
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 24 January 2024
Sec. Pharmacoepidemiology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1303382
This article is part of the Research Topic The Future of Third Molar Surgery View all 5 articles
 Régis Penha Pimenta1
Régis Penha Pimenta1 Cristiane Midori Takahashi1
Cristiane Midori Takahashi1 Silvio Barberato-Filho1Delaine Cristina Ferreira McClung2
Silvio Barberato-Filho1Delaine Cristina Ferreira McClung2 Fabio da Silva Moraes1Isabela Muniz de Souza2
Fabio da Silva Moraes1Isabela Muniz de Souza2 Cristiane de Cássia Bergamaschi1*
Cristiane de Cássia Bergamaschi1*Objectives: This review of systematic reviews evaluated the effectiveness and safety of the preemptive use of anti-inflammatory and analgesic drugs in the management of postoperative pain, edema, and trismus in oral surgery.
Materials and methods: The databases searched included the Cochrane Library, MEDLINE, EMBASE, Epistemonikos, Scopus, Web of Science, and Virtual Health Library, up to March 2023. Pairs of reviewers independently selected the studies, extracted the data, and rated their methodological quality using the AMSTAR-2 tool.
Results: All of the 19 studies reviewed had at least two critical methodological flaws. Third molar surgery was the most common procedure (n = 15) and the oral route the most frequent approach (n = 14). The use of betamethasone (10, 20, and 60 mg), dexamethasone (4 and 8 mg), methylprednisolone (16, 20, 40, 60, 80, and 125 mg), and prednisolone (10 and 20 mg) by different routes and likewise of celecoxib (200 mg), diclofenac (25, 30, 50, 75, and 100 mg), etoricoxib (120 mg), ibuprofen (400 and 600 mg), ketorolac (30 mg), meloxicam (7.5, 10, and 15 mg), nimesulide (100 mg), and rofecoxib (50 mg) administered by oral, intramuscular, and intravenous routes were found to reduce pain, edema, and trismus in patients undergoing third molar surgery. Data on adverse effects were poorly reported.
Conclusion: Further randomized clinical trials should be conducted to confirm these findings, given the wide variety of drugs, doses, and routes of administration used.
Postoperative responses such as pain, swelling, and trismus resulting from a physiological inflammatory process following surgical tissue injury have been widely investigated in dentistry. Intense prolonged deleterious effects can occur if adequate management of the post-surgical inflammatory process is not carried out (Cetira Filho et al., 2020). Psychological, anatomical, and neurophysiological aspects, as well as the type of dental surgery and surgical technique, number among the variables that can influence immediate and late postoperative responses (Ashley et al., 2016; Fonseca et al., 2017). A greater degree of tissue trauma leads to more intense inflammatory signs and symptoms. Excessive inflammation often causes exacerbated pain, swelling, and postoperative trismus. This ultimately impairs the quality of life of patients, directly impacting their daily routine (Varvara et al., 2017).
Opioid and non-opioid analgesics, non-steroidal anti-inflammatory drugs (NSAIDs), and steroidal anti-inflammatory drugs (corticosteroids) are analgesics used to control the physiological effects of dental surgical procedures, attenuating inflammatory reactions (Fonseca et al., 2017). Knowing the ideal timing of the action of these drugs can improve effectiveness in reducing postoperative responses (Thieme et al., 2020).
The literature has shown that analgesia in oral surgery can be effective if administered to the patient prior to the start of the procedure. This concept is referred to as preemptive analgesia and aims to control postoperative pain, swelling, and trismus (Penprase et al., 2015).
Preventive drugs are those administered before the onset of tissue damage and maintained for a given period after the surgical procedure has been completed. By contrast, preemptive drugs are administered before the start of surgery and not continued after the intervention. Both of these protocols involve drug administration prior to surgical incision in a bid to minimize intraoperative nociception and postoperative inflammatory responses (Doleman et al., 2018).
NSAIDs and corticosteroids are commonly used agents after dental surgery, administered alone or in combination (Au et al., 2015; Cetira Filho et al., 2020). Although long-term steroid therapy can lead to adverse effects, such as adrenal insufficiency, increased risk of infection, hyperglycemia, hypertension, osteoporosis, and development of diabetes mellitus, these effects are unlikely to occur at the low doses commonly used in dental surgical procedures (Larsen et al., 2018).
There is a dearth of systematic reviews investigating the effectiveness and safety of the preemptive use of anti-inflammatory and analgesic drugs after oral surgeries. A previous overview of systematic reviews provided a summary of the available evidence on the effectiveness and safety of using opioid and non-opioid analgesics in acute dental pain (Moore et al., 2018). However, the study failed to address the preemptive use of corticosteroids in dental surgery, and the search only included studies published up until 2017. The present review synthesized the available evidence from findings of published systematic reviews on the effectiveness and safety of the preemptive use of analgesic and anti-inflammatory drugs in the management of postoperative pain, edema, and trismus in oral surgery. More specifically, the review question was as follows: is the preemptive use of anti-inflammatory and analgesic drugs effective and safe for the management of postoperative pain, edema, and trismus in patients undergoing dental surgery aged 12 years or older?
This review of systematic reviews followed the protocol recommended by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2022) and was described according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021). The protocol was registered on PROSPERO, under number CRD42022352803.
Eligibility criteria were described using the population, intervention, comparison, outcome, and type of study (PICOT) framework.
Population: Patients, aged 12 years or older, undergoing dental surgery (third molar surgery, dental implant, periodontal surgery, dental extraction, soft and hard tissue grafts, or biopsies).
Intervention: Preemptive use of anti-inflammatory drugs (non-steroidal anti-inflammatory drugs/NSAIDs and corticosteroids) and analgesic drugs (opioids and non-opioids) at any dose.
Outcomes: Effectiveness and safety.
Comparator: Placebo or other active control.
Type of study: Systematic review of randomized clinical trials (RCTs).
Population: Patients undergoing dental surgery procedures performed under general anesthesia; patients diagnosed with malignant neoplasms, diabetes mellitus, hypertension, liver and kidney diseases; and immunosuppressed patients.
Intervention: Studies in which the time of drug use was uncertain or the drug was administered via the rectal route.
Type of study: Systematic review with all the RCTs included in another review. Abstracts presented at scientific events were also excluded.
Primary outcomes: Relief of inflammatory events such as pain, swelling/edema, and trismus. The description of symptoms may be by self-report, validated questionnaires, or clinical diagnosis.
Secondary outcomes: Improved quality of life, rescue medication, and the presence of adverse drug events.
The databases searched included the Cochrane Library, MEDLINE (via PubMed), EMBASE, Epistemonikos, Scopus, Web of Science, and Virtual Health Library. The search applied no language restrictions or time limits on the studies included. The information sources were searched to identify all relevant studies published up to 23 March 2023.
The reference lists of the reviews included were also checked by the reviewers to identify other relevant studies. When necessary, the corresponding authors of the studies were contacted for additional information.
The search strategy was devised using search terms based on Medical Subject Headings (MeSH) descriptors and is described in Supplementary Material SA.
Pairs of reviewers (RP and IM; CT and FM) independently assessed potentially relevant titles and abstracts and applied the eligibility criteria. The full text of systematic reviews was obtained. The same reviewers independently assessed the eligibility of each full text and settled any disagreements by consensus. Calibration exercises were performed for data extraction by using a standardized Excel form. A third reviewer (CB or SB-F) helped reach a final decision, when necessary.
The quality of systematic reviews was assessed independently by the same pairs of reviewers using the Assessing the Methodological Quality of Systematic Reviews-2 (AMSTAR-2) tool (Shea et al., 2017). This tool assesses the methodological aspects of systematic reviews using 16 items and classifies the overall confidence in the review results as follows: high (no or one non-critical weakness), moderate (more than one non-critical weakness), low (one critical flaw with or without non-critical weaknesses), and critically low (more than one critical flaw with or without non-critical weaknesses). Any disagreements were settled by consensus.
A data extraction worksheet was previously developed to record the information collected. Calibration exercises were conducted to ensure consistency across reviewers.
Extraction was carried out in accordance with the instruction manual prepared. Pairs of reviewers (CB and IM, CT and FM, and RP and DM) independently extracted the data and recorded information about patients, interventions, and comparators (drug, dose and route of administration, or placebo), follow-up time, and outcomes. Data were collected from systematic reviews, and, when necessary, RCTs were read to collect information.
In cases of missing information, the corresponding author of the study was contacted. Disagreements were settled by consensus, and any unresolved issues were referred to a third reviewer (CB or SB-F).
The results of the systematic reviews included were summarized by narrative synthesis and grouped by the type of surgery, drug class, and route of administration. The results of meta-analyses were collected based on outcomes assessed, according to the measures presented in the reviews [odds ratio, relative risk, weighted mean difference, 95% confidence interval (95% CI), and others].
The measure of heterogeneity was described mainly by I-square (I2), where 0%–25% indicated low heterogeneity, 50% moderate heterogeneity, and 75% high heterogeneity (Higgins et al., 2003).
The quality of evidence, when available, was collected for each outcome according to Grading of Recommendations Assessment, Development, and Evaluation (GRADE). This tool grades evidence as follows: high quality (confidence true effect is close to the estimate of effect); moderate quality (moderate confidence in effect estimate: true effect is likely to be close to the estimate of effect, but there is possibility it is substantially different); low quality (confidence in effect estimate is limited: true effect may be substantially different from the estimate of effect); and very low quality (very little confidence in effect estimate: true effect is likely to be substantially different from the estimate of effect) (Guyatt et al., 2013).
Ethical approval was not required for the present review of systematic reviews as this type of study does not involve the presentation of individual patient data.
A total of 2,101 records were initially identified. After the removal of duplicate records, 1,517 studies remained for title and abstract screening. Of the 90 studies eligible for full text reading, 19 systematic reviews were selected for data extraction (Figure 1). The list of excluded studies and reasons for exclusion are given in Supplementary Material SB.
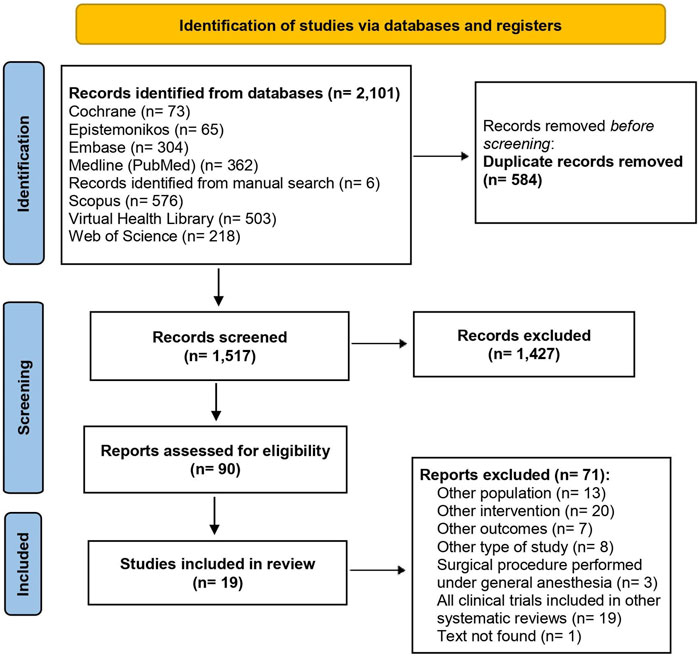
Figure 1. Flowchart of the included studies.
Nineteen systematic reviews, encompassing a total of 203 clinical trials (with overlap), published between 2008 and 2022, were included. Regarding procedures performed, third molar surgery (n = 16) predominated, followed by periodontal (n = 2), and implant (n = 1) surgery. In general, the reviews included RCTs with different routes of drug administration, with the oral route being the most investigated (n = 12). Of the reviews about third molar surgery, eight compared the use of corticosteroids versus placebo, four compared corticosteroids versus other drugs or placebo, and six evaluated the use of NSAIDs versus NSAIDs or placebo Table 1.
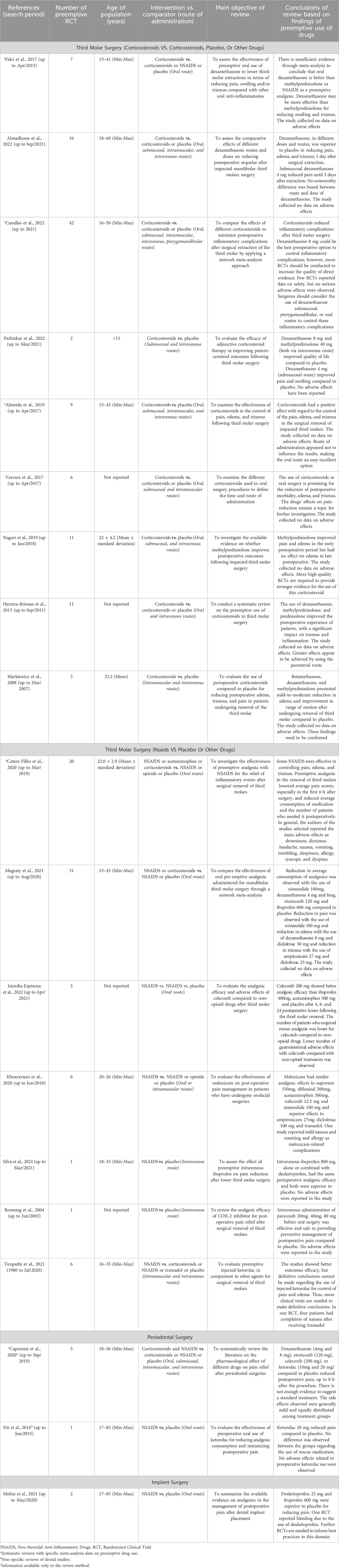
Table 1. Characteristics of systematic reviews on preemptive use of anti-inflammatory drugs and analgesics in dental procedures (n = 19).
Most reviews had at least two critical flaws, mainly related to the fact that they failed to explain the selection criteria for the designs of the studies included (n = 15), failed to provide the list of excluded studies (n = 13), and failed to report on funding sources for clinical trials (n = 17) Table 2.
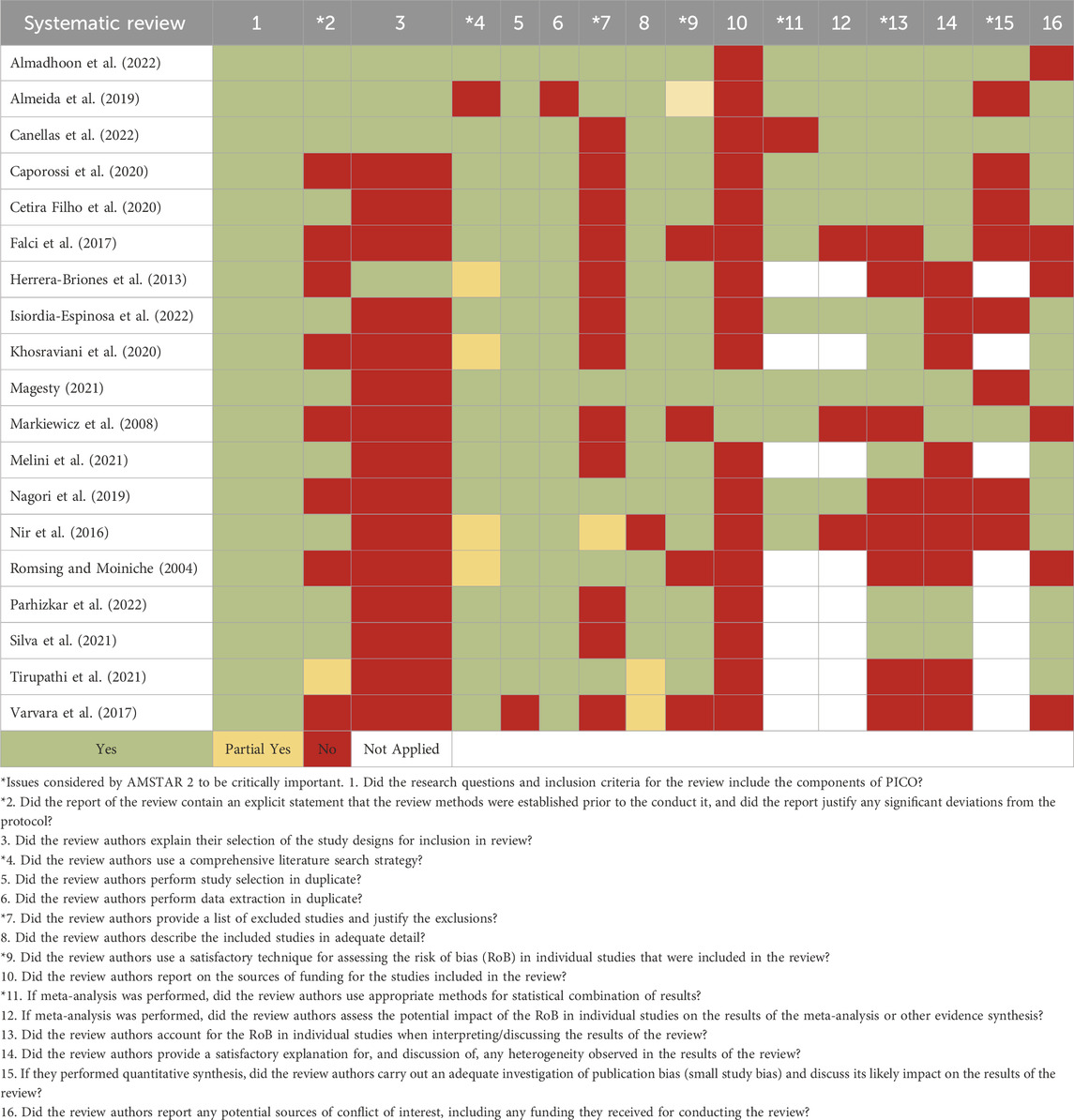
Table 2. Risk of bias of systematic reviews included (n = 19).
For reviews in which it was not possible to perform meta-analysis, or where the meta-analysis included RCTs not addressing preemptive use only, the results were described based on the main findings of the studies (Table 1).
The results of meta-analyses are presented in Table 3. Falci et al. (2017), Almeida et al. (2019), Caporossi et al. (2020), Almadhoon et al. (2022), and Canellas et al. (2022) evaluated the use of corticosteroids, while Caporossi et al. (2020) and Cetira Filho et al. (2020) assessed the use of NSAIDs.

Table 3. Results of meta-analysis on the use of corticosteroids (n = 5 reviews) and NSAIDs (n = 2 reviews).
The results were described by the type of dental procedure (third molar, implant, or periodontal surgery), class of drug (corticosteroids or NSAIDs), and route of administration (oral; submucosal; intramuscular, IM; or intravenous, IV).
Oral route: Meta-analyses showed that dexamethasone (8 mg) was superior to methylprednisolone (40 mg) for reducing trismus and swelling within 4 days (quality of evidence was not reported) (Table 3). However, the findings proved insufficient to state that the use of preemptive dexamethasone was superior to methylprednisolone or NSAIDs (Falci et al., 2017).
Meta-analyses evaluated the preemptive oral use of anti-inflammatory drugs compared to placebo. There was reduction in pain with the use of nimesulide (100 mg) up to 24 h after surgery (high quality of evidence). Reduction in edema was also observed with the use of dexamethasone (8 mg) (high quality of evidence) and diclofenac (50 mg). A reduction in trismus was observed with the use of ampiroxicam (27 mg) and diclofenac (25 mg), both on the first day after surgery. Reduction in the average consumption of analgesics was also attributed to the use of nimesulide (100 mg), dexamethasone (4 and 8 mg), etoricoxib (120 mg), and ibuprofen (600 mg) compared to placebo. The study collected no data on adverse effects. The quality of evidence, when reported, was low or moderate (Table 3) (Cetira Filho et al., 2020).
More than one route: A meta-analysis evaluated the use of corticosteroids compared to placebo (via oral, submucosal, IM, or IV routes). Dexamethasone (4 and 8 mg) and methylprednisolone (40, 60, and 80 mg) both showed superior results to placebo for pain relief (within 24 h) and trismus reduction (within 72 h after surgery). The quality of evidence was not reported (Table 3). The route of administration appeared not to influence results, with the oral route representing the easiest option (Almeida et al., 2019).
Indirect meta-analyses observed that dexamethasone (4 mg, pterygomandibular or submandibular routes), dexamethasone (8 mg, pterygomandibular or submandibular), triamcinolone (4 mg, submandibular), and methylprednisolone (40, 80 mg, oral) were more effective than placebo for reducing pain on the first day after surgery. Dexamethasone (0.1 mg/kg, IM route), dexamethasone (4 mg, submandibular), dexamethasone (8 mg, submandibular, IM, or IV), and methylprednisolone (40 mg, oral or submandibular) were more effective than placebo for this outcome on the second day after surgery (Canellas et al., 2022).
Dexamethasone (8 mg, submucosal or pterygomandibular routes) was more effective for reducing edema after 2 days of surgery. With regard to reducing trismus, dexamethasone (4 mg, submandibular route) and methylprednisolone (125 mg, IV route) were more effective than placebo 7 days postoperatively. Safety data were poorly reported by clinical trials, but no serious complications were attributed to the use of corticosteroid (Table 3). Overall, corticosteroids reduced inflammatory complications, where dexamethasone (8 mg) appeared to be the best preoperative option for controlling these events. However, further RCTs should be performed to improve the quality of evidence (Canellas et al., 2022).
Indirect meta-analyses observed that dexamethasone (4 mg, IM or submucosal or local anesthetic twin-mixed routes), compared to placebo, reduced pain outcome on the first day after surgery and dexamethasone (4 mg, oral, IM, submucosal, or IV) reduced pain on the third day after surgery. Trismus measurements were reduced with the use of dexamethasone (4 mg, IM, IV, submucosal, or admixed with local anesthetic) and of dexamethasone (4 and 8 mg, oral) compared to placebo on the first day after surgery. On the third day after surgery, dexamethasone (4 mg, IV, submucosal, or administered with local anesthetic) also reduced trismus compared to placebo. Swelling measurements were reduced after the use of dexamethasone (4 mg, IM, IV, submucosal, or admixed with local anesthetic) and of dexamethasone (4 and 8 mg, oral) compared to placebo 1 day postoperatively. Three days after surgery, swelling was reduced with the use of dexamethasone (4 mg, oral, IM, IV, submucosal, or admixed with local anesthetic) compared to placebo. However, the quality of evidence was low for most of the findings (Table 3). Safety data were not reported by Cetira Filho et al. (2020).
Dexamethasone (4 mg) and prednisolone (10 mg) were compared to dexamethasone (8 mg), prednisolone (20 mg), or placebo via the oral, submucosal, and IM routes. According to the authors, although corticosteroids reduced edema and trismus compared to placebo, the effects on pain reduction remained a topic for further investigation (Varvara et al., 2017).
Methylprednisolone (16, 40, 60, and 80 mg) via the oral, submucosal, and IV routes was evaluated. Oral methylprednisolone reduced pain and trismus in the early postoperative period and reduced late postoperative pain compared to placebo. The reported effects of submucosal methylprednisolone (40 mg) on pain and trismus were conflicting. Methylprednisolone (20, 40, 80, and 125 mg, by IV) had no significant effect on pain and trismus but reduced edema (Nagori et al., 2019).
Dexamethasone (4 and 8 mg), methylprednisolone (16, 20, 40, and 125 mg), and prednisolone (10 and 20 mg), by oral and IV routes, were compared to placebo. In general, these corticosteroids reduced trismus and swelling, promoting a superior effect for the IV route to the oral route (Herrera-Briones et al., 2013).
Betamethasone (60 mg, IM route), dexamethasone (4 mg, IV), and methylprednisolone (40, 80, and 125 mg, IV) were compared to placebo. Data from meta-analyses were not collected, since the review summarized the results of studies that evaluated the pre- and postoperative uses of these drugs. The findings showed that corticosteroids promoted mild-to-moderate reduction in early edema and trismus, but the confidence in findings was limited due to the small number of trials 24.
Dexamethasone (8 mg) and methylprednisolone (40 mg) (both IV route) compared to placebo had limited impact on the quality of life. Dexamethasone (4 mg, submucosal route) reduced pain (2nd to 10th days postoperatively) and swelling (2nd day postoperatively) compared to placebo. No significant group difference in the reduction of trismus was observed, and no adverse effects were reported (Parhizkar et al., 2022).
Oral route: Meta-analyses showed that preemptive analgesia with ibuprofen (400 mg), rofecoxib (50 mg), or diclofenac (50 mg) during the first 6 h postoperatively was superior to placebo or dexamethasone (8 mg) (moderate-quality evidence). NSAIDs (diclofenac 50, 100, or 150 mg; etoricoxib 90 mg; ibuprofen 400 and 800 mg; ibuprofen 600 mg + arginine 555 and 120 mg; and ketoprofen 100 and 150 mg) were associated with lower consumption of rescue medication than placebo, dexamethasone (8 mg), or codeine (30 mg) (moderate-quality evidence) (Table 3). The side effects most reported by the study were drowsiness, dizziness, headache, nausea, vomiting, trembling, sleepiness, allergy, syncope, and dyspnea (Cetira Filho et al., 2020).
Celecoxib (200 mg) was compared to ibuprofen (400 and 600 mg), acetaminophen (500 mg), and placebo at 4, 8, 24, and 48 h postoperatively. Celecoxib demonstrated better analgesic activity, with a lower number of patients requiring rescue analgesia than for the other drugs and placebo. The adverse effects reported were nausea (25%, 8.3%, and 18.1%), headache (14.1%, 9.2%, and 8.7%), and vomiting (11.3%, 1.3%, and 9.1%), as observed in placebo, celecoxib, and ibuprofen groups, respectively. Celecoxib had lower postoperative pain scores compared to acetaminophen, up until 12 h postoperatively. The number of patients requiring a rescue analgesic was lower in the celecoxib group than in the acetaminophen group (Isiordia-Espinoza et al., 2022).
IV route: The systematic review included one clinical trial that evaluated the preemptive use of parecoxib in third molar surgery. Parecoxib (20, 40, and 80 mg) was more effective for the management of postoperative pain than placebo. No reports of gastrointestinal, hematological, or renal adverse effects were found in the study (Romsing and Moiniche, 2004).
Oral and IM routes: Meloxicam (7.5, 10, and 15 mg, oral route) and meloxicam (7.5 and 15 mg, IM) were evaluated for postoperative pain management in patients undergoing third molar surgery. Meloxicam (any dose) had similar analgesic effects to naproxen (550 mg), diflunisal (500 mg), acetaminophen (500 mg), rofecoxib (12.5 mg), and nimesulide (100 mg) and a superior analgesic effect compared to ampiroxicam (27 mg), diclofenac (100 mg), salicylates, and tramadol (Khosraviani et al., 2020).
IM and IV routes: Ketorolac (30 mg, IM or IV routes) was compared to placebo or other drugs. Improvements in postoperative pain, median time taken for rescue medication, the total number of analgesics taken, and overall patient satisfaction were observed with the use of ketorolac (30 mg, IM) compared to diclofenac (75 mg, IM) and tramadol (50 mg, IV). However, further studies with a larger sample size are needed to inform best practices in this domain (Tirupathi et al., 2021).
The systematic review included one clinical trial which found that the preemptive use of ibuprofen (800 mg) + dexketoprofen (50 mg) or ibuprofen 800 mg (both IV route) reduced pain compared to placebo, within 48 h postoperatively. No adverse effects were reported (Silva et al., 2021).
Meta-analyses showed a superior effect of dexamethasone (4 and 8 mg, oral route) compared to placebo for controlling postoperative pain up to 8 h after surgery (moderate quality of evidence). There was also a superior effect of oral drugs etoricoxib (120 mg), celecoxib (200 mg), or ketorolac (10 and 20 mg) compared to placebo for controlling postoperative pain up to 8 h after the procedure (moderate quality of evidence) (Table 3). Regarding the occurrence of side effects, patients had no adverse effects after the use of analgesics in 16 studies. When side effects were reported, these were generally mild and equally distributed among treatment groups. The most frequently reported adverse effects were drowsiness, nausea, headache, and dizziness (Caporossi et al., 2020).
Another review included one clinical trial which showed that oral preemptive ketorolac 20 mg reduced pain compared to placebo. No difference was observed between the groups regarding the use of rescue medication (Nir et al., 2016).
Of the 11 clinical trials evaluating the use of analgesics after dental implant, two studies were specifically on oral preemptive use. The results showed that ibuprofen (600 mg) and dexketoprofen (25 mg) were superior to placebo for reducing pain. Further RCTs with an adequate sample size comparing standardized implant approaches are needed to inform best practices in this domain (Melini et al., 2021).
Of the total 203 RCTs identified within systematic reviews, 93 (45.8%) were included in more than one review. Data on the clinical trials included in systematic reviews (without overlap = 110) are described in Supplementary Materials SC, SD. Data on interventions, comparators, follow-up time, and main effectiveness and safety outcomes were extracted, with this information collected from reviews and RCTs, when necessary.
A total of 70 clinical trials evaluated the use of corticosteroids: dexamethasone by oral (n = 20), submucosal (n = 17), pterygomandibular (n = 4), IM (n = 9), and IV (n = 5) routes; methylprednisolone by oral (n = 3), IM (n = 3), and IV (n = 6) routes; and oral prednisolone (n = 3) (Supplementary Material SC).
A total of 40 clinical trials evaluating the use of NSAIDs are described as follows: ibuprofen by oral (n = 7) and IV (n = 1) routes; ketorolac by oral (n = 2), IM (n = 1), and IV (n = 3) routes; meloxicam by oral (n = 3) and IM (n = 2) routes; diclofenac by oral (n = 4) and IM (n = 1) routes; oral diflunisal (n = 2); oral nimesulide (n = 2); and oral celecoxib (n = 3). Oral acetaminophen was evaluated in three RCTs. Dexketoprofen, rofecoxib, tenoxicam, parecoxib, and tramadol were evaluated by only one RCT (Supplementary Material SD).
The present review summarized the available evidence on the preemptive use of anti-inflammatory and analgesic drugs in oral surgery. Third molar surgery was the dental procedure most investigated. The reviews evaluated the use of corticosteroids and NSAIDs, where none of the studies were restricted to the use of opioids and acetaminophen. The oral route was involved in most studies. Furthermore, the majority of the reviews had at least two critical methodological flaws. The outcomes most reported included pain, edema, and trismus, while safety findings were rarely reported by the reviews.
Based on the review results, patients can benefit from the preemptive use of betamethasone (10, 20, and 60 mg), dexamethasone (4 and 8 mg), methylprednisolone (16, 20, 40, 60, 80, and 125 mg), or prednisolone (10 and 20 mg) by different routes (oral, pterygomandibular, submandibular, submucosal, IM, or IV) to minimize postoperative inflammatory complications after third molar surgery. However, the reviews reported the need for further RCTs, given the wide variety of drugs, doses, and routes of administration used, as well as issues with the methodological quality of studies, limiting the reliability of their findings. Only 3 out of the 10 reviews on corticosteroids reported information on adverse reactions, and no serious adverse effects were associated with the use of these drugs.
Celecoxib (200 mg), diclofenac (25, 30, 50, 75, and 100 mg), etoricoxib (120 mg), ibuprofen (400 and 600 mg), ketorolac (30 mg), meloxicam (7.5, 10, and 15 mg), nimesulide (100 mg), and rofecoxib (50 mg) were studied for different routes (oral, IM, and IV) and compared to corticosteroids, other NSAIDs, placebo, and tramadol. These drugs appear to be effective mainly for reducing pain (outcome most reported by studies) in patients undergoing third molar surgery. Although six systematic reviews with NSAIDs reported adverse effects data, information was sparse. No serious adverse effects were reported with the preemptive use of NSAIDs.
Celecoxib (200 mg), dexamethasone (4 and 8 mg), etoricoxib (120 mg), and ketorolac (10 and 20 mg), administered by oral or submucosal or IM or IV routes, reduced postoperative pain compared to placebo and were considered safe for use in patients undergoing periodontal surgery. In implant surgery, findings for the preemptive use of drugs were available only for ibuprofen (600 mg) and dexketoprofen (25 mg). Both drugs were shown to reduce postoperative pain, although the reliability of these findings needs to be confirmed.
The literature search identified an overview of systematic reviews that summarized the available evidence on the effectiveness and safety of opioid and non-opioid analgesics in acute dental pain in a population which included children (Moore et al., 2018). In this study, corticosteroids were not studied, and the combination of ibuprofen and acetaminophen showed the greatest treatment benefit in pain reduction. Diflunisal, acetaminophen, and oxycodone had the longest duration of action in adult patients. The present study updated part of the findings of this review and also included corticosteroids, drugs widely used in dentistry.
The present study entailed a comprehensive literature search in which all stages of selection and data extraction were performed by reviewers, in pairs and independently. There was no restriction on the language of publication with respect to the reviews included. Although the quality of the evidence reported was based on information provided by the reviews and, hence, might have been affected by the methodological quality of the studies, the strength of this review was in providing an outline of the state of the art according to the available literature and to highlight information gaps.
It is important to note that adverse drug reactions, quality of life, and rescue medications were described by few systematic reviews, despite being relevant outcomes when assessing interventions. Furthermore, the heterogeneity of the reviews regarding drugs, doses, routes of administration, comparators, follow-up time, and outcomes, as well as the poorly reported quality of evidence, limited the findings of this review.
In general, the certainty of evidence of findings was poorly reported by the systematic reviews. In cases where certainty was evaluated, the quality of evidence tended to be rated as low or moderate, limiting the reliability of findings of the present review.
Preemptive analgesia in oral surgery has been widely performed for reduction and control of postoperative inflammatory processes. Most of the reviews included in the present study found that the use of corticosteroids and NSAIDs showed good results for reducing pain, edema, and trismus of patients undergoing dental surgeries. Cetira Filho et al. (2020) and Isiordia-Espinoza et al. (2022) reported the use of rescue medication, showing a reduction in medication consumption. However, the quality of evidence of these findings ranged from low to moderate.
Pain, swelling, and trismus often occur postoperatively and can affect the patient’s quality of life. Because it is a highly vascularized region of the body, there is a large release of exudate and mediators that cause the migration of inflammatory cells to the operated area (Cetira Filho et al., 2020). Oral surgery promotes injury to the surrounding tissues, producing pain, acute inflammation in the masseter muscle and submandibular regions, and trismus (Herrera-Briones et al., 2013). Thus, pharmacological management is designed to control and minimize these inflammatory sequelae.
The wide variety of clinical trials evaluating different drugs, doses, routes of administration, and follow-up times, precluded further analyses of specific or commonly used protocols for preemptive analgesia in dental surgery. Taken together, the findings of this review suggest that further RCTs with rigorous methodological designs should be carried out to provide clinical evidence on dose and administration route of drugs for the preemptive use in oral surgical procedures performed under local anesthesia. This information is valuable for the scientific community and dentists, contributing toward a better management of exacerbated inflammatory responses in intraoral surgical procedures.
The preemptive use of corticosteroids and NSAIDs can reduce pain, edema, and trismus in oral surgeries, particularly in third molar surgeries, the procedure most studied in the literature reviewed. These drugs also proved to be safe at the doses evaluated, although data on adverse effects were poorly reported. However, given the wide variety of drugs, doses, administration routes, and follow-up times, coupled with the low or moderate quality of evidence, further RCTs should be conducted to confirm these findings. The information can help guide the decision-making of patients and dentists on the use of drugs for preemptive analgesia and pave the way for future scientific studies defining more precise protocols for the preemptive use of these drugs in dental surgeries.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
RP: conceptualization, formal analysis, investigation, methodology, validation, visualization, writing–original draft, and writing–review and editing. CT: conceptualization, formal analysis, methodology, validation, visualization, writing–original draft, and writing–review and editing. SB-F: conceptualization, methodology, validation, visualization, writing–original draft, and writing–review and editing. DM: methodology, validation, visualization, and writing–review and editing. FM: formal analysis, methodology, visualization, writing–original draft, and writing–review and editing. IdS: formal analysis, methodology, validation, visualization, and writing–original draft. CB: conceptualization, formal analysis, investigation, methodology, project administration, supervision, validation, visualization, writing–original draft, and writing–review and editing.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1303382/full#supplementary-material
Almadhoon, H. W., Hamdallah, A., Abu Eida, M., Al-Kafarna, M., Atallah, D. A., AbuIriban, R. W., et al. (2022). Efficacy of different dexamethasone routes and doses in reducing the postoperative sequelae of impacted mandibular third-molar extraction: a network meta-analysis of randomized clinical trials. J. Am. Dent. Assoc. 153, 1154–1170. doi:10.1016/j.adaj.2022.08.017
Almeida, R. de A. C., Lemos, C. A. A., de Moraes, S. L. D., Pellizzer, E. P., and Vasconcelos, B. C. (2019). Efficacy of corticosteroids versus placebo in impacted third molar surgery: systematic review and meta-analysis of randomized controlled trials. Int. J. Oral Maxillofac. Surg. 48, 118–131. doi:10.1016/j.ijom.2018.05.023
Ashley, P. F., Parekh, S., Moles, D. R., Anand, P., and Macdonald, L. C. I. (2016). Preoperative analgesics for additional pain relief in children and adolescents having dental treatment. Cochrane Database Syst. Rev. 2016. doi:10.1002/14651858.CD008392.pub3
Au, A. H. Y., Choi, S. W., Cheung, C. W., and Leung, Y. Y. (2015). The efficacy and clinical safety of various analgesic combinations for post-operative pain after third molar surgery: a systematic review and meta-analysis. PLoS One 10. doi:10.1371/journal.pone.0127611
Canellas, J. V., Dos, S., Ritto, F. G., and Tiwana, P. (2022). Comparative efficacy and safety of different corticosteroids to reduce inflammatory complications after mandibular third molar surgery: a systematic review and network meta-analysis. Br. J. Oral Maxillofac. Surg. 60, 1035–1043. doi:10.1016/j.bjoms.2022.05.003
Caporossi, L. S., dos Santos, C. S., Calcia, T. B. B., Cenci, M. S., Muniz, F. W. M. G., and da Silveira Lima, G. (2020). Pharmacological management of pain after periodontal surgery: a systematic review with meta-analysis. Clin. Oral Investig. 24, 2559–2578. doi:10.1007/s00784-020-03401-6
Cetira Filho, E. L., Carvalho, F. S. R., de Barros Silva, P. G., Barbosa, D. A. F., Alves Pereira, K. M., Ribeiro, T. R., et al. (2020). Preemptive use of oral nonsteroidal anti-inflammatory drugs for the relief of inflammatory events after surgical removal of lower third molars: a systematic review with meta-analysis of placebo-controlled randomized clinical trials. J. Cranio-Maxillofacial Surg. 48, 293–307. doi:10.1016/j.jcms.2020.01.016
Doleman, B., Tp, H., Bhattacharjee, D., Jn, L., and Jp, W. (2018). Pre-emptive and preventive opioids for postoperative pain in adults undergoing all types of surgery (Review). Cochrane Database Syst. Rev., doi:10.1002/14651858.CD012624.pub2
Falci, S. G. M., Lima, T. C., Martins, C. C., Dos Santos, C. R. R., and Pinheiro, M. L. P. (2017). Preemptive effect of dexamethasone in third-molar surgery: a Meta-analysis. Anesth. Prog. 64, 136–143. doi:10.2344/anpr-64-05-08
Fonseca, P. R. B. da, Gatto, B. E. O., and Tondato, V. A. (2017). Post-trauma and postoperative painful neuropathy. Rev. Dor. 17, 59–62. doi:10.5935/1806-0013.20160050
Guyatt, G. H., Thorlund, K., Oxman, A. D., Walter, S. D., Patrick, D., Furukawa, T. A., et al. (2013). GRADE guidelines: 13. Preparing Summary of Findings tables and evidence profiles - continuous outcomes. J. Clin. Epidemiol. 66, 173–183. doi:10.1016/j.jclinepi.2012.08.001
Herrera-Briones, F. J., Prados Sánchez, E., Reyes Botella, C., and Vallecillo Capilla, M. (2013). Update on the use of corticosteroids in third molar surgery: systematic review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 116, e342–e351. doi:10.1016/j.oooo.2012.02.027
Higgins, J. P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2022). Cochrane Handbook for systematic reviews of interventions. Hoboken, New Jersey, United States: Wiley.
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327, 557–560. doi:10.1136/bmj.327.7414.557
Isiordia-Espinoza, M. A., Franco-González, M. A., Alonso-Castro, Á. J., and Franco-de la Torre, L. (2022). Analgesic effectiveness and safety of celecoxib versus non-opioid active controls after third molar surgery: a meta-analytical evaluation. J. Stomatol. Oral Maxillofac. Surg. 123, e1–e9. doi:10.1016/j.jormas.2021.06.015
Khosraviani, F., Saberi-Demneh, A., Asadollahifar, R., Nakhostin, A., and Khazaei, P. (2020). Post-operative pain management with meloxicam: a systematic literature review in the field of dentistry. Oral Surg. 13, 188–196. doi:10.1111/ors.12462
Larsen, M. K., Kofod, T., Christiansen, A.-E., and Starch-Jensen, T. (2018). Different dosages of corticosteroid and routes of administration in mandibular third molar surgery: a systematic review. J. oral Maxillofac. Res. 9, e1. doi:10.5037/jomr.2018.9201
Magesty, R. A. (2021). Analgesia preemptiva oral em cirurgias de terceiros molares inferiores: uma meta-análise em rede. Programa Pós-Graduação em Odontol. UFVJM 168.
Markiewicz, M. R., Brady, M. F., Ding, E. L., and Dodson, T. B. (2008). Corticosteroids reduce postoperative morbidity after third molar surgery: a systematic review and meta-analysis. J. Oral Maxillofac. Surg. 66, 1881–1894. doi:10.1016/j.joms.2008.04.022
Melini, M., Forni, A., Cavallin, F., Parotto, M., and Zanette, G. (2021). Analgesics for dental implants: a systematic review. Front. Pharmacol. 11, 634963–634969. doi:10.3389/fphar.2020.634963
Moore, P. A., Ziegler, K. M., Lipman, R. D., Aminoshariae, A., Carrasco-labra, A., and Mariotti, A. (2018). Benefits and harms associated with analgesic medications used in the management of acute dental pain: an overview of systematic reviews. J. Am. Dent. Assoc. 149, 256–265.e3. doi:10.1016/j.adaj.2018.02.012
Nagori, S. A., Jose, A., Roy, I. D., Chattopadhyay, P. K., and Roychoudhury, A. (2019). Does methylprednisolone improve postoperative outcomes after mandibular third molar surgery? A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 48, 787–800. doi:10.1016/j.ijom.2018.09.005
Nir, R. R., Nahman-Averbuch, H., Moont, R., Sprecher, E., and Yarnitsky, D. (2016). Preoperative preemptive drug administration for acute postoperative pain: a systematic review and meta-analysis. Eur. J. Pain (United Kingdom) 20, 1025–1043. doi:10.1002/ejp.842
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Parhizkar, P., Schmidlin, P. R., Bornstein, M. M., and Fakheran, O. (2022). Can adjunctive corticosteroid therapy improve patient-centered outcomes following third molar surgery? A systematic review. Oral Patol. Oral Cir. Bucal 27, e410–e418. doi:10.4317/medoral.25177
Penprase, B., Brunetto, E., Dahmani, E., Forthoffer, J. J., and Kapoor, S. (2015). The efficacy of preemptive analgesia for postoperative pain control: a systematic review of the literature. AORN J. 101, 94–105. doi:10.1016/j.aorn.2014.01.030
Romsing, J., and Moiniche, S. (2004). A systematic review of COX-2 inhibitors compared with traditional NSAIDs, or different COX-2 inhibitors for post-operative pain. Acta Anaesthesiol. Scand. 48, 525–546. doi:10.1111/j.0001-5172.2004.00379.x
Shea, B. J., Reeves, B. C., Wells, G., Thuku, M., Hamel, C., Moran, J., et al. (2017). AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358, j4008–j4009. doi:10.1136/bmj.j4008
Silva, P. U. J., Meneses-Santos, D., Vieira, W. A., Ramacciato, J. C., Silva, R. P. D., Silva, M. C. P. D., et al. (2021). Preemptive use of intravenous ibuprofen to reduce postoperative pain after lower third molar surgery: a systematic review of randomized controlled trials. Clin. (Sao Paulo. 76, e2780. doi:10.6061/clinics/2021/e2780
Thieme, R., Jennings, E., Nimmo, A., and Stokes, K. (2020). International prospective register of systematic reviews to investigate the efficacy of pre-emptive analgesia and the relationship with reducing post-operative side effects in dental patients: a systematic review and a meta analysis. Review question Pa. Natl. Inst. Heal. Reasearch, 1–5.
Tirupathi, S., Rajasekhar, S., Maloth, S. S., Arya, A., Tummalakomma, P., and Lanke, R. B. (2021). Pre-emptive analgesic efficacy of injected ketorolac in comparison to other agents for third molar surgical removal: a systematic review. J. Dent. Anesth. pain Med. 21, 1–14. doi:10.17245/jdapm.2021.21.1.1
Keywords: analgesics, oral surgical procedures, preoperative period, postoperative pain, anti-inflammatory
Citation: Pimenta RP, Takahashi CM, Barberato-Filho S, McClung DCF, Moraes FdS, de Souza IM and Bergamaschi CdC (2024) Preemptive use of anti-inflammatories and analgesics in oral surgery: a review of systematic reviews. Front. Pharmacol. 14:1303382. doi: 10.3389/fphar.2023.1303382
Received: 27 September 2023; Accepted: 22 December 2023;
Published: 24 January 2024.
Edited by:
Christos Kontogiorgis, Democritus University of Thrace, GreeceReviewed by:
Richard McGowan, New York University, United StatesCopyright © 2024 Pimenta, Takahashi, Barberato-Filho, McClung, Moraes, de Souza and Bergamaschi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristiane de Cássia Bergamaschi, Y3Jpc3RpYW5lLm1vdHRhQHByb2YudW5pc28uYnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.