 Shuang Dai
Shuang Dai Yukun Ding
Yukun Ding Jianbo Guo
Jianbo Guo Xian Wang
Xian Wang- 1Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China
- 2Science and Education Departmen, Beijing Fengtai Hospital of Integrated Traditional Chinese and Modern Medicine, Beijing, China
- 3LKS Faculty of Medicine, The University of Hong Kong, Pokfulam, Hong Kong SAR, China
Background: Danshen [Salvia miltiorrhiza Bunge (Lamiaceae; Salviae miltiorrhizae radix et rhizoma)] class injections (DSCIs) are widely used in the treatment of coronary heart disease (CHD). However, there are various types of DSCIs available on the market, and it remains uncertain which DSCI has the best clinical efficacy, as well as which one is most effective in regulating inflammatory markers and oxidative stress indicators. The aim of this network meta-analysis (NMA) is to compare the therapeutic effects of different DSCIs to identify the optimal DSCI for the treatment of CHD.
Methods: The databases searched to identify randomized controlled trials (RCTs) of DSCIs for CHD included the China National Knowledge Infrastructure (CNKI), Wanfang Database, China Science and Technology Journal Database (VIP), Chinese Biomedical Literature Database (CBM), PubMed, Web of Science, and Cochrane Library. The search period spanned from the inception of each database up to June 2024. NMA was conducted using RevMan 5.3 and Stata 16.0 software.
Results: A total of 106 studies including 14,979 patients, involving 10,931 patients, with 5,640 in the experimental group and 5,291 in the control group. And ten DSCIs were extracted, namely: Danhong injection (DH), Danshen injection (DS), Danshenchuanxiongqin injection (DSCXQ), Dansenduofensuanyan injection (DSDFSY), Danshenfen injection (DSFZ), Fufang Danshen injection (FFDS), Guanxinning injection (GXN), Sodium Tanshinone IIA Sulfonate injection (STS), Xiangdan injection (XD), Shenxiongputaotang injection (SXPTT). The results of NMA showed that, XD injection significantly enhances clinical efficacy; STS is more effective in reducing hs-CRP levels; DSDFSY shows better efficacy in decreasing IL-1 and increasing NO levels; DSCXQ has a greater advantage in reducing IL-6 levels; GXN is more effective in regulating SOD levels; and DH is better at reducing MDA levels.
Conclusion: The combined treatment of DSCIs and WM more significant efficacy in patients with CHD compared to WM treatment alone, including clinical efficacy evaluation, inflammatory markers, and oxidative stress markers. Overall, DSDFSY and DSCXQ show better performance in clinical efficacy evaluation and regulation of inflammatory markers, while DH exhibits a more stable effect in regulating oxidative stress. However, larger sample sizes and high-quality RCTs are still necessary to further compare the various DSCIs.
Systematic Review Registration: [PROSPERO], identifier [CRD42024548928].
1 Introduction
CHD is one of the most common cardiovascular diseases, with approximately 11.39 million patients in China (National Center for Cardiovascular Disease, 2023). According to the “China Health and Family Planning Statistical Yearbook 2021” (National Health Commission of the People’s Republic of China, 2021), the mortality rate of CHD in urban residents in China was 126.91/100,000 and 135.88/100,000 in rural areas in 2020, showing a continuous upward trend. Dyslipidemia (Martin et al., 2014) and inflammation (Hansson, 2005) jointly induce the formation of atherosclerotic plaques, which obstruct the coronary arteries and lead to CHD. CHD is a dynamic process characterized by the accumulation of atherosclerotic plaques and changes in coronary circulation. Clinically, CHD can be divided into chronic coronary syndrome (CCS) and acute coronary syndrome (ACS). The “2019 ESC Guidelines for the Diagnosis and Management of Chronic Coronary Syndromes” (Knuuti et al., 2020) recommend that conventional treatments for CCS include anti-ischemic therapy (Wight et al., 1992; Wei et al., 2011), antiplatelet therapy (Mehta et al., 2010), lipid-lowering therapy (Mach et al., 2020), and revascularization (Neumann et al., 2019). The “2023 ESC Guidelines for the Management of Acute Coronary Syndromes” (Byrne et al., 2023) suggest that the primary treatments for ACS should include percutaneous coronary intervention (PCI) (Huynh et al., 2009), thrombolytic therapy (Fibrinolytic Therapy Trialists FTT, 1994), and antithrombotic therapy (Valgimigli et al., 2018; Eikelboom et al., 2000). Additionally, anti-inflammatory and antioxidant treatments have been studied for decades in CHD patients (Malekmohammad et al., 2019), such as low-dose colchicine (Nidorf et al., 2020), IL-6 inhibitors (Broch et al., 2021), IL-1 inhibitors (Everett et al., 2020), vitamin C (Kaufmann et al., 2000), vitamin E (Riemersma, 1996), and β-carotene (Törnwall et al., 2004). Despite the gradual improvement of current treatment methods, challenges such as angina, antiplatelet drug resistance (Gorog et al., 2009), and microcirculation disorders (Padro et al., 2020) still exist. Therefore, comprehensively improving the quality of life for CHD patients remains a significant challenge.
CHD falls under the categories of “chest impediment and heart pain”, “sudden heart pain”, and “true heart pain” in traditional Chinese medicine (TCM). The earliest Chinese medicinal text, “Shen Nong’s Materia Medica,” documented that Danshen could treat evil qi in the heart and abdomen. In ancient China, decoctions and pills were the primary preparations of Danshen [Salvia miltiorrhiza Bunge (Lamiaceae; Salviae miltiorrhizae radix et rhizoma)], with the dried root being the most commonly used part. According to the “Chinese Pharmacopoeia” (2020), Danshen possesses effects such as promoting blood circulation, removing blood stasis, and cooling the blood. Modern research has identified various chemical metabolites in Danshen (Su et al., 2015), which can be categorized into three main types: diterpene quinones, including tanshinone-type diterpenes; hydrophilic phenolic acids, mainly phenolic acids; and essential oil metabolites, with diterpene quinones and hydrophilic phenolic acids being the primary active metabolites (Gao et al., 2012). Modern studies have discovered that Danshen has multiple pharmacological effects, including anti-myocardial ischemia, improvement of atherosclerosis, anti-inflammatory, antihypertensive, lipid-lowering, hypoglycemic, antithrombotic, and anti-tumor effects (Su et al., 2015). Therefore, DSCIs, which are TCM injections with Danshen as the main component, are widely used in treating CHD.
Previous studies have conducted meta-analyses on stable angina, unstable angina, or myocardial infarction (Zhang et al., 2017; Wu et al., 2017; Liu et al., 2018; Li et al., 2022), but no comprehensive meta-analysis on CHD as a whole has been done, and it remains unclear which injection is more effective for CHD. NMA was chosen for this study as it allows for the simultaneous comparison of multiple treatments, even when direct head-to-head trials are unavailable, by combining both direct and indirect evidence. This approach provides a more comprehensive and precise assessment of the relative efficacy of different DSCIs, offering insights that would be difficult to obtain through traditional Meta-Analysis alone. Therefore, we decided to use a network meta-analysis, incorporating both direct comparisons from RCTs and indirect comparisons based on shared control RCTs (Nikolakopoulou et al., 2018). We aim to identify the most reliable DSCIs for the treatment of CHD through relevant RCT-based network meta-analyses and to evaluate the relative efficacy and safety of different DSCIs in CHD patients, providing a reference for clinical application. This study focuses on patients with coronary heart disease (CHD), addressing a gap in previous research that has primarily focused on other conditions. We extended the search period to include studies from the past 2 years, enhancing the relevance and timeliness of our findings. Additionally, we explored changes in inflammatory markers and oxidative stress indicators, providing deeper insight into the underlying mechanisms of Danshen’s therapeutic effects. We also compared different Danshen injections, an area that has not been extensively addressed in previous meta-analyses, offering more precise conclusions about the relative efficacy of various formulations. These distinctive aspects highlight the originality and value of our study in advancing the understanding of Danshen’s role in treating CHD.
2 Methods
2.1 Study registering
The review protocol was registered at PROSPERO (No: CRD42024548928, https://www.crd.york.ac.uk/prospero/). The current research procedure was conducted following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Hutton et al., 2015).
2.2 Inclusion and exclusion criteria
The inclusion criteria for this study adhered to the PICOS framework, encompassing participants, interventions, comparisons, outcomes, and study design. Therefore, clinical trials meeting the following criteria were included:
(1) Participants: This study included patients diagnosed with CHD, including chronic coronary syndrome and acute coronary syndrome, without restrictions on race, gender, age, or nationality. Study design. Only RCTs mentioned in articles were enrolled.
(2) Interventions and comparisons: The experimental group received DSCIs combined with guideline-recommended Western medicine. Patients in the control group received Western medicine treatment alone, without the use of other Chinese medicine. Commonly used Western medicines included antiplatelet agents, statins, nitrates, β-receptor blockers, and Angiotensin-Converting Enzyme Inhibitors. There were no restrictions on dosage and duration of treatment. Appropriate treatment measures were taken for patients with additional comorbidities.
(3) Outcomes: The primary outcome of this study was the clinical effectiveness rate. Based on changes in clinical symptoms and objective indicators, the effectiveness status was categorized as effective or ineffective. When patients’ clinical symptoms showed no significant change or even worsened (e.g., increased frequency, longer duration, more intense pain), and there was no improvement in the electrocardiogram, it was considered ineffective. Secondary outcomes included high-sensitivity C-reactive protein (hs-CRP), interleukin-1 (IL-1), interleukin-6 (IL-6), nitric oxide (NO), superoxide dismutase (SOD), malondialdehyde (MDA), and adverse reactions. Included studies should have at least one outcome measure.
(4) Study design: Only Randomized Controlled Trial (RCT) were enrolled.
We excluded the following studies: (1) studies using other traditional Chinese medicine preparations or external traditional Chinese medicine therapies (such as massage, gua sha, cupping); (2) studies related to percutaneous coronary intervention (PCI) or thrombolytic surgery; (4) studies with incomplete or erroneous data; (5) studies for which the full text could not be obtained.
2.3 Search strategy
A systematic electronic search was conducted across eight databases to identify RCT studies published from their inception up to June 2024. The databases searched included the China National Knowledge Infrastructure Database (CNKI), the Chinese Scientific Journals Full-text Database (VIP), the Wan-Fang Database, the Chinese Biomedical Literature Database (SinoMed), the Cochrane Library, PubMed, Web of Science and Embase. The search was not restricted by language or country. For detailed search strategies, please refer to the appendix.
2.4 Data extraction
Two researchers (DS and DYK) used EndNote X9 for reference management, removing duplicate records and excluding irrelevant or non-compliant studies according to the inclusion and exclusion criteria. Subsequently, a database was established using Microsoft Excel to meticulously record study information, including publication details (title, author names, and publication date), patient information (sample size, mean age and gender composition, classification of coronary artery disease), interventions (name of the injection, dosage, and duration of administration), outcomes (primary and secondary outcomes), and study design (randomization, allocation concealment, and blinding). To ensure data accuracy, two independent researchers entered the data and cross-checked for inconsistencies. For studies with missing data, we contacted the original authors for clarification; if no accurate data was provided, the study was excluded from the analysis.
2.5 Quality assessment
Two researchers independently assessed the quality of all included studies according to the Cochrane Intervention Reviewer’s Handbook version 5.1.0 (Cumpston et al., 2019). The assessment criteria included random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other biases. Each criterion could be rated as low, high, or unclear risk of bias.
In cases of discrepancies in data extraction and quality assessment, resolution was achieved through the judgment of a third researcher or consensus.
2.6 Statistical analysis
Statistical and network meta-analysis were conducted using Stata 16.0 software. For dichotomous outcomes, results were presented as odds ratios (OR) with corresponding 95% confidence intervals (95% CI); for continuous variable outcomes, results were shown as mean differences (MD) with 95% CI. Additionally, if a particular outcome had two or more studies directly compared, a pairwise meta-analysis using a random-effects model was employed. Different interventions were compared through network meta-analysis using a frequentist framework and a random-effects model, and the results were presented in a ranking format. The surface under the cumulative ranking curve (SUCRA) was plotted according to the size of the cumulative ranking area under the curve, providing a more intuitive display of the ranking of each treatment measure. SUCRA ranges from 0% to 100%, assigned to the worst and best treatment measures respectively. Since no closed loops were formed in the analysis, inconsistency assessment was not feasible. Furthermore, publication bias of the included RCT was examined by comparing funnel plots corrected by regression lines.
3 Results
3.1 Literature selection
A total of 8,605 articles were retrieved by searching eight databases. After removing duplicate articles, 2,656 articles remained for abstract screening. Excluding reviews, meta-analyses, systematic reviews, animal studies, and other u—elated topics, 116 articles were left for full-text review. Ultimately, 106 RCTs met the criteria for inclusion in this network meta-analysis. The detailed process of article selection is illustrated in Figure 1.
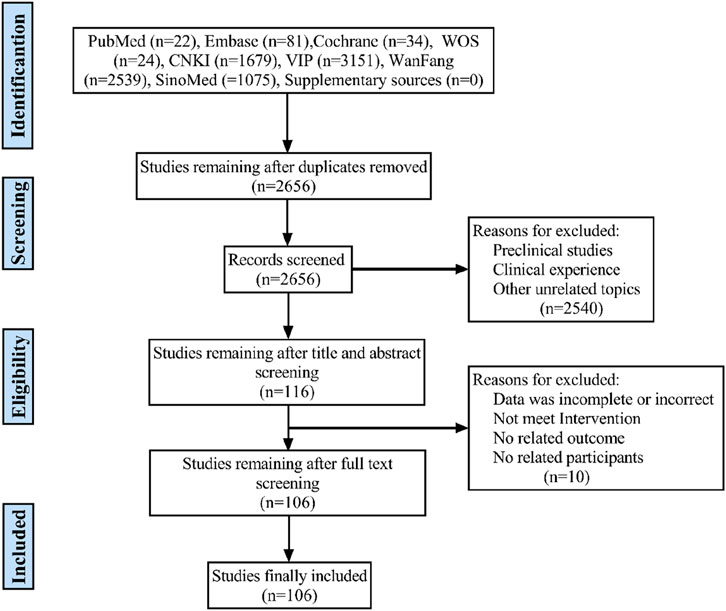
Figure 1. Flow diagram of eligible literature selection. CNKI, the China National Knowledge Infrastructure Database; WanFang, Wanfang Database; VIP, the Chinese Scientific Journals Full-text Database; SinoMed, the Chinese Biomedical Literature Database; n, number of publications.
3.2 Study characteristic
A total of 106 RCTs were included in this research, involving 10,931 patients, with 5,640 in the experimental group and 5,291 in the control group. All included studies were conducted in China. The research covered 10 types of DSCIs, including DSDFSY + WM vs. WM (n = 44), DH + WM vs. WM (n = 31), DSCXQ + WM vs. WM (n = 9), STS + WM vs. WM (n = 8), DS + WM vs. WM (n = 2), SXPTT + WM vs. WM (n = 2), GXN + WM vs. WM (n = 4), XD + WM vs. WM (n = 1), DSFZ + WM vs. WM (n = 1), DH + WM vs. DS + WM (n = 1), DH + WM vs. FFDS + WM (n = 1), FFDS + WM vs. DH + WM (n = 1), and DSDFSY + WM vs. DS + WM (n = 1). The control group treatment was WM, mainly consisting of antiplatelet aggregation drugs, β-blockers, statins, nitrates, etc. Detailed information on the characteristics of the included studies is shown in Table 1.
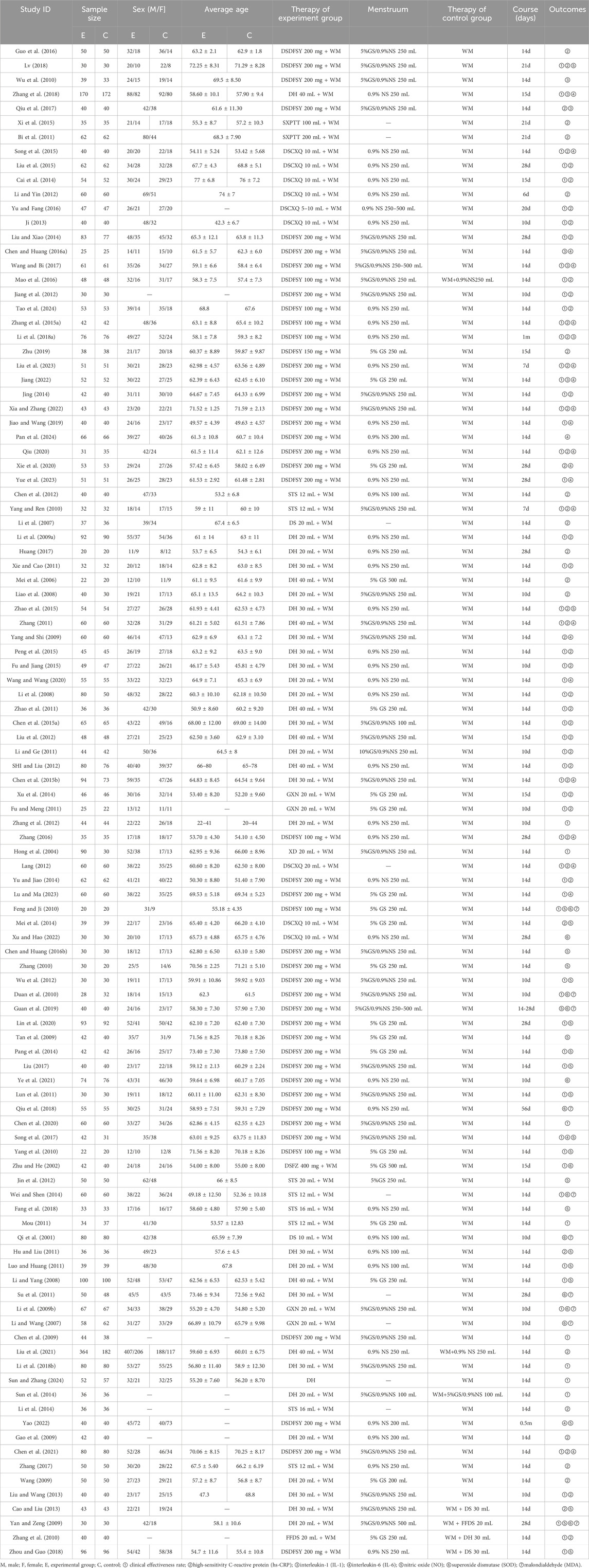
Table 1. Characteristics of included studies.
3.3 Quality evaluation
A risk of bias assessment was conducted on the 106 included studies. (1) Selection bias: Two studies did not mention randomization and were considered “unclear risk,” while the remaining studies mentioned random allocation but may not have reported the specific randomization method; these were also evaluated as “low risk”. (2) Allocation concealment: One study mentioned using allocation concealment and was considered “low risk”, while the rest did not mention this information and were deemed “unclear risk”. (3) Performance bias: Four studies explicitly stated that the trial design was “single-blind”, thus considered “low risk”. Studies that did not report relevant information were deemed “unclear risk”. (4) Detection bias: One study mentioned blinding the outcome assessors, considered “low risk”, while other studies did not mention this information and were deemed “unclear risk”. (5) Attrition bias: All included studies had no incomplete data, so the risk of attrition bias was considered “low risk”. (6) Reporting bias: Eight studies reported fewer outcomes, potentially indicating reporting bias, and were evaluated as “unclear risk”, while the remaining studies were “low risk.” (7) Other biases: Two studies did not report whether the experimental and control groups were comparable at baseline and were evaluated as “unclear risk”, while the remaining studies were considered “low risk”. Overall, the quality of the included studies was suboptimal, with summary results shown in Figure 2 and ROB 2.0 evaluation results in Supplementary table.
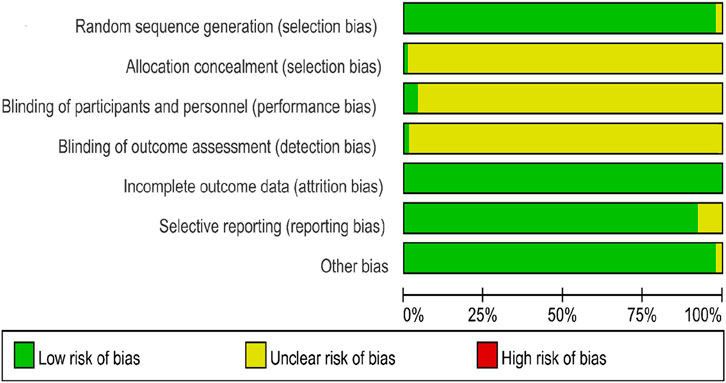
Figure 2. Results of risk of bias evaluation of included studies.
3.4 Results of network meta-analysis
3.4.1 Consistency testing
None of the interventions in this study formed a closed loop, so consistency testing was not required.
3.4.2 Clinical effectiveness rate
A total of 69 randomized controlled trials involving 9 types of DSCIs were included in the analysis of clinical effectiveness rate: DSDFSY + WM vs. WM (n = 30), DSFZ + WM vs. WM (n = 1), DH + WM vs. FFDS + WM (n = 1), FFDS + WM vs. DH + WM (n = 1), DH + WM vs. WM (n = 22), XD + WM vs. WM (n = 1), DSDFSY + WM vs. DS + WM (n = 1), DSCXQ + WM vs. WM (n = 6), GXN + WM vs. WM (n = 3), and STS + WM vs. WM (n = 3). The network relationship diagram is shown in Figure 3. Connections between nodes represent direct comparative evidence between the two interventions, while the absence of a connection indicates no direct comparison. The thickness of the lines indicates the number of included studies comparing each treatment, and the size of the circles represents the sample size of the population using each intervention. Except for the DS + WM and FFDS + WM groups, all other DSCIs combined with WM showed superior clinical efficacy compared to WM alone. Additionally, compared to DS + WM, the clinical efficacy rates of DSCXQ + WM, DSDFSY + WM, XD + WM, and DH + WM were significantly higher. No significant differences were observed between other interventions (Table 2). According to the SUCRA probabilities ranking, XD + WM (94.0%) was the most likely to be the best intervention to improve the clinical efficacy rate, followed by DSDFSY + WM (73.1%) > DSCXQ + WM (68.7%) > DH + WM (60.7%) > DSFZ + WM (58.4%) > STS + WM (53.7%) > GXN + WM (40.5%) > FFDS + WM (33.7%) > DS + WM (10.9%) > WM (6.2%). The specific results are shown in the Table 3 and Figure 4.
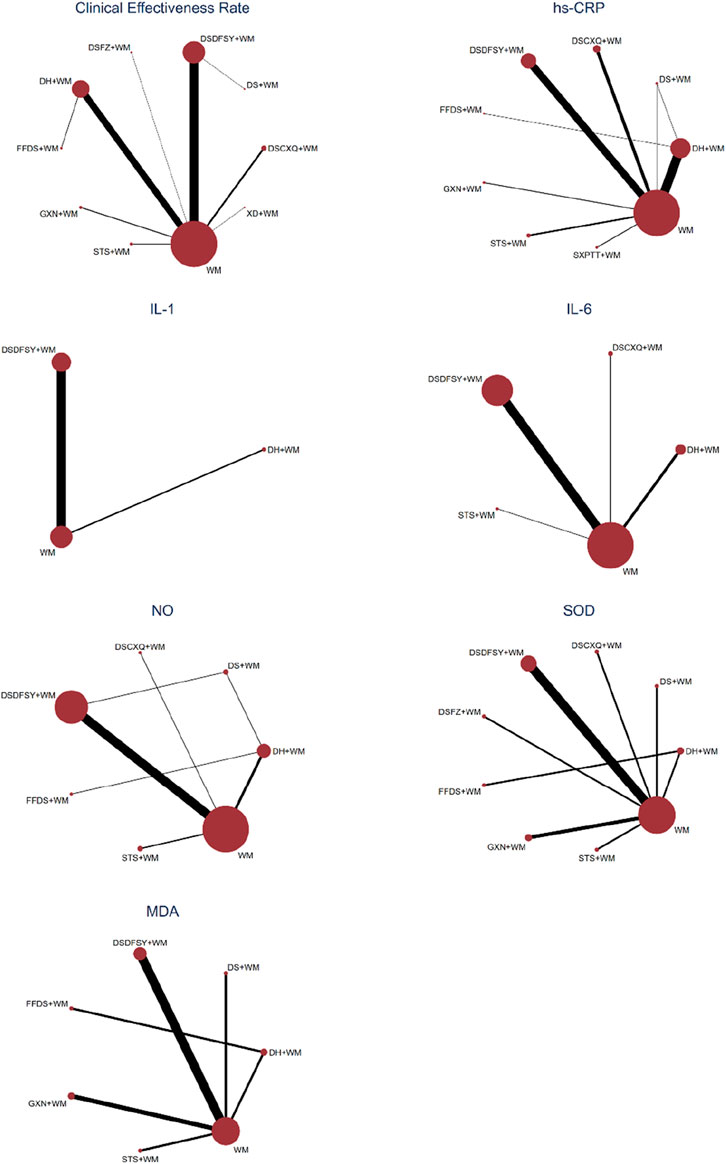
Figure 3. Network diagram of various outcomes. WM, western medicine; DH, Danhong injection; DS, Danshen injection; DSCXQ, Danshenchuanxiongqin injection; DSDFSY, Dansenduofensuanyan injection; DSFZ, Danshenfen injection; FFDS, Fufang Danshen injection; GXN, Guanxinning injection; STS, Sodium Tanshinone IIA Sulfonate injection; XD, Xiangdan injection; SXPTT, Shenxiongputaotang injection. hs-CRP, high-sensitivity C-reactive protein; IL-1, interleukin-1; IL-6, interleukin-6; NO, nitric oxide; SOD, superoxide dismutase; MDA, malondialdehyde.
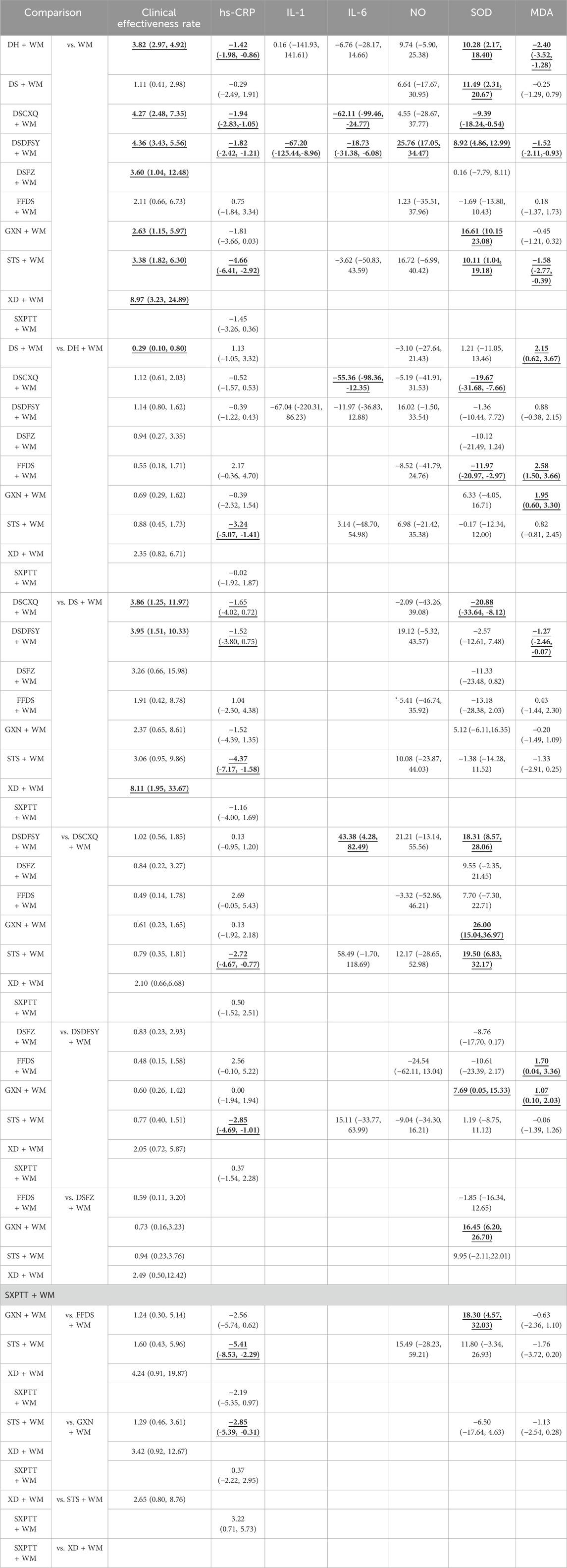
Table 2. OR/MD (95%CIs) of all interventions. The bolded and underlined results indicate statistical significance.
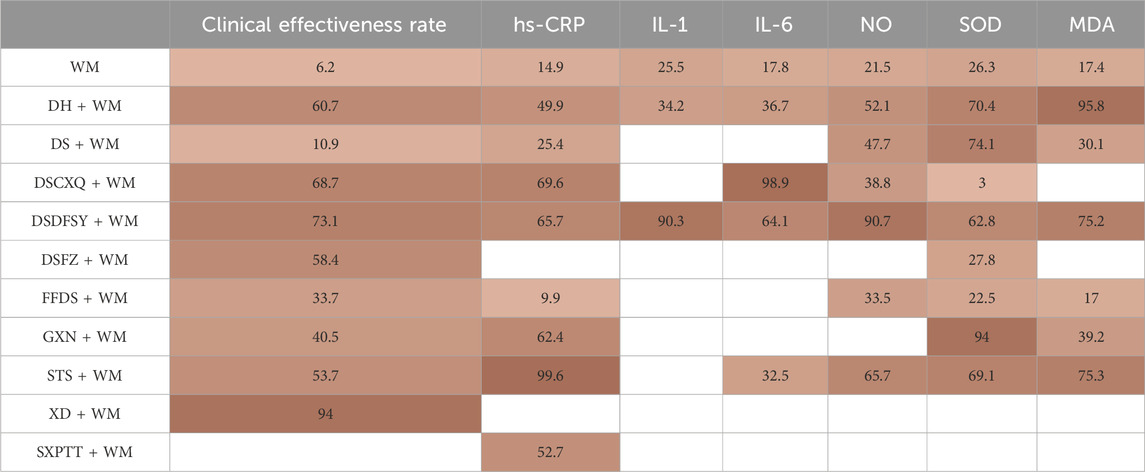
Table 3. SUCRA (%) of all therapeutic measures. The redder color in the table means the higher the ranking of the corresponding intervention.
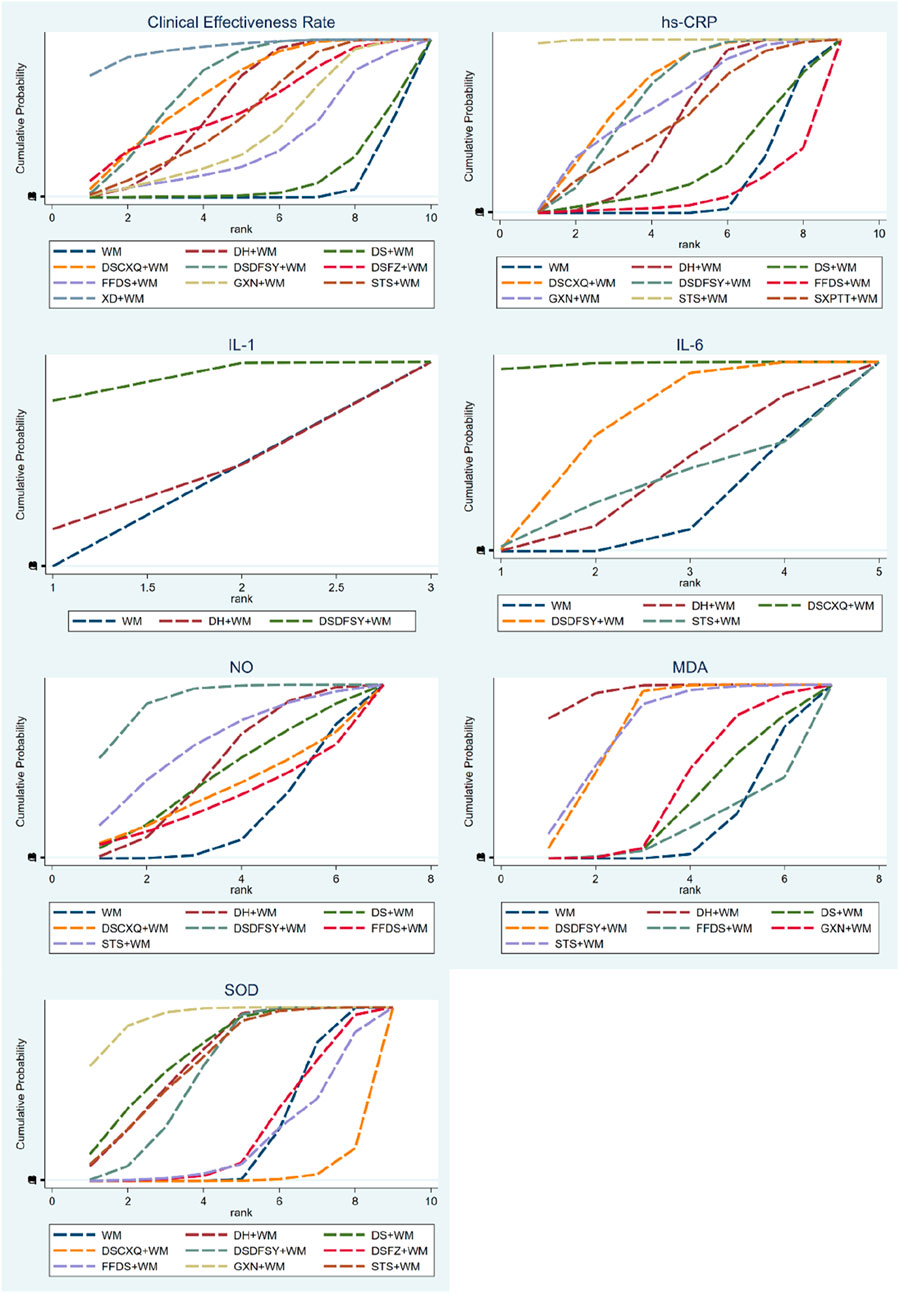
Figure 4. SUCRA for different outcomes.
3.4.3 Hs-CRP
A total of 59 randomized controlled trials involving 8 types of DSCIs were analyzed for hs-CRP: DH + WM vs. WM (n = 22), DS + WM vs. WM (n = 1), DSCXQ + WM vs. WM (n = 8), DSDFSY + WM vs. WM (n = 18), GXN + WM vs. WM (n = 2), STS + WM vs. WM (n = 4), SXPTT + WM vs. WM (n = 2), FFDS + WM vs. DH + WM (n = 1), and DH + WM vs. DS + WM (n = 1). The network relationship diagram is shown in Figure 3. DH, DSCXQ, DSDFSY, and STS combined with WM were superior to WM alone in reducing hs-CRP. Moreover, STS + WM was more effective than DH + WM, DS + WM, DSCXQ + WM, DSDFSY + WM, FFDS + WM, or GXN + WM in reducing hs-CRP, with statistically significant differences (Table 2). According to the SUCRA probability ranking, STS + WM (99.6%) is most likely to be the best intervention for reducing hs-CRP, followed by DSCXQ + WM (69.6%) > DSDFSY + WM (65.7%) > GXN + WM (62.4%) > SXPTT + WM (52.7%) > DH + WM (49.9%) > DS + WM (25.4%) > WM (14.9%) > FFDS + WM (9.9%). The specific results are shown in the Table 3 and Figure 4.
3.4.4 IL-1
7 randomized controlled trials involving IL-1, including 2 types of DSCIs [DH + WM vs. WM (n = 1) and DSDFSY + WM vs. WM (n = 6)], were analyzed. The network relationship diagram is shown in Figure 3. DSDFSY + WM was more effective than WM alone in reducing IL-1, with statistically significant differences (Table 2). According to the SUCRA probability ranking, DSDFSY + WM (90.3%) is most likely to be the best intervention for reducing IL-1, followed by DH + WM (34.2%) and WM (25.5%). The specific results are shown in the Table 3 and Figure 4.
3.4.5 IL-6
24 randomized controlled trials involving 4 types of DSCIs were analyzed for IL-6: DH + WM vs. WM (n = 5), DSCXQ + WM vs. WM (n = 2), DSDFSY + WM vs. WM (n = 16), and STS + WM vs. WM (n = 1). The network relationship diagram is shown in Figure 3. DSCXQ and DSDFSY combined with WM were more effective than WM alone in reducing IL-6. DSCXQ + WM was more effective than DH + WM in reducing IL-6, while DSDFSY + WM was less effective than DSCXQ + WM (Table 2). According to the SUCRA probability ranking, DSCXQ + WM (98.9%) is most likely to be the best intervention for reducing IL-6, followed by DSDFSY + WM (64.1%) > DH + WM (36.7%) > STS + WM (32.5%) > WM (17.8%). The specific results are shown in the Table 3 and Figure 4.
3.4.6 NO
24 randomized controlled trials involving 6 types of DSCIs were analyzed for NO: DH + WM vs. WM (n = 4), DSCXQ + WM vs. WM (n = 1), DSDFSY + WM vs. WM (n = 14), STS + WM vs. WM (n = 2), DH + WM vs. FFDS + WM (n = 1), DH + WM vs. DS + WM (n = 1), and DSDFSY + WM vs. DS + WM (n = 1). The network relationship diagram is shown in Figure 3. DSDFSY + WM was more effective than WM alone in increasing NO (Table 2). According to the SUCRA probability ranking, DSDFSY + WM (90.7%) is most likely to be the best intervention for increasing NO, followed by STS + WM (65.7%) > DH + WM (52.1%) > DS + WM (47.7%) > DSCXQ + WM (38.8%) > FFDS + WM (33.5%) > WM (21.5%). The specific results are shown in the Table 3 and Figure 4.
3.4.7 SOD
13 randomized controlled trials involving 8 types of DSCIs were analyzed for SOD: DH + WM vs. WM (n = 1), DS + WM vs. WM (n = 1), DSCXQ + WM vs. WM (n = 1), DSDFSY + WM vs. WM (n = 5), GXN + WM vs. WM (n = 2), STS + WM vs. WM (n = 1), DSFZ + WM vs. WM (n = 1), and FFDS + WM vs. DH + WM (n = 1). The network relationship diagram is shown in Figure 3. Except for DSFZ, FFDS, and DSCXQ, other types of DSCIs combined with WM were more effective than WM alone in increasing SOD (Table 2). According to the SUCRA probability ranking, GXN + WM (94.0%) is most likely to be the best intervention for increasing SOD, followed by DS + WM (74.1%) > DH + WM (70.4%) > STS + WM (69.1%) > DSDFSY + WM (62.8%) > DSFZ + WM (27.8%) > WM (26.3%) > FFDS + WM (22.5%) > DSCXQ + WM (3.00%). The specific results are shown in the Table 3 and Figure 4.
3.4.8 MDA
10 randomized controlled trials involving 6 types of DSCIs were analyzed for MDA: DH + WM vs. WM (n = 1), DS + WM vs. WM (n = 1), DSDFSY + WM vs. WM (n = 4), GXN + WM vs. WM (n = 2), STS + WM vs. WM (n = 1), and FFDS + WM vs. DH + WM (n = 1). The network relationship diagram is shown in Figure 3. DH, DSDFSY, and STS combined with WM were more effective than WM alone in reducing MDA (Table 2). According to the SUCRA probability ranking, DH + WM (95.8%) is most likely to be the best intervention for reducing MDA, followed by STS + WM (75.3%) > DSDFSY + WM (75.2%) > GXN + WM (39.2%) > DSCXQ + WM (30.1%) > WM (17.4%) > FFDS + WM (17.0%). The specific results are shown in the Table 3 and Figure 4.
3.4.9 Adverse reactions
A total of 49 studies reported adverse reaction events, with 17 studies detailing specific adverse reactions. These included the following manifestations: circulatory system: dizziness, headache, palpitations, fatigue; digestive system: nausea, abdominal distension, vomiting; peripheral vasculature: facial flushing; skin: rash, bruising. The specific results are shown in Table 4.
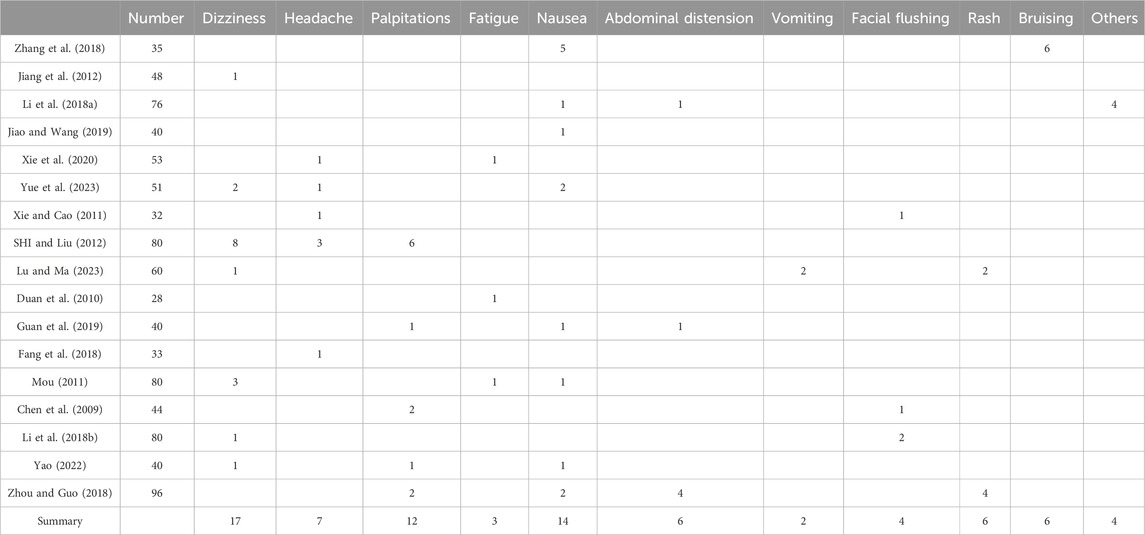
Table 4. Adverse reactions.
3.4.10 Publication bias
A funnel plot was used to test for publication bias in this study (Figure 5 and Supplementary Figure). As shown in the figure, most points are concentrated in the middle, with a few at the bottom, indicating that some studies had small sample sizes, which may lead to bias. Additionally, the points in the funnel plot are asymmetrically distributed relative to the centerline, and the regression line forms an angle with the centerline, suggesting the presence of publication bias in this study.
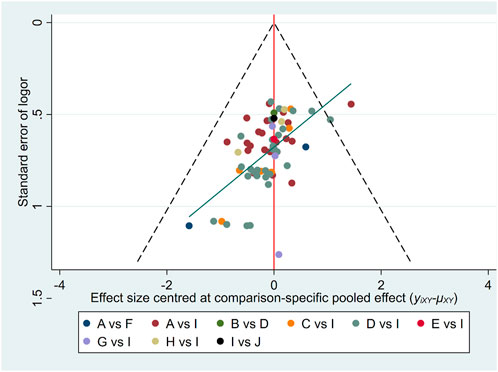
Figure 5. Funnel plots of clinical effectiveness rate. The vertical axis represents “standard error of effect size” and horizontal axis represents “effect size centred at comparison-specific pooled effect (yixy-μxy).” A, DH + WM; B, DS + WM; C, DSCXQ + WM; D, DSDFSY + WM; E, DSFZ + WM; F, FFDS + WM; G, GXN + WM; H, STS + WM; I, WM; J, XD + WM.
4 Discussion
Although DSCIs are widely used in China to treat CHD, they are mostly used as adjunctive therapies and rarely used alone. Their acceptance in other countries is relatively poor. The reasons for this may include: ① Although multiple clinical studies have confirmed the efficacy of DSCIs, the trial designs are not rigorous enough, and there is still a lack of large-scale, high-quality evidence-based medical evidence to verify their efficacy and safety. ② Most DSCIs are compound preparations containing various active metabolites, making their mechanisms of action complex. Notably, current basic research is often focused on simple target points and pathways, lacking in-depth studies on pharmacokinetics and pharmacological and toxicological mechanisms. ③ The complex composition of traditional Chinese medicine injections increases the probability of adverse reactions when used in combination with other drugs, limiting their clinical use by physicians. ④ There are many types of DSCIs, with both similarities and differences, making clinical drug selection challenging.
Based on these issues, this study employs the NMA method to fully utilize existing clinical research and compare the efficacy and safety of multiple DSCIs. By pooling small sample data, we expand the sample size, reduce bias and errors, improve statistical power, and obtain more reliable results. Additionally, the NMA results provide efficacy rankings for different outcome indicators, offering reference suggestions for clinical drug selection and helping clinicians understand the associations and differences between various treatment options.
This study used the NMA method to evaluate 106 randomized controlled trials that met the inclusion and exclusion criteria, involving 10 types of DSCIs. The outcomes included clinical efficacy, inflammatory markers (hs-CRP, IL-1, IL-6), oxidative stress markers (NO, SOD, MDA), and safety. The NMA results indicate that seven types of DSCIs combined with WM achieved better efficacy than WM alone. According to the SUCRA probability ranking, XD + WM showed the most significant improvement in clinical efficacy, followed by DSDFSY + WM and DSCXQ + WM. However, the relatively small sample size for XD + WM might lead to greater errors, potentially interfering with the results. Additionally, due to differences in the active ingredients of each DSCIs, their effects vary among different types of patients. Clinically, the appropriate injection can be chosen based on the patient’s symptoms and signs to achieve better clinical efficacy. In reducing inflammatory markers, STS + WM had an advantage in lowering hs-CRP, DSDFSY + WM was more effective in reducing IL-1, and DSCXQ + WM was better at reducing IL-6. Regarding the impact on oxidative stress markers, DSDFSY + WM had a more significant effect on NO regulation, GXN + WM was more evident in SOD regulation, and DH + WM had an advantage in MDA regulation.
This study found that 49 RCTs included adverse reactions as an observed outcome, with 17 RCTs reporting specific adverse reactions. Clinical manifestations were mainly concentrated in the circulatory system, digestive system, peripheral vessels, and skin. The most common adverse reactions were dizziness, nausea, and palpitations (n = 17, n = 14, n = 12), followed by headache (n = 7), abdominal distension, rash, bruising (n = 6), facial flushing (n = 4), and fatigue (n = 3). The active ingredients in Danshen have vasodilatory effects (Deng et al., 2014; Lin et al., 2022), which may cause dizziness, headache, and facial flushing in users. These conditions are generally tolerable and can resolve with reduced infusion speed or discontinuation of the drug. Traditional Chinese medicine injections, containing large molecular metabolites, are prone to allergic reactions, such as rashes. Rapid infusion of multiple drugs can increase the incidence of allergic reactions (Zou et al., 2023) Therefore, we recommend the following precautions when using injections: ① Infusion speed should not be too fast and can be slowed down according to the patient’s age and tolerance. ② Do not combine with other injections, especially other traditional Chinese medicine injections. ③ Strictly follow the instructions, and do not arbitrarily change the dosage or frequency of administration. We recommend that future studies place greater emphasis on safety monitoring, including: ① Routine monitoring of liver and renal function, especially in patients with pre-existing conditions, due to the known effects of herbal treatments. ② Observation for allergic reactions, particularly during the initial stages of treatment. ③ Careful monitoring for bleeding risks, given the potential anticoagulant effects of Danshen injections, particularly when used alongside antiplatelet or anticoagulant drugs.
Danshen, a commonly used herbal medicine in TCM for the treatment of CHD, has a long history of clinical application due to its blood-activating and stasis-removing properties, which promote blood circulation and remove blood stasis. Danshen contains two major metabolites: hydrophilic phenolic acids and lipophilic tanshinones, both of which possess anti-oxidative stress, anti-inflammatory, and anti-thrombotic effects (Li et al., 2020; Ke et al., 2023). Among these, tanshinones (TSN) have potent cardiovascular protective effects (Li ZM. et al., 2018). TSN modulates multiple pathways to inhibit the development of atherosclerosis. For instance, study (Ma et al., 2023) has shown that Tanshinone IIA (Tan IIA) can reduce vascular endothelial inflammation and prevent plaque formation through the COX-2/TNF-α/NF-κB signaling pathway. Tanshinone I (Tan I) can inhibit oxidative stress and oxidative stress-induced cardiomyocyte damage by regulating the Nrf2 signaling pathway (Wu et al., 2021). Salvia acid A (SAA) inhibits TLR2/TLR4-mediated Myd88 activation and its downstream molecules TRAF6 and IRAK4, thereby reducing the release of pro-inflammatory cytokines and mediators (Dawuti et al., 2023). Additionally, research indicates that SAA significantly enhances the expression of Nrf2 and HO-1 in a dose-dependent manner, improving atherosclerosis (Song et al., 2019). Furthermore, study has demonstrated that intraperitoneal injection of Danshen in chronic iron overload mice can decrease MDA levels, increase SOD activity, and reverse oxidative stress-induced damage (Zhang Y. et al., 2015). DSCIS inhibits endothelial cell autophagy via the miR-19a/SIRT1 pathway, mitigating the effects of oxidative stress (Guo et al., 2021). Study has found that DSCIS reduces MDA levels and increases SOD activity in a dose-dependent manner, reducing oxidative stress (Du et al., 2021). Other research has shown that DSCIS has a disease-specific bidirectional regulatory effect on angiogenesis, promoting the repair of ischemic vascular injury through angiogenic activity while inhibiting tumor growth through anti-angiogenic activity (He et al., 2022). The observed differences in efficacy among the various DSCIs may be attributed to differences in their active ingredients, formulations, and mechanisms of action. However, the complex composition of traditional Chinese medicine injections warrants further investigation to fully understand the underlying mechanisms.
However, this study has several limitations. Firstly, the quality of the included literature is not high, with most RCTs not detailing the methods of random allocation and blinding, potentially leading to selection bias and detection bias, thus reducing the accuracy of the study. Secondly, there is heterogeneity in this study, which may be related to various factors such as different WM treatment methods, inclusion of populations at different stages of CHD, and varying doses and intervention times of DSCIs. Thirdly, the studies included are concentrated in different regions of China, and the efficacy in other countries and ethnic groups has not been evaluated, which may affect the generalizability of the results. Fourthly, this study focuses on the overall CHD population, and the recommendations for individualized treatment for patients at different stages of the disease are not sufficiently accurate. To reduce potential biases, we established transparent inclusion and exclusion criteria to ensure consistency across studies. For missing data, we applied multiple imputation techniques, and studies of low quality were excluded to improve the overall reliability of the results.
Therefore, we believe that to improve the accuracy of NMA results and provide more effective treatment recommendations, future clinical studies should adhere to RCT standard designs, improve methodological quality, and describe methodological key points in detail when publishing results to enhance the quality of evidence-based medicine. We hope future research directions that emphasize the need for larger, multicenter trials involving diverse populations across different countries and ethnic groups. This approach will enhance the robustness of our findings and contribute to a more comprehensive understanding of the studied phenomena. Despite certain limitations, the NMA analysis in this study evaluates the effects of different treatment regimens on various outcome indicators, providing recommendations for clinical treatment of CHD.
5 Conclusion
In summary, this study demonstrates that the combination of DSCIs and WM treatment is more effective than WM treatment alone for patients with CHD. This includes improvements in clinical symptoms, electrocardiogram efficacy evaluation, and hematological parameters (inflammatory markers and oxidative stress markers). Overall, DSDFSY and DSCXQ showed favorable performance in clinical efficacy evaluation and inflammatory marker modulation, while DH exhibited stable performance in oxidative stress regulation. Although this study partially confirmed the efficacy of DSCIs, there are still shortcomings in the level of evidence and clinical application. In the future, we hope to conduct rigorous, high-quality randomized controlled trials to further clarify the efficacy and mechanisms of DSCIs, thereby facilitating their clinical use.
Author contributions
SD: Conceptualization, Data curation, Investigation, Software, Validation, Visualization, Writing–original draft. YD: Data curation, Investigation, Software, Validation, Visualization, Writing–original draft. JG: Formal Analysis, Methodology, Supervision, Writing–review and editing. XW: Formal Analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by Grants from the National Natural Science Foundation of China (No. 8227142388), the National Administration of Traditional Chinese Medicine (No. ZYYZDXK-2023259 and No. 2024-JYB-KYPT-10).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1487119/full#supplementary-material
Abbreviations
DSCIs, Danshen class injection; CHD, coronary heart disease; NMA, network meta-analysis; RCT, randomized controlled trials; CNKI, China National Knowledge Infrastructure; VIP, China Science and Technology Journal Database; CBM, Chinese Biomedical Literature Database; CCS, chronic coronary syndrome; ACS, acute coronary syndrome; PCI, percutaneous coronary intervention; TCM, traditional Chinese medicine; TSN, tanshinones; Tan IIA, Tanshinone IIA; Tan I, Tanshinone I; SAA, Salvia acid A; WM, western medicine; DH, Danhong injection; DS, Danshen injection; DSCXQ, Danshenchuanxiongqin injection; DSDFSY, Dansenduofensuanyan injection; DSFZ, Danshenfen injection; FFDS, Fufang Danshen injection; GXN, Guanxinning injection; STS, Sodium Tanshinone IIA Sulfonate injection; XD, Xiangdan injection; SXPTT, Shenxiongputaotang injection. hs-CRP, high-sensitivity C-reactive protein; IL-1, interleukin-1; IL-6, interleukin-6; NO, nitric oxide; SOD, superoxide dismutase; MDA, malondialdehyde.
References
Bi, C. W., Chen, Z. L., and Bi, C. F. (2011). The effect of Shenxiong glucose injection on high-sensitivity C-reactive protein, endothelin, and quality of life in elderly patients with unstable angina pectoris. Shandong Med. J. 51 (41), 65–66.
Broch, K., Anstensrud, A. K., Woxholt, S., Sharma, K., Tøllefsen, I. M., Bendz, B., et al. (2021). Randomized trial of interleukin-6 receptor inhibition in patients with acute ST-segment elevation myocardial infarction. J. Am. Coll. Cardiol. 77 (15), 1845–1855. doi:10.1016/j.jacc.2021.02.049
Byrne, R. A., Rossello, X., Coughlan, J. J., Barbato, E., Berry, C., Chieffo, A., et al. (2023). 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 44 (38), 3720–3826. doi:10.1093/eurheartj/ehad191
Cai, L. L., Li, J. H., Xu, J. G., and Li, D. M. (2014). Effect of Danshen ligustrazine for injection on blood rheology, hs-CRP and fat metabolism on elderly patients with unstable angina pectoris. Pract. Pharm. Clin. Remedies 17 (3), 267–270.
Cao, X. F., and Liu, C. R. (2013). The effect of Danhong injection on blood lipids, endothelial function, and inflammatory markers in patients with coronary heart disease and angina pectoris. China Rural. Health, 103.
Chen, F. L., Wang, X. L., and Ma, B. (2020). Evaluation for the treatment effect of salvianolate and its influence on the hemorheology and oxidative stress in angina pectoris patients. Chin. J. Disaster Med. 8 (3), 137–141.
Chen, J. H., Han, Y., and Wang, X. F. (2015b). Danhong injection for the treatment of 94 cases of unstable angina pectoris with blood stasis type. Henan Tradit. Chin. Med. 35 (7), 1525–1527.
Chen, J. L., Wan, J., and Wang, A. L. (2012). Influence of sodium tanshinon Ⅱasilate on high sensitivity C-reactive protein and matrix metalloproteinase-9 of patients with unstable angina pectoris. Shandong Med. J. 52 (29), 41–42.
Chen, S., Zhang, J., Yan, F. D., Yan, J. F., Yuan, B., and He, S. H. (2009). Changes in serum levels of nitric oxide, endothelin, and vascular endothelial growth factor in patients with stable angina pectoris and the intervention effect of salvianolic acid salts. Chin. J. Clin. Pharmacol. Ther. 14 (10), 1160–1163.
Chen, S. L., and Huang, S. B. (2016a). Effect of Salvia miltiorrhiza on cytokines in patients with unstable angina pectoris. J. Hainan Med. Univ. 22 (8), 744–746.
Chen, S. L., and Huang, S. B. (2016b). Effects of Salvia miltiorrhiza on hemorheology and vascular endothelial function in patients with unstable angina pectoris. J. Hainan Med. Univ. 22 (10), 954–956.
Chen, S. Q., Li, L. P., Ning, P., and Wang, B. D. (2015a). The therapeutic effect and pharmacological analysis of Danhong injection in the treatment of unstable angina pectoris. J. China Prescr. Drug 13 (07), 37–38.
Chen, Y. J., Jian, F., and Chen, Y. K. (2021). Effeet of salvianolate on serum IL-6 and hs-CRP in patients with unstable angina pectoris. Chongqing Med. J. 50 (S1), 28–31.
Cumpston, M., Li, T., Page, M. J., Chandler, J., Welch, V. A., Higgins, J. P., et al. (2019). Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 10 (10), ED000142. doi:10.1002/14651858.ED000142
Dawuti, A., Sun, S., Wang, R., Gong, D., Liu, R., Kong, D., et al. (2023). Salvianolic acid A alleviates heart failure with preserved ejection fraction via regulating TLR/Myd88/TRAF/NF-κB and p38MAPK/CREB signaling pathways. Biomed. Pharmacother. 168, 115837. doi:10.1016/j.biopha.2023.115837
Deng, Y., Ng, E. S., Kwan, Y. W., Lau, C. B. S., Cheung, D. W. S., Koon, J. C. M., et al. (2014). Cerebral vasodilator properties of Danshen and Gegen: a study of their combined efficacy and mechanisms of actions. Phytomedicine 21 (4), 391–399. doi:10.1016/j.phymed.2013.09.016
Du, H., Li, C., Wang, Z., He, Y., Wang, Y., Zhou, H., et al. (2021). Effects of Danhong injection on dyslipidemia and cholesterol metabolism in high-fat diets fed rats. J. Ethnopharmacol. 274, 114058. doi:10.1016/j.jep.2021.114058
Duan, X. L., Ji, X. W., Zhang, A. Y., Zhang, J. G., Zhao, C. H., and Yang, L. L. (2010). The effect of Salvianolate on unstable angina pectoris and its influence on the levels of SOD and MDA. Acta Acad. Med. Weifang 32 (1), 23–25.
Eikelboom, J. W., Anand, S. S., Malmberg, K., Weitz, J. I., Ginsberg, J. S., and Yusuf, S. (2000). Unfractionated heparin and low-molecular-weight heparin in acute coronary syndrome without ST elevation: a meta-analysis. Lancet 355 (9219), 1936–1942. doi:10.1016/S0140-6736(00)02324-2
Everett, B. M., MacFadyen, J. G., Thuren, T., Libby, P., Glynn, R. J., and Ridker, P. M. (2020). Inhibition of interleukin-1β and reduction in atherothrombotic cardiovascular events in the CANTOS trial. J. Am. Coll. Cardiol. 76 (14), 1660–1670. doi:10.1016/j.jacc.2020.08.011
Fang, Y., Yang, K. P., and Jin, D. (2018). The effects of vascular endothelial growth factor, serum brain natriuretic peptide precursor, and soluble signaling hormone 4D. Mod. J. Integr. Traditional Chin. West. Med. 27 (35), 3964–3967.
Feng, Z. H., and Ji, X. W. (2010). Clinical study of salvianolate in early admission period in patients with unstable angina. J. Liaoning Univ. Traditional Chin. Med. 12 (4), 54–56.
Fibrinolytic Therapy Trialists (FTT) (1994). Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Fibrinolytic Therapy Trialists' (FTT) Collaborative Group. Lancet 343 (8893), 311–322.
Fu, T., and Jiang, C. H. (2015). Effects of Danhong injection on serum sICAM-1 and hs-CRP in patients with unstable angina pectoris. J. Electrocardiol. Circulation 34 (4), 256–258, 278.
Fu, Y. C., and Meng, L. Q. (2011). Clinical observation on the treatment of coronary heart disease and angina pectoris with Guanxinning injection. New Chin. Med. 43 (8), 8–9.
Gao, S., Liu, Z., Li, H., Little, P. J., Liu, P., and Xu, S. (2012). Cardiovascular actions and therapeutic potential of tanshinone IIA. Atherosclerosis 220 (1), 3–10. doi:10.1016/j.atherosclerosis.2011.06.041
Gao, W., Shi, Y. Y., and Suo, D. M. (2009). Clinical efficacy observation of Beitong Danhong injection in the treatment of unstable angina pectoris. Liaoning J. Traditional Chin. Med. 36 (2), 235–236.
Gorog, D. A., Sweeny, J. M., and Fuster, V. (2009). Antiplatelet drug 'resistance'. Part 2: laboratory resistance to antiplatelet drugs-fact or artifact? Nat. Rev. Cardiol. 6 (5), 365–373. doi:10.1038/nrcardio.2009.13
Guan, J. S., Zhou, Y., Miao, Z. J., Gao, S. Z., and Chen, J. (2019). Effect of salvianolate on endothelial function and oxidative stress in patients with coronary heart disease. China Pharm. 28 (24), 75–77.
Guo, G. l., Li, C. H., and Sun, L. Q. (2016). The effects of visfatin. matrix metalloproteinases-9 and hypersensitive C-reactive protein by the treatment of depside salt from salvia miltiorrhiza in ST-segment elevation myocardial infarction patient. J. Clin. Intern Med. 33 (9), 614–616.
Guo, Y., Yang, J. H., Cao, S. D., Gao, C. X., He, Y., Wang, Y., et al. (2021). Effect of main ingredients of Danhong Injection against oxidative stress induced autophagy injury via miR-19a/SIRT1 pathway in endothelial cells. Phytomedicine 83, 153480. doi:10.1016/j.phymed.2021.153480
Hansson, G. K. (2005). Inflammation, atherosclerosis, and coronary artery disease. N. Engl. J. Med. 352 (16), 1685–1695. doi:10.1056/NEJMra043430
He, S., Chen, R., Peng, L., Jiang, Z., Liu, H., Chen, Z., et al. (2022). Differential action of pro-angiogenic and anti-angiogenic components of Danhong injection in ischemic vascular disease or tumor models. Chin. Med. 17 (1), 4. doi:10.1186/s13020-021-00557-5
Hong, Y. D., Wu, H., Mo, H. H., and Li, F. Y. (2004). Effeet of xiangdan injection in treating acute coronary syndrome and inflammatory markers. Traditional Chin. Drug Res. Clin. Pharmacol. 15 (6), 425–428.
Hu, A. Y., and Liu, L. (2011). The effect of Danhong injection on vascular endothelial function and inflammatory factors in patients with unstable angina pectoris. Her. Med. 30 (3), 319–321.
Huang, D. P. (2017). The therapeutic effect of Danhong injection on unstable angina pectoris patients and its effect on serum CRP, Cys-C, and Hcy. World Clin. Med. 11 (21), 74–75.
Hutton, B., Salanti, G., Caldwell, D. M., Chaimani, A., Schmid, C. H., Cameron, C., et al. (2015). The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern Med. 162 (11), 777–784. doi:10.7326/M14-2385
Huynh, T., Perron, S., O’Loughlin, J., Joseph, L., Labrecque, M., Tu, J. V., et al. (2009). Comparison of primary percutaneous coronary intervention and fibrinolytic therapy in ST-segment-elevation myocardial infarction: bayesian hierarchical meta-analyses of randomized controlled trials and observational studies. Circulation 119 (24), 3101–3109. doi:10.1161/CIRCULATIONAHA.108.793745
Ji, S. L. (2013). Clinical efficacy analysis of Danshen Chuanxiong Injection in the treatment of acute coronary syndrome. Mod. Diagnosis Treat. 24 (4), 794–795.
Jiang, X. (2022). Effect of salvianolate adjuvant therapy on hemodynamics, inflammatory factors and cardiomyocyte apoptosis in patients with unstable angina pectoris. Med. Innovation China 19 (13), 58–63.
Jiang, Z. P., Ji, X. W., Zhang, A. Y., Zhang, J. G., Zhao, C. H., Chen, Y. B., et al. (2012). The effect of salvianolic acid salts on inflammatory response in patients with unstable angina pectoris. Chin. J. Clin. Electron. Ed. 6 (19), 6097–6098.
Jiao, W. P., and Wang, Q. F. (2019). Clinical effect of salvianolate in the treatment of unstable angina pectoris. Clin. Res. Pract. 4 (5), 29–30.
Jin, J., Liu, L., and Du, L. J. (2012). The effect of tanshinone IIA on plasma endothelin and nitric oxide levels in patients with unstable angina pectoris. Inf. Traditional Chin. Med. 29 (6), 62–63.
Jing, L. X. (2014). Effects of Salvianolate intervention on heart rate turbulence and myocardial injury serum index in patients with unstable angina. Med. J. Chin. People's Health 26 (21), 8–10.
Kaufmann, P. A., Gnecchi-Ruscone, T., di Terlizzi, M., Schäfers, K. P., Lüscher, T. F., and Camici, P. G. (2000). Coronary heart disease in smokers: vitamin C restores coronary microcirculatory function. Circulation 102 (11), 1233–1238. doi:10.1161/01.cir.102.11.1233
Ke, L., Zhong, C., Chen, Z., Zheng, Z., Li, S., Chen, B., et al. (2023). Tanshinone I: pharmacological activities, molecular mechanisms against diseases and future perspectives. Phytomedicine 110, 154632. doi:10.1016/j.phymed.2022.154632
Knuuti, J., Wijns, W., Saraste, A., Capodanno, D., Barbato, E., Funck-Brentano, C., et al. (2020). 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 41 (3), 407–477. doi:10.1093/eurheartj/ehz425
Lang, X. F. (2012). 60 cases of unstable angina treated with integrated traditional Chinese and Western medicine. Acta Chin. Med. Pharmacol. 40 (6), 96–98.
Li, C., Kang, D., and Wu, Y. S. (2008). Clinical research of Danhong injection for amelioration of microcirculation in patients with unstable angina. Clin. J. Med. Officers 36 (3), 402–404.
Li, H., Chai, H., Wang, L. Z., Yang, H. Y., and Ma, D. M. (2009b). Observation of guanxinning injection on antioxidant damage in initial type of exercised angina pectoris. China Med. Her. 30 (24), 24–25.
Li, H., Li, X. C., Jia, X. R., Wei, C., Xu, Z. R., and Huang, Y. Q. (2009a). The effect and therapeutic effect of Danhong injection on hypersensitive C-reactive protein in patients with unstable angina pectoris. Shaanxi Med. J. 37 (8), 1054–1055.
Li, H., and Wang, L. Z. (2007). Clinical observation of the anti free radical effect of Guanxinning injection on patients with worsening fatigue angina pectoris. Clin. Med. China 23 (10), 874–876.
Li, H., and Yang, H. Y. (2008). The therapeutic effect and endothelial function of Danhong injection on elderly patients with unstable angina pectoris. Shandong Med. J. 48 (32), 92–93.
Li, H. D., Lin, X. Y., Liu, Q. W., and Zhang, Y. (2018b). Curative effect of Danhong injection on the clinical symptoms, adverse reactions and electrocardiogram of angina pectoris of coronary heart disease. Int. J. Clin. Exp. Med. 11 (2), 910–915.
Li, M., Li, H., Liu, H., Lai, X., and Xing, W. (2022). Efficacy and safety of eight types Salvia miltiorrhiza injections in the treatment of unstable angina pectoris: a network meta-analysis. Front. Pharmacol. 13, 972738. doi:10.3389/fphar.2022.972738
Li, S. M., Shang, Q. H., Chen, K. J., and Hao, X. (2014). GW25-e4351 sodium tanshinone IIA sulfate reduces elevated serum high sensitivity C-reactive protein in patients with coronary heart disease: a prospective randomized open-label blinded end point trial. J. Am. Coll. Cardiol. 64 (16), C206. doi:10.1016/j.jacc.2014.06.956
Li, X., Wang, W. B., Cao, S. J., and Zhang, Y. (2018a). The effects of salvianolic acid salts on TNF - alpha, hs - CRP, IL - 1, and cardiac function in patients with unstable angina pectoris. J. Clin. Exp. Med. 17 (5), 499–503.
Li, Y. F., and Yin, G. (2012). The effect of Salvia miltiorrhiza ligustrazine injection in UAP for aged people. Qingdao Med. J. 44 (2), 130–132.
Li, Y. H., and Ge, H. Y. (2011). Observation on the treatment of acute coronary syndrome with Danhong injection. J. Med. Forum 32 (11), 150–152.
Li, Y. M., Chen, X. H., Li, J., Hu, J. P., Bian, Y. L., and Wu, Y. J. (2007). Clinical study on danshen injection in the treatment of acute coronary syndrome. Chin. J. Traditional Med. Sci. Technol. 14 (6), 392–393.
Li, Z., Zou, J., Cao, D., and Ma, X. (2020). Pharmacological basis of tanshinone and new insights into tanshinone as a multitarget natural product for multifaceted diseases. Biomed. Pharmacother. 130, 110599. doi:10.1016/j.biopha.2020.110599
Li, Z. M., Xu, S. W., and Liu, P. Q. (2018c). Salvia miltiorrhizaBurge (Danshen): a golden herbal medicine in cardiovascular therapeutics. Acta Pharmacol. Sin. 39 (5), 802–824. doi:10.1038/aps.2017.193
Liao, Y. H., Liu, X., Deng, Y. M., and Hu, J. J. (2008). The effect of Danhong injection on serum high-sensitivity C-reactive protein in patients with unstable angina pectoris. China Med. 3 (6), 334–335.
Lin, Q. W., Wei, Z. B., Yao, C. Y., and Lu, Y. L. (2020). Effect of salvianolic acid salt on endothelial function in patients with coronary atherosclerotic heart disease. Chin. J. Mod. Drug Appl. 14 (21), 147–148.
Lin, Y. K., Chen, Y. J., Li, J. Y., Chen, Y. L., He, D., Zuo, R., et al. (2022). Salvianolic acid A from Danhong Injection induces vasorelaxation by Regulating L-type calcium channel in isolated mouse arteries. J. Ethnopharmacol. 296, 115431. doi:10.1016/j.jep.2022.115431
Liu, B., and Wang, B. J. (2013). Observation on the therapeutic effect of Danhong injection in the treatment of unstable angina pectoris. Guide China Med. 11 (1), 606–607.
Liu, G. D., and Xiao, G. L. (2014). Effect of the salvia phenolic acid on high sensitivity C reactive protein and hemorheology in patients with unstable angina. J. Emerg. Traditional Chin. Med. 23 (1), 3–5.
Liu, J., Li, D. D., Dong, W., Liu, Y. Q., Wu, Y., Tang, D. X., et al. (2021). Detection of an anti-angina therapeutic module in the effective population treated by a multi-target drug Danhong injection: a randomized trial. Signal Transduct. Target Ther. 26 (1), 329. doi:10.1038/s41392-021-00741-x
Liu, J. Z., Wang, T., Zhao, Y. G., Pan, Z. X., and Yuan, X. Q. (2015). The therapeutic effect of Danshen Chuanxiong Injection on elderly patients with unstable angina pectoris and its effects on serum hs-CRP and blood lipids. Pharmacol. Clin. Chin. Materia. 31 (4), 237–239.
Liu, L. L., Yan, Y. J., and Gu, S. Z. (2023). Evaluation of the efficacy of salvianolate adjuvant therapy in patients with unstable angina pectoris. Northwest Pharm. J. 38 (4), 169–173.
Liu, M. Y. (2017). Study on the effect and therapeutic effect of salvianolic acid salts on hemorheology in elderly patients with unstable angina pectoris. Pract. Clin. J. Integr. Traditional Chin. West. Med. 17 (1), 15–16.
Liu, S., Wu, J., Zhang, D., and Tan, D. (2018). What are the best Salvia miltiorrhiza injection classes for treatment of unstable angina pectoris? A systematic review and network Meta-analysis. J. Tradit. Chin. Med. 38 (3), 321–338. doi:10.1016/s0254-6272(18)30623-x
Liu, Y. F., Xu, L. J., Xu, Z. X., Zhao, W. H., and Liu, X. T. (2012). Danhong injection in the treatment of 48 cases of unstable angina pectoris with coronary atherosclerotic heart disease. China Pharm. 21 (20), 109–110.
Lu, J., and Ma, P. X. (2023). Observation on the clinical effect of injectable salvianolic acid salts in the treatment of coronary heart disease angina pectoris. Pract. Clin. J. Integr. Traditional Chin. West. Med. 23 (6), 11–13.
Lun, J., Ji, X. W., Zhang, A. Y., Zhao, C. H., Zhang, J. G., and Chen, Y. B. (2011). Effect of Salvianolate on unstable angina and its influence on NO and ET. Chin. J. Clin. Ration. Drug Use. 4 (2), 1–2.
Luo, X. C., and Huang, T. (2011). The effect of Danhong injection on vascular endothelial function and cardiac function in unstable angina pectoris. J. Mil. Surg. Southwest China 13 (03), 469–470.
Lv, X. S. (2018). Influence of salvianolate on endothelial function and homocysteine level in elderly patients with unstable angina pectoris. J. Electrocardiol. Circulation 37 (2), 117–120.
Ma, X., Zhang, L., Gao, F., Jia, W., and Li, C. (2023). Salvia miltiorrhiza and Tanshinone IIA reduce endothelial inflammation and atherosclerotic plaque formation through inhibiting COX-2. Biomed. Pharmacother. 167, 115501. doi:10.1016/j.biopha.2023.115501
Mach, F., Baigent, C., Catapano, A. L., Koskinas, K. C., Casula, M., Badimon, L., et al. (2020). 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur. Heart J. 41 (1), 111–188. doi:10.1093/eurheartj/ehz455
Malekmohammad, K., Sewell, R. D. E., and Rafieian-Kopaei, M. (2019). Antioxidants and atherosclerosis: mechanistic aspects. Biomolecules 9 (8), 301. doi:10.3390/biom9080301
Mao, Y. Y., Wang, J. Q., Wang, C. X., and Wang, C. X. (2016). Effect of salvianolate on serum levels of hs-CRP and TNF a in unstable angina patients. Clin. Focus 31 (2), 191–192, 197.
Martin, S. S., Blaha, M. J., Blankstein, R., Agatston, A., Rivera, J. J., Virani, S. S., et al. (2014). Dyslipidemia, coronary artery calcium, and incident atherosclerotic cardiovascular disease: implications for statin therapy from the multi-ethnic study of atherosclerosis. Circulation 129 (1), 77–86. doi:10.1161/CIRCULATIONAHA.113.003625
Mehta, S. R., Bassand, J. P., Chrolavicius, S., Diaz, R., Eikelboom, J. W., Fox, K. A., et al. (2010). Dose comparisons of clopidogrel and aspirin in acute coronary syndromes. N. Engl. J. Med. 363 (10), 930–942. doi:10.1056/NEJMoa0909475
Mei, F. G., Wang, Z. L., Zhang, Y. Q., and Zhao, G. (2014). Clinical study on the effect of Danshen Chuanxiong Injection on endothelial function in patients with unstable angina pectoris. Chin. J. Traditional Med. Sci. Technol. 21 (z2), 17.
Mei, F. G., Zhang, Y. Q., Wang, Z. L., and Zhao, G. (2006). The effect of Danhong injection on serum hypersensitive C-reactive protein in patients with unstable angina pectoris. Pract. J. Cardiac Cereb. Pneumal Vasc. Dis. 14 (12), 972–973.
Mou, L. N. (2011). Clinical observation of sodium tanshinone IIA sulfonate in the treatment of coronary heart disease angina pectoris. Guide China Med. 9 (27), 252–253.
National Center for Cardiovascular Disease (2023). China cardiovascular Health and disease report 2022. Beijing: Science Press.
National Health Commission of the People's Republic of China (2021). China Health statistics Yearbook 2021. Beijing: Peking Union Medical College Press.
Neumann, F. J., Sousa-Uva, M., Ahlsson, A., Alfonso, F., Banning, A. P., Benedetto, U., et al. (2019). 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 40 (2), 87–165. doi:10.1093/eurheartj/ehy394
Nidorf, S. M., Fiolet, A. T. L., Mosterd, A., Eikelboom, J. W., Schut, A., Opstal, T. S. J., et al. (2020). Colchicine in patients with chronic coronary disease. N. Engl. J. Med. 383 (19), 1838–1847. doi:10.1056/NEJMoa2021372
Nikolakopoulou, A., Mavridis, D., Furukawa, T. A., Cipriani, A., Tricco, A. C., Straus, S. E., et al. (2018). Living network meta-analysis compared with pairwise meta-analysis in comparative effectiveness research: empirical study. BMJ 360, k585. doi:10.1136/bmj.k585
Padro, T., Manfrini, O., Bugiardini, R., Canty, J., Cenko, E., De Luca, G., et al. (2020). ESC Working Group on Coronary Pathophysiology and Microcirculation position paper on 'coronary microvascular dysfunction in cardiovascular disease. Cardiovasc Res. 116 (4), 741–755. doi:10.1093/cvr/cvaa003
Pan, D. M., Liu, Q. P., and Yang, C. J. (2024). Clinical efficacy and safety analysis of salvianolate in treatment of coronary heart disease. Med. Innovation China 15 (35), 50–53.
Pang, Z., Zha, G., and Xu, E. F. (2014). Influence of salvia miltiorrhiza phenolic acid salt on blood rheology and endothelial function in elderly patients with unstable angina. Pract. Geriatr. 17 (1), 38–40.
Peng, H. S., Liu, C. Y., Yang, Y. P., and Lai, Y. W. (2015). Influence study of danhong injection in the serum GDF-15, hs-CRP and NT-proBNP of unstable angina pectoris patients. China and Foreign Med. Treat. 34 (23), 108–110.
Qi, L. P., Wang, T. P., Shi, X. G., and Li, Q. (2001). Study on the antioxidant effect of Danshen injection on patients with stable angina pectoris. Acta Univ. Med. Anhui 36 (4), 287–288.
Qiu, C. Z., Lu, Y. G., Huang, J. Z., Chen, L. Y., He, D. M., and Chen, L. (2017). Changes and significance of serum inflammatory factors and endothelial cell microparticle levels in unstable angina patients treated with salvianolic acid salts as adjunctive therapy. Shandong Med. J. 57 (7), 52–54.
Qiu, D., Wang, F., and Zhao, T. (2018). Treatment effect of salvianolateand its influence on the hemorheology and oxidative stress in angina pectoris patients. Anhui Med. Pharm. J. 22 (1), 147–151.
Qiu, Y. H. (2020). Clinical efficacy analysis of salvianolic acid salts in the treatment of stable angina pectoris. Chin. J. Urban Rural Enterp. Hyg. (1), 158–159.
Riemersma, R. A. (1996). Coronary heart disease and vitamin E. Lancet 347 (9004), 776–777. doi:10.1016/s0140-6736(96)90861-2
Shi, Y. P., and Liu, B. (2012). Efficacy observation of 156 cases of senile unstable angina pectoris treated with danhong injection. World J. Integr. Traditional West. Med. 7 (10), 883–886.
Song, G. M., Li, Y., and Gao, Y. (2015). Effect of Salvia TMP on laboratory indicators and its efficacy on patients with unstable angina pectoris. Chin. J. Biochem. Pharm. 35 (12), 102–104, 107.
Song, J. J., Yang, Y. J., Su, T., and Zhao, Q. X. (2017). Effect of salvia miltiorrhiza injection on unstable angina pectoris, serum inflammatory factors and metabonomics. Zhejiang J. Integr. Traditional Chin. West. Med. 27 (12), 1026–1031.
Song, Q. T., Zhang, Y. Y., Han, X., Zhang, Y., Zhang, X., Gao, Y. G., et al. (2019). Potential mechanisms underlying the protective effects of salvianic acid A against atherosclerosis in vivo and vitro. Biomed. Pharmacother. 109, 945–956. doi:10.1016/j.biopha.2018.10.147
Su, C. Y., Ming, Q. L., Rahman, K., Han, T., and Qin, L. P. (2015). Salvia miltiorrhiza: traditional medicinal uses, chemistry, and pharmacology. Chin. J. Nat. Med. 13 (3), 163–182. doi:10.1016/S1875-5364(15)30002-9
Su, X. M., Zhi, X. W., Liu, J. X., He, Y. J., Ma, Y., and Wang, Y. X. (2011). Impact of danhong injection on paraoxonase 1, superoxide dismutase activity and malondialdehyde levels in aged patients with coronary heart disease. Chin. General Pract. 14 (33), 3804–3806.
Sun, K., Fu, C., Nie, S. H., and You, Y. (2014). The index and improvement effect of using Danhong injection to patients with atherosclerosis symptoms of coronary heart disease (CHD). Pak J. Pharm. Sci. 27 (5), 1699–1704.
Sun, L., and Zhang, S. H. (2024). Sixty cases with chronic heart failure treated with shenmai rongxin decoction. Henan Tradit. Chin. Med. 35 (7), 1520–1521.
Tan, S. J., Guo, H. F., and Lu, Y. (2009). The effect of salvianolic acid salts on endothelial function in elderly patients with unstable angina pectoris. Pract. Geriatr. 23 (2), 126–128.
Tao, L., Song, C. Y., and Chen, D. (2024). Efficacy of salvianolate in the treatment of patients with unstable angina pectoris and its effect on hs - CRP. Chin J Clin. Ration. Drug Use 7 (2), 46–47.
Törnwall, M. E., Virtamo, J., Korhonen, P. A., Virtanen, M. J., Taylor, P. R., Albanes, D., et al. (2004). Effect of alpha-tocopherol and beta-carotene supplementation on coronary heart disease during the 6-year post-trial follow-up in the ATBC study. Eur. Heart J. 25 (13), 1171–1178. doi:10.1016/j.ehj.2004.05.007
Valgimigli, M., Bueno, H., Byrn, R. A., Collet, J. P., Costa, F., Jeppsson, A., et al. (2018). 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 39 (3), 213–260. doi:10.1093/eurheartj/ehx419
Wang, N., and Bi, Y. (2017). The effect of salvianolic acid salts on related cytokines in patients with unstable angina pectoris. Mod. J. Integr. Traditional Chin. West. Med. 26 (2), 184–186.
Wang, S. (2009). Observation on the therapeutic effect of Danhong injection in the treatment of unstable angina pectoris. Guide China Med. 11 (5), 113.
Wang, S. J., and Wang, Y. H. (2020). Study on the effect of Danhong injection on endothelial glycocalyx in patients with coronary heart disease. J. Med. Theory Pract. 33 (16), 2648–2650.
Wei, J., Wu, T., Yang, Q., Chen, M., Ni, J., and Huang, D. (2011). Nitrates for stable angina: a systematic review and meta-analysis of randomized clinical trials. Int. J. Cardiol. 146 (1), 4–12. doi:10.1016/j.ijcard.2010.05.019
Wei, Q., and Shen, X. J. (2014). Effects of tanshinone Ⅱ on clinical symptoms and vascular aging factor in angina pectoris of coronary heart disease patients. J. Basic Chin. Med. 20 (6), 783–785.
Wight, L. J., VandenBurg, M. J., Potter, C. E., and Freeth, C. J. (1992). A large scale comparative study in general practice with nitroglycerin spray and tablet formulations in elderly patients with angina pectoris. Eur. J. Clin. Pharmacol. 42 (3), 341–342. doi:10.1007/BF00266360
Wu, J. R., Liu, S., Zhang, X. M., and Zhang, B. (2017). Danshen injection as adjuvant treatment for unstable angina pectoris: a systematic review and meta-analysis. Chin. J. Integr. Med. 23 (4), 306–311. doi:10.1007/s11655-016-2272-0
Wu, X. L., Pei, X., Li, D. Y., Li, J. M., Yang, D. Y., Gao, Y. L., et al. (2010). Effect of salvianolate on serum cytokins level in elderly patients with unstable angina pectoris. Chin. J. Integr. Med. Cardio-Cerebrovascular Dis. 8 (2), 158–160.
Wu, Y. T., Xie, L. P., Hua, Y., Xu, H. L., Chen, G. H., Han, X., et al. (2021). Tanshinone I inhibits oxidative stress-induced cardiomyocyte injury by modulating Nrf2 signaling. Front. Pharmacol. 12, 644116. doi:10.3389/fphar.2021.644116
Wu, Z. M., Luo, X. Y., and Wang, S. H. (2012). The therapeutic effect of salvianolic acid salts on unstable angina pectoris and their effects on CRP, NO, and ET-1. Henan Tradit. Chin. Med. 32 (7), 864–865.
Xi, H. W., Liu, G. F., and Yang, W. (2015). Influence of Shenxiong glucose injection on heart function, blood lipid and inflammatory factors in patients with unstable angina. J. Liaoning Univ. Traditional Chin. Med. 17 (9), 82–84.
Xia, L., and Zhang, H. L. (2022). Efficacy of salvia polyphenolic acid salt in elderly patients with coronary artery disease and its effect on blood lipids. Med. Innovation China 19 (26), 56–59.
Xie, Q. T., Liu, J. L., Wang, H. R., Yuan, S. F., Zhao, J., and Yang, X. H. (2020). Clinical trial of salvianolate in the treatment of patients with angina pectoris. Chin. J. Clin. Pharmacol. 36 (1), 3–6.
Xie, S., and Cao, C. (2011). Affection of hemorrheology and hyper - sensitive C – RP of danhong injection on unstable angina. Heilongjiang Med. J. 35 (9), 660–662.
Xu, L. J., Liu, X. K., and Liu, Y. F. (2014). Treatment of 46 cases of coronary heart disease and angina pectoris with guanxinning injection. China Pharm. 23 (14), 107.
Xu, Z. J., and Hao, S. Y. (2022). Effects of salviae miltiorrhizae and ligustrazine hydrochloride injection on cardiovascular function and antioxidant function in patients with unstable angina pectoris of coronary heart disease. Clin. Res. Pract. 7 (10), 122–125.
Yan, C. G., and Zeng, J. Q. (2009). The effect of Danhong injection on vascular endothelial function in patients with unstable angina pectoris. Shandong Med. J. 49 (8), 78–79.
Yang, C. P., and Shi, G. (2009). The effect of Danhong injection on inflammatory factors in patients with unstable angina pectoris. J. Pingxiang Univ. 26 (3), 99–101.
Yang, L. L., Ji, X. W., Zhang, A. Y., Zhang, J. G., and Duan, X. L. (2010). Clinical observation of salvianolic acid injection in the treatment of unstable angina pectoris. Chin. J. Clin. Ration. Drug Use. 3 (2), 1–2.
Yang, N., and Ren, F. X. (2010). Sulfotanshinone sodium for unstable angina pectoris: a study of clinical application. China Mod. Dr. 48 (21), 47–49.
Yao, H. (2022). Treatment methods and clinical application analysis of coronary heart disease in elderly people over 60 years old. Med. Health (4), 5–8.
Ye, T. H., Li, X. H., Zhong, Y. T., and Chen, H. X. (2021). The effect of salvianolic acid salts as adjunctive therapy for coronary heart disease angina pectoris and their impact on oxidative stress. Inner Mongolia. J. Traditional Chin. Med. 40 (1), 58–60.
Yu, M. H., and Fang, S. (2016). Clinical curative effect observation of salvia miltiorrhiza ligustrazine injection in treating angina pectoris of coronary heart disease. Clin. J. Chin. Med. 8 (6), 44–45.
Yu, M. K., and Jiao, L. Q. (2014). Effect of salvianolate injection on plasma high-sensitivity C reactive protein and tumor necrosis factor and soluble cell apoptosis factor in unstable angina patients. Hebei J. Traditional Chin. Med. 36 (1), 11–13.
Yue, H. J., Yang, P. P., and Li, L. M. (2023). Effect of salvianolic acid on ischemic cardiomyopathy. Henan Med. Res. 32 (13), 2447–2450.
Zhang, B. H. (2011). The effects of Danhong injection on inflammatory factors, thromboxane B2, and hemorheology in patients with unstable angina pectoris. Chin. J. Integr. Med. Cardio-Cerebrovascular Dis. 9 (9), 1055–1057.
Zhang, C. J., An, Q. H., and Zheng, Y. M. (2018). Expression and intervention study of NF-κB, TNF-α, IL-1 and IL-6 in patients with unstable angina pectoris. J. Binzhou Med. Univ. 41 (3), 168–170.
Zhang, L. L., Jiang, N., Qu, G., and Gao, S. S. (2010). A comparative study of three commonly used traditional Chinese medicine preparations combined with conventional Western medicine therapy for the treatment of unstable angina pectoris. Chin. J. Integr. Med. Cardio-Cerebrovascular Dis. 8 (4), 388–390.
Zhang, R. H. (2010). Influence of salvianolate on clinical efficacy, endothelial function and C-reactive protein in patients with unstable angina pectoris. Mod. Hosp. 10 (5), 35–37.
Zhang, S. G., He, L. M., Liu, S. Y., Li, Q. Y., and Tan, R. R. (2012). Clinical observation on the efficacy and safety of traditional Chinese medicine for promoting blood circulation and removing blood stasis in the treatment of acute coronary syndrome. China and Foreign Med. Treat. 31 (13).
Zhang, W., Ji, N. J., Mei, Y. B., and Hu, C. S. (2015a). The effect of salvianolic acid salts on serum Ang Ⅱ, IL-6, and hs CRP in elderly patients with unstable angina pectoris. Chin. J. Traditional Med. Sci. Technol. 22 (6), 683–684.
Zhang, X. Y. (2016). Effect discussion of salvianolic acid on blood lipid and inflammatory factors of patients with unstable angina pectoris of coronary heart disease. World Latest Med. Inf. 16 (59), 13–14.
Zhang, Y., Wang, H., Cui, L. J., Zhang, Y. Y., Liu, Y., Chu, X., et al. (2015b). Continuing treatment with Salvia miltiorrhiza injection attenuates myocardial fibrosis in chronic iron-overloaded mice. PLoS One 10 (4), e0124061. doi:10.1371/journal.pone.0124061
Zhang, Y., Xie, Y., Liao, X., Jia, Q., and Chai, Y. (2017). A Chinese patent medicine Salvia miltiorrhiza depside salts for infusion combined with conventional treatment for patients with angina pectoris: a systematic review and meta-analysis of randomized controlled trials. Phytomedicine 25, 100–117. doi:10.1016/j.phymed.2017.01.002
Zhang, Z. J. (2017). The effect of tanshinone IIA sodium sulfonate injection on inflammatory factors in unstable angina pectoris. all Health 11 (2), 130–131.
Zhao, B., Wang, J., and Song, Y. B. (2015). Effects of Danhong Iniection on unstable factors and vascular endothelial function of inflammation in patients with angina pectoris. J. Liaoning Univ. Traditional Chin. Med. 17 (9), 182–184.
Zhao, H., Zhang, Y. C., and Pu, S. J. (2011). Clinical application and evaluation of Danhong injection for patients with unstable angina. Sichuan J. Anat. 19 (4), 10–12.
Zhou, S. N., and Guo, H. (2018). The effect of salvianolic acid salts in the treatment of coronary heart disease and their impact on ET-1 and NO levels. Laboratory Med. Clin. 15 (11), 1680–1683.
Zhu, Q. K. (2019). The effect of salvianolic acid salts as adjunctive therapy for unstable angina on inflammatory response and angina attacks. J. Med. Theory Pract. 32 (13), 2015–2016.
Zhu, Y., and He, Y. H. (2002). Clinical observation of Danshen powder injection in the treatment of unstable angina pectoris. J. Emerg. Traditional Chin. Med. 11 (4), 253–254.
Keywords: danshen class injections, Chinese medicine injection, coronary heart disease, network meta-analysis, randomized controlled trial
Citation: Dai S, Ding Y, Guo J and Wang X (2024) Efficacy and safety of danshen class injections in the treatment of coronary heart disease: a network meta-analysis. Front. Pharmacol. 15:1487119. doi: 10.3389/fphar.2024.1487119
Received: 27 August 2024; Accepted: 25 November 2024;
Published: 12 December 2024.
Edited by:
Qing Yong He, China Academy of Chinese Medical Sciences, ChinaReviewed by:
Jiale Zhang, China Academy of Chinese Medical Sciences, ChinaChenyang Ji, University of Malaya, Malaysia
Copyright © 2024 Dai, Ding, Guo and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xian Wang, d3hpYW4yMDIyMTJAMTYzLmNvbQ==
†These authors have contributed equally to this work.