 Yang Wang
Yang Wang Feng Wan
Feng Wan Peiqun Hu
Peiqun Hu Benxiang He4*
Benxiang He4* Yunlu Liu
Yunlu Liu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 15 November 2023
Sec. Ethnopharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1290755
This article is part of the Research Topic Women in Ethnopharmacology: 2023 View all 12 articles
Background: Acute ischemic stroke (AIS) is a leading cause of death and disability worldwide. This study aimed to evaluate the efficacy and safety of anisodine hydrobromide (Ani) injection in the treatment of AIS.
Methods: Randomized controlled trials (RCTs) based on Ani injection for the treatment of AIS were retrieved from both Chinese and English databases. The retrieval period was from the databases’ inception to May 2023. The Cochrane Collaboration Risk of Bias Tool was used to assess the methodological quality. The outcome indicators were analyzed using RevMan 5.3 software.
Results: We included the findings of 11 RCTs encompassing 1,337 patients with AIS. Our meta-analysis revealed that Ani injection supplementation significantly reduced the National Institutes of Health Stroke Scale [MD = −1.53, 95%CI = (−1.94, −1.12), p < 0.00001], modified Rankin Scale [MD = −0.89, 95%CI = (−0.97, −0.81), p < 0.00001], and the relative time to peak [SMD = −0.81, 95%CI = (−1.08, −0.55), p < 0.00001] significantly. Additionally, Ani injection significantly increased the Barthel Index [MD = 10.65, 95%CI = (4.30, 17.00), p = 0.001], relative cerebral blood volume [SMD = 0.28, 95%CI = (0.02, 0.53), p = 0.03], and clinical efficacy [RR = 1.2, 95%CI = (1.08, 1.34), p = 0.001]. No statistically significant difference in the rate of adverse events was observed between the Ani injection supplemental group and the control group.
Conclusion: Based on currently published evidence, Ani injection was found to be effective and safe in improving AIS outcome. Nevertheless, limitations of the included RCTs still exist, and thus, more multi-center, large-sample, high-quality RCTs are required to further verify the efficacy and safety of Ani injection in patients with AIS.
Systematic Review Registration: [https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023427591], identifier [PROSPERO 2023 CRD42023427591].
Acute ischemic stroke (AIS) is characterized by ischemia, hypoxic necrosis, and softening of the brain tissue due to a sudden interruption of the cerebral blood supply with inadequate collateral circulation, resulting in a series of symptoms of neurological dysfunction (Zhang et al., 2020). AIS is the most common type of cerebral stroke, accounting for approximately 70% of all strokes. Worldwide, AIS is a leading cause of death and disability (Wang et al., 2019). In China, the mortality rate of hospitalized AIS patients within 1 month of onset is approximately 2.3%–3.2%, the 1-year mortality rate after onset is 14.4%–15.4%, and the disability rate is 33.4%–33.8% (Wang et al., 2013; Wang et al., 2017). The associated socioeconomic burden of AIS is huge; for example, the annual expenditure related to AIS, including long-term rehabilitation and unemployment, is estimated to be £ 25.6 billion in the United Kingdom (Robert et al., 2020). Therefore, AIS has become a major global health concern.
At present, regular treatment of AIS consists of a multidisciplinary approach. Treatment management for AIS includes drug therapy, limb rehabilitation, language training, psychological rehabilitation, and health education (Trialists’Collaboration, 2013). Intravenous thrombolysis with recombinant tissue-type plasminogen activator (rtPA) and endovascular therapy have been the mainstay treatments for AIS in recent years (Powers et al., 2018). Both therapeutic strategies aim to rescue ischemic brain tissue with viable potential by recanalization of occluded cerebral arteries and reperfusion of the ischemic penumbra (Robert et al., 2020). Nevertheless, the number of patients with AIS who are eligible for such reperfusion strategies remains low due to the narrow time window of reperfusion therapy (Rodrigues et al., 2016; Bhaskar et al., 2018). More specifically, the therapeutic effect is heavily time dependent; therefore, the stroke symptom onset should be recorded accurately as a clock time to avoid treatment failure. Intravenous thrombolysis and endovascular thrombectomy for AIS patients with an unclear onset time require further exploration (Qiang et al., 2017). Furthermore, clinical evidence has shown that only patients with large vessel occlusive-type AIS are candidates for endovascular therapy, which accounts for less than 20% of AIS cases (Yasha et al., 2019). Symptomatic intracranial hemorrhage after thrombolysis and endovascular treatment in patients with AIS is a major complication that is associated with a devastating clinical outcome. The high frequency of intracranial hemorrhage poses a huge challenge to the clinical management of AIS (Seet and Rabinstein, 2012; Hao et al., 2017). In addition, as a serious complication of vascular recanalization, ischemia–reperfusion injury in the setting of cerebral ischemia following vascular restoration occurs because of a complex series of events, which can evoke parenchymal brain damage (Nour et al., 2013). Therefore, novel therapeutic strategies are urgently required to improve the efficacy and safety of AIS treatment.
A tenet of traditional folk medicine in China is that herbs possess the ability to treat various diseases. Modern researchers have demonstrated that compounds in these medicinal herbs, which consist of multiple ingredients, have multiple pharmacological actions, which are compatible with the complex pathogenesis of diverse human diseases (Chen et al., 2022). For many years in China, various traditional folk herbs have been applied in the treatment of AIS based on the theory of promoting blood circulation and removing blood stasis (Gong and Sucher, 2002). In-depth studies have elucidated the underlying mechanisms of the therapeutic effect of traditional medicinal herbs, which involve the inhibition of excitotoxicity, inflammation, oxidative damage, ionic imbalances, apoptosis, and so on, in the pathophysiological process of AIS (Sucher, 2006). A meta-analysis including 191 clinical trials involving 22 types of traditional Chinese medicine has demonstrated the improvement of neurological deficits after administration (Wu et al., 2007).
Anisodus tanguticus (Maxim.) Pascher, also named “Tang Chuan Na Bao” in Ethnologue, one of the indigenous Chinese ethnological plants of the Solanaceae, is mainly grown in the Qinghai–Tibet Plateau (Liu et al., 2005). In traditional Chinese medical theory, A. tanguticus possesses the traditional characteristics of nature of a warm, bitter flavor and functions to activate the blood to remove stasis (Chen et al., 2022). Anisodine, a tropane alkaloid extracted from the root of A. tanguticus, has been used as an ingredient in the compound preparation for treating ischemic stroke in China for more than a decade due to its significant properties of vasoactivity and improvements in microcirculation. To improve the chemical instability, researchers have developed a hydrobromide form of anisodine (Liu et al., 2020). Recently, anisodine hydrobromide (Ani) injection has been used in the clinical setting for the treatment of AIS in China. Multiple clinical studies have demonstrated the neuroprotective effect of Ani in AIS, which can not only alleviate neurological impairment and reduce dependency in activities of daily living but also improve the cerebral collateral circulation and increase cerebral tissue blood flow perfusion in ischemic areas (Zou et al., 2018; Zhang, 2022). Basic research has revealed that, as a central muscarinic cholinergic receptor blocker, the neuroprotective and cerebral circulation-promoting effect of Ani injection in the treatment of AIS can be correlated to the pharmacological actions of anti-oxidative damage, anti-inflammation, inhibition of neuronal apoptosis, and amelioration of hemorheological changes through regulation of the nitric oxide synthase system, preventing Ca2+ influx, decreasing IL-6 serum levels, and modulating angiogenic factors. Furthermore, the ability of Ani to activate the ERK1/2 signaling pathway and regulate ATPase activity is also a key underlying mechanism of action (Chen et al., 2017; Wang et al., 2017; Chen et al., 2017d; Xu et al., 2020; Zeng et al., 2021).
The impact of Ani injection on patients with AIS has been investigated in many clinical trials. In 2021, the earliest meta-analysis conducted by Wang et al. (2021) reported that Ani may have a positive effect in the treatment of ischemic stroke. However, the subjects included in Wang’s study were patients with ischemic stroke at various stages, including both the acute stage and the convalescent stage. In addition, the study objective of several included randomized controlled trials (RCTs) focused on the synergistic effect of Ani combined with acupuncture or butylphthalide. There were certain limitations without further assessment targeting each specific clinical stage (including the acute stage of ischemic stroke) and the pure effect of Ani injection. Therefore, the present study aimed to systematically collect the current clinical evidence regarding Ani injection in the treatment of the acute stage of ischemic stroke and, more specifically, evaluate its efficacy and safety. We hope this meta-analysis and systematic review will provide an accurate and reliable evidence-based reference for its rational use in the clinic.
This meta-analysis was performed in strict accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and was registered in PROSPERO (CRD42023427591).
Both English databases (including EMBASE, PubMed, Cochrane library, and Web of Science) and Chinese databases (including CNKI, VIP, Wanfang, and Chinese Biomedical Literature Database) were searched comprehensively from the date of their respective inception to May 2023 for the identification of eligible data. The following terms used in the search are a combination of MESH terms and free-text words: (“Anisodine hydrobromide injection” (Text word) OR “Anisodine hydrobromide” (Text word) OR “Anisodine” (Text word) AND [“Acute ischemic stroke” (Text Word) OR “ischemic stroke” (MESH) OR “brain ischemia” (MESH) OR “stroke” (MESH) OR “cerebral infarction” (MESH) OR “Cerebrovascular ischemia” (Text word) OR “Infarction, Anterior Cerebral Artery” (Text word) OR “Infarction, Middle Cerebral Artery” (Text word) OR “Infarction, Posterior Cerebral Artery” (Text word) OR “Apoplexy” (Text word)]. Potential studies in the reference lists of valid studies were also considered as information sources.
The inclusion criteria were as follows: 1) patients with AIS, regardless of age, gender, and disease stage; 2) parallel RCTs of Ani injection for AIS patients published in English or Chinese databases; 3) control group treated with regular therapies, while Ani injection was not applied in the control group; and 4) the trial groups were treated with Ani injection, used alone or in combination with the same regular therapies used in the control groups, regardless of the dose or duration of administration.
The exclusion criteria were as follows: 1) cerebral hemorrhage in patients with AIS; 2) reviews, letters, conference reports, cohort studies, case reports, cross-over studies, and animal studies; 3) duplicate studies or those with no comparison group; 4) literature without essential information or unable to obtain the related data; and 5) the trial group underwent acupuncture.
In this systematic review and meta-analysis, the primary outcomes were as follows: National Institutes of Health Stroke Scale (NIHSS), modified Rankin Scale (mRS), and Barthel Index (BI). The secondary outcomes were computed tomography parameters (CTP), effective rate, and adverse events.
All electronic bibliographic databases mentioned above were scanned with a pre-designed search strategy. Duplicate articles were removed first. Next, two independent reviewers reviewed the titles and abstracts of the studies to select appropriate studies according to the eligibility criteria. The full texts of the selected studies were downloaded for further assessment. Three initial articles were used as a pilot to establish a standard extraction form, which contains the following domains: study information (title, first author, language, magazine, and year of publication), participant information (e.g., age, sex ratio, sample size, and disease course), intervention information (e.g., type, duration, frequency, and dose of treatment in the trial and control groups), and outcome indexes (primary outcomes and secondary outcomes). Reasons for the exclusion of ineligible studies were identified and recorded. Available data were extracted by two independent reviewers from the full texts. The two reviewers addressed disagreements through discussion or via consultation with a third reviewer.
The Cochrane Collaboration Risk of Bias Tool in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2022) was used by two independent researchers to evaluate the methodological quality. According to the Cochrane Handbook, the risk of bias assessment was divided into seven domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other bias. Each domain in the included RCTs was marked according to a low risk of bias, high risk of bias, or an unclear risk of bias. Disagreement between the two researchers was arbitrated by a third researcher.
The RevMan 5.3 software was used for meta-analysis. The relative risk (RR) was used as the effect index for the dichotomous variables, and the mean differences (MD) or standardized mean difference (SMD) were used as the effect index for continuous variables. The confidence interval (CI) of each effect index was set to 95%. The I2 statistic was adopted to assess the heterogeneity. If I2 > 50%, there was heterogeneity between the studies, and the random-effect model was selected; otherwise, the fixed-effect model was utilized. The heterogeneity was explained by sensitivity analysis or subgroup analysis. In addition, descriptive analysis was performed if the clinical data provided by the included studies were incomplete and could not be systematically evaluated. Potential publication bias was evaluated through a funnel plot.
The PRISMA flowchart of the literature screening process is presented in Figure 1. Initially, according to the search strategy, a total of 179 studies were obtained through retrieval from multiple databases; after the deletion of 85 duplicate publications, the remaining 94 articles were screened. After examination of the titles and abstracts, 58 irrelevant studies were removed. The full texts of the 36 remaining articles were assessed for eligibility. Preclinical studies (n = 10), non-RCTs (n = 3), and studies that did not meet the inclusion or met the exclusion criteria (n = 12) were excluded. Finally, 11 studies were included in the meta-analysis (Zou et al., 2018; Wang et al., 2020; Dong et al., 2021; Li et al., 2021; Zhang et al., 2021; Jiang et al., 2022; Kang, 2022; Zhang, 2022; Zhang et al., 2022; Zhou, 2022; Yan et al., 2023).
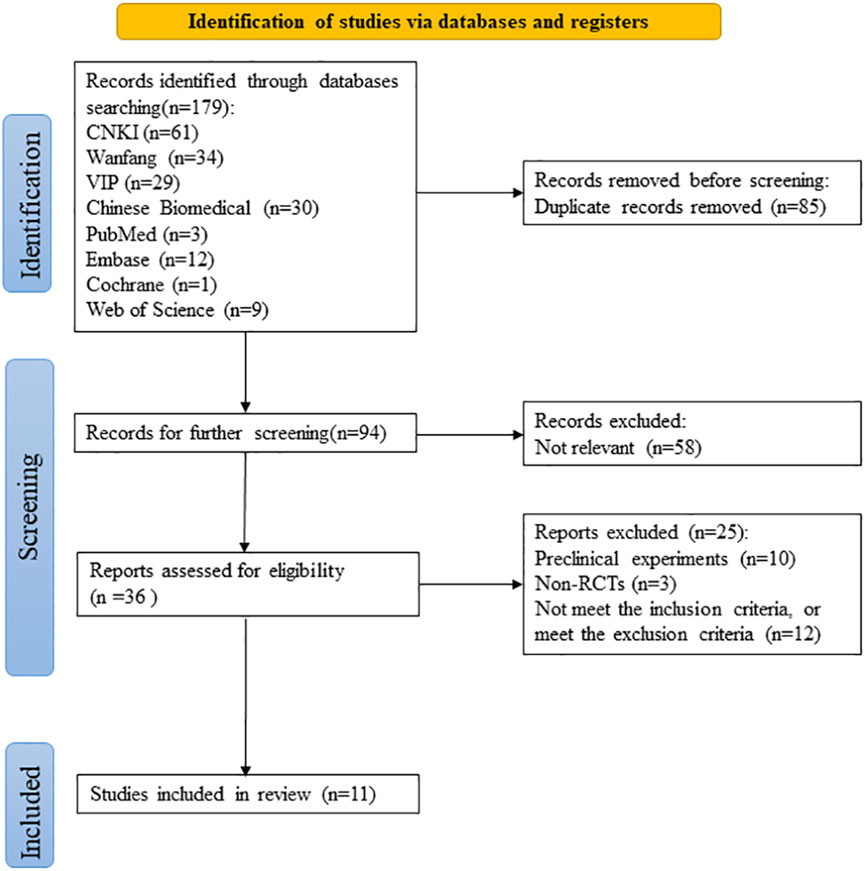
FIGURE 1. PRISMA flowchart for literature screening.
A total of 1,337 patients with AIS were included in the meta-analysis, including 668 patients in the trial group and 669 patients in the control group. All included studies were conducted in China. The sample size in each included study ranged from 21 to 193. The shortest treatment duration of an Ani injection was 7 days, and the longest was 30 days. The time period from AIS symptom onset to hospital admission was ≤72 h in all studies. Regarding the outcome measurements, the NIHSS was adopted in all studies (Zou et al., 2018; Wang et al., 2020; Dong et al., 2021; Li et al., 2021; Zhang et al., 2021; Jiang et al., 2022; Kang, 2022; Zhang, 2022; Zhang et al., 2022; Zhou, 2022; Yan et al., 2023), five studies used the mRS (Wang et al., 2020; Dong et al., 2021; Kang, 2022; Zhang, 2022; Zhang et al., 2022), four studies used the BI (Zou et al., 2018; Jiang et al., 2022; Zhang et al., 2022; Zhou, 2022), three studies reported the CTP (Zou et al., 2018; Zhang et al., 2022; Zhou, 2022), two studies mentioned the effective rate (Kang, 2022; Yan et al., 2023), and adverse events were described in seven studies (Zou et al., 2018; Dong et al., 2021; Li et al., 2021; Zhang et al., 2021; Jiang et al., 2022; Zhang, 2022; Zhang et al., 2022), while three studies reported the adverse rate (Dong et al., 2021; Li et al., 2021; Zhang et al., 2021). The characteristics of the included studies are presented in Table 1.
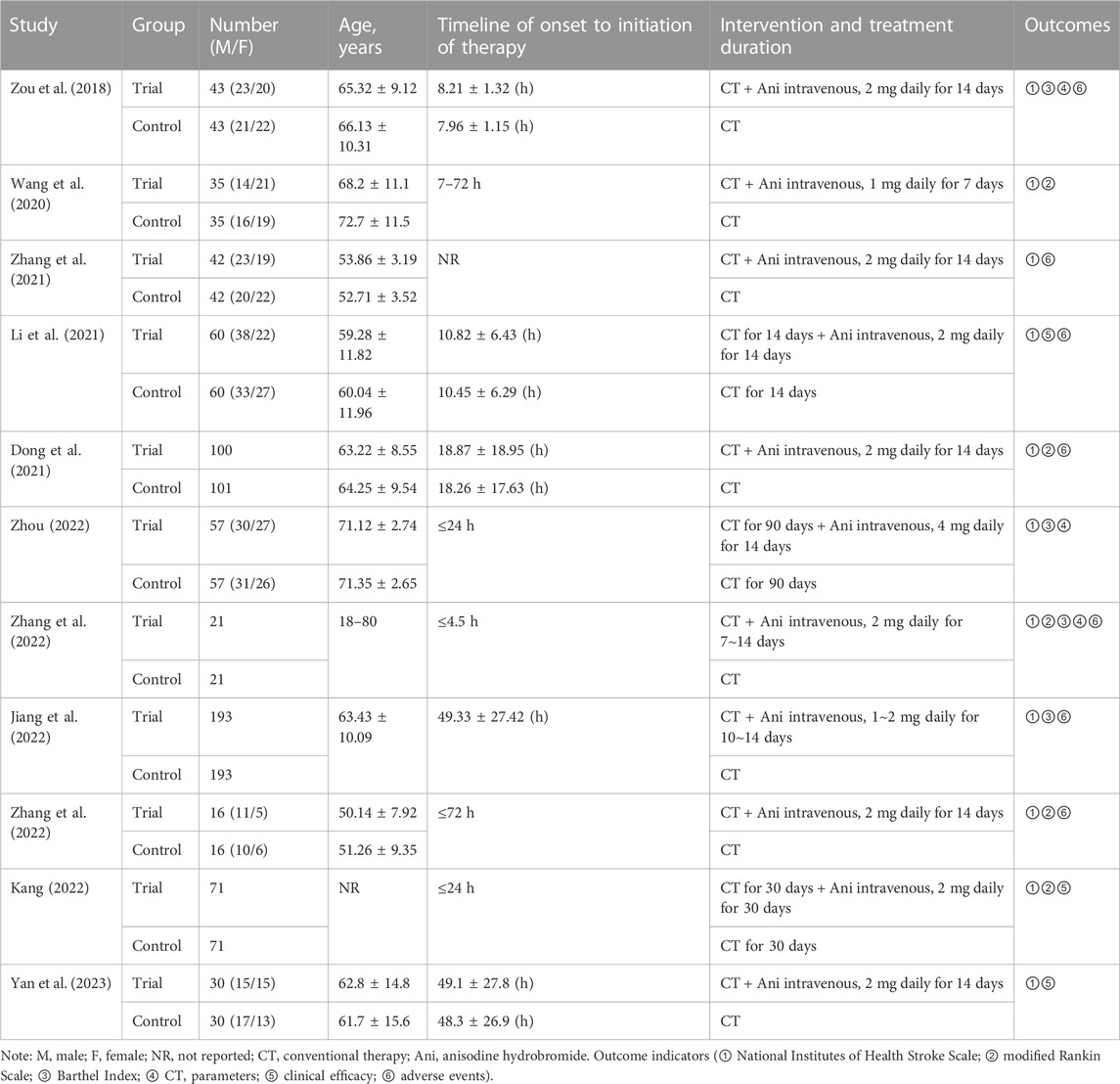
TABLE 1. Characteristics of included studies.
The assessment of bias risk of each eligible study was performed according to the Cochrane bias risk tool. Nine of the included studies mentioned grouping by a random method, three of which specified that a random sequence was generated through the random number table method (Dong et al., 2021; Li et al., 2021; Zhou, 2022). None of these studies referred to information on allocation concealment, blinding of participants and personnel, or blinding of the outcome assessment; therefore, all the studies were rated as having an unclear risk of bias in these three sections. All other bias evaluation risks were unclear. The results of the risk of bias assessment are presented in Figures 2, 3. See the supplementary document of Supplementary Material for rating bias (Supplementary Table S1).
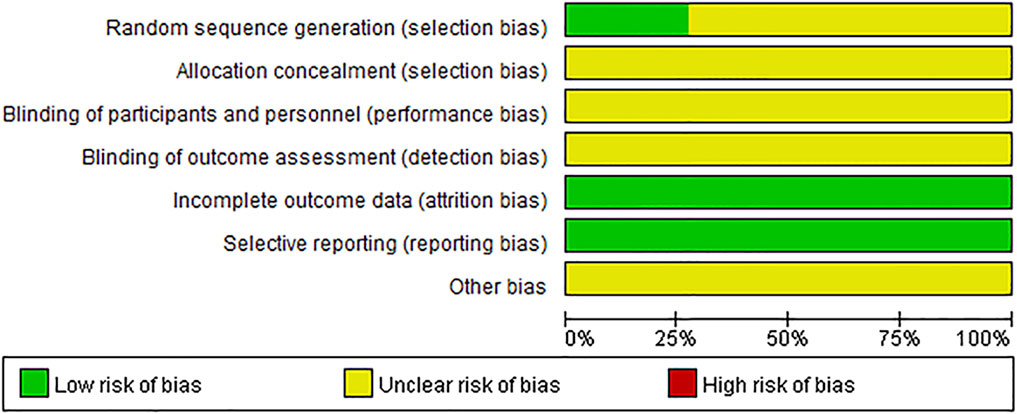
FIGURE 2. Risk of bias graph.
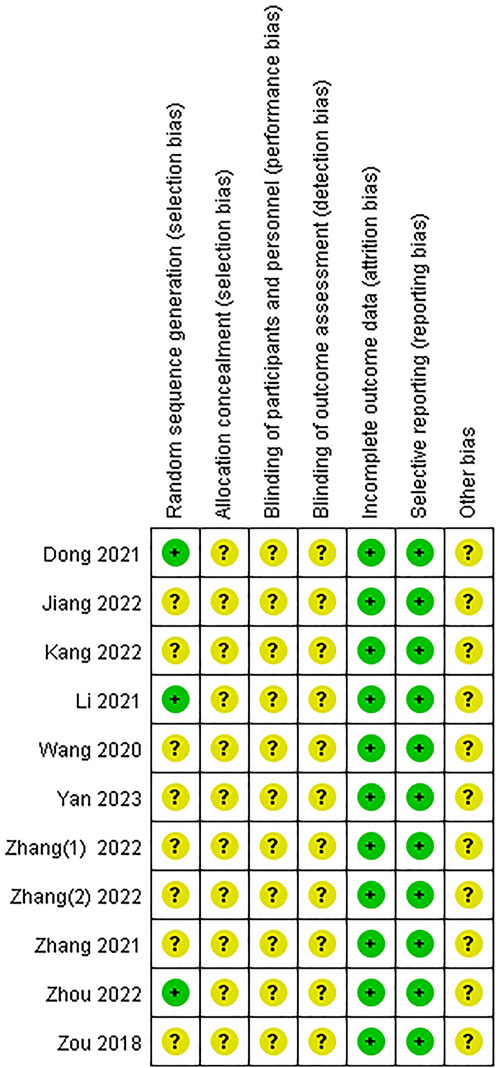
FIGURE 3. Risk of bias summary.
Eleven studies included the NIHSS score, of which one study (Zhang, 2022) did not report the post treatment NIHSS score; this data could not be extracted from the existing information. Thus, ten articles (Zou et al., 2018; Wang et al., 2020; Dong et al., 2021; Li et al., 2021; Zhang et al., 2021; Jiang et al., 2022; Kang, 2022; Zhang et al., 2022; Zhou, 2022; Yan et al., 2023) with 1,305 participants were included in the meta-analysis regarding the NIHSS score. The heterogeneity test results showed that p < 0.0001, I2 = 75%, and there was significant heterogeneity among the studies. Therefore, a random-effect model was adopted. The pooled results of the post-treatment NIHSS score indicated that compared with the control group, Ani injection could significantly reduce the NIHSS score after treatment [MD = −1.53, 95%CI = (−1.94, −1.12), p < 0.00001], as shown in Figure 4.
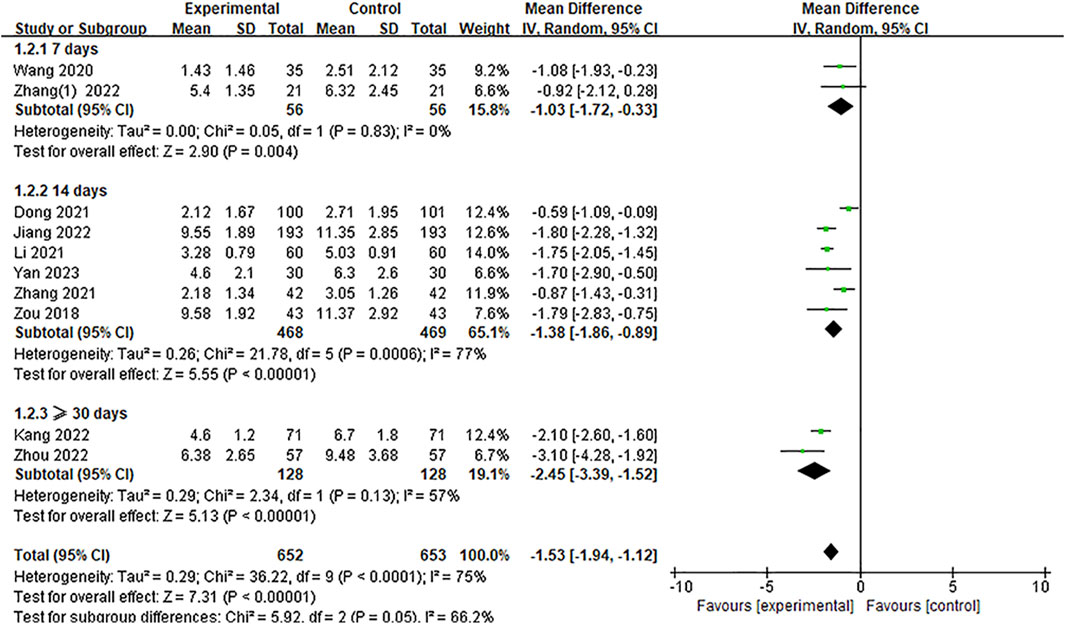
FIGURE 4. A meta-analysis of the NIHSS.
In these studies, the NIHSS score was evaluated at different treatment time periods, which ranged from 7 days to 90 days of treatment. Therefore, we used treatment duration to conduct further NIHSS evaluations (7 days, 14 days, and ≥30 days) as the criteria for the subgroup analysis. The results of the subgroup analysis are shown in Figure 4. It can be clearly seen that at the different time periods of 7 days, 14 days, and ≥30 days for implementing the NIHSS assessment, the NIHSS score of the experimental group was significantly lower than that of the control group [MD = −1.03, 95%CI = (−1.72, −0.33), p = 0.004; MD = −1.38, 95%CI = (−1.86, −0.89), p < 0.00001; MD = −2.45, 95%CI = (−3.39, −1.52), p < 0.00001, respectively]. The result of the subgroup differences (p = 0.05, I2 = 66.2%) indicated that this subgrouping factor might be a source of heterogeneity in the overall meta-analysis regarding the NIHSS score.
Five studies reported the mRS score; however, the data could not be extracted from one study (Dong et al., 2021) due to the provided data being dichotomous. Thus, a total of four studies (Wang et al., 2020; Kang, 2022; Zhang, 2022; Zhang et al., 2022) were included. The results of the heterogeneity test demonstrated that p = 0.81 and I2 = 0%; no significant heterogeneity was observed. Using the fixed-effect model, the results of the meta-analysis showed that the mRS score in the experimental group was significantly lower than that of the control group [MD = −0.89, 95%CI = (−0.97, −0.81), p < 0.00001], as shown in Figure 5.

FIGURE 5. A meta-analysis of mRS.
Four studies (Zou et al., 2018; Jiang et al., 2022; Zhang et al., 2022; Zhou, 2022) included the BI score. A meaningful increasing effect of Ani treatment was observed with the BI score level from the meta-analysis [MD = 10.65, 95%CI = (4.30, 17.00), p = 0.001]. Meanwhile, a significance between heterogeneity was observed (p < 0.00001, I2 = 96%); thus, a random-effect model was adopted for the meta-analysis (Figure 6). The test for subgroup differences between trials that adopted the BI measurement [two RCTs (Zhang et al., 2022; Zhou, 2022)] [MD = 5.82, 95%CI = (4.07, 7.57), p < 0.00001] and modified BI measurement [two RCTs (Zou et al., 2018; Jiang et al., 2022)] [MD = 15.10, 95%CI = (2.62, 27.59), p = 0.02] was non-significant (p = 0.15, I2 = 52%) (Figure 6).
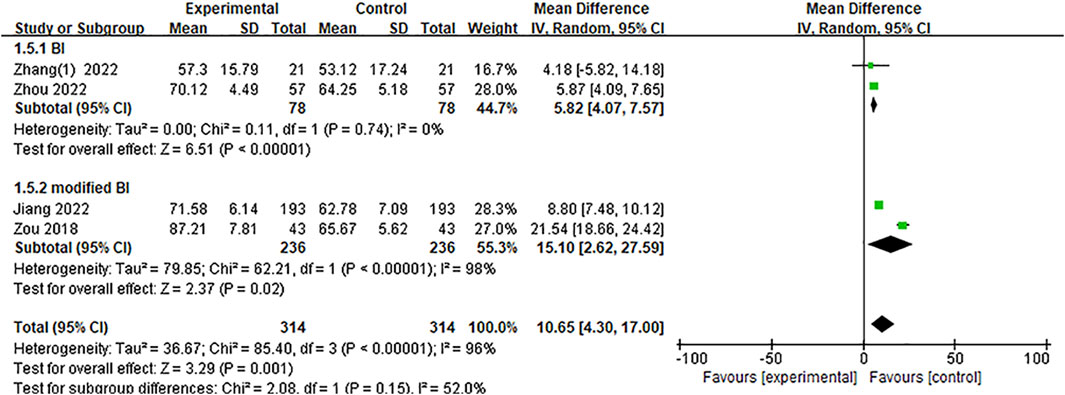
FIGURE 6. A meta-analysis of BI.
Three studies (Zou et al., 2018; Zhang et al., 2022; Zhou, 2022) reported the CTP, including relative cerebral blood flow (rCBF), relative cerebral blood volume (rCBV), relative time to peak (rTTP), and relative mean transit time (rMTT). The SMD was used as a summary statistic due to the consistency of the units in these studies being unclear. The pooled results indicated no statistically significant differences in the rCBF [SMD = 0.27, 95%CI = (−0.47, 1.01), p = 0.48] and rMTT [SMD = −0.71, 95%CI = (−2.20, 0.79), p = 0.35] between the Ani injection and the conventional therapy group and showed large heterogeneity (p = 0.0006, I2 = 87%; p < 0.00001, I2 = 96%, respectively) (Figures 7, 8). The effect of Ani injection on rCBF and rMTT, however, was not substantial. After sensitivity analysis by deleting one study (Zhang et al., 2022), the overall effect of Ani injection on rCBF and rMTT was significantly changed [SMD = 0.68, 95%CI = (0.40, 0.97), p < 0.00001; SMD = −1.57, 95%CI = (−1.89, −1.25), p < 0.00001, respectively]. Heterogeneity in both outcomes was also significantly reduced to 0%, which suggested that this study (Zhang et al., 2022) might be the source of the heterogeneity of the rCBF and rMTT data. Both the rCBV and rTTP levels were significantly changed by Ani injection therapy [SMD = 0.28, 95%CI = (0.02, 0.53), p = 0.03; SMD = −0.81, 95%CI = (−1.08, −0.55), p < 0.00001, respectively] without between-study heterogeneity (p = 0.36, I2 = 3%; p = 0.90, I2 = 0%, respectively) (Figures 9, 10).

FIGURE 7. A meta-analysis of rCBF.

FIGURE 8. A meta-analysis of rMTT.

FIGURE 9. A meta-analysis of rCBV.

FIGURE 10. A meta-analysis of rTTP.
Two studies (Kang, 2022; Yan et al., 2023) reported the clinical effective rate, which was evaluated according to the NIHSS score for stroke patients. The heterogeneity test results showed that there was no significant heterogeneity among these studies (p = 0.82, I2 = 0%); therefore, the fixed-effect model was adopted. The pooled results showed that the effective rate of the Ani injection-treated group was significantly better than that of the conventional therapy group [RR = 1.2, 95%CI = (1.08, 1.34), p = 0.001] (Figure 11).

FIGURE 11. A meta-analysis of clinical efficacy.
A total of seven articles (Zou et al., 2018; Dong et al., 2021; Li et al., 2021; Zhang et al., 2021; Jiang et al., 2022; Zhang, 2022; Zhang et al., 2022) recorded adverse reactions, of which two (Zhang, 2022; Zhang et al., 2022) reported that no adverse events occurred during treatment and two (Zou et al., 2018; Jiang et al., 2022) reported mild side effects, including dry mouth and facial flushing; these symptoms had completely disappeared after slowing down the drip rate.
The other three articles (Dong et al., 2021; Li et al., 2021; Zhang et al., 2021) reported the incidence of adverse reactions. Using the random-effect model (p = 0.12, I2 = 53%) for the meta-analysis, the pooled results showed that there were no significant differences between the Ani injection supplemental group and the control group [RR = 1.25, 95%CI = (0.52, 3.03), p = 0.62] (Figure 12). Dong et al. (2021) observed 12 cases of dry mouth and facial flushing in the experimental group and 8 cases of nausea and vomiting in the control group. Zhang et al. (2021) reported 6 cases of nausea, vomiting, dry mouth, and facial flushing in the control group and 2 cases of nausea and vomiting in the experimental group. Li et al. (2021) found 2 cases of elevated alanine aminotransferase (ALT), 2 cases of dizziness, 3 cases of weakness, and 6 cases of gastrointestinal reactions in the experimental group and 1 case of elevated ALT, 1 case of weakness, and 4 cases of gastrointestinal reactions in the control group. Table 2 presents the adverse reactions of the involved studies.
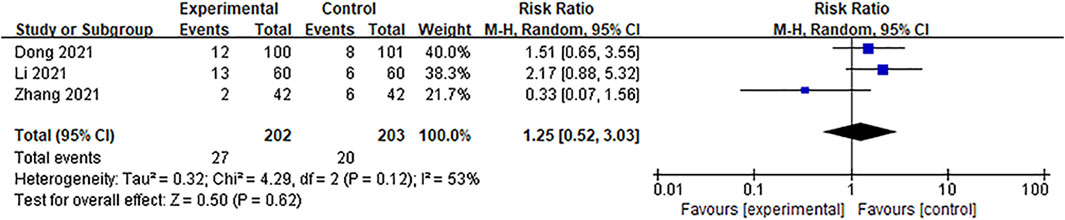
FIGURE 12. A meta-analysis of the rate of adverse events.
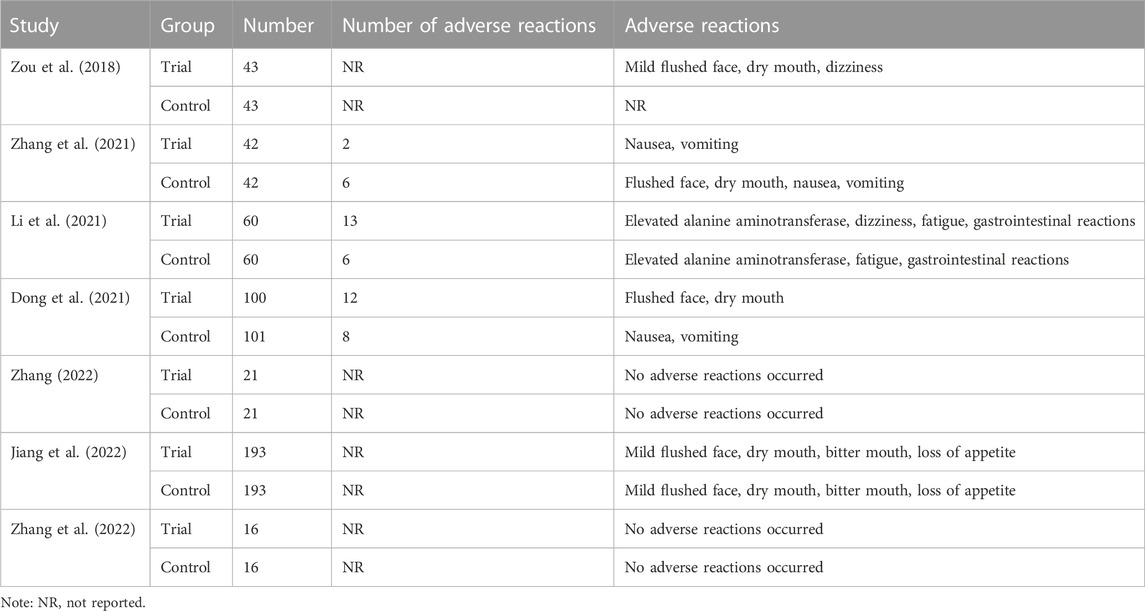
TABLE 2. Summary of adverse events of the involved studies.
A funnel plot was conducted to assess the publication bias of 10 trials or more. Thus, the 10 included studies that included available NIHSS score data were used for publication bias assessment, as shown in Figure 13. The shape of the funnel plot of the NIHSS showed the moderate symmetry between the included studies, which indicated that the potential of publication bias was low.
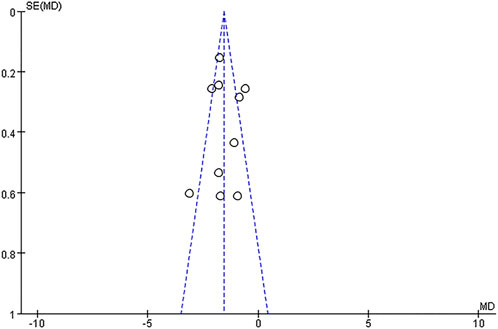
FIGURE 13. Funnel plot for the publication bias of the NIHSS.
A total of 11 RCTs were included in this meta-analysis. Combined with conventional therapy, Ani injection was used to treat 1,337 patients with AIS. The NIHSS, mRS, BI, CTP, effective rate, and adverse events were evaluated in the analysis. According to the findings, the NIHSS score of Ani injection therapy was much lower than that of conventional therapy alone. Other primary indicators showed that Ani injection significantly reduced the mRS score and increased the BI score. The secondary outcome indicators revealed that treatment with Ani injection increased the rCBV, reduced the rTTP, and improved the clinical efficacy, with significant differences observed. The pooled analysis of the included studies failed to identify a significant change in the rCBF, rMTT, and rate of adverse reactions.
Subgroup analyses indicated that at the different time periods of 7 days, 14 days, and ≥30 days for implementing the NIHSS assessment, the NIHSS score of the Ani treatment group was considerably decreased. Furthermore, the subgrouping factor might be a source of significant heterogeneity for the NIHSS. Subgroup analyses on the BI score based on the BI assessment method (original BI and modified BI) suggest that regardless of the BI assessment method used, Ani treatment exhibits an advantage in significantly increasing the BI score. However, the subgroup analysis of BI did not identify the source of heterogeneity; significant heterogeneity may be associated with factors such as small sample sizes and few included studies.
A sensitivity analysis of rCBF and rMTT suggested that the pooled results are not robust and that the study of Zhang et al. (2022) might be the source of rCBF and rMTT heterogeneity.
In the risk of bias section, the quality assessment of the current included studies showed that allocation concealment, blinding of participants and employees, and blinding of the outcome assessment, as well as other forms of bias, were not disclosed in any of the included studies, which suggested that the certainty of evidence in the included RCTs was not high. Consequently, the results of the meta-analysis may be influenced, and our findings based on the current evidence should be considered carefully in the clinic. More precise RCTs are needed to further validate the curative effect of Ani injection in patients with AIS.
Traditional Chinese herbal medicines have a long history of clinical application in treating various vascular diseases, with distinctive theories and rich practices (Hung et al., 2015; Hao et al., 2017). Products from traditional Chinese medicinal herbs have been widely described in various ancient medicine systems for treating ischemic stroke, myocardial infarction, and so on (Hung et al., 2015). Anisodine is one of the most important ingredients of the tropane-type alkaloids extracted from the traditional folk medicinal herb A. tanguticus, with significant biological activities for promoting blood circulation and removing blood stasis (Meng et al., 2023). Pharmaceutical products containing anisodine are frequently used in the clinic for the treatment of vascular diseases, including ischemic stroke (Zou et al., 2018), retinal artery occlusion (Wu et al., 2016), ischemic optic neuropathy (Zhang et al., 2019), and cerebral small vessel disease (Gui et al., 2019). Ani injection has been developed for improved chemical stability and is a promising treatment for AIS.
Poor perfusion of brain tissue caused by the abrupt interruption or reduction of cerebral blood flow is the etiology of AIS, which can then induce ischemic hypoxic necrosis, clinically manifesting as different degrees of neurological impairment (Brott and Bogousslavsky, 2000). The molecular mechanism of AIS can be summarized as a complex series of ischemic cascades, characterized by cellular bioenergetic failure, excitotoxicity, excessive intraneuronal accumulation of Na+, Cl−, and Ca2+, oxidative damage, inflammatory reaction, mitochondrial injury, and, finally, cell death (Rosenblum, 1997; Brouns and De Deyn, 2009). Guidelines for the management of AIS have been reported by various countries (Swain et al., 2008; Di et al., 2019; Powers et al., 2019); the fundamental goals of the intervention have been focused on restoring or increasing the blood supply to the brain and blockading or slowing of the cerebral ischemic cascade (Olsen et al., 1983; Escuret, 1995; Brott and Bogousslavsky, 2000). The conventional therapy adopted in the 11 included studies varied across different care settings, including general management (such as respiratory and oxygen intake, cardiac monitoring and cardiac disease management, temperature control, blood pressure control, blood sugar control, and nutritional support, etc.) and specific treatment (thrombolysis, antiplatelet drugs, anticoagulants, statins, defibrase, and diuretics, etc.). Nevertheless, the narrow treatment window and hemorrhagic complications have limited the utilization and therapeutic effect of conventional therapy.
Recent studies have revealed that in addition to the recanalization of the large cerebral vessels, the restoration of normal vasomotor function around the ischemic area, the improvement in micro-perfusion, and neuronal cell protection are crucial for the treatment of cerebral infarction and are closely related to the prognosis of AIS (Tuttolomondo et al., 2009; Shuaib et al., 2011; Bang et al., 2015). As a central muscarinic cholinergic antagonist, Ani can effectively relieve vasospasm, open closed arterioles and the anterior capillary sphincter, and restore the perfusion of brain tissue (Wang et al., 2018). Research has demonstrated that following Ani administration, the microvascular autonomic motion reappears in the small intestinal wall micro-artery ischemia model, with a significant increase in microvascular amplitude, blood velocity, and flow (Zhang et al., 2019). Through the establishment of a hypoxia/reoxygenation (H/R)-induced brain microvascular endothelial cell injury model, Ani injection has been shown to suppress H/R-induced hypoxia-inducible transcription factor 1(HIF-α) over-expression, nitric oxide (NO), and reactive oxygen species (ROS) production, and all these effects were dependent on M4-AchR (Zeng et al., 2021). Additionally, Ani has multiple non-cholinergic effects, including cell protective effects, autophagy (Chen et al., 2017b), attenuating neuronal cell death and apoptosis (Chen et al., 2017d), alleviating oxidative stress damage and decreasing Ca2+ accumulation (Chen et al., 2017; Wang et al., 2017; Chen et al., 2017e), and inhibiting membrane lipid peroxidation (Zhao and Chen, 2010), thereby alleviating cell damage caused by ischemia and hypoxia. Further studies have found that Ani can decrease the Longa rodent stroke scores and cerebral infarction area in middle cerebral artery occlusion (MCAO) rats (Chen et al., 2017c). Moreover, the underlying mechanism of the effect of Ani on AIS can also be attributed to the ability to improve hemorheology and resist platelet aggregation so as to improve cerebral microcirculation disorders (Xu et al., 2020).
In short, based on current evidence, Ani injection therapy was found to be effective and safe in patients with AIS. The positive effect of Ani injection may be attributed to the ability of Ani to penetrate the blood–brain barrier and act as a non-specific muscarinic cholinergic receptor antagonist, competing with acetylcholine in the central nervous system, resulting in increased cerebral blood supply and neuroprotection effects (Liu et al., 2020; Jiang et al., 2022). The results of this meta-analysis demonstrated that the efficacy of Ani injection in the treatment of AIS was superior to that of conventional therapy; however, several limitations still exist. First, the sample size of the included RCTs was small, so the subgroup analysis and publication bias assessment could not be conducted for all indicators, which may have affected the accuracy and reliability of the results. Second, all trials lacked a precise description of the allocation concealment and blinding methods (for participants, personnel, and outcome assessments); the description of random sequence generation was also missed in some studies. As a consequence, the general methodological quality of the studies was not satisfactory. Third, the longest intervention duration in all the articles was 90 days, and there was a lack of long-term follow-up visits for more than 90 days after treatment, which was insufficient to assess the long-term impact of Ani therapy on the health of patients. Additionally, all the included RCTs were conducted in China; therefore, it is necessary to utilize multi-regional clinical trials for Ani treatment evaluation in different regions of the world in the future to provide strong evidence for the efficacy and safety of Ani treatment in patients with AIS.
Taken together, the meta-analysis results from the included RCTs revealed that Ani injection is effective and safe in the treatment of patients with AIS, with positive impacts on the NIHSS, mRS, BI, rCBV, rTTP, and clinical efficacy. However, due to limitations in the number and quality of included studies, more multi-center, large-sample, high-quality RCTs are needed for further verification of the efficacy and safety of Ani injection in treating AIS.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
YW: Data curation, Formal Analysis, Methodology, Writing–original draft. FW: Conceptualization, Investigation, Writing–review and editing. PH: Data curation, Investigation, Writing–review and editing. BH: Funding acquisition, Supervision, Writing–review and editing. YH: Funding acquisition, Supervision, Writing–review and editing. YL: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Writing–original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Natural Science Foundation of Sichuan Province (No. 2022NSFSC1529), S&T Project of Sichuan Provincial Administration of Traditional Chinese Medicine (No. 2021MS519), and the Fund of Key Laboratory for Sports Medicine of Sichuan Province and General Administration of Sport (No. 2023-A032).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1290755/full#supplementary-material
Bang, O. Y., Goyal, M., and Liebeskind, D. S. (2015). Collateral circulation in ischemic stroke: assessment tools and therapeutic strategies. Stroke 46 (11), 3302–3309. doi:10.1161/strokeaha.115.010508
Bhaskar, S., Stanwell, P., Cordato, D., Attia, J., and Levi, C. (2018). Reperfusion therapy in acute ischemic stroke: dawn of a new era? BMC Neurol. 18 (1), 8. doi:10.1186/s12883-017-1007-y
Brott, T., and Bogousslavsky, J. (2000). Treatment of acute ischemic stroke. N. Engl. J. Med. 343 (10), 710–722. doi:10.1056/nejm200009073431007
Brouns, R., and De Deyn, P. P. (2009). The complexity of neurobiological processes in acute ischemic stroke. Clin. Neurology Neurosurg. 111 (6), 483–495. doi:10.1016/j.clineuro.2009.04.001
Chen, C., Peng, C., Wan, F., Liu, H., Ao, H., and Xie, X. (2017a). Study on the mechanism of action of anisodine hydrobromide against acute cerebral ischemia/reperfusion injury in rats. Chin. Pharmacol. Bull. 33 (8), 1096–1102. doi:10.3969/j.issn.1001-1978.2017.08.012
Chen, C., Wang, B., Li, J., Xiong, F., and Zhou, G. (2022). Multivariate statistical analysis of metabolites in anisodus tanguticus (maxim.) pascher to determine geographical origins and network Pharmacology. Front. Plant Sci. 13, 927336. doi:10.3389/fpls.2022.927336
Chen, D., Peng, C., Li, M., Yu, S., Wan, F., and Xie, X. (2017b). Autophagy participates in the protective effect of anisodine hydrobromide on PC12 cell damage under hypoxic conditions. Chin. J. Exp. Traditional Med. Formulae 23 (20), 144–149. doi:10.13422/j.cnki.syfjx.2017200144
Chen, D., Peng, C., Xie, X., Ao, H., Pan, Y., Liu, H., et al. (2017c). Protective effect of anisodine hydrobromide on acute cerebral ischemia-reperfusion injury in rats. Heilongjiang animal Sci. veterinary Med. 26 (5), 51–54. doi:10.13881/j.cnki.hljxmsy.2017.0766
Chen, D., Peng, C., Xie, X., Chen, Q., Liu, H., Zhang, S., et al. (2017d). Low dose of anisodine hydrobromide induced neuroprotective effects in chronic cerebral hypoperfusion rats. CNS Neurol. Disord. Drug Targets 16 (10), 1111–1119. doi:10.2174/1871527316666171026114043
Chen, D., Xie, X., Wan, F., Liu, H., Chen, S., Chen, Q., et al. (2017e). The effect of anisodine hydrobromide on brain tissue cell apoptosis and ERK1/2 phosphorylation level in acute cerebral ischemia-reperfusion injury model rats. China Pharm. 28 (28), 3907–3910. doi:10.6039/j.issn.1001-0408.2017.28.06
Di, Z., Shu-ting, Z., and Bo, W. (2019). Interpretation of" Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018. Chin. J. Contemp. Neurology Neurosurg. 19 (11), 897–901. doi:10.3969/j.issn.1672-6731.2019.11.015
Dong, Z., Han, L., Duan, P., Liang, J., Dong, R., Liu, N., et al. (2021). Anisodine hydrobromide injection for the treatment of acute ischemic stroke: a randomized controlled trial. J. Pharmacoepidemiol. 30 (5), 296–300. doi:10.19960/j.cnki.issn1005-0698.2021.05.002
Escuret, E. (1995). Cerebral ischemic cascade. Ann. francaises d'anesthesie de Reanim. 14 (1), 103–113. doi:10.1016/s0750-7658(05)80158-3
Gong, X., and Sucher, N. J. (2002). Stroke therapy in traditional Chinese medicine (TCM): prospects for drug discovery and development. Phytomedicine 9 (5), 478–484. doi:10.1078/09447110260571760
Gui, Y., Du, R., Sun, Y., Guo, Z., Tian, J., Li, L., et al. (2019). Clinical study of anisodine hydrobromide in treatment of cognitive impairment associated with cerebral small vessel disease. World Clin. Drugs 40 (12), 850–857. doi:10.13683/j.wph.2019.12.006
Hao, P., Jiang, F., Cheng, J., Ma, L., Zhang, Y., and Zhao, Y. (2017a). Traditional Chinese medicine for cardiovascular disease: evidence and potential mechanisms. J. Am. Coll. Cardiol. 69 (24), 2952–2966. doi:10.1016/j.jacc.2017.04.041
Hao, Y., Zhang, Z., Zhang, H., Xu, L., Ye, Z., Dai, Q., et al. (2017b). Risk of intracranial hemorrhage after endovascular treatment for acute ischemic stroke: systematic review and meta-analysis. Interv. Neurol. 6 (1-2), 57–64. doi:10.1159/000454721
Higgins, J. P. T., Thomas, J., and Chandler, J. (2022). Cochrane Handbook for systematic reviews of interventions version 6.3. Available from: www.training.cochrane.org/handbook (Accessed February 22, 2022).
Hung, I. L., Hung, Y. C., Wang, L. Y., Hsu, S. F., Chen, H. J., Tseng, Y. J., et al. (2015). Chinese herbal products for ischemic stroke. Am. J. Chin. Med. 43 (7), 1365–1379. doi:10.1142/s0192415x15500779
Jiang, R., Zheng, W., and Yi, K. (2022). The effect and safety of anisodine hydrobromide as an adjuvant treatment for acute ischemic stroke on neurological function and activity of life in patients. Chin J Clin. Ration. Drug Use 15 (11), 49–51.
Kang, X. (2022). The effect of anisodine hydrobromide injection combined with butylphthalide injection in the treatment of acute ischemic stroke. Med. INNOVATION CHINA 19 (9), 58–62. doi:10.3969/j.issn.1674-4985.2022.09.015
Li, W., Wang, H., Cao, J., and Yu, R. (2021). Study on the therapeutic effect of anisodine hydrobromide combined with butylphthalide in the treatment of progressive cerebral infarction and its impact on neurological function. Chin. J. Ration. Drug Use 18 (4), 62–65. doi:10.3969/j.issn.2096-3327.2021.4.015
Liu, T., Zhu, P., Cheng, K. D., Meng, C., and He, H. X. (2005). Molecular cloning, expression and characterization of hyoscyamine 6beta-hydroxylase from hairy roots of Anisodus tanguticus. Planta Med. 71 (03), 249–253. doi:10.1055/s-2005-837825
Liu, Y., Wang, L., Wan, F., and Yang, N. (2020). Effects of anisodine hydrobromide on the cardiovascular and respiratory functions in conscious dogs. Drug Des. Dev. Ther. 14, 4263–4276. doi:10.2147/DDDT.S268113
Meng, C. W., Zhao, H. Y., Zhu, H., Peng, C., Zhou, Q. M., and Xiong, L. (2023). Novel indane derivatives with antioxidant activity from the roots of anisodus tanguticus. Molecules 28 (3), 1493. doi:10.3390/molecules28031493
Nour, M., Scalzo, F., and Liebeskind, D. S. (2013). Ischemia-reperfusion injury in stroke. Interv. Neurol. 1 (3-4), 185–199. doi:10.1159/000353125
Olsen, T. S., Larsen, B., Herning, M., Skriver, E. B., and Lassen, N. A. (1983). Blood flow and vascular reactivity in collaterally perfused brain tissue. Evidence of an ischemic penumbra in patients with acute stroke. Stroke 14 (3), 332–341. doi:10.1161/01.str.14.3.332
Powers, W. J., Rabinstein, A. A., Ackerson, T., Adeoye, O. M., Bambakidis, N. C., Becker, K., et al. (2018). 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American heart association/American stroke association. Am. Heart Association/American Stroke Assoc. 49 (3), e46–e99. doi:10.1161/str.0000000000000158
Powers, W. J., Rabinstein, A. A., Ackerson, T., Adeoye, O. M., Bambakidis, N. C., Becker, K., et al. (2019). Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke 50 (12), e344–e418. doi:10.1161/str.0000000000000211
Qiang, D., Yi, D., Liping, L., Anding, X., Yusheng, Z., Huaguang, Z., et al. (2017). The Chinese Stroke Association scientific statement: intravenous thrombolysis in acute ischaemic stroke. Stroke Vasc. Neurology 2 (3), 147–159. doi:10.1136/svn-2017-000074
Robert, H., Alakendu, S., Tom, A. T. H., and Keith, W. M. (2020). Diagnosis and management of acute ischaemic stroke. Pract. Neurol. 20 (4), 304–316. doi:10.1136/practneurol-2020-002557
Rodrigues, F. B., Neves, J. B., Caldeira, D., Ferro, J. M., Ferreira, J. J., and Costa, J. (2016). Endovascular treatment versus medical care alone for ischaemic stroke: systematic review and meta-analysis. BMJ 353, i1754. doi:10.1136/bmj.i1754
Rosenblum, W. I. (1997). Histopathologic clues to the pathways of neuronal death following ischemia/hypoxia. J. neurotrauma 14 (5), 313–326. doi:10.1089/neu.1997.14.313
Seet, R. C. S., and Rabinstein, A. A. (2012). Symptomatic intracranial hemorrhage following intravenous thrombolysis for acute ischemic stroke: a critical review of case definitions. Cerebrovasc. Dis. 34 (2), 106–114. doi:10.1159/000339675
Shuaib, A., Butcher, K., Mohammad, A. A., Saqqur, M., and Liebeskind, D. S. (2011). Collateral blood vessels in acute ischaemic stroke: a potential therapeutic target. Lancet Neurol. 10 (10), 909–921. doi:10.1016/s1474-4422(11)70195-8
Sucher, N. J. (2006). Insights from molecular investigations of traditional Chinese herbal stroke medicines: implications for neuroprotective epilepsy therapy. Epilepsy & Behav. 8 (2), 350–362. doi:10.1016/j.yebeh.2005.11.015
Swain, S., Turner, C., Tyrrell, P., and Rudd, A.Guideline Development Group (2008). Diagnosis and initial management of acute stroke and transient ischaemic attack: summary of NICE guidance. Bmj 337, a786. doi:10.1136/bmj.a786
Trialists’Collaboration, S. U. (2013). Organised inpatient (stroke unit) care for stroke. J. Cochrane database Syst. Rev. 9 (9). doi:10.1002/14651858.CD000197
Tuttolomondo, A., Di Sciacca, R., Di Raimondo, D., Arnao, V., Renda, C., Pinto, A., et al. (2009). Neuron protection as a therapeutic target in acute ischemic stroke. Curr. Top. Med. Chem. 9 (14), 1317–1334. doi:10.2174/156802609789869646
Wang, D., Liu, J., Liu, M., Lu, C., Brainin, M., and Zhang, J. (2017a). Patterns of stroke between university hospitals and nonuniversity hospitals in mainland China: prospective multicenter hospital-based registry study. World Neurosurg. 98, 258–265. doi:10.1016/j.wneu.2016.11.006
Wang, L., Mao, L., and Chen, W. (2020). Clinical observation on the treatment of acute cerebral infarction with anisodine hydrobromide injection. Chin. Community Dr. 36 (31), 54–55. doi:10.3969/j.issn.1007-614x.2020.31.026
Wang, Q., Gao, S., Luo, Y., and Kang, Q. Y. (2017b). Compound anisodine affects the proliferation and calcium overload of hypoxia-induced rat retinal progenitor cells and brain neural stem cells via the p-ERK1/2/HIF-1α/VEGF pathway. Exp. Ther. Med. 14 (1), 600–608. doi:10.3892/etm.2017.4528
Wang, S. B., Yang, X. Y., and Du, G. H. (2018). “Anisodine,” in Natural small molecule drugs from plants. Editor G. H. Du (Singapore: Springer Singapore), 175–180.
Wang, Y., Jing, J., Meng, X., Pan, Y., Wang, Y., Zhao, X., et al. (2019). The Third China National Stroke Registry (CNSR-III) for patients with acute ischaemic stroke or transient ischaemic attack: design, rationale and baseline patient characteristics. Stroke Vasc. Neurology 4 (3), 158–164. doi:10.1136/svn-2019-000242
Wang, Y., Li, B., Tan, Y., and Yang, D. (2021). Meta-analysis of efficacy and safety of anisodine hydrobromide in the treatment of cerebral infarction. World Latest Med. Inf. 21 (71), 32–35. doi:10.3969/j.issn.1671-3141.2021.71.011
Wang, Z., Li, J., Wang, C., Yao, X., Zhao, X., Wang, Y., et al. (2013). Gender differences in 1-year clinical characteristics and outcomes after stroke: results from the China National Stroke Registry. PLoS One 8 (2), e56459. doi:10.1371/journal.pone.0056459
Wu, B., Liu, M., Liu, H., Li, W., Tan, S., Zhang, S., et al. (2007). Meta-analysis of traditional Chinese patent medicine for ischemic stroke. Stroke 38 (6), 1973–1979. doi:10.1161/strokeaha.106.473165
Wu, X. J., Gao, F., Liu, X., and Zhao, Q. (2016). Observation on therapeutic efficacy of rt-PA intravenous thrombolysis combined with compound anisodine injection on central retinal artery occlusion. Exp. Ther. Med. 12 (4), 2617–2621. doi:10.3892/etm.2016.3681
Xu, X., Pan, Y., Xie, X., Tang, G., and Peng, C. (2020). Effects of anisodine hydrobromide on hemorheology, microcirculation and platelet aggregation. Chin. Tradit. Pat. Med. 42 (9), 2438–2445. doi:10.3969/j.issn.1001-1528.2020.09.036
Yan, F., Ma, Q., Liu, X., Jiang, X., and Yao, Y. (2023). Clinical study of anisodine hydrobromide injection to improve cerebral vascular reserve function after acute massive cerebral infarction. J. Med. Forum 44 (8), 31–34.
Yasha, K., Philip, M. M., Charles, J. P., Peter, K., and Justin, F. F.Society of NeuroInterventional Surgery (2019). Current endovascular strategies for posterior circulation large vessel occlusion stroke: report of the Society of NeuroInterventional Surgery Standards and Guidelines Committee. J. NeuroInterventional Surg. 11 (10), 1055–1062. doi:10.1136/neurintsurg-2019-014873
Zeng, Y., Du, X., Qiu, Y., and Jiang, W. (2021). Anisodine hydrobromide alleviates hypoxia/reoxygenation (H/R)-induced brain microvascular endothelial cell injury via muscarinic acetylcholine receptor 4. FASEB J. 35 (S1), 1722. doi:10.1096/fasebj.2021.35.S1.01722
Zhang, B., Zhang, Y., Zhao, P., Zhang, X., and Li, R. (2022). CT perfusion imaging to evaluate the efficacy of adding anisodine hydrobromide in the treatment of acute cerebral infarction after thrombolysis. J. Mod. Med. Health 38 (7), 1199–1202. doi:10.3969/j.issn.1009-5519.2022.07.027
Zhang, J., Rong, S., and Meng, Y. (2021). Clinical analysis of anisodine hydrobromide injection in the treatment of acute ischemic stroke. Health Manag. 13, 109.
Zhang, J., Yang, M., Liu, M., Li, Y., and Sun, B. (2019a). Effects of compound anisodine on microvascular blood perfusion and vasomotion of ischemia arte-riole in rats. Chin. J. Microcirc. 29 (3), 1–5. doi:10.3969/j.issn.1005-1740.2019.03.001
Zhang, Y. (2022). Effect and safety analysis of anisodine hydrobromide injection in the treatment of acute ischemic stroke. Smart Healthc. 8 (8), 23–25. doi:10.19335/j.cnki.2096-1219.2022.08.008
Zhang, Y., Cao, Y., and Liu, C. (2020). “Autophagy and ischemic stroke,” in Autophagy: biology and diseases: clinical science. Editor W. Le (Singapore: Springer Singapore), 111–134.
Zhang, Y., He, M., Yu, X., He, L., Zhang, X., and Huang, Y. (2019b). Deffect of compound anisodine combined with cobamamide on treating patients with ischemic optic neuropathy and their hemodynamics and hemorheology. Acta Medica Mediterr. 35 (3), 1463–1467. doi:10.19193/0393-6384_2019_3_226
Zhao, Y., and Chen, L. (2010). Protection effect of compound anisodine in rats with retinal ischemia-reperfusion injury. Int. Eye Sci. 10 (12), 2268–2270. doi:10.3969/j.issn.1672-5123.2010.12.012
Zhou, Q. (2022). Clinical observation of anisodine hydrobromide combined with atorvastatin in the treatment of acute cerebral infarction. Chin. Sci. Technol. J. database Med. Health 22 (5), 0037–0039.
Keywords: acute ischemic stroke, anisodine hydrobromide injection, systematic review, meta-analysis, efficacy
Citation: Wang Y, Wan F, Hu P, He B, Hu Y and Liu Y (2023) Efficacy and safety of anisodine hydrobromide injection for acute ischemic stroke: a systematic review and meta-analysis. Front. Pharmacol. 14:1290755. doi: 10.3389/fphar.2023.1290755
Received: 08 September 2023; Accepted: 30 October 2023;
Published: 15 November 2023.
Edited by:
Marilena Gilca, Carol Davila University of Medicine and Pharmacy, RomaniaReviewed by:
Stefan Strilciuc, University of Medicine and Pharmacy Iuliu Hatieganu, RomaniaCopyright © 2023 Wang, Wan, Hu, He, Hu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yunlu Liu, a2FlbGE4NUBxcS5jb20=; Yushi Hu, aHV5dXNoaUBjZHN1LmVkdS5jbg==; Benxiang He, MTAwNTM5QGNkc3UuZWR1LmNu
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.