 Hao Fan
Hao Fan I-Chun Liu2
I-Chun Liu2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol., 18 April 2024
Sec. Gastrointestinal and Hepatic Pharmacology
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1361501
Background: Bismuth subsalicylate (BSS), probiotics, rifaximin, and vaccines have been proposed as preventive modalities for patients with travelers’ diarrhea (TD), but their comparative effectiveness for prevention has rarely been studied. We aimed to perform a systematic review and network meta-analysis to test whether one of these modalities is more effective than the others in reducing the incidence of TD.
Methods: We searched Pubmed, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, and clinical registries from inception of the databases through 18 November 2023, without language restriction, for randomized controlled trials (RCTs) evaluating the efficacy of BSS, probiotics, rifaximin, and vaccines in preventing TD. The primary outcome was the incidence of TD and the safety outcome was the incidence of adverse events. The relative ratio (RR) was used to assess the effect of the modalities, and RR estimates between any two of the modalities were calculated and pooled using a frequentist network meta-analysis model.
Results: Thirty-one studies (recruiting 10,879 participants) were included in the analysis. Sixteen were judged to have a low risk of bias. In the aggregate analysis, BSS and rifaximin were more effective than placebo and other treatment modalities, which was further confirmed in the individual analysis. The comparison between rifaximin and placebo achieved high confidence, while the comparisons between BSS and placebo, ETEC and probiotics, and rifaximin and vaccines achieved moderate confidence. BSS had a higher rate of adverse events compared with other treatments.
Conclusion: Rifaximin had a relative lower TD incidence and lower adverse event rate, and the evidence was with moderate confidence.
Systematic Review Registration: https://osf.io/dxab6, identifier.
Traveler’s diarrhea is a common medical condition that affects at least 60% of people who travel (Ng et al., 2017; Riddle et al., 2017). While it is usually non-fatal and self-healing, it can cause severe symptoms such as fever, vomiting, abdominal pain or cramps, and dehydration, which can disrupt travel plans or require hospitalization (Steffen et al., 2015; Giddings et al., 2016).
Antibiotics and adequate hydration are recommended for treating TD due to strong evidence. However, evidence for the effectiveness of prevention methods is not convincing, and the comparative effectiveness between treatment modalities is unknown. This causes confusion for clinicians and individuals planning trips to high TD risk destinations.
Bismuth subsalicylate (BSS), the active ingredient in adult formulations of Pepto-Bismol, is the primary agent studied for the prevention of TD. According to reports, taking 2 chewable tablets of BSS 4 times per day reduces the incidence of TD by approximately 50% (Budisak and Abbas, 2023).
TD is caused by bacterial infection, with the most commonly reported pathogens being Escherichia coli (ETEC), Campylobacter jejuni, Salmonella species, and Shigella species (Riddle et al., 2016, 2017; Ng et al., 2017). Therefore, antibiotics and antimicrobials (probiotics and prebiotics) are proposed for the treatment of TD (Riddle et al., 2017). Two meta-analyses have confirmed the efficacy of rifaximin in preventing TD (Traveler’s Diarrhea) (Hu et al., 2012; Ng et al., 2017). Additionally, a recent meta-analysis published in 2018 concluded that probiotics are statistically significant in TD prophylaxis (Bae, 2018). Vaccines against the common pathogen ETEC are also proposed for the preventive treatment of TD. ETEC bacteria adhere to the lining of the gut and secrete either one or both types of enterotoxins: the heat-labile toxin (LT) and the heat-stable toxin. Different strains of ETEC can be further characterized based on the antigens expressed on the cell surface, such as the colonization factor (CF) (Ahmed et al., 2013). The LT and CFs are important antigens for ETEC vaccine development. The cholera vaccine contains a recombinant B subunit of the cholera toxin that is antigenically similar to the LT of ETEC. Therefore, it is also used for the prevention of TD (Walker et al., 2007).
There was limited evidence on the comparative effectiveness of these agents, particularly vaccines, probiotics, and rifaximin, in preventing TD. To address this gap, we conducted a systematic review and network meta-analysis to evaluate the efficacy of Bismuth Subsalicylate, probiotics, rifaximin, and vaccines in relation to each other for TD prevention.
A systematic review and network meta-analysis were conducted to test the relative effectiveness of Bismuth Subsalicylate, probiotics, rifaximin, and vaccines in reducing the incidence of TD. The review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) extension statement for reporting systematic reviews incorporating network meta-analyses of healthcare interventions (Hutton et al., 2015). The study used publicly available data, so no additional ethical approval is required. The systematic review was registered with the Open Science Framework (https://osf.io/dxab6).
Potentially eligible articles were identified from Medline, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, and clinical registries from the inception of the databases until 18 November 2023. Search strategies for the databases were developed (see Supplementary Table S1), and searches were performed without any language restrictions. Clinical registers, including clinicaltrials.gov and chictr.org.cn, were searched for completed studies that were not reported in peer-reviewed journals. In addition, previously published reviews were examined, and their reference lists were screened for potentially missing studies.
After conducting a literature search, two reviewers independently screened the retrieved articles. The screening process was conducted first at the title-and-abstract level and then at the full-text level. Any discrepancies in study selection were resolved through group discussion and arbitrated by a third reviewer. Only studies that met all of the following conditions were included: (1) reported as a randomized controlled trial; (2) included healthy adults over the age of 18 who planned to travel and took preventative measures; (3) assessing the effectiveness of various preventative measures, including bismuth subsalicylate, probiotics, rifaximin, and vaccines; (4) reporting the incidence of TD after travel to high-risk areas.
The study’s primary outcome was the incidence of TD. TD was defined as the passage of at least three unformed stools within a 24-hour period accompanied by at least one of the following conditions: abdominal pain or cramps, nausea, vomiting, fever (≥37.8°C), fecal urgency, passage of gross blood or mucus in stool, tenesmus, or moderate to severe increase in intestinal gas, according to our previous systematic review (Fan et al., 2022) and the American College of Gastroenterology (AGC) guideline (Riddle et al., 2016). The safety outcome will be treatment-related adverse events.
Two independent reviewers performed data extraction. The eligible trials’ characteristics, including baseline parameters of participants, details of interventions and controls, and outcome measures, were extracted and presented. The authors, year of publication, total sample size of the trial, study design, and follow-up period were recorded. Baseline parameters of the participants were recorded as mean age, proportion of females, and mean scores of body mass index, and travel destination. The study recorded the dosage and frequency of treatment interventions. Missing data were obtained by contacting the authors via email. A third reviewer checked the extracted data for accuracy before preparing it for meta-analysis.
The Cochrane risk of bias tool (RoB 2) was used to assess the risk of bias in eligible trials (Sterne et al., 2019). The tool assessed five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. The RoB 2 tool provided an overall evaluation of each trial, classifying it as having low risk of bias, high risk of bias, or some concerns based on the response to signaling questions for each domain.
The Confidence in Network Meta-Analysis (CINeMA) tool was used to grade the evidence. This tool is based on a methodological framework that assesses evidence of network meta-analysis in six domains: within-study bias, reporting bias, indirectness, imprecision, heterogeneity, and incoherence (Nikolakopoulou et al., 2020).
The main objective of this study was to compare the incidence of TD when treated with bismuth subsalicylate, probiotics, rifaximin, and vaccines. To achieve this, we conducted a frequentist-approach network meta-analysis to perform pairwise comparisons since there is a lack of head-to-head comparison between these treatments. Placebo control was used as a common comparator, and the treatment effects were calculated relative to the placebo control. Pairwise comparisons were made based on the calculated estimates using relative ratios (RRs), where a lower value of RR indicated a better treatment effect. The analysis was performed using a random-effect model. The Surface Under the Cumulative Ranking curve (SUCRA) score was estimated using the network meta-analysis model. This provides information on the probability of a treatment being the best among all treatments (Daly et al., 2019).
To test the robustness of the results, two subgroup analyses were conducted. The first analysis focused on studies with low RoB, while the second analysis focused on studies with some concerns or high RoB. The results from these two subgroups were compared to determine whether RoB had an impact on the study results. We conducted separate analyses on participants traveling to Mexico and those traveling to other regions. This was done because many studies have tested the preventive effects of treatments specifically for those traveling to Mexico. We compared the results from these two subgroups to determine if travel destination had an impact on the study outcomes.
Consistency of the network meta-analysis was assessed by comparing results from direct and indirect evidence. A significant inconsistency was considered when the z-test indicated a p-value less than 0.05. Global heterogeneity of the network meta-analysis was examined using Cochran’s Q test and the I2 statistics. An I2 value less than 40% was considered unimportant heterogeneity (Higgins, 2011).
The characteristics of the included RCTs are summarized in Figure 1, which presents the process and results of the literature search and study selection. A total of 1,095 records were found during the literature search, and 31 trials (recruiting 10,879 participants) were included in the analysis (de dios Pozo-Olano et al., 1978; DuPont et al., 1980, 1987, 2005; Graham et al., 1983; Steffen et al., 1986; Black et al., 1989; Kollaritsch and Wiedermann, 1989; Oksanen et al., 1990; Peltola et al., 1991; Kollaritsch et al., 1993; Katelaris et al., 1995; Scerpella et al., 1995; Hilton et al., 1997; Wiedermann et al., 2000; Leyten et al., 2005; Briand et al., 2006; McKenzie et al., 2007, McKenzie et al., 2008; Sack et al., 2007; Armstrong et al., 2010; Drakoularakou et al., 2010; Martinez-Sandoval et al., 2010; Flores et al., 2011; Virk et al., 2013; Zanger et al., 2013; Krokowicz et al., 2014; Hasle et al., 2017; Savarino et al., 2019; Anu et al., 2023; Maier et al., 2023). Table 1 shows the characteristics of the included studies.
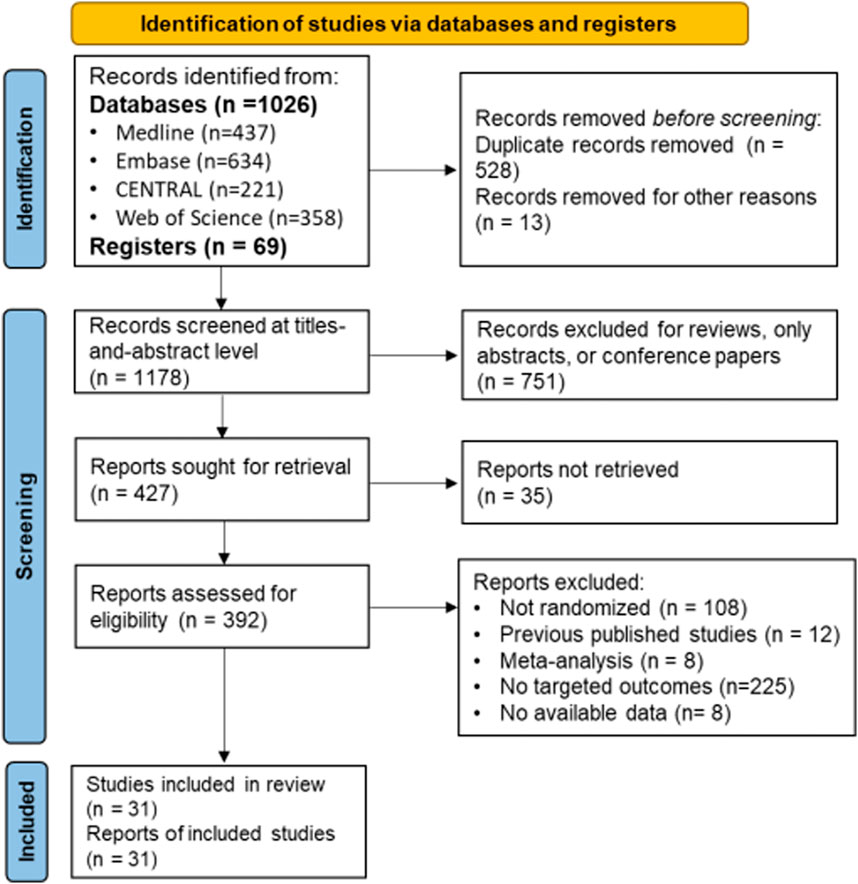
Figure 1. Study flowchart.
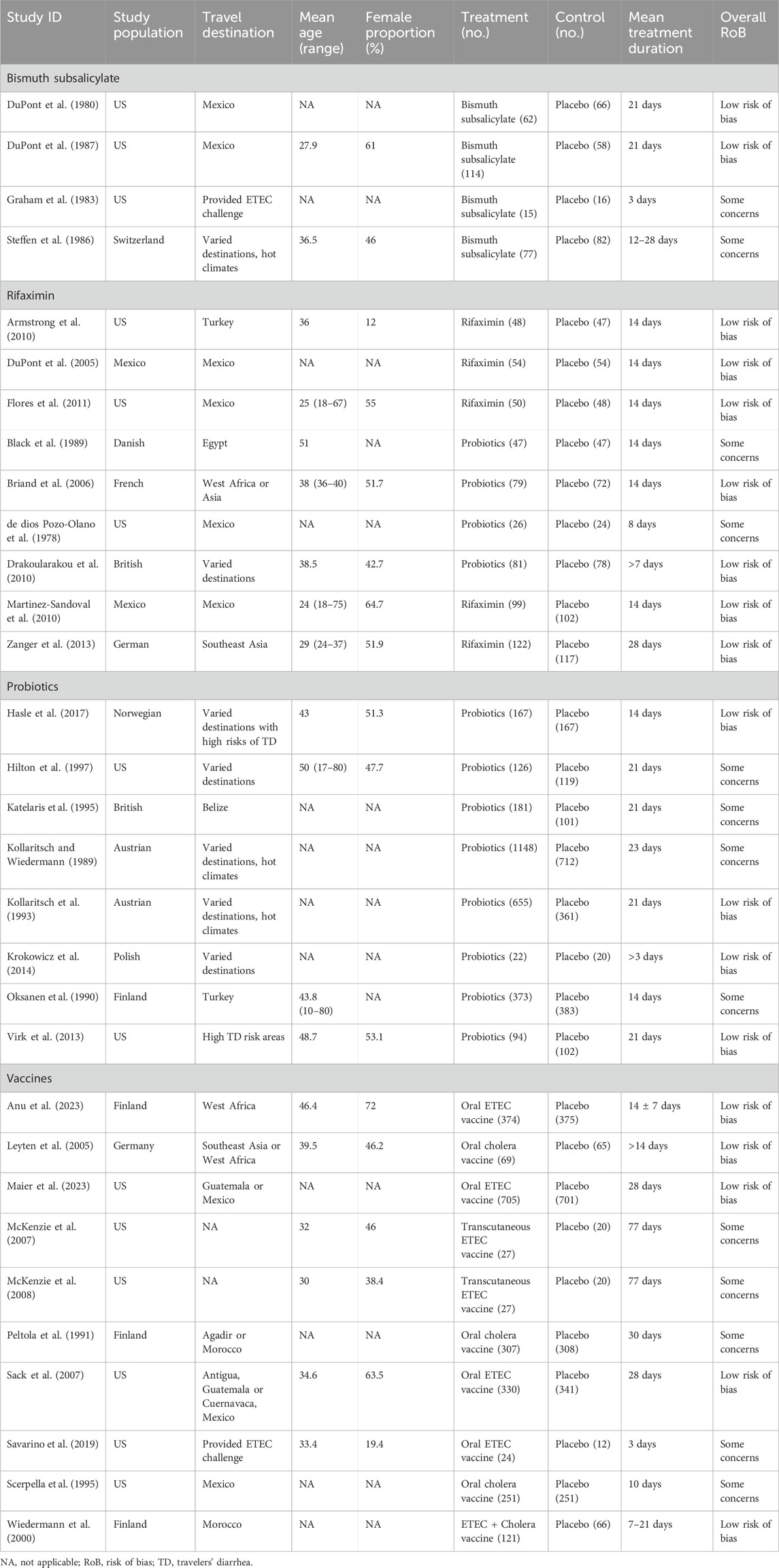
Table 1. Trial characteristics.
Of these studies, sixteen were evaluated as having a low risk of bias, while fifteen were classified as having some concerns. Supplementary Figure S1 displays a detailed assessment of the risk of bias. The most common concerns were deviations from the intended interventions in eight studies and missing outcome data in eleven studies.
In this aggregate-level network meta-analysis, we included all 31 studies, comparing five categories of treatments: bismuth subsalicylate (209 participants), placebo (5,034 participants), probiotics (2,977 participants), rifaximin (373 participants), and vaccine (2,286 participants). Figure 2 displays the net-graph of this network meta-analysis. In the study, Bismuth subsalicylate, rifaximin, and probiotics were found to significantly reduce the incidence of TD when compared to the placebo (Figure 2). Bismuth subsalicylate was the most effective treatment (SUCRA score, 0.972) according to Table 2, which shows the results of pairwise comparisons. Bismuth subsalicylate was found to be more effective in reducing TD incidence than probiotics and vaccines (Table 2). There was no evidence of inconsistency between direct and indirect estimates. The test of heterogeneity showed slight heterogeneity (I2 = 40.2%, tau2 = 0.015, Cochran’s Q = 45.2).
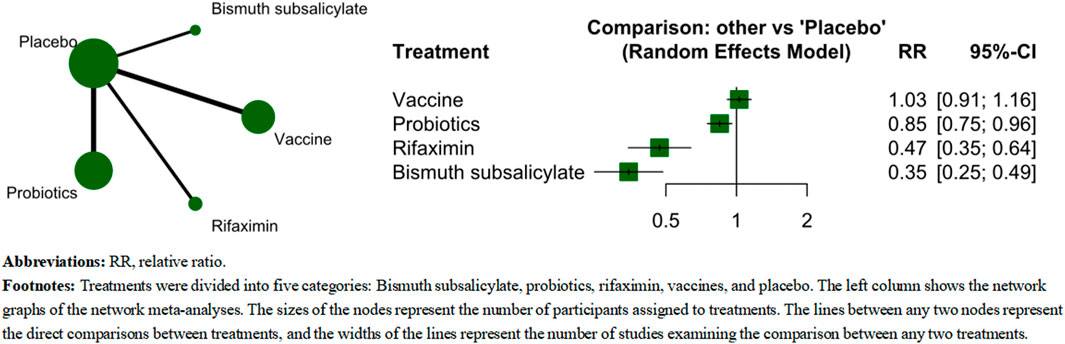
Figure 2. The comparative effectiveness of category-level analysis.
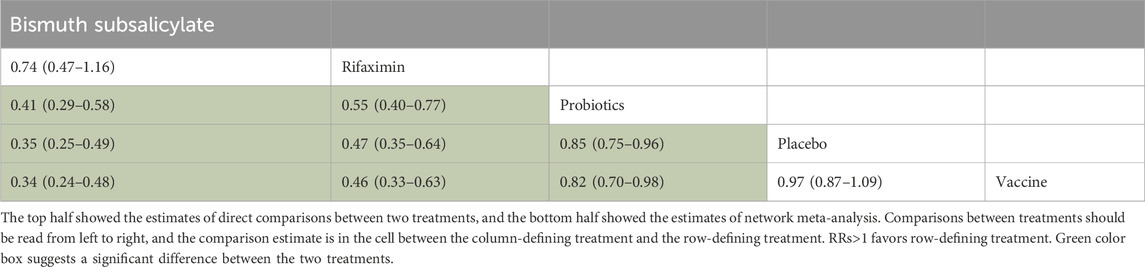
Table 2. Pairwise comparison between probiotics and rifaximin.
The individual-level network meta-analysis included 31 studies, comparing 14 treatments: (BSS, n = 209), cholera vaccines (n = 627), Entero. faecium SF68 + S. cerevisiae CNCM I-4444 + fructo-oliogosaccharide (ESCF, n = 94), enterotoxigenic Escherichia coli (ETEC, n = 1,538), ETEC + cholera vaccines (n = 121), galacto-oligosaccharide (GAO, n = 248), L. acidophilus + L. bulgaricus + Bifido.bifidum + Strept. Thermophilus (LABST, n = 47), (LAN, n = 260), (LHG, n = 26), (LRG, n = 499), Placebo (n = 5,054), Rifaximin (n = 373), S. boulardii CNCM I-745 (SBC, n = 1803), and sodium butyrate (SOB, n = 22). The result showed that SOB, BSS, and rifaximin ranked the most effective treatments in the analysis (Figure 3). In pairwise comparisons, BSS was superior than most of the other treatments (Table 3). The test of heterogeneity showed unimportant heterogeneity (I2 = 39.7%, tau2 = 0.0174, Cochran’s Q = 31.51).
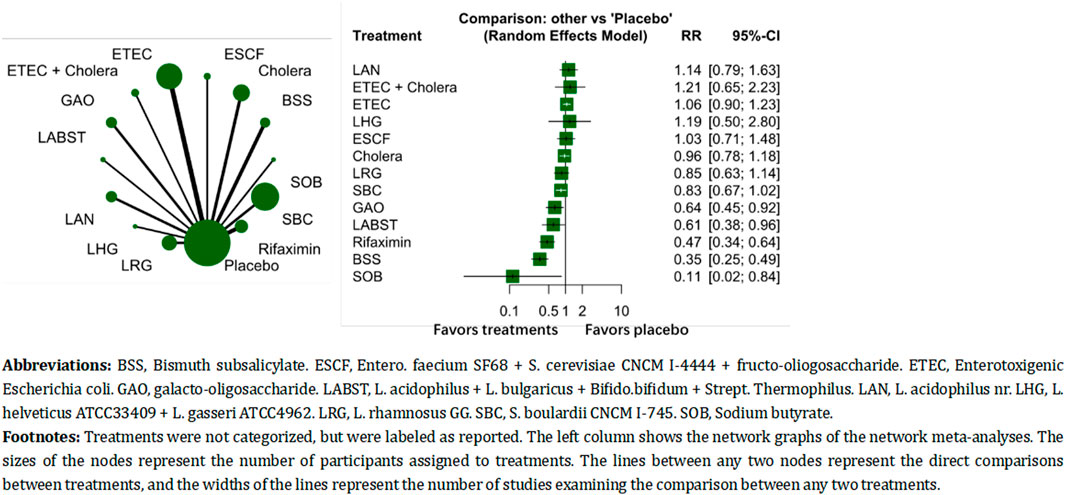
Figure 3. The comparative effectiveness of differential individual treatments.
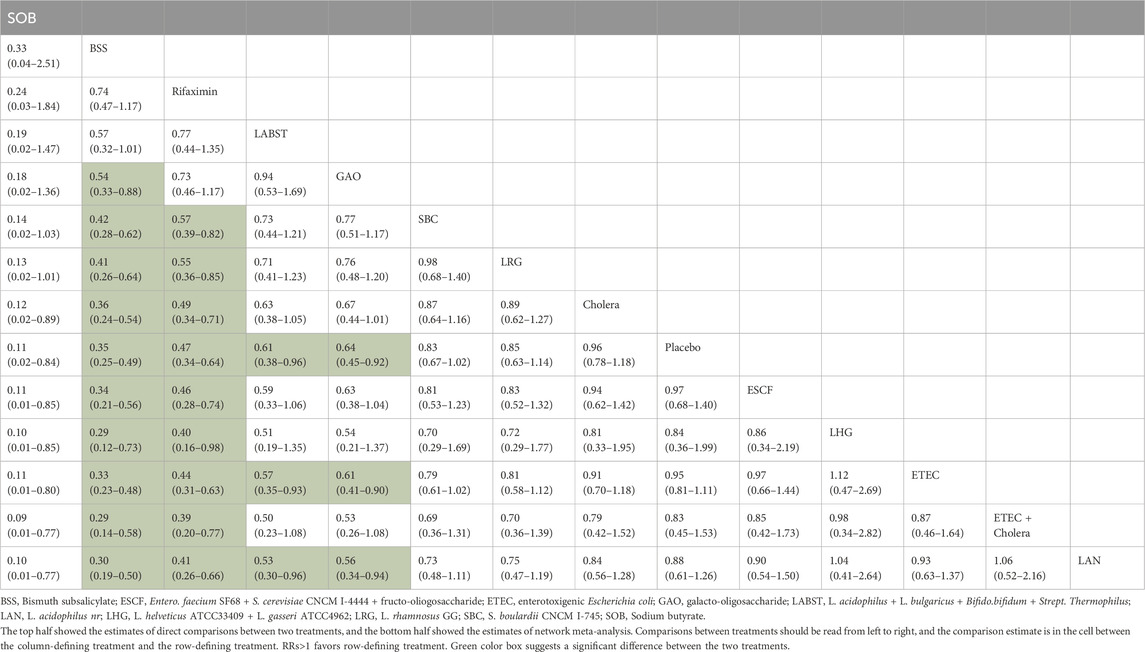
Table 3. Pairwise comparisons of differential probiotics and rifaximin.
In the category-level analysis, the first subgroup analysis revealed that BSS was the most effective treatment when studies with high risk of bias or some concerns were excluded (Supplementary Figure S2). However, when studies with high risk of bias or some concerns were included, rifaximin was found to be the most effective treatment (Supplementary Figure S3). In the individual-level analysis, BSS was ranked as the most effective treatment when studies with a high risk of bias or some concerns were excluded (see Supplementary Figure S4). On the other hand, SOB was ranked as the most effective when studies with high risk or some concerns were included (see Supplementary Figure S5).
The second subgroup analysis in the category-level analysis showed that BSS was the most effective in participants with a destination to Mexico (see Supplementary Figures S6, S7). In the individual-level analysis, SOB was the most effective (see Supplementary Figures S8, S9).
Supplementary Figure S11 presents the results of evidence grading for aggregate-level analysis. The comparison between rifaximin and placebo achieved high confidence, while the comparisons between BSS and placebo, ETEC and probiotics, and rifaximin and vaccines achieved moderate confidence.
Supplementary Figure S12 displays the results of evidence grading for individual-level analysis. The remaining comparisons achieved low confidence. The majority of comparisons achieved very low to low confidence.
The analysis at the aggregate level revealed that rifaximin had a lower adverse event rate than placebo, while BSS had a significantly higher adverse event rate than placebo (I2 = 20.6%, tau2 = 0.01, Cochran’s Q = 23.92) (Figure 4). At the individual level, most treatments had similar adverse event rates (I2 = 0%, tau2 = 0, Cochran’s Q = 11.1) (Figure 4).
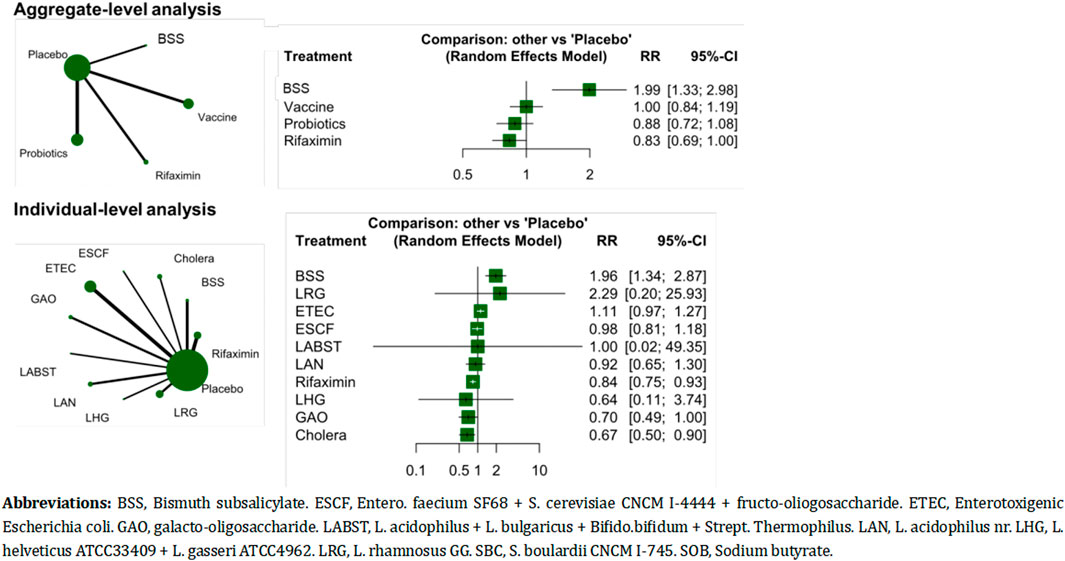
Figure 4. The adverse event rates of the treatments.
The network meta-analysis compared BSS, probiotics, rifaximin, and vaccines for preventing TD at both the category and individual levels. The results showed that BSS and rifaximin were both effective compared to placebo, with at least moderate certainty. Furthermore, rifaximin was more effective than vaccines and probiotics, with moderate evidence. Considering the adverse event rate, rifaximin was a better treatment option than placebo due to its lack of significant adverse events. On the other hand, BSS had a higher adverse event rate. Therefore, rifaximin had a better balance between benefit and harm.
This network meta-analysis is the first to compare the effectiveness of all currently available pharmacological treatments for preventing TD. The previous meta-analysis compared only three categories of treatments: rifaximin, probiotics, and BSS. In this network meta-analysis, we added oral ETEC vaccines and cholera vaccines. We also used the CINeMA tool to appraise the certainty of the evidence, which was not done in the previous review. The CINeMA appraisal results assist clinicians in evaluating the comparative effectiveness of a treatment and their confidence in its effectiveness.
Previous meta-analyses have suggested a marginal benefit of using antibiotics in the prevention of TD (Alajbegovic et al., 2012), in addition to our network meta-analyses. However, this is hindered in clinical practice by short follow-up periods, variability in settings and causes of acute diarrhea, and a deficiency in person-time analysis. Furthermore, there are significant differences in dosages, administration frequencies, and formulations. Additional variation can be observed in the timing and administration of these preparations in relation to various factors such as travel populations and locations, as well as concurrent antimicrobial treatment. In summary, future studies should aim to prolong the follow-up period, determine the pathogens that are suitable for rifaximin prevention of TD, study the impact of setting variability on the prevention effect, and perform person-time analysis.
We conducted an exploratory study to analyze the impact of setting variability on the preventive effect. To achieve this, we performed a subgroup analysis by separately analyzing the population with a destination to Mexico and those with a destination to other locations. This was necessary because numerous studies have been conducted in populations with a destination to Mexico. The results showed that setting variability did not affect the preventive effect of BSS and rifaximin.
Our network meta-analysis indicates a higher rate of adverse events associated with BSS in TD prevention, which limits its use in clinical practice. The adverse events commonly encountered include nausea, bitter taste, diarrhea, and dark/black stools. These events are usually mild and do not require special medical care. However, prolonged overconsumption of bismuth subsalicylate can lead to BSS toxicity, which is characterized by blackening of the tongue and teeth, fatigue, mood changes, and deterioration of mental status (Budisak and Abbas, 2023). Therefore, future studies should collect dose-effect data of adverse events and provide clinicians with the necessary information to weigh the benefits and harms.
Our study had limitations. Firstly, we may have missed eligible trials despite our comprehensive search for trials examining the effect of pharmacological treatment on TD prevention. Secondly, we were unable to study the source of infection due to insufficient background information, which may be an important factor that influences the prevention effect. Third, the allocation of participants to each treatment arm was greatly imbalanced in the network meta-analysis, which may have caused estimation bias and indicated a lack of trials in this field. Fourth, our study may have limitations in the generalizability of the results. TD is not only attributed to bacterial infection, but also to parasitic infection, especially in the tropics, or viral infection (mainly Noro virus). The treatments, antibiotic treatments or probiotics, may be appropriate for bacterial infection.
In conclusion, our network meta-analysis found that BSS and rifaximin were relatively effective treatments for the prevention of TD. Considering the grading of evidence and safety issues, rifaximin is recommended among the treatments.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
HF: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Investigation, Writing–original draft. ICL: Data curation, Project administration, Validation, Writing–review and editing. LG: Data curation, Project administration, Writing–review and editing. LW: Data curation, Software, Supervision, Visualization, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Scientific and Technological Research Program of Chongqing Municipal Education Commission (grant no. KJQN202301613). Regional Tourism Industry Development Research Collaborative Innovation Center, Chongqing University of Education (2021XJPT07). High level Talent Research Initiation Project of Chongqing University of Education (2023BSRC022). This research was partially supported by grants from the Chongqing Federation of Social Science Associations (2022PY29), the Scientific and Technological Research Program of Chongqing Municipal Education Commission (KJQN202001603), and the Scientific and Technological Project in Henan Province (242102321142).
We extend our deepest gratitude to all investigators who have made their valuable statistics publicly accessible, contributing significantly to the research community. We would also like to acknowledge Miss. Huaxia Yang, Miss. Fang Fang, Miss. Yan Liu, Mr. Dong Liu, Mr. Chenglin Du, Mr. Yuyang Zhang, and Miss. Tingting Li for their indispensable assistance in performing the quality review of our findings, the analysis, and the creation of figures.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1361501/full#supplementary-material
Ahmed, T., Bhuiyan, T. R., Zaman, K., Sinclair, D., and Qadri, F. (2013). Vaccines for preventing enterotoxigenic Escherichia coli (ETEC) diarrhoea. Cochrane Database Syst. Rev. 2013, CD009029. doi:10.1002/14651858.CD009029.pub2
Alajbegovic, S., Sanders, J. W., Atherly, D. E., and Riddle, M. S. (2012). Effectiveness of rifaximin and fluoroquinolones in preventing travelers’ diarrhea (TD): a systematic review and meta-analysis. Syst. Rev. 1, 39. doi:10.1186/2046-4053-1-39
Anu, K., Marianna, R., Sakari, J. T., Pakkanen Sari, H., Jukka-Pekka, P., Anu, P., et al. (2023). Safety and immunogenicity of ETVAX®, an oral inactivated vaccine against enterotoxigenic Escherichia coli diarrhoea: a double-blinded, randomized, placebo-controlled trial amongst Finnish travellers to Benin, West Africa. J. Travel Med. 30, taad045. doi:10.1093/jtm/taad045
Armstrong, A. W., Ulukan, S., Weiner, M., Mostafa, M., Shaheen, H., Nakhla, I., et al. (2010). A randomized, double-blind, placebo-controlled study evaluating the efficacy and safety of rifaximin for the prevention of travelers’ diarrhea in US military personnel deployed to Incirlik Air Base, Incirlik, Turkey. J. Travel Med. 17, 392–394. doi:10.1111/j.1708-8305.2010.00462.x
Bae, J.-M. (2018). Prophylactic efficacy of probiotics on travelers’ diarrhea: an adaptive meta-analysis of randomized controlled trials. Epidemiol. Health 40, e2018043. doi:10.4178/epih.e2018043
Black, F. T., Andersen, P. L., Ørskov, J., Ørskov, F., Gaarslev, K., and Laulund, S. (1989). “Prophylactic efficacy of lactobacilli on traveler’s diarrhea,” in Travel medicine: proceedings of the first conference on international travel medicine, zürich, Switzerland, 5–8 april 1988. Editors R. Steffen, H. Lobel, J. Haworth, and D. J. Bradley (Berlin, Heidelberg: Springer), 333–335. doi:10.1007/978-3-642-73772-5_70
Briand, V., Buffet, P., Genty, S., Lacombe, K., Godineau, N., Salomon, J., et al. (2006). Absence of efficacy of nonviable Lactobacillus acidophilus for the prevention of traveler’s diarrhea: a randomized, double-blind, controlled study. Clin. Infect. Dis. 43, 1170–1175. doi:10.1086/508178
Budisak, P., and Abbas, M. (2023). Bismuth subsalicylate. Available at: http://www.ncbi.nlm.nih.gov/books/NBK560697/ (Accessed December 21, 2023).
Daly, C. H., Neupane, B., Beyene, J., Thabane, L., Straus, S. E., and Hamid, J. S. (2019). Empirical evaluation of SUCRA-based treatment ranks in network meta-analysis: quantifying robustness using Cohen’s kappa. BMJ Open 9, e024625. doi:10.1136/bmjopen-2018-024625
de dios Pozo-Olano, J., Warram, J. H., Gómez, R. G., and Cavazos, M. G. (1978). Effect of a lactobacilli preparation on traveler's diarrhea. Gastroenterology 74, 829–830. doi:10.1016/0016-5085(78)90135-x
Drakoularakou, A., Tzortzis, G., Rastall, R. A., and Gibson, G. R. (2010). A double-blind, placebo-controlled, randomized human study assessing the capacity of a novel galacto-oligosaccharide mixture in reducing travellers’ diarrhoea. Eur. J. Clin. Nutr. 64, 146–152. doi:10.1038/ejcn.2009.120
DuPont, H. L., Ericsson, C. D., Johnson, P. C., Bitsura, J. A., DuPont, M. W., and de la Cabada, F. J. (1987). Prevention of travelers’ diarrhea by the tablet formulation of bismuth subsalicylate. JAMA 257, 1347–1350. doi:10.1001/jama.1987.03390100085031
DuPont, H. L., Jiang, Z.-D., Okhuysen, P. C., Ericsson, C. D., de la Cabada, F. J., Ke, S., et al. (2005). A randomized, double-blind, placebo-controlled trial of rifaximin to prevent travelers’ diarrhea. Ann. Intern Med. 142, 805–812. doi:10.7326/0003-4819-142-10-200505170-00005
DuPont, H. L., Sullivan, P., Evans, D. G., Pickering, L. K., Evans, D. J., Vollet, J. J., et al. (1980). Prevention of traveler’s diarrhea (emporiatric enteritis). Prophylactic administration of subsalicylate bismuth. JAMA 243, 237–241. doi:10.1001/jama.243.3.237
Fan, H., Gao, L., Yin, Z., Ye, S., Zhao, H., and Peng, Q. (2022). Probiotics and rifaximin for the prevention of travelers’ diarrhea: a systematic review and network meta-analysis. Med. Baltim. 101, e30921. doi:10.1097/MD.0000000000030921
Flores, J., Dupont, H. L., Jiang, Z.-D., Okhuysen, P. C., Melendez-Romero, J. H., Gonzalez-Estrada, A., et al. (2011). A randomized, double-blind, pilot study of rifaximin 550 mg versus placebo in the prevention of travelers’ diarrhea in Mexico during the dry season. J. Travel Med. 18, 333–336. doi:10.1111/j.1708-8305.2011.00549.x
Giddings, S. L., Stevens, A. M., and Leung, D. T. (2016). Traveler’s diarrhea. Med. Clin. North Am. 100, 317–330. doi:10.1016/j.mcna.2015.08.017
Graham, D. Y., Estes, M. K., and Gentry, L. O. (1983). Double-blind comparison of bismuth subsalicylate and placebo in the prevention and treatment of enterotoxigenic Escherichia coli-induced diarrhea in volunteers. Gastroenterology 85, 1017–1022. doi:10.1016/s0016-5085(83)80066-3
Hasle, G., Raastad, R., Bjune, G., Jenum, P. A., and Heier, L. (2017). Can a galacto-oligosaccharide reduce the risk of traveller’s diarrhoea? A placebo-controlled, randomized, double-blind study. J. Travel Med. 24. doi:10.1093/jtm/tax057
Higgins, J. P. T. (2011). Cochrane handbook for systematic reviews of interventions version 5.1.0. The Cochrane Collaboration.
Hilton, E., Kolakowski, P., Singer, C., and Smith, M. (1997). Efficacy of lactobacillus GG as a diarrheal preventive in travelers. J. Travel Med. 4, 41–43. doi:10.1111/j.1708-8305.1997.tb00772.x
Hu, Y., Ren, J., Zhan, M., Li, W., and Dai, H. (2012). Efficacy of rifaximin in prevention of travelers’ diarrhea: a meta-analysis of randomized, double-blind, placebo-controlled trials. J. Travel Med. 19, 352–356. doi:10.1111/j.1708-8305.2012.00650.x
Hutton, B., Salanti, G., Caldwell, D. M., Chaimani, A., Schmid, C. H., Cameron, C., et al. (2015). The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162, 777–784. doi:10.7326/M14-2385
Katelaris, P. H., Salam, I., and Farthing, M. J. G. (1995). Lactobacilli to prevent traveler’s diarrhea? N. Engl. J. Med. 333, 1360–1361. doi:10.1056/NEJM199511163332016
Kollaritsch, H., Holst, H., Grobara, P., and Wiedermann, G. (1993). Prevention of traveler’s diarrhea with Saccharomyces boulardii. Results of a placebo controlled double-blind study. Fortschr Med. 111, 152–156.
Kollaritsch, H. H., and Wiedermann, G. (1989). “Prevention of traveler’s diarrhea: a double-blind randomized trial with Saccharomyces cerevisiae hansen CBS 5926,” in Travel medicine: proceedings of the first conference on international travel medicine, zürich, Switzerland, 5–8 april 1988. Editors R. Steffen, H. Lobel, J. Haworth, and D. J. Bradley (Berlin, Heidelberg: Springer), 328–332. doi:10.1007/978-3-642-73772-5_69
Krokowicz, L., Kaczmarek, B. F., Krokowicz, P., Stojcev, Z., Mackiewicz, J., Walkowiak, J., et al. (2014). Sodium butyrate and short chain fatty acids in prevention of travellers’ diarrhoea: a randomized prospective study. Travel Med. Infect. Dis. 12, 183–188. doi:10.1016/j.tmaid.2013.08.008
Leyten, E. M. S., Soonawala, D., Schultsz, C., Herzog, C., Ligthelm, R. J., Wijnands, S., et al. (2005). Analysis of efficacy of CVD 103-HgR live oral cholera vaccine against all-cause travellers’ diarrhoea in a randomised, double-blind, placebo-controlled study. Vaccine 23, 5120–5126. doi:10.1016/j.vaccine.2005.05.022
Maier, N., Grahek, S. L., Halpern, J., Restrepo, S., Troncoso, F., Shimko, J., et al. (2023). Efficacy of an enterotoxigenic Escherichia coli (ETEC) vaccine on the incidence and severity of traveler’s diarrhea (TD): evaluation of alternative endpoints and a TD severity score. Microorganisms 11, 2414. doi:10.3390/microorganisms11102414
Martinez-Sandoval, F., Ericsson, C. D., Jiang, Z.-D., Okhuysen, P. C., Romero, J. H. M. M., Hernandez, N., et al. (2010). Prevention of travelers’ diarrhea with rifaximin in US travelers to Mexico. J. Travel Med. 17, 111–117. doi:10.1111/j.1708-8305.2009.00385.x
McKenzie, R., Bourgeois, A. L., Frech, S. A., Flyer, D. C., Bloom, A., Kazempour, K., et al. (2007). Transcutaneous immunization with the heat-labile toxin (LT) of enterotoxigenic Escherichia coli (ETEC): protective efficacy in a double-blind, placebo-controlled challenge study. Vaccine 25, 3684–3691. doi:10.1016/j.vaccine.2007.01.043
McKenzie, R., Darsley, M., Thomas, N., Randall, R., Carpenter, C., Forbes, E., et al. (2008). A double-blind, placebo-controlled trial to evaluate the efficacy of PTL-003, an attenuated enterotoxigenic E. coli (ETEC) vaccine strain, in protecting against challenge with virulent ETEC. Vaccine 26, 4731–4739. doi:10.1016/j.vaccine.2008.06.064
Ng, Q. X., Ho, C. Y. X., Shin, D., Venkatanarayanan, N., and Chan, H. W. (2017). A meta-analysis of the use of rifaximin to prevent travellers’ diarrhoea. J. Travel Med. 24. doi:10.1093/jtm/tax025
Nikolakopoulou, A., Higgins, J. P. T., Papakonstantinou, T., Chaimani, A., Del Giovane, C., Egger, M., et al. (2020). CINeMA: an approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 17, e1003082. doi:10.1371/journal.pmed.1003082
Oksanen, P. J., Salminen, S., Saxelin, M., Hämäläinen, P., Ihantola-Vormisto, A., Muurasniemi-Isoviita, L., et al. (1990). Prevention of travellers’ diarrhoea by Lactobacillus GG. Ann. Med. 22, 53–56. doi:10.3109/07853899009147242
Peltola, H., Siitonen, A., Kyrönseppä, H., Simula, I., Mattila, L., Oksanen, P., et al. (1991). Prevention of travellers’ diarrhoea by oral B-subunit/whole-cell cholera vaccine. Lancet 338, 1285–1289. doi:10.1016/0140-6736(91)92590-x
Riddle, M. S., Connor, B. A., Beeching, N. J., DuPont, H. L., Hamer, D. H., Kozarsky, P., et al. (2017). Guidelines for the prevention and treatment of travelers’ diarrhea: a graded expert panel report. J. Travel Med. 24, S57–S74. doi:10.1093/jtm/tax026
Riddle, M. S., DuPont, H. L., and Connor, B. A. (2016). ACG clinical guideline: diagnosis, treatment, and prevention of acute diarrheal infections in adults. Am. J. Gastroenterol. 111, 602–622. doi:10.1038/ajg.2016.126
Sack, D. A., Shimko, J., Torres, O., Bourgeois, A. L., Francia, D. S., Gustafsson, B., et al. (2007). Randomised, double-blind, safety and efficacy of a killed oral vaccine for enterotoxigenic E. Coli diarrhoea of travellers to Guatemala and Mexico. Vaccine 25, 4392–4400. doi:10.1016/j.vaccine.2007.03.034
Savarino, S. J., McKenzie, R., Tribble, D. R., Porter, C. K., O’Dowd, A., Sincock, S. A., et al. (2019). Hyperimmune bovine colostral anti-CS17 antibodies protect against enterotoxigenic Escherichia coli diarrhea in a randomized, doubled-blind, placebo-controlled human infection model. J. Infect. Dis. 220, 505–513. doi:10.1093/infdis/jiz135
Scerpella, E. G., Sanchez, J. L., Mathewson, I. I. I., Torres-Cordero, J. V., Sadoff, J. C., Svennerholm, A. M., et al. (1995). Safety, immunogenicity, and protective efficacy of the whole-cell/recombinant B subunit (WC/rBS) oral cholera vaccine against travelers’ diarrhea. J. Travel Med. 2, 22–27. doi:10.1111/j.1708-8305.1995.tb00615.x
Steffen, R., DuPont, H. L., Heusser, R., Helminger, A., Witassek, F., Manhart, M. D., et al. (1986). Prevention of traveler’s diarrhea by the tablet form of bismuth subsalicylate. Antimicrob. Agents Chemother. 29, 625–627. doi:10.1128/AAC.29.4.625
Steffen, R., Hill, D. R., and DuPont, H. L. (2015). Traveler’s diarrhea: a clinical review. JAMA 313, 71–80. doi:10.1001/jama.2014.17006
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., et al. (2019). RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898. doi:10.1136/bmj.l4898
Virk, A., Mandrekar, J., Berbari, E. F., Boyce, T. G., Fischer, P. R., Kasten, M. J., et al. (2013). A randomized, double blind, placebo-controlled trial of an oral synbiotic (AKSB) for prevention of travelers’ diarrhea. J. Travel Med. 20, 88–94. doi:10.1111/jtm.12008
Walker, R. I., Steele, D., and Aguado, T.Ad Hoc ETEC Technical Expert Committee (2007). Analysis of strategies to successfully vaccinate infants in developing countries against enterotoxigenic E. coli (ETEC) disease. Vaccine 25, 2545–2566. doi:10.1016/j.vaccine.2006.12.028
Wiedermann, G., Kollaritsch, H., Kundi, M., Svennerholm, A. M., and Bjare, U. (2000). Double-blind, randomized, placebo controlled pilot study evaluating efficacy and reactogenicity of an oral ETEC B-subunit-inactivated whole cell vaccine against travelers’ diarrhea (preliminary report). J. Travel Med. 7, 27–29. doi:10.2310/7060.2000.00007
Zanger, P., Nurjadi, D., Gabor, J., Gaile, M., and Kremsner, P. G. (2013). Effectiveness of rifaximin in prevention of diarrhoea in individuals travelling to south and southeast Asia: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Infect. Dis. 13, 946–954. doi:10.1016/S1473-3099(13)70221-4
Keywords: prevention modalities, systematic review, network meta-analysis, travelers’, diarrhea
Citation: Fan H, Liu I-C, Gao L and Wu L (2024) Bismuth subsalicylate, probiotics, rifaximin and vaccines for the prevention of travelers’ diarrhea: a systematic review and network meta-analysis. Front. Pharmacol. 15:1361501. doi: 10.3389/fphar.2024.1361501
Received: 26 December 2023; Accepted: 26 February 2024;
Published: 18 April 2024.
Edited by:
Guoxun Chen, Huazhong Agricultural University, ChinaReviewed by:
Lixin Zhu, The Sixth Affiliated Hospital of Sun Yat-sen University, ChinaCopyright © 2024 Fan, Liu, Gao and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hao Fan, ZmFuaGFvY3EwNUBvdXRsb29rLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.