 Yanrong Shi
Yanrong Shi Jichao Wu2
Jichao Wu2 Cuicui Lu
Cuicui Lu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pharmacol., 22 January 2024
Sec. Renal Pharmacology
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1329307
With the increasing prevalence of multidrug-resistant Gram-negative bacterial pathogens worldwide, antimicrobial resistance has become a significant public health concern. Ceftazidime-avibactam (CAZ-AVI) exhibited excellent in vitro activity against many carbapenemase-producing pathogens, and was widely used for the treatment of various complicated infections. CAZ-AVI is well tolerated across all dosing regimens, and its associated acute kidney injury (AKI) in phase II/III clinical trials is rare. However, recent real-world studies have demonstrated that CAZ-AVI associated AKI was more frequent in real-world than in phase II and III clinical trials, particularly in patients receiving concomitant nephrotoxic agents, with critically ill patients being at a higher risk. Herein, we reviewed the safety data related to renal impairment of CAZ-AVI, and discussed its pharmacokinetic/pharmacodynamic targets and dosage adjustment in patients with impaired renal function. This review aimed to emphasize the importance for healthcare professionals to be aware of this adverse event of CAZ-AVI and provide practical insights into the dosage optimization in critically ill patients with renal dysfunction.
Antimicrobial resistance has become a significant global public health concern, with the escalating prevalence of multidrug-resistant (MDR) Gram-negative bacterial pathogens worldwide, especially of carbapenemase-producing pathogens, including carbapenem-resistant Enterobacteriaceae (CRE), carbapenem-resistant Pseudomonas aeruginosa (CRPA), and carbapenem-resistant Acinetobacter baumannii (CRAB) (Zowawi et al., 2015). The emergence and spread of these carbapenemase-producing pathogens thus posed serious clinical treatment challenges and spurred renewed efforts to develop novel antimicrobial agents to treat such infections.
Ceftazidime-avibactam (CAZ-AVI) is an intravenously administered antimicrobial consisting of a third-generation cephalosporin ceftazidime and a novel non-β-lactam β-lactamase inhibitor avibactam, at a fixed ceftazidime: avibactam ratio of 4:1 (Shirley, 2018). It exhibited excellent in vitro activity against many extended-spectrum β-lactamase (ESBL)-, Klebsiella pneumoniae carbapenemase (KPC)-, AmpC-, and OXA-48-producing bacteria, including Enterobacteriaceae and P. aeruginosa, while showed no activity against metallo-β-lactamase (MBL)-producing strains or most Acinetobacter spp. isolates (Ehmann et al., 2012; Berkhout et al., 2015; Levasseur et al., 2015). CAZ-AVI has been demonstrated the clinical efficacy for the treatment of adults with complicated intra-abdominal infection (cIAI), complicated urinary tract infection (cUTI) [including pyelonephritis], hospital-acquired pneumonia (HAP) [including ventilator-associated pneumonia (VAP)], as well as other infections caused by aerobic Gram-negative organisms in patients with limited treatment options, ever since been approved by US Food and Drug Administration (FDA) in 2015 (Shirley, 2018).
CAZ-AVI was generally well tolerated with most adverse events (AEs) being of mild to moderate intensity. Overall, the most commonly reported AEs (occurring in ≥ 5% of patients) across phase II and III clinical trials were positive direct Coombs test, nausea, and diarrhea. The reported frequency of acute kidney injury (AKI) ranged from 0.1% to 1% in its prescribing information. However, accumulating evidence suggests that the incidence of AKI in real-world experience is much higher (Shirley, 2018). Thus, we summarized and discussed the current evidence regarding on CAZ-AVI induced renal disorders and its dosage adjustment in patients with impaired renal function.
The clinical efficacy and safety of ceftazidime-avibactam in the treatment of cUTI, cIAI, and HAP (including VAP) was demonstrated in phase II and III trials with carbapenem comparators. Herein, we summarized CAZ-AVI related renal impairment in clinical trials.
In 2012, Vazquez et al. conducted a phase II study (NCT00690378) to compare the efficacy and safety of CAZ-AVI and imipenem-cilastatin in hospitalized adults with serious cUTI (Vazquez et al., 2012). Over the course of the study, serious adverse events (SAEs) were reported in 6 (8.8%) patients in the CAZ-AVI arm and 2 (3.0%) patients in the imipenem-cilastatin arm, from which acute renal failure was observed in 1 (1.5%) patient in the CAZ-AVI arm, and none was observed in the imipenem-cilastatin arm (Table 1, Entry 1). Bradley et al. evaluated the efficacy and safety of CAZ-AVI in children (≥ 3 months to < 18 years) with cUTI through a phase II study (NCT02497781) in 2019 (Bradley et al., 2019b). Similarly, nephrolithiasis was observed in 1 (1.5%) patient in the CAZ-AVI arm and none was observed in the cefepime arm (Table 1, Entry 2). However, in the phase III RECAPTURE program (Wagenlehner et al., 2016) and REPRISE trial (Carmeli et al., 2016) that compared the efficacy and safety of CAZ-AVI and carbapenems in patients with cUTI (REPRISE trial also analyzed the patients with cIAI), no renal impairment was reported (Table 1, Entries 3–4).
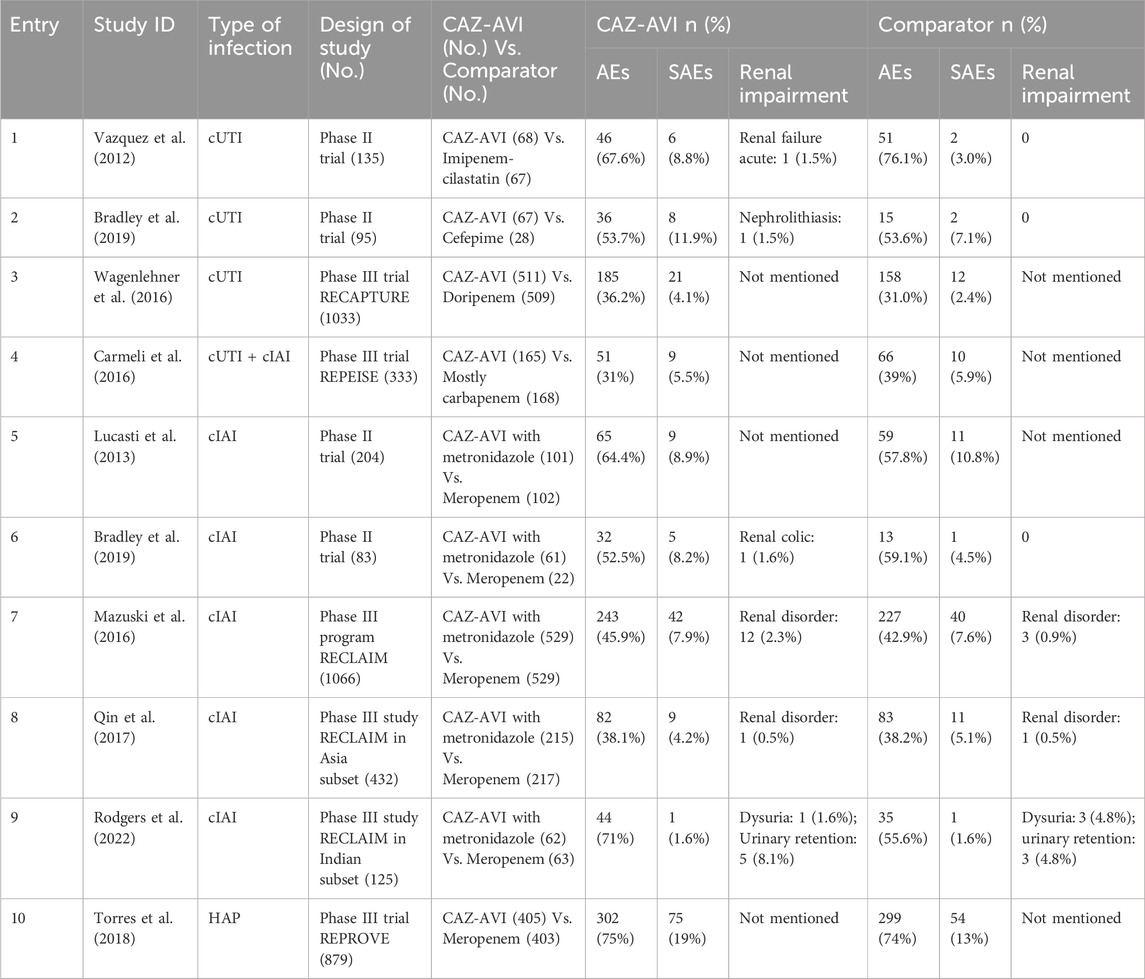
TABLE 1. Summary of CAZ-AVI associated renal impairment in phase II and III clinical trials.
In 2013, Lucasti et al. conducted a phase II trial (NCT 00752219) aimed to evaluate the safety and efficacy the CAZ-AVI plus metronidazole compared with meropenem in hospitalized patients with cIAI (Lucasti et al., 2013). The incidence of treatment-emergent AEs was similar to each other, and no renal failure was observed (Table 1, Entry 5). In another phase II study (NCT02475733), Bradley et al. also evaluated the safety and efficacy of CAZ-AVI plus metronidazole compared with meropenem in children with cIAI (Bradley et al., 2019), and renal colic occurred in 1 (1.6%) patient in CAZ-AVI plus metronidazole group (Table 1, Entry 6). In 2016, Mazuski et al. conducted a multicenter global phase III RECLAIM program that enrolled 1066 patients with cIAI and proved that CAZ-AVI plus metronidazole was non-inferior to meropenem across all populations (Mazuski et al., 2016). AEs occurred at a similar frequency in the two treatment groups, and renal disorders were observed in 12 (2.3%) and 3 (0.9%) patients in the CAZ-AVI plus metronidazole and meropenem arms, respectively (Table 1, Entry 7). Qin et al. and Rodgers et al. reinvestigated the safety and efficacy results of the Asian and Indian population subset from the RECLAIM trial (Qin et al., 2017; Rodgers et al., 2022). In the Asian subset, renal disorder was observed in 1 (0.5%) patient in both groups, while in the Indian subset, dysuria and urinary retention were newly reported (Table 1, Entries 8–9).
In 2018, Torres et al. conducted a phase III REPROVE trial to assess the efficacy and safety of CAZ-AVI in patients with nosocomial pneumonia, compared with meropenem (Torres et al., 2018). SAEs occurred in 75 (19%) patients in the CAZ-AVI arm and 54 (13%) patients in the meropenem arm, while renal disorders were not mentioned in both groups (Table 1, Entry 10).
In a word, renal impairment was rare in patients treated with CAZ-AVI in phase II and III clinical trials, although slightly higher than in the carbapenems group.
As mentioned above, CAZ-AVI showed potent activity against class A (including ESBLs and KPC-type carbapenemases), class C (AmpC), and some class D (including OXA-48) β-lactamase-producing bacteria, mainly belong to CRE and CRPA. Herein, we summarized the safety data related to renal impairment reported in real-world for MDR Gram-negative infections (MDR-GNIs), as well as the safety data in the critically ill patients. We also compared the data about the incidence of AKI among patients receiving CAZ-AVI or polymyxins in the treatment of MDR-GNIs.
In 2019, Jorgensen et al. conducted a multicenter, retrospective cohort study that enrolled 203 patients treated with CAZ-AVI for MDR-GNIs, from which CRE and CRPA were isolated from 117 (57.6%) and 63 (31.0%) culture specimens, respectively (Jorgensen et al., 2019). With regards to safety, 10 (4.9%) patients developed AKI, and 9 of them were receiving concomitant nephrotoxic agents (especially aminoglycosides or polymyxins) around the time of the event (Table 2, Entry 1).
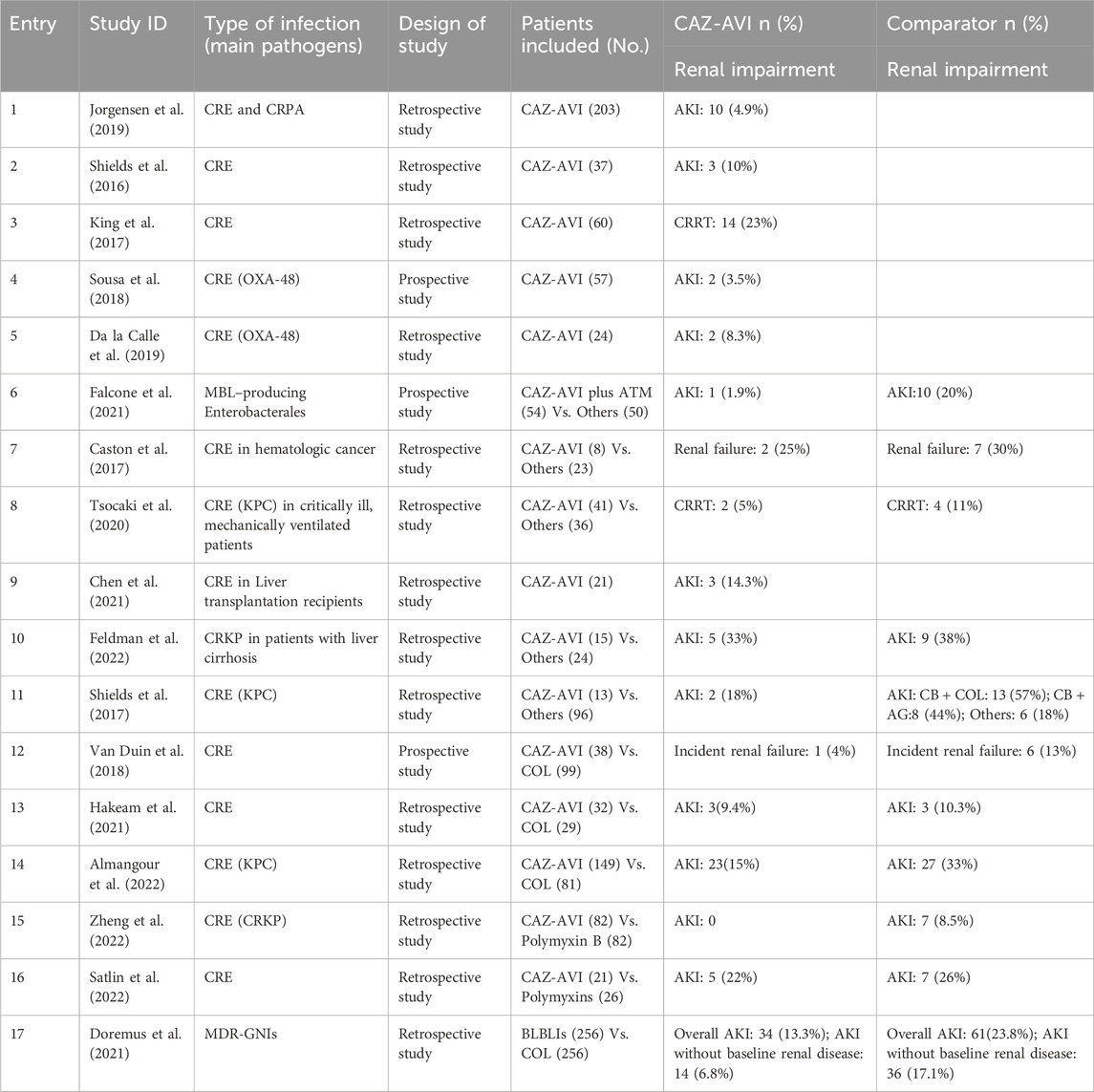
TABLE 2. Summary of CAZ-AVI associated renal impairment in real-world studies.
For the treatment of patients with CRE infection, Shields et al. conducted a retrospective study enrolled 37 patients in 2016 (Shields et al., 2016), and mentioned that 3 (10%) patients developed AKI, including 1 patient in combination with colistin (COL) (Table 2, Entry 2). In 2017, King et al. also described a retrospective review of 60 patients with CRE infection, from which 33 (55%) patients required renal dose adjustment, and 14 (23.3%) of these patients underwent further continuous renal replacement therapy (CRRT) (King et al., 2017) (Table 2, Entry 3).
Although KPC-type carbapenemase-producing Enterobacterales (CPE) were the most frequently isolated organisms, the experience in the treatment for OXA-48 CPE has also been reported. Sousa et al. designed a prospective observational study that enrolled 57 patients receiving CAZ-AVI for any infection produced by OXA-48 CPE (Sousa et al., 2018), and 2 (3.5%) patients developed AKI with one of them on concomitant COL during the treatment (Table 2, Entry 4). Da la Calle et al. also reviewed the characteristics of OXA-48 CPE infection (De la Calle et al., 2019), and 2 (8.3%) patients showed impaired renal function with neurological symptoms (Table 2, Entry 5). On the other hand, CAZ-AVI plus aztreonam (ATM) has also been considered as a potential therapeutic option for metallo-β-lactamase (MBL)-producing Enterobacterales. Falcone et al. conducted a prospective study enrolled 102 patients with bloodstream infections (BSI) due to MBL-producing Enterobacterales (Falcone M et al., 2021), and 1 (1.9%) patient developed drug-induced AKI (Table 2, Entry 6).
Critically ill patients, characterized by immune suppression, are a particularly vulnerable subpopulation to MDR-GNIs during hospitalization and after hospital discharge. Thus, the safety data of CAZ-AVI in these patients were also reviewed. Castón et al. (2017) conducted a multicenter retrospective study that included 31 patients with hematologic malignancies, from which 8 patients received CAZ-AVI treatment and two of them (25%) developed renal failure during treatment (Table 2, Entry 7). In 2020, Tsolaki et al. conducted a retrospective observational cohort study to evaluate the effectiveness of CAZ-AVI in critically ill, mechanically ventilated patients (Tsolaki et al., 2020), and 2 (5%) patients in the CAZ-AVI group required initiation of CRRT (Table 2, Entry 8). Liver transplantation (LT) recipients with carbapenem-resistant Klebsiella pneumoniae (CRKP) infection who received CAZ-AVI treatment were also reviewed retrospectively, and AEs were assessed by Haomin Zhang group (Chen et al., 2021). Three (14.3%) patients developed AKI, and two of them need further hemodialysis (Table 2, Entry 9). Recently, Feldman et al. also conducted a retrospective analysis that enrolled 39 patients with liver cirrhosis and CRKP infection (Feldman et al., 2022), and 5 (33%) patients in the CAZ-AVI group developed AKI (Table 2, Entry 10).
With the increasing prevalence of antibiotic resistance, polymyxins and CAZ-AVI have been used as the last-line therapeutic option for the treatment of MDR-GNIs, thus a comparison of safety, particularly in renal disorders, between CAZ-AVI and polymyxins was made. In 2017, Shields et al. conducted a retrospective study to compare the outcomes of patients treated with CAZ-AVI versus comparators for CRE infections (Shields et al., 2017). At the end of treatment, AKI rates were 18% (2/11), 57% (13/23), 44% (8/18), and 18% (6/33) for CAZ-AVI, carbapenem (CB) + COL, CB + aminoglycoside (AG), and other regimens, respectively (Table 2, Entry 11). AKI incidence was significantly higher among patients receiving AG or COL, and it was significantly more common with COL-containing than with AG-containing regimens.
In 2018, Van Duin et al. conducted a prospective multicenter study that enrolled 38 patients treated with CAZ-AVI and 99 with COL in the treatment of infections due to CRE (Van Duin et al., 2018). The inverse probability of treatment weighting (IPTW)-adjusted estimates for not observed die with incident renal failure was 4% (1/38) and 13% (6/99) for CAZ-AVI and COL groups, respectively (Table 2, Entry 12). Hakeam et al. conducted a retrospective, multicenter study that included 61 patients with CRE treated with CAZ-AVI or COL (Hakeam et al., 2021), and no difference in AKI development between CAZ-AVI and COL groups was observed (9.4% and 10.3%, respectively) (Table 2, Entry 13). Almangour et al. also compared the safety and effectiveness of CAZ-AVI to COL-based regimen in the treatment of infections caused by CRE (Almangour et al., 2022), while AKI was significantly less common in patients who received CAZ-AVI than COL (15% and 33%, respectively) (Table 2, Entry 14).
Recently, Zhang et al. conducted a retrospective study in two Chinese tertiary hospitals for critically ill patients with CRKP infection who received CAZ-AVI or polymyxin B (PMB)-based treatment (Zheng et al., 2022). According to safety evaluation results, 7 (8.5%) patients developed AKI in the PMB-based group, while AKI was not mentioned in CAZ-AVI-based patients (Table 2, Entry 15). In a study that assessed the impact of a rapid molecular test for KPC, the outcomes of CAZ-AVI and polymyxin (including COL and PMB) targeted therapies were also evaluated (Satlin et al., 2022). 5 (22%) and 7 (26%) patients developed AKI in CAZ-AVI and polymyxin groups, respectively (Table 2, Entry 16). In 2021, Doremus et al. evaluated the incidence of AKI among patients receiving COL or novel β-lactam β-lactamase inhibitors (BLBLIs). The overall AKI incidence was 13.3% and 23.8% in BLBLIs and COL groups, respectively (Doremus et al., 2021). For patients without baseline renal disease, the odds of AKI in patients on COL were three times higher than that of patients receiving BLBLIs agents (17.1% vs. 6.8%) (Table 2, Entry 17).
In short, CAZ-AVI associated AKI was more frequent in real-world than in phase II and III clinical trials. Although the underlying mechanism of CAZ-AVI associated AKI is unclear, it is likely that concomitant nephrotoxin exposure and special disease status may play an essential role.
In 2015, both Das et al. and Merdjan et al. assessed the pharmacokinetic (PK) and safety profiles of CAZ-AVI and whether drug-drug interactions existed between each other (Das et al., 2015; Merdjan et al., 2015). The results indicated that both ceftazidime and avibactam exhibited approximate dose linearity when administered in combination with clinically relevant doses, and the PK of avibactam is unaffected when administered alone or with ceftazidime. On the other hand, neither ceftazidime nor avibactam appear to undergo significant metabolism, and both drugs are primarily eliminated unchanged in the urine (Shirley, 2018). Vishwanathan et al. also evaluated the metabolism and drug-drug interaction potential of ceftazidime and avibactam. They suggested that ceftazidime mainly excreted through glomerular filtration, while the elimination of avibactam involved active tubular secretion in addition to glomerular filtration (Vishwanathan et al., 2014). Additionally, CAZ-AVI shares the typical PK features of β-lactams (BLs), such as hydrophilicity, low plasma protein binding, low molecular weight, and small volume of distribution (VD) (Yahav et al., 2020). Consistently, dosage adjustments are recommended in patients with impaired renal function (Giri et al., 2019).
On the other hand, ceftazidime exhibits time-dependent pharmacodynamics (PD), and its effect is related to the percentage of time that free drug concentration remains above the minimum inhibitory concentration (MIC) of the targeted pathogen (% fT > MIC) (Sader et al., 2017; Nichols et al., 2018a). For avibactam (in combination with ceftazidime), the PK/PD index was defined as the free time above a critical concentration(CT)below which sufficient inhibition of ceftazidime was lost (% fT > CT) (Coleman et al., 2014; Berkhout et al., 2016; Nichols et al., 2018b). Ceftazidime and avibactam were coadministered in a fixed dose ratio (4:1), and a joint probability of target attainment (PTA) was calculated to guide the dosage regimen selection and validation on the basis of the simultaneous achievement of separate PK/PD targets and population PK modeling through Monte Carlo simulation (Li et al., 2018; Gatti et al., 2024). According to the nonclinical studies, the joint PTA of CAZ-AVI was defined as ceftazidime 50% fT > 8 mg/L and avibactam 50% fT > 1 mg/L, and dosage selection was dependent on the achievement of a high (>90%) joint PTA (Li et al., 2018; Das et al., 2019; Li et al., 2020). In a phase III clinical trial, the joint PTA analyses supported the CAZ-AVI dosage regimen of 2.5 g q8 h for patients with estimated creatinine clearance (CrCl) above 50 mL/min, and modified dosage adjustment for patients with moderate or severe renal impairment (CrCl < 50 mL/min) (Li et al., 2020).
In consideration of the fact that the degree of renal dysfunction is an essential factor in dosage adjustment for patients with renal impairment, we are wondering how to conduct renal dosage adjustment to achieve equivalent exposures in patients with AKI. Indeed, a phase I study demonstrated that increased severity of renal impairment was associated with decreased total plasma clearance (CL) of avibactam, as previously observed for ceftazidime (Nicolau et al., 2015). However, a Phase III clinical study suggested that in patients with moderate renal dysfunction, the efficacy of CAZ-AVI was worse than that of meropenem, which was related to insufficient dosage of CAZ-AVI (Mazuski et al., 2016). In this trial, patients with normal kidney function receiving 2.5 g q8 h CAZ-AVI showed a higher response rate compared to patients with moderate renal impairment treated with 1.25 g q12 h. Moreover, in patients with moderate renal impairment, there was a lower response rate in the CAZ-AVI arm (1.25 g q12 h) in comparison with the meropenem arm (1 g q12 h; 45.2% vs. 74.3%; p = 0.016), which potentially was a result of a higher proportional dose reduction in CAZ-AVI arm than in meropenem arm (66% vs. 33%). Notably, among patients with moderate renal impairment at baseline, 67.9% showed improvements to CrCl above 50 mL/min within 48–72 h (Mazuski et al., 2016). Consequently, the recommended dose of CAZ-AVI in patients with moderate renal impairment was increased from 1.25 g q12 h to 1.25 g q8 h based on the above-mentioned PK/PD targets to achieve a higher joint PTA (Li et al., 2020). Likewise, the modified dosage adjustment was validated in another phase III trial (Torres et al., 2018) and thus applied in real-world experience (Jorgensen et al., 2019). In 2019, Crass et al. (2019) retrospectively reviewed the records of 18,500 patients with infectious diseases, and they identified that the overall rate of AKI on admission was 17.5%, with 57.2% of cases achieving kidney injury resolution by 48 h. Besides that, 47.9% of patients with moderate renal impairment on admission had an improvement of CrCl above 50 mL/min within 48 h (Crass et al., 2019), which was consistent with the results of the above phase III study (Mazuski et al., 2016). These data highlight the dynamic nature of renal function and the potential for rapid recovery in patients with AKI. Therefore, unnecessary dose reduction in the setting of transient AKI may have played a role in the decreased clinical response in patients with moderate renal impairment.
In fact, AKI is a dynamic perturbation of renal steady-state, which makes it challenging to conduct an accurate characterization of patient kidney function. The current renal dose adjustment protocols are based on small, early-phase PK studies that enroll patients with stable chronic kidney disease (CKD) before testing in registered clinical trials. Of note, the most common formulas to evaluate kidney function are Cockcroft-Gault, Modification of Diet in Renal Disease (MDRD), and CKD epidemiology collaboration (CKD-EPI). However, these equations are based on the serum creatine (Scr) under the steady-state conditions and may be inaccurate to estimate renal function in the dynamic setting of AKI. Therefore, these paradigmas are appropriate for maintenance therapeutics in CKD patients, and may overestimate dose reductions for patients with AKI in ultimately clinical practice (Crass et al., 2019). Moreover, the kinetic eGFR equation has also been developed to assess eGFR in the setting of dynamic renal states, which included the magnitude to which Scr concentration was increased or decreased relative to the baseline steady-state value and the rapidity of the variation tendency. Rather than relying on a single Scr concentration, this equation was based on multiple Scr measurements and the mathematics of creatinine mass balance (Chen, 2013). However, it does not take into consideration the creatinine production due to infection and loss of muscle mass, and changes in VD in acutely ill patients (Chen, 2018), as significant alterations of VD may occur in patients with AKI, thus affecting the drug exposure profile (Bidell and Lodise, 2018). As a consequence, the inappropriate empirical dose reduction in the setting of transient AKI may contribute to the decreased clinical response in patients with moderate renal impairment. On the other hand, it has been well documented that adequate antibiotic therapy within the first 48 h is a significant determinant of outcomes for critically ill patients (Leibovici et al., 1998; Lee et al., 2017; Crass et al., 2019). Patients with severe infections often show dynamic changes in CrCl, and prompt recovery of renal function generally occurs within the first 48 h as a result of fluid resuscitation or other supportive care (Gatti and Pea, 2021). Thus, to minimize the risk-to-benefit ratio, standard dosing of CAZ-AVI (2.5 g q8 h) may be optimal for patients with and without renal dysfunction during the first 48 h. Deferral of renal dosage adjustment should be applied only after 48 h for patients with persistent AKI (Lewis and Muller, 2016; Crass et al., 2019; Gorham et al., 2022).
Except for the frequently occurred AKI mentioned in this study, other renal variations are also observed in critically ill patients, like renal replacement therapy (RRT) or augmented renal clearance (ARC), thus data about appropriate dosage regimens based on PK/PD targets are strongly needed under these circumstances (Gatti and Pea, 2021; Gorham et al., 2022). It has been demonstrated that 5%–10% of critically ill patients with AKI eventually require RRT during their hospital stay (Tolwani, 2012). Wenzler et al. (2017) found that a 1.25 g q8 h CAZ-AVI could achieve optimal drug concentrations (100% fT > MIC 6 mg/L) against MDR-GNIs in critically ill patients on continuous venovenous hemofiltration (CVVH). Conversely, in a case report of a 50-year-old critically ill patient with MDR Pseudomonas aeruginosa (MIC 8 mg/L) pneumonia receiving continuous venovenous hemodiafiltration (CVVHDF), only standard drug regimens (2.5 g q8h) could achieve high trough concentrations (Soukup et al., 2019). Moreover, in a study of 77 patients treated with CAZ-AVI for CRE infections, high emergence of resistance was reported in patients requiring RRT, which was defined as an independent predictor of clinical failure and development of resistance (Shields et al., 2018). As such, in critically ill patients receiving RRT, a drug regimen of 1.25 g q8 h could be used for susceptible strains (MIC < 4 mg/L), while higher regimens and/or prolonged infusion, even continuous infusion, should be considered for less susceptible strains (Fresan et al., 2023).
A recent study indicated that ARC may cause higher drug clearance and underexposure, thus resulting in poor clinical outcomes (Cook and Hatton-Kolpek, 2019). A subgroup analysis of 239 patients with ARC included in the REPROVE trial showed that the standard dosage of 2.5 g q8 h over 2 h ensured > 95% PTA of 50% fT > MIC up to 16 mg/L, despite a 35% decrease in drug exposure compared to patients with normal renal function (Torres et al., 2018). In 2019, Stein et al. conducted a PK/PD analysis of CAZ-AVI in 10 critically ill patients, of whom two had ARC. Serum concentrations of ceftazidime and avibactam were measured individually, and optimal joint PTA was achieved under the current dosage regimens of CAZ-AVI, including these two with ARC treated with 2.5 g q8 h over 2 h (Stein et al., 2019). In a study evaluating the efficacy of different CAZ-AVI dosage regimens against some Enterobacteriaceae members and P. aeruginosa by Monte Carlo simulation, patients with ARC failed to reach 90% cumulative fraction of response under the standard dose of 2.5 g q8 h (Dai et al., 2021). This phenomenon was also observed in a therapeutic drug monitoring (TDM) of CAZ-AVI concentration in CRKP-infected patients with different kidney statuses. In this study, two patients with ARC showed lower ceftazidime and avibactam serum concentrations, even though receiving 2.5 g q6 h CAZ-AVI (Teng et al., 2022). These results implied that increased dosing or dose optimization using prolonged duration may be needed in ARC patients to maintain therapeutic exposure.
As mentioned above, only conservative PK/PD targets of ceftazidime 50% fT > MIC 8 mg/L and avibactam 50% fT > CT 1 mg/L were used in phase II/III clinical trials (Li et al., 2018; Das et al., 2019). However, several experiences in critically ill patients reported that higher PK/PD target achievement was related to better clinical outcomes. In 2014, Roberts et al. conducted a prospective study including 384 patients to define BLs levels in critically ill patients, and they found that positive clinical outcome was associated with more aggressive PK/PD targets of 100% fT > MIC compared to 50% fT > MIC (Roberts et al., 2014). Notably, a review describing PK/PD issues associated with renal dose adjustments of CAZ-AVI demonstrated that antibiotic exposure showed a close relationship not only with clinical outcomes but also with the emergence of resistance (Bidell and Lodise, 2018). Therefore, more aggressive PK/PD targets of ceftazidime 100% fT > 4–8 × MIC and avibactam 100% fT > CT 4 mg/L were suggested to maximize bacteriological and clinical response, as well as suppress the emergence of resistance and prevent any toxicity risk (Gatti and Pea, 2021). This suggestion was consistent with the guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique—SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Société Française d’Anesthésie et Réanimation—SFAR) for the optimization of BLs in critically ill patients (Guilhaumou et al., 2019). Furthermore, according to a recent definition, the joint PK/PD targets of CAZ-AVI were considered optimal when ceftazidime 100% fT > 4 × MIC and avibactam 100% fT > CT 4 mg/L (Gatti et al., 2023). Unfortunately, several risk factors, especially the variation in renal function, render the achievement of aggressive PK/PD targets unpredictable in critically ill patients. Hence, TDM-guided dosage adjustment may represent a helpful tool for achieving aggressive PK/PD targets, thus maximizing effectiveness and minimizing toxicity and resistance development (Gatti and Pea, 2021).
In sum, although alternative dosing strategies based on multiple daily dosing coupled with prolonged infusion may represent the best approach to maximize the time-dependent antimicrobial activity of BLs. However, it is worth noting that clinicians still face several challenges when making dosage optimization of CAZ-AVI, especially among critically ill renal patients. In all of the scenarios as mentioned above, implementation of adaptive real-time TDM focused on attaining more aggressive PK/PD targets of ceftazidime 100% fT > 4–8 × MIC and avibactam 100% fT > CT 4 mg/L may be the most powerful strategy in maximizing the clinical response and in preventing the development of resistance.
CAZ-AVI was used for the treatment of cUTI, cIAI, HAP, and other infections caused by aerobic Gram-negative bacteria in patients with limited treatment options. It is an intravenously administered combination of ceftazidime and avibactam, which can be almost completely eliminated through glomerular filtration. In this review, we collected the safety data related to renal impairment from clinical trials and real-world studies. The results indicated that the incidence of AKI in real-world was significantly higher than reported in the local prescribing information. Therefore, CAZ-AVI should receive particular attention as a possible cause of renal disorders, especially for critically ill patients or concomitant administration with other nephrotic agents, such as polymyxin and aminoglycosides. Notably, AKI is transient in the majority of cases and may resolve within the first 48 h. Therefore, inappropriate dose reduction in this window may result in increased clinical failure. To minimize toxicity without compromising efficacy, we suggest an unadjusted dosing for 48 h with a subsequent renal dose reduction if renal impairment persists. Whether transient or persistent, renal impairment should be thoroughly evaluated so as to make informed decisions related to renal dosage adjustment. Besides, appropriate dosage adjustment should also be carefully taken into consideration in critically ill patients with ARC or requiring RRT. TDM-guided dosage optimization intended to achieve more aggressive PK/PD targets of ceftazidime 100% fT > 4–8 × MIC and avibactam 100% fT > CT 4 mg/L may represent a helpful strategy in maximizing clinical response and minimizing toxicity and resistance development.
YS: Data curation, Investigation, Methodology, Writing–original draft, Formal Analysis. JW: Conceptualization, Writing–review and editing. WM: Data curation, Investigation, Writing–original draft. XZ: Data curation, Investigation, Writing–original draft. XR: Data curation, Investigation, Writing–original draft. CS: Writing–review and editing, Supervision. CL: Conceptualization, Writing–review and editing, Supervision, Formal Analysis.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Natural Science Foundation of Shandong Province, China (Nos ZR2022QH109, ZR2023LSW013, and ZR2023MH077), and the National Natural Science Foundation of China (82104016).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Almangour, T. A., Ghonem, L., Aljabri, A., Alruwaili, A., Al Musawa, M., Damfu, N., et al. (2022). Ceftazidime-avibactam versus colistin for the treatment of infections due to carbapenem-resistant Enterobacterales: a multicenter cohort study. Infect. Drug Resist. 15, 211–221. doi:10.2147/idr.s349004
Berkhout, J., Melchers, M. J., Van Mil, A. C., Nichols, W. W., and Mouton, J. W. (2015). In vitro activity of ceftazidime-avibactam combination in in vitro checkerboard assays. Antimicrob. Agents Chemother. 59, 1138–1144. doi:10.1128/aac.04146-14
Berkhout, J., Melchers, M. J., van Mil, A. C., Seyedmousavi, S., Lagarde, C. M., Schuck, V. J., et al. (2016). Pharmacodynamics of ceftazidime and avibactam in neutropenic mice with thigh or lung infection. Antimicrob. Agents Chemother. 60, 368–375. doi:10.1128/aac.01269-15
Bidell, M. R., and Lodise, T. P. (2018). Suboptimal clinical response rates with newer antibiotics among patients with moderate renal impairment: review of the literature and potential pharmacokinetic and pharmacodynamic considerations for observed findings. Pharmacotherapy 38, 1205–1215. doi:10.1002/phar.2184
Bradley, J. S., Broadhurst, H., Cheng, K., Mendez, M., Newell, P., Prchlik, M., et al. (2019). Safety and efficacy of ceftazidime-avibactam plus metronidazole in the treatment of children ≥3 Months to <18 Years with complicated intra-abdominal infection: results from a phase 2, randomized, controlled trial. Pediatr. Infect. Dis. 38, 816–824. doi:10.1097/inf.0000000000002392
Bradley, J. S., Roilides, E., Broadhurst, H., Cheng, K., Huang, L.-M., MasCasullo, V., et al. (2019). Safety and efficacy of ceftazidime–avibactam in the treatment of children ≥3 Months to <18 Years with complicated urinary tract infection: results from a phase 2 randomized, controlled trial. Pediatr. Infect. Dis. 38, 920–928. doi:10.1097/inf.0000000000002395
Carmeli, Y., Armstrong, J., Laud, P. J., Newell, P., Stone, G., Wardman, A., et al. (2016). Ceftazidime-avibactam or best available therapy in patients with ceftazidime-resistant Enterobacteriaceae and Pseudomonas aeruginosa complicated urinary tract infections or complicated intra-abdominal infections (REPRISE): a randomised, pathogen-directed, phase 3 study. Lancet Infect. Dis. 16, 661–673. doi:10.1016/s1473-3099(16)30004-4
Castón, J. J., Lacort-Peralta, I., Martín-Dávila, P., Loeches, B., Tabares, S., Temkin, L., et al. (2017). Clinical efficacy of ceftazidime/avibactam versus other active agents for the treatment of bacteremia due to carbapenemase-producing Enterobacteriaceae in hematologic patients. Int. J. Infect. Dis. 59, 118–123. doi:10.1016/j.ijid.2017.03.021
Chen, F., Zhong, H., Yang, T., Shen, C., Deng, Y., Han, L., et al. (2021). Ceftazidime-avibactam as salvage treatment for infections due to carbapenem-resistant Klebsiella pneumoniae in liver transplantation recipients. Infect. Drug Resist. 14, 5603–5612. doi:10.2147/idr.s342163
Chen, S. (2013). Retooling the creatinine clearance equation to estimate kinetic GFR when the plasma creatinine is changing acutely. J. Am. Soc. Nephrol. 24, 877–888. doi:10.1681/asn.2012070653
Chen, S. (2018). Kinetic glomerular filtration rate in routine clinical practice—applications and possibilities. Adv. Chronic Kidney Dis. 25, 105–114. doi:10.1053/j.ackd.2017.10.013
Coleman, K., Levasseur, P., Girard, A. M., Borgonovi, M., Miossec, C., Merdjan, H., et al. (2014). Activities of ceftazidime and avibactam against β-lactamase-producing Enterobacteriaceae in a hollow-fiber pharmacodynamic model. Antimicrob. Agents Chemother. 58, 3366–3372. doi:10.1128/aac.00080-14
Cook, A. M., and Hatton-Kolpek, J. (2019). Augmented renal clearance. Pharmacotherapy 39, 346–354. doi:10.1002/phar.2231
Crass, R. L., Rodvold, K. A., Mueller, B. A., and Pai, M. P. (2019). Renal dosing of antibiotics: are we jumping the gun? Clin. Infect. Dis. 68, 1596–1602. doi:10.1093/cid/ciy790
Dai, Y., Chang, W., Zhou, X., Yu, W., Huang, C., Chen, Y., et al. (2021). Evaluation of ceftazidime/avibactam administration in enterobacteriaceae and Pseudomonas aeruginosa bloodstream infections by Monte Carlo simulation. Drug Des. devel. Ther. 15, 2899–2905. doi:10.2147/dddt.s309825
Das, S., Li, J., Armstrong, J., Learoyd, M., and Edeki, T. (2015). Randomized pharmacokinetic and drug–drug interaction studies of ceftazidime, avibactam, and metronidazole in healthy subjects. Pharmacol. Res. Perspect. 3, e00172. doi:10.1002/prp2.172
Das, S., Li, J., Riccobene, T., Carrothers, T. J., Newell, P., Melnick, D., et al. (2019). Dose selection and validation for ceftazidime-avibactam in adults with complicated intra-abdominal infections, complicated urinary tract infections, and nosocomial pneumonia. Antimicrob. Agents Chemother. 63, e02187-18. doi:10.1128/AAC.02187-18
De la Calle, C., Rodríguez, O., Morata, L., Marco, F., Cardozo, C., García-Vidal, C., et al. (2019). Clinical characteristics and prognosis of infections caused by OXA-48 carbapenemase-producing Enterobacteriaceae in patients treated with ceftazidime-avibactam. Int. J. Antimicrob. Agents. 53, 520–524. doi:10.1016/j.ijantimicag.2018.11.015
Doremus, C., Marcella, S. W., Cai, B., and Echols, R. M. (2021). Utilization of colistin versus β-lactam and β-lactamase inhibitor agents in relation to acute kidney injury in patients with severe gram-negative infections. J. Infect. Dis. Ther. 11, 187–199. doi:10.1007/s40121-021-00556-x
Ehmann, D. E., Jahić, H., Ross, P. L., Gu, R.-F., Hu, J., Kern, G., et al. (2012). Avibactam is a covalent, reversible, non-β-lactam β-lactamase inhibitor. Proc. Natl. Acad. Sci. 109, 11663–11668. doi:10.1073/pnas.1205073109
Falcone, M., Daikos, G. L., Tiseo, G., Bassoulis, D., Giordano, C., Galfo, V., et al. (2021). Efficacy of ceftazidime-avibactam plus aztreonam in patients with bloodstream infections caused by metallo-β-lactamase-producing Enterobacterales. Clin. Infect. Dis. 72, 1871–1878. doi:10.1093/cid/ciaa586
Feldman, S., Russo, A., Ceccarelli, G., Borrazzo, C., Madge, C., Venditti, M., et al. (2022). Ceftazidime-avibactam for the treatment of carbapenem-resistant Klebsiella pneumoniae infections in patients with liver cirrhosis. J. Clin. Exp. Hepatol. 12, 1293–1300. doi:10.1016/j.jceh.2022.04.016
Fresan, D., Luque, S., Benítez-Cano, A., Sorlí, L., Milagro Montero, M., De-Antonio, M., et al. (2023). Pharmacokinetics/pharmacodynamics and therapeutic drug monitoring of ceftazidime/avibactam administered by continuous infusion in patients with MDR Gram-negative bacterial infections. J. Antimicrob. Chemother. 78, 678–683. doi:10.1093/jac/dkac439
Gatti, M., Pascale, R., Cojutti, P. G., Rinaldi, M., Ambretti, S., Conti, M., et al. (2023). A descriptive pharmacokinetic/pharmacodynamic analysis of continuous infusion ceftazidime-avibactam in a case series of critically ill renal patients treated for documented carbapenem-resistant Gram-negative bloodstream infections and/or ventilator-associated pneumonia. Int. J. Antimicrob. Agents. 61, 106699. doi:10.1016/j.ijantimicag.2022.106699
Gatti, M., and Pea, F. (2021). Pharmacokinetic/pharmacodynamic target attainment in critically ill renal patients on antimicrobial usage: focus on novel beta-lactams and beta lactams/beta-lactamase inhibitors. Expert Rev. Clin. Pharmacol. 14, 583–599. doi:10.1080/17512433.2021.1901574
Gatti, M., Viale, P., and Pea, F. (2024). Therapeutic drug monitoring of ceftazidime/avibactam: why one leg is not enough to run. J. Antimicrob. Chemother. 79, 195–199. doi:10.1093/jac/dkad367
Giri, P., Patel, H., and Srinivas, N. R. (2019). Review of clinical pharmacokinetics of avibactam, A newly approved non-β lactam β-lactamase inhibitor drug, in combination use with ceftazidime. Drug Res. (Stuttg). 69, 245–255. doi:10.1055/a-0748-5548
Gorham, J., Taccone, F. S., and Hites, M. (2022). Drug regimens of novel antibiotics in critically ill patients with varying renal functions: a rapid review. Antibiotics 11, 546. doi:10.3390/antibiotics11050546
Guilhaumou, R., Benaboud, S., Bennis, Y., Dahyot-Fizelier, C., Dailly, E., Gandia, P., et al. (2019). Optimization of the treatment with beta-lactam antibiotics in critically ill patients—guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique—SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Société Française d’Anesthésie et Réanimation—SFAR). Crit. Care 23, 104. doi:10.1186/s13054-019-2378-9
Hakeam, H. A., Alsahli, H., Albabtain, L., Alassaf, S., Al Duhailib, Z., and Althawadi, S. (2021). Effectiveness of ceftazidime–avibactam versus colistin in treating carbapenem-resistant Enterobacteriaceae bacteremia. Int. J. Infect. Dis. 109, 1–7. doi:10.1016/j.ijid.2021.05.079
Jorgensen, S. C. J., Trinh, T. D., Zasowski, E. J., Lagnf, A. M., Bhatia, S., Melvin, S. M., et al. (2019). Real-world experience with ceftazidime-avibactam for multidrug-resistant gram-negative bacterial infections. Open Forum Infect. Dis. 6, ofz522. ofz522. doi:10.1093/ofid/ofz522
King, M., Heil, E., Kuriakose, S., Bias, T., Huang, V., El-Beyrouty, C., et al. (2017). Multicenter study of outcomes with ceftazidime-avibactam in patients with carbapenem-resistant enterobacteriaceae infections. Antimicrob. Agents Chemother. 61, 004499–e517. doi:10.1128/aac.00449-17
Lee, C. C., Lee, C. H., Hong, M. Y., Tang, H. J., and Ko, W. C. (2017). Timing of appropriate empirical antimicrobial administration and outcome of adults with community-onset bacteremia. Crit. Care 21, 119–128. doi:10.1186/s13054-017-1696-z
Leibovici, I., Shraga, I., Drucker, M., Konigsberger, H., Samra, Z., Pitlik, S. D., et al. (1998). The benefit of appropriate empirical antibiotic treatment in patients with bloodstream infection. J. Intern Med. 244, 379–386. doi:10.1046/j.1365-2796.1998.00379.x
Levasseur, P., Girard, A.-M., Miossec, C., Pace, J., and Coleman, K. (2015). In vitro antibacterial activity of the ceftazidime-avibactam combination against enterobacteriaceae, including strains with well-characterized β-lactamases. Antimicrob. Agents Chemother. 59, 1931–1934. doi:10.1128/aac.04218-14
Lewis, S. J., and Mueller, B. A. (2016). Antibiotic dosing in patients with acute kidney injury: "enough but not too much. J. Intensive Care Med. 31, 164–176. doi:10.1177/0885066614555490
Li, J., Lovern, M., Green, M. L., Chiu, J., Zhou, D., Comisar, C., et al. (2018). Ceftazidime-avibactam population pharmacokinetic modeling and pharmacodynamic target attainment across adult indications and patient subgroups. Clin. Transl. Sci. 12, 151–163. doi:10.1111/cts.12585
Li, J., Lovern, M., Riccobene, T., Carrothers, T. J., Newell, P., Das, S., et al. (2020). Considerations in the selection of renal dosage adjustments for patients with serious infections and lessons learned from the development of ceftazidime-avibactam. Antimicrob. Agents Chemother. 64, e02105-19. doi:10.1128/aac.02105-19
Lucasti, C., Popescu, I., Ramesh, M. K., Lipka, J., and Sable, C. (2013). Comparative study of the efficacy and safety of ceftazidime/avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infections in hospitalized adults: results of a randomized, double-blind, Phase II trial. J. Antimicrob. Chemother. 68, 1183–1192. doi:10.1093/jac/dks523
Mazuski, J. E., Gasink, L. B., Armstrong, J., Broadhurst, H., Stone, G. G., Rank, D., et al. (2016). Efficacy and safety of ceftazidime-avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infection: results from a randomized, controlled, double-blind, phase 3 program. Clin. Infect. Dis. 62, 1380–1389. doi:10.1093/cid/ciw133
Merdjan, H., Rangaraju, M., and Tarral, A. (2015). Safety and pharmacokinetics of single and multiple ascending doses of avibactam alone and in combination with ceftazidime in healthy male volunteers: results of two randomized, placebo-controlled studies. Clin. Drug Invest. 35, 307–317. doi:10.1007/s40261-015-0283-9
Nichols, W. W., Newell, P., Critchley, I. A., Riccobene, T., and Das, S. (2018a). Avibactam pharmacokinetic/pharmacodynamic targets. Pharmacodyn. Targets. Antimicrob. Agents Chemother. 62, e02446-17. doi:10.1128/aac.02446-17
Nichols, W. W., Stone, G. G., Newell, P., Broadhurst, H., Wardman, A., MacPherson, M., et al. (2018b). Ceftazidime-avibactam susceptibility breakpoints against enterobacteriaceae and Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 62, e02590–e02517. doi:10.1128/AAC.02590-17
Nicolau, D. P., Siew, L., Armstrong, J., Li, J., Edeki, T., Learoyd, M., et al. (2015). Phase 1 study assessing the steady-state concentration of ceftazidime and avibactam in plasma and epithelial lining fluid following two dosing regimens. J. Antimicrob. Chemother. 70, 2862–2869. doi:10.1093/jac/dkv170
Qin, X., Tran, B. G., Kim, M. J., Wang, L., Nguyen, D. A., Chen, Q., et al. (2017). A randomised, double-blind, phase 3 study comparing the efficacy and safety of ceftazidime/avibactam plus metronidazole versus meropenem for complicated intra-abdominal infections in hospitalised adults in Asia. Int. J. Antimicrob. Agents. 49, 579–588. doi:10.1016/j.ijantimicag.2017.01.010
Roberts, J. A., Paul, S. K., Akova, M., Bassetti, M., De Waele, J. J., Dimopoulos, G., et al. (2014). DALI: defining antibiotic levels in intensive care unit patients: are current -lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. 58, 1072–1083. doi:10.1093/cid/ciu027
Rodgers, P., Kamat, S., and Adhav, C. (2022). Ceftazidime-avibactam plus metronidazole vs. meropenem in complicated intra-abdominal infections: Indian subset from RECLAIM. J. Infect. Dev. Ctries. 16, 305–313. doi:10.3855/jidc.14912
Sader, H. S., Castanheira, M., Shortridge, D., Mendes, R. E., and Flamm, R. K. (2017). Antimicrobial activity of ceftazidime-avibactam tested against multidrug-resistant enterobacteriaceae and Pseudomonas aeruginosa isolates from U.S. Medical centers, 2013 to 2016. Antimicrob. Agents Chemother. 61, e01045-17. doi:10.1128/aac.01045-17
Satlin, M. J., Chen, L., Gomez-Simmonds, A., Marino, J., Weston, G., Bhowmick, T., et al. (2022). Impact of a rapid molecular test for Klebsiella pneumoniae carbapenemase and ceftazidime-avibactam use on outcomes after bacteremia caused by carbapenem-resistant Enterobacterales. Clin. Infect. Dis. 75, 2066–2075. doi:10.1093/cid/ciac354
Shields, R. K., Nguyen, M. H., Chen, L., Press, E. G., Kreiswirth, B. N., and Clancy, C. J. (2018). Pneumonia and renal replacement therapy are risk factors for ceftazidime-avibactam treatment failures and resistance among patients with carbapenem-resistant enterobacteriaceae infections. Antimicrob. Agents Chemother. 62, e02497-17. doi:10.1128/aac.02497-17
Shields, R. K., Nguyen, M. H., Chen, L., Press, E. G., Potoski, B. A., Marini, R. V., et al. (2017). Ceftazidime-avibactam is superior to other treatment regimens against carbapenem-resistant Klebsiella pneumoniae bacteremia. Antimicrob. Agents Chemother. 61, e00883-17. doi:10.1128/aac.00883-17
Shields, R. K., Potoski, B. A., Haidar, G., Hao, B., Doi, Y., Chen, L., et al. (2016). Clinical outcomes, drug toxicity, and emergence of ceftazidime-avibactam resistance among patients treated for carbapenem-resistant enterobacteriaceae infections. Clin. Infect. Dis. 63, 1615–1618. doi:10.1093/cid/ciw636
Shirley, M. (2018). Ceftazidime-avibactam: a review in the treatment of serious gram-negative bacterial infections. Drugs 78, 675–692. doi:10.1007/s40265-018-0902-x
Soukup, P., Faust, A. C., Edpuganti, V., Putnam, W. C., and McKinnell, J. A. (2019). Steady-state ceftazidime-avibactam serum concentrations and dosing recommendations in a critically ill patient being treated for Pseudomonas aeruginosa pneumonia and undergoing continuous venovenous hemodiafiltration. Pharmacotherapy 39, 1216–1222. doi:10.1002/phar.2338
Sousa, A., Pérez-Rodríguez, M. T., Soto, A., Rodríguez, L., Pérez-Landeiro, A., Martínez-Lamas, L., et al. (2018). Effectiveness of ceftazidime/avibactam as salvage therapy for treatment of infections due to OXA-48 carbapenemase-producing Enterobacteriaceae. J. Antimicrob. Chemother. 73, 3170–3175. doi:10.1093/jac/dky295
Stein, G. E., Smith, C. L., Scharmen, A., Kidd, J. M., Cooper, C., Kuti, J., et al. (2019). Pharmacokinetic and pharmacodynamic analysis of ceftazidime/avibactam in critically ill patients. Surg. Infect. 20, 55–61. doi:10.1089/sur.2018.141
Teng, X. Q., Qu, Q., Luo, Y., Long, W. M., Zhuang, H. H., Xu, J. H., et al. (2022). Therapeutic drug monitoring of ceftazidime-avibactam concentrations in carbapenem-resistant K. Pneumoniae-infected patients with different kidney statuses. Front. Pharmacol. 13, 780991. doi:10.3389/fphar.2022.780991
Tolwani, A. (2012). Continuous renal-replacement therapy for acute kidney injury. N. Engl. J. Med. 367, 2505–2514. doi:10.1056/NEJMct1206045
Torres, A., Zhong, N., Pachl, J., Timsit, J. F., Kollef, M., Chen, Z., et al. (2018). Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): a randomised, double-blind, phase 3 non-inferiority trial. Lancet Infect. Dis. 18, 285–295. doi:10.1016/s1473-3099(17)30747-8
Tsolaki, V., Mantzarlis, K., Mpakalis, A., Malli, E., Tsimpoukas, F., Tsirogianni, A., et al. (2020). Ceftazidime-avibactam to treat life-threatening infections by carbapenem-resistant pathogens in critically ill mechanically ventilated patients. Antimicrob. Agents Chemother. 64, e02320-19. doi:10.1128/aac.02320-19
Van Duin, D., Lok, J. J., Earley, M., Cober, E., Richter, S. S., Perez, F., et al. (2018). Colistin versus ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant enterobacteriaceae. Clin. Infect. Dis. 66, 163–171. doi:10.1093/cid/cix783
Vazquez, J. A., González Patzán, L. D., Stricklin, D., Duttaroy, D. D., Kreidly, Z., Lipka, J., et al. (2012). Efficacy and safety of ceftazidime–avibactam versus imipenem–cilastatin in the treatment of complicated urinary tract infections, including acute pyelonephritis, in hospitalized adults: results of a prospective, investigator-blinded, randomized study. Curr. Med. Res. Opin. 28, 1921–1931. doi:10.1185/03007995.2012.748653
Vishwanathan, K., Mair, S., Gupta, A., Atherton, J., Clarkson-Jones, J., Edeki, T., et al. (2014). Assessment of the mass balance recovery and metabolite profile of avibactam in humans and in vitro drug-drug interaction potential. Drug Metab. Dispos. 42, 932–942. doi:10.1124/dmd.113.055335
Wagenlehner, F. M., Sobel, J. D., Newell, P., Armstrong, J., Huang, X., Stone, G. G., et al. (2016). Ceftazidime-avibactam versus doripenem for the treatment of complicated urinary tract infections, including acute pyelonephritis: RECAPTURE, a phase 3 randomized trial program. Clin. Infect. Dis. 63, 754–762. doi:10.1093/cid/ciw378
Wenzler, E., Bunnell, K. L., Bleasdale, S. C., Benken, S., Danziger, L. H., and Rodvold, K. A. (2017). Pharmacokinetics and dialytic clearance of ceftazidime-avibactam in a critically ill patient on continuous venovenous hemofiltration. Antimicrob. Agents Chemother. 61, e00464-17. doi:10.1128/aac.00464-17
Yahav, D., Giska, C. G., Grāmatniece, A., Abodakpi, H., Tam, V. H., and Leibovici, L. (2020). New β-Lactam-β-Lactamase inhibitor combinations. Clin. Microbiol. Rev. 34, e00115–e00120. doi:10.1128/CMR.00115-20
Zheng, G., Cai, J., Zhang, L., Chen, D., Wang, L., Qiu, Y., et al. (2022). Ceftazidime/avibactam-based versus polymyxin B-based therapeutic regimens for the treatment of carbapenem-resistant Klebsiella pneumoniae infection in critically ill patients: a retrospective cohort study. J. Infect. Dis. Ther. 11, 1917–1934. doi:10.1007/s40121-022-00682-0
Keywords: ceftazidime-avibactam, acute kidney injury, clinical trials, real-world studies, pharmacokinetic/pharmacodynamic
Citation: Shi Y, Wu J, Mi W, Zhang X, Ren X, Shen C and Lu C (2024) Ceftazidime-avibactam induced renal disorders: past and present. Front. Pharmacol. 15:1329307. doi: 10.3389/fphar.2024.1329307
Received: 30 October 2023; Accepted: 16 January 2024;
Published: 22 January 2024.
Edited by:
Arnaud Del Bello, Centre Hospitalier Universitaire de Toulouse, FranceReviewed by:
Yongbing Qian, Shanghai Jiao Tong University, ChinaCopyright © 2024 Shi, Wu, Mi, Zhang, Ren, Shen and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cuicui Lu, Y2VjZTIwMjFAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.