
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 02 February 2024
Sec. Neuropharmacology
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1330589
 Shaohua Lyu1,2
Shaohua Lyu1,2 Claire Shuiqing Zhang2
Claire Shuiqing Zhang2 Anthony Lin Zhang2
Anthony Lin Zhang2 Xinfeng Guo1
Xinfeng Guo1 Rong Hua1
Rong Hua1 Zhenhui Mao1
Zhenhui Mao1 Qiaozhen Su1
Qiaozhen Su1 Charlie Changli Xue1,2*
Charlie Changli Xue1,2* Jingbo Sun1,3,4*
Jingbo Sun1,3,4*Background: Migraine is a prevalent, recurrent condition with substantial disease burden. Chinese herbal medicine (CHM) has been used frequently for migraine in controlled clinical settings. This study is to summarise the characteristics of patients who seek clinical care in a tertiary Chinese medicine hospital in China; to gather their preferences and values of using CHM; to explore the effect of CHM for migraine and its comorbidities in a real-world setting, and to collect first-hand expertise of clinicians’ practice pattern in prescribing CHM for migraine.
Methods: This registry-based cohort study was prospectively conducted at Guangdong Provincial Hospital of Chinese Medicine from December 2020 to May 2022. Adult migraine patients seeking their initial anti-migraine clinical care at the hospital were consecutively recruited and followed up for 12 weeks. Practitioners specialised in headache management prescribed individualised treatments without research interference. Standardised case report forms were employed to gather information on patients’ preferences and perspective of seeking clinical care, as well as to assess participants’ migraine severity, comorbidities, and quality of life, at 4-weeks intervals. Various analytical methods were utilised based on the computed data.
Results: In this study, we observed 248 participants. Of these, 73 received CHM treatment for 28 days or longer. Notably, these participants exhibited a greater disease severity, compared to those treated with CHM for less than 28 days. Of the 248 participants, 83.47% of them expected CHM would effectively reduce the severity of their migraine, around 50% expected effects for migraine-associated comorbidities, while 51.61% expressing concerns about potential side effects. CHM appeared to be effective in reducing monthly migraine days and pain intensity, improving patients’ quality of life, and potentially reducing comorbid anxiety, with a minimum of 28 days CHM treatment. Herbs such as gan cao, gui zhi, chuan xiong, fu ling, bai zhu, yan hu suo, etc. were frequently prescribed for migraine, based on patients’ specific symptoms.
Conclusion: CHM appeared to be beneficial for migraine and comorbid anxiety in real-world clinical practice when used continuously for 28 days or more.
Clinical Trial Registration: clinicaltrials.gov, identifier ChiCTR2000041003.
Migraine is a primary headache disorder characterised by recurrent, unilateral, pulsing or throbbing, moderate to severe headaches (Headache Classification Committee of the International Headache Society IHS, 2018). It is prevalent among 14% of global population (Stovner et al., 2022), and ranked as the second disabling condition with 42.1 million of global age-standardised years lived with disability (YLDs) (Safiri et al., 2022). Notably, females are more susceptible to migraine, and tend to report heightened migraine severity and associated disability (Pavlovic et al., 2017; Vetvik and MacGregor, 2017; Lipton et al., 2018). Additionally, migraine commonly coexists with anxiety, depression and insomnia (Kelman and Rains, 2005; Freedom and Evans, 2013; Buse et al., 2020; Caponnetto et al., 2021), and these comorbidities, in return, exacerbate the burden of migraine (Kelman, 2007; Walters et al., 2014; Seng et al., 2017; Buse et al., 2020; Klonowski et al., 2022) and predict a less favourable prognosis (Bigal and Lipton, 2006; Lipton et al., 2019a).
Migraine is conventionally managed by prophylactic medications to reduce the frequency and severity of migraine attacks, as well as acute medications for temporary relief of pain and associated symptoms (Evers et al., 2009; Pringsheim et al., 2012; Worthington et al., 2013; Orr et al., 2015; Scottish Intercollegiate Guidelines Network SIGN, 2018; Kouremenos et al., 2019; Kowacs et al., 2019; Ailani et al., 2021; Diener et al., 2022; Domitrz et al., 2022; Dong et al., 2022; Wu et al., 2022; The British Association for the study of headache BASH, 2023). However, lack of efficacy and undesirable side effects associated with the conventional pharmacotherapies were widely reported (Malik et al., 2006; Blumenfeld et al., 2013; Ford et al., 2017; Lipton et al., 2019b; Takeshima et al., 2019; Ueda et al., 2019; Lombard et al., 2020; Hirata et al., 2021; Kim et al., 2021). Inadequate treatment responses can lead to increased reliance on acute medications, while overuse of acute medications has emerged as a significant risk factor for migraine chronification (Xu et al., 2020). Effective patient education can potentially reverse the overuse of acute medications (Probyn et al., 2017). Investigation on patients’ preferences and values, especially the knowledge and behaviour regarding acute medication use, could form the basis for developing a customised patient education strategy.
Furthermore, due to the limitations of pharmacotherapies, migraine patients often seek complementary and alternative treatments, including Chinese herbal medicine (CHM), to complement their current treatment strategies (Wells et al., 2011; Rhee and Harris, 2018). In China, CHM is prescribed to over 60% of outpatient migraine cases according to a retrospective analysis of the China Health Insurance Research Association medical insurance claims database (Yu et al., 2020). Meta-analyses of randomised controlled trials (RCTs) have demonstrated the effectiveness of CHM for migraine in controlled settings (Zhou et al., 2013; Li et al., 2015; Lyu et al., 2020; Lyu et al., 2022a). However, this existing evidence has limitations in terms of generalisability because of the highly selective eligibility criteria, unified interventions, and predefined treatment duration in RCT designs. CHM therapies in RCTs with these constraints do not align with real-world Chinese medicine clinical practices. As revealed by our earlier real-world analysis based on medical records, migraine patients with varied comorbidities received individually tailored CHM prescriptions over varying treatment durations (Lyu et al., 2022b). Quantitative evaluation is needed to assess the real-world effects of CHM on migraine and its comorbidities, complementing the evidence from RCTs. Moreover, the distinct patient profiles encountered in real-world clinical practice, along with their preferences and values regarding treatments from a Chinese medicine hospital, have been insufficiently explored. Nonetheless, this information has the potential to provide valuable insights for informed medical decision-making in clinical practice.
In light of these considerations, a prospective registry-based cohort study was undertaken to bridge the gap between research evidence and real-world clinical practice, and to support evidence-based Chinese medicine practice in managing migraines (Lyu et al., 2022c). The present manuscript is to portray a real-world representation of patients’ clinical characteristics, their preferences and values, their utilisation of treatment, and their responses to CHM interventions within the context of the studied Chinese medicine hospital.
This registry-based cohort study was undertaken at the Headache Department of the Guangdong Provincial Hospital of Chinese Medicine (GPHCM), a tertiary hospital in southern China (Guangdong Provincial Hospital of Chinese Medicine, 2021). Participant recruitment and follow-up observations commenced in December 2020 and ended in May 2022.
The study was approved by the ethics committee of GPHCM (ZE 2020-243-01) and registered with the Human Research Ethics Committee of RMIT University (#24235). Conduction of the study complied with the Declaration of Helsinki, Ethical Guidelines for Medical Research on Humans (World Medical Association, 2013), and the reporting of this study abides by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cohort studies (von Elm et al., 2007).
Adult migraine patients seeking anti-migraine treatments in the studied Chinese medicine hospital for the first time were eligible for the study. Once patients were confirmed with a diagnosis of migraine according to the International Classification of Headache Disorders, third edition (ICHD-3) (Headache Classification Committee of the International Headache Society IHS, 2018), and were prescribed tailored treatments by headache specialists, they were invited to provide a written informed consent of participating in the study. A consecutive sampling method was applied to screen and recruit participants, as it is the best nonprobability sampling methods at controlling sampling bias (Polit and Beck, 2020). Migraine patients would be excluded for registration and participation if they were not capable of giving written informed consent or completing case report forms (CRFs).
Headache specialists prescribed individually tailored treatments to each participant, without additional interference from our research team. Participants would decide their treatment duration, with guidance from their headache specialists. Treatment details were later collected from participants’ medical records at completion of the 12-week observation period.
Case report form was utilised to collect data. The CRFs encompassed a set of standardised questions and several validated questionnaires, to collect the demographic and general information, patients’ preferences and values, migraine severity (including monthly migraine frequency, monthly migraine days, peak pain measured by numeric rating scale (NRS) and migraine duration), migraine comorbidities (anxiety assessed by generalised anxiety disorder 7-item (GAD-7), depression by patient health questionnaire-9 (PHQ-9) and insomnia by insomnia severity index (ISI)), and migraine-specific quality of life (MSQ, in domains of role function-restrictive (RFR), role function-preventive (RFP), and emotional function (EF)). More details can be referred to the published study protocol and, the Chinese Clinical Trial Registry (No. ChiCTR2000041003) (Lyu et al., 2022c).
Participants completed their CRFs with assistance of researchers during their initial evaluation, via either hardcopy or digital web link. Subsequent rounds of data collection occurred at week 4, week 8 and week 12. Scheduled reminders were sent to participants to enhance their compliance during the follow-up period. Participants were encouraged to maintain a digital migraine diary to document their migraine attacks throughout the observation period, which was then cross-referenced with data collected from their CRFs.
In this real-world cohort study, CHM treatment was predefined as the main exposure factor, and exposure levels were further measured by duration of CHM treatment. The participants were divided into two subgroups based on a cut-off duration of CHM treatment at 28 days, which is recommended as the least duration for migraine prophylaxis by clinical guidelines (Scottish Intercollegiate Guidelines Network SIGN, 2018; Dong et al., 2022):
• Subgroup A: CHM ≥28 days
• Subgroup B: CHM <28 days
In addition, comorbidities of migraine, along with gender, baseline severity of migraine, and aura, were predefined as confounders.
This registry-based cohort study aimed to gather and investigate the real-world data in terms of migraine management and was conducted within a specific timeframe using a migraine cohort from a tertiary hospital. Given that no pre-determined hypotheses were to be tested, the necessity for sample size calculation was obviated (Gliklich et al., 2014).
Data analyses were performed based on imputed dataset, which was dealt with ‘multiple imputation’ by SPSS in advance (IBM Corp, 2017). Continuous variables such as monthly migraine days were described with mean values and standard deviation, and compared between subgroups using t-test. While categorical variables, like gender, were presented as frequencies and percentages, and compared using chi square test. In addition, generalised linear mixed models (GLMM) were utilised to analyse repeated-measured outcomes. The GLMMs accommodate both normally and non-normally distributed dependent variables, allowing for the incorporation of covariates and factors. GLMMs with random effects were deemed appropriate to analyse repeated-measured, and longitudinal data from the same subjects (Cnaan et al., 1997; IBM, 2021). During conduction of GLMM analyses, continuous variables such as age, disease duration and the corresponding baseline assessment of the dependent variable, dichotomous variable of chronic migraine, and time-varying dichotomous variables of western medication usage for migraine prophylaxis and acute pain relief, were included as covariates.
A total of 248 migraine patients participated in this longitudinal observational study. Among them, 164 participants completed three follow-up assessments at Week 4, Week 8, and Week 12. However, 84 participants missed at least one follow-up evaluation due to personal reasons. Specifically, 206 participants completed assessment at week 4, 179 participants completed assessments at week 8, and 184 individuals completed it at week 12 (Figure 1). It is notably that participation or absence in one follow-up assessment did not determine their involvement status in subsequent assessments. All the 248 participants were included for analyses based on an imputed dataset.
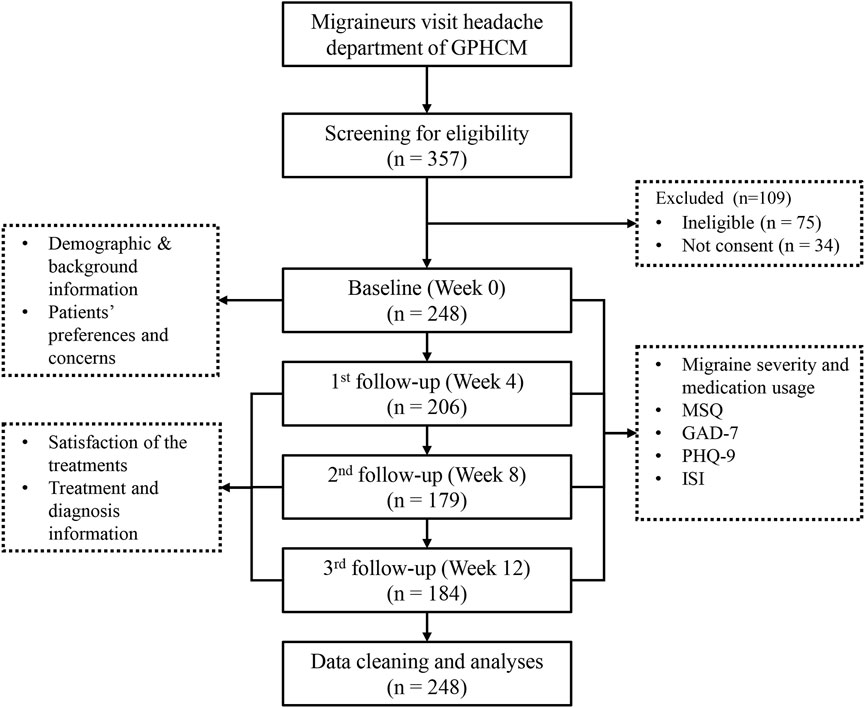
FIGURE 1. Flowchart of the cohort study.
The mean times of hospital visits of the 248 migraine participants was 2.98, and 92 (37.1%) participants visited the hospital only once for their migraines within 12 weeks-observation period. As for treatment duration, 73 participants received CHM treatment for 28 days or more, and they were categorised as subgroup A (CHM ≥28 days). The remaining 175 participants undertook CHM treatment for less than 28 days, therefore were included in subgroup B (CHM <28 days).
Notably, participants from subgroup A exhibited a more advanced age and a longer migraine disease duration. In addition, disease severity measured by monthly migraine days, peak pain NRS and monthly migraine frequency in subgroup A significantly surpassed that of subgroup B. Moreover, the frequency of days on acute medications over the 4 weeks preceding the baseline assessment was notably higher in subgroup A in comparison to subgroup B (Table 1).
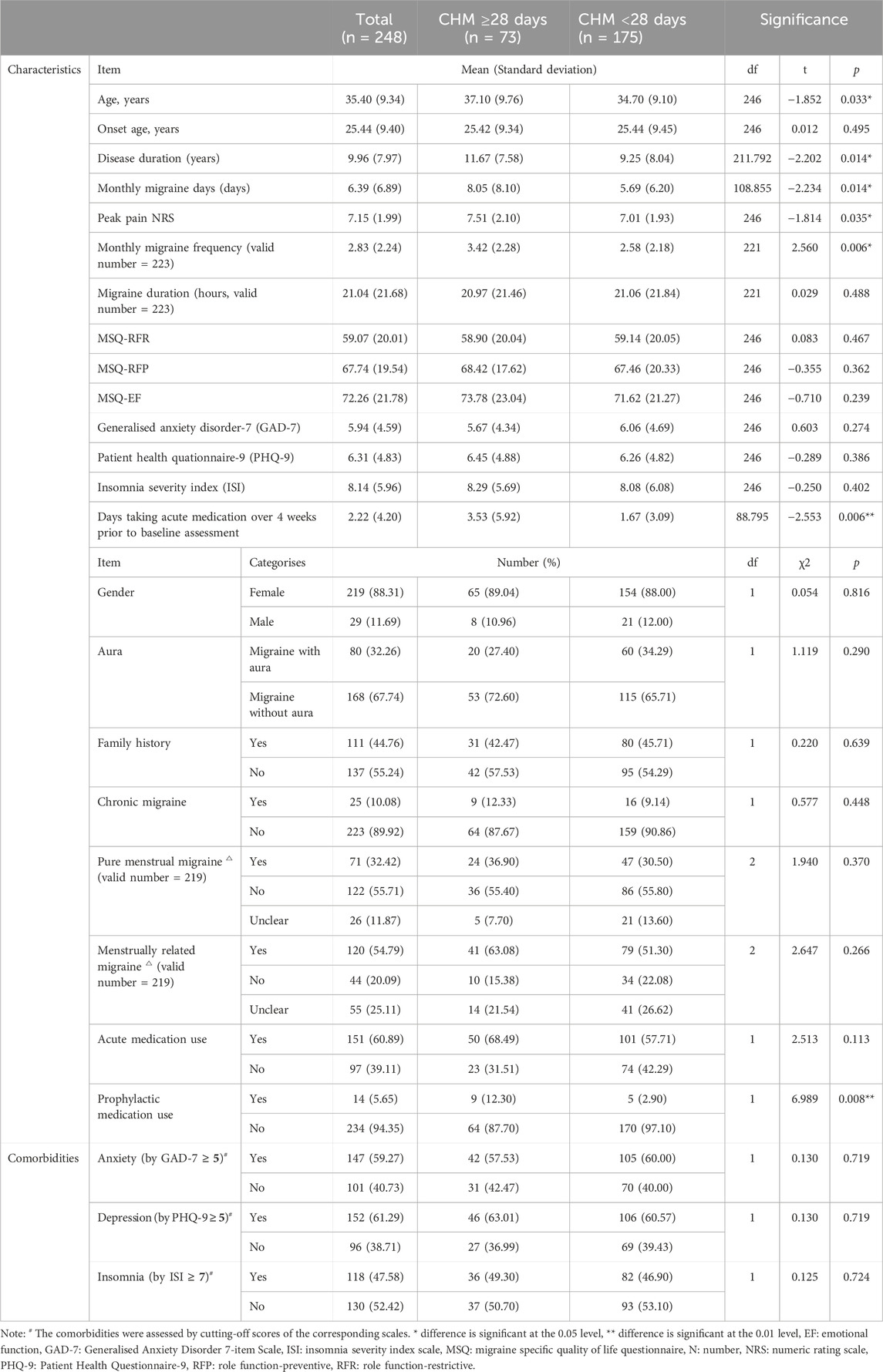
TABLE 1. Baseline characteristics, comorbidities of migraine participants.
Patients’ preferences and values regarding their coming treatments at their initial visits are presented in Table 2. The effect of treatments on migraine severity was unsurprisingly the most popular expectation by 207 (83.47%) of the participants, while the potential side effects of the treatments were concerned by 128 (51.61%) of the participants. In addition, nearly half of the participants expected their treatments to show extended effects in improving sleeping quality (n = 116, 46.77%), regulating psychological status (n = 110, 44.35%) and promoting quality of life (n = 104, 41.94%). Furthermore, 115 (46.37%) of the participants voiced apprehensions regarding the treatment duration. Interestingly, only one third (n = 80, 32.26%) of the participants expected the treatment effects in reducing their usage of acute medications. There was not statistical between-subgroup difference regarding any item of the preferences and values.

TABLE 2. Patients’ preferences and values.
As indicated by Figure 2, the percentage of participants taking acute medications declined from 60.89% at baseline to 43.48% at week 4 but climbed up again to 58.38% at week 12. In contrast, the percentage of participants taking prophylactic medications remained around 5% throughout the observation period.
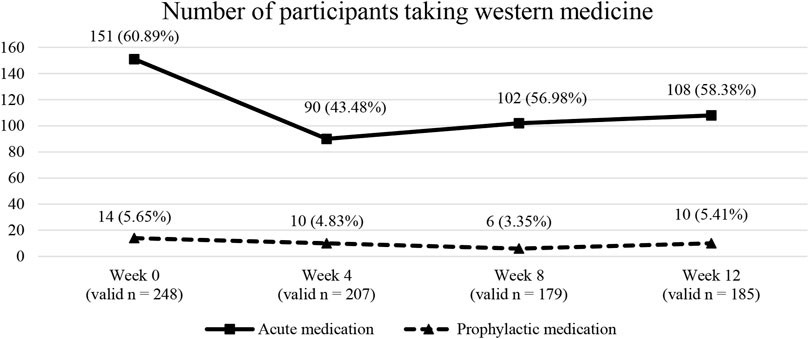
FIGURE 2. Number of participants taking western medications at different timepoints.
Detailed descriptions of self-administrated acute medication usage at baseline are presented in Table 3. Among the 151 participants reporting taking acute medications for their migraines at baseline, the most common classification of acute medications was monotherapy of non-migraine specific acute medications, including Ibuprofen (n = 80, 52.98%) and Paracetamol (n = 31, 20.53%). In contrast, migraine specific acute medication, such as triptans (n = 5, 3.31%) and ergotamine (n = 1, 0.66%), were only used by a limited number of migraine participants (Table 3).
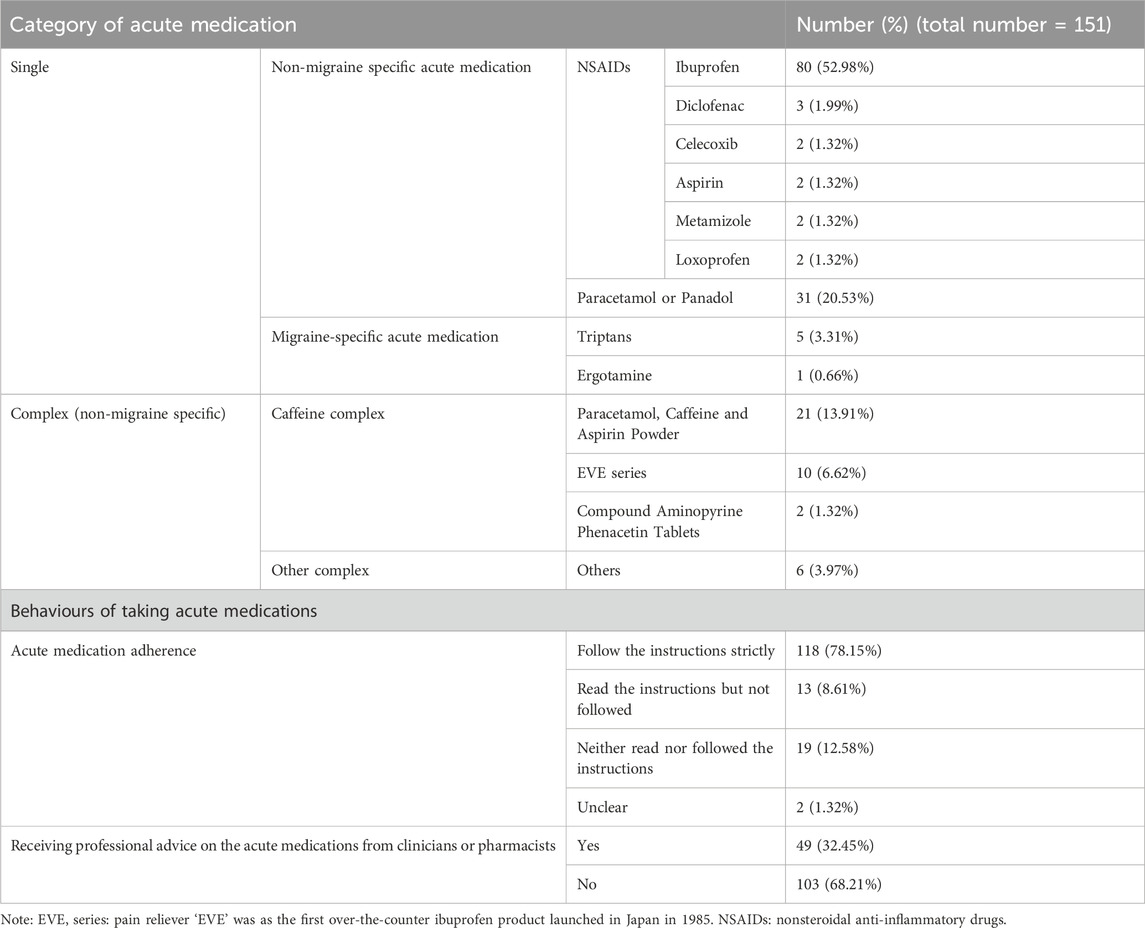
TABLE 3. Category of acute medications at baseline and the corresponding behaviours.
In addition, 78.15% of the 151 participants strictly followed the drug dosage as instructed. However, 13 (8.61%) of them did not adhere to the instructed drug dosage despite having read the instructions, and 19 (12.58%) of them did not read the instructions at all. Moreover, less than one third (32.45%) of these participants received professional advice regarding their usage of acute medication (Table 3).
According to the controlled GLMMs results, both changes of monthly migraine days and changes of peak pain NRS at follow-up timepoints from baseline were not significantly different between subgroup A and B (Table 4).
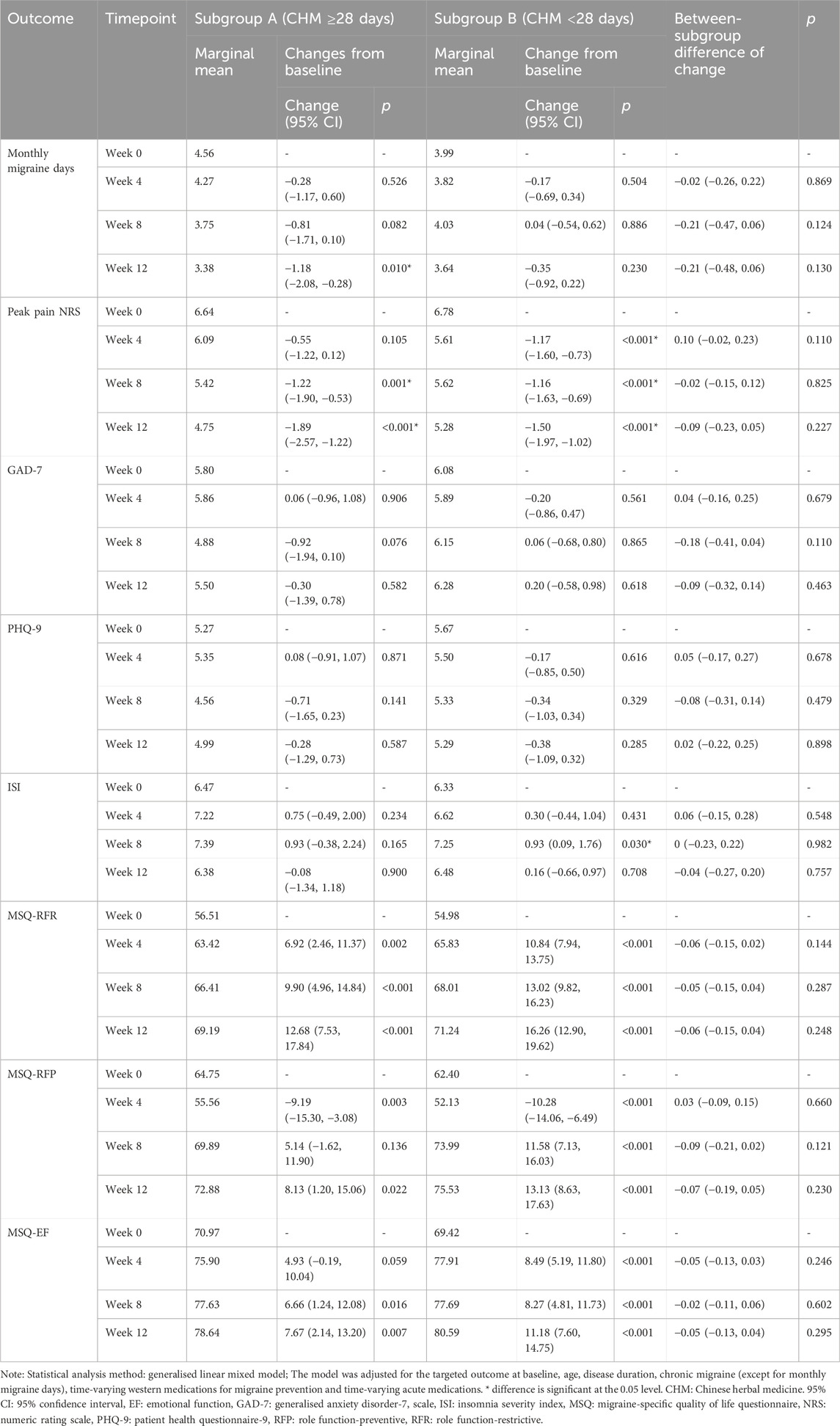
TABLE 4. Changes from baseline and the between-subgroup comparisons.
Monthly migraine days in the entire cohort declined from week 0 to week 12 (p = 0.05), as well as from week 4 to week 12 (p = 0.038). These reductions could be primarily attributed to subgroup A, as similar reductions were observed in subgroup A. In contrast, patients within subgroup B did not achieve any reduction in monthly migraine days throughout the 12-week observation period (Table 5).
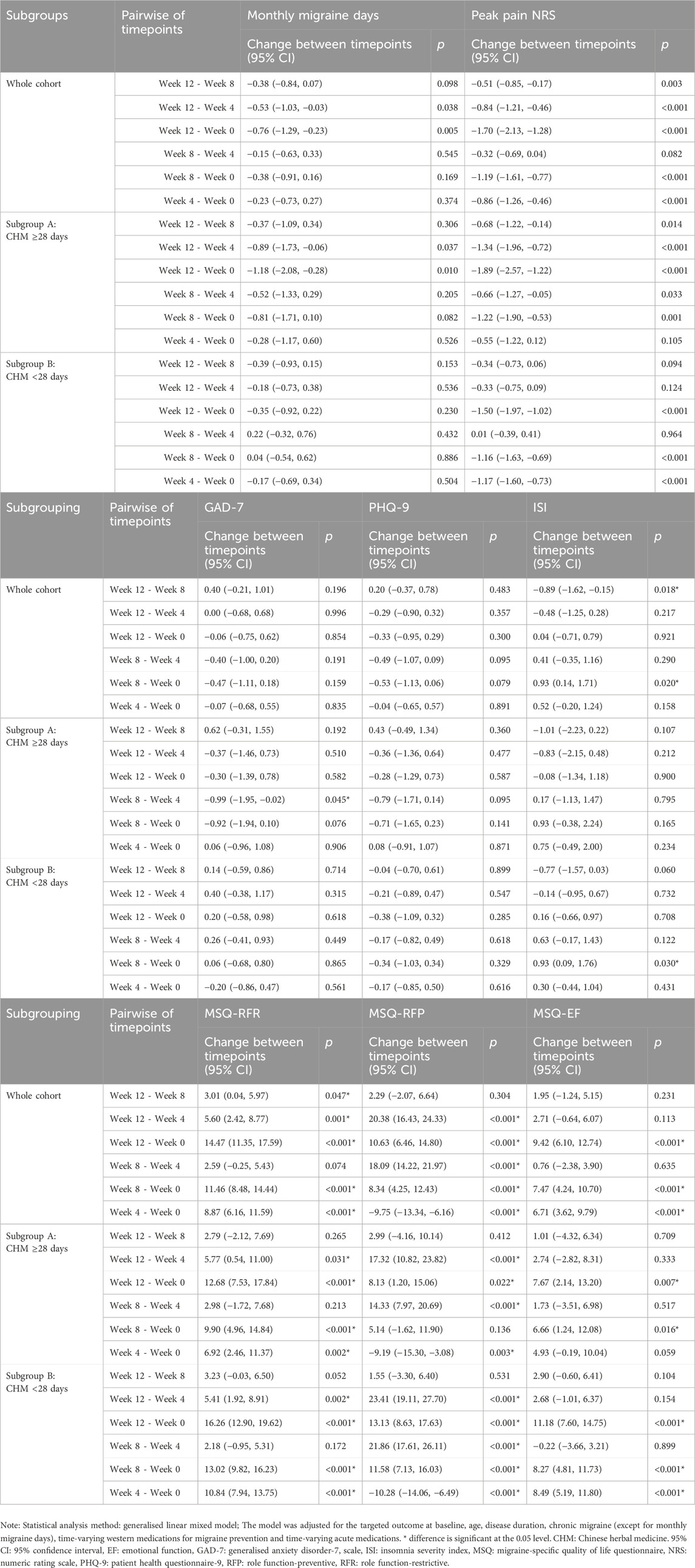
TABLE 5. Pairwise comparisons between timepoints.
In terms of the peak pain NRS, there was a consistent and prolonged downward trend observed within the entire cohort and either subgroup. Notably, the reduction in peak pain NRS scores within subgroup A was sustained not only from week 0 to the subsequent follow-up timepoints, but also from week 4 to week 8 and week 12, as well as persisting from week 8 to week 12. In contrast, the deduction of peak pain NRS scores in subgroup B was not consistently maintained from week 4 to week 8 or week 12, nor from week 8 to week 12 (Table 5).
As Table 4 indicated, changes of GAD-7, PHQ-9 and ISI scores at follow-up timepoints from week 0 were not significantly different between subgroups.
In terms of PHQ-9, no significant variations were observed across the entire cohort or within either of the subgroups.
Regarding GAD-7, the scores remained consistent throughout the observation period for the entire cohort and subgroup B. However, within subgroup A, a significant reduction in GAD-7 scores emerged from week 4 to week 8 (p = 0.045).
As for ISI, the score within the entire cohort exhibited a significant increase from week 0 to week 8 (p = 0.020), followed by a reduction from week 8 to week 12 (p = 0.018). The substantial deterioration in ISI scores from week 0 to week 8 was primarily attributed to subgroup B (p = 0.03), whereas the ISI score in subgroup A did not significantly increased (Table 5).
Both subgroups gained a steady increase in MSQ-RFR from week 0 to each follow-up timepoint, and they also achieved a significant increase in MSQ-RFP and MSQ-EF from week 0 to week 12. However, only subgroup B exhibited an increase in MSQ-RFP from week 0 to week 8, and an increase in MSQ-EF from week 0 to week 4, whereas these changes were not observed in subgroup A (Table 5). Nevertheless, the changes of MSQ-RFR, MSQ-RFP and MSQ-EF scores at follow-up timepoints from baseline were not significantly different between subgroups (Table 4).
Patient-reported adverse events (AEs) were collected from CRFs. Throughout the observation period, 30 participants reported a total of 51 AEs, involving 17 symptoms. The most common AE reported was discomfort in the stomach (n = 18), followed by diarrheal (n = 8), fatigue (n = 4) and dizziness (n = 4). No severe AEs were reported. Furthermore, the number of participants reporting AEs and the number of AE cases appeared comparable between the two subgroups based on CHM treatment duration (≥28 days vs. < 28 days) (Table 6). No statistical difference was detected between subgroup A (CHM treatment duration ≥28 days) and subgroup B (CHM treatment duration <28 days) regarding the number of patients reporting AEs (χ2 = 3.174, p = 0.075).
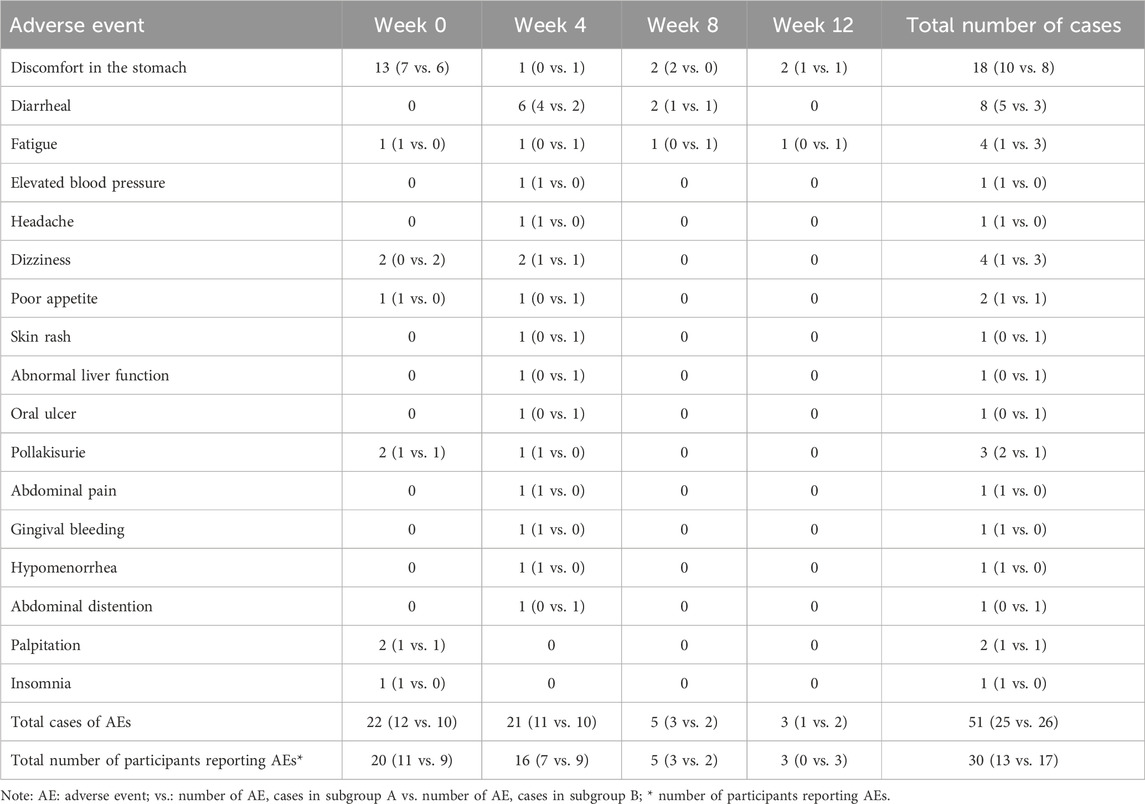
TABLE 6. Adverse events reported by participants.
The medical records of the responders (≥50% reduction in monthly migraine days at week 12) were retrieved for treatment pattern analysis.
A total of 341 herbal prescriptions involving 147 herbs were eligible for analyses. The most commonly used herb was gan cao, which was prescribed 315 times, followed by gui zhi (n = 265) and chuan xiong (n = 246). The remaining herbs with top ten frequency included fu ling (n = 241), bai zhu (n = 231), yan hu suo (n = 222), ban xia (n = 220), chen pi (n = 218), bai shao (n = 210), and xiang fu (n = 204).
Patented Chinese herbal medicine products (PCHMPs) used for migraines were presented in Table 7. Interestingly, the most commonly used PCHMPs were Wei su granule (n = 75) and Jian wei yu yang tablet (n = 73), which mainly targeted at gastrointestinal conditions. Headache-specific PCHMPs like Tian shu tablet and Tong tian oral solution were prescribed by less than 10% of the cases.

TABLE 7. Frequency and functions of commonly used PCHMPs.
The mean age of the migraine participants in this study is 35.40 (±9.34) years, falling within the age range with the highest prevalence of migraines (Safiri et al., 2022). Chronic migraine constitutes over 10% of the included participants, a percentage similar to that of chronic migraine among the migraine population in United State (13.65%) (Buse et al., 2021).
The female-to-male ratio in this observational study (7.5: 1) surpasses the general migraine population ratio (3–4:1) (Vetvik and MacGregor, 2017; Lipton et al., 2018), rendering the findings of this study particularly relevant to female migraine patients. This higher percentage of female participants may be attributed to the fact that female participants tend to experience more severe and disabling migraine attacks (Neumeier et al., 2021). In addition, the female-predominance aligns with findings from a previous report, which concluded that female migraine patients were more likely to be Chinese medicine users (Chang et al., 2014).
Aura was reported in over 32% of the migraine participants in this study, which is higher than the occurrence among the general migraine populations (25%) (Rasmussen and Olesen, 1992). Migraine with aura was reported to be associated with reluctant response to conventional pharmacotherapies (Hansen et al., 2015; Hansen and Charles, 2019), which might explain the higher proportion of migraine with aura in the Chinese medicine hospital.
Anxiety, depression and insomnia are the most common comorbidities among the migraine participants, consistent with previous reports (Caponnetto et al., 2021; Lyu et al., 2022b). Notably, depression was comorbid in 61.29% of the migraine participants in this study, the percentage is higher than that among the general migraine population (16%–18%) (Yong et al., 2012; Lee et al., 2020). An increased likelihood of comorbid depression was reported among migraine patients visiting a headache clinic (Amoozegar et al., 2017). Additionally, it was noted that this comorbid depression was inadequately treated (Amoozegar et al., 2017).
Patients’ preferences and values encompass the distinct understandings, individual preferences, concerns, expectations and life circumstances (Straus et al., 2018). Values refer to a patient’s attitudes and perceptions regarding various healthcare alternatives, while preferences represent their favoured choices after accounting for their values (Llewellyn-Thomas and Crump, 2013). Established methods to investigate patients’ preferences and values include interviews, focus groups, observation, surveys, narrative description, etc. (Michael et al., 2022). This study employed a combination of behavioural observations, treatment utilisation patterns analysis, and targeted surveys focusing on narrative preferences and values. These approaches collectively facilitated a comprehensive exploration of the diverse spectrum of migraine patients’ preferences and values.
More than 60% of the migraine participants in the study reported using acute medications for their migraines prior to their initial treatments in the studied Chinese hospital. However, over 60% of them utilised non-specific migraine acute medications like nonsteroidal anti-inflammatory drugs (NSAIDs), while migraine-specific acute medications like triptans was used by less than 5% of the patients. The discrete percentages of patients taking migraine-specific and non-specific acute medications closely resembled findings from a prior report (Zhao et al., 2023). The potential reasons contributing to the high prevalence of NSAIDs mainly involve their low prices and high patient accessibility as over-the-counter medications (Zhao et al., 2023). In contrast, the low patient accessibility and limited choices of drugs restricted the limited spread of triptans among migraine patients (Zhao et al., 2023). Low application of triptans and low adherence to the therapeutic guideline was also reported in Denmark and the United States (Marmura et al., 2015; Lipton et al., 2022; Olesen et al., 2022).
Additionally, up to 68% of the participants did not receive professional advice on their acute medications for migraine, and over one third of them reported poor adherence to the medication instructions. Inadequate consultation rate was reported in the United States, with 27.6% of episodic migraine and 40.8% of chronic migraine responders (Buse et al., 2021). It is appealed to increase consultation and diagnosis rates, as well as promoted patient education, to improve the delivery of appropriate guideline-based treatment, and avoidance of medication overuse (Buse et al., 2021; Katsuki et al., 2023).
Earlier research has indicated that patients possessing multiple comorbidities, complex symptoms, residing in rural areas, being females, and being in the middle to old age group, were more likely to receive CHM treatment (Chang et al., 2014; Lin et al., 2015; Xin et al., 2020). The present study has shed light on the fact that participants undergoing a longer duration CHM therapy in the studied hospital were experiencing more severe migraines, and they tended to be older in age with a longer disease duration of migraine.
Within the 12-week observation period, the mean CHM treatment duration was found to be 20.72 days, and the mean frequency of hospital visits was only 2.98 times. In contrast, the mean primary care physical visits for migraine within 3 months was reported to be 2.57 for chronic migraine and 2.54 for episodic migraine in Europe, and the corresponding neurologist specialist visits was 1.53 and 1.73, respectively (Bloudek et al., 2012). In this study, the limited treatment duration and times of hospital visits might have been interrupted by the quarantine of COVID-19 (Buse et al., 2022; Jokubaitis et al., 2023). Low adherence and persistence for prophylactic migraine medication were reported to be associated with low response rate and unwanted side effects (Lafata et al., 2010; Hepp et al., 2014; Rimmele et al., 2023). CHM has been identified as an effective therapy for migraine with an adequate treatment duration, and the side effects were mild. The positive treatment effects of CHM at a sufficient treatment duration may be advertised to the migraine patients to increase the adherence and persistence.
The survey for patients’ preferences and values in this study was refined based on commonly reported items in previous studies and new insights from our previous research (Wenzel et al., 2004; Kelman, 2006; Rozen, 2006; Peres et al., 2007; Mansfield et al., 2019; Lyu et al., 2022b). Consistent with previous reports, increased efficacy was the most reported expectation, while side effects were the top concern, among the migraine participants (Kelman, 2006; Rozen, 2006; Peres et al., 2007; Mansfield et al., 2019). Improved quality of life after treatments was also expected by migraine patients (Kelman, 2006). No statistical difference was observed between subgroups regarding any item of preferences and values. It is novel to reveal that a substantial percentage of migraine participants expected the extended effects on migraine comorbidities of anxiety, depression, and insomnia in our report, while migraine comorbidities issues were seldom addressed by previous studies. In addition, as the increased concern about medication overuse, our study incorporated a novel option regarding reducing acute medication usage. The result indicated that limited number of participants expressed expectation to reduce their acute medications, as the number of days taking acute medication at baseline was merely 2.22/4 weeks. Near half of the migraine participants showed attention to treatment duration, meanwhile around 75% of the participants discontinued their treatments within 28 days. The relationship between treatment effect and treatment duration needs further investigation.
As indicated by the outcomes derived from the GLMM analyses above, CHM appeared beneficial in reducing monthly migraine days and peak pain NRS. Particularly, the beneficial effects required a minimum of 28 days CHM treatment. Furthermore, when administered for 28 days or more, CHM might lead to a more sustained effects in reducing peak pain NRS, compared to that when administered for less than 28 days. In summary, a longer CHM treatment duration is associated with a better treatment response, this is consistent with the conclusions from our previous systematic review (Lyu et al., 2022a).
In addition, a minimum duration of CHM treatment for 28 days appears to be beneficial for reducing migraine-comorbid anxiety, and preventing the worsening of insomnia, but it has limited effect on depression. However, it is important to note that depression and insomnia might have been affected by the stress caused by the unanticipated COVID-19 pandemic (Suzuki et al., 2021; Buse et al., 2022; Thaxter and Smitherman, 2022), which was not systematically assessed in this study. Clinical evidence has found that several CHM formulae were effective in controlling anxiety, depression and insomnia, either as independent conditions or as comorbidities of other conditions such as heart failure, chronic obstructive pulmonary disease, etc. (Hu et al., 2021; Yang et al., 2021; Wang et al., 2022). The extended effects of CHM on the psychological comorbidities of migraine need further examination.
Moreover, CHM may effectively improve specific quality of life for the migraine patients, regardless of the treatment duration. The beneficial effects of CHM in improving patients’ quality of life were also reported in our previous systematic reviews for migraines (Lyu et al., 2020; Lyu et al., 2022a), and for other conditions, such as atopic dermatitis, cancer, perimenopausal women, etc. (Hon et al., 2007; Chan et al., 2011; Xia et al., 2012).
These effectiveness evaluations in return addressed the leading expectations of the participants in this study, which were also in consistent with previous reports on patients’ preferences and values (Kelman, 2006; Rozen, 2006; Peres et al., 2007; Mansfield et al., 2019).
Acute medication overuse is a major but modifiable risk factor for chronic migraine (Buse et al., 2019). Approximately 60% of the migraine participants took acute medications for their migraines at baseline. Notably, the proportion of participants taking acute medication reduced significantly at week 4 but increased at around 58% towards the end of the observation period. Previously, CHM-induced reduction in acute medications for chronic tension-type headaches was reported in another observational study (Tong et al., 2015). The reduction in acute medication usage and the potential of CHM for preventing and reversing medication overuse headache warranted more robust investigation.
Throughout the 12-week observation period, a total of 51 AEs were documented by 30 (12.10%) of the participants. The incidence rate of AEs was comparatively lower than those reported for erenumab (37%) and onabotulinumtoxinA (25%) based on real-world observations (Matharu et al., 2017; Schenk et al., 2022). In addition, among the instances, 18 (35.29%) of the patient-reported AEs were gastrointestinal discomforts, and these discomforts were also the most commonly reported AEs in previous reports (Schenk et al., 2022; Silberstein et al., 2023). Moreover, no severe AEs were reported in the current study. The safety profile of CHM for migraine, including the low rate of AEs and the prevailing occurrence of gastrointestinal discomforts, was consistent with our previous findings (Lyu et al., 2020; Lyu et al., 2022a).
The frequency analysis indicated that herbs gan cao, gui zhi, chuan xiong, fu ling, bai zhu, yan hu suo, ban xia, chen pi, bai shao and xiang fu, were widely utilised for migraine, which is similar to the findings of our previous research (Lyu et al., 2020; Lyu et al., 2022a; Lyu et al., 2022b; Zhang et al., 2022). These herbs were reported to exhibit anti-migraine, anti-depression, neuroprotective, sedative-hypnotic and/or antiemetic actions, as summarised in Table 8. These effects not only address the migraine headaches, but also benefit migraine-associated comorbidities including depression and insomnia, as well as accompany symptoms such as nausea and vomiting. Specifically, the anti-migraine actions are frequently linked to the modulation of monoamine neurotransmitters (e.g., 5-HT, CGRP) and their turnover rates, as investigated in the case of chuan xiong (Wang et al., 2011; Pu et al., 2019).

TABLE 8. Potential mechanisms of frequent herbs for migraine and associated comorbidities.
The frequently used PCHMPs exhibit diverse functions, including modulating gastrointestinal functions, improving sleeping quality, relieving neck pain and headache, regulating emotions, and treating stroke, as instructed in the Chinese Pharmacopoeia 2020 (State Pharmacopoeia Committee of China, 2020). According to the Chinese medicine holistic theory, various organs and systems interact with each other. Since migraine is a neurological condition often comorbid with depression, anxiety and sleeping disorders, and commonly presents with gastrointestinal symptoms like vomiting and nausea, it is understandable that PCHMPs prescribed for migraine patients would aim to address these issues. Anti-migraine effects of some specific PCHMPs like Tian shu capsule and Tong tian oral solution have been confirmed in clinical trials (Xia et al., 2013; Yu et al., 2019; Liu, 2021a; Liu., 2021b; Lu, 2021). Specifically, Tian shu capsule/tablet achieved its analgesic effects via regulating calcitonin gene-related peptide, adenosine A2a receptor and adenosine A1 receptor (Lu et al., 2016). In addition, Tian shu capsule/tablet also exhibited anti-depression effects in mice model via regulating 5-hydroxytryptamine, dopamine, and norepinephrine in brain (Sun et al., 2018).
Presently, evidence supporting the use of CHM for migraine-comorbid depression and insomnia remains insufficient. However, there is practical merit in considering CHM as a recommended approach to mitigate migraine severity, alleviate anxiety symptoms, and enhance migraine patients’ quality of life. A minimum treatment duration of 28 days is suggested to achieve these effects based on the results of the current study. The finding may fill in the gap of CHM treatment duration for migraine. Unfortunately, patient adherence and persistence with treatment regimen are often lacking and inadequate, resulting in many patients receiving an insufficient duration of CHM therapy for their migraines.
It is crucial to emphasise the positive correlations between an extended treatment duration and the potential for enhanced treatment outcomes. Disseminating this information to migraine patients could serve to bolster their commitment to treatment adherence and persistence.
Within real-world clinical practice, CHM decoctions for migraines can be modified based on classical formulae, tailored to individual patent characteristics and symptoms. Additionally, prescribing PCHMPs guided by holistic principles and syndrome differentiation is a viable strategy.
The excessive use of acute medications is widely acknowledged as a risk factor for chronic migraine (Cevoli et al., 2009). Given CHM’s potential to alleviate migraine pain, it could serve as a valuable complementary approach alongside traditional acute medications. However, it is important to note that patients demonstrate suboptimal adherence to acute medication instructions, coupled with limited awareness of the necessity of reducing acute medications. While patient education has been shown to enhance clinical effectiveness for migraine treatment (Probyn et al., 2017), the availability of patient education remains inadequate, especially concerning chronic migraine (Short, 2019). As a result, incorporating patient education on appropriate acute medication usage and the perils of medication overuse in migraine management is imperative.
In the realm of clinical research for migraine, it is advisable to incorporate assessments of comorbid anxiety, depression, and insomnia into trial designs. This inclusion is vital for addressing the preferences and values of migraine patients. Moreover, when designing clinical trials to assess the effects of CHM on migraines, a minimum intervention period of 28 days is recommended, based on the GLMM analyses of this study. Additionally, it is advisable to conduct controlled clinical trials to investigate different durations of CHM treatment to further deepen our understanding of the relationship between the length of treatment and the therapeutic effects.
As a cohort study, several biases could originate from various stages throughout the study, including selection bias and confusion bias (Barría and Barría, 2018). However, effective measures have been implemented to control and minimise potential biases. Firstly, standardised inclusion criteria and a rigorous screening procedure were introduced to select representative migraine participants using a consecutive recruiting method. This method not only maintains external validity but also encompasses participants from a typical age range with a moderate disease duration, covering various migraine subtypes. Consequently, the study’s findings hold significant potential for sustainable generalisability. Secondly, strict follow-up plans with scheduled reminders and flexible response methods were employed to minimise the loss of follow-up bias. Thirdly, sophisticated multivariate analytical techniques were employed to minimise the confusion bias.
However, some inevitable limitations have been identified in this study. Firstly, the actual number of registered participants fell below the estimated count, and the rate of loss to follow-up remained noteworthy due to COVID-19-related quarantines, which may have influenced the availability of follow-up data. Secondly, due to its single-centre nature situation in southern China, the generalisability of the results might be compromised, limiting their applicability to migraine patients and Chinese medicine clinicians primarily in southern China. Moreover, the exceptional predominance of female participants in the study may restrict the generalisability of the findings to male migraine patients. This aspect warrants further investigation in future studies.
Nevertheless, it is important to recognise that the clinical expertise derived from real-world clinical practice, without researchers’ interference, adds practicality and relevance to clinical applications.
In real-world clinical practice, migraine patients undergoing an extended course of CHM (≥28 days) exhibited more severe migraine severity at baseline. However, they also achieved significant improvements in terms of monthly migraine days, peak pain NRS score, anxiety, and MSQ, which align with their primary preferences and values. Nonetheless, the current CHM treatment strategy employed in this study did not demonstrate effectiveness in addressing comorbid depression. Conversely, when administrated for less than 28 days, CHM treatment appeared to contribute primarily to the reduction of migraine pain and improvement in MSQ, without conferring sufficient benefits in preventing migraine attacks or addressing comorbidities.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the ethics committee of Guangdong Provincial Hospital of Chinese Medicine (ZE 2020-243-01). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
SL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Visualization, Writing–original draft, Writing–review and editing. CZ: Conceptualization, Methodology, Supervision, Writing–review and editing. AZ: Conceptualization, Methodology, Supervision, Writing–review and editing. XG: Conceptualization, Methodology, Supervision, Writing–review and editing. RH: Investigation, Project administration, Writing–review and editing. ZM: Data curation, Writing–review and editing. QS: Investigation, Project administration, Writing–review and editing. CX: Conceptualization, Methodology, Supervision, Writing–review and editing. JS: Conceptualization, Funding acquisition, Methodology, Supervision, Writing–review and editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was supported by the China-Australia International Research Centre for Chinese Medicine. It was funded by National Key Research and Development Program of China (No. 2019YFC1708601) and the Specific Fund of State Key Laboratory of Dampness Syndrome of Chinese Medicine (SZ2021ZZ14), and Guangdong Administration of Traditional Chinese Medicine (No: 20242024).
Firstly, the authors sincerely acknowledge, Dr Hui Li, Dr Xiaodong Luo, Dr Daoyou Zhou, Dr Lijun Qiao, Dr Manli Wu, Dr Lianghui Wu, Dr Keyi Lin, Dr Xinxin Liu, for their pivotal roles in participants screening and recruitment for my project. Secondly, the authors’ appreciation extends to the participants who graciously took part in the project, enabling the advancement of knowledge and research. Last but not least, the authors appreciated the statistical advice from Professor Cliff Da Costa, Dr Wenwei Ouyang and Dr Genghang Chen.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AE, adverse event; CHM, Chinese herbal medicine; CRF, case report form; GAD-7, generalised anxiety disorder 7-item; GLMM, generalised linear mixed model; GPHCM, Guangdong Provincial Hospital of Chinese Medicine; ICHD-3, International Classification of Headache Disorders, third edition; ISI, insomnia severity index; MSQ, migraine-specific quality of life questionnaire; MSQ-EF, migraine-specific quality of life questionnaire-emotional function; MSQ-RFP, migraine-specific quality of life questionnaire-role function-preventive; MSQ-RFR, migraine-specific quality of life questionnaire-role function-restrictive; NRS, numeric rating scale; NSAIDs, nonsteroidal anti-inflammatory drugs; PCHMP, patented Chinese herbal medicine product; PHQ-9, patient health questionnaire-9.
Ailani, J., Burch, R. C., Robbins, M. S., and Society tBoDotAH, (2021). The American Headache Society Consensus Statement: update on integrating new migraine treatments into clinical practice. Headache 61 (7), 1021–1039. doi:10.1111/head.14153
Amoozegar, F., Patten, S. B., Becker, W. J., Bulloch, A. G. M., Fiest, K. M., Davenport, W. J., et al. (2017). The prevalence of depression and the accuracy of depression screening tools in migraine patients. Gen. Hosp. Psychiatry 48, 25–31. doi:10.1016/j.genhosppsych.2017.06.006
Barría, R. M., and Barría, R. M. (2018). Cohort studies in health sciences. London, England: IntechOpen.
Bigal, M. E., and Lipton, R. B. (2006). Modifiable risk factors for migraine progression. Headache 46 (9), 1334–1343. doi:10.1111/j.1526-4610.2006.00577.x
Bloudek, L. M., Stokes, M., Buse, D. C., Wilcox, T. K., Lipton, R. B., Goadsby, P. J., et al. (2012). Cost of healthcare for patients with migraine in five European countries: results from the International Burden of Migraine Study (IBMS). J. Headache Pain 13 (5), 361–378. doi:10.1007/s10194-012-0460-7
Blumenfeld, A. M., Bloudek, L. M., Becker, W. J., Buse, D. C., Varon, S. F., Maglinte, G. A., et al. (2013). Patterns of use and reasons for discontinuation of prophylactic medications for episodic migraine and chronic migraine: results from the second international burden of migraine study (IBMS-II). Headache 53 (4), 644–655. doi:10.1111/head.12055
Buse, D. C., Armand, C. E., Charleston, Lt, Reed, M. L., Fanning, K. M., Adams, A. M., et al. (2021). Barriers to care in episodic and chronic migraine: results from the chronic migraine epidemiology and outcomes study. Headache 61 (4), 628–641. doi:10.1111/head.14103
Buse, D. C., Gerstein, M. T., Houts, C. R., McGinley, J. S., Uzumcu, A. A., McCarrier, K. P., et al. (2022). Impact of the COVID-19 pandemic on people living with migraine: results of the MiCOAS qualitative study. Headache 62 (3), 284–293. doi:10.1111/head.14274
Buse, D. C., Greisman, J. D., Baigi, K., and Lipton, R. B. (2019). Migraine progression: a systematic review. Headache 59 (3), 306–338. doi:10.1111/head.13459
Buse, D. C., Reed, M. L., Fanning, K. M., Bostic, R., Dodick, D. W., Schwedt, T. J., et al. (2020). Comorbid and co-occurring conditions in migraine and associated risk of increasing headache pain intensity and headache frequency: results of the migraine in America symptoms and treatment (MAST) study. J. Headache Pain 21 (1), 23. doi:10.1186/s10194-020-1084-y
Caponnetto, V., Deodato, M., Robotti, M., Koutsokera, M., Pozzilli, V., Galati, C., et al. (2021). Comorbidities of primary headache disorders: a literature review with meta-analysis. J. Headache Pain 22 (1), 71. doi:10.1186/s10194-021-01281-z
Cevoli, S., Sancisi, E., Grimaldi, D., Pierangeli, G., Zanigni, S., Nicodemo, M., et al. (2009). Family history for chronic headache and drug overuse as a risk factor for headache chronification. Headache 49 (3), 412–418. doi:10.1111/j.1526-4610.2008.01257.x
Chan, K. K., Yao, T. J., Jones, B., Zhao, J. F., Ma, F. K., Leung, C. Y., et al. (2011). The use of Chinese herbal medicine to improve quality of life in women undergoing chemotherapy for ovarian cancer: a double-blind placebo-controlled randomized trial with immunological monitoring. Ann. Oncol. 22 (10), 2241–2249. doi:10.1093/annonc/mdq749
Chang, Y. Y., Tsai, Y. T., Lai, J. N., Yeh, C. H., and Lin, S. K. (2014). The traditional Chinese medicine prescription patterns for migraine patients in Taiwan: a population-based study. J. Ethnopharmacol. 151 (3), 1209–1217. doi:10.1016/j.jep.2013.12.040
Chen, K. Z., Chen, S., Ren, J. Y., Lin, S., Xiao, M. J., Cheng, L., et al. (2021). Antidepressant effect of acidic polysaccharides from Poria and their regulation of neurotransmitters and NLRP3 pathwayss. Zhongguo Zhong Yao Za Zhi 46 (19), 5088–5095. doi:10.19540/j.cnki.cjcmm.20210610.705
Choi, J. G., Kang, S. Y., Kim, J. M., Roh, D. H., Yoon, S. Y., Park, J. B., et al. (2012). Antinociceptive effect of cyperi rhizoma and corydalis tuber extracts on neuropathic pain in rats. Korean J. Physiol. Pharmacol. 16 (6), 387–392. doi:10.4196/kjpp.2012.16.6.387
Choi, M., Lim, C., Lee, B. K., and Cho, S. (2022). Amelioration of Brain Damage after Treatment with the Methanolic Extract of Glycyrrhizae Radix et Rhizoma in Mice. Pharmaceutics 14 (12), 2776. doi:10.3390/pharmaceutics14122776
Cnaan, A., Laird, N. M., and Slasor, P. (1997). Using the general linear mixed model to analyse unbalanced repeated measures and longitudinal data. Stat. Med. 16 (20), 2349–2380. doi:10.1002/(sici)1097-0258(19971030)16:20<2349::aid-sim667>3.0.co;2-e
Diener, H. C., Kropp, P., Dresler, T., Evers, S., Förderreuther, S., Gaul, C., et al. (2022). Management of medication overuse (MO) and medication overuse headache (MOH) S1 guideline. Neurol. Res. Pract. 4 (1), 37. doi:10.1186/s42466-022-00200-0
Diener, H. C., Tassorelli, C., Dodick, D. W., Silberstein, S. D., Lipton, R. B., Ashina, M., et al. (2020). Guidelines of the International Headache Society for controlled trials of preventive treatment of migraine attacks in episodic migraine in adults. Cephalalgia 40 (10), 1026–1044. doi:10.1177/0333102420941839
Domitrz, I., Kozubski, W., Rożniecki, J. J., Stępień, A., and Boczarska-Jedynak, M. (2022). The Polish Headache Society and the Headache Section of the Polish Neurological Society Consensus Statement: update on new pharmacological therapies for migraine in clinical practice and public medication reimbursement program for chronic migraine. Arch. Med. Sci. 18 (6), 1705–1707. doi:10.5114/aoms/153955
Dong, Z., Wang, X., He, M., Zhang, M., Han, X., Ran, Y., et al. (2022). Guidelines for diagnosis and treatment of migraine in China. Chin. J. Pain Med. 28 (12), 18. doi:10.3969/j.issn.1006-9852.2022.12.001
Evers, S., Afra, J., Frese, A., Goadsby, P. J., Linde, M., May, A., et al. (2009). EFNS guideline on the drug treatment of migraine--revised report of an EFNS task force. Eur. J. Neurol. 16 (9), 968–981. doi:10.1111/j.1468-1331.2009.02748.x
Ford, J. H., Jackson, J., Milligan, G., Cotton, S., Ahl, J., and Aurora, S. K. (2017). A real-world analysis of migraine: a cross-sectional study of disease burden and treatment patterns. Headache 57 (10), 1532–1544. doi:10.1111/head.13202
Freedom, T., and Evans, R. W. (2013). Headache and sleep. Headache 53 (8), 1358–1366. doi:10.1111/head.12178
Gao, H., Zhu, X., Xi, Y., Li, Q., Shen, Z., and Yang, Y. (2018). Anti-depressant-like effect of atractylenolide I in a mouse model of depression induced by chronic unpredictable mild stress. Exp. Ther. Med. 15 (2), 1574–1579. doi:10.3892/etm.2017.5517
Gliklich, R. E., Dreyer, N. A., and Leavy, M. B. (2014). Registries for evaluating patient outcomes: a user's guide. Rockville, MD, USA: Agency for Healthcare Research and Quality. Available from: https://www.ncbi.nlm.nih.gov/books/NBK208632/.
Guangdong Provincial Hospital of Chinese Medicine (2021). Introduction to Guangdong provincial hospital of Chinese medicine. Available from: http://www.gdhtcm.com/index.html.
Hansen, J. M., and Charles, A. (2019). Differences in treatment response between migraine with aura and migraine without aura: lessons from clinical practice and RCTs. J. Headache Pain 20 (1), 96. doi:10.1186/s10194-019-1046-4
Hansen, J. M., Goadsby, P. J., and Charles, A. (2015). Reduced efficacy of sumatriptan in migraine with aura vs without aura. Neurology 84 (18), 1880–1885. doi:10.1212/WNL.0000000000001535
Headache Classification Committee of the International Headache Society (IHS) (2018). Headache classification committee of the international headache society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia 38 (1), 1–211. doi:10.1177/0333102417738202
Hepp, Z., Bloudek, L. M., and Varon, S. F. (2014). Systematic review of migraine prophylaxis adherence and persistence. J. Manag. Care Pharm. 20 (1), 22–33. doi:10.18553/jmcp.2014.20.1.22
Hirata, K., Ueda, K., Komori, M., Ye, W., Kim, Y., Cotton, S., et al. (2021). Unmet needs in Japanese patients who report insufficient efficacy with triptans for acute treatment of migraine: retrospective analysis of real-world data. Pain Ther. 10 (1), 415–432. doi:10.1007/s40122-020-00223-y
Hon, K. L., Leung, T. F., Ng, P. C., Lam, M. C., Kam, W. Y., Wong, K. Y., et al. (2007). Efficacy and tolerability of a Chinese herbal medicine concoction for treatment of atopic dermatitis: a randomized, double-blind, placebo-controlled study. Br. J. Dermatol 157 (2), 357–363. doi:10.1111/j.1365-2133.2007.07941.x
Hu, J., Teng, J., Wang, W., Yang, N., Tian, H., Zhang, W., et al. (2021). Clinical efficacy and safety of traditional Chinese medicine Xiao Yao San in insomnia combined with anxiety. Med. Baltim. 100 (43), e27608. doi:10.1097/MD.0000000000027608
Huang, Y. J., Hsu, N. Y., Lu, K. H., Lin, Y. E., Lin, S. H., Lu, Y. S., et al. (2020). Poria cocos water extract ameliorates the behavioral deficits induced by unpredictable chronic mild stress in rats by down-regulating inflammation. J. Ethnopharmacol. 258, 112566. doi:10.1016/j.jep.2020.112566
IBM (2021). SPSS statistics: IBM. Available from: https://www.ibm.com/docs/en/spss-statistics/26.0.0?topic=edition-generalized-linear-mixed-models&mhsrc=ibmsearch_a&mhq=Generalized%20linear%20mixed%20models.
Jebasingh, D., Devavaram Jackson, D., Venkataraman, S., Adeghate, E., and Starling Emerald, B. (2014). The protective effects of Cyperus rotundus on behavior and cognitive function in a rat model of hypoxia injury. Pharm. Biol. 52 (12), 1558–1569. doi:10.3109/13880209.2014.908395
Jokubaitis, M., Bakutis, J., and Ryliškienė, K. (2023). COVID-19 pandemic: impact of quarantine on migraine and patients' care in Lithuania. Clin. Neurol. Neurosurg. 226, 107615. doi:10.1016/j.clineuro.2023.107615
Katsuki, M., Matsumori, Y., Kawahara, J., Yamagishi, C., Koh, A., Kawamura, S., et al. (2023). Headache education by leaflet distribution during COVID-19 vaccination and school-based on-demand e-learning: itoigawa Geopark Headache Awareness Campaign. Headache J. Head Face Pain 63 (3), 429–440. doi:10.1111/head.14472
Kelman, L. (2006). The broad treatment expectations of migraine patients. J. Headache Pain 7 (6), 403–406. doi:10.1007/s10194-006-0322-2
Kelman, L. (2007). The triggers or precipitants of the acute migraine attack. Cephalalgia 27 (5), 394–402. doi:10.1111/j.1468-2982.2007.01303.x
Kelman, L., and Rains, J. C. (2005). Headache and sleep: examination of sleep patterns and complaints in a large clinical sample of migraineurs. Headache 45 (7), 904–910. doi:10.1111/j.1526-4610.2005.05159.x
Kim, B. K., Chu, M. K., Yu, S. J., Dell'Agnello, G., Han, J. H., and Cho, S. J. (2021). Burden of migraine and unmet needs from the patients' perspective: a survey across 11 specialized headache clinics in Korea. J. Headache Pain 22 (1), 45. doi:10.1186/s10194-021-01250-6
Kim, H., Park, I., Park, K., Park, S., Kim, Y. I., and Park, B. G. (2022). The positive effects of poria cocos extract on quality of sleep in insomnia rat models. Int. J. Environ. Res. Public Health 19 (11), 6629. doi:10.3390/ijerph19116629
Klonowski, T., Kropp, P., Straube, A., and Ruscheweyh, R. (2022). Psychological factors associated with headache frequency, intensity, and headache-related disability in migraine patients. Neurol. Sci. 43 (2), 1255–1266. doi:10.1007/s10072-021-05453-2
Kouremenos, E., Arvaniti, C., Constantinidis, T. S., Giannouli, E., Fakas, N., Kalamatas, T., et al. (2019). Consensus of the hellenic headache society on the diagnosis and treatment of migraine. J. Headache Pain 20 (1), 113. doi:10.1186/s10194-019-1060-6
Kowacs, F., Roesler, C. A. P., Piovesan É, J., Sarmento, E. M., Campos, H. C., Maciel, J. A., et al. (2019). Consensus of the Brazilian Headache Society on the treatment of chronic migraine. Arq. Neuropsiquiatr. 77 (7), 509–520. doi:10.1590/0004-282X20190078
Kwangjai, J., Cheaha, D., Manor, R., Sa-Ih, N., Samerphob, N., Issuriya, A., et al. (2021). Modification of brain waves and sleep parameters by Citrus reticulata Blanco. cv. Sai-Nam-Phueng essential oil. Biomed. J. 44 (6), 727–738. doi:10.1016/j.bj.2020.05.017
Lafata, J. E., Tunceli, O., Cerghet, M., Sharma, K. P., and Lipton, R. B. (2010). The use of migraine preventive medications among patients with and without migraine headaches. Cephalalgia 30 (1), 97–104. doi:10.1111/j.1468-2982.2009.01909.x
Lee, D. H., Kim, K. M., Cho, S.-J., Kim, W.-J., Yang, K. I., Yun, C.-H., et al. (2020). Impacts of migraine on the prevalence and clinical presentation of depression: a population-based study. J. Affect. Disord. 272, 215–222. doi:10.1016/j.jad.2020.03.102
Li, F., Zhang, K., Yu, M., Chen, T., Ma, L., Zhang, H., et al. (2021b). Antidepressant-like effect and phytochemical profile of supercritical CO₂ extract from Citri reticulatae pericarpium. Pharmazie 76 (6), 249–255. doi:10.1691/ph.2021.1408
Li, H., Bai, F., Cong, C., Chen, B., Xie, W., Li, S., et al. (2021a). Effects of ligustrazine on the expression of neurotransmitters in the trigeminal ganglion of a rat migraine model. Ann. Transl. Med. 9 (16), 1318. doi:10.21037/atm-21-3423
Li, J.-H., Cao, X.-P., Wei, J.-J., Song, L., Liao, F.-J., Zheng, G.-Q., et al. (2015). Chuanxiong chadiao powder, a famous Chinese herbal prescription, for headache: a systematic review and meta-analysis. Complementary Ther. Med. 23 (4), 577–590. doi:10.1016/j.ctim.2015.06.012
Li, Y., Wang, L., Zhang, B., Gao, F., and Yang, C. (2019). Glycyrrhizin, an HMGB1 inhibitor, exhibits neuroprotective effects in rats after lithium-pilocarpine-induced status epilepticus. J. Pharm. Pharmacol. 71 (3), 390–399. doi:10.1111/jphp.13040
Lin, S., Chen, H., Nie, B., Jiang, C., Yang, H., Wang, Q., et al. (2023). Raw Pinelliae Rhizoma: examination of sedative and hypnotic effects in mice and chemical analysis. Sleep. Breath. 27 (3), 1143–1153. doi:10.1007/s11325-022-02714-y
Lin, S., Nie, B., Song, K., Ye, R., and Yuan, Z. (2019). Pinelliae rhizoma praeparatum cum alumine extract: sedative and hypnotic effects in mice and component compounds. Biomed. Res. Int. 2019, 6198067. doi:10.1155/2019/6198067
Lin, S. K., Tsai, Y. T., Lai, J. N., and Wu, C. T. (2015). Demographic and medication characteristics of traditional Chinese medicine users among dementia patients in Taiwan: a nationwide database study. J. Ethnopharmacol. 161, 108–115. doi:10.1016/j.jep.2014.12.015
Lipton, R. B., Fanning, K. M., Buse, D. C., Martin, V. T., Hohaia, L. B., Adams, A. M., et al. (2019a). Migraine progression in subgroups of migraine based on comorbidities: results of the CaMEO Study. Neurology 93 (24), e2224–e2236. doi:10.1212/WNL.0000000000008589
Lipton, R. B., Munjal, S., Alam, A., Buse, D. C., Fanning, K. M., Reed, M. L., et al. (2018). Migraine in America symptoms and treatment (MAST) study: baseline study methods, treatment patterns, and gender differences. Headache 58 (9), 1408–1426. doi:10.1111/head.13407
Lipton, R. B., Munjal, S., Buse, D. C., Alam, A., Fanning, K. M., Reed, M. L., et al. (2019b). Unmet acute treatment needs from the 2017 migraine in America symptoms and treatment study. Headache 59 (8), 1310–1323. doi:10.1111/head.13588
Lipton, R. B., Nicholson, R. A., Reed, M. L., Araujo, A. B., Jaffe, D. H., Faries, D. E., et al. (2022). Diagnosis, consultation, treatment, and impact of migraine in the US: results of the OVERCOME (US) study. Headache 62 (2), 122–140. doi:10.1111/head.14259
Liu, S. (2021a). Effect of tongtian oral liquid on chronic migraine of blood stasis clip wind type and mechanism of effect on CGRP, SP and 5-HT, 通天口服液治疗血瘀夹风型慢性偏头痛发作期疗效及对CGRP、SP、5-HT影响的机制初探, dissertation in Chinese 硕士. Chengdu, China: Chengdu University of Traditional Chinese Medicine.
Liu, X. (2021b). Study on the mechanism of Tongtian Oral liquid in treating chronic migraine with blood stasis and Wind based on coagulation related indexes and evaluation of curative effect, 基于凝血相关指标初探通天口服液治疗血瘀夹风型慢性偏头痛发作期的机制研究及疗效评价, Dissertation in Chinese 硕士. Chengdu, China: Chengdu University of Traditional Chinese Medicine.
Llewellyn-Thomas, H. A., and Crump, R. T. (2013). Decision support for patients: values clarification and preference elicitation. Med. Care Res. Rev. 70 (1 Suppl. l), 50S–79s. doi:10.1177/1077558712461182
Lombard, L., Farrar, M., Ye, W., Kim, Y., Cotton, S., Buchanan, A. S., et al. (2020). A global real-world assessment of the impact on health-related quality of life and work productivity of migraine in patients with insufficient versus good response to triptan medication. J. Headache Pain 21 (1), 41. doi:10.1186/s10194-020-01110-9
Lu, M. (2021). Preliminary study on the mechanism and efficacy evaluation of Tongtian Oral Liquid in the treatment of Chronic Migraine attacks with blood stasis and wind based on indicators related to vascular endothelial function, 基于血管内皮功能相关指标初探通天口服液治疗血瘀夹风型慢性偏头痛发作期的机制研究及疗效评价, Dissertation in Chinese 硕士. Chengdu, China: Chengdu University of Tradictional Chinese Medicine.
Lu, W., Li, B., Chen, J., Su, Y., Dong, X., Su, X., et al. (2016). Expression of calcitonin gene-related peptide, adenosine A2a receptor and adenosine A1 receptor in experiment rat migraine models. Biomed. Rep. 4 (3), 379–383. doi:10.3892/br.2016.591
Lyu, S., Zhang, C. S., Guo, X., Zhang, A. L., Sun, J., Chen, G., et al. (2022a). Efficacy and safety of oral Chinese herbal medicine for migraine: a systematic review and meta-analyses using robust variance estimation model. Front. Neurology 13, 889336. doi:10.3389/fneur.2022.889336
Lyu, S., Zhang, C. S., Guo, X., Zhang, A. L., Sun, J., Lu, C., et al. (2020). Oral Chinese herbal medicine as prophylactic treatment for episodic migraine in adults: a systematic review and meta-analysis of randomized controlled trials. Evid. Based Complement. Altern. Med. 2020, 5181587. doi:10.1155/2020/5181587
Lyu, S., Zhang, C. S., Sun, J., Weng, H., Xue, C. C., Guo, X., et al. (2022b). Chinese herbal medicine for migraine management: a hospital-based retrospective analysis of electronic medical records. Front. Med. (Lausanne) 9, 936234. doi:10.3389/fmed.2022.936234
Lyu, S., Zhang, C. S., Zhang, A. L., Sun, J., Xue, C. C., and Guo, X. (2022c). Migraine patients visiting Chinese medicine hospital: protocol for a prospective, registry-based, real-world observational cohort study. PLoS One 17 (3), e0265137. doi:10.1371/journal.pone.0265137
Malik, S. N., Hopkins, M., Young, W. B., and Silberstein, S. D. (2006). Acute migraine treatment: patterns of use and satisfaction in a clinical population. Headache 46 (5), 773–780. doi:10.1111/j.1526-4610.2006.00437.x
Mansfield, C., Gebben, D. J., Sutphin, J., Tepper, S. J., Schwedt, T. J., Sapra, S., et al. (2019). Patient preferences for preventive migraine treatments: a discrete-choice experiment. Headache 59 (5), 715–726. doi:10.1111/head.13498
Marmura, M. J., Silberstein, S. D., and Schwedt, T. J. (2015). The acute treatment of migraine in adults: the American headache society evidence assessment of migraine pharmacotherapies. Headache 55 (1), 3–20. doi:10.1111/head.12499
Matharu, M., Pascual, J., Nilsson Remahl, I., Straube, A., Lum, A., Davar, G., et al. (2017). Utilization and safety of onabotulinumtoxinA for the prophylactic treatment of chronic migraine from an observational study in Europe. Cephalalgia 37 (14), 1384–1397. doi:10.1177/0333102417724150
Meng, Q., Cheng, Q., Feng, X., Chen, S., Li, Y., Zhang, G., et al. (2020). The antiemetic effect of xiao-ban-xia-tang formula against cisplatin-induced emesis is mediated through inhibition of NLRP3 inflammasome activation in a rat Pica model. Evid. Based Complement. Altern. Med. 2020, 5497078. doi:10.1155/2020/5497078
Michael, T., Genia, S., Anne-Marie, B., and Carl, H. (2022). Integrating patient values and preferences in healthcare: a systematic review of qualitative evidence. BMJ Open 12 (11), e067268. doi:10.1136/bmjopen-2022-067268
Neumeier, M. S., Pohl, H., Sandor, P. S., Gut, H., Merki-Feld, G. S., and Andrée, C. (2021). Dealing with headache: sex differences in the burden of migraine- and tension-type headache. Brain Sci. 11 (10), 1323. doi:10.3390/brainsci11101323
Olesen, A., Schytz, H. W., Ostrowski, S. R., Topholm, M., Nielsen, K., Erikstrup, C., et al. (2022). Low adherence to the guideline for the acute treatment of migraine. Sci. Rep. 12 (1), 8487. doi:10.1038/s41598-022-12545-2
Orr, S. L., Aubé, M., Becker, W. J., Davenport, W. J., Dilli, E., Dodick, D., et al. (2015). Canadian Headache Society systematic review and recommendations on the treatment of migraine pain in emergency settings. Cephalalgia 35 (3), 271–284. doi:10.1177/0333102414535997
Pang, Y., Zhu, S., and Pei, H. (2020). Pachymic acid protects against cerebral ischemia/reperfusion injury by the PI3K/Akt signaling pathway. Metab. Brain Dis. 35 (4), 673–680. doi:10.1007/s11011-020-00540-3
Pavlovic, J. M., Akcali, D., Bolay, H., Bernstein, C., and Maleki, N. (2017). Sex-related influences in migraine. J. Neurosci. Res. 95 (1-2), 587–593. doi:10.1002/jnr.23903
Peng, C., Xie, X., Wang, L., Guo, L., and Hu, T. (2009). Pharmacodynamic action and mechanism of volatile oil from Rhizoma Ligustici Chuanxiong Hort. on treating headache. Phytomedicine 16 (1), 25–34. doi:10.1016/j.phymed.2008.10.010
Peres, M. F., Silberstein, S., Moreira, F., Corchs, F., Vieira, D. S., Abraham, N., et al. (2007). Patients' preference for migraine preventive therapy. Headache 47 (4), 540–545. doi:10.1111/j.1526-4610.2007.00757.x
Polit, D., and Beck, C. (2020). Essentials of nursing research: appraising evidence for nursing practice. Philadelphia, Pennsylvania, United States: Lippincott Williams and Wilkins.
Pringsheim, T., Davenport, W., Mackie, G., Worthington, I., Aube, M., Christie, S. N., et al. (2012). Canadian Headache Society guideline for migraine prophylaxis. Can. J. Neurol. Sci. 39 (2 Suppl. 2), S1–S59.
Probyn, K., Bowers, H., Mistry, D., Caldwell, F., Underwood, M., Patel, S., et al. (2017). Non-pharmacological self-management for people living with migraine or tension-type headache: a systematic review including analysis of intervention components. BMJ Open 7 (8), e016670. doi:10.1136/bmjopen-2017-016670
Pu, Z. H., Peng, C., Xie, X. F., Luo, M., Zhu, H., Feng, R., et al. (2019). Alkaloids from the rhizomes of Ligusticum striatum exert antimigraine effects through regulating 5-HT(1B) receptor and c-Jun. J. Ethnopharmacol. 237, 39–46. doi:10.1016/j.jep.2019.03.026
Rasmussen, B. K., and Olesen, J. (1992). Migraine with aura and migraine without aura: an epidemiological study. Cephalalgia 12 (4), 221–228. doi:10.1046/j.1468-2982.1992.1204221.x
Rhee, T. G., and Harris, I. M. (2018). Reasons for and perceived benefits of utilizing complementary and alternative medicine in U.S. adults with migraines/severe headaches. Complement. Ther. Clin. Pract. 30, 44–49. doi:10.1016/j.ctcp.2017.12.003
Rimmele, F., Müller, B., Becker-Hingst, N., Wegener, S., Rimmele, S., Kropp, P., et al. (2023). Medication adherence in patients with cluster headache and migraine: an online survey. Sci. Rep. 13 (1), 4546. doi:10.1038/s41598-023-30854-y
Rozen, T. D. (2006). Migraine prevention: what patients want from medication and their physicians (a headache specialty clinic perspective). Headache 46 (5), 750–753. doi:10.1111/j.1526-4610.2006.00429.x
Safiri, S., Pourfathi, H., Eagan, A., Mansournia, M. A., Khodayari, M. T., Sullman, M. J. M., et al. (2022). Global, regional, and national burden of migraine in 204 countries and territories, 1990 to 2019. Pain 163 (2), e293–e309. doi:10.1097/j.pain.0000000000002275
Schenk, H., Holle, D., Nsaka, M., Kleinschnitz, C., Glas, M., and Scheffler, A. (2022). Twelve-month safety, tolerability and susceptibility to adverse events of prophylactic migraine therapy with erenumab: a retrospective real-world study. J. Headache Pain 23 (1), 55. doi:10.1186/s10194-022-01426-8
Scottish Intercollegiate Guidelines Network (SIGN) (2018). Pharmacological management of migraine. https://www.sign.ac.uk/our-guidelines/pharmacological-management-of-migraine/.
Seng, E. K., Buse, D. C., Klepper, J. E., Mayson, S. J., Grinberg, A. S., Grosberg, B. M., et al. (2017). Psychological factors associated with chronic migraine and severe migraine-related disability: an observational study in a tertiary headache center. Headache 57 (4), 593–604. doi:10.1111/head.13021
Shah, V. K., Choi, J. J., Han, J. Y., Lee, M. K., Hong, J. T., and Oh, K. W. (2014). Pachymic acid enhances pentobarbital-induced sleeping behaviors via GABAA-ergic systems in mice. Biomol. Ther. Seoul. 22 (4), 314–320. doi:10.4062/biomolther.2014.045
Short, A. L. (2019). Enhancing migraine self-efficacy and reducing disability through a self-management program. J. Am. Assoc. Nurse Pract. 33 (1), 20–28. doi:10.1097/JXX.0000000000000323
Silberstein, S. D., Reshef, S., Cohen, J. M., Gandhi, S., Seminerio, M., Ramirez Campos, V., et al. (2023). Adverse events reported with therapies targeting the CGRP pathway during the first 6 Months post-launch: a retrospective analysis using the fda adverse events reporting system. Adv. Ther. 40 (2), 445–459. doi:10.1007/s12325-022-02346-4
State Pharmacopoeia Committee of China (2020). Chinese Pharmacopoeia. Xicheng, Beijing, China: Chinese Pharmacopoeia Commission.
Stovner, L. J., Hagen, K., Linde, M., and Steiner, T. J. (2022). The global prevalence of headache: an update, with analysis of the influences of methodological factors on prevalence estimates. J. Headache Pain 23 (1), 34. doi:10.1186/s10194-022-01402-2
Straus, S. E., Glasziou, P., Richardson, W. S., and Haynes, R. B. (2018). Evidence-based medicine: how to practice and teach EBM. Philadelphia, PA, USA: Elsevier.
Sun, J. Y., Liu, Y. T., Jiang, S. N., Guo, P. M., Wu, X. Y., and Yu, J. (2022). Essential oil from the roots of Paeonia lactiflora pall. has protective effect against corticosterone-induced depression in mice via modulation of PI3K/Akt signaling pathway. Front. Pharmacol. 13, 999712. doi:10.3389/fphar.2022.999712
Sun, X., Zhu, F., Zhou, J., Chang, X., Li, L., Hu, H., et al. (2018). Anti-migraine and anti-depression activities of Tianshu capsule by mediating Monoamine oxidase. Biomed. Pharmacother. 100, 275–281. doi:10.1016/j.biopha.2018.01.171
Suzuki, K., Takeshima, T., Igarashi, H., Imai, N., Danno, D., Yamamoto, T., et al. (2021). Impact of the COVID-19 pandemic on migraine in Japan: a multicentre cross-sectional study. J. Headache Pain 22 (1), 53. doi:10.1186/s10194-021-01263-1
Takeshima, T., Wan, Q., Zhang, Y., Komori, M., Stretton, S., Rajan, N., et al. (2019). Prevalence, burden, and clinical management of migraine in China, Japan, and South Korea: a comprehensive review of the literature. J. Headache Pain 20 (1), 111. doi:10.1186/s10194-019-1062-4
Thaxter, L. Y., and Smitherman, T. A. (2022). The effect of the COVID-19 pandemic on headache-related disability among young adults with migraine. Headache 62 (10), 1293–1301. doi:10.1111/head.14411
The British Association for the study of headache (BASH) (2023). National headache management system for adults 2019. Available from: https://www.bash.org.uk/guidelines/.
Tong, Y., Yu, L., and Sun, Y. (2015). Chinese herbal therapy for chronic tension-type headache. Evid. Based Complement. Altern. Med. 2015, 208492. doi:10.1155/2015/208492
Ueda, K., Ye, W., Lombard, L., Kuga, A., Kim, Y., Cotton, S., et al. (2019). Real-world treatment patterns and patient-reported outcomes in episodic and chronic migraine in Japan: analysis of data from the Adelphi migraine disease specific programme. J. Headache Pain 20 (1), 68. doi:10.1186/s10194-019-1012-1
Vetvik, K. G., and MacGregor, E. A. (2017). Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 16 (1), 76–87. doi:10.1016/S1474-4422(16)30293-9
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., Vandenbroucke, J. P., et al. (2007). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370 (9596), 1453–1457. doi:10.1016/S0140-6736(07)61602-X
Walters, A. B., Hamer, J. D., and Smitherman, T. A. (2014). Sleep disturbance and affective comorbidity among episodic migraineurs. Headache 54 (1), 116–124. doi:10.1111/head.12168
Wang, B., Lian, Y., Dong, X., Peng, W., Liu, L., Su, W., et al. (2018). Glycyrrhizic acid ameliorates the kynurenine pathway in association with its antidepressant effect. Behav. Brain Res. 353, 250–257. doi:10.1016/j.bbr.2018.01.024
Wang, B., Teng, Y., Li, Y., Lai, S., Wu, Y., Chen, S., et al. (2022). Evidence and characteristics of traditional Chinese medicine for coronary heart disease patients with anxiety or depression: a meta-analysis and systematic review. Front. Pharmacol. 13, 854292. doi:10.3389/fphar.2022.854292
Wang, L., Zhang, Y., Wang, Z., Gong, N., Kweon, T. D., Vo, B., et al. (2016). The antinociceptive properties of the corydalis yanhusuo extract. PLoS One 11 (9), e0162875. doi:10.1371/journal.pone.0162875
Wang, Y. H., Liang, S., Xu, D. S., Lin, X., He, C. Y., Feng, Y., et al. (2011). Effect and mechanism of senkyunolide I as an anti-migraine compound from Ligusticum chuanxiong. J. Pharm. Pharmacol. 63 (2), 261–266. doi:10.1111/j.2042-7158.2010.01191.x
Wells, R. E., Bertisch, S. M., Buettner, C., Phillips, R. S., and McCarthy, E. P. (2011). Complementary and alternative medicine use among adults with migraines/severe headaches. Headache 51 (7), 1087–1097. doi:10.1111/j.1526-4610.2011.01917.x
Wenzel, R. G., Schommer, J. C., and Marks, T. G. (2004). Morbidity and medication preferences of individuals with headache presenting to a community pharmacy. Headache 44 (1), 90–94. doi:10.1111/j.1526-4610.2004.04016.x
World Medical Association, W. M. (2013). World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. Jama 310 (20), 2191–2194. doi:10.1001/jama.2013.281053
Worthington, I., Pringsheim, T., Gawel, M. J., Gladstone, J., Cooper, P., Dilli, E., et al. (2013). Canadian Headache Society Guideline: acute drug therapy for migraine headache. Can. J. Neurol. Sci. 40 (5 Suppl. 3), S1–S3. doi:10.1017/s0317167100017819
Wu, J. W., and Yang, C. P.Treatment Guideline Subcommittee of the Taiwan Headache Society (2022). 2022 taiwan guidelines for preventive treatment of migraine. Acta Neurol. Taiwan 31 (3), 164–202.
Wu, S., Guo, L., Qiu, F., and Gong, M. (2019). Anti-migraine effect of the herbal combination of chuanxiong rhizoma and cyperi rhizoma and UPLC-MS/MS method for the simultaneous quantification of the active constituents in rat serum and cerebral cortex. Molecules 24 (12), 2230. doi:10.3390/molecules24122230
Xia, W., Zhu, M., Zhang, Z., Kong, D., Xiao, W., Jia, L., et al. (2013). Effect of Tianshu capsule in treatment of migraine: a meta-analysis of randomized control trials. J. Tradit. Chin. Med. 33 (1), 9–14. doi:10.1016/s0254-6272(13)60093-x
Xia, Y., Zhao, Y., Ren, M., Zhang, J., Wang, Y., Chang, Y., et al. (2012). A randomized double-blind placebo-controlled trial of a Chinese herbal medicine preparation (Jiawei Qing'e Fang) for hot flashes and quality of life in perimenopausal women. Menopause 19 (2), 234–244. doi:10.1097/gme.0b013e3182273177
Xin, B., Mu, S., Tan, T., Yeung, A., Gu, D., and Feng, Q. (2020). Belief in and use of traditional Chinese medicine in Shanghai older adults: a cross-sectional study. BMC Complementary Med. Ther. 20 (1), 128. doi:10.1186/s12906-020-02910-x
Xu, J., Kong, F., and Buse, D. C. (2020). Predictors of episodic migraine transformation to chronic migraine: a systematic review and meta-analysis of observational cohort studies. Cephalalgia 40 (5), 503–516. doi:10.1177/0333102419883355
Xu, Y., Sun, J., Li, W., Zhang, S., Yang, L., Teng, Y., et al. (2021). Analgesic effect of the main components of Corydalis yanhusuo (yanhusuo in Chinese) is caused by inhibition of voltage gated sodium channels. J. Ethnopharmacol. 280, 114457. doi:10.1016/j.jep.2021.114457
Yang, S., Xu, Y., Peng, W., Han, D., Feng, F., Wang, Z., et al. (2021). Chinese herbal medicine for symptoms of depression and anxiety in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Complement. Ther. Clin. Pract. 45, 101470. doi:10.1016/j.ctcp.2021.101470
Yong, N., Hu, H., Fan, X., Li, X., Ran, L., Qu, Y., et al. (2012). Prevalence and risk factors for depression and anxiety among outpatient migraineurs in mainland China. J. Headache Pain 13 (4), 303–310. doi:10.1007/s10194-012-0442-9
Yu, S., Ran, Y., Xiao, W., Tang, W., Zhao, J., Chen, W., et al. (2019). Treatment of migraines with Tianshu capsule: a multi-center, double-blind, randomized, placebo-controlled clinical trial. BMC Complementary Altern. Med. 19 (1), 370. doi:10.1186/s12906-019-2775-2
Yu, S., Zhang, Y., Yao, Y., and Cao, H. (2020). Migraine treatment and healthcare costs: retrospective analysis of the China Health Insurance Research Association (CHIRA) database. J. Headache Pain 21 (1), 53. doi:10.1186/s10194-020-01117-2
Zareie, A., Sahebkar, A., Khorvash, F., Bagherniya, M., Hasanzadeh, A., and Askari, G. (2020). Effect of cinnamon on migraine attacks and inflammatory markers: a randomized double-blind placebo-controlled trial. Phytother. Res. 34 (11), 2945–2952. doi:10.1002/ptr.6721
Zhang, C. S., Lyu, S., Zhang, A. L., Guo, X., Sun, J., Lu, C., et al. (2022). Natural products for migraine: data-mining analyses of Chinese Medicine classical literature. Front. Pharmacol. 13, 995559. doi:10.3389/fphar.2022.995559
Zhao, H., Xiao, Z., Zhang, L., Ford, J., Zhong, S., Ye, W., et al. Real-world treatment patterns and outcomes among patients with episodic migraine in China: results from the adelphi migraine disease specific Programme™. J. Pain Res., 2023;16:357–371. doi:10.2147/JPR.S371887
Zhou, J., Wang, J., Li, W., Wang, C., Wu, L., and Zhang, J. (2017). Paeoniflorin attenuates the neuroinflammatory response in a rat model of chronic constriction injury. Mol. Med. Rep. 15 (5), 3179–3185. doi:10.3892/mmr.2017.6371
Zhou, K., Chen, J., Wu, J., Wu, Q., Jia, C., Xu, Y. X. Z., et al. (2019). Atractylenolide III ameliorates cerebral ischemic injury and neuroinflammation associated with inhibiting JAK2/STAT3/Drp1-dependent mitochondrial fission in microglia. Phytomedicine 59, 152922. doi:10.1016/j.phymed.2019.152922
Zhou, L., Chen, P., Liu, L., Zhang, Y., Liu, X., Wu, Y., et al. (2013). Systematic review and meta-analysis of traditional Chinese medicine in the treatment of migraines. Am. J. Chin. Med. 41 (5), 1011–1025. doi:10.1142/S0192415X13500687
Zhou, M. Y., Yao, C. H., Yang, Y. J., Li, X., Yang, J., Liu, J. H., et al. (2023). Based on spinal central sensitization creating analgesic screening approach to excavate anti-neuropathic pain ingredients of Corydalis yanhusuo W.T.Wang. J. Ethnopharmacol. 319 (Pt 1), 117084. doi:10.1016/j.jep.2023.117084
Zhou, Y., Huang, S., Wu, F., Zheng, Q., Zhang, F., Luo, Y., et al. (2021). Atractylenolide III reduces depressive- and anxiogenic-like behaviors in rat depression models. Neurosci. Lett. 759, 136050. doi:10.1016/j.neulet.2021.136050
Keywords: migraine, Chinese herbal medicine, real-world, cohort study, preferences and values, clinical expertise
Citation: Lyu S, Zhang CS, Zhang AL, Guo X, Hua R, Mao Z, Su Q, Xue CC and Sun J (2024) Real-world observations and impacts of Chinese herbal medicine for migraine: results of a registry-based cohort study. Front. Pharmacol. 15:1330589. doi: 10.3389/fphar.2024.1330589
Received: 31 October 2023; Accepted: 15 January 2024;
Published: 02 February 2024.
Edited by:
Tzer-Bin Lin, Taipei Medical University, TaiwanReviewed by:
Francesco Fazio, University of California, San Diego, United StatesCopyright © 2024 Lyu, Zhang, Zhang, Guo, Hua, Mao, Su, Xue and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Charlie Changli Xue, Y2hhcmxpZS54dWVAcm1pdC5lZHUuYXU=; Jingbo Sun, Z2Rzenl5c2piQGd6dWNtLmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.