is a noted association between early initiation of ivabradine and a more rapid reversion to sinus rhythm (Younis et al., 2021; Tolani et al., 2024; Karmegaraj et al., 2021). The only adverse effect reported in the studies has been bradycardia, which underscores the importance of close monitoring (Tolani et al., 2024).
Consistent with the reviewed publications, this study observed a statistically significant reduction in HR among patients receiving ivabradine for SVT. Additionally, ivabradine could be withdrawn in four patients (57%) following reversion to sinus rhythm. The median starting dose of ivabradine was 0.1 (0.1 - 0.12) mg/kg/day every 12 h, with a median maintenance dose of 0.24 (0.12 - 0.32) mg/kg/day every 12 h, results comparable to those reported in the literature. The median time from diagnosis to initiation of ivabradine was 3 days, which can be considered an early initiation of treatment, a relevant factor as it may influence the response. The only adverse effect observed in this study was bradycardia in two patients, an event previously reported by other authors, but it did not lead to discontinuation of treatment in any patient. Although the overall median number of concomitant treatments was not reduced, it was possible to discontinue some of the initial therapies in five patients (71%).
4.3 Study limitations
The primary limitations and biases of the study arise from its retrospective nature, such as the lack of data in some cases. However, despite the limited number of patients, this is currently the first published study that includes patients under 6 months of age with symptomatic HF treated with ivabradine and represents the largest cohort of patients under 6 months receiving ivabradine for the diagnosis of SVT.
5 Conclusion
In conclusion, in patients under 6 months of age with symptomatic HF or SVT, ivabradine improved clinical parameters with a satisfactory safety profile and proved to be an effective and safe therapeutic alternative for this patient population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Ethics Committee for medicinal products (Study code EOM(AMI)054/2024 (6325)) of Vall d’Hebron University Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the minor(s)’legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
LG-G: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing. CP-T: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing. GG-G: Conceptualization, Data curation, Investigation, Methodology, Supervision, Validation, Writing–original draft, Writing–review and editing. CF-G: Conceptualization, Data curation, Investigation, Methodology, Supervision, Validation, Writing–original draft, Writing–review and editing. QF-M: Conceptualization, Data curation, Investigation, Methodology, Supervision, Validation, Writing–original draft, Writing–review and editing. MC-P: Writing–review and editing, Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing–original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Asfour, S. S., Al-Omran, K. A., Alodhaidan, N. A., Asfour, R. S., Khalil, T. M., and Al-Mouqdad, M. M. (2021). Ivabradine monotherapy for the treatment of congenital junctional ectopic tachycardia in a premature neonate. J. Pediatr. Pharmacol. Ther. 26 (4), 414–417. doi:10.5863/1551-6776-26.4.414
Bohora, S., Lokhandwala, Y., Parekh, P., and Vasavda, A. (2011). Reversal of tachycardiomyopathy due to left atrial tachycardia by ivabradine. J. Cardiovasc Electrophysiol. 22 (3), 340–342. doi:10.1111/j.1540-8167.2010.01860.x
Bonnet, D., Berger, F., Jokinen, E., and Kantor, P. F. (2017). Ivabradine in children with dilated cardiomyopathy and symptomatic chronic heart failure. J. Am. Coll. Cardiol. 70 (10), 1262–1272. doi:10.1016/j.jacc.2017.07.725
Cohen, M. I., Cohen, J. A., Shope, C., Stollar, L., and Collazo, L. (2020). Ivabradine as a stabilising anti-arrhythmic agent for multifocal atrial tachycardia. Cardiol. Young. 30 (6), 899–902. doi:10.1017/S1047951120001195
Dasgupta, S., and Johnsrude, C. (2023). Combination therapy of ivabradine with procainamide for the management of pediatric postoperative junctional ectopic tachycardia. J. Innov. Card. Rhythm Manag. 14 (7), 5528–5532. doi:10.19102/icrm.2023.14075
Devaprasath, S., Buddhavarapu, S., Mariam, S., and Krishna, M. R. (2022). Ivabradine monotherapy in congenital junctional ectopic tachycardia. Ann. Pediatr. Cardiol. 15 (1), 61–63. doi:10.4103/apc.apc_264_20
Dieks, J. K., Klehs, S., Müller, M. J., Paul, T., and Krause, U. (2016). Adjunctive ivabradine in combination with amiodarone: a novel therapy for pediatric congenital junctional ectopic tachycardia. Heart rhythm. 13 (6), 1297–1302. doi:10.1016/j.hrthm.2016.03.015
EMA (2024). Data sheet of Procoralan® (ivabradine) film-coated tablets (les laboratoires servier). Netherlands: European Medicines Agency EMA. Available at: https://www.ema.europa.eu/en/documents/product-information/procoralan-epar-product-information_en.pdf (Accessed September 18, 2024).
Ergul, Y., Ozturk, E., Ozgur, S., Ozyurt, A., Cilsal, E., and Guzeltas, A. (2018). Ivabradine is an effective antiarrhythmic therapy for congenital junctional ectopic tachycardia-induced cardiomyopathy during infancy: case studies. Pacing Clin. Electrophysiol. 41 (10), 1372–1377. doi:10.1111/pace.13402
FDA (2024). Data sheet of Corlanor® (ivabradine) film-coated tablets (Amgen Inc.). Spain: U.S. Food and Drug Administration FDA. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/209964lbl.pdf (Accessed September 18, 2024).
Gómez-Guzmán, E., Tejero-Hernández, M. A., and Pérez-Navero, J. L. (2013). Tratamiento actual de la insuficiencia cardiaca pediátrica. Cardiocore 48 (1), 12–16. doi:10.1016/j.carcor.2012.09.011
Gul, O., Kafali, H. C., and Ergul, Y. (2023). Successful treatment of the focal ectopic atrial tachycardia in an infant with a single dose of ivabradine. Cardiol. Young 33 (9), 1750–1752. doi:10.1017/S1047951123000409
Janson, C. M., Tan, R. B., Iyer, V. R., Vogel, R. L., Vetter, V. L., and Shah, M. J. (2019). Ivabradine for treatment of tachyarrhythmias in children and young adults. Heart Rhythm Case Rep. 5 (6), 333–337. doi:10.1016/j.hrcr.2019.03.007
Karmegaraj, B., Balaji, S., Raju, P. N., Subramanian, P., Subramanian, R., Ibrahim, S., et al. (2021). Tachycardia-induced cardiomyopathy secondary to incessant ectopic atrial tachycardia in two infants: potential new indication for early initiation of enteral ivabradine. Ann. Pediatr. Cardiol. 14 (3), 422–427. doi:10.4103/apc.apc_37_21
Khan, N., Salvi, P., Dharod, D., Chokhandre, M., Mandrekar, A., and Joshi, S. (2020). Use of ivabradine in the treatment of tachyarrhythmias after surgery for congenital heart diseases. J. Cardiothorac. Vasc. Anesth. 34 (9), 2395–2400. doi:10.1053/j.jvca.2020.02.047
Krishna, M. R., Kunde, M. F., Kumar, R. K., and Balaji, S. (2019). Ivabradine in post-operative junctional ectopic tachycardia (JET): breaking new ground. Pediatr. Cardiol. 40 (6), 1284–1288. doi:10.1007/s00246-019-02149-5
Kumar, V., Kumar, G., Joshi, S., and Sharma, V. (2017). Ivabradine for junctional ectopic tachycardia in post congenital heart surgery. Indian Heart J. 69 (5), 666–667. doi:10.1016/j.ihj.2017.09.007
Kumar, V., Kumar, G., Tiwari, N., Joshi, S., Sharma, V., and Ramamurthy, R. (2019). Ivabradine as an adjunct for refractory junctional ectopic tachycardia following pediatric cardiac surgery: a preliminary study. World J. Pediatr. Congenit. Heart Surg. 10 (6), 709–714. doi:10.1177/2150135119876600
López Fernández, E., Montañes Delmas, E., Granados Ruiz, M. Á., Oviedo Melgares, L., and Ramos, C. V. (2021). Use of ivabradine in pediatric post-operative junctional ectopic tachycardia. Pediatr (Engl Ed) 95 (2), 118–120. doi:10.1016/j.anpede.2020.09.008
Marín-García, J. (2004). Cardiología pediátrica en la era de la genómica. Rev. Esp. Cardiol. 57 (4), 331–346. doi:10.1157/13059726
Memon, D., Larkin, E., and Varghese, M. (2022). Congenital junctional ectopic tachycardia in the paediatric emergency department. Cardiol. Young 32, 1510–1512. doi:10.1017/S1047951121005187
Michel, H., Heißenhuber, F., Wellmann, S., Melter, M., and Gerling, S. (2020). Ectopic atrial tachycardia in a 12-month-old girl treated with ivabradine and beta-blocker, a case report. Front. Pediatr. 8, 313. doi:10.3389/fped.2020.00313
National Institute for Occupational Safety and Health (NIOSH) (2020). NIOSH list of hazardous drugs in healthcare settings, 2020. Available at: https://www.cdc.gov/niosh/docket/review/docket233c/pdfs/DRAFT-NIOSH-Hazardous-Drugs-List-2020.pdf (Accessed September 18, 2024).
Penslar, J., and Udupa, S. (2023). Ivabradine in the management of pediatric arrhythmias. Can. J. Cardiol. 39 (1), 11–13. doi:10.1016/j.cjca.2022.10.029
Ríos, M., Chiesa, P., Arhcilles, S., Cuesta, A., and Moltedo, J. M. (2021). Uso de la ivabradina para el tratamiento de la taquicardia ectópica de la unión congénita. Med. (Buenos Aires) 81, 293–296.
SECPCC (2015). “Sociedad Española de Cardiología Pediátrica y Cardiopatías Congénitas (SECPCC),” in Cardiología pediátrica y cardioaptías congénitas del niño y del adolescente. Volumen II. 1a ed. (Madrid: CTO EDITORIAL, S.L.).
Tasci, O., and Karadeniz, C. (2023). Ivabradine in a 15-day-old male neonate with refractory focal atrial tachycardia. Pacing Clin. Electrophysiol. 46 (8), 924–927. doi:10.1111/pace.14781
Tolani, D., Ramdat Misier, N. L., Alqahtani, M., Tindel, K., de Groot, N. M. S., Scott, W. A., et al. (2024). Early experience with ivabradine for focal atrial tachycardia in pediatric patients with congenital heart disease. Heart rhythm. 21 (1), 115–116. doi:10.1016/j.hrthm.2023.10.013
Xu, X., Guo, Y., Gao, W., Huang, M., Liu, T., and Li, F. (2023). Ivabradine monotherapy in pediatric patients with focal atrial tachycardia: a single-center study. Eur. J. Pediatr. 182 (5), 2265–2271. doi:10.1007/s00431-023-04891-8
Younis, N. K., Abi-Saleh, B., Al Amin, F., El Sedawi, O., Tayeh, C., Bitar, F., et al. (2021). Ivabradine: a potential therapeutic for children with refractory SVT. Front. Cardiovasc Med. 8, 660855. doi:10.3389/fcvm.2021.660855
Glossary
ACEIs Angiotensin-converting enzyme inhibitors
AV Atrioventricular
bpm Beats per minute
CHD Congenital heart diseases
d Days
DCM Dilated cardiomyopathy
EAT Ectopic atrial tachycardia
EMA European Medicines Agency
FAT Focal atrial tachycardia
FDA Food and drug administration
GW Gestational weeks
HF Heart failure
HR Heart rate
JET Junctional ectopic tachycardia
LV Left ventricular
LVEF Left ventricular ejection fraction
M Man
MAT Multifocal atrial tachycardia
m Months
NA Not available
NG Nasogastric
NIOSH National Institute for Occupational Safety and Health
OR Oral
RV Right ventricular
SD Standard deviation
SVT Supraventricular tachycardias
W Woman
y Years
Keywords: heart failure, ivabradine, pediatrics, tachycardia, atrial tachycardia, ectopic atrial tachycardia, supraventricular tachycardia, junctional ectopic tachycardia
Citation: Gómez-Ganda L, Parramón-Teixidó CJ, Giralt-García G, Fernández-García C, Ferrer-Menduiña Q and Cabañas-Poy MJ (2025) Ivabradine in treatment of symptomatic heart failure and supraventricular tachycardias in patients under six months of age. Front. Pharmacol. 16:1502375. doi: 10.3389/fphar.2025.1502375
Received: 26 September 2024; Accepted: 27 January 2025;
Published: 18 February 2025.
Edited by:
Tamer M. Mohamed, University of Louisville, United StatesReviewed by:
Gabriele De Masi De Luca, University of L'Aquila, ItalyHe Jiang, Children’s Hospital of Capital Institute of Pediatrics, China
Copyright © 2025 Gómez-Ganda, Parramón-Teixidó, Giralt-García, Fernández-García, Ferrer-Menduiña and Cabañas-Poy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: C. J. Parramón-Teixidó, Y2FybG9zamF2aWVyLnBhcnJhbW9uQHZhbGxoZWJyb24uY2F0
†ORCID: L. Gómez-Ganda, orcid.org/0000-0003-2441-8607; C. J. Parramón-Teixidó, orcid.org/0000-0001-8023-3979; G. Giralt-García, orcid.org/0000-0002-8186-7073; C. Fernández-García, orcid.org/0000-0002-1935-1906; Q. Ferrer-Menduiña, orcid.org/0000-0003-3177-4618; M. J. Cabañas-Poy, orcid.org/0000-0003-2724-2715