
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 15 July 2024
Sec. Drugs Outcomes Research and Policies
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1385401
 Lívio Portela de Deus Lages1
Lívio Portela de Deus Lages1 Cristiane de Cássia Bergamaschi2
Cristiane de Cássia Bergamaschi2 Luciane Cruz Lopes2
Luciane Cruz Lopes2 Eduardo Gomes da Frota1
Eduardo Gomes da Frota1 Marcus Tolentino Silva3
Marcus Tolentino Silva3 Thiago Lima Monte4
Thiago Lima Monte4 Rogério Heládio Lopes Motta5*
Rogério Heládio Lopes Motta5*Introduction: Periodontal procedures can promote prolonged intense pain, particularly in clinical situations requiring surgical procedures. In this context, preemptive analgesia has also been assessed for its utility in controlling post-operative pain and discomfort in patients undergoing periodontal invasive procedures. This study assessed the efficacy and safety of preemptive oral analgesia with steroidal and non-steroidal anti-inflammatory drugs in periodontal surgeries.
Methods: This systematic review performed a search in the following electronic sources: the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (via PubMed), EMBASE (via Ovid), Web of Science, Virtual Health Library and in clinical trials electronic databases for relevant randomized clinical trials (RCTs); published up to July 2023. Primary outcomes assessed were post-operative pain, edema and trismus. A narrative synthesis of the findings was carried out.
Results: Six RCTs, involving a total of 250 participants, were included. The studies reviewed had a high risk of bias, particularly due to allocation concealment and blinding of participants and personnel. The RCTs reported only the outcome pain. The preemptive use of dexamethasone 8 mg, etoricoxib 90 mg or 120 mg and ketorolac 20 mg seems to be more effective for controlling post-operative pain than placebo.
Discussion: The anti-inflammatory drugs evaluated proved to be effective for controlling post-operative pain. However, given the limitations regarding lack of studies, methodological biases, disparities in drugs and doses, report restricted the pain outcome; further RCTs confirming the effectiveness and safety of these drugs in periodontal surgical procedures are warranted.
Periodontal surgical procedures, including scaling and root planning, can cause prolonged intense pain (Pihlstrom et al., 1999; Rathore et al., 2024). Thus, patients undergoing periodontal surgeries can be managed using pharmacological strategies which promote greater comfort (Steffens et al., 2010; Giorgetti et al., 2018).
Preemptive analgesia has been employed for reducing and controlling pain and discomfort in patients postoperatively after periodontal invasive surgical procedures (Konuganti et al., 2015; Malamed, 2023). The term “preemptive” refers to a form of analgesia administered before the onset of pain stimuli to prevent or reduce subsequent pain (Garcia et al., 2021; Myers and Jeske, 2023).
Some studies suggest that pre-operative administration of different anti-inflammatory agents, such as steroidal or non-steroidal anti-inflammatory drugs (NSAIDs), can reduce the intensity of post-operative pain and the need for supplementary analgesics in more invasive oral procedures (Vicentini et al., 2018; Bhutani et al., 2019).
There are concerns over the use of NSAIDs which, while inhibiting cyclooxygenases (COX-1 and COX-2) may cause adverse reactions such as gastric irritation, renal and cardiovascular adverse effects (Harirforoosh et al., 2013). Moreover, NSAIDs are also one of the main drugs that can cause hypersensitivity reactions (Blanca-Lopez et al., 2019). Considering these possible implications, a systematic review was conducted to examine the available scientific evidence regarding the possible adverse effects and safety of NSAIDs in patients who take NSAIDs for 10 days or less to relieve pain (as usually occurs in more invasive dental procedures). It was observed that most patients who take NSAIDs for a short period are not at increased risk of developing cardiovascular, gastric, renal or respiratory adverse effects when compared to patients who have not been exposed to these drugs (Aminoshariae et al., 2016).
Therefore, some investigations have explored the preemptive use of more specific NSAIDs for COX-2 inhibition in dental surgical procedures (Peres et al., 2012; Piecuch, 2012; Xie et al., 2020). Additionally, systematic reviews have assessed the effectiveness of the use of steroidal anti-inflammatory drugs for preemptive analgesia in procedures such as third molar removal (Herrera-Briones et al., 2013; Cetira Filho et al., 2020).
In this context, doubts remain regarding the optimal choice of anti-inflammatory agent, dose and interval for preemptive use of the medication in periodontal surgical procedures to ensure treatment which improves post-operative pain control and prevents patient discomfort, while not exposing them to increased risk of complications (Choi et al., 2021).
A previous systematic review assessed the effectiveness of oral use of corticosteroids to control pain and swelling of patients undergoing third molar extraction, periodontal procedures or implant surgeries (Wagner et al., 2022). Recently, a clinical practice guideline for management of acute dental pain was published (Carrasco-Labra, et al., 2024). However, these guidelines were largely based on studies in patients after third molar extraction. Another recent publication evaluated systematic reviews regarding the effectiveness and safety of the preemptive use of anti-inflammatory and analgesic drugs in the management of postoperative pain, edema, and trismus in oral surgery. It was also noted that third molar surgery was the most studied procedure and that more randomized clinical trials are still needed (Pimenta et al., 2024). Moreover, systematic reviews assessing the effectiveness of preemptive use of oral steroidal and non-steroidal anti-inflammatory drugs in patients undergoing periodontal surgical procedures are still scarce.
Therefore, the present study assessed the preemptive use of oral steroidal and non-steroidal anti-inflammatory drugs in controlling patient post-operative pain and discomfort after periodontal surgical procedures with the aim of aiding professionals in decision-making for optimal management in effective and safe use of this medication.
This systematic review was reported according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green, 2020) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021). The study protocol was registered (CRD42022324766) on the PROSPERO platform (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=324766).
These criteria were described using the Population, Intervention, Comparison, Outcome and Study type (PICOS) framework.
Participants: adults aged ≥18 years who required periodontal surgical interventions, such as subgingival scaling, clinical crown augmentation, and grafts;
Intervention: preemptive analgesia using oral corticosteroids or NSAIDS;
Control: placebo or active control (other steroidal or nonsteroidal anti-inflammatory drug);
Outcomes: effectiveness and safety outcomes;
Study type: randomized controlled trials (RCT).
Participants: pregnant or nursing women; patients in continuous use of anti-inflammatories or analgesics for at least 14 days prior to the study, or with a history of allergy or intolerance to these drugs, or in use of drugs that may affect the perception of pain. Individuals with a history of alcoholism or substance abuse.
Clinical trials must report at least one of the following primary outcomes: pain reduction or control and patient discomfort (for at least 8 h after the surgical procedures), swelling/edema, and trismus. Pain must be assessed using a visual analogue scale or other scale; and edema should be assessed by angles or distances between different facial landmarks; and trismus by interincisal distance.
Secondary outcomes evaluated were the occurrence of adverse drug reactions, need for clinical reintervention, and satisfaction with the treatment.
The following databases were searched: Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (via PubMed), Web of Science, Excerpta Medica dataBASE (EMBASE), Biblioteca Virtual em Saúde (BVS) and the thesis database of the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - CAPES (Brazilian Catalogue of Theses and Dissertations – https://catalogodeteses.capes.gov.br/catalogo-teses/#!/).
The search by RCT registry was performed on ClinicalTrials.gov (www.clinicaltrials.gov) and ISRCTN Register (www.isrctn.com). There were no restrictions for language or publication date and a search of all studies published up until July 2023 was carried out.
Grey Literature Report (https://www.greylit.org/library/search) and OpenGrey (http://www.opengrey.eu/) were the grey literature sources searched.
A manual search was performed by searching the list of eligible studies, literature review studies and systematic review studies. No lead authors of the studies needed to be contacted to obtain the full text or the necessary information for the data extraction.
The search was conducted using Medical Subject Headings (MeSH) terms, with the strategy adapted for each database (see Supplementary Material SA).
After executing the search strategies on each database, the researchers imported the results of each search into an EndNote® library for removal of duplicates and selection of the studies for review.
Four reviewers (LPL, CBM, EGF, and TLM), working in pairs and independently, screened potentially relevant citations and abstracts and applied the selection criteria. Full texts of all potentially eligible articles were obtained. The same reviewers confirmed the eligibility of each article by reading the full text. Disagreements were resolved by consensus and, when necessary, a third reviewer was consulted for a final decision (RHLM).
Pairs of reviewers (LPL, CBM, EGF and TLM), independently, performed the data extraction, using a Microsoft Excel form, standardized and pretexted for this step. Reviewers extracted patient data, methods, interventions and outcomes evaluated. Disagreements were resolved by consensus and, when necessary, arbitrated by a third reviewer (RHLM or LCL).
The version of the Cochrane Collaboration was used to assess risk of bias. The reviewers, in pairs and independently (LPL,CBM, EGF and TLM), assigned the risk of bias for each clinical trial according to the following criteria: sequence generation: was the allocation sequence adequately generated?; Allocation concealment: was allocation adequately concealed?; Blinding of participants and care providers for each main outcome: was the knowledge of the allocated treatment adequately prevented during the trial?; Blinding of outcome assessors for each main outcome: was the knowledge of the allocated treatment adequately prevented during the trial?; Incomplete outcome data for each main outcome: did more than 10% of participants withdraw, and were incomplete outcome data adequately addressed?; Selective outcome reporting: was there any suggestion of selective outcome reporting?; Other sources of bias: was the trial apparently free of other problems that could put it at high risk of bias?
The reviewers assigned response options of “definitely yes,” “probably yes,” “probably no,” and “definitely no” for each of the domains, with “definitely yes” and “probably yes” ultimately being assigned a low risk of bias, and “definitely no” and “probably no,” a high risk of bias (Akl et al., 2013). The reviewers settled disagreements by consensus and a third reviewer (RHLM or LCL) was consulted when necessary.
The results were summarized through narrative synthesis, since it was not possible to perform meta-analyses due to disparities among the clinical procedures, drugs and doses used. Further information regarding the methods adopted is described in the protocol registered as already mentioned.
The search strategy led to the identification of 1,866 publications. After removal of duplicates and reading of titles and abstracts, 20 studies remained for full-text screening. Based on the eligibility criteria, a total of 6 RCTs were included in the review (Figure 1). The excluded studies are listed in Supplementary Material SB.
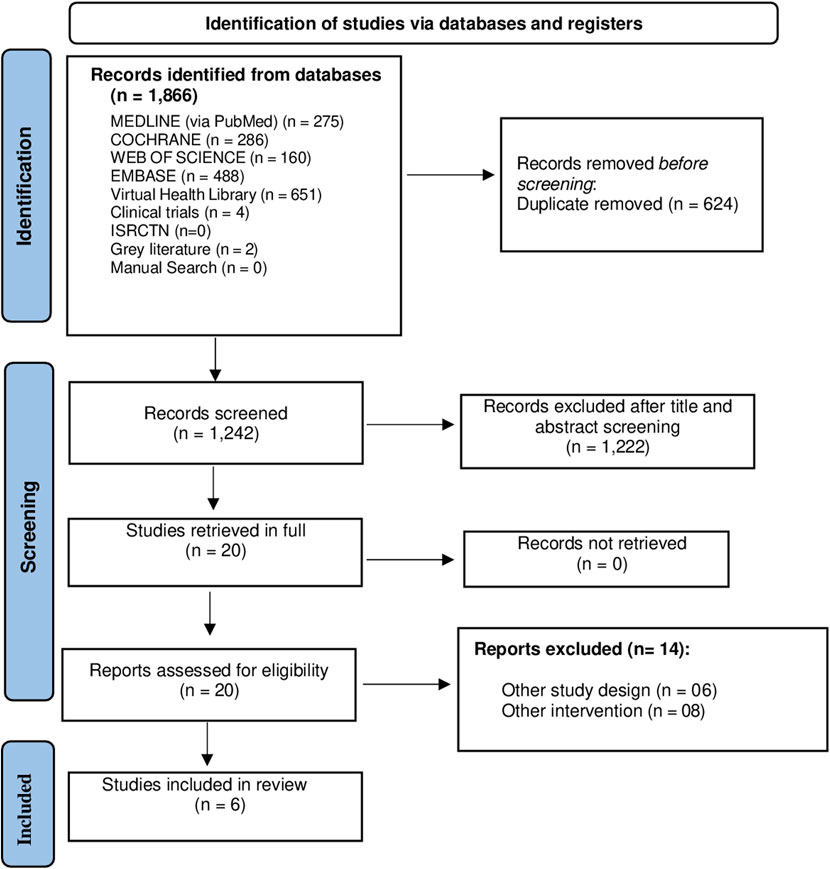
Figure 1. Flow diagram of study search process.
Six RCTs included involved 250 participants undergoing periodontal surgeries. Of the individuals for whom gender was reported, 75 were women and 57 men. Gender was not reported for the remaining 118 participants. The anti-inflammatory agents assessed in the clinical trials included dexamethasone 8 mg, celecoxib 200 mg, etoricoxib 90 mg and 120 mg, and ketorolac 20 mg. Patient follow-up ranged from the first 8 h to 4 days.
Of the 250 participants, 134 underwent flap debridement, 43 mucoperiosteal flap surgery, 15 root debridement and osseous recontouring, and 58 mucogingival grafts.
The studies included were published between 2010 and 2015. Four of the RCTs were conducted in Brazil, and the other 2 in India and Italy, respectively. The studies reported no information on research funding and did not register their protocols (Table 1).
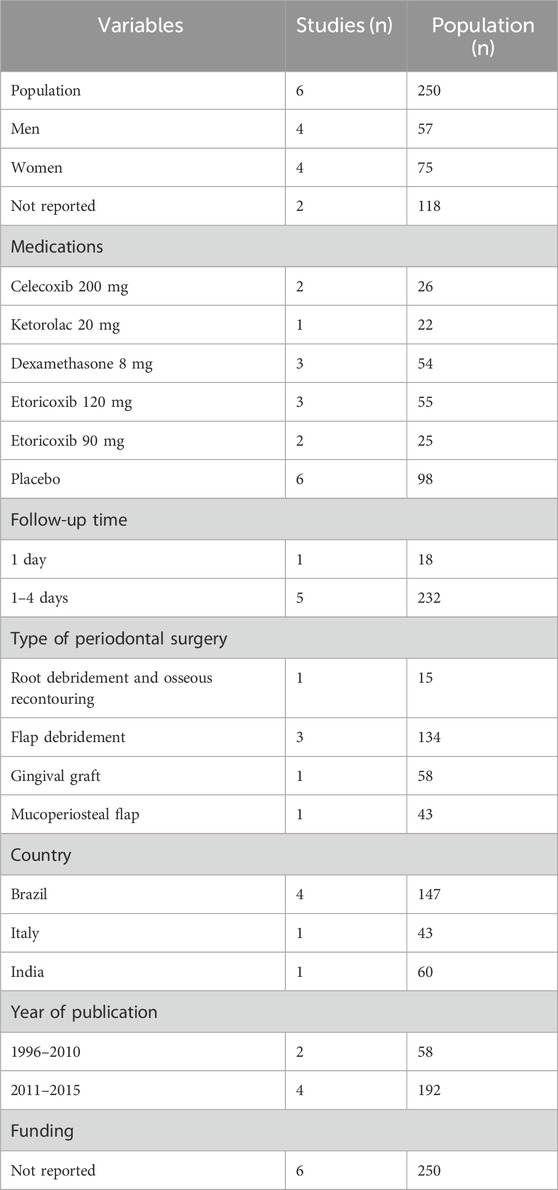
Table 1. Characteristics of studies included (n = 6 studies).
Information about the risk of bias is described in Figure 2.

Figure 2. Risk of bias due to randomized clinical trial included.
Two studies reported the methods used as random assigning by draw (Steffens et al., 2012) and randomization list (Trombelli et al., 1996). The other four studies stated that patients were randomized into groups but failed to describe the method used (Steffens et al., 2010; Steffens et al., 2011; Zardo et al., 2013; Konuganti et al., 2015).
None of the studies reported the approach used for concealment of allocation of participants and were therefore rated as high risk of bias.
One study described that designated a researcher solely to administer the drugs, thereby ensuring blinding of both patients and researchers (Steffens et al., 2012). The other studies claimed to be double-blind but provided no details on blinding procedures (Trombelli et al., 1996; Steffens et al., 2010; Steffens et al., 2011; Zardo et al., 2013; Konuganti et al., 2015).
One study reported details on blinding of outcome assessors (Steffens et al., 2012). The remaining studies reported no further information, indicating detection bias. (Trombelli et al., 1996; Steffens et al., 2010; Steffens et al., 2011; Zardo et al., 2013; Konuganti et al., 2015).
One of the studies reported loss of 5 (25%) of its total of 20 participants due to reasons including dentin hypersensitivity (n = 1) and moving to a new city (n = 4) (Steffens et al., 2010). In another RCT, 4 (6.6%) out of the total sample of 60 patients were lost for failing to attend post-operative return visits or not filling out the pain report form properly (Steffens et al., 2011). Another study reported loss of 5 (12%) out of the 43 participants because the pain questionnaire was not completed properly (Trombelli et al., 1996). Two individuals (3.3%) failed to return the pain score form in another study (Zardo et al., 2013).The remaining studies had no losses to follow-up (Steffens et al., 2012; Konuganti et al., 2015).
None of the studies registered the protocol, precluding any check on whether all the proposed outcomes were measured.
All studies carried declarations stating there were no external sources of funding and, thus, were considered low risk of bias given the absence of potential conflict of interest regarding results.
The studies reported the outcomes pain (n = 6) and anxiety (n = 2). The effectiveness of ketorolac 20 mg for reducing post-operative pain was compared to placebo (Trombelli et al., 1996) (Table 2). Three clinical trials assessed the use of dexamethasone 8 mg compared to etoricoxib (90 and 120 mg) and placebo for controlling post-operative pain (Steffens et al., 2010; Zardo et al., 2013; Konuganti et al., 2015). The use of celecoxib 200 mg was compared to etoricoxib (90 and 120 mg) and placebo for post-operative pain control (Steffens et al., 2011; Steffens et al., 2012). The effectiveness of ketorolac 20 mg for reducing post-operative pain was compared to placebo (Trombelli et al., 1996).
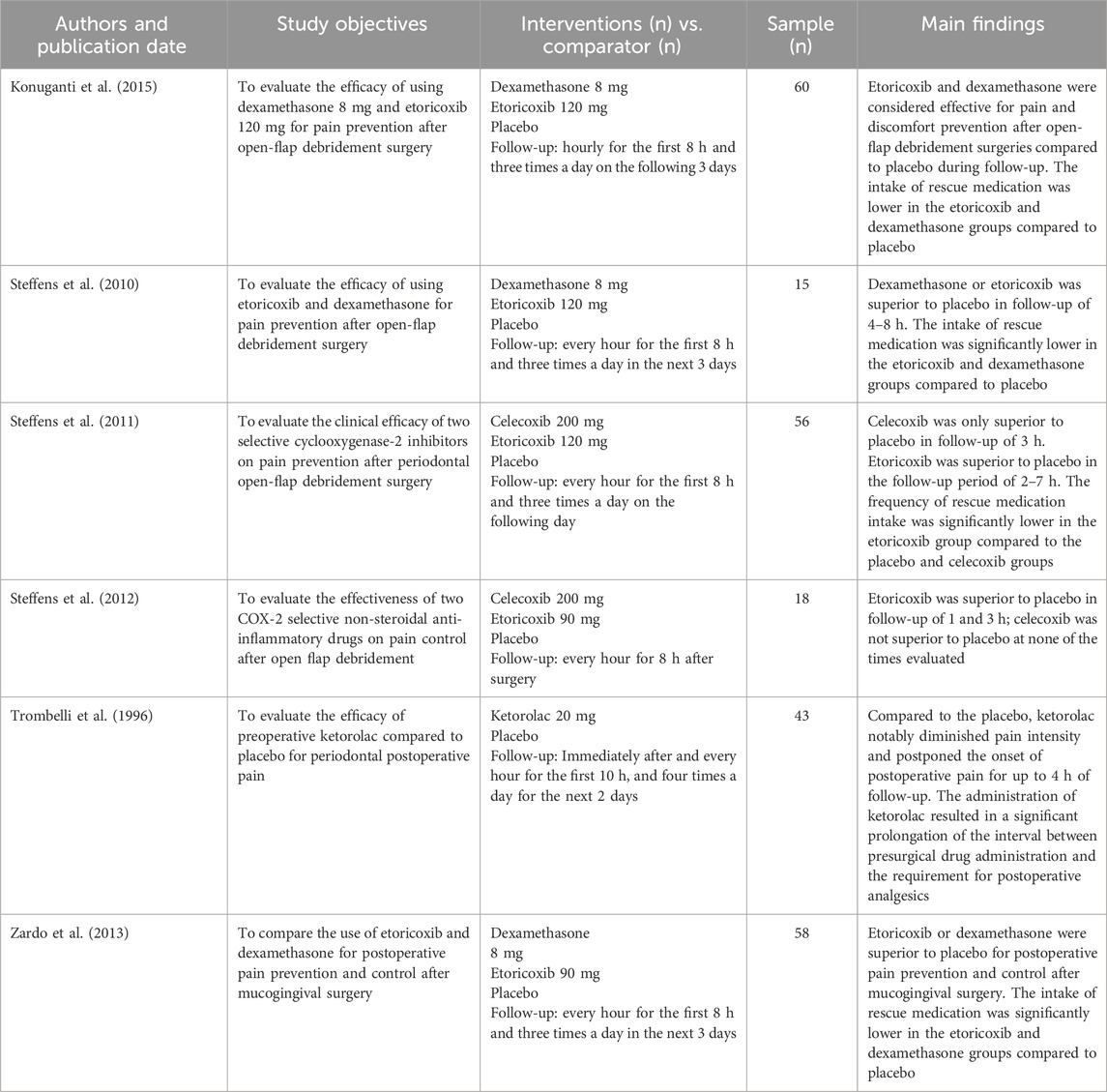
Table 2. Description of information from studies included and outcomes assessed (n = 6 studies, n = 250 participants).
The main findings for effectiveness reported by the clinical trials are outlined below:
Two clinical trials compared the effectiveness of the preemptive use of dexamethasone 8 mg or etoricoxib 120 mg to placebo in patients undergoing periodontal flap debridement surgery. The 101-point numeric rate scale and the four point verbal rating scale were used to rate post-operative pain and discomfort. In both trials, dexamethasone 8 mg and etoricoxib 120 mg proved to be more effective than placebo for controlling pain (Steffens et al., 2010; Konuganti et al., 2015). In one study, each patient underwent three surgical procedures at intervals of 30 days with different formulations (Steffens et al., 2010).
Another clinical trial compared the use of dexamethasone 8 mg or etoricoxib 90 mg to placebo for controlling post-operative pain in patients undergoing mucogingival surgery. The NRS-101 scale was used to rate post-operative pain. Dexamethasone 8 mg and etoricoxib 90 mg proved to be superior to placebo for reducing post-operative pain, and both drugs administered preoperatively resulted in a lower intake of rescue medication (Zardo et al., 2013).
Two clinical trials compared the use of celecoxib 200 mg, and etoricoxib 90 mg and 120 mg to placebo for controlling post-operative pain in patients undergoing open-flap debridement procedures.
Celecoxib 200 mg and etoricoxib 120 mg were superior to placebo for controlling post-operative pain, and rescue medication intake was significantly less frequent in the etoricoxib group. In another study, etoricoxib 90 mg were superior to placebo and celecoxib for this outcome. The VAS was used to measure pain outcome in both studies (Steffens et al., 2011; Steffens et al., 2012).
Ketorolac 20 mg was compared to placebo for controlling post-operative pain in patients undergoing periodontal flap debridement surgeries. The preoperative ketorolac administration was more effective than placebo for reducing initial pain intensity and delayed the onset of postoperative pain (Trombelli et al., 1996).
The present study reviewed the available evidence on the effectiveness and safety of the use of preemptive analgesia in patients undergoing periodontal surgical procedures: open-flap debridement (Steffens et al., 2011; Steffens et al., 2012; Konuganti et al., 2015), mucoperiosteal flap (Trombelli et al., 1996), root debridement with osseous recontouring (Steffens et al., 2010) and gingival graft (Zardo et al., 2013). None of the studies reviewed met all the assessment criteria for risk of bias, where the main issues found pertained to allocation concealment and blinding of individuals involved. The most investigated drugs were dexamethasone 8 mg and etoricoxib 90 mg and 120 mg. Meta-analyses were not performed owing to the disparities in clinical procedures, drugs and doses studied.
Preemptive analgesia with dexamethasone 8 mg were more effective than placebo for controlling post-operative pain (Steffens et al., 2010; Zardo et al., 2013; Konuganti et al., 2015). Likewise, etoricoxib 90 mg or 120 mg were also superior to placebo for controlling post-operative pain (Steffens et al., 2010; Steffens et al., 2011; Steffens et al., 2012; Zardo et al., 2013; Konuganti et al., 2015). Ketorolac 20 mg was more effective than placebo for pain control (Trombelli et al., 1996).
None of the studies assessed adverse effects, precluding any conclusion on the safety of the interventions studied. Furthermore, the outcomes swelling, trismus, need for clinical reintervention and treatment satisfaction were not addressed in the clinical trials, limiting out findings about this topic on the preemptive use of analgesia in periodontal surgeries. Since stress and dental anxiety can vary among patients and potentially impact pain perception, the State-Trait Anxiety Inventory and Corah’s Dental Anxiety Scale were applied in two studies (Steffens et al., 2010; Steffens et al., 2011). However, there was no statistical difference between the patients in different groups of both studies.
Although no information was collected on the safety of using the drugs investigated by the studies, when administered as a single oral dose, these medications are likely to be safe for use. In addition, lost follow-up reported by some of the studies reviewed were for reasons unrelated to safety of the medications.
Notably, a previous systematic review assessed the effectiveness of the use of oral anti-inflammatory corticosteroids in patients undergoing third molar extraction, periodontal or implant surgeries. This review included three of the clinical trials included in our study (Wagner et al., 2022).
This review was methodologically robust, employing explicit eligibility criteria, risk of bias rating, a broad comprehensive search of databases, and independent dual review of each study included.
The primary studies included were a factor limiting the review findings, given the methodological quality of the clinical trials, different comparators and doses and failure to address relevant clinical outcomes, ultimately preventing meta-analyses.
This review provided a synthesis of the available evidence in the literature on the effectiveness of preemptive analgesia with oral use of dexamethasone 8 mg, etoricoxib (90 mg and 120 mg) and ketorolac 20 mg in periodontal surgical procedures. The findings suggest that preemptive oral use of these anti-inflammatory drugs appears to control post-operative pain and discomfort after periodontal surgical procedures. The study findings can help inform decision-making in dental practice regarding the control of post-operative pain induced by periodontal surgeries.
Considering the various limitations, further clinical trials involving more rigorous methodology and standardized methods of gathering outcome data should by conducted. These investigations could increase the reliability of findings, indicating which medications are deemed effective and safe for preemptive analgesia in periodontal surgical procedures.
Preemptive analgesia with a single oral dose of dexamethasone 8 mg, etoricoxib (90 mg and 120) mg and ketorolac 20 mg appear to control post-operative pain in periodontal surgeries compared to the use of placebo. However, the evidence is insufficient to support the effectiveness and safety of these anti-inflammatory drugs for use in patients undergoing periodontal surgeries. In view of the limitations of this review such as small number of studies and participants, high risk of bias, different comparators across studies, lack of findings on the safety outcomes; further clinical trials should be carried out to confirm the effectiveness and safety of the use of anti-inflammatory medications in periodontal surgeries.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
LPDL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing–original draft, Writing–review and editing. CB: Conceptualization, Data curation, Formal Analysis, Investigation, Writing–review and editing. LCL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing–review and editing. EF: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing–review and editing. MS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing–review and editing. TM: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing–review and editing. RM: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing–original draft, Writing–review and editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1385401/full#supplementary-material
Akl, E. A., Johnston, B. C., Alonso-Coello, P., Neumann, I., Ebrahim, S., Briel, M., et al. (2013). Addressing dichotomous data for participants excluded from trial analysis: a guide for systematic reviewers. PLoS ONE 8, e57132. doi:10.1371/journal.pone.0057132
Aminoshariae, A., Kulild, J. C., and Donaldson, M. (2016). Short-term use of nonsteroidal anti-inflammatory drugs and adverse effects: an updated systematic review. J. Am. Dent. Assoc. 147 (2), 98–110. doi:10.1016/j.adaj.2015.07.020
Bhutani, N., Sangolikar, D., Bhutani, S., Tapashetti, R., and Pushpalatha, H. (2019). Sublingual piroxicam as preemptive analgesia in single implant surgery. J. Contemp. Dent. Pract. 20 (6), 750–753. doi:10.5005/jp-journals-10024-2591
Blanca-Lopez, N., Soriano, V., Garcia-Martin, E., Canto, G., and Blanca, M. (2019). NSAID-induced reactions: classification, prevalence, impact, and management strategies. J. Asthma Allergy 12, 217–233. doi:10.2147/JAA.S164806
Carrasco-Labra, A., Polk, D. E., Urquhart, O., Aghaloo, T., Claytor, J. W. Jr., Dhar, V., et al. (2024). Evidence-based clinical practice guideline for the pharmacologic management of acute dental pain in adolescents, adults, and older adults: a report from the American Dental Association Science and Research Institute, the University of Pittsburgh, and the University of Pennsylvania. J. Am. Dent. Assoc. 155 (2), 102–117.e9. doi:10.1016/j.adaj.2023.10.009
Cetira Filho, E. L., Carvalho, F. S. R., de Barros Silva, P. G., et al., , Alves Pereira, K. M., Ribeiro, T. R., et al. (2020). Preemptive use of oral nonsteroidal anti-inflammatory drugs for the relief of inflammatory events after surgical removal of lower third molars: a systematic review with meta-analysis of placebo-controlled randomized clinical trials. J. Craniomaxillofac Surg. 48 (3), 293–307. doi:10.1016/j.jcms.2020.01.016
Choi, M., Wang, L., Coroneos, C. J., Voineskos, S. H., and Paul, J. (2021). Managing postoperative pain in adult outpatients: a systematic review and meta-analysis comparing codeine with NSAIDs. CMAJ 193 (24), E895–E905. doi:10.1503/cmaj.201915
Garcia, J. B. S., Issy, A. M., and Sakata, R. K. (2021). Analgesia preemptiva. Rev. Bras. Anestesiol. 51 (5), 448–463. doi:10.1590/s0034-70942001000500011
Giorgetti, A. P. O., Matos, R., Casarin, R. C. V., Pimentel, S. P., Cirano, F. R., and Ribeiro, F. V. (2018). Preemptive and postoperative medication protocols for root coverage combined with connective tissue graft. Braz Dent. J. 29 (1), 23–29. doi:10.1590/0103-6440201801452
Harirforoosh, S., Asghar, W., and Jamali, F. (2013). Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. J. Pharm. Pharm. Sci. 16 (5), 821–847. doi:10.18433/j3vw2f
Herrera-Briones, F. J., Prados Sánchez, E., Reyes Botella, C., and Vallecillo, C. M. (2013). Update on the use of corticosteroids in third molar surgery: systematic review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 116 (5), e342–e351. doi:10.1016/j.oooo.2012.02.027
Higgins J. P. T., and Green S. (Editors) (2020). Cochrane Handbook for systematic reviews of interventions. London, England: The Cochrane Collaboration.
Konuganti, K., Rangaraj, M., and Elizabeth, A. (2015). Pre-emptive 8 mg dexamethasone and 120 mg etoricoxib for pain prevention after periodontal surgery: a randomised controlled clinical trial. J. Indian Soc. Periodontol. 19 (4), 474–476. doi:10.4103/0972-124X.153475
Malamed, S. F. (2023). Pain management following dental trauma and surgical procedures. Dent. Traumatol. 39 (4), 295–303. doi:10.1111/edt.12840
Myers, A. L., and Jeske, A. H. (2023). Provider-directed analgesia for dental pain. Expert Rev. Clin. Pharmacol. 16 (5), 435–451. doi:10.1080/17512433.2023.2206118
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Peres, M. F., Ribeiro, F. V., Ruiz, K. G., Nociti, F. H., Sallum, E. A., and Casati, M. Z. (2012). Steroidal and non-steroidal cyclooxygenase-2 inhibitor anti-inflammatory drugs as pre-emptive medication in patients undergoing periodontal surgery. Braz Dent. J. 23 (6), 621–628. doi:10.1590/s0103-64402012000600001
Piecuch, J. F. (2012). What strategies are helpful in the operative management of third molars? J. Oral Maxillofac. Surg. 70 (9 Suppl. 1), S25–S32. doi:10.1016/j.joms.2012.04.027
Pihlstrom, B. L., Hargreaves, K. M., Bouwsma, O. J., Myers, W. R., Goodale, M. B., and Doyle, M. J. (1999). Pain after periodontal scaling and root planing. J. Am. Dent. Assoc. 130 (6), 801–807. doi:10.14219/jada.archive.1999.0303
Pimenta, R. P., Takahashi, C. M., Barberato-Filho, S., McClung, D. C. F., Moraes, F. D. S., de Souza, I. M., et al. (2024). Preemptive use of anti-inflammatories and analgesics in oral surgery: a review of systematic reviews. Front. Pharmacol. 14, 1303382. doi:10.3389/fphar.2023.1303382
Rathore, P., Manjunath, S., and Singh, R. (2024). Evaluating and comparing the efficacy of the microsurgical approach and the conventional approach for the periodontal flap surgical procedure: a randomized controlled trial. Dent. Med. Probl. 61 (1), 23–28. doi:10.17219/dmp/147183
Steffens, J. P., Santos, F. A., and Pilatti, G. L. (2011). The use of etoricoxib and celecoxib for pain prevention after periodontal surgery: a double-masked, parallel-group, placebo-controlled, randomized clinical trial. J. Periodontol. 82 (9), 1238–1244. doi:10.1902/jop.2011.100682
Steffens, J. P., Santos, F. A., and Pilatti, G. L. (2012). COX-2 selective nonsteroidal anti-inflammatory drugs and pain control after periodontal surgeries: a pilot study. Rev. Gaucha Odontol. 60 (1), 85–89.
Steffens, J. P., Santos, F. A., Sartori, R., and Pilatti, G. L. (2010). Preemptive dexamethasone and etoricoxib for pain and discomfort prevention after periodontal surgery: a double-masked, crossover, controlled clinical trial. J. Periodontol. 81 (8), 1153–1160. doi:10.1902/jop.2010.100059
Trombelli, L., Schincaglia, G. P., Zangari, F., Scapoli, C., and Calura, G. (1996). Effect of pretreatment with ketorolac tromethamine on post-operative pain following periodontal surgery. J. Clin. Periodontol. 23 (2), 128–132. doi:10.1111/j.1600-051x.1996.tb00545.x
Vicentini, C. B., Ramacciato, J. C., Groppo, F. C., Teixeira, R. G., and Motta, R. H. L. (2018). Clinical evaluation of two dexamethasone regimens in the extractions of impacted third molars-a randomized clinical trial. Oral Maxillofac. Surg. 22 (2), 177–183. doi:10.1007/s10006-018-0687-9
Wagner, J. C., Johnson, T. M., and Gilbert, W. A. (2022). Should periodontists prescribe postoperative oral corticosteroids to control pain and swelling? A systematic review. Clin. Adv. Periodontics. 12 (2), 134–142. doi:10.1002/cap.10169
Xie, L., Yang, R. T., Lv, K., Zhou, H. H., and Li, Z. (2020). Comparison of low pre-emptive oral doses of celecoxib versus acetaminophen for postoperative pain management after third molar surgery: a randomized controlled study. J. Oral Maxillofac. Surg. 78 (1), 75.e1–75.e6. doi:10.1016/j.joms.2019.09.022
Keywords: periodontal surgery, preemptive analgesia, systematic review, anti-inflammatory drugs, dentistry
Citation: Lages LPdD, Bergamaschi CdC, Lopes LC, da Frota EG, Silva MT, Monte TL and Motta RHL (2024) Preemptive oral analgesia with steroidal and nonsteroidal anti-inflammatory drugs in periodontal surgery: a systematic review. Front. Pharmacol. 15:1385401. doi: 10.3389/fphar.2024.1385401
Received: 12 February 2024; Accepted: 21 June 2024;
Published: 15 July 2024.
Edited by:
Heike Wulff, University of California, Davis, United StatesReviewed by:
Katherine N. Theken, University of Pennsylvania, United StatesCopyright © 2024 Lages, Bergamaschi, Lopes, da Frota, Silva, Monte and Motta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rogério Heládio Lopes Motta, cm9nZXJpby5tb3R0YUBzbG1hbmRpYy5lZHUuYnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.