
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 06 August 2024
Sec. Pharmacology of Infectious Diseases
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1406960
 Adina Fésüs1,2*
Adina Fésüs1,2* Phiona Baluku1Éva Sipos1Sándor Somodi3
Phiona Baluku1Éva Sipos1Sándor Somodi3 Enikő Berczi-Kun1
Enikő Berczi-Kun1 István Lekli1Ildikó Bácskay2,4Ria Benkő5,6Attila Vaskó7
István Lekli1Ildikó Bácskay2,4Ria Benkő5,6Attila Vaskó7Background: Community-acquired pneumonia (CAP) is one of the leading causes of death worldwide. Antibiotic stewardship program (ASP) has been implemented to improve rational and responsible antibiotic use by encouraging guideline adherence.
Objective: This retrospective observational before–after study aimed to evaluate whether the ASP may improve guideline adherence, antibiotic exposure, and clinical outcomes in patients hospitalized due to CAP in Hungary.
Methods: The study was conducted at a pulmonology department of a tertiary care medical center in Hungary. The ASP implementation consisted of written and published guidelines available to all professionals, continuous supervision, and counseling services on antibiotic therapies at an individual level, with the aim of ensuring compliance with CAP guidelines. Overall guideline adherence (agent selection, route of administration, and dose), clinical outcomes (length of stay and 30-day mortality), antibiotic exposure, and direct costs were compared between the two periods. Fisher’s exact test and t-test were applied to compare categorical and continuous variables, respectively. P-values below 0.05 were defined as significant.
Results: Significant improvement in overall CAP guideline adherence (30.2%), sequential therapy (10.5%), and a significant reduction in the total duration of antibiotic therapy (13.5%) were observed. Guideline non-adherent combination therapies with metronidazole decreased significantly by 28.1%. Antibiotic exposure decreased by 7.2%, leading to a significant decrease in direct costs (23.6%). Moreover, the ASP had benefits for clinical outcomes, and length of stay decreased by 13.5%.
Conclusion: The ASP may play an important role in optimizing empirical antibiotic therapy in CAP having a sustained long-term effect.
The use of antibiotics is a cornerstone for the causal treatment of bacterial pneumonia, especially of community-acquired pneumonia (CAP), one of the most common infectious diseases requiring hospitalization (Kosar et al., 2017).
Mortality and morbidity due to antibiotic resistance have increased significantly in recent years (Antimicrobial Resistance et al., 2022). Although the use of antibacterial agents has significantly reduced CAP-related mortality, their inappropriate use has led to the emergence of antibiotic resistance (Lopez-Lozano et al., 2019; Ghosh et al., 2020). Consequently, inappropriately treated CAP may be associated with prolonged hospital stay, placing a heavy financial burden on the healthcare system (Fine et al., 2000; Luthi-Corridori et al., 2023). In 2020 in Hungary, standardized death rates for pneumonia were 8.9 per 100,000 inhabitants for women and 17.1 per 100,000 inhabitants for men. However, these rates included deaths caused by COVID pneumonia (Eurostat, 2024). Moreover, between 2016 and 2021, the average length of stay for pneumonia among in-patients decreased from 12.2 to 10.9 days (Eurostat, 2024). In our country, based on the latest surveillance data on the antimicrobial consumption of the ECDC (European Center for Disease Prevention and Control), the total antimicrobial consumption (community and hospital sector) was 14.4 DDD/1000 inhabitants/day, out of which 1.04 DDD/1000 inhabitants/day indicates the use of antibiotics in the hospital sector (Control, 2023). Furthermore, in the last 10 years, based on the ECDC surveillance report, there has been no decrease in antibiotic consumption in the Hungarian hospital care sector. In fact, a marked increase could be observed in the proportional use of reserve antibiotics used for the treatment of confirmed or suspected infections due to multidrug resistant organisms (Benko et al., 2022; Control, 2024; EC, 2024; ECDC, 2024).
At the same time, prescribing antibiotic treatment has become a major health challenge worldwide. The antibiotic stewardship program (ASP) is implemented to improve the rational and responsible use of antibiotics to improve disease outcomes and reduce antibiotic resistance, healthcare-related infections, and healthcare costs (Tiri et al., 2020). However, the appropriate ASP can only be planned after the identification of antibiotic treatment practices (choice of agent, dosage, dosage form, and duration) (Szalka, 2013; Tiri et al., 2020).
The use of the ASP resulted in significantly lower antibiotic exposure, decreased inappropriate antibiotic use, and limited unintended consequences such as antimicrobial resistance development (Garau et al., 2014). According to a multicenter controlled before-and-after study in Denmark, the ASP led to significantly lower antibiotic exposure and a higher guideline-adherent empirical antibiotic exposure, but without reduction in intravenous therapy (Fally et al., 2021). Another pre–post-intervention study conducted in a pediatric community healthcare center in Israel shows that the ASP resulted in a reduction in broad-spectrum antibiotic use and an increase in guideline-adherent treatment of CAP (Cohen et al., 2022).
To our knowledge, there has been no published official national ASP strategy yet in Hungary. Nevertheless, at the department of pulmonology, a local ASP was implemented with the aim to slow the emergence of antibiotic resistance and optimize antibiotic use. The aims of this study were to evaluate the impact of ASP on guideline adherence in relation to antibiotic selection, route of administration, dose and duration, antibiotic exposure, and costs, as well as clinical outcomes in CAP.
This was a single-center retrospective observational before–after study managed at the pulmonology department of a tertiary care center in Hungary. At the tertiary care center level, an ASP (titled antibiotic stewardship pilot project) was implemented in June 2019 with the aim of controlling antibiotic use. Restricted antibiotics were listed, which were allowed to be prescribed by physicians and dispensed by the clinical pharmacist only with the permission of infectious disease specialists. Furthermore, written local guidelines for CAP were available at the wards in the pulmonology department, adherence to which was not mandatory but strongly recommended. The COVID pandemic interrupted the ASP, which was resumed in June 2022. However, written guidelines remained available even after the pandemic (10 January 2021). Consequently, data collection in the pre-intervention phase was carried out from 1 January to 30 April 2022, while in the ASP phase, it was from 1 January to 31 March 2023, months with the highest number of CAP cases. Ethics approval was obtained from the Regional Institutional Research Ethics Committee, Clinical Center, University of Debrecen (DE RKEB/IKEB: 6267-2022).
The ASP was introduced in all inpatient care units of the aforementioned center in order to plan the analysis and control of the reasonable and cost-effective use of antibiotics (Center, 2022). The ASP was carried out by the AST (antimicrobial stewardship team) interdisciplinary team consisting of physician specialists (in this study pulmonologists), microbiologists, infectious disease specialists, and pharmacists. The ASP instructions included antibiotic protocols (prophylaxis and empirical therapy), restricted (controlled) antibiotic agents, individual regulation of antibiotic use by infectious disease specialists, elements of infection control, and analysis of antibiotic use. Furthermore, the ASP-guided empirical antibiotic therapy, which was developed based on the local microbiological resistance map and evidence-based antibiotic use. According to these criteria, the narrowest-spectrum agent was recommended in an appropriate dose, adapted to the location and type of infection, for the shortest possible therapeutic period, and in the most optimal route of administration, preferably in monotherapy. Moreover, to reduce the risk of spreading resistance and ensure prudent use, a restriction on antibiotics has been introduced. Restricted antibiotics are as follows: ciprofloxacin, levofloxacin, moxifloxacin, cefiderocol, ceftaroline, ceftazidime/avibactam, ceftolozane/tazobactam, imipenem/cilastatin, meropenem, imipenem/cilastatin/relebactam, meropenem/vaborbactam, linezolid, tedizolid, aztreonam, and colistin. The use of these antibiotics was allowed only after infectious disease specialist approval. An electronic approval request form was filled by the pulmonologist and sent to the infectious disease specialist. Required data consisted of patient data, required agent (based on positive microbiological test results—pathogen and sensitivity—or pulmonologist decision when no microbiological test is available and no clinical improvement), first empirical antibiotic therapy, present clinical outcomes, and pulmonologist contact information. Restricted antibiotics could have been dispensed only by the clinical pharmacist under strict control after the approval of the consultant infectologist (Figure 1).
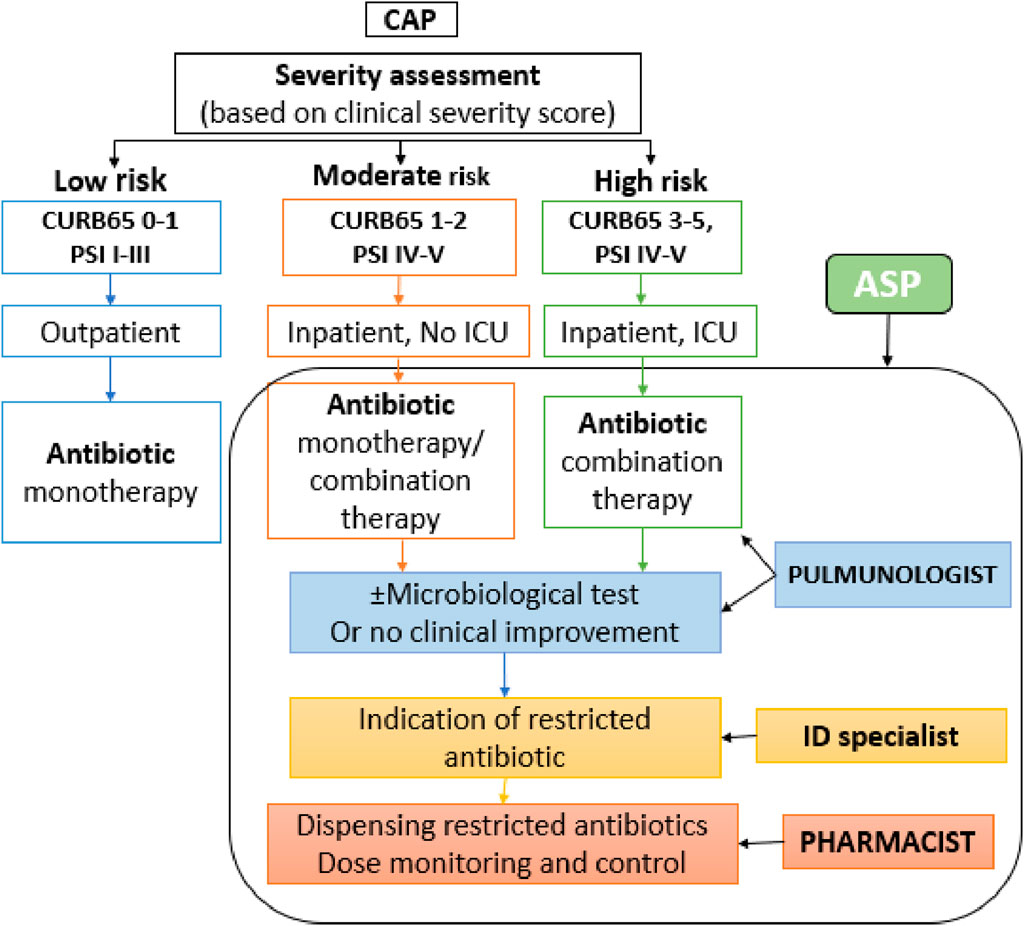
Figure 1. Implemented ASP. CAP, community-acquired pneumonia; CURB-65, confusion, uremia, respiratory rate, blood pressure, (age ≥65 years) score; PSI, Pneumonia Severity Index; ICU, intensive care unit; ID: infectious diseases.
To predict 30-day mortality in CAP, CURB-65 (NICE—National Institute for Health and Care Excellence guideline) score and PSI (Pneumonia Severity Index) were used and determined (Fine, 2023; Macfarlane, 2023). According to the local guideline, patients with CURB65 score 1–5 or PSI IV–V mostly required hospitalization. The local guideline for CAP for inpatients is presented in Table 1.
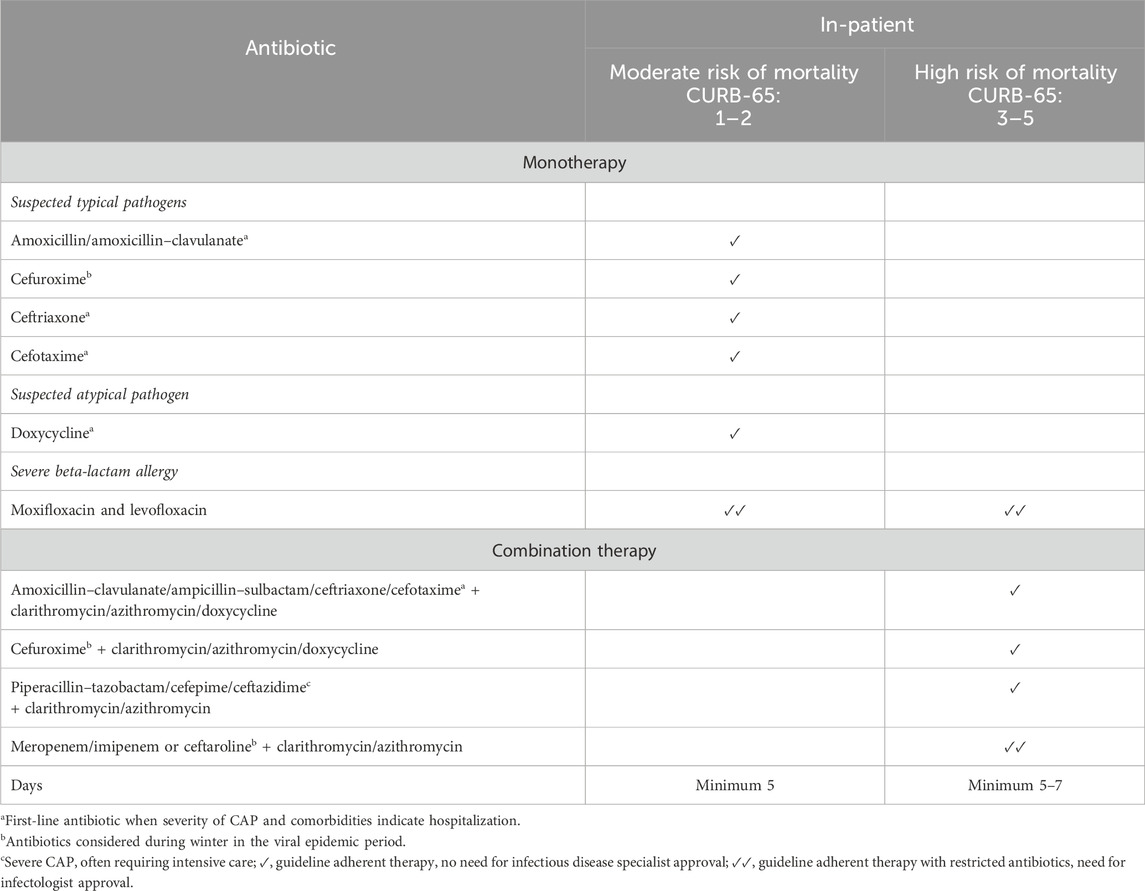
Table 1. Guideline-adherent empirical antibiotic therapy in this study (Debrecen, 2023).
Based on the local guidelines, the recommended systemic antibiotic for moderate risk of mortality was mainly monotherapy, while combination therapy was recommended mainly for high risk of mortality (Debrecen, 2023). Empirical antibiotic treatment was recommended to start within 4 to 6 hours after hospital admission. According to the route of administration, starting therapy with intravenous administration was recommended. Switching from intravenous to oral therapy should be considered after clinical stability, in the case of a moderate infection of CAP, as far as absorption and pharmacokinetics allow. Furthermore, contraindications, severe penicillin allergy, and dose adjustment in kidney failure (after an adequate loading dose) should be considered. The proposal for the total duration of empirical antibiotic therapy was 5 days, with prolongation only in particularly justified cases (e.g., immunodeficiency or positive microbiological tests).
Adult (18 years or above) patients hospitalized due to CAP (based on ICD–International Classification of Disease code) who started their first empirical antibacterial therapy at the above-mentioned department were included in the study. All patients with CAP admitted from another hospital/ward having antibiotic therapy or coinfections at admission were excluded from the study.
All patient- and therapy-related data were collected manually by pharmacists. All data were assembled from medication charts and UD-MED Hospital Information System (IT Services, Hungary) and recorded in Microsoft Excel by using a predefined format of the data entity. Data collection forms were designed by the pharmacists. Demographics and clinical characteristics (gender, age, allergies, Charlson Comorbidity Index (CCI), weight, comorbidities, and discharge type), signs and symptoms (chills, fever, cough, dyspnea, chest pain, breathlessness, malaise, collapse, confusion, respiratory rate, blood pressure, presence of sputum, and dehydration) at admission, chest X-ray examination, laboratory test results (blood urea nitrogen (BUN) concentration, sodium, glucose, hematocrit, partial pressure of oxygen, respiratory rate, blood pressure, heart rate, pH, white blood cells (WBC), C-reactive protein (CRP), creatinine, estimated glomerular filtration rate (eGFR), lactase dehydrogenase enzyme (LDH), microbiological tests, and pathogens), empirical antibiotic therapy (agent selection, route of administration, dose, and duration), and clinical outcomes (30-day survival and length of stay (LOS)) were recorded on data collection forms. Empirical treatment is defined as the antibacterial therapy initiated based on the presence of suspected pathogens without any microbiological testing. Patients were anonymized, thus making them unidentifiable in the study.
The data obtained in both (pre-intervention phase and ASP phase) periods were analyzed and compared. We compared empirical antibiotic use regimen (types: mono- or combination therapy of the first empirical therapy, agent selection, dosage, and duration), the rate of guideline adherence, need for antibiotic change, antibiotic exposure (DDD/patient), antibiotic costs, as well as clinical outcomes (30-day survival and length of stay), and the need for antibiotic prescription at discharge.
Antibiotic exposure was determined using the World Health Organization’s ATC/DDD index (version 2023). The defined daily dose (DDD) is the assumed average maintenance dose per day for an agent used for its main indication in adults. Direct empirical antibiotic costs were calculated based on actual prices obtained from the central hospital pharmacy and expressed in HUF/patient. Antibiotic selection and duration of antibiotic use recommended for CAP are included in Table 5. One treatment followed by another was considered consecutive therapy. Any switch from an intravenous to oral regimen was considered sequential therapy. Empirical antibiotic therapy was considered guideline-adherent when all members were used appropriately regarding the severity of CAP. LOS indicated the number of days that the patient spent in the hospital.
The obtained data were compared to evaluate the effects of ASP implementation on empirical antibiotic use. We applied interrupted time-series analysis (ITSA) to express antibiotic prescription patterns in CAP in pre-intervention and ASP periods.
Fisher’s exact test was applied to compare categorical variables, while Pearson’s correlation coefficient and t-test were used to compare continuous variables between the two study periods. P values below 0.05 were defined as significant.
In the pre-intervention and ASP periods, data from n = 131 and n = 227 patients, respectively, were collected, out of which data obtained from 78.6% to 85.5% patients met the study criteria and were included in the research. Included and excluded patients are mentioned in Table 2.
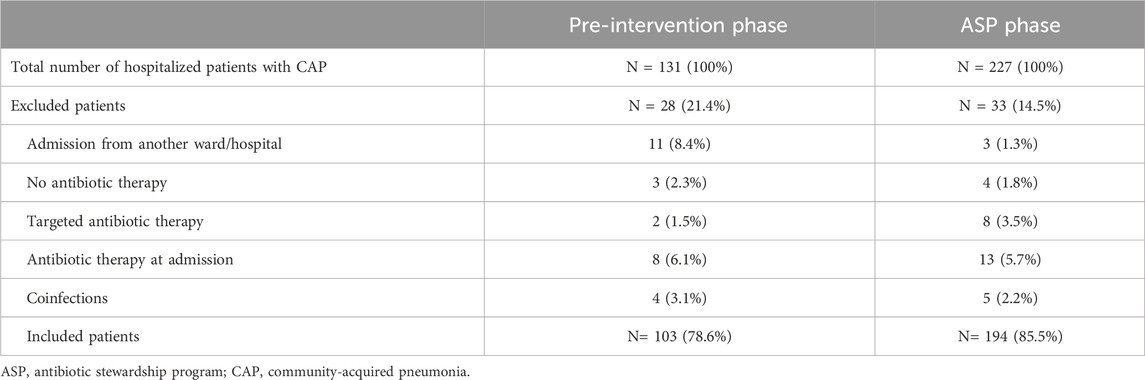
Table 2. Patients included and excluded from the study.
Demographic and clinical characteristics of patients hospitalized with CAP are described in Table 3. No significant differences were found regarding their gender, age, comorbidities, discharge types, outcomes, PSI, and CURB-65 scores between the two periods. In both periods, more than half of the patients (61–59.2% and 112–57.7%, respectively) were men, aged between 65 and 84 years, and had a CCI score above 4. The most common comorbidities included chronic obstructive pulmonary diseases and cardiovascular diseases. The majority of patients were discharged home. The 30-day mortality rates were 27.2% and 21.6%, with 21.4% and 19.1% being in-hospital deaths (Table 3).
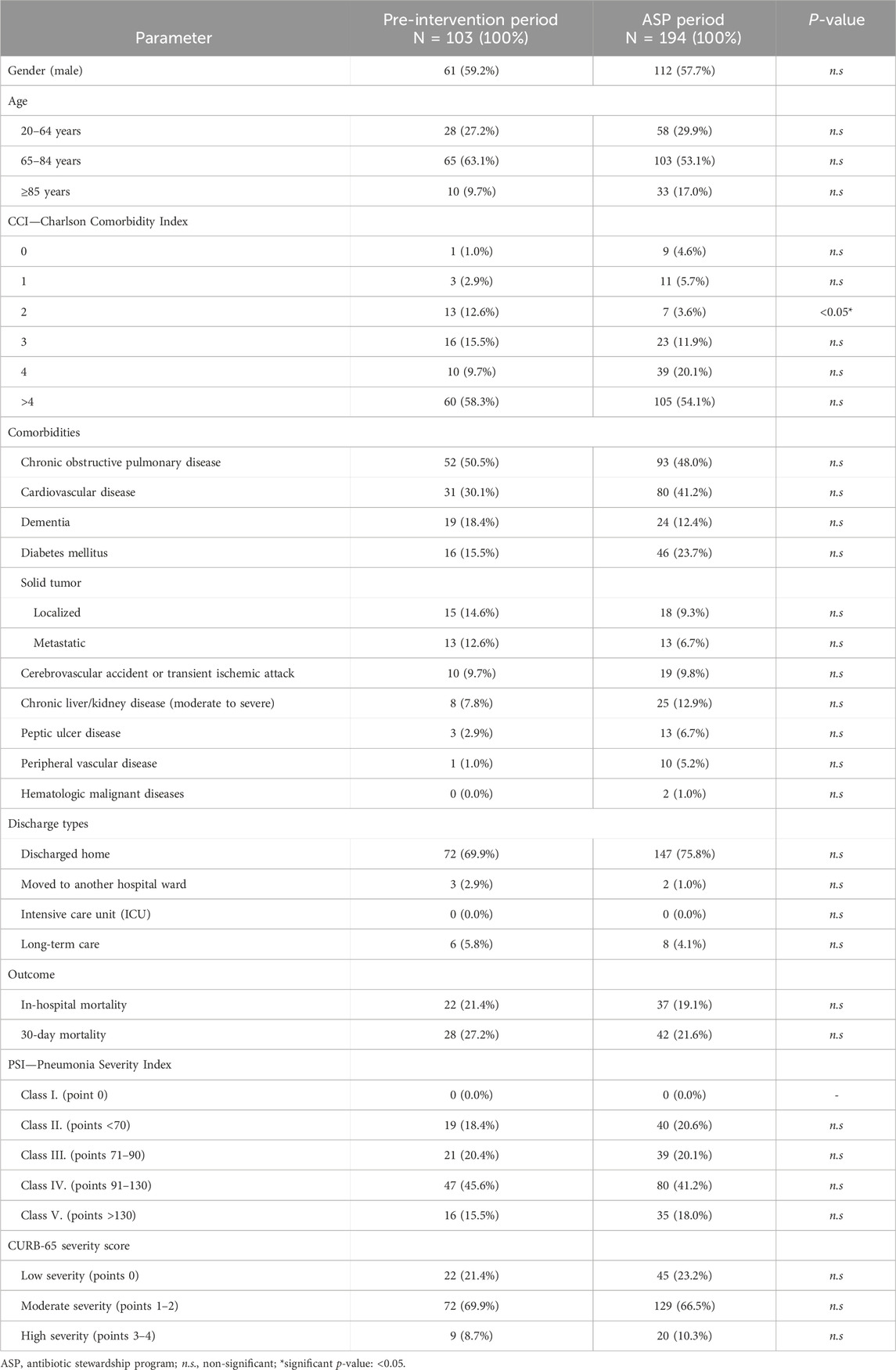
Table 3. Demographic and clinical characteristics of patients with CAP in the pre-intervention and ASP periods.
Signs and symptoms at admission are listed in Table 4. No significant differences were found regarding signs and symptoms between the two periods.
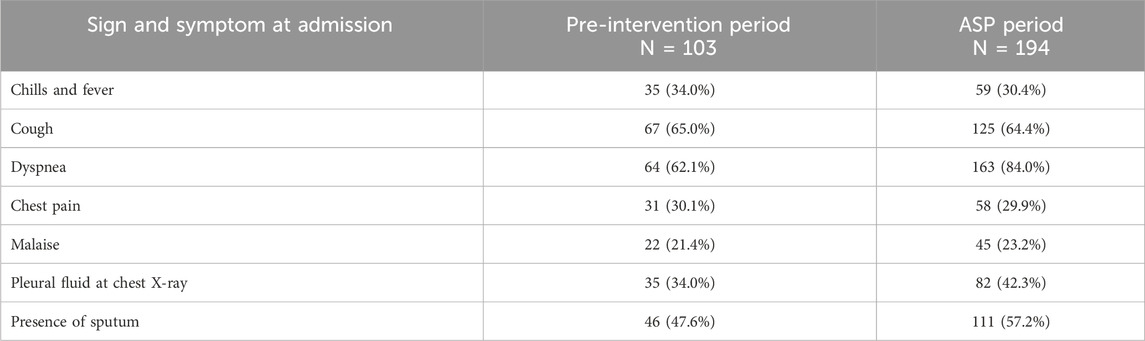
Table 4. Sign and symptoms at admission.
The characteristics of empirical antibiotic therapy in CAP and outcomes are summarized in Table 5. Combination therapy was used for CAP in both the periods in the vast majority of cases (pre-intervention period: 74.8% vs ASP period: 76.8%). In the ASP period, the guideline-adherent agent selection increased significantly by 35% (from 58.3% to 93.3%; p = 0.015). However, the overall (agent selection, route of administration, dosage, and duration) guideline adherence increased only by 6.2% (p > 0.05). The inappropriate use of clarithromycin and doxycycline decreased by 38.2% (pre-intervention period: 5.8% vs., ASP period: 3.6%; p > 0.05), while respiratory fluoroquinolones were not used in the ASP period. At the same time, significant decreases in the use of guideline non-adherence combinations with metronidazole (p < 0.05) were observed between the two periods. In both periods, overdosing was relatively high (7.8% and 8.2%, respectively), while underdosing was not frequent. In the ASP period, shorter-duration antibiotic therapy (˂7 days) was significantly more frequent (47.0% vs. 22.3%; p = 0.004), while the total duration of in-hospital antibiotic therapy decreased significantly by 16% (from median 8 to 6 days; p < 0.001). Moreover, the total duration of antibiotic therapy, including antibiotic prescriptions at discharge, decreased by 4.5% (from 10.74 ± 4.78, median 11 days to 9.87 ± 4.95, median 10 days; p > 0.05). Furthermore, in the ASP period, a significant increase in the number of consecutive therapies (by 13.2%, from 14.6% to 27.8%; p = 0.045) was observed, whereas switching from intravenous to oral route of administration resulted in an increase by 10.5% (from 3.9% to 14.4%; p = 0.010). However, in the majority of cases, there were no significant differences in changes between the first empirical therapy (80.6% and 72.2%, respectively) and escalation (14.6% and 11.3%; p > 0.05).
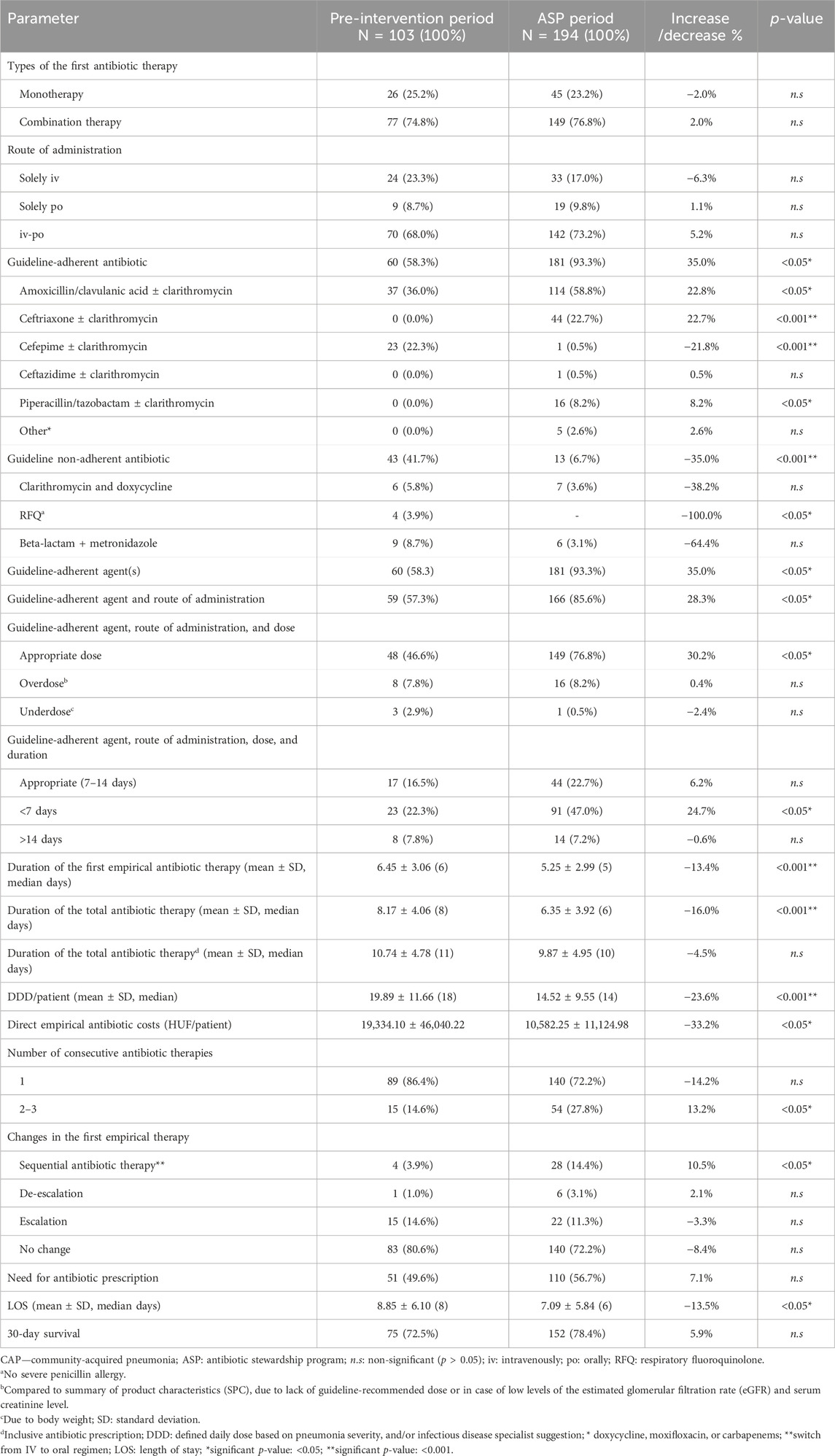
Table 5. Characteristics of empirical antibacterial therapy of CAP in the study periods.
Antibiotic exposure in the ASP period decreased significantly by 23.6% (from 19.89 ± 11.66 to 14.52 ± 9.55 DDD/patient; p < 0.001). As expected, the decrease in the CAP duration led to a lower costs of direct antibiotic therapy after ASP implementation (by 33.2%, from 19,334.10 ± 46,040.22 to 10,582.25 ± 11,124.98 HUF/patient; p < 0.001) (Table 5).
The correlation coefficient between the two periods was −0.19 DDD/patient/day (95% CI –0.3831 to 0.0096), suggesting that the ASP has a sustained long-term effect (Figures 2, 3).
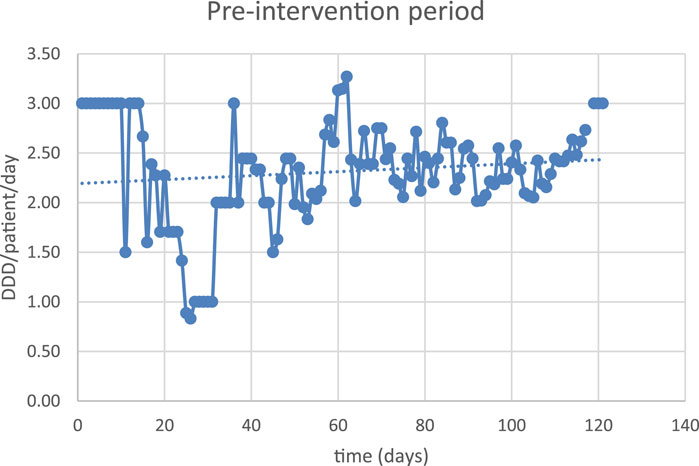
Figure 2. Antibiotic exposure in the pre-intervention period.
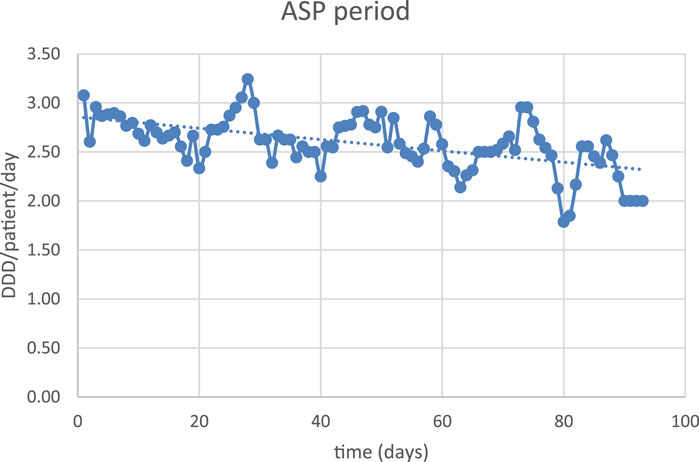
Figure 3. Antibiotic exposure in the ASP period.
In our study, comparing the pre-intervention period and ASP period revealed that the mean LOS decreased significantly by 13.5% (from 8.85 ± 6.10, median 8 days to 7.09 ± 5.84, median 6 days; p = 0.016). Guideline non-adherent combination therapies of beta-lactams with metronidazole were associated with prolonged LOS in both periods (pre-intervention period: 13.33 ± 9.79, median 11 days and ASP period: 9.5 ± 5.68, median 7 days) compared to the average LOS. Furthermore, we found that the 30-day survival rate increased by 5.9% (from 72.5% to 78.4%; p > 0.05) (Table 5).
Antimicrobial resistance continues to spread rapidly worldwide, threatening global public health (Allel et al., 2023). Antimicrobial stewardship programs (ASP) and local guidelines for empirical antibiotic therapies aim to slow the evolution of antibiotic resistance and improve clinical outcomes (WHO, 2021). CAP is still one of the most common acute infections requiring antibiotic therapy, and irresponsible antibiotic prescription may lead to overuse and misuse of these agents. The descriptions of guideline-adherent empirical antibiotic use in hospitalized patients with CAP vary widely (47.8%–65%) in the literature (Blasi et al., 2008; McCabe et al., 2009; Munther et al., 2023). In our previous study evaluating antibiotic prescription patterns, guideline adherence, and clinical outcomes in patients hospitalized with CAP (Fesus et al., 2022), there were no available local guidelines, and guideline adherence for agent selection was found to be low (30.6%). In contrast, in the pre-intervention period, when written guidelines were present on the ward, guideline adherence was found to be higher (58.3%).
Our healthcare center implemented its own strategy to optimize antibiotic use, in which physicians, infectious disease specialists, and clinical pharmacists had opportunities and responsibilities in optimizing empirical antibiotic therapies inclusive for CAP at the pulmonological department.
This study shows that in the pre-intervention period, the guideline non-adherent antibiotic use was relatively common (41.7%) for CAP in the pulmonological department. The quite frequent (8.7%) and redundant combinations of beta-lactams with metronidazole were associated with prolonged LOS.
In contrast, in the ASP period, the combination of the written local guideline and the restricted use of antibiotics resulted in significantly higher guideline adherence in agent selection (by 35%, from 58.3% to 93.3%) and remarkable improvement in LOS (by 13.5%, from mean 8.85 to 7.09 and median 8 to 6 days) in CAP. Although the 30-day survival also increased by 5.9% (from 72.5% to 78.4%), it was not statistically significant. Moreover, a significant improvement (by 30.2%, from 46.6% to 76.8%) in the appropriate use of antibiotics regarding agent selection, route of administration, and dosage was observed in the ASP period. Inappropriate use of metronidazole combination therapy was also decreased (by 64.4%, from 8.7% to 3.1%). Moreover, ASP led to a significant decrease in the total duration of antibiotic therapy (by 16.0%, from median 8 to 6 days), which in fact was associated with the significant decrease in direct empirical antibiotic costs. It should be noted that the sequential antibiotic therapy increased significantly by 10.5%. Although de-escalation and escalation also occurred, these efforts were not significant. At the same time, despite the lower antibiotic exposure and shorter duration of total empirical antibiotic therapy, the clinical outcomes (LOS) were improved (Table 5).
Based on the available evidence, it was found that ASP implementation was safe and led to benefits both for healthcare systems and patients (Viasus et al., 2017). In line with our results, the findings worldwide show that the ASP in CAP led to an increase in appropriate antibiotic therapy as well as a lower antibiotic exposure and duration of the antibiotic therapy (Markus Fally et al., 2020). A single-centered prospective pre- and post-intervention study showed an excessive decrease (from a median of 10 to 7 days, p ˂ 0.001) in the duration of antibiotic therapy with an ASP intervention (Avdic et al., 2012). In a study conducted at the Johns Hopkins Hospital among patients with CAP, the shorter-duration antibiotic therapy was shown to be as clinically effective as the longer-duration one (Nussenblatt et al., 2013). As indicated by our study results, half of the patients needed antibiotic prescriptions at discharge, and there was no difference between the two periods.
Several studies focused on de-escalation of empirical antibiotic therapy in CAP (Fally et al., 2021; Helen Umpleby et al., 2022; Waagsbo et al., 2022). According to a multi-center prospective study, the ASP resulted in a significantly higher rate of guideline-adherent antibiotic treatment and lower overall antibiotic exposure. However, there was no observed decrease in sequential therapy (Fally et al., 2021). At the same time, an observational study conducted in a teaching university hospital in Norway found that there was an existing need to complete the ASP for better antibiotic de-escalation strategies (Waagsbo et al., 2022). A narrative review evaluating the efficacy and risks of the ASP focused on de-escalation found that de-escalation is safe and encourages application of efforts also in this direction (Helen Umpleby et al., 2022). A cross-sectional study with the implemented ASP focused on decreasing the mean broad-spectrum days of the therapy, which yielded an absolute reduction of 1.7 days. The authors stated that a multifaceted ASP might safely reduce broad-spectrum antibiotic use (Schweitzer et al., 2022).
In line with the literature, in our study, the implementation of the ASP led to better clinical outcomes (LOS) and a significant decrease in direct empirical antibiotic therapy costs. A systematic review evaluating LOS, antibiotic exposure, and total costs after ASP implementation states that the highest cost savings came from scaling down of LOS, a fact observed mainly in those hospitals where the ASP included antibiotic restrictions as well (Nathwani et al., 2019).
The manual data collection provided us first-hand observations on the antibiotic use in CAP at the pulmonological department. However, retrospective data collection from medical charts may contain inaccurate information or biases arising from inappropriate coding in electronic medical systems.
One of the most important limitations of the present study was that it is a single-center study involving a limited number of patients. The second limitation was that the study was conducted after 6 months of ASP implementation since in the pre-intervention period, due to the COVID pandemic, infectious disease specialists were redirected to infectious wards, and data collection was also obstructed. The ASP was implemented in January with the aim of collecting data according to the seasonal occurrence of CAP, and in June 2023, the CAP guidelines included in the ASP also underwent a few modifications.
ASP implementation led to a significant improvement in overall guideline adherence, appropriate antibiotic use, sequential therapy, and a significant reduction in the total duration of empirical antibiotic therapy. The ASP was accompanied by a significant decrease in the hospital length of stay. Our study result suggests that the ASP may play an important role in optimizing empirical antibiotic therapy in CAP with a sustained long-term effect.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Regional Institutional Research Ethics Committee, Clinical Center, University of Debrecen (DE RKEB/IKEB: 6267-2022). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
AF: conceptualization, data curation, formal analysis, investigation, methodology, writing–original draft, and writing–review and editing. PB: data curation, formal analysis, investigation, writing–original draft. ÉS: data curation, investigation, and writing–original draft. SS: resources and writing–review and editing. EB-K: data curation, investigation, writing–review and editing. IL: resources, validation, and writing–review and editing. IB: resources and writing–review and editing. RB: formal analysis, investigation, validation, and writing–review and editing. AV: supervision, and writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. AF was supported by the University of Debrecen Program for Scientific Publication.
The authors would like thank the staff of the Department of Pulmonology at the Faculty of Medicine of the University of Debrecen Clinical Center, Hungary.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Allel, K., Day, L., Hamilton, A., Lin, L., Furuya-Kanamori, L., Moore, C. E., et al. (2023). Global antimicrobial-resistance drivers: an ecological country-level study at the human-animal interface. Lancet Planet Health 7 (4), e291–e303. doi:10.1016/S2542-5196(23)00026-8
Antimicrobial Resistance, C., Ikuta, K. S., Sharara, F., Swetschinski, L., Robles Aguilar, G., Gray, A., et al. (2022). Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 399 (10325), 629–655. doi:10.1016/s0140-6736(21)02724-0
Avdic, E., Cushinotto, L. A., Hughes, A. H., Hansen, A. R., Efird, L. E., Bartlett, J. G., et al. (2012). Impact of an antimicrobial stewardship intervention on shortening the duration of therapy for community-acquired pneumonia. Clin. Infect. Dis. 54 (11), 1581–1587. doi:10.1093/cid/cis242
Benko, R., Matuz, M., Pető, Z., Weist, K., Heuer, O., Vlahović-Palčevski, V., et al. (2022). Trends in the hospital-sector consumption of the WHO AWaRe Reserve group antibiotics in EU/EEA countries and the United Kingdom, 2010 to 2018. Euro Surveill. 27 (41), 2101058. doi:10.2807/1560-7917.ES.2022.27.41.2101058
Blasi, F., Iori, I., Bulfoni, A., Corrao, S., Costantino, S., and Legnani, D. (2008). Can CAP guideline adherence improve patient outcome in internal medicine departments? Eur. Respir. J. 32 (4), 902–910. doi:10.1183/09031936.00092607
Center, U. (2022). Antibiotikum stewardship pilot project MU 069. Available at: https://klinikaikozpont.unideb.hu/munkautasitasok.
Cohen, H. A., Gerstein, M., Loewenberg Weisband, Y., Richenberg, Y., Jacobson, E., Cohen, M., et al. (2022). Pediatric antibiotic stewardship for community-acquired pneumonia: a pre-post intervention study. Clin. Pediatr. (Phila) 61 (11), 795–801. doi:10.1177/00099228221102827
Control, E.-E. C. (2023). Latest surveilance data on antimicrobial consumption-Total care antimicrobial consumption for the year. Available at: https://qap.ecdc.europa.eu/public/extensions/AMC2_Dashboard/AMC2_Dashboard.html#eu-consumption-tab.
Control, E.-E. C. (2024). Survellance report-antimicrobial consumption in the EU/EEA (ESAC-NET). Annual Epidemiological Report. Available at: https://www.ecdc.europa.eu/sites/default/files/documents/AER-antimicrobial-consumption.pdf.
Debrecen, U. (2023). Antibiotic stewardship program, MF 28. Available at: https://klinikaikozpont.unideb.hu/folyamatleirasok.
EC (2024). E.C. EU Guidelines for the prudent use of antimicrobials in human health, C/2017/4326. Commission notice. Brussels: European Commission. Available at: https://eurlex.europa.eu/legal-content/EN/TXT/?uri=CELEX:52017XC0701(01.
ECDC (2024). European Centre for disease Prevention and control- Antimicrobial consumption in the EU/EEA (ESAC-Net) - annual epidemiological Report for 2022. Available at: https://www.ecdc.europa.eu/sites/default/files/documents/AER-antimicrobial-consumption.pdf.
Eurostat (2024). Statistics explained, Respiratory diseases statistics. Available at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Respiratory_diseases_statistics&oldid=541149#Deaths_from_diseases_of_the_respiratory_system.
Fally, M., Diernaes, E., Israelsen, S., Tarp, B., Benfield, T., Kolte, L., et al. (2021). The impact of a stewardship program on antibiotic administration in community-acquired pneumonia: results from an observational before-after study. Int. J. Infect. Dis. 103, 208–213. doi:10.1016/j.ijid.2020.11.172
Fesus, A., Benkő, R., Matuz, M., Engi, Z., Ruzsa, R., Hambalek, H., et al. (2022). Impact of guideline adherence on outcomes in patients hospitalized with community-acquired pneumonia (CAP) in Hungary: a retrospective observational study. Antibiot. (Basel) 11 (4), 468. doi:10.3390/antibiotics11040468
Fine, M. J. (2023). PSI/PORT Score: pneumonia Severity Index for CAP. Estimates mortality for adult patients with community-acquired pneumonia. Available at: https://www.mdcalc.com/calc/33/psi-port-score-pneumonia-severity-index-cap.
Fine, M. J., Pratt, H. M., Obrosky, D. S., Lave, J. R., McIntosh, L. J., Singer, D. E., et al. (2000). Relation between length of hospital stay and costs of care for patients with community-acquired pneumonia. Am. J. Med. 109 (5), 378–385. doi:10.1016/s0002-9343(00)00500-3
Garau, J., Nicolau, D. P., Wullt, B., and Bassetti, M. (2014). Antibiotic stewardship challenges in the management of community-acquired infections for prevention of escalating antibiotic resistance. J. Glob. Antimicrob. Resist 2 (4), 245–253. doi:10.1016/j.jgar.2014.08.002
Ghosh, D., Veeraraghavan, B., Elangovan, R., and Vivekanandan, P. (2020). Antibiotic resistance and epigenetics: more to it than meets the eye. Antimicrob. Agents Chemother. 64 (2), e02225. doi:10.1128/AAC.02225-19
Helen Umpleby, A. D., Catton, T., and Saeed, K. (2022). Antimicrobial stewardship programmes focused on de-escalation: a narrative review of efficacy and risks.
Kosar, F., Alici, D. E., Hacibedel, B., Arpınar Yigitbas, B., Golabi, P., and Cuhadaroglu, C. (2017). Burden of community-acquired pneumonia in adults over 18 y of age. Hum. Vaccin Immunother. 13 (7), 1673–1680. doi:10.1080/21645515.2017.1300730
Lopez-Lozano, J. M., Lawes, T., Nebot, C., Beyaert, A., Bertrand, X., Hocquet, D., et al. (2019). A nonlinear time-series analysis approach to identify thresholds in associations between population antibiotic use and rates of resistance. Nat. Microbiol. 4 (7), 1160–1172. doi:10.1038/s41564-019-0410-0
Luthi-Corridori, G., Boesing, M., Roth, A., Giezendanner, S., Leuppi-Taegtmeyer, A. B., Schuetz, P., et al. (2023). Predictors of length of stay, rehospitalization and mortality in community-acquired pneumonia patients: a retrospective cohort study. J. Clin. Med. 12 (17), 5601. doi:10.3390/jcm12175601
Macfarlane, J. (2023). CURB-65 Score for Pneumonia Severity. Estimates mortality of community-acquired pneumonia to help determine inpatient vs. outpatient treatment. Available at: https://www.mdcalc.com/calc/324/curb-65-score-pneumonia-severity#creator-insights.
Markus Fally, S. I., Tarp, B., Benfield, T., and Ravn, P. (2020). The impact of a stewardship programme on outcomes in patients admitted with community-acquired pneumonia. Eur. Respir. J. 56, 4668. doi:10.1183/13993003.congress-2020.4668
McCabe, C., Kirchner, C., Zhang, H., Daley, J., and Fisman, D. N. (2009). Guideline-concordant therapy and reduced mortality and length of stay in adults with community-acquired pneumonia: playing by the rules. Arch. Intern Med. 169 (16), 1525–1531. doi:10.1001/archinternmed.2009.259
Munther, S., Alnajjar, L. A., Saeed, D., Kurdi, H. B., Bsoul, S., Aburuz, S., et al. (2023). The impact of adherence to community-acquired pneumonia (CAP) management guidelines on improving clinical outcomes in hospitalized patients. Pharm Pract (Granada). Pharm. Pract. (Granada) 21 (3).
Nathwani, D., Varghese, D., Stephens, J., Ansari, W., Martin, S., and Charbonneau, C. (2019). Value of hospital antimicrobial stewardship programs [ASPs]: a systematic review. Antimicrob. Resist Infect. Control 8, 35. doi:10.1186/s13756-019-0471-0
Nussenblatt, V., Avdic, E., and Cosgrove, S. (2013). What is the role of antimicrobial stewardship in improving outcomes of patients with CAP? Infect. Dis. Clin. North Am. 27 (1), 211–228. doi:10.1016/j.idc.2012.11.008
Schweitzer, V. A., van Heijl, I., Boersma, W. G., Rozemeijer, W., Verduin, K., Grootenboers, M. J., et al. (2022). Narrow-spectrum antibiotics for community-acquired pneumonia in Dutch adults (CAP-PACT): a cross-sectional, stepped-wedge, cluster-randomised, non-inferiority, antimicrobial stewardship intervention trial. Lancet Infect. Dis. 22 (2), 274–283. doi:10.1016/S1473-3099(21)00255-3
Szalka, A. (2013). Az antibiotikum stewardship aktuális helyzete és feladatai. J. Hung. Interdiscip. Med. XII (3), 30–34.
Tiri, B., Bruzzone, P., Priante, G., Sensi, E., Costantini, M., Vernelli, C., et al. (2020). Impact of antimicrobial stewardship interventions on appropriateness of surgical antibiotic prophylaxis: how to improve. Antibiot. (Basel) 9 (4), 168. doi:10.3390/antibiotics9040168
Viasus, D., Vecino-Moreno, M., De La Hoz, J. M., and Carratalà, J. (2017). Antibiotic stewardship in community-acquired pneumonia. Expert Rev. Anti Infect. Ther. 15 (4), 351–359. doi:10.1080/14787210.2017.1274232
Waagsbo, B., Tranung, M., Damås, J. K., and Heggelund, L. (2022). Antimicrobial therapy of community-acquired pneumonia during stewardship efforts and a coronavirus pandemic: an observational study. BMC Pulm. Med. 22 (1), 379. doi:10.1186/s12890-022-02178-6
WHO (2021). WHO policy guidance on integrated antimicrobial stewardship activities. Available at: https://www.who.int/publications/i/item/9789240025530.
Keywords: community-acquired pneumonia, hospitalized patients, empirical antibiotic therapy, antibiotic stewardship, clinical outcomes, intervention
Citation: Fésüs A, Baluku P, Sipos É, Somodi S, Berczi-Kun E, Lekli I, Bácskay I, Benkő R and Vaskó A (2024) The effect of the antibiotic stewardship program (ASP) on community-acquired pneumonia (CAP): a before–after study. Front. Pharmacol. 15:1406960. doi: 10.3389/fphar.2024.1406960
Received: 25 March 2024; Accepted: 23 July 2024;
Published: 06 August 2024.
Edited by:
Muhammad Ayaz, University of Malakand, PakistanReviewed by:
Gabriela Cristina Fernandez, National Scientific and Technical Research Council (CONICET), ArgentinaCopyright © 2024 Fésüs, Baluku, Sipos, Somodi, Berczi-Kun, Lekli, Bácskay, Benkő and Vaskó. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adina Fésüs, ZmVzdXMuYWRpbmFAcGhhcm0udW5pZGViLmh1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.