 Paul Laffont-Lozes1
Paul Laffont-Lozes1 Tayma Naciri2
Tayma Naciri2 Alix Pantel3,4Aurélie Martin2Anne-Sophie Pruvot-Occean5Vincent Haignere6
Alix Pantel3,4Aurélie Martin2Anne-Sophie Pruvot-Occean5Vincent Haignere6 Paul Loubet2,4
Paul Loubet2,4 Albert Sotto2,4
Albert Sotto2,4 Romaric Larcher2,7*†
Romaric Larcher2,7*†- 1Department of Pharmacy, Nimes University Hospital, Nîmes, France
- 2Department of Infectious and Tropical Diseases, Nimes University Hospital, Nîmes, France
- 3Department of Microbiology and Hospital Hygiene, Nimes University Hospital, Nîmes France
- 4VBIC (Bacterial Virulence and Chronic Infection), INSERM (French Institute of Health and Medical Research), Montpellier University, Montpellier, France
- 5Department of Neurosurgery, Nimes University Hospital, Nîmes, France
- 6Department of Orthopaedic Surgery and Traumatology, Nimes University Hospital, Nîmes, France
- 7PhyMedExp (Physiology and Experimental Medicine), INSERM (French Institute of Health and Medical Research), CNRS (French National Centre for Scientific Research), University of Montpellier, Montpellier, France
Introduction: Bone and joint infections (BJIs) caused by multidrug-resistant bacteria are becoming more frequent. However, data on the use of novel β-lactam/β-lactamase inhibitors, such as imipenem/cilastatin/relebactam (I-R) and meropenem/vaborbactam (MVB), to treat BJIs is lacking. Furthermore, prolonged infusions of these β-lactams should theoretically optimize pharmacokinetic/pharmacodynamics target in these indications, but there are currently no reports on this type of infusions, especially in the setting of BJI.
Case Presentation: We report a case of a vertebral osteomyelitis caused by carbapenem-resistant Enterobacter cloacae successfully treated with extended-infusion of I-R (1.25 g q6h over 2 h), then with continuous infusion of MVB (2 g q4h as over 4 h). Therapeutic drug monitoring confirmed that extended-infusion of I-R and continuous infusion of MVB achieved serum concentrations up to 12 mg/L of imipenem and 19 mg/L of meropenem, respectively.
Conclusion: The favourable outcome of this patient treated for a vertebral osteomyelitis caused by carbapenem-resistant E. cloacae suggest that extended- and continuous infusions of I-R and MVB, are promising regimens for treatment of BJIs caused by carbapenem-resistant Enterobacterales.
1 Introduction
The incidence of multidrug resistance (MDR) is increasing worldwide, leading to higher mortality and longer hospital stays (Murray et al., 2022). In response to this issue, new antimicrobials have recently been developed. Novel β-lactam/β-lactamase inhibitors are now the first treatment option for carbapenem-resistant Gram-negative bacteria (Tamma et al., 2022). Meropenem/vaborbactam (MVB) and imipenem/cilastatin/relebactam (I-R) are antimicrobials combining a carbapenem and a new β-lactamase inhibitor active against carbapenemase. They are approved by the European Medicines Agency and/or the US Food and Drug Administration (Summary of product characteristics: Vaborem, 2018; Summary of product characteristics: Recarbrio, 2020), for the treatment of bacteraemia, hospital-acquired pneumonia including ventilator associated pneumonia, complicated urinary tract infection and complicated intra-abdominal infection. However, the use of these molecules in more complex infections such as bone and joint infections (BJIs) has not been studied.
Data on the use of these novel antimicrobials for treating BJIs are needed, as they represent a promising therapeutic option for managing BJIs caused by MDR bacteria, which are an increasing concern (Rebold et al., 2021; Rempenault et al., 2021; Larcher et al., 2022; Davido et al., 2023). In addition, previous data (Roberts et al., 2016; Rebold et al., 2021; Larcher et al., 2022; Le Vavasseur and Zeller, 2022) have suggested that it could be interesting to use these new β-lactams in prolonged or continuous infusion, to improve pharmacokinetic, bacteriological eradication and clinical success in BJIs caused by carbapenem-resistant Enterobacterales.
We aimed to report the first case of vertebral osteomyelitis caused by carbapenem-resistant Enterobacter cloacae successfully treated with extended infusion of I-R then continuous infusion of MVB. This case provides important data on using novel antimicrobials for BJIs and offers insights into their optimized administration for effective management.
2 Case description
In November 2022, a 77-year-old man, weighing 78 kg, was admitted to a French tertiary hospital for opiate-resistant back pain. He had a medical history of hypertension, Parkinson’s disease and atrial fibrillation. Two months prior, he had also been treated with ofloxacin for 21 days, for prostatitis caused by extended spectrum beta-lactamase (ESBL) producing-E. cloacae. On admission to the emergency room, a neutrophil count of 8.3 G/L (N = 1.5–7 G/L) and C reactive protein (CRP) level at 87.5 mg/L (N < 0.5 mg/L) prompted the physicians to perform a lumbar magnetic resonance imaging (MRI). A T11-T12 vertebral osteomyelitis with a significant infiltration of the surrounding soft tissues and an epiduritis was found (Figure 1). The patient was admitted to the infectious disease department and a couple of days later, ertapenem 1 g q12 h was started when blood cultures flagged positive for Gram-negative bacilli. An ESBL-producing-E. cloacae (Table 1) was identified. After 8 days of ertapenem therapy, the patient still had fever and CRP level remained at a plateau of 70 mg/L. Blood cultures drawn at this point were positive for carbapenem-resistant E. cloacae (Table 1). No carbapenemase enzyme was found (Xpert® Carba-R test, Cepheid, CA, United States and β CARBA test®, Bio-Rad, CA,USA) and resistance to ertapenem was explained by a combination of impermeability with ESBL and AmpC-beta-lactamase. Extended-infusion meropenem 2 g q8h over 3 h was started according to the 2022 Infectious Diseases Society of America (IDSA) guidelines (Tamma et al., 2022) for infections caused by non-carbapenemase producing carbapenem-resistant Enterobacterales (non-CP-CRE) resistant to ertapenem, that remain susceptible to meropenem (Table 1). On the first day of treatment, a single dose of amikacin (30 mg/kg) was also administered. Blood cultures were negative after 5 days of treatment. However, back pain and fever persisted, the patient became disoriented, and CRP level rose to 99 mg/L. Clinical failure and drug neurotoxicity related to the use of a high dose of meropenem despite reduced renal clearance (estimated glomerular filtration rate, eGFR, at around 40 mL/min/1.73 m2 at this point) were suspected. Therefore, we decided to change the antibiotic therapy.

Figure 1. Medullar magnetic resonance imaging: Decreased height and STIR hypersignal of disc (white arrow) with irregularity and erosion of T11-T12 vertebral body endplates (white dotted arrow), and epidural collections (white dashed arrow).

Table 1. Antibiotic susceptibility testing (AST) of Enterobacter cloacae isolates.
Among the available therapeutic options tested, only the novel β-lactam-β-lactamase inhibitor agents, namely, ceftazidime/avibactam (CZA), I-R and MVB remained active against the carbapenem-resistant E. cloacae strain (Table 1). On the one hand, given the presumed toxicity of meropenem, we initially decided not to use MVB. On the other hand, I-R had the lowest minimum inhibitory concentration (MIC), at 0.06 mg/L, more than four times lower than the MIC of meropenem (0.25 mg/L) and eight time lower than the MIC of CZA (0.5 mg/L), see Table 1. A treatment with I-R was therefore administered at 1.25 g (i.e. 500 mg of imipenem, 500 mg of cilastatin and 250 mg of relebactam) as a 2 h infusion every 8 h. As the renal function improved (eGFR = 65 mL/min) we performed a therapeutic drug monitoring (TDM) of imipenem 7 days after I-R initiation. Blood samples for imipenem plasma concentration measurement were collected 15–30 min prior to the start of the subsequent infusion (trough or Cmin levels), then imipenem concentration were assessed utilizing an ultra-high performance liquid chromatography technique combined with high-resolution mass spectrometry as previously described (Bouglé et al., 2019). Plasma trough concentration were at 0.4 mg/L (Figure 2; Table 2). We then increased the I-R dose at 1.25 g q6h over 2 h, which allowed plasma through concentration of imipenem to reach 12 mg/L at day 12 (Figure 2; Table 2). The patient was afebrile, and the CRP level decreased to 37 mg/L. He was discharged to a rehabilitation centre.
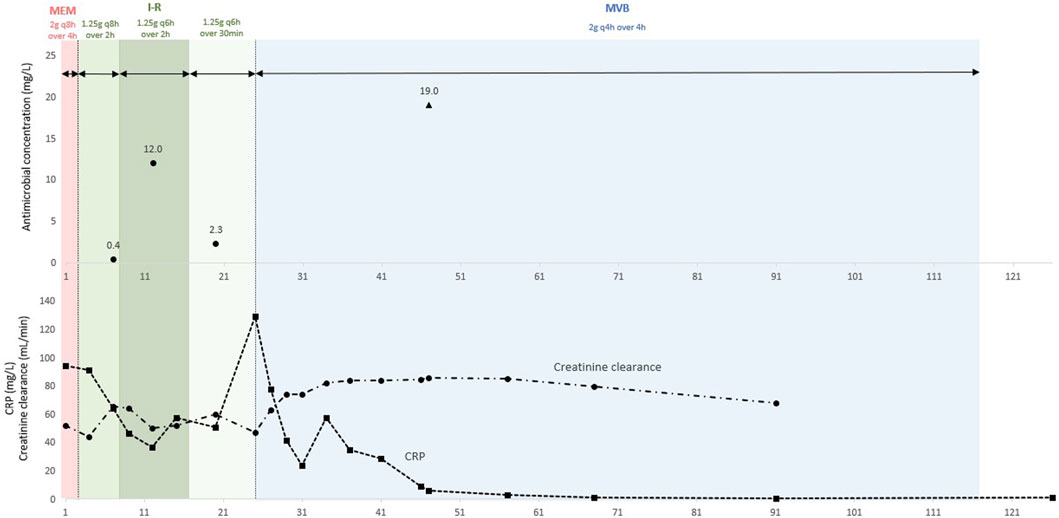
Figure 2. Therapeutic drug monitoring of imipenem and meropenem plasma concentrations in the patient. Imipenem through concentrations are represented by black circles and meropenem steady-state concentrations are represented by black triangles. Creatinine clearance is represented by black circles and dotted line, and C-reactive protein (CRP) is represented by black squares and dotted line.
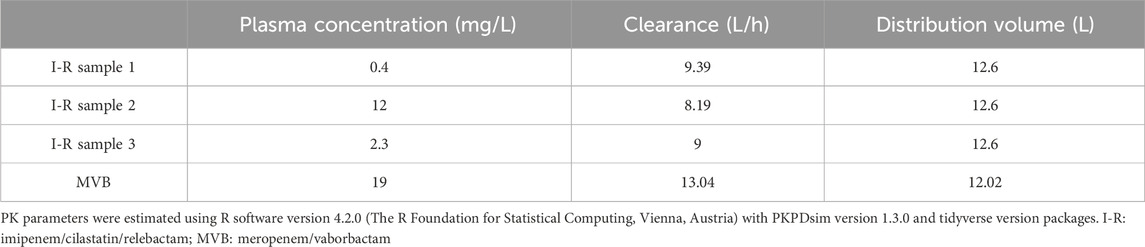
Table 2. Pharmacokinetic models parameter estimates.
During his stay in the rehabilitation centre, I-R dosing regimen was changed in 1.25 g as a 30 min infusion every 6 h and the TDM performed at day 20 days found an imipenem plasma through concentration of 2.3 mg/L (Figure 2; Table 2). At day 25, as the patient experienced a relapse in thoracic back pain, and CRP levels rose to 130 mg/L, he was readmitted to the infectious diseases department (Figure 2). A new spinal CT-scan showed severe osteolysis of T11-T12 with a significant posterior wall recession, resulting in a 60% central canal stenosis. At this time, we discussed two antimicrobial strategies: restarting the extended-infusion I-R over 2 h or modifying the treatment in favor of continuous infusion of MVB. As the patient renal function continued to improve (eGFR = 85 mL/min), we selected MVB 2 g (meropenem 1 g and vaborbactam 1 g) q4h as a 4-h infusion, resulting in a continuous infusion of 12 g/day of MVB. Surgical laminectomy of T11-T12 and percutaneous osteosynthesis of T9-T10 and L1-L2 were performed on day 36, to relieve central canal stenosis responsible for the pain the patient. No surgical debridement could be performed due to the spinal instability caused by the extensive osteolysis of T11-12 and no orthopaedic hardware was implanted in T11-T12 to limit the risk of bacterial biofilm formation on such implants, which would hinder antimicrobial therapy. Microbiological cultures of the biopsies of the affected bone and intervertebral disc were sterile. Pain gradually decreased after the surgery. At day 47, 20 days after MVB initiation, CRP levels were at 6 mg/L. At the time, plasma concentration of meropenem was measured at 19 mg/L (Figure 2; Table 2), in a blood sample collected at steady-state using high-performance liquid chromatography coupled with Ultraviolet Detection as previously described (Larcher et al., 2023). Importantly, no sign of clinical or biological toxicity was evidenced during I-R or MVB treatment course. At day 50, the patient was afebrile with normal CRP levels and was discharged to a rehabilitation centre. One month after an antibiotic course of 90 days, the clinical outcome was favourable, and the CRP decreased to 0.5 mg/L (Figure 2).
3 Discussion
To the best of our knowledge, this is the first case of successful treatment of a vertebral osteomyelitis caused by carbapenem-resistant E. cloacae with continuous infusion of MVB at 2 g q4h as a 4-h infusion in a patient with normal renal clearance. This dosing regimen achieved plasma steady-state concentrations of meropenem up to 19 mg/L. In addition, our data also suggest the feasibility of extended-infusion of I-R as 1.25 g q6h over 2 h to achieve plasma through concentration of imipenem up to 12 mg/L. There were no adverse effects associated to prolonged treatment with I-R and MVB.
The treatment strategies reported herein were based on limited evidence. Few cases reported successful treatment of BJIs with novel antibiotics such as CZA (Rempenault et al., 2021; Davido et al., 2023) and I-R (Rebold et al., 2021; Larcher et al., 2022). Data on bone diffusion of ceftazidime, meropenem, and imipenem encourage their use in BJI treatments (Landersdorfer et al., 2009; Thabit et al., 2019), but no data on beta-lactamase inhibitors diffusion in bones and joints are available. However, β-lactamase inhibitors appear to have the same pharmacokinetics as the beta-lactam with which they are associated (Nicolau et al., 2015; Wenzler et al., 2017; Rizk et al., 2018) suggesting novel β-lactam/β-lactamase inhibitors could be used in treatment of BJIs. Additionally, these new antimicrobials offer the advantage of being less nephrotoxic compared to treatment regimens based on colistin (Wunderink et al., 2018; Brown et al., 2020). Recent data indicate that while colistin monotherapy for treating BJIs caused by MDR bacteria is associated with high toxicity and mortality rates, these rates are even higher when colistin is combined with fosfomycin (Katip et al., 2024). This highlights the challenges of managing colistin and underscores the urgent need to explore more effective and less toxic alternatives, such as I-R and MVB.
As β-lactams and β-lactamase inhibitors displays mainly time-dependent killing, either extended or continuous infusion are recognized options for optimizing the time during which the antimicrobials concentration is maintained above the MIC of the treated bacteria (Abdul-Aziz et al., 2020). Optimized administrations of antimicrobial aim to improve microbiological and clinical outcome in the setting of severe diseases caused by difficult to treat bacteria (Roberts et al., 2016; Abdul-Aziz et al., 2020; Le Vavasseur and Zeller, 2022). However, few data have been published on MVB administration by continuous infusion (Larcher et al., 2023) and none on the use of I-R extended infusion. This case report therefore represents the first data available in the literature, especially in the setting of BJIs.
To improve the safety and the efficiency of off-label use of I-R and MVB in extended or prolonged infusion, we complied with the product stabilities recommended by the manufacturers (2 h for I-R and 6 h for MVB) (Summary of product characteristics: Vaborem, 2018; Summary of product characteristics: Recarbrio, 2020), and carried out therapeutic monitoring of plasma concentrations of imipenem and meropenem using a high performance liquid chromatography method (Larcher et al., 2023). We report optimized dosing regimens of I-R and MVB that achieved plasma concentrations above the MIC of most susceptible pathogens throughout the whole dosing interval (and more than 100%ƒT>4xMIC for many pathogens) (Abdul-Aziz et al., 2020). These dosing regimens enable sufficiently high plasma concentrations to be achieved, making it possible to treat infections at sites where antibiotic distribution is limited, such as BJIs (Landersdorfer et al., 2009; Thabit et al., 2019). It should be noted that surgical debridement plays an important part in achieving clinical cure, in addition to antimicrobials, especially in case of MDR bacteria, in order to reduce bacterial inoculum (Papadopoulos et al., 2019). However, in our case, surgical intervention was necessary due to spinal instability. The surgery was not specifically intended to control the source of infection but rather for mechanical reasons, as the infection was considered controlled prior to the intervention. It is also important to note that the surgical bone biopsy was negative in culture, which provides further evidence of the microbiological effectiveness of the treatments used in this case report.
Our work has limitations. First, this is a single case report, and larger-scale studies are needed to confirm our results. Second, TDM of I-R and MVB was based solely on the plasma concentration of beta-lactams (namely, imipenem and meropenem). However, as beta-lactamase inhibitors have the same pharmacokinetics as the beta-lactam with which they are associated (Nicolau et al., 2015; Wenzler et al., 2017; Rizk et al., 2018), the plasma concentration of the later can be used as a surrogate. Nonetheless, we did not obtain I-R and MVB concentrations in bone biopsies to confirm the diffusion of these new antibiotics in the affected bone, which would have been the preferred method of TDM. Last, TDM of beta-lactam is not performed every day in our hospital, and due to this fact, we were unable to confirm the meropenem overdose suspected at the beginning of the patient care.
Despite the limitations inherent to the level of evidence provided by case reports, we believe that documenting novel treatment strategies (Tamma et al., 2022) is urgently needed to address the growing challenge of antimicrobial resistance (Murray et al., 2022). This case report, in particular, illustrates how healthcare professionals, through interdisciplinary collaboration, can pave the way for novel therapeutic approaches and propose innovative solutions for managing the most challenging infections caused by MDR bacteria. Nonetheless, it remains necessary to validate these strategies on a larger scale through well-conducted clinical studies, ideally randomized controlled trials.
In conclusion, the case reported here suggest that I-R extended infusion and MVB continuous infusion are promising options for treatment of BJI caused by non-CP-CRE and CPE, provided that susceptibility to these agents is confirmed by antibiotic susceptibility testing. Further studies are essential to assess the pharmacokinetics of these β-lactam-β-lactamase inhibitor associations in BJIs. Notably, data on simultaneous measurements of β-lactam and β-lactamase inhibitor concentrations in both plasma and bone, using various administration strategies, particularly extended or continuous infusions, are needed. Additionally, clinical studies are required to validate the use of I-R and MVB for treating BJIs caused by MDR bacteria and to confirm that protocols derived from pharmacokinetic studies are effective and safe in such indications.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
PL-L: Writing–original draft, Writing–review and editing. TN: Writing–review and editing. AP: Writing–review and editing. AM: Writing–review and editing. A-SP-O: Writing–review and editing. VH: Writing–review and editing. PL: Supervision, Validation, Writing–review and editing. AS: Supervision, Validation, Writing–review and editing. RL: Methodology, Supervision, Validation, Writing–original draft, Writing–review and editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abdul-Aziz, M. H., Alffenaar, J.-W. C., Bassetti, M., Bracht, H., Dimopoulos, G., Marriott, D., et al. (2020). Antimicrobial therapeutic drug monitoring in critically ill adult patients: a Position Paper<sub/>. Intensive Care Med. 46, 1127–1153. doi:10.1007/s00134-020-06050-1
Bouglé, A., Dujardin, O., Lepère, V., Ait Hamou, N., Vidal, C., Lebreton, G., et al. (2019). PHARMECMO: therapeutic drug monitoring and adequacy of current dosing regimens of antibiotics in patients on Extracorporeal Life Support. Anaesth. Crit. Care and Pain Med. 38, 493–497. doi:10.1016/j.accpm.2019.02.015
Brown, M. L., Motsch, J., Kaye, K. S., File, T. M., Boucher, H. W., Vendetti, N., et al. (2020). Evaluation of renal safety between imipenem/relebactam and colistin plus imipenem in patients with imipenem-nonsusceptible bacterial infections in the randomized, phase 3 RESTORE-IMI 1 study. Open Forum Infect. Dis. 7, ofaa054. doi:10.1093/ofid/ofaa054
Davido, B., Crémieux, A.-C., Vaugier, I., Gatin, L., Noussair, L., Massias, L., et al. (2023). Efficacy of ceftazidime-avibactam in various combinations for the treatment of experimental osteomyelitis due to Klebsiella pneumoniae carbapenemase (KPC)-producing Klebsiella pneumoniae. Int. J. Antimicrob. Agents 61, 106702. doi:10.1016/j.ijantimicag.2022.106702
Katip, W., Rayanakorn, A., Oberdorfer, P., Taruangsri, P., Nampuan, T., and Okonogi, S. (2024). Comparative effectiveness and mortality of colistin monotherapy versus colistin-fosfomycin combination therapy for the treatment of carbapenem-resistant Enterobacteriaceae (CRE) infections: a propensity score analysis. J. Infect. Public Health 17, 727–734. doi:10.1016/j.jiph.2024.03.010
Landersdorfer, C. B., Bulitta, J. B., Kinzig, M., Holzgrabe, U., and Sörgel, F. (2009). Penetration of antibacterials into bone: pharmacokinetic, pharmacodynamic and bioanalytical considerations. Clin. Pharmacokinet. 48, 89–124. doi:10.2165/00003088-200948020-00002
Larcher, R., Laffont-Lozes, P., Naciri, T., Bourgeois, P.-M., Gandon, C., Magnan, C., et al. (2023). Continuous infusion of meropenem–vaborbactam for a KPC-3-producing Klebsiella pneumoniae bloodstream infection in a critically ill patient with augmented renal clearance. Infection 51, 1835–1840. doi:10.1007/s15010-023-02055-2
Larcher, R., Laffont-Lozes, P., Roger, C., Doncesco, R., Groul-Viaud, C., Martin, A., et al. (2022). Last resort beta-lactam antibiotics for treatment of New-Delhi Metallo-Beta-Lactamase producing Enterobacterales and other Difficult-to-Treat Resistance in Gram-negative bacteria: a real-life study. Front. Cell. Infect. Microbiol. 12, 1048633. doi:10.3389/fcimb.2022.1048633
Le Vavasseur, B., and Zeller, V. (2022). Antibiotic therapy for prosthetic joint infections: an overview. Antibiotics 11, 486. doi:10.3390/antibiotics11040486
Murray, C. J., Ikuta, K. S., Sharara, F., Swetschinski, L., Robles Aguilar, G., Gray, A., et al. (2022). Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 399, 629–655. doi:10.1016/S0140-6736(21)02724-0
Nicolau, D. P., Siew, L., Armstrong, J., Li, J., Edeki, T., Learoyd, M., et al. (2015). Phase 1 study assessing the steady-state concentration of ceftazidime and avibactam in plasma and epithelial lining fluid following two dosing regimens. J. Antimicrob. Chemother. 70, 2862–2869. doi:10.1093/jac/dkv170
Papadopoulos, A., Ribera, A., Mavrogenis, A. F., Rodriguez-Pardo, D., Bonnet, E., Salles, M. J., et al. (2019). Multidrug-resistant and extensively drug-resistant Gram-negative prosthetic joint infections: role of surgery and impact of colistin administration. Int. J. Antimicrob. Agents 53, 294–301. doi:10.1016/j.ijantimicag.2018.10.018
Rebold, N., Morrisette, T., Lagnf, A. M., Alosaimy, S., Holger, D., Barber, K., et al. (2021). Early multicenter experience with imipenem-cilastatin-relebactam for multidrug-resistant gram-negative infections. Open Forum Infect. Dis. 8, ofab554. doi:10.1093/ofid/ofab554
Recarbrio (2020). Summary of product characteristics: Recarbrio. Available at: https://www.ema.europa.eu/en/documents/product-information/recarbrio-epar-product-information_en.pdf (Accessed May 28, 2023).
Rempenault, C., Pagis, V., Noussair, L., Berbescu, S., Duran, C., Bouchand, F., et al. (2021). Treatment of bone and joint infections by ceftazidime/avibactam and ceftolozane/tazobactam: a cohort study. J. Glob. Antimicrob. Resist. 25, 282–286. doi:10.1016/j.jgar.2021.04.003
Rizk, M. L., Rhee, E. G., Jumes, P. A., Gotfried, M. H., Zhao, T., Mangin, E., et al. (2018). Intrapulmonary pharmacokinetics of relebactam, a novel β-lactamase inhibitor, dosed in combination with imipenem-cilastatin in healthy subjects. Antimicrob. Agents Chemother. 62, e01411–e01417. doi:10.1128/aac.01411-17
Roberts, J. A., Abdul-Aziz, M.-H., Davis, J. S., Dulhunty, J. M., Cotta, M. O., Myburgh, J., et al. (2016). Continuous versus intermittent β-lactam infusion in severe sepsis. A meta-analysis of individual patient data from randomized trials. Am. J. Respir. Crit. Care Med. 194, 681–691. doi:10.1164/rccm.201601-0024OC
Tamma, P. D., Aitken, S. L., Bonomo, R. A., Mathers, A. J., van Duin, D., and Clancy, C. J. (2022). Infectious diseases society of America 2022 guidance on the treatment of extended-spectrum β-lactamase producing Enterobacterales (ESBL-E), carbapenem-resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 75, 187–212. doi:10.1093/cid/ciac268
Thabit, A. K., Fatani, D. F., Bamakhrama, M. S., Barnawi, O. A., Basudan, L. O., and Alhejaili, S. F. (2019). Antibiotic penetration into bone and joints: an updated review. Int. J. Infect. Dis. 81, 128–136. doi:10.1016/j.ijid.2019.02.005
Vaborem (2018). Summary of product characteristics: Vaborem. Available at: https://www.ema.europa.eu/en/documents/product-information/vaborem-epar-product-information_en.pdf (Accessed July 16, 2023).
Wenzler, E., Ellis-Grosse, E. J., and Rodvold, K. A. (2017). Pharmacokinetics, safety, and tolerability of single-dose intravenous (ZTI-01) and oral fosfomycin in healthy volunteers. Antimicrob. Agents Chemother. 61, 00775-17–e817. doi:10.1128/AAC.00775-17
Wunderink, R. G., Giamarellos-Bourboulis, E. J., Rahav, G., Mathers, A. J., Bassetti, M., Vazquez, J., et al. (2018). Effect and safety of meropenem–vaborbactam versus best-available therapy in patients with carbapenem-resistant enterobacteriaceae infections: the TANGO II randomized clinical trial. Infect. Dis. Ther. 7, 439–455. doi:10.1007/s40121-018-0214-1
Keywords: bone and joint infection, vertebral osteomyelitis, meropenem/vaborbactam, continuous infusion, imipenem/cilastatin/relebactam, extended infusion, therapeutic drug monitoring
Citation: Laffont-Lozes P, Naciri T, Pantel A, Martin A, Pruvot-Occean A-S, Haignere V, Loubet P, Sotto A and Larcher R (2024) First case report of a vertebral osteomyelitis caused by carbapenem-resistant Enterobacter cloacae treated with imipenem/cilastatin/relebactam prolonged infusion then meropenem/vaborbactam in continuous infusion. Front. Pharmacol. 15:1347306. doi: 10.3389/fphar.2024.1347306
Received: 30 November 2023; Accepted: 18 September 2024;
Published: 30 October 2024.
Edited by:
Mingkai Li, Air Force Medical University, ChinaReviewed by:
Zhihong Peng, Hubei University, ChinaMohamed Said, University of Pretoria, South Africa
Wasan Katip, Chiang Mai University, Thailand
Copyright © 2024 Laffont-Lozes, Naciri, Pantel, Martin, Pruvot-Occean, Haignere, Loubet, Sotto and Larcher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Romaric Larcher, cm9tYXJpYy5sYXJjaGVyQGNodS1uaW1lcy5mcg==
†ORCID: Romaric Larcher, orcid.org/0000-0002-7591-0901