 Haiyan Xu
Haiyan Xu Wanxiang Zheng2
Wanxiang Zheng2 Min Li
Min Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 09 April 2024
Sec. Drugs Outcomes Research and Policies
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1355231
Background: Medication adherence in patients after percutaneous coronary intervention (PCI) is suboptimal, and discontinuation is common. Information on the temporal characteristics and associated factors of discontinuation and outcomes after PCI is insufficient to improve medication adherence interventions.
Methods: We conducted a single-center retrospective study of post-PCI patients by telephone survey and medical record extraction. Temporal characteristics and associated factors of discontinuation and outcomes were examined by survival curve analysis, Cox regression, or time-dependent Cox regression.
Results: Discontinuation and major adverse cardiovascular events (MACE) after PCI had similar temporal characteristics, with the highest incidence in the first year, followed by a decline. Temporary discontinuation was associated with pre-PCI medication nonadherence (HR 1.63; 95% CI: 1.09–2.43), lack of medication necessity (HR 2.33; 95% CI: 1.44–3.78), economic difficulties (HR 2.09; 95% CI: 1.26–3.47), routine disruption (HR 2.09; 95% CI: 1.10–3.99), and emotional distress (HR 2.76; 95% CI: 1.50–5.09). Permanent discontinuation was associated with residence in rural areas (HR 4.18; 95% CI: 1.84–9.46) or small to medium-sized cities (HR 4.21; 95% CI: 1.82–9.73), lack of medication necessity (HR 10.60; 95% CI: 6.45–17.41), and side effects (HR 3.30; 95% CI: 1.94–5.62). The MACE after PCI was associated with pre-PCI hypertension (HR 1.42; 95% CI: 1.04–1.96), two coronary stents (HR 1.42; 95% CI: 1.01–1.99) or three coronary stents (HR 1.66; 95% CI: 1.11–2.49) compared to one coronary stent up to this PCI, and temporary discontinuation (≤60 months HR 2.18; 95% CI: 1.47–3.25; >60 months HR 8.82; 95% CI: 3.65–21.28).
Conclusion: Discontinuation and MACE after PCI have similar temporal characteristics, temporary discontinuation and permanent discontinuation have different associated factors, and the former is associated with MACE. These findings may provide guidance for medication adherence interventions.
Globally, and particularly in developed countries, ischemic heart disease is the leading cause of death in people over 50 years of age (Diseases and Injuries, 2020). Percutaneous coronary intervention (PCI) is widely used to treat severe ischemic heart disease and has significantly improved outcomes (Hoole and Bambrough, 2020; Writing Committee et al., 2022). After PCI, patients need to take secondary preventive medications regularly for a long period of time, and medication adherence affects the long-term cardiovascular outcomes after PCI (Xie et al., 2019; Lee et al., 2023; Zhang et al., 2023), while it is suboptimal (Zhang et al., 2023). Although effective medication adherence interventions are significantly associated with improved outcomes (Allemann et al., 2017), current medication adherence interventions after PCI are unsatisfactory (Boyd et al., 2020; Chidester et al., 2022; Ho et al., 2022) and even produce mixed results (Ho et al., 2022).
To improve the effectiveness of medication adherence interventions, a deep understanding of the nature of medication adherence, especially its time-varying nature and associated factors, is essential (Gellad et al., 2017; Bosworth et al., 2018). According to the ABC terminology, medication adherence is a dynamic process with three phases, namely, initiation, implementation, and persistence, and survival analyses, such as K-M analysis and Cox regression, are advocated to fully embody this process (Vrijens et al., 2012). Discontinuation of medication based on patients’ own decision is a common behavior of medication nonadherence after PCI (Ofori-Asenso et al., 2018; Redfors et al., 2022), with a clear time of occurrence suitable for survival analyses. According to whether the medication is taken again, it can be divided into temporary discontinuation (also be called reinitiation) (Wawruch et al., 2023) and permanent discontinuation, reflecting the phases of implementation and persistence respectively (Vrijens et al., 2012; Kronish et al., 2021). At present, the time-varying nature of these two types of discontinuation and the factors associated with them are poorly understood. Research on the temporal characteristics of discontinuation after PCI mainly focuses on statins and antiplatelet agents (Franchi and Rollini, 2022; Yamamoto et al., 2023), with less attention paid to the overall trend of secondary preventive medications. This is a disadvantage to master its integrated characteristics. More importantly, there is still relatively little research on the factors associated with discontinuation after PCI (Harris et al., 2019; Yamamoto et al., 2023), especially for different patterns of discontinuation as well as their relationships with outcomes.
The purpose of this research is to investigate the temporal characteristics and associated factors of discontinuation and outcomes in patients with ischemic heart disease after PCI using survival analysis. It is part of a post-PCI medication adherence study and was approved for medical ethics review by the First Affiliated Hospital of the Army Medical University (Southwest Hospital) (approval number: KY2020050).
A single-center, retrospective cohort design was used to evaluate the temporal characteristics and associated factors of discontinuation and outcomes in patients after PCI. Patients with ischemic heart disease who had successfully undergone PCI at Southwest Hospital, had valid contact information, and were willing to participate in the study were enrolled as subjects. We identified the final participants for the following reasons. (1) Most existing post-PCI surveys focus on the first 3 years after PCI, and there are fewer data on the follow-up of patients beyond 3 years after PCI (Zhang et al., 2021; Zhang et al., 2023). (2) Our pre-survey showed that the success rate of surveying patients more than 10 years after PCI was very low (<20%) due to patient death, change of contact phone number, and unwillingness to cooperate. Therefore, we limited the survey population to patients 4–10 years after PCI. (3) The average annual volume of PCI performed in the Department of Cardiology at Southwest Hospital 4–10 years before the time of the present survey was approximately 1,000 cases. According to our previous survey experience, the incidence of medication nonadherence in patients with ischemic heart disease is about 40%, and the incidence of medication nonadherence in patients after PCI is even lower, especially the percentage of discontinuation. If we select a certain number of patients for investigation in each surgical year, it is not easy to grasp the final amount of valid data as a whole, nor is it conducive to obtaining sufficient data reflecting the characteristics of discontinuation and clinical outcomes at a certain period of time after PCI. Therefore, we selected 2 years of the 4–10 years after PCI and all their post-PCI patients as the study population, namely, all patients in the fourth year after PCI (surgery in 2016, n = 959) and the seventh year after PCI (surgery in 2013, n = 913).
According to the list of patients who successfully underwent PCI in the cardiology department of Southwest Hospital in 2013 and 2016, we found their telephone numbers from the hospital’s office computer. Patients and/or their family members were contacted by telephone, verbally solicited their opinions, and after their consent, the telephone survey was conducted and the results were recorded. Complete questionnaires from the telephone survey were extracted and completed with the medical record for baseline data at the time of PCI and information on discontinuation and outcomes after PCI. The pre-survey was conducted in May-July 2020, the centralized survey was conducted in October-December 2020, and the extraction of medical record information was centralized in January 2021, with a total of 1,811 patients surveyed. The data collection process is shown in Figure 1.
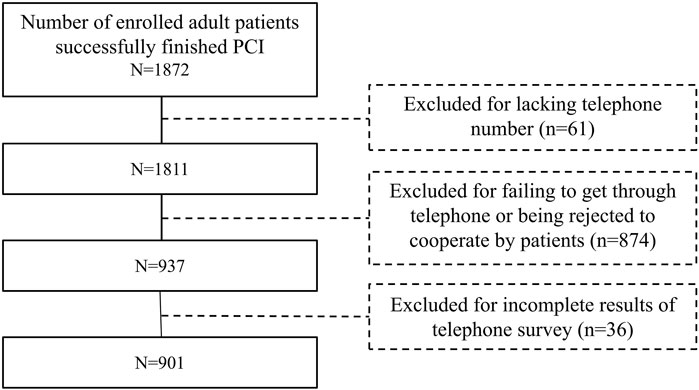
Figure 1. Flowchart of the study population enrollment.
The primary outcomes were discontinuation and MACE after PCI. Discontinuation was defined as patients stopping some or all of their prescribed medications for more than 1 week after PCI without consulting their physician or following their physician’s instructions. This includes both temporary and permanent discontinuation, with the former including resumption of medication at any time prior to our study and the latter not including resumption of medication at any time prior to our study. Due to the operability of telephone surveys, we did not differentiate between drug categories. This means that the discontinuation may include all medications prescribed by the patient’s physician for secondary prevention after PCI. MACE was defined as the composite of cardiac death, myocardial infarction, stroke, and coronary revascularization. Discontinuation and MACE after PCI were obtained by a combination of direct telephone inquiry and medical record extraction.
Related variables included baseline data at the time of PCI and barriers to medication adherence after PCI. Baseline data at the time of PCI were primarily obtained by chart review. It included demographic variables, such as sex, age, place of residence, province, education, marriage, and economic level; pre-PCI clinical characteristics, including Charlson Comorbidity Index (CCI), smoking, alcohol consumption, hypertension, hyperlipidemia, diabetes mellitus, myocardial infarction, stroke, coronary revascularization (CRV), pre-PCI medication nonadherence, meaning that the patient had any performance of these three phases of medication nonadherence before PCI; and vascular conditions up to this PCI, including number of coronary stents, noncoronary atherosclerosis or stenosis, and noncoronary stents. Barriers to medication adherence after PCI were assessed using a self-developed checklist based on the literature review, pre-survey, and interviews with clinical medical staff. The checklist includes 13 items, namely, lack of medication necessity, side effects, economic difficulties, complex prescriptions, memory decline, emotional distress, inconvenience, asymptomatic, dissatisfied with medication efficacy, disruptive routine, busy, extensive travel, and feelings of shame, each of which was self-reported as “yes” or “no” by the patient. During the telephone survey, patients were asked to rate each item according to their actual situation.
Statistical analysis was performed using SPSS v. 22.0 (SPSS, IBM, Chicago, United States of America) and R-4.3.3 for Windows (https://posit.co/). Proportional hazards hypothesis testing and Cox regression and time-dependent Cox regression analysis of the association between MACE and potential variables were performed with R, and other statistical analyses were performed with SPSS. Categorical variables were reported as absolute values with percentages and compared by the chi-squared test. Continuous variables (age and CCI) were divided into segments according to their valid data status and treated as categorical variables. Variables with missing data were not analyzed and are not reported in the results. Kaplan-Meier survival curves (tested with log-rank and plotted with GraphPad Prism 8) were used to analyze the association between MACE after PCI and related variables, including baseline data at the time of PCI, barriers to medication adherence, and discontinuation after PCI. Variables with p < 0.05 in the univariate analysis were tested for the proportional hazards hypothesis and then subjected to Cox regression or time-dependent Cox regression. When the potential factors associated with discontinuation or MACE included time-dependent variables or the proportional hazards hypothesis was not met, time-dependent Cox regression model was used. Multivariable Cox regression performed with SPSS used the “Forward: LR” method to assess the association between discontinuation and related variables. The multivariable time-dependent Cox regression performed by R used the “both” direction to assess the association between MACE and related variables. A two-tailed test with p < 0.05 was considered as statistically significant.
A total of 901 cases with valid data were obtained in this study, 357 PCI performed in 2013 and 544 PCI performed in 2016. All stents are drug-eluting stents. The age range for PCI was 34–90 years with a median of 64 years. Post-PCI time was 48–59 months for PCI in 2016 and 84–95 months for PCI in 2013. Education, marital status, and economic level were not included in the statistical analysis due to missing data. Other baseline characteristics at the time of PCI are shown in Table 1.

Table 1. Baseline characteristics of the study cohort.
Number of cases and incidence of discontinuation and MACE after PCI: temporary discontinuation (100, 11.1%), permanent discontinuation (80, 8.9%), and total discontinuation (180, 20.0%); cardiac death (21, 2.3%), myocardial infarction (22, 2.4%), stroke (48, 5.3%), CRV (113, 12.5%), and total MACE (180, 20.0%). Regarding the temporal distribution (Figure 2 and Supplementary Table S1), discontinuation occurred mainly in the first year after PCI with a gradual decrease over time. The temporal distributions of cardiac death, myocardial infarction, and stroke were all roughly wavy with two to three peaks; however, their sum, CRV, and MACE, were all highest in the first year after PCI and then declined either slowly or rapidly. The common trend of discontinuation and MACE may reflect specific changes in the psychological status of patients after PCI.
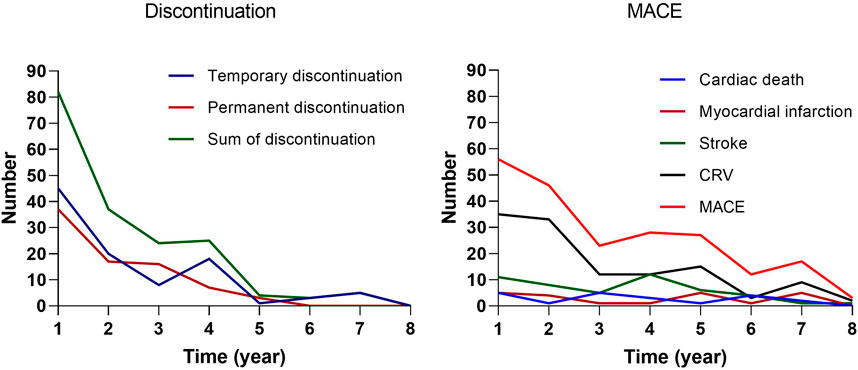
Figure 2. The number of discontinuation and MACE after PCI.
Barriers to medication adherence after PCI: We removed the barriers with less valid data, and merged asymptomatic with lack of medication necessity because they overlapped a lot and the latter is the result of the former as reflected by the patients. A total of 10 barriers to medication adherence were obtained, which, in descending order of the number of valid cases and incidence rate, were lack of medication necessity (123, 13.7%), economic difficulties (75, 8.3%), memory decline (57, 6.3%), side effects (49, 5.4%), complex prescriptions (38, 4.2%), inconvenience in accessing medical care (37, 4.1%), routine disruption (33, 3.7%), emotional distress (32, 3.6%), busy (28, 3.1%), and extensive travel (24, 2.7%).
The log-rank tests of the Kaplan-Meier analysis showed that pre-PCI CCI, pre-PCI hypertension, pre-PCI diabetes mellitus, pre-PCI CRV, pre-PCI medication nonadherence, number of coronary stents up to this PCI, and discontinuation after PCI were associated with MACE after PCI in the survival curves (Figure 3). Discontinuation after PCI did not meet the proportional hazards hypothesis, and the survival curves of no discontinuation and permanent discontinuation crossed at 60 months.
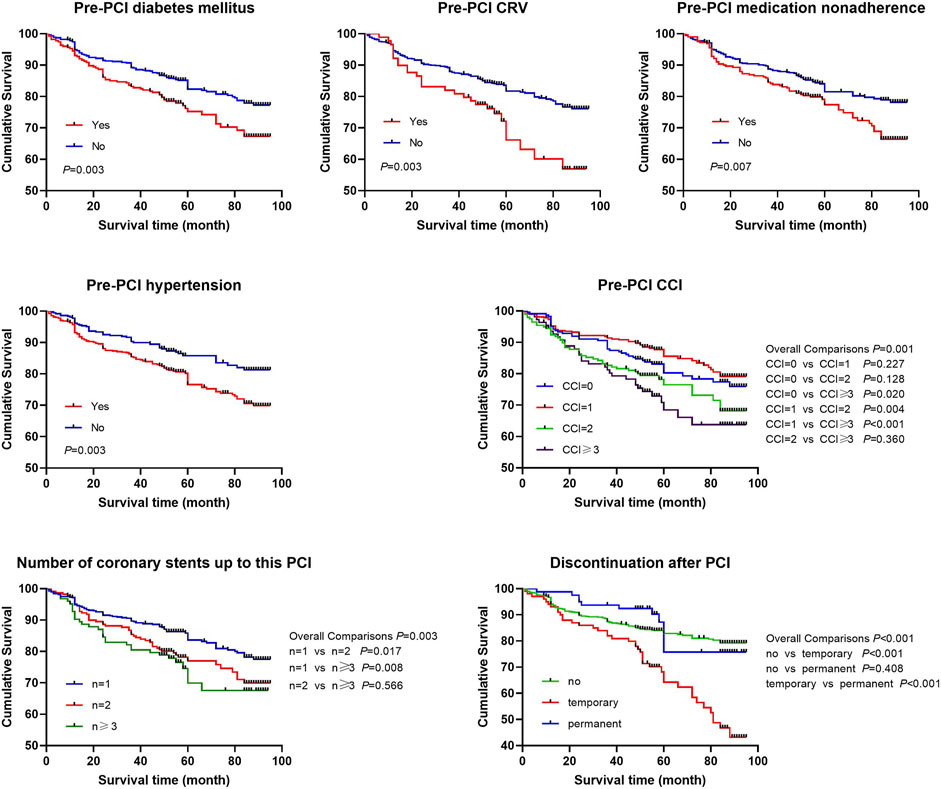
Figure 3. The survival curves after PCI.
Univariate analysis showed that (Table 2) place of residence, province, lack of medication necessity, economic difficulties, side effects, complex prescriptions, inconvenience, and routine disruption were associated with permanent discontinuation; place of residence, pre-PCI medication nonadherence and all barriers to medication adherence except extensive travel were associated with temporary discontinuation; pre-PCI CCI, pre-PCI hypertension, pre-PCI diabetes mellitus, pre-PCI CRV, pre-PCI medication nonadherence, number of coronary stents up to this PCI, time after PCI, and discontinuation were associated with MACE. These results were consistent with the unadjusted estimates from univariate Cox regression (Table 3). All of the above potential variables met the proportional hazards hypothesis except discontinuation after PCI.
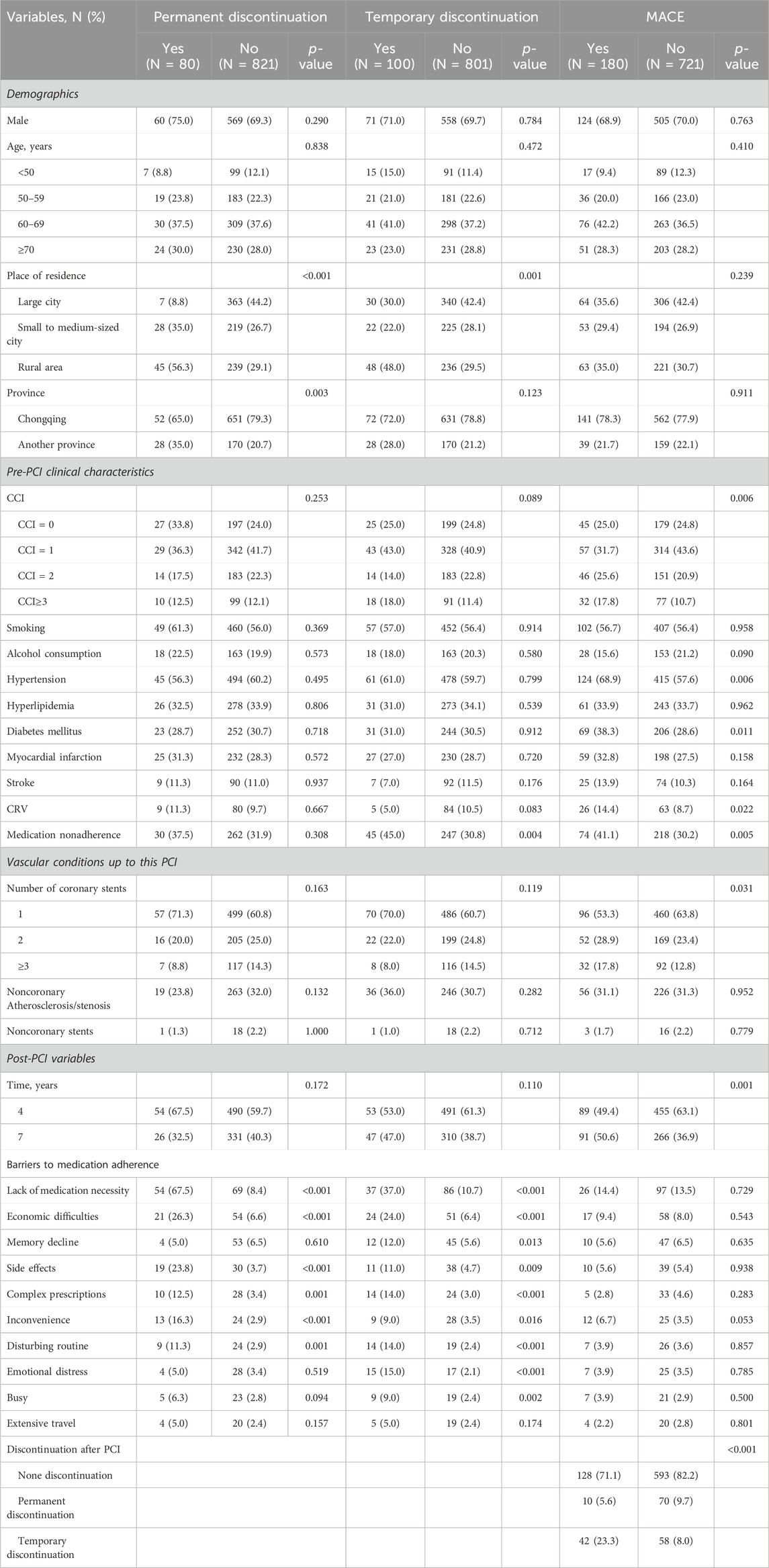
Table 2. Univariate associations with discontinuation and MACE after PCI.
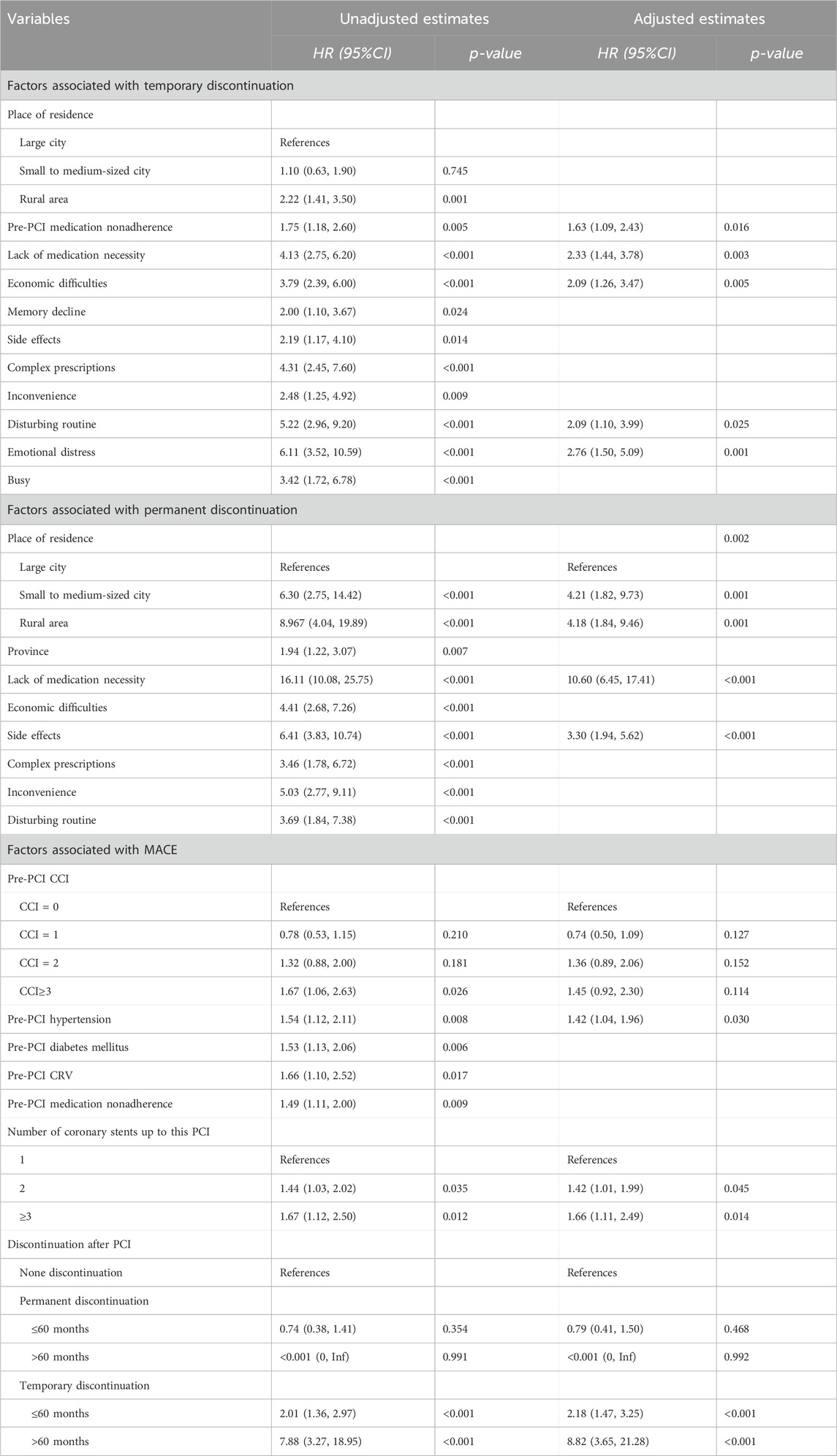
Table 3. Factors associated with discontinuation and MACE after PCI.
Multivariate Cox regression analysis with adjusted hazard ratio (HR) showed that (Table 3), pre-PCI medication nonadherence (HR 1.63; 95% CI: 1.09–2.43), lack of medication necessity (HR 2.33; 95% CI: 1.44–3.78), economic difficulties (HR 2.09; 95% CI: 1.26–3.47), routine disruption (HR 2.09; 95% CI: 1.10–3.99), and emotional distress (HR 2.76; 95% CI: 1.50–5.09) were associated with temporary discontinuation after PCI; compared with living in a large city, living in a rural area (HR 4.18; 95% CI: 1.84–9.46) or small to medium-sized city (HR 4.21; 95% CI: 1.82–9.73), lack of medication necessity (HR 10.60; 95% CI: 6.45–17.41) and side effects (HR 3.30; 95% CI: 1.94–5.62) were associated with permanent discontinuation after PCI. For discontinuation, according to the point of crossed survival curves, the time was divided into two periods, namely, ≤60 months and >60 months, and its association with MACE was analyzed separately. The multivariate time-dependent Cox regression showed that pre-PCI hypertension (HR 1.42; 95% CI: 1.04–1.96), two coronary stents (HR 1.42; 95% CI: 1.01–1.99) or three coronary stents (HR 1.66; 95% CI: 1.11–2.49) compared to one coronary stent up to this PCI, and temporary discontinuation (≤60 months HR 2.18; 95% CI: 1.47–3.25; >60 months HR 8.82; 95% CI: 3.65–21.28) were associated with MACE. It is evident that temporary discontinuation and permanent discontinuation were associated with different factors, and temporary discontinuation was associated with MACE after PCI.
We found that discontinuation and MACE after PCI had similar temporal characteristics, both with the highest incidence in the first year after PCI, and then either rapidly or slowly declining. Pre-PCI CCI, pre-PCI hypertension, pre-PCI diabetes mellitus, pre-PCI CRV, pre-PCI medication nonadherence, number of coronary stents up to current PCI, and temporary discontinuation after PCI were associated with the survival curves. The factors associated with temporary discontinuation and permanent discontinuation are different. Pre-PCI medication nonadherence, lack of medication necessity, economic difficulties, routine disruption, and emotional distress were associated with temporary discontinuation, whereas place of residence, lack of medication necessity, and side effects were associated with permanent discontinuation. Pre-PCI hypertension, number of coronary stents up to this PCI, and temporary discontinuation after PCI were associated with MACE after PCI. These findings may provide important guidance for medication adherence interventions in patients undergoing PCI.
The temporal characteristics of discontinuation and MACE after PCI had a similar pattern, which may reflect the same reason. Because temporary discontinuation was associated with MACE in the survival curves and time-dependent Cox regression analyses, this temporal characteristic may reflect the impact of medication adherence on adverse outcomes (Kronish et al., 2020; Princip et al., 2023). However, the existing literature also shows that other outcomes and psychological symptoms after PCI have a similar temporal characteristic (Gu et al., 2016; Williams et al., 2021; Murad et al., 2022; Vulcanescu et al., 2023). Therefore, in addition to the effect of medication adherence on outcomes, this temporal characteristic may also reflect the physical and psychological stress effect of ischemic heart disease or PCI (Vilchinsky et al., 2017; Birk et al., 2019; Kronish et al., 2020; Henein et al., 2022; Princip et al., 2023). The stress effect diminishes over time, resulting in a trend toward a decrease in associated medication nonadherence, psychological symptoms, and clinical outcomes. Thus, medication nonadherence after PCI may also be a consequence of patient maladaptation to the stress of the disease and/or PCI (Vilchinsky et al., 2017; Kronish et al., 2020; Narisawa et al., 2021; Princip et al., 2023). Clinical outcomes, on the other hand, may be influenced by both medication nonadherence and the stress of disease and/or PCI (Vilchinsky et al., 2017; Henein et al., 2022; Princip et al., 2023). Future work is needed to test these possibilities and to explore the possibility of developing medication adherence interventions from a stress perspective for patients undergoing PCI (Birk et al., 2019; von Känel et al., 2022).
Differences in the factors associated with temporary and permanent discontinuation may have interesting implications for medication adherence interventions. This difference may be relative and due to the fact that temporary and permanent discontinuation belong to different phases of medication adherence, namely, the implementation and persistence. Importantly, these differences may suggest that the two patterns of discontinuation require different models of medication adherence interventions. The lack of medication necessity is associated with both types of medication discontinuation, but it may be more closely associated with permanent discontinuation, in terms of its HR values. It can be concluded that discontinuations related to pre-PCI medication nonadherence, financial difficulties, routine disruption, and emotional distress are more likely to be transient and less difficult to intervene with, and tailored interventions may be appropriate (Xu et al., 2020). In contrast, discontinuation due to lack of medication necessity (West et al., 2020), living in a nonmetropolitan area (Pietrzykowski et al., 2020; Simon et al., 2021), and side effects (Zhou et al., 2021; Golder et al., 2022; Redfors et al., 2022; Yamamoto et al., 2023) may be more likely to be permanent and more difficult to intervene with, and an integrative consideration of patient perceptions, healthcare resources, medication characteristics, and therapeutic guidelines is needed to maximize benefit (Simon et al., 2021).
We found that temporary discontinuation was associated with MACE in survival curves and time-dependent Cox regression results, whereas permanent discontinuation was not. This suggests that temporary discontinuation after PCI may have a significant effect on MACE (Sorrentino et al., 2020; Redfors et al., 2022; Yamamoto et al., 2023), which is the basis for the need for adherence interventions. On the other hand, it suggests that permanent discontinuation after PCI has a nonsignificant effect on MACE, which is inconsistent with the results of previous studies and may be related to the design of our telephone survey (Xie et al., 2019). In clinical practice, certain medications, such as P2Y12 inhibitors and β-blockers, can be discontinued under physician supervision at specific times after PCI in certain patients without being associated with an increased risk of MACE (Sorrentino et al., 2020; Redfors et al., 2022; Halili et al., 2023; Kinlay et al., 2023; Park et al., 2023). Our telephone survey did not differentiate between the types of medications discontinued by self-administration, which may have led patients to confuse self-discontinuation with physician-guided discontinuation and to categorize physician-guided discontinuation as self-discontinuation. It is necessary to re-validate the current results again by distinguishing between medication classes in the future.
Our study provides guidance for medication adherence interventions after PCI. First, we found that both discontinuation and MACE had the highest incidence in the first year after PCI and then either rapidly or slowly decreased. We hypothesized that the stress of disease and/or PCI may be the common factors influencing discontinuation and outcomes after PCI. Therefore, theoretical constructs and practical tests of medication adherence interventions from a stress perspective would be worth trying. Second, we found that temporary and permanent discontinuation were associated with two different types of factors, which may require different intervention patterns. Third, temporary discontinuation after PCI associated with MACE provided evidence for the need for medication adherence interventions. Taken together, our study strengthens the rationale for medication adherence interventions in patients undergoing PCI and informs their theoretical construction and practical implementation.
Our study has shortcomings. First, we used a combination of patient self-report and medical records to assess discontinuation without differentiating medication classes for ease of use. Patient self-report may overestimate medication adherence (Fanaroff et al., 2020; Lauffenburger et al., 2020). More importantly, failure to categorize medications may confuse patients, as we discussed above, as well as adversely affect the association of discontinuation of different medications with MACE. These shortcomings may limit the generalizability of our research findings, as well as be disadvantageous for tailored medication adherence intervention. Therefore, it is necessary to combine objective assessments of medication adherence and categorize medication classes in the future (Kronish et al., 2021). Second, the medication adherence process includes multiple indicators other than discontinuation (Ho et al., 2009; Vrijens et al., 2012), and discontinuation in this study is only one of them, and the scope of investigation can be comprehensive enough to include more indicators in the future. Third, we discussed the possible psychological mechanisms of patients undergoing PCI related to our findings, which is mainly a theoretical speculation based on the existing literature and psychological general knowledge, which needs to be investigated by clinical trials.
To provide guidance for interventions to improve medication adherence after PCI, we analyzed the temporal characteristics and associated factors of discontinuation and MACE after PCI in patients with ischemic heart disease. Discontinuation and MACE had similar temporal characteristics, which may reflect the stressful effects of disease and/or PCI on medication adherence and outcomes. The factors associated with temporary and permanent discontinuation are different, which may suggest that they require different intervention patterns. Temporary discontinuation was associated with MACE after PCI, highlighting the need for medication adherence interventions. Permanent discontinuation was not associated with MACE after PCI, which may be related to the design of the telephone survey and needs to be retested in the future with differentiation of medications.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Committee of the First Affiliated Hospital of Army Medical University, PLA. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because this study conducted a retrospective investigation of self-discontinuation of medication and MACE after PCI based on telephone contact and medical record information. The patient’s informed consent was solicited over the phone, and the investigation continued if the patient agreed. If they did not agree, the investigation ended. Therefore, no paper informed consent form was signed.
HX: Conceptualization, Data curation, Funding acquisition, Project administration, Supervision, Validation, Writing–original draft, Writing–review and editing, Methodology. WZ: Conceptualization, Data curation, Formal Analysis, Writing–original draft, Investigation, Resources. JT: Data curation, Formal Analysis, Investigation, Writing–original draft. ML: Conceptualization, Supervision, Writing–review and editing, Project administration.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Humanities and Social Science Foundation of Army Military Medical University (2018XRW13).
We thank Houyuan Hu for his critical review and valuable input on the manuscript. We also thank Xiaolong Qu, Dan Deng, Jing Men, Yinping Yang, and Shiyi Qin for their help with data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1355231/full#supplementary-material
Allemann, S. S., Nieuwlaat, R., Navarro, T., Haynes, B., Hersberger, K. E., and Arnet, I. (2017). Congruence between patient characteristics and interventions may partly explain medication adherence intervention effectiveness: an analysis of 190 randomized controlled trials from a Cochrane systematic review. J. Clin. Epidemiol. 91, 70–79. doi:10.1016/j.jclinepi.2017.07.011
Birk, J. L., Sumner, J. A., Haerizadeh, M., Heyman-Kantor, R., Falzon, L., Gonzalez, C., et al. (2019). Early interventions to prevent posttraumatic stress disorder symptoms in survivors of life-threatening medical events: a systematic review. J. Anxiety Disord. 64, 24–39. doi:10.1016/j.janxdis.2019.03.003
Bosworth, H. B., Blalock, D. V., Hoyle, R. H., Czajkowski, S. M., and Voils, C. I. (2018). The role of psychological science in efforts to improve cardiovascular medication adherence. Am. Psychol. 73 (8), 968–980. doi:10.1037/amp0000316
Boyd, A. D., Ndukwe, C. I., Dileep, A., Everin, O. F., Yao, Y., Welland, B., et al. (2020). Elderly medication adherence intervention using the my interventional drug-eluting stent educational app: multisite randomized feasibility trial. JMIR Mhealth Uhealth 8 (6), e15900. doi:10.2196/15900
Chidester, J., Bennett, D., Mathew, C., Denkins, T., Vigen, R., Addo, T., et al. (2022). Telephone-based reminder to improve safety after percutaneous coronary intervention. Sci. Rep. 12 (1), 8597. doi:10.1038/s41598-022-12722-3
Diseases, G. B. D., and Injuries, C. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396 (10258), 1204–1222. doi:10.1016/S0140-6736(20)30925-9
Fanaroff, A. C., Peterson, E. D., Kaltenbach, L. A., Cannon, C. P., Choudhry, N. K., Henry, T. D., et al. (2020). Agreement and accuracy of medication persistence identified by patient self-report vs pharmacy fill: a secondary analysis of the cluster randomized artemis trial. JAMA Cardiol. 5 (5), 532–539. doi:10.1001/jamacardio.2020.0125
Franchi, F., and Rollini, F. (2022). Patterns and outcomes of dual antiplatelet therapy discontinuation after percutaneous coronary intervention. JACC Cardiovasc Interv. 15 (8), 807–809. doi:10.1016/j.jcin.2022.02.048
Gellad, W. F., Thorpe, C. T., Steiner, J. F., and Voils, C. I. (2017). The myths of medication adherence. Pharmacoepidemiol Drug Saf. 26 (12), 1437–1441. doi:10.1002/pds.4334
Golder, S., Weissenbacher, D., O'Connor, K., Hennessy, S., Gross, R., and Hernandez, G. G. (2022). Patient-reported reasons for switching or discontinuing statin therapy: a mixed methods study using social media. Drug Saf. 45 (9), 971–981. doi:10.1007/s40264-022-01212-0
Gu, G., Zhou, Y., Zhang, Y., and Cui, W. (2016). Increased prevalence of anxiety and depression symptoms in patients with coronary artery disease before and after percutaneous coronary intervention treatment. BMC Psychiatry 16, 259. doi:10.1186/s12888-016-0972-9
Halili, A., Holt, A., Eroglu, T. E., Haxha, S., Zareini, B., Torp-Pedersen, C., et al. (2023). The effect of discontinuing beta-blockers after different treatment durations following acute myocardial infarction in optimally treated, stable patients without heart failure: a Danish, nationwide cohort study. Eur. Heart J. Cardiovasc Pharmacother. 9 (6), 553–561. doi:10.1093/ehjcvp/pvad046
Harris, D. E., Lacey, A., Akbari, A., Obaid, D. R., Smith, D. A., Jenkins, G. H., et al. (2019). Early discontinuation of P2Y(12) antagonists and adverse clinical events post-percutaneous coronary intervention: a hospital and primary care linked cohort. J. Am. Heart Assoc. 8 (21), e012812. doi:10.1161/JAHA.119.012812
Henein, M. Y., Vancheri, S., Longo, G., and Vancheri, F. (2022). The impact of mental stress on cardiovascular health—Part II. J. Clin. Med. 11 (15), 4405. doi:10.3390/jcm11154405
Ho, P. M., Bryson, C. L., and Rumsfeld, J. S. (2009). Medication adherence: its importance in cardiovascular outcomes. Circulation 119 (23), 3028–3035. doi:10.1161/CIRCULATIONAHA.108.768986
Ho, P. M., O'Donnell, C. I., McCreight, M., Bavry, A. A., Bosworth, H. B., Girotra, S., et al. (2022). Multifaceted intervention to improve P2Y12 inhibitor adherence after percutaneous coronary intervention: a stepped wedge trial. J. Am. Heart Assoc. 11 (13), e024342. doi:10.1161/JAHA.121.024342
Hoole, S. P., and Bambrough, P. (2020). Recent advances in percutaneous coronary intervention. Heart 106 (18), 1380–1386. doi:10.1136/heartjnl-2019-315707
Kinlay, S., Young, M. M., Sherrod, R., and Gagnon, D. R. (2023). Long-term outcomes and duration of dual antiplatelet therapy after coronary intervention with second-generation drug-eluting stents: the veterans affairs extended DAPT study. J. Am. Heart Assoc. 12 (2), e027055. doi:10.1161/JAHA.122.027055
Kronish, I. M., Cornelius, T., Schwartz, J. E., Shechter, A., Diaz, K. M., Romero, E. K., et al. (2020). Posttraumatic stress disorder and electronically measured medication adherence after suspected acute coronary syndromes. Circulation 142 (8), 817–819. doi:10.1161/CIRCULATIONAHA.120.045714
Kronish, I. M., Thorpe, C. T., and Voils, C. I. (2021). Measuring the multiple domains of medication nonadherence: findings from a Delphi survey of adherence experts. Transl. Behav. Med. 11 (1), 104–113. doi:10.1093/tbm/ibz133
Lauffenburger, J. C., Fontanet, C. P., Isaac, T., Gopalakrishnan, C., Sequist, T. D., Gagne, J. J., et al. (2020). Comparison of a new 3-item self-reported measure of adherence to medication with pharmacy claims data in patients with cardiometabolic disease. Am. Heart J. 228, 36–43. doi:10.1016/j.ahj.2020.06.012
Lee, K., Han, S., Lee, M., Kim, D. W., Kwon, J., Park, G. M., et al. (2023). Evidence-based optimal medical therapy and mortality in patients with acute myocardial infarction after percutaneous coronary intervention. J. Am. Heart Assoc. 12 (10), e024370. doi:10.1161/JAHA.121.024370
Murad, H., Basheikh, M., Zayed, M., Albeladi, R., and Alsayed, Y. (2022). The association between medication non-adherence and early and late readmission rates for patients with acute coronary syndrome. Int. J. Gen. Med. 15, 6791–6799. doi:10.2147/IJGM.S376926
Narisawa, T., Nishi, D., Okubo, R., Noguchi, H., Hamazaki, K., Yamashita, A., et al. (2021). Impact of peritraumatic distress on posttraumatic stress disorder symptoms at 6 months after acute coronary syndrome: a prospective cohort study. Eur. J. Psychotraumatol 12 (1), 1854511. doi:10.1080/20008198.2020.1854511
Ofori-Asenso, R., Ilomaki, J., Tacey, M., Zomer, E., Curtis, A. J., Si, S., et al. (2018). Switching, discontinuation, and reinitiation of statins among older adults. J. Am. Coll. Cardiol. 72 (21), 2675–2677. doi:10.1016/j.jacc.2018.08.2191
Park, J. S., Seo, K. W., Choi, S. Y., Yoon, M. H., Hwang, G. S., Tahk, S. J., et al. (2023). Sustained beneficial effect of β-blockers on clinical outcomes after discontinuation in patients with ST elevation myocardial infarction. Medicine 102 (37), e35187. doi:10.1097/MD.0000000000035187
Pietrzykowski, Ł., Michalski, P., Kosobucka, A., Kasprzak, M., Fabiszak, T., Stolarek, W., et al. (2020). Medication adherence and its determinants in patients after myocardial infarction. Sci. Rep. 10 (1), 12028. doi:10.1038/s41598-020-68915-1
Princip, M., Ledermann, K., and von Kanel, R. (2023). Posttraumatic stress disorder as a consequence of acute cardiovascular disease. Curr. Cardiol. Rep. 25 (6), 455–465. doi:10.1007/s11886-023-01870-1
Redfors, B., Kirtane, A. J., Liu, M., Musikantow, D. R., Witzenbichler, B., Rinaldi, M. J., et al. (2022). Dual antiplatelet therapy discontinuation, platelet reactivity, and adverse outcomes after successful percutaneous coronary intervention. JACC Cardiovasc Interv. 15 (8), 797–806. doi:10.1016/j.jcin.2022.01.300
Simon, S. T., Kini, V., Levy, A. E., and Ho, P. M. (2021). Medication adherence in cardiovascular medicine. BMJ 374, n1493. doi:10.1136/bmj.n1493
Sorrentino, S., Sartori, S., Baber, U., Claessen, B. E., Giustino, G., Chandrasekhar, J., et al. (2020). Bleeding risk, dual antiplatelet therapy cessation, and adverse events after percutaneous coronary intervention: the PARIS registry. Circ. Cardiovasc Interv. 13 (4), e008226. doi:10.1161/CIRCINTERVENTIONS.119.008226
Vilchinsky, N., Ginzburg, K., Fait, K., and Foa, E. B. (2017). Cardiac-disease-induced PTSD (CDI-PTSD): a systematic review. Clin. Psychol. Rev. 55, 92–106. doi:10.1016/j.cpr.2017.04.009
von Känel, R., Meister-Langraf, R. E., Barth, J., Znoj, H., Schmid, J.-P., Schnyder, U., et al. (2022). Early trauma-focused counseling for the prevention of acute coronary syndrome-induced posttraumatic stress: social and health care resources matter. J. Clin. Med. 11 (7), 1993. doi:10.3390/jcm11071993
Vrijens, B., De Geest, S., Hughes, D. A., Przemyslaw, K., Demonceau, J., Ruppar, T., et al. (2012). A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 73 (5), 691–705. doi:10.1111/j.1365-2125.2012.04167.x
Vulcanescu, D., Gheorman, V., Pirvu, D. C., Dinescu, V. C., Gheorman, V., Udristoiu, I., et al. (2023). Primary PCI and mental health: a 12-month follow-up study. Healthc. (Basel) 11 (11), 1620. doi:10.3390/healthcare11111620
Wawruch, M., Murin, J., Tesar, T., Petrova, M., Paduchova, M., Celovska, D., et al. (2023). Reinitiation and subsequent discontinuation of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers among new and prevalent users aged 65 Years or more with peripheral arterial disease. Biomedicines 11 (2), 368. doi:10.3390/biomedicines11020368
West, L. M., Borg Theuma, R., and Cordina, M. (2020). The 'Necessity-Concerns Framework' as a means of understanding non-adherence by applying polynomial regression in three chronic conditions. Chronic Illn. 16 (4), 253–265. doi:10.1177/1742395318799847
Williams, B. A., Riangwiwat, T., Voyce, S., and Blankenship, J. C. (2021). Burden and predictors of chest pain-related health-care utilization following percutaneous coronary intervention. Am. J. Cardiol. 160, 31–39. doi:10.1016/j.amjcard.2021.07.051
Writing Committee, M., Lawton, J. S., Tamis-Holland, J. E., Bangalore, S., Bates, E. R., Beckie, T. M., et al. (2022). 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J. Am. Coll. Cardiol. 79 (2), e21–e129. doi:10.1016/j.jacc.2021.09.006
Xie, J. X., Gunzburger, E. C., Kaun, L., Plomondon, M. E., Baron, A. E., Waldo, S. W., et al. (2019). Medical therapy utilization and long-term outcomes following percutaneous coronary intervention: five-year results from the veterans affairs clinical assessment, reporting, and tracking system program. Circ. Cardiovasc Qual. Outcomes 12 (11), e005455. doi:10.1161/CIRCOUTCOMES.118.005455
Xu, H.-Y., Yu, Y.-J., Zhang, Q.-H., Hu, H.-Y., and Li, M. (2020). Tailored interventions to improve medication adherence for cardiovascular diseases. Front. Pharmacol. 11, 510339. doi:10.3389/fphar.2020.510339
Yamamoto, K., Morimoto, T., Natsuaki, M., Shiomi, H., Ogita, M., Tada, T., et al. (2023). Statin discontinuation after coronary revascularization. Am. J. Cardiol. 207, 479–489. doi:10.1016/j.amjcard.2023.09.047
Zhang, J., Hao, J. Y., Jing, R., Liu, J. J., Di, C. Y., Lu, Y. J., et al. (2021). Current trends in optimal medical therapy after PCI and its influence on clinical outcomes in China. BMC Cardiovasc Disord. 21 (1), 258. doi:10.1186/s12872-021-02052-z
Zhang, L., Wang, W., Man, F., Pan, Q., and Guo, L. (2023). The effect of statin adherence on patients with type 2 diabetes after percutaneous coronary intervention for acute coronary syndrome. Cardiovasc Drugs Ther. 37 (3), 539–547. doi:10.1007/s10557-021-07260-5
Keywords: medication adherence, discontinuation, percutaneous coronary intervention, major adverse cardiovascular events, medication adherence intervention
Citation: Xu H, Zheng W, Tan J and Li M (2024) Temporal characteristics and associated factors of discontinuation and outcomes after percutaneous coronary intervention. Front. Pharmacol. 15:1355231. doi: 10.3389/fphar.2024.1355231
Received: 15 December 2023; Accepted: 20 March 2024;
Published: 09 April 2024.
Edited by:
Tomoya Tachi, Nagoya City University, JapanReviewed by:
Akhmetzhan Galimzhanov, Semey State Medical University, KazakhstanCopyright © 2024 Xu, Zheng, Tan and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Li, bGltaW41MjI2N0B0bW11LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.