 Li Lin
Li Lin Lu Xiao2†
Lu Xiao2† Chen Chen
Chen Chen Anhua Wei
Anhua Wei Wei Li
Wei Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 05 February 2024
Sec. Pharmacology of Anti-Cancer Drugs
Volume 15 - 2024 | https://doi.org/10.3389/fphar.2024.1267763
Background: Immune checkpoint inhibitors (ICIs), either as monotherapy or in combination with chemotherapy, have improved the therapeutic outcome for non-small cell lung cancer (NSCLC). However, the efficacy of combination therapies, such as programmed cell death 1(PD-1)/its ligand (PD-L1) and cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) inhibitors, in targeting different pathways remains unclear. We performed a meta-analysis to determine whether the addition of a CTLA-4 inhibitor to PD-1/PD-L1 therapy improves the efficacy of PD-1/PD-L1 monotherapy in NSCLC.
Methods: We systematically searched various electronic databases for suitable trials. Only randomized controlled trials (RCTs) comparing the clinical efficacy of PD-1/PD-L1 with and without CTLA-4 were included in the analyses. The meta-analysis software RevMan 5.3 was used for statistical analyses.
Results: A total of seven RCTs were retrieved. The results suggested that the combination of CTLA-4 and PD-1/PDL-1 inhibitors did not show enhanced efficacy over PD1/PDL-1 inhibitor monotherapy as determined by overall survival (OS) (HR = 0.98, 95% CI = 0.84–1.14, p = 0.79), progression-free survival (PFS) (HR = 0.92, 95% CI = 0.81–1.06, p = 0.25), and objective response rate (ORR) (HR = 1.08, 95% CI = 0.96–1.21, p = 0.19). Furthermore, the combination immunotherapy was associated increased toxicity as evidenced by increased incidence of any type adverse events (AEs) (RR = 1.06, 95% CI = 1.00–1.13, p = 0.03), grade ≥3 immune-mediated AEs (RR = 1.58, 95% CI = 1.36–1.82, p < 0.05), and treatment discontinuation (RR = 1.83, 95% CI = 1.46–2.28, p < 0.05).
Conclusion: Combining anti-CTLA-4 with anti-PD-1/PD-L1 therapy did not improve the therapeutic efficacy, and was associated with greater toxicity than anti-PD-1/PD-L1 monotherapy in patients with advanced NSCLC. Further investigation of the combination immunotherapy in specific subsets of patients is warranted to identify and define the patient-specific benefits of this combination.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42023435399
In recent years, monoclonal antibodies (mAbs) have revolutionized cancer therapy. Immunotherapy with monoclonal antibodies targeting programmed cell death 1 (PD-1) or its ligand (PD-L1) have become the standard salvage therapy approved for the treatment of advanced non-small cell lung cancer (NSCLC), either as a monotherapy or in combination with chemotherapy (Gandhi et al., 2018; Paz-Ares et al., 2018; Socinski et al., 2018).
Because of the limitations of treatment-related toxicities and PD-L1 tumor proportion score, only a minority of patients demonstrate notable anti-tumor effects (Camidge et al., 2019), and the efficacy of ICI combinations over that of PD-1/PD-L1 monotherapy remains under detable. Some meta-analyses had been done previously. A meta-analysis by Shen et al.reported that the PD-1/PD-L1suppressors in combination with conventional chemotherapy have promising ORR rate and survival efficacy (Shen et al., 2023). Another recent research by Chen et al.demonstrated that PD-1/PD-L1 inhibitors plus anti-angiogenic agents obviously enhance the efficacy and safety as second or later-line therapy in NSCLC (Chen et al., 2023).
Monoclonal immunoglobulin G2 antibodies targeting cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) prevent normal downregulation of T cells and prolong T-cell action, thereby enhancing immune function (Tarhini and Kirkwood, 2008). Previous studies have shown an additive or synergistic antitumor activity of simultaneous blockade of the PD-1/PD-L1 and CTLA-4 pathways, and support the combination as a therapeutic option for patients with low/negative PD-L1 expression (Antonia et al., 2016; Hellmann et al., 2017; Hellmann et al., 2018).
However, there are still conflicting reports on the benefits of the combination therapies because of toxicity, lack of therapeutic efficacy, or because of differences in response arising from variations in tumor mutational burden (TMB) and PD-1 expression levels (Liu et al., 2021). Therefore, more evidence is needed to demonstrate that the addition of CTLA-4 to PD-1/PD-L1 therapy is superior to PD-1/PD-L1 monotherapy in NSCLC.
We conducted a meta-analysis to determine whether the addition of a CTLA-4 inhibitor to PD-1/PD-L1 therapy improves the efficacy of PD-1/PD-L1 alone in NSCLC.
A literature search of studies published until June 2023 in the PubMed, Embase, and Cochrane databases was performed by two independent reviewers. The keywords and relevant Medical Subject Heading (MeSH) terms used for the searches included the following: “Pembrolizumab,” “Nivolumab,” “Atezolizumab,” “Cemiplimab,” “Avelumab,” “Durvalumab” and “Ipilimumab,” “Tremelimumab” and “Non-small cell lung cancer.” Reference lists and materials were manually retrieved to identify potentially eligible articles.
Inclusion criteria were as follows: (Gandhi et al., 2018): participants: studies that enrolled patients diagnosed with NSCLC; (Socinski et al., 2018); interventions: comparing the clinical efficacy of PD-1/PD-L1 with or without CTLA-4; (Paz-Ares et al., 2018); outcomes: overall survival (OS), progression-free survival (PFS), objective response rate (ORR), and adverse events (AEs); and (Camidge et al., 2019) study design: randomized controlled trials (RCTs).
All the cohort articles were assessed for risk of bias using the Cochrane Collaboration’s “risk of bias” tool for the RCTs (Higgins et al., 2011). The process was conducted in two separate studies, and disagreements were resolved by discussion.
Two reviewers independently extracted the following information: author’s name, year of publication, trial, therapy arm, follow-up period, number of patients, mean patient age, and relevant outcome data. Disagreements were resolved through discussion. Publication bias was evaluated using funnel plots.
The experimental group was defined as the one receiving the combination immunotherapy and the control group as that receiving anti-PD-1/PD-L1 monotherapy. Heterogeneity of the articles were assessed using the I2 statistic and Chi-square test (Higgins and Thompson, 2002). I2 ≥ 50% was considered to indicate high heterogeneity, whereas I2 < 50% was suggested to indicate low heterogeneity (Higgins et al., 2003). The fixed-effects model was used when there was a low degree of heterogeneity among the studies; otherwise, the random-effects model was used. Statistical significance was set at p < 0.05. Review Manager version 5.3 software (RevMan; The Cochrane Collaboration, Oxford, United Kingdom) was used for statistical analysis. The results are shown as forest plots.
A total of 527 publications were retrieved. Following a review of the titles and abstracts, 11 studies were evaluated by reading the complete article. However, four of these were excluded based on the inclusion criteria. Finally, seven RCTs were included in the analyses (Planchard et al., 2020a; Rizvi et al., 2020; Boyer et al., 2021; Cascone et al., 2021; Gettinger et al., 2021; Paz-Ares et al., 2022; Johnson et al., 2023). Figure 1 illustrates the search process in detail. Figures 2, 3 summarize the quality assessment process.
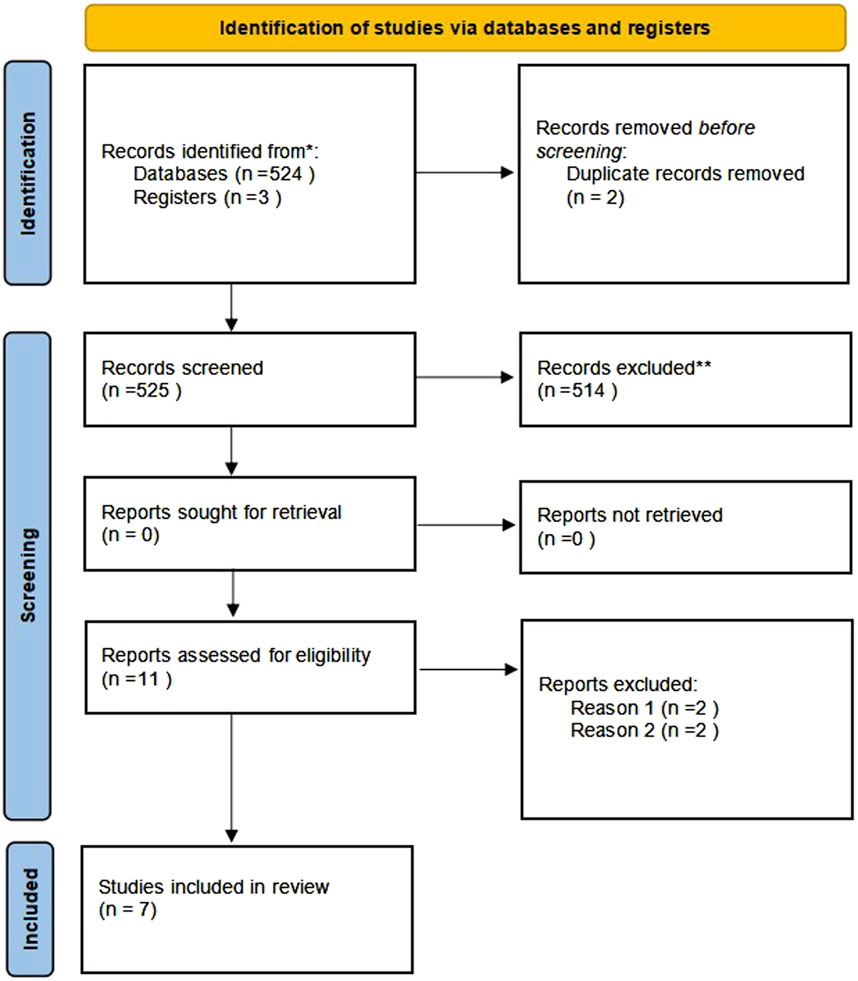
FIGURE 1. PRISMA flow chart of selection process to identify studies eligible for pooling Reason 1.
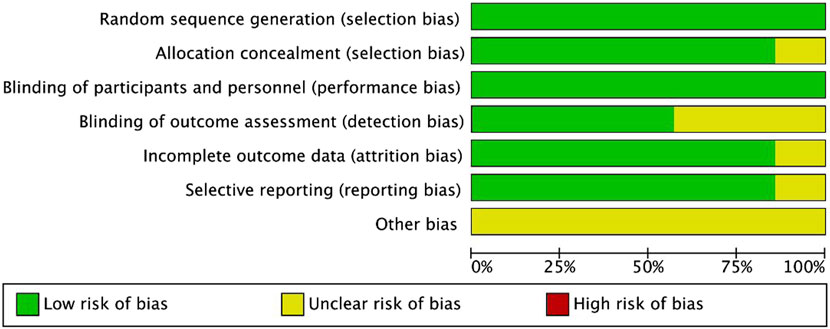
FIGURE 2. Methodological quality assessment for each included study.
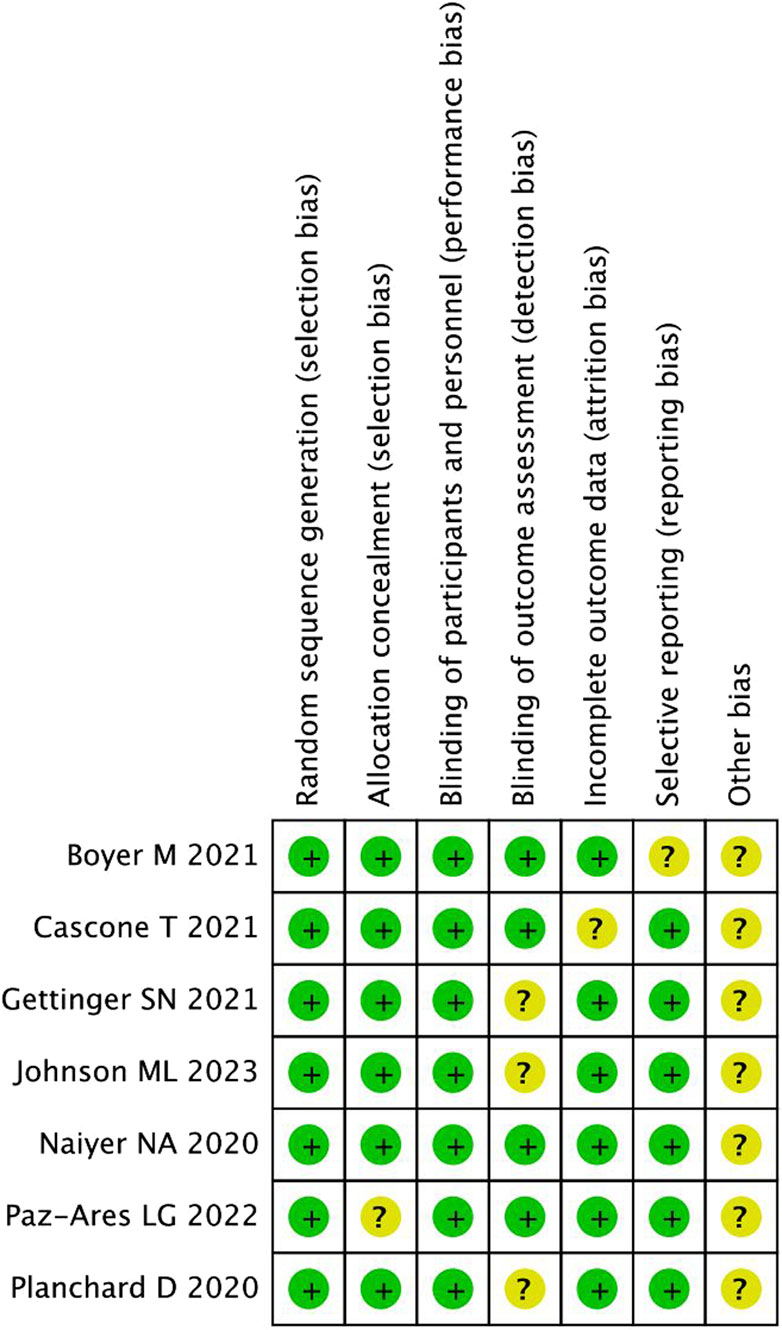
FIGURE 3. Quality assessment summary for included studies.
All included publications were based on moderate-quality evidence. Table 1 describes the primary characteristics of the eligible studies in detail.

TABLE 1. Characteristics of the include studies.
Because there was no heterogeneity among the studies, we applied a fixed-effects model to the relevant analysis. The pooled result for OS showed no significant benefit of the combination immunotherapy over anti-PD-1/PD-L1 monotherapy (HR = 0.98, 95% CI = 0.84–1.14, p = 0.79) (Figure 4).
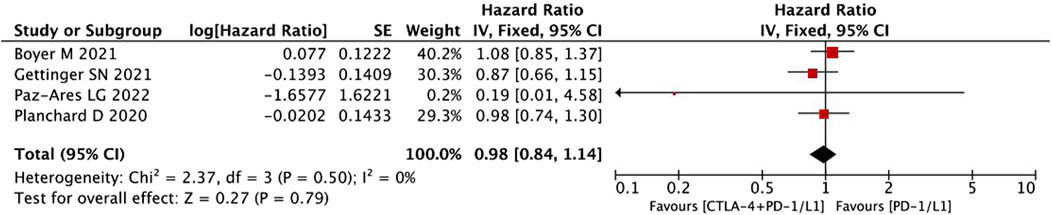
FIGURE 4. Pooled analysis of OS.
A fixed-effects model was used to analyze the pooled PFS data because heterogeneity across the included studies was low. The pooled data for PFS did not show any significant effect of the combination immunotherapy over anti-PD-1/PD-L1 monotherapy (HR = 0.92, 95% CI = 0.81–1.06, p = 0.25) (Figure 5).

FIGURE 5. Pooled analysis of PFS.
The ORR showed no significant difference between the two treatment regimens in the fixed-effects model (HR = 1.08, 95% CI = 0.96–1.21, p = 0.19) (Figure 6). The addition of CTLA-4 to PD-1/PD-L1 therapy did not improve the ORR compared to PD-1/PD-L1 alone in NSCLC.
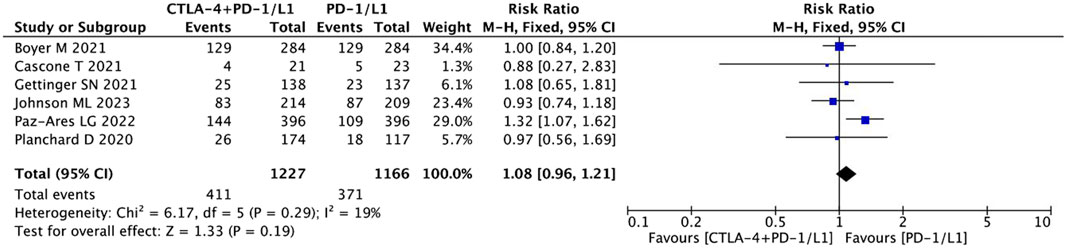
FIGURE 6. Pooled analysis of objective response rates (ORR).
The combination immunotherapy arm was associated with increased rates of any type AEs (RR = 1.06, 95% CI = 1.00–1.13, p = 0.03) (Figure 7), higher grade 3 AEs (RR = 1.58, 95% CI = 1.36–1.82, p < 0.05), and AEs leading to treatment discontinuation (RR = 1.83, 95% CI = 1.46–2.28, p < 0.05) compared with the antiPD-1/PD-L1 monotherapy arm. Whereas, the pooled data showed that the rate of AEs leading to death (RR = 1.93, 95% CI = 1.00–3.71, p = 0.05) was not significantly different between the two treatment regimens (Figure 8).

FIGURE 7. Pooled analysis of adverse effects (AEs).
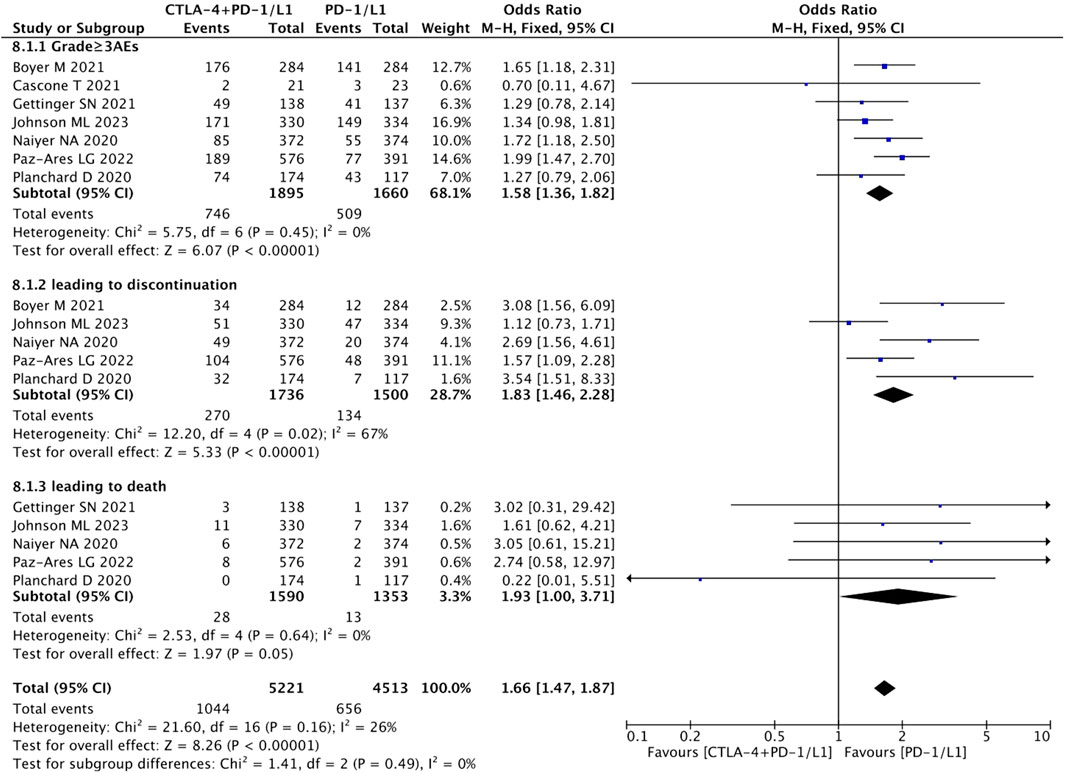
FIGURE 8. Pooled analysis of sub-group adverse effects.
Forest plots were used to present publication bias. Figure 9 shows funnel plots of the OS (Figure 9A), PFS (Figure 9B), ORR (Figure 9C), and any type of AEs (Figure 9D).
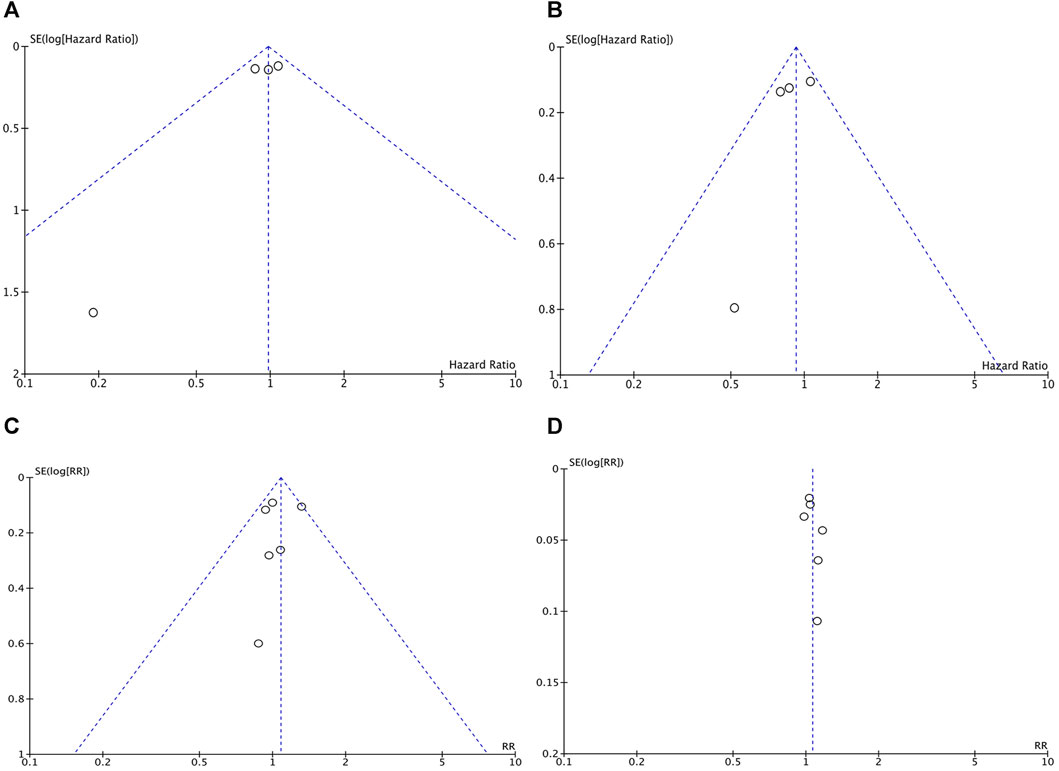
FIGURE 9. The funnel plots of the OS (A), PFS (B), ORR (C), and any type of AEs (D).
The combination of anti-PD-1/PD-L1 therapy with anti-CTLA-4 is considered to amplify the anti-tumor T-cell responses through non-redundant immune checkpoint blockade, and provide additive or synergistic antitumor activity. However, previous trials suggest that this combination does not provide any additional benefits beyond that of PD-1 inhibition alone (Gettinger et al., 2021).
To determine the efficacy of PD-1/PD-L1, with or without CTLA-4, we performed a comprehensive meta-analysis, and evaluated the benefits and risks of the combination immunotherapy versus PD-1/PDL-1 inhibitor monotherapy.
From a biological perspective, the combination immunotherapy should provide superior efficacy compared to PD-1/PDL-1monotherapy. The results of the Lung-MAP S1400I trial (Gettinger et al., 2021) and the CheckMate 227 trial (Paz-Ares et al., 2022) have supported this view. However, we found that adding CTLA-4 inhibitors to PD-1/PD-L1 therapy did not significantly improve the antitumor efficacy indices (survival outcomes including PFS and OS and drug response including ORR) compared to those of PD-1/PD-L1 inhibitors alone.
These findings may be explained by the influence of differences in PD-L1 expression levels and TMB, which have been mentioned in previous trials (Planchard et al., 2020b). PD-L1 expression, measured by immunohistochemistry, is currently the most widely used decision-making tool in clinical practice for selecting patients who will derive the greatest benefit from ICIs, at least in a first-line setting (Reck et al., 2016).
PD-L1 negative tumors do not respond to ICIs. Some reports have indicated a trend toward a better response rate associated with increased PD-L1 expression levels. The analysis of the POSEIDON (Johnson et al., 2023) has demonstrated that patients with PD-L1–low/negative are more likely to show primary resistance to anti–PD-(L)1 therapy. Paz-Ares LG (Paz-Ares et al., 2022) shown that efficacy benefit with nivolumab plus ipilimumab versus nivolumab monotherapy for both PD-L1 expression greater than or equal to 1% and 50%. These findings suggest the existence of inherent differences in the immune milieu associated with PD-L1 expression levels, and the complex relationship between tumors and the immune system. However, the optimal cut-off value of PD-L1 expression has not yet been defined.
TMB has recently emerged as a biomarker, independent of PD-L1 expression, for identifying patients who may clinically benefits from ICI therapies (Carbone et al., 2017; Hellmann et al., 2018; Ready et al., 2019). Previous NSCLC trials revealed that PD-1/CTLA-4 combination blockade improved PFS in patients with high TMB, independent of PD-L1 expression (Hellmann et al., 2018; Ready et al., 2019). However, the OS was similar regardless of the TMB level (Jiang et al., 2018). In our opinion, the cut-off point for TMB may provide a reasonable explanation for this observation. In their study, Gettinger et al. (2021) reported that a high TMB (defined as a cut-off of 10 mut/Mb) did not result in a superior outcome with combination therapy. However, Rizvi et al. (2020) reported that a high TMB was associated with a significant favorable contribution of CTLA-4 in combination therapy vs. that of PD-1 monotherapy. They defined high TMB as a cut-off value of 20 mut/Mb. Because the optimal cut-off for TMB differed across the studies included in our analysis, the predictive effect of TMB on survival outcomes could not be established in our study. Therefore, standardization of TMB calculation and reporting as well as a universal threshold for defining high TMB remain challenges that need to be investigated further.
In terms of AEs, we consistently found that the combination therapy increased the incidence of grade 3 AEs and AEs that lead to discontinuation. This finding indicates that the AEs associated with the combination therapy worsened in patients on treatment, thereby providing minimal benefits from the drugs. We expect that the risk of immune-related AEs can be reduced by carefully selecting patients for treatment with ICI combinations.
The limitations of our study include its retrospective nature and the various ICIs used in the studies included in our analysis, resulting in an imbalance between the two groups. Analyses of subgroups based on the ICIs are warranted to answer these questions. In addition, we could not draw any conclusions regarding the influence of PD-L1 expression level and TMB on ICIs because of the limited data on the covariates available for analysis. Further high-quality studies with additional data are required to clarify this issue.
In summary, our analysis suggests that addition of CTLA-4 to PD-1 therapy failed to improve the survival efficacy, but also increased the incidence of grade 3 AEs and AEs leading to discontinuation when compared with PD-1/PD-L1 monotherapy. The predictive values of TMB and PD-L1 expression need to be addressed in future studies.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
LiL: Software, Writing–original draft. LX: Formal Analysis, Writing–original draft. LeL: Conceptualization, Investigation, Writing–review and editing. CC: Data curation, Investigation, Writing–review and editing. HZ: Conceptualization, Investigation, Writing–review and editing. CY: Conceptualization, Investigation, Writing–review and editing. LZ: Conceptualization, Investigation, Writing–review and editing. AW: Project administration, Writing–review and editing. WL: Formal Analysis, Project administration, Writing–review and editing, Software.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
NSCLC, Non-small cell lung cancer; PD-1, Programmed cell death 1.
Antonia, S., Goldberg, S. B., Balmanoukian, A., Chaft, J. E., Sanborn, R. E., Gupta, A., et al. (2016). Safety and antitumour activity of durvalumab plus tremelimumab in non-small cell lung cancer: a multicentre, phase 1b study. Lancet Oncol. 17 (3), 299–308. doi:10.1016/S1470-2045(15)00544-6
Boyer, M., Şendur, M. A. N., Rodríguez-Abreu, D., Park, K., Lee, D. H., Çiçin, I., et al. (2021). Pembrolizumab plus ipilimumab or placebo for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score ≥ 50%: randomized, double-blind phase III KEYNOTE-598 study. J. Clin. Oncol. 39 (21), 2327–2338. doi:10.1200/JCO.20.03579
Camidge, D. R., Doebele, R. C., and Kerr, K. M. (2019). Comparing and contrasting predictive biomarkers for immunotherapy and targeted therapy of NSCLC. Nat. Rev. Clin. Oncol. 16 (6), 341–355. doi:10.1038/s41571-019-0173-9
Carbone, D. P., Reck, M., Paz-Ares, L., Creelan, B., Horn, L., Steins, M., et al. (2017). First-line nivolumab in stage IV or recurrent non-small-cell lung cancer. N. Engl. J. Med. 376 (25), 2415–2426. doi:10.1056/NEJMoa1613493
Cascone, T., William, W. N., Weissferdt, A., Leung, C. H., Lin, H. Y., Pataer, A., et al. (2021). Neoadjuvant nivolumab or nivolumab plus ipilimumab in operable non-small cell lung cancer: the phase 2 randomized NEOSTAR trial. Nat. Med. 27 (3), 504–514. doi:10.1038/s41591-020-01224-2
Chen, S., Mo, W., Jiang, W., Zhou, S., Gan, H., and Yu, Q. (2023). The benefit and risk of PD-1/PD-L1 inhibitors plus anti-angiogenic agents as second or later-line treatment for patients with advanced non-small-cell lung cancer: a systematic review and single-arm meta-analysis of prospective clinical trials. Front. Immunol. 14, 1218258. PMID: 37614237; PMCID: PMC10442655. doi:10.3389/fimmu.2023.1218258
Gandhi, L., Rodríguez-Abreu, D., Gadgeel, S., Esteban, E., Felip, E., De Angelis, F., et al. (2018). Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 378 (22), 2078–2092. doi:10.1056/NEJMoa1801005
Gettinger, S. N., Redman, M. W., Bazhenova, L., Hirsch, F. R., Mack, P. C., Schwartz, L. H., et al. (2021). Nivolumab plus ipilimumab vs nivolumab for previously treated patients with stage IV squamous cell lung cancer: the lung-MAP S1400I phase 3 randomized clinical trial. JAMA Oncol. 7 (9), 1368–1377. doi:10.1001/jamaoncol.2021.2209
Hellmann, M. D., Ciuleanu, T. E., Pluzanski, A., Lee, J. S., Otterson, G. A., Audigier-Valette, C., et al. (2018). Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N. Engl. J. Med. 378 (22), 2093–2104. doi:10.1056/NEJMoa1801946
Hellmann, M. D., Rizvi, N. A., Goldman, J. W., Gettinger, S. N., Borghaei, H., Brahmer, J. R., et al. (2017). Nivolumab plus ipilimumab as first-line treatment for advanced non-small-cell lung cancer (CheckMate 012): results of an open-label, phase 1, multicohort study. Lancet Oncol. 18 (1), 31–41. doi:10.1016/S1470-2045(16)30624-6
Higgins, J. P., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928. doi:10.1136/bmj.d5928
Higgins, J. P., and Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Stat. Med. 21 (11), 1539–1558. doi:10.1002/sim.1186
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327 (7414), 557–560. doi:10.1136/bmj.327.7414.557
Jiang, P., Gu, S., Pan, D., Fu, J., Sahu, A., Hu, X., et al. (2018). Signatures of T cell dysfunction and exclusion predict cancer immunotherapy response. Nat. Med. 24 (10), 1550–1558. doi:10.1038/s41591-018-0136-1
Johnson, M. L., Cho, B. C., Luft, A., Alatorre-Alexander, J., Geater, S. L., Laktionov, K., et al. (2023). Durvalumab with or without tremelimumab in combination with chemotherapy as first-line therapy for metastatic non-small-cell lung cancer: the phase III POSEIDON study. J. Clin. Oncol. 41 (6), 1213–1227. doi:10.1200/JCO.22.00975
Liu, Q., Fang, Z., Liu, M., Xu, R., Yi, F., Wei, Y., et al. (2021). The benefits and risks of CTLA4 inhibitor plus PD1/PDL1 inhibitor in stage IIIB/IV non-small cell lung cancer: a systematic analysis and meta-analysis based on randomized controlled trials. J. Clin. Pharm. Ther. 46 (6), 1519–1530. doi:10.1111/jcpt.13465
Paz-Ares, L., Luft, A., Vicente, D., Tafreshi, A., Gümüş, M., Mazières, J., et al. (2018). Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N. Engl. J. Med. 379 (21), 2040–2051. doi:10.1056/NEJMoa1810865
Paz-Ares, L. G., Ramalingam, S. S., Ciuleanu, T. E., Lee, J. S., Urban, L., Caro, R. B., et al. (2022). First-line nivolumab plus ipilimumab in advanced NSCLC: 4-year outcomes from the randomized, open-label, phase 3 CheckMate 227 Part 1 trial. J. Thorac. Oncol. 17 (2), 289–308. doi:10.1016/j.jtho.2021.09.010
Planchard, D., Reinmuth, N., Orlov, S., Fischer, J. R., Sugawara, S., Mandziuk, S., et al. (2020a). ARCTIC: durvalumab with or without tremelimumab as third-line or later treatment of metastatic non-small-cell lung cancer. Ann. Oncol. 31 (5), 609–618. doi:10.1016/j.annonc.2020.02.006
Planchard, D., Reinmuth, N., Orlov, S., Fischer, J. R., Sugawara, S., Mandziuk, S., et al. (2020b). ARCTIC: durvalumab with or without tremelimumab as third-line or later treatment of metastatic non-small-cell lung cancer. Ann. Oncol. 31 (5), 609–618. doi:10.1016/j.annonc.2020.02.006
Ready, N., Hellmann, M. D., Awad, M. M., Otterson, G. A., Gutierrez, M., Gainor, J. F., et al. (2019). First-line nivolumab plus ipilimumab in advanced non-small-cell lung cancer (CheckMate 568): outcomes by programmed death ligand 1 and tumor mutational burden as biomarkers. J. Clin. Oncol. 37 (12), 992–1000. doi:10.1200/JCO.18.01042
Reck, M., Rodríguez-Abreu, D., Robinson, A. G., Hui, R., Csőszi, T., Fülöp, A., et al. (2016). Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 375 (19), 1823–1833. doi:10.1056/NEJMoa1606774
Rizvi, N. A., Cho, B. C., Reinmuth, N., Lee, K. H., Luft, A., Ahn, M. J., et al. (2020). Durvalumab with or without tremelimumab vs standard chemotherapy in first-line treatment of metastatic non-small cell lung cancer: the MYSTIC phase 3 randomized clinical trial. JAMA Oncol. 6 (5), 661–674. Erratum in: JAMA Oncol. 2020;6(11):1815. doi:10.1001/jamaoncol.2020.0237
Shen, M., Lu, C., and Gao, J. (2023). Prognostic influence of PD-1/PD-L1 suppressors in combination with chemotherapeutic agents for non-small cell pulmonary carcinoma: system review and meta-analysis. Front. Oncol. 19 (13), 1137913. doi:10.3389/fonc.2023.1137913
Socinski, M. A., Jotte, R. M., Cappuzzo, F., Orlandi, A. J., Stroyakovskiy, D., Nogami, N., et al. (2018). Overall survival (OS) analysis of IMpower150, a randomized Ph 3 study of atezolizumab (atezo) + chemotherapy (chemo) ± bevacizumab (bev) vs chemo + bev in 1L nonsquamous (NSQ) NSCLC. JCO 36, 9002. (15_suppl):9002. doi:10.1200/jco.2018.36.15_suppl.9002
Keywords: CTLA-4 inhibitor, PD-1/PD-L1 inhibitor, non-small cell lung cancer, meta-analysis, NSCLC
Citation: Lin L, Xiao L, Li L, Chen C, Zhang H, Yu C, Zhang L, Wei A and Li W (2024) A meta-analysis of the efficacy of programmed cell death 1/its ligand inhibitors plus cytotoxic T-lymphocyte-associated antigen 4 inhibitors in non-small cell lung cancer. Front. Pharmacol. 15:1267763. doi: 10.3389/fphar.2024.1267763
Received: 27 July 2023; Accepted: 23 January 2024;
Published: 05 February 2024.
Edited by:
Andrea Messori, Regione Toscana, ItalyReviewed by:
Daniele Mengato, University Hospital of Padua, ItalyCopyright © 2024 Lin, Xiao, Li, Chen, Zhang, Yu, Zhang, Wei and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anhua Wei, YWh3ZWkwNzE2QDE2My5jb20=; Wei Li, aXNsaXdlaV90aWFvQDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.