 Marcin Siwek
Marcin Siwek Adrian Andrzej Chrobak
Adrian Andrzej Chrobak Aleksandra Gorostowicz
Aleksandra Gorostowicz Patrycja Król2
Patrycja Król2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 04 January 2024
Sec. Neuropharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1321112
The aim of our study was to evaluate the efficacy of cariprazine augmentation of clozapine in treatment-resistant schizophrenia in a retrospective chart review. Among 916 medical records of schizophrenia patients, we identified 12 individuals treated with a combination of those drugs for a duration of 3–60 weeks [median 32 (10–40)]. Clinical Global Impression–Improvement (CGI-I) scores were used to measure the treatment response between the introduction of cariprazine augmentation of clozapine and the last point of observation. The majority of the patients presented treatment response (9/12 patients, 75%) after 4–16 weeks of therapy [median 6 (4–12)]. Treatment was associated with the decrease in positive, negative, affective, and anxiety symptom severity, as well as improvement of patient global functioning. One patient discontinued the treatment due to side effects (akathisia), and two patients halted the therapy due to the exacerbation of psychotic symptoms. Our study presents a thorough clinical description of the largest number of treatment-resistant schizophrenia patients medicated using cariprazine augmentation of clozapine in a “real-world” setting. Our results suggest that the use of this combination may lead to the improvement in a broad range of symptoms of patients with this condition.
Schizophrenia is a chronic and devastating mental illness characterized by the occurrence of negative, positive, and cognitive symptoms (Suttajit et al., 2015). Despite the observable progress in the field of psychopharmacotherapy, approximately 30%–50% of patients still present treatment resistance, which is defined as the persistence of psychotic symptoms after at least two subsequential antipsychotic drug monotherapies with an adequate dose, duration, and patient compliance (Nucifora et al., 2019; Correll and Howes, 2021). The only medicine that received FDA recommendation in the case of treatment-resistant schizophrenia is clozapine, which has been shown to be the most effective antipsychotic drug for reducing positive symptoms, suicidal risk, and the frequency and duration of hospitalizations (Kane et al., 1988; Chakos et al., 2001; Siskind et al., 2016; 2019; Wimberley et al., 2017; Cho et al., 2019). Even though clozapine has been shown to be more effective than other neuroleptics, as many as 40%–70% of patients do not achieve a satisfactory response to the treatment with the use of this drug (Rajkumar et al., 2013; McCutcheon et al., 2015; Sagud, 2015; Chakrabarti, 2021). A common strategy to overcome clozapine resistance is augmentation using a second antipsychotic drug. However, data supporting this method come from low-quality studies, e.g., open-label trials or case studies (Wagner et al., 2019). A recent meta-analysis of randomized controlled trials evaluating treatment strategies for clozapine-resistant schizophrenia showed that none of the analyzed neuroleptics (aripiprazole, amisulpride, sulpiride, risperidone, sertindole, pimozide, and quetiapine) differed from placebo (Yeh et al., 2023). The use of more modern antipsychotics such as lurasidone and cariprazine as a method of clozapine augmentation is limited (De Berardis et al., 2021; Oloyede et al., 2022; Pappa et al., 2022; Weise et al., 2022; Siwek et al., 2023).
Cariprazine is a novel antipsychotic drug characterized by D2/D3 partial agonism with almost 10-fold higher affinity to D3 than D2 receptors, as well as partial agonistic activity at serotonin 5-HT1a receptors (Misiak et al., 2018). Table 1 summarizes the affinities of cariprazine and its clinical effects compared to other partial D2 agonists (Siwek et al., 2023). Due to its unique pharmacokinetic features, this drug has been referred to as an “oral depot,” as the half-time of cariprazine ranges between 2 and 4 days, and in the case of its metabolite didesmethyl cariprazine, it may be up to even 2–3 weeks (Misiak et al., 2018; Oloyede et al., 2022). The efficacy of the monotherapy using this drug in schizophrenia has been proved in several short-term randomized controlled trials and a double-blinded extension study (Misiak et al., 2018). Recent studies suggest that due to the abovementioned unique pharmacokinetic and pharmacodynamic properties, cariprazine may also be beneficial in combination with other antipsychotics (Hjorth 2021; Boydstun et al., 2023). Its noticeable effectiveness has been shown in the area of negative symptoms. In a 26-week placebo-controlled double-blinded study, performed on a group of 461 schizophrenia patients, cariprazine monotherapy has shown high efficacy in the treatment of persistent and predominant negative symptoms compared to risperidone (Németh et al., 2017). Taking into account the frequent occurrence of these symptoms in treatment-resistant schizophrenia and the small effect of clozapine on their improvement, the use of cariprazine for its augmentation may be beneficial (Krause et al., 2018; Correll and Schooler, 2020). While there are many studies evaluating the efficacy of the augmentation of clozapine with the use of other antipsychotics in treatment-resistant schizophrenia (Yeh et al., 2023), data concerning the use of cariprazine for this purpose are limited to case reports and one observational study (De Berardis et al., 2021; Oloyede et al., 2022; Pappa et al., 2022). Authors have suggested that cariprazine may be uniquely effective in combinations with other antipsychotic drugs. Pappa et al. (2022) performed a pilot prospective study evaluating the efficacy and safety of this combination in a group of patients with sub-optimal treatment response to clozapine. The study was performed on a heterogeneous group of 10 patients diagnosed with schizophrenia, schizoaffective disorder, and personality disorder, in which augmentation with cariprazine was introduced due to the presence of negative symptoms, treatment resistance, and/or tolerability issues with clozapine or previous augmentation options. The authors observed a reduction in both positive and negative symptom scores after 3 months of therapy, indicating good tolerance to the treatment. Due to those results indicating a beneficial effect of cariprazine augmentation of clozapine, the purpose of our study was to evaluate the effectiveness of this combination in treatment-resistant schizophrenia by performing a retrospective chart review.
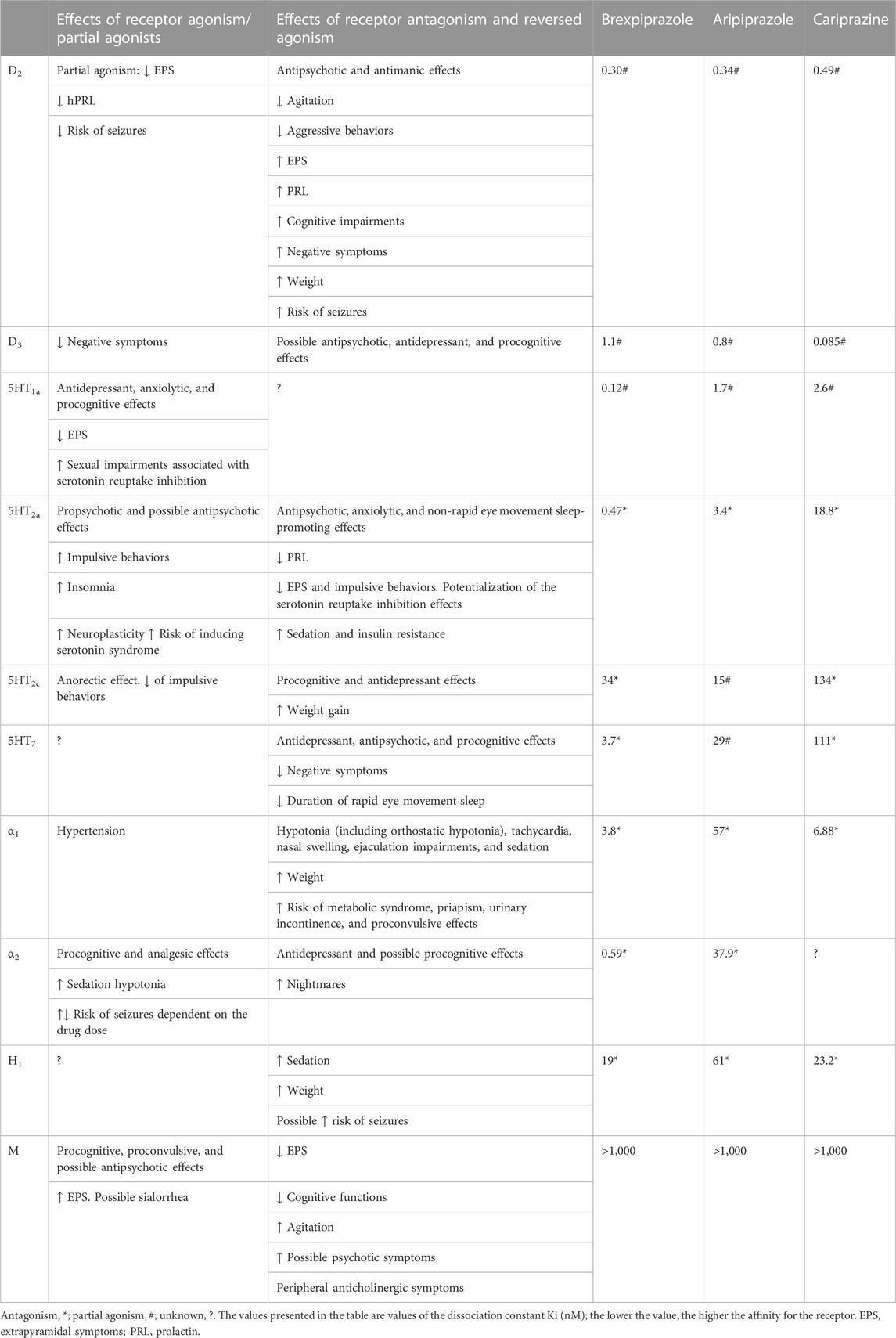
TABLE 1. Comparison of affinities of cariprazine and other partial agonists of D2 for specific receptors. Additionally, the clinical effects of agonism and antagonism of those receptors are summarized based on the study by Siwek et al. (2023) with some modifications.
In order to evaluate the efficacy of cariprazine augmentation of clozapine in treatment-resistant schizophrenia, we performed a retrospective chart review according to the methodology of our previous studies (Siwek et al., 2021; 2023). All the authors analyzed the data. The dataset consisted of medical records (paper and electronic) of all schizophrenia patients (diagnosed in accordance with the ICD-10 criteria) treated in the Department of Adult Psychiatry of University Hospital in Krakow between 2018 and 2022. The data were included in the analysis if they met the following inclusion criteria: diagnosis of schizophrenia, age above 18 years, and treatment with a combination of clozapine and cariprazine. The exclusion criteria were as follows: no documented follow-up observations and missing data relevant to the analysis. Figure 1 shows a flowchart of the retrospective chart review.
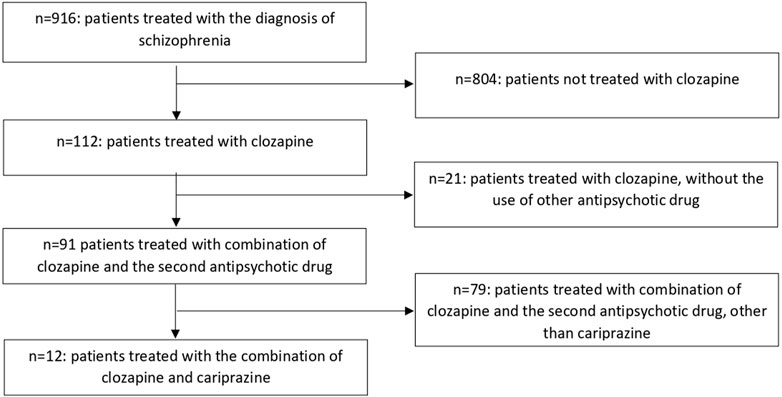
FIGURE 1. Flowchart of the retrospective chart review.
Before carrying out data abstraction, the researchers were trained in order to establish a common procedure for the data analysis. The authors organized regular meetings in order to discuss potential doubts occurring during the abstraction process. In the cases of incomplete or missing data, the researchers contacted the psychiatrist who was taking care of the particular patient. Data-collecting forms were based on the methodology of our previous study and are provided with this article.
The authors screened medical records of 916 patients diagnosed with schizophrenia. Among these, 112 were treated using clozapine, and 91 of those patients were treated using an additional neuroleptic. In this group, 12 patients were treated using a clozapine and cariprazine combination. Similar to our previous study, we achieved high inter-rater reliability, as there were only several features on which authors disagreed during data abstraction (Cohen’s kappa >0.8 for all variables). The disagreements were resolved by the discussion. The intra-rater reliability was assessed on a sample of 10 patients, for which Cohen’s kappa was also very high with values >0.8.
Data were extracted from medical records through the use of chart files in the form of an electronic table with the following variables: age, sex, duration of illness, the number of previous ineffective pharmacotherapy trials prior to the use of clozapine and cariprazine combination, dose of clozapine that was combined with cariprazine, antipsychotics used in combination with clozapine prior to the switch to cariprazine, somatic comorbidities, presence of substance abuse according to the ICD-10 classifications, other psychotropic medications used at the time of cariprazine augmentation of clozapine, non-psychiatric medications with their daily doses, initial and final doses of cariprazine, duration of the combined treatment (clozapine and cariprazine) in weeks, the number of weeks until the observable therapeutic effect was achieved, and effects of the addition of cariprazine. Moreover, we evaluated data for the occurrence of the following psychopathological symptoms and somatic conditions presented by the patients before initiation of cariprazine augmentation of clozapine: residual positive symptoms, exacerbation of positive symptoms, negative symptoms, depressive symptoms, anxiety, suicidal thoughts, cognitive dysfunctions, hyperprolactinemia, increased appetite and body weight/obesity, and disorders of glucose metabolism.
We calculated Clinical Global Impression-Improvement (CGI-I) scores with the aim to evaluate the treatment response between the first and last points of observation. The patients were classified as responding to cariprazine augmentation of clozapine if they achieved 1 or 2 points on the CGI-I scale (“Very much improved” or “Much improved”) at any point of the follow-up. In the case of every patient fulfilling the abovementioned criteria, we presented the number of weeks of treatment after which therapeutic effect was observable.
Data extracted from the medical records of 12 patients treated with the combination of cariprazine and clozapine are given in Table 2 and summarized in Table 3. The patients’ median age was 38 (range 23–59). There were seven men and five women of Caucasian ethnicity. The median duration of illness was 16.5 (range 5–30). All of the patients fulfilled the criteria of treatment-resistant schizophrenia, defined as the persistence of psychotic symptoms after at least two subsequential antipsychotic drug monotherapies with an adequate dose, duration, and patient compliance (Nucifora et al., 2019; Correll and Howes, 2021). The minimal number of previous ineffective psychopharmacotherapy trials prior to the use of cariprazine augmentation of clozapine was four. Four patients underwent more than 10 unsuccessful trials. Table 4 shows the psychopathological symptoms and somatic conditions presented before the initiation of the evaluated therapy.
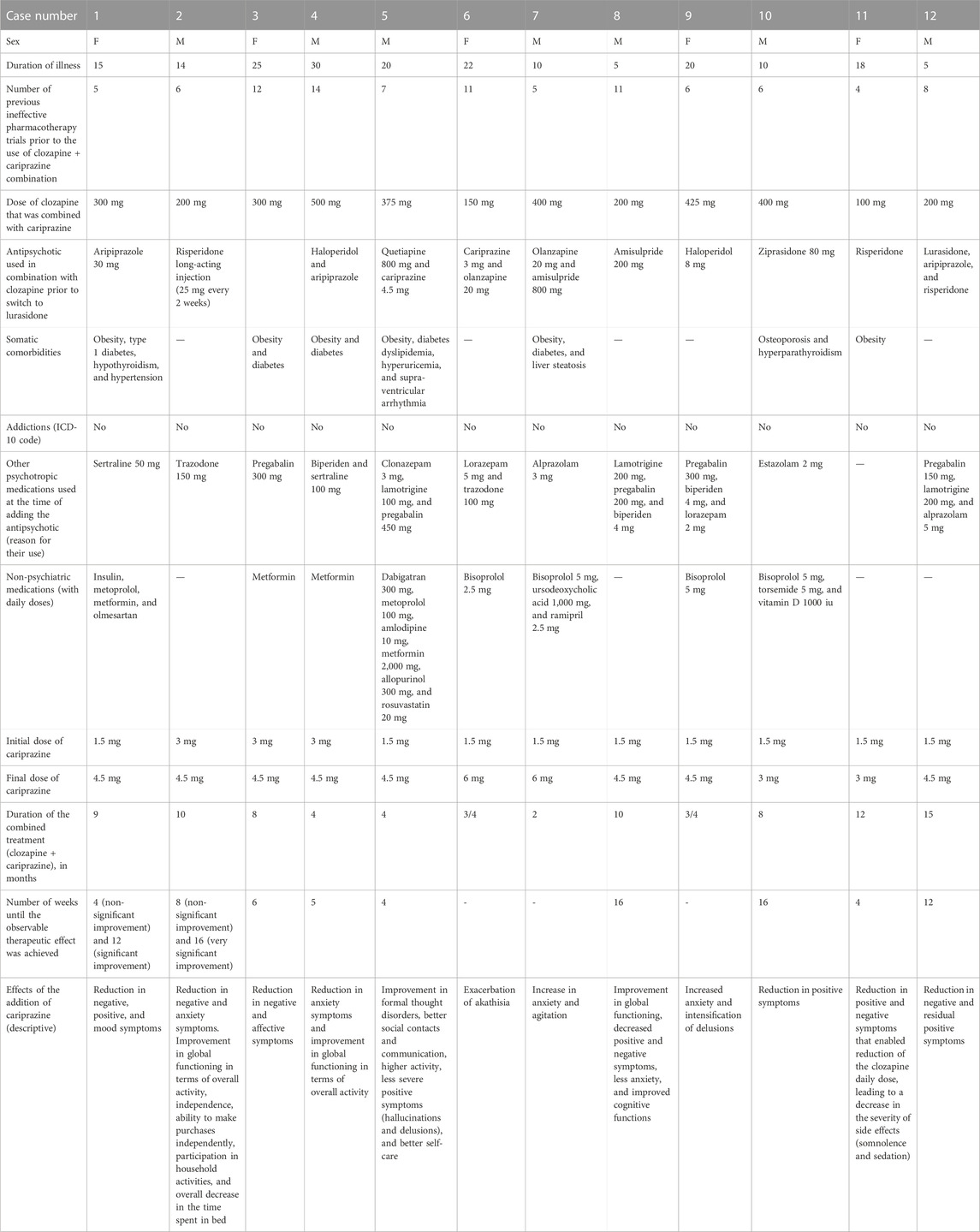
TABLE 2. Detailed description of treatment-resistant schizophrenia patients treated using cariprazine augmentation of clozapine.
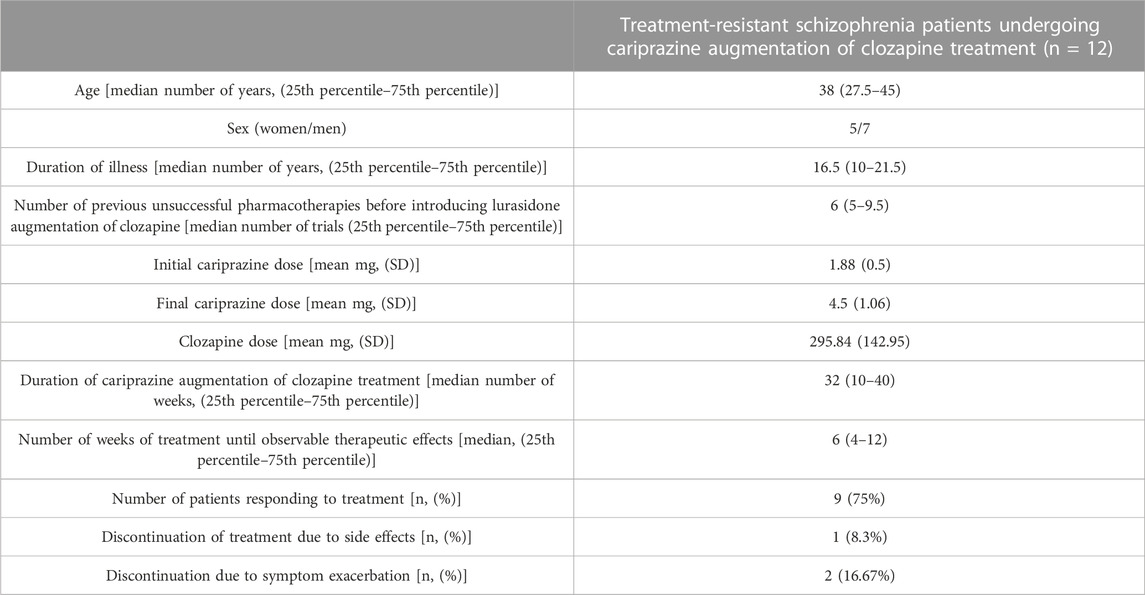
TABLE 3. Summarized description of the schizophrenia patient group treated with cariprazine augmentation of clozapine.
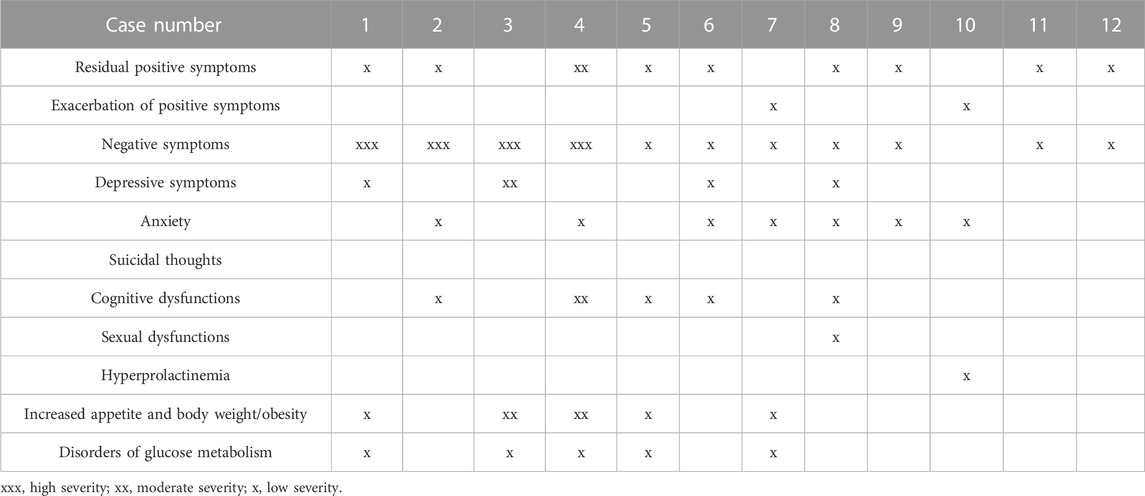
TABLE 4. Characteristics of the psychopathological symptoms and somatic conditions presented by schizophrenia patients before initiation of cariprazine augmentation of clozapine.
In nine out of twelve patients, cariprazine replaced other antipsychotic drugs that were used in combination with clozapine, particularly aripiprazole (one patient), risperidone (two patients: one treated with the use of oral tablets and the other with the use of long-acting injections), haloperidol (two patients), amisulpride (two patients), ziprasidone (one patient), and lurasidone (one patient). In one case, cariprazine was added to clozapine monotherapy. In two patients, clozapine replaced the other antipsychotic drugs that were used in combination with cariprazine, particularly olanzapine (one patient) and quetiapine (one patient).
The mean daily dose of clozapine that was used with cariprazine was 295.83 ± 142.95 mg (dose range 100–500 mg). In every case, the clozapine serum concentration remained at a therapeutic level. The mean initial and final doses of cariprazine added to clozapine were 1.88 ± 0.5 mg (dose range 1.5–3 mg) and 4.5 ± 1.06 mg (dose range 3–6 mg), respectively. The duration of cariprazine augmentation of clozapine ranged from 0.5 to 15 months (median: 8 months).
A positive therapeutic effect (CGI-I = 2) was observed in nine out of twelve patients (75%) after 4–12 weeks of treatment (median 6). Medical records revealed that the patients showed an observable improvement in terms of negative symptoms (seven patients), positive symptoms (five patients), general functioning (six patients), affective symptoms (two patients), anxiety (two patients), and cognitive functions (one patient). In one patient, a decrease in the severity of positive and negative symptoms allowed the clozapine dose to be reduced, which contributed to the reduction of sedation and somnolence. In three patients, exacerbation of symptoms was observed during the treatment using a combination of cariprazine and clozapine, particularly anxiety (two patients), agitation (one patient), delusions (one patient), and akathisia (one patient).
Our study presents the first retrospective chart review of cariprazine augmentation of clozapine effects in the management of treatment-resistant schizophrenia. We demonstrated a thorough clinical description of 12 schizophrenia patients treated using a combination of clozapine and cariprazine for a period ranging from 3 weeks to 15 months. Despite the high level of treatment resistance, the majority of the patients (9/12, 75%) presented a therapeutic response, resulting in an improvement in terms of negative, positive, affective, and anxiety symptoms, as well as global functioning.
Taking into account that treatment-resistant schizophrenia is associated with severe negative symptoms, and the fact that cariprazine is particularly effective in their improvement, it is surprising that so few studies assessed the efficacy of the cariprazine augmentation of clozapine in this clinical group (Iasevoli et al., 2018; Misiak et al., 2018). Pappa et al. (2022) evaluated the use of this combination in a heterogeneous group of 10 patients with a non-satisfactory response to clozapine, which consisted of 6 patients with schizophrenia, 3 with schizoaffective disorder, and 1 with personality disorder with autism spectrum disorder. Cariprazine was introduced due to inadequate treatment response, persistent negative symptoms, clozapine-induced side effects, and/or lack of tolerance to previous augmentation strategies (Pappa et al., 2022). During the 3 months of the treatment, the authors observed a significant reduction in terms of positive, negative, and total Positive and Negative Syndrome Scale (PANSS) scores (Pappa et al., 2022). Similarly, case studies indicated that the combination of cariprazine and clozapine may lead to a marked reduction in negative and positive symptoms and improvement of patient global functioning (De Berardis et al., 2021; Bogren et al., 2022; Oloyede et al., 2022).
Our study presents the largest up-to-date sample of treatment-resistant schizophrenia patients treated with the cariprazine augmentation of clozapine. While most of the previous reports focused on the beneficial effect of this combination on negative symptoms, we showed that cariprazine augmentation of clozapine may also lead to a significant improvement across positive, depressive, and anxiety symptoms, as well as in global and cognitive functioning, despite a high number of previously failed treatment trials. Those results are in line with the observations from the four cases, indicating that cariprazine was effective where other augmentation antipsychotics failed, including the often preferred amisulpride (Oloyede et al., 2022). Case reports indicate that the introduction of cariprazine may reduce the severity of negative and positive symptoms to such an extent that it allows clozapine reduction (De Berardis et al., 2021) or even discontinuation (Aubel, 2021). In our study, we identified a similar case of a patient in whom the introduction of cariprazine led to a significant reduction in those symptoms and enabled the clozapine dose to be decreased. This contributed to the reduction of sedation and somnolence associated with the use of this drug.
We showed that cariprazine augmentation of clozapine was relatively well tolerated. Three out of twelve patients (25%) discontinued the treatment due to the exacerbation of symptoms or the occurrence of side effects. In one patient, there was an observable increase in anxiety and agitation. A second patient revealed the intensification of delusions with concomitant anxiety. Side effects (akathisia) occurred in only one patient. The management of the adverse events relied on the discontinuation of the cariprazine treatment, which resulted in amelioration of those symptoms in every mentioned case. Tolerance rates in our retrospective chart review were comparable to those presented in the much shorter study by Pappa et al. (2022), in which 80% of the patients adhered to the treatment throughout the 3 months of the treatment. In the aforementioned study, one patient developed dizziness that required dose optimization, while two patients discontinued the treatment due to poor response or restlessness. However, overall cariprazine augmentation was well tolerated by the rest of the group, including patients in whom previous treatment strategies had to be changed due to the lack of tolerance of side effects (Pappa et al., 2022).
Our study significantly contributes to the evidence supporting the use of modern antipsychotics as augmentation agents of clozapine in treatment-resistant schizophrenia (Siwek et al., 2023). While the observation time in previous studies was limited to 3 months (Pappa et al., 2022), our retrospective chart review presents the cases in which the duration of the combined treatment reached up to 15 months (median 8 months). Long-term observations are crucial in terms of evaluating cariprazine efficacy, especially in the area of negative symptoms. For instance, a 26-week-long, double-blind, placebo-controlled randomized trial comparing the effects of this drug with those of risperidone has shown that statistically significant difference in favor of cariprazine appears only after 14 weeks of treatment (Németh et al., 2017). In our study, the therapeutic effect of cariprazine augmentation of clozapine was observable after a median of 8 weeks. It is noteworthy that in four patients, significant improvement emerged after 4 months of therapy. Thus, it is crucial for future studies evaluating the efficacy of cariprazine augmentation of clozapine to implement long-term observations of patient treatment.
Positive effects of cariprazine augmentation of clozapine treatment may be associated with the significant pharmacodynamic complementarity of both drugs. Both antipsychotics act as 5-HT2a and 5-HT7 antagonists, but clozapine affinity to those receptors is significantly higher. Unlike clozapine, cariprazine is a D2/D3 partial agonist with unique high affinity to D3 receptors. This feature allows this drug to elicit differential activities depending on the synaptic environment. Particularly, it inhibits the receptor in the presence of agonists with higher intrinsic activity but acts as an agonist in their absence (Misiak et al., 2018). Cariprazine activity related to D3 receptors is associated with the improvement in positive, negative, and depressive symptoms, as well as with procognitive effects (Misiak et al., 2018). Contrary to clozapine, cariprazine presents negligible affinity to M1, α1, and α2 receptors and low affinity to H1 receptors, which is associated with the low risk of sedation, metabolic side effects, and hypotension (Misiak et al., 2018). Co-administration of those antipsychotics is associated with the low risk of significant pharmacokinetic interactions. Cariprazine metabolites are eliminated mainly by CYP3A4, and they act as weak competitive inhibitors of CYP2D6 and CYP3A4; thus, they have a minimal impact on clozapine, which is extensively metabolized via CYP1A2 (Mauri et al., 2018; Misiak et al., 2018). We are aware of the limitations of our study: the heterogeneous group of the analyzed patients (e.g., variability in the duration of treatment and differences in terms of the history of the unsuccessful treatment trials), a relatively small number of cases, no data on socioeconomic background, lack of a control group, and no access to the clozapine blood levels of most of the patients. Our study did not implement the use of specific clinical tools measuring negative, positive, anxiety, or affective symptoms or measures of cognitive and global functioning. Data regarding the abovementioned areas were derived from patient medical documentation. Being a retrospective chart review, the study might have inherent biases, such as selection bias and information bias. Those limitations decrease the strength of the conclusions that can be drawn from our study. However, we believe that due to the significant research gap in the area of a clozapine augmentation strategy with the use of modern antipsychotics, our studies provide valuable data that can be used in future randomized controlled trials addressing this issue.
To the best of our knowledge, our study presents a thorough description of the largest number of treatment-resistant schizophrenia patients medicated using cariprazine augmentation of clozapine in a “real-world” setting. The majority of the analyzed cases responded to the combination of the abovementioned drugs with a relatively good tolerance to the treatment. The use of cariprazine augmentation of clozapine was associated with an observable improvement in patient global functioning as well as a decrease in the severity of positive, negative, depressive, and anxiety symptoms. It is noteworthy that this effect was observed in the cases of individuals who underwent more than 10 ineffective antipsychotic treatment trials. Our preliminary study points out the need of well-designed, long-term, randomized clinical trials evaluating the efficacy of the cariprazine augmentation of clozapine in a group of treatment-resistant schizophrenia patients.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
MS: conceptualization, investigation, methodology, supervision, writing–original draft, and writing–review and editing. AC: formal analysis, methodology, writing–original draft, and writing–review and editing. AG: data curation, investigation, methodology, writing–original draft, and writing–review and editing. PK: data curation, investigation, writing–original draft, and writing–review and editing. DD: conceptualization, investigation, methodology, supervision, and writing–review and editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1321112/full#supplementary-material
Aubel, T. (2021). Cariprazine: patients with treatment-resistant schizophrenia. Neuropsychiatr. Dis. Treat. 17, 2327–2332. doi:10.2147/NDT.S315653
Bogren, M., Soltesz, M., and Hjorth, S. (2022). Remission of persistent negative symptoms and psychosocial consequences by combined clozapine and cariprazine treatment in a patient with long-standing treatment-resistant schizoaffective disorder. Front. Psychiatry 13, 887547. doi:10.3389/FPSYT.2022.887547
Boydstun, C., Lynch, S., and Digenova, P. (2023). Cariprazine: an augmentation strategy for treatment-resistant schizophrenia with pro-cognitive and anti-hostility effects. Int. Clin. Psychopharmacol. 38, 361–366. doi:10.1097/YIC.0000000000000469
Chakos, M., Lieberman, J., Hoffman, E., Bradford, D., and Sheitman, B. (2001). Effectiveness of second-generation antipsychotics in patients with treatment-resistant schizophrenia: a review and meta-analysis of randomized trials. Am. J. Psychiatry 158, 518–526. doi:10.1176/APPI.AJP.158.4.518
Chakrabarti, S. (2021). Clozapine resistant schizophrenia: newer avenues of management. World J. Psychiatry 11, 429–448. doi:10.5498/wjp.v11.i8.429
Cho, J., Hayes, R. D., Jewell, A., Kadra, G., Shetty, H., MacCabe, J. H., et al. (2019). Clozapine and all-cause mortality in treatment-resistant schizophrenia: a historical cohort study. Acta Psychiatr. Scand. 139, 237–247. doi:10.1111/ACPS.12989
Correll, C. U., and Howes, O. D. (2021). Treatment-resistant schizophrenia: definition, predictors, and therapy options. J. Clin. Psychiatry 82. doi:10.4088/JCP.MY20096AH1C
Correll, C. U., and Schooler, N. R. (2020). Negative symptoms in schizophrenia: a review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr. Dis. Treat. 16, 519–534. doi:10.2147/NDT.S225643
De Berardis, D., Rapini, G., Olivieri, L., Giardini, A., De Lauretis, I., Serroni, N., et al. (2021). Cariprazine add-on in inadequate clozapine response: a report on two cases. Clin. Psychopharmacol. Neurosci. 19, 174–178. doi:10.9758/CPN.2021.19.1.174
Hjorth, S. (2021). The More, the Merrier…? Antipsychotic Polypharmacy Treatment Strategies in Schizophrenia From a Pharmacology Perspective. Front. Psychiatry. 12, 760181. doi:10.3389/fpsyt.2021.760181
Iasevoli, F., Avagliano, C., Altavilla, B., Barone, A., D’Ambrosio, L., Matrone, M., et al. (2018). Disease severity in treatment resistant schizophrenia patients is mainly affected by negative symptoms, which mediate the effects of cognitive dysfunctions and neurological soft signs. Front. Psychiatry 9, 425442. doi:10.3389/fpsyt.2018.00553
Kane, J., Honigfeld, G., Singer, J., and Meltzer, H. (1988). Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch. Gen. Psychiatry 45, 789–796. doi:10.1001/ARCHPSYC.1988.01800330013001
Krause, M., Zhu, Y., Huhn, M., Schneider-Thoma, J., Bighelli, I., Nikolakopoulou, A., et al. (2018). Antipsychotic drugs for patients with schizophrenia and predominant or prominent negative symptoms: a systematic review and meta-analysis. Eur. Arch. Psychiatry Clin. Neurosci. 268, 625–639. doi:10.1007/S00406-018-0869-3
Mauri, M. C., Paletta, S., Di Pace, C., Reggiori, A., Cirnigliaro, G., Valli, I., et al. (2018). Clinical pharmacokinetics of atypical antipsychotics: an update. Clin. Pharmacokinet. 57, 1493–1528. doi:10.1007/s40262-018-0664-3
McCutcheon, R., Beck, K., Bloomfield, M. A. P., Marques, T. R., Rogdaki, M., and Howes, O. D. (2015). Treatment resistant or resistant to treatment? Antipsychotic plasma levels in patients with poorly controlled psychotic symptoms. J. Psychopharmacol. 29, 892–897. doi:10.1177/0269881115576688
Misiak, B., Bieńkowski, P., and Samochowiec, J. (2018). Cariprazine - a novel antipsychotic drug and its place in the treatment of schizophrenia. Psychiatr. Pol. 52, 971–981. doi:10.12740/PP/ONLINEFIRST/80710
Németh, G., Laszlovszky, I., Czobor, P., Szalai, E., Szatmári, B., Harsányi, J., et al. (2017). Cariprazine versus risperidone monotherapy for treatment of predominant negative symptoms in patients with schizophrenia: a randomised, double-blind, controlled trial. Lancet 389, 1103–1113. doi:10.1016/S0140-6736(17)30060-0
Nucifora, F. C., Woznica, E., Lee, B. J., Cascella, N., and Sawa, A. (2019). Treatment resistant schizophrenia: clinical, biological, and therapeutic perspectives. Neurobiol. Dis. 131, 104257. doi:10.1016/j.nbd.2018.08.016
Oloyede, E., Clark, I., Mace, S., Whiskey, E., and Taylor, D. (2022). Clozapine augmentation with cariprazine for negative symptoms: a case series and literature review. Ther. Adv. Psychopharmacoldoi 12, 204512532110666. doi:10.1177/20451253211066642
Pappa, S., Kalniunas, A., Sharma, H., Raza-Syed, A., Kamal, M., and Larkin, F. (2022). Efficacy and safety of cariprazine augmentation in patients treated with clozapine: a pilot study. Ther. Adv. Psychopharmacol. 12, 204512532211320. doi:10.1177/20451253221132087
Rajkumar, A. P., Poonkuzhali, B., Kuruvilla, A., Jacob, M., and Jacob, K. S. (2013). Clinical predictors of serum clozapine levels in patients with treatment-resistant schizophrenia. Int. Clin. Psychopharmacol. 28, 50–56. doi:10.1097/YIC.0B013E32835AC9DA
Sagud, M. (2015). Treatment-resistant schizophrenia: challenges and implications for clinical practice. Psychiatr. Danub 27, 319–326.
Siskind, D., McCartney, L., Goldschlager, R., and Kisely, S. (2016). Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis. Br. J. Psychiatry 209, 385–392. doi:10.1192/BJP.BP.115.177261
Siskind, D., Reddel, T., MacCabe, J. H., and Kisely, S. (2019). The impact of clozapine initiation and cessation on psychiatric hospital admissions and bed days: a mirror image cohort study. Psychopharmacol. Berl. 236, 1931–1935. doi:10.1007/S00213-019-5179-6
Siwek, M., Wojtasik-Bakalarz, K., Krupa, A. J., and Chrobak, A. A. (2023). Brexpiprazole-pharmacologic properties and use in schizophrenia and mood disorders. Brain Sci. 13, 397. doi:10.3390/BRAINSCI13030397
Suttajit, S., Arunpongpaisal, S., Srisurapanont, M., Thavichachart, N., Kongsakon, R., Chantakarn, S., et al. (2015). Psychosocial functioning in schizophrenia: are some symptoms or demographic characteristics predictors across the functioning domains?. Neuropsychiatr. Dis. Treat. 11, 2471–2477. doi:10.2147/NDT.S88085
Wagner, E., Löhrs, L., Siskind, D., Honer, W. G., Falkai, P., and Hasan, A. (2019). Clozapine augmentation strategies – a systematic meta-review of available evidence. Treat. options clozapine Resist. 33, 423–435. doi:10.1177/0269881118822171
Weise, J., Schomerus, G., and Speerforck, S. (2022). Add-on cariprazine in patients with long-term clozapine treatment and treatment resistant schizophrenia: two cases of psychotic deterioration and pisa syndrome. Clin. Psychopharmacol. Neurosci. 20, 398–401. doi:10.9758/CPN.2022.20.2.398
Wimberley, T., MacCabe, J. H., Laursen, T. M., Sørensen, H. J., Astrup, A., Horsdal, H. T., et al. (2017). Mortality and self-harm in association with clozapine in treatment-resistant schizophrenia. Am. J. Psychiatry 174, 990–998. doi:10.1176/APPI.AJP.2017.16091097
Yeh, T. C., Correll, C. U., Yang, F. C., Chen, M. H., Tseng, P. T., Hsu, C. W., et al. (2023). Pharmacological and nonpharmacological augmentation treatments for clozapine-resistant schizophrenia: a systematic review and network meta-analysis with normalized entropy assessment. Asian J. Psychiatr. 79, 103375. doi:10.1016/J.AJP.2022.103375
Keywords: clozapine resistance, negative symptoms, positive symptoms, psychosis, pharmacotherapy, antipsychotic drugs
Citation: Siwek M, Chrobak AA, Gorostowicz A, Król P and Dudek D (2024) Cariprazine augmentation of clozapine in schizophrenia—a retrospective chart review. Front. Pharmacol. 14:1321112. doi: 10.3389/fphar.2023.1321112
Received: 13 October 2023; Accepted: 06 December 2023;
Published: 04 January 2024.
Edited by:
Francisco Lopez-Munoz, Camilo José Cela University, SpainReviewed by:
Alessandro Cuomo, University of Siena, ItalyCopyright © 2024 Siwek, Chrobak, Gorostowicz, Król and Dudek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcin Siwek, bWFyY2luLnNpd2VrQHVqLmVkdS5wbA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.