
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pharmacol., 14 November 2023
Sec. Drugs Outcomes Research and Policies
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1266034
This article is part of the Research TopicMethods and Metrics to Measure Medication AdherenceView all 6 articles
 Eduardo Gutiérrez-Abejón1,2,3,4*
Eduardo Gutiérrez-Abejón1,2,3,4* M. Aránzazu Pedrosa-Naudín3
M. Aránzazu Pedrosa-Naudín3 Diego Fernández-Lázaro5,6
Diego Fernández-Lázaro5,6 F. Javier Alvarez1,7
F. Javier Alvarez1,7Introduction: Non-adherence to antidepressants is associated with worse disease outcomes (morbidity and mortality) and correlates with higher healthcare resource utilization and costs.
Methods: A population-based registry study was conducted to assess non-adherence and to analyze the economic burden of treatment and from non-adherence to antidepressants in 2021. Non-adherence was measured by the Medication Possession Ratio and those below 80% were classified as non-adherent.
Results: In 2021, 246,718 patients (10.60% [95% CI: 10.48–10.72]) received antidepressants at a cost of €29 million. The median antidepressant cost per patient/year was €70.08€, ranging from €7.58 for amitriptyline to €396.66 for agomelatine. Out-of-pocket costs represented 6.09% of total expenditures, with a median copayment of €2.78 per patient. The 19.87% [95% CI 19.52–20.22)] of patients were non-adherent to antidepressants, costing €3.9 million (13.30% of total antidepressant costs). Non-adherence rates exceeded 20% for the tricyclic antidepressants, fluoxetine (23.53%), fluvoxamine (22.42%), and vortioxetine (20.58%). Venlafaxine (14.64%) and citalopram (14.88%) had the lowest non-adherence rates, of less than 15%. The median cost of non-adherent medications per patient/year was €18.96 and ranged from €2.50 (amitriptyline) to €133.42 (agomelatine).
Conclusion: Reducing non-adherence to antidepressants is critical to improving clinical and economic outcomes. The implementation of interventions and standardized measures, including early detection indicators, is urgently needed. Antidepressants differ with regard to non-adherence and their cost, and this should be considered when prescribing this medication. The Medication Possession Ratio could be used by the healthcare provider and clinician to identify non-adherent patients for monitoring, and to take necessary corrective actions.
Depression is the most common mental health disorder, affecting more than 300 million people worldwide (GBD, 2019 Mental Disorders Collaborators, 2022). Depressive disorders are associated with high economic costs to society and healthcare systems; in particular, major depressive disorder accounted for $326.2 billion in global expenditures in the United States in 2018 (Greenberg et al., 2021). In addition, pharmacy expenditures were $20.4 billion, representing 6% of direct costs (Greenberg et al., 2021), much higher lees than a decade ago. Based on European labeling, antidepressants are also used in the treatment of anxiety, insomnia, eating disorders and pain of neuropathic origin, among others.
Non-adherence is an important precipitating factor in the loss of efficacy of antidepressants. Non-adherence to antidepressants is not only associated with worse disease outcomes (morbidity and mortality), but is also strongly correlated with healthcare resource utilization and costs (Ho et al., 2016). Non-adherence to antidepressants is a major problem worldwide, estimated at up to 50% (WHO, 2003; Wong et al., 2022). In Spain, 10.6% of the population was reported to be taking antidepressants in 2021and 19.9% of the patients were non-adherent (Pedrosa-Naudín et al., 2022). Information on the costs of antidepressant non-adherence is lacking. A real-world population-based registry study was conducted to assess antidepressant non-adherence, pharmacy costs of antidepressants, and pharmacy costs of non-adherent patients to antidepressants in the free public national health system in Castille and Leon (Spain) in 2021. This study aimed to describe i) antidepressant non-adherence, ii) medication costs of antidepressant use, and iii) medication costs of those non-adherents to antidepressants. This is analyzed for each of the 26 antidepressants available in Spain.
We conducted a population-based economic evaluation of antidepressant use in Castile and Leon, Spain, in 2021, covering a population of 2,327,420. We followed the CHEERS (Husereau et al., 2022) reporting guideline.
The focus was on patients who used at least one antidepressant in 2021. Data were collected from CONCYLIA (http://www.saludcastillayleon.es/portalmedicamento/es/indicadores-informes/concylia, accessed on 5 May 2023), the pharmacy information system for Castile and Leon (Spain). CONCYLIA integrates information on medicines dispensed in pharmacies and reimbursed by the Spanish National Health System. It also includes prescription records and is linked to the electronic prescription system in Castile and Leon (Spain). The data are anonymized using the patient identification code, which also allows the retrieval of sociodemographic and health data, including diagnoses. However, data on hospital care and private prescriptions are not available in CONCYLIA. The database is considered to be highly valid and reliable due to the integration of prescription and dispensing data (Pedrosa-Naudín et al., 2022). In this study, all dispensations were considered equivalent to consumption, following the approach used previously (Gutiérrez-Abejón et al., 2017; 2020; Pedrosa-Naudín et al., 2022). In the region of Castile and Leon (Spain), the typical duration of antidepressant treatment is usually between 6 months and a year (Gutiérrez-Abejón et al., 2020).
Access to the information was granted by the Castile and Leon Health Council Pharmacy Directorate, and the study protocol was approved by the East Valladolid Area Ethics Committee on 24 February 2022 (reference number PI 22-2622).
Non-adherence to antidepressants was determined using the medication possession ratio (MPR) (Pedrosa-Naudín et al., 2022). MPR is a method based on pharmacy records that indirectly measures medication adherence. It was calculated for each patient by dividing the days of supply during a specific monitoring period (1 year) by the number of days from the first dispensing to the end of the monitoring period (Andrade et al., 2006). MPR was determined based on prescribing and dispensing records for each patient and for each type of antidepressant used. MPR is expressed as a percentage and considered a continuous variable. Patients with an MPR below 80% were categorized as non-adherent, which is a commonly accepted cut-off point in the literature (Baumgartner et al., 2018; Liu et al., 2022).
Other variables collected in the study included sociodemographic information, such as age and gender, and health-related variables, such as diagnoses.
Diagnoses were categorized into different groups based on the International Classification of Diseases-10 (ICD-10) criteria. These groups included depression, anxiety, depression and anxiety, pain of various causes (neuropathic pain, cephalalgia, and migraine), and other psychiatric disorders. The categorization was done according to the approved indications of the relevant drugs, following the European labeling guidelines (EMA, 2022). Twenty-six antidepressants available in Spain were included in the analysis, identified using the ATC (Anatomical Therapeutic Chemical) classification system (WHO Collaborating Centre for Drug Statistics Methodology, 2020). Antidepressant dispensing was measured by the number of packages and the defined daily doses (DDDs) for each medication.
Medication expenditures were calculated using the prices listed in the official medicines formulary of the Spanish National Health System (https://www.sanidad.gob.es/profesionales/nomenclator.do, accessed on 5 May 2023). In terms of cost/DDD, the most expensive antidepressants were agomelatine (€1.25/DDD), reboxetine (€1.20/DDD), and vortioxetine (€1.10/DDD). On the other hand, the cheapest antidepressants were fluoxetine (€0.09/DDD), amitriptyline (€0.17/DDD) and imipramine (€0.21/DDD) (Table 1). All costs were reported in euros using 2021 values. The exchange rate of €1 = US$1.1326 was based on the European Central Bank rate on 31 December 2021.
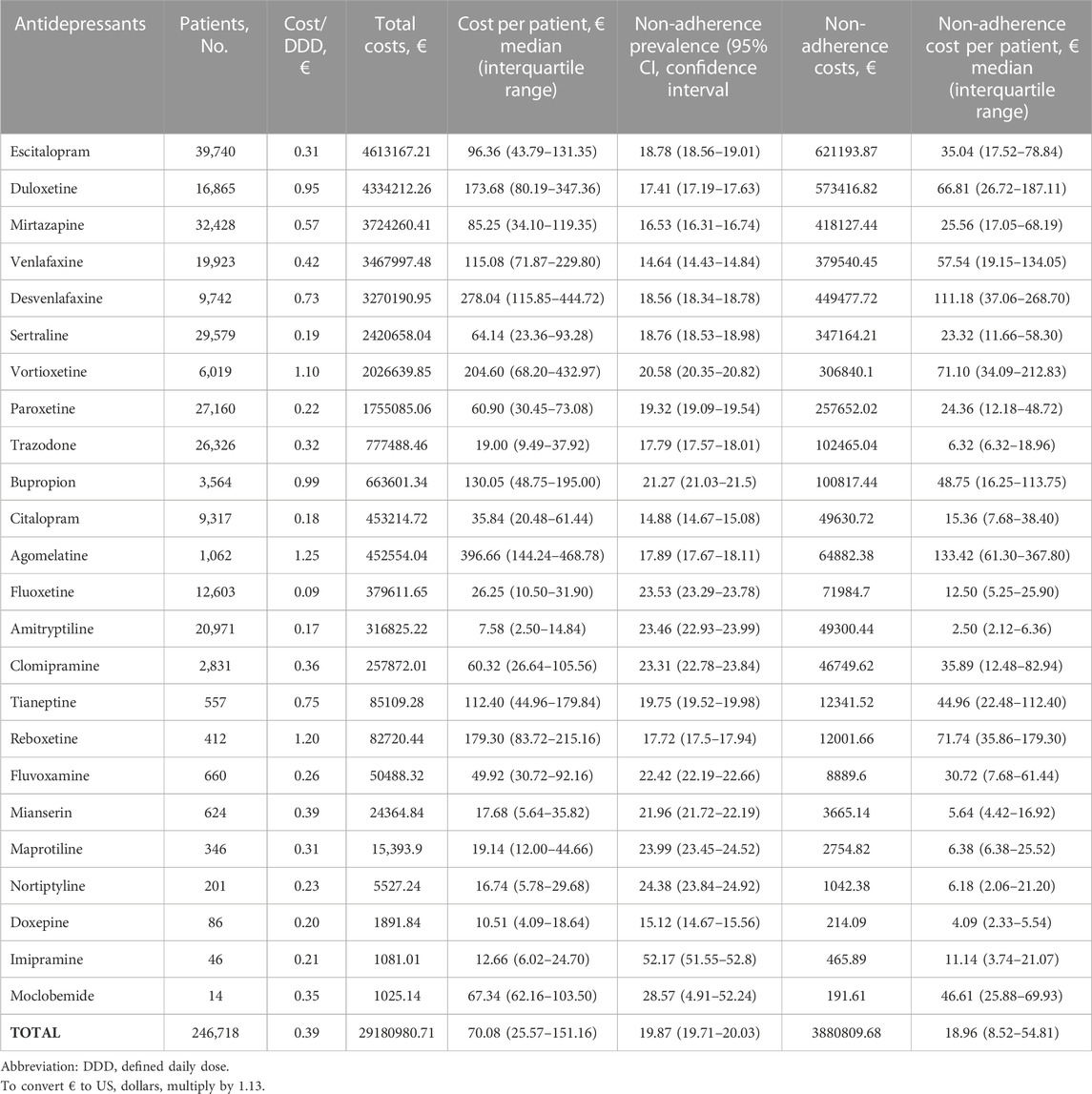
TABLE 1. Antidepressants Non-adherence and cost in Castille and Leon (Spain) in 2021. Data is presented according to the highest to the lowest cost of antidepressants.
Results are presented as percentages with 95% confidence intervals (95% CI) or medians with interquartile ranges (IQR). Differences between groups were assessed using the Mann-Whitney test and Kruskal–Wallis test for continuous variables, as appropriate. Statistical analyses were performed with SPSS version 24.0 (SPSS Inc, Chicago, IL). A significance level of p ≤ 0.05 was used to determine statistical significance.
In 2021, 246,718 patients (10.60% [95% CI: 10.48–10.72]) received antidepressants at a cost of €29 million. The five most prescribed drugs were escitalopram, mirtazapine, sertraline, paroxetine, and trazodone, accounting for 63.49% of prescriptions. The combined cost of escitalopram, duloxetine, mirtazapine, venlafaxine, and desvenlafaxine accounted for 66.51% of expenditures. The median cost of antidepressants per patient/year was €70.08€, ranging from €7.58 for amitriptyline to €396.66 for agomelatine (Table 1). Out-of-pocket costs accounted for 6.09% (€1,775,910) of total expenditures, with a median copayment of €2.78 95% CI: (0.58–9.00) per patient. A total of 49,024 patients (19.87% [95% CI 19.52–20.22)] were non-adherent to antidepressants, costing €3.9 million (13.30% of total antidepressant costs, Table 1). Nonadherence rates exceeded 20% for tricyclic antidepressants and for fluoxetine (23.53%), fluvoxamine (22.42%), and vortioxetine (20.58%). Venlafaxine (14.64%) and citalopram (14.88%) had the lowest non-adherence rates, below 15%, and minimal impact on total costs (10.94% and 10.95%, respectively). The median cost of non-adherent medications per patient/year was €18.96 and ranged from €2.50 (amitriptyline) to €133.42 (agomelatine) (Table 1).
Male patients (€70.49), those aged 65–79 years (€76.72), and those with a mixed diagnosis of depression and anxiety (€105.10) had the highest medication costs per patient. The costs of non-adherent patients showed the same pattern (Table 2).
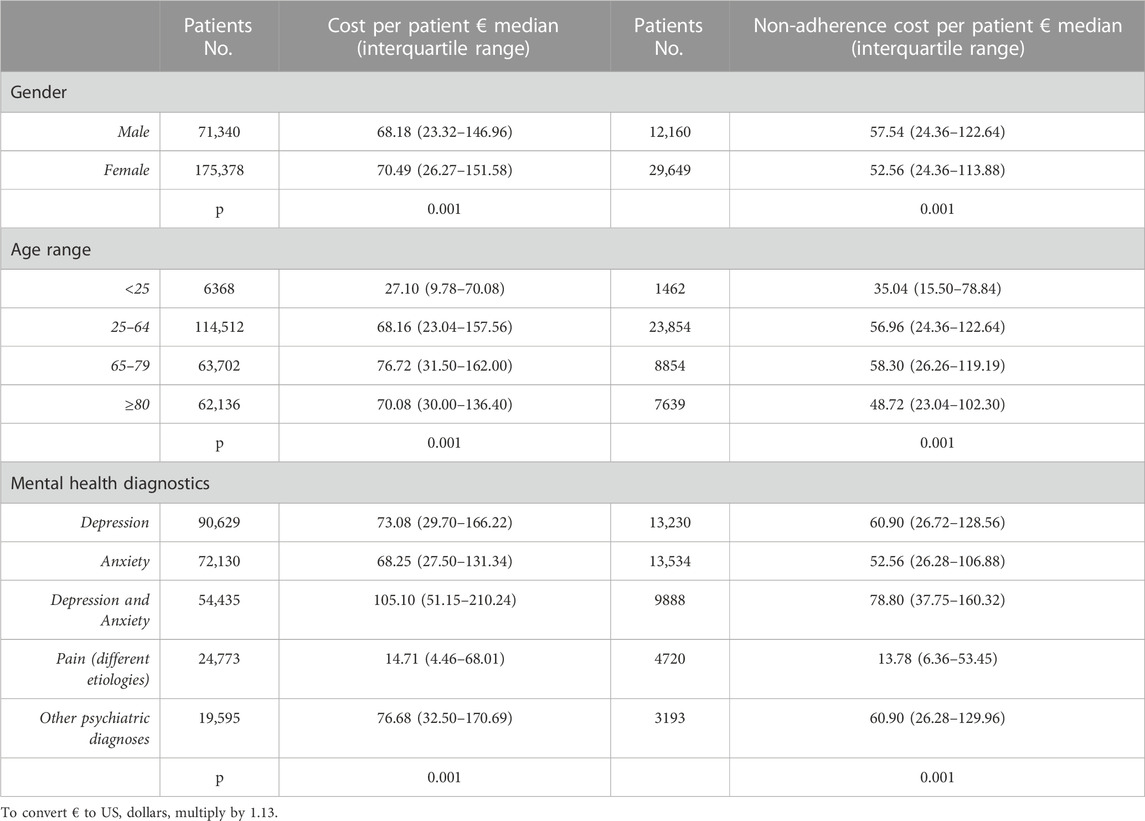
TABLE 2. Antidepressant cost per patient analyzed by gender, age range, and mental health diagnosis.
The 10.6% of the population was taking antidepressants and 19.87% of the patients were non-adherent. Urban residence, male sex, use of tricyclic antidepressants, and a diagnosis of neuropathic pain were underlying predictors of medication non-adherence, as we have previously reported (Pedrosa-Naudín et al., 2022). In the current study, we show results for each of the 26 antidepressants available in Spain.
The use of antidepressants is high and has been increasing for several years (COVID-19 Mental Disorders Collaborators, 2021). The pattern of antidepressant use and gender distribution in our study was consistent with other manuscripts (Cutler et al., 2018; COVID-19 Mental Disorders Collaborators, 2021). The most used antidepressant was escitalopram, ahead of citalopram, which has been the most used in recent years (Lalji et al., 2021). This is logical because escitalopram has been shown to be the most effective of the SSRIs (Khoo et al., 2015). However, escitalopram has been reported to be associated with higher costs and higher rates of nonadherence than citalopram. In addition, escitalopram has been surpassed in efficacy by other antidepressants such as mirtazapine, venlafaxine, and agomelatine. In this case, agomelatine will not be cost-effective (Khoo et al., 2015) because its cost/DDD is the highest of all antidepressants. As a result, the use of agomelatine has been reduced.
Antidepressant non-adherence was lower than previously reported in other countries (WHO, 2003; Kales et al., 2016; Wong et al., 2022) and in Spain (Párraga Martínez et al., 2014; Baeza-Velasco et al., 2019). Nevertheless, comparisons should be made with caution due to methodological differences, particularly in the measurement of adherence. In addition to citalopram, venlafaxine and mirtazapine were the antidepressants associated with lower rates of non-adherence, because these drugs improve situations that promote non-adherence, such as reduced cognitive and sexual function or weight gain (Lalji et al., 2021). The total cost of antidepressant was €29 million, and non-adherence to antidepressants accounted for 13.30% of the total cost, representing a significant economic burden for the Spanish national health system. To our knowledge, this is the first study in our country to measure the economic impact of medication non-adherence on drug expenditures. While most research has focused on the increase in healthcare services utilization and associated costs due to non-adherence, this study shows that the cost of discontinued antidepressant is not insignificant. The median cost of antidepressant medication was of €70.08 per patient/year, which is significantly lower than that reported in the United States (Greenberg et al., 2021), and in other European countries, as Germany (Jacob and Kostev, 2016). One factor contributing to non-adherence is out-of-pocket costs (Luiza et al., 2015; Sinnott et al., 2016; González López-Valcárcel et al., 2017), particularly for high-cost medications (Schneeweiss et al., 2007). In a study conducted in our country (González López-Valcárcel et al., 2017), a reduction in adherence of 6.8%–8.3% was observed for medications such as statins, angiotensin-converting enzyme inhibitors (ACEI), and angiotensin II receptor blockers (ARB). This decrease occurred primarily among older, retired patients and those with lower incomes. On the other hand, the researchers observed that the co-payment increase had no significant effect on lower-priced drugs such as antiplatelet agents and beta-blockers (González López-Valcárcel et al., 2017).
Conflicting results have been observed with antidepressants. Co-payments of between €0.50 and €1.50 per package have been shown to promote non-adherence more for antidepressants than for other medications (Sinnott et al., 2016). However, other studies found no differences with other medications (Goldman et al., 2004) or only in women (Ong et al., 2003). In contrast, one study found that a €1 increase in co-payment did not affect antidepressant non-adherence (Linnet et al., 2013).
In Spain, chronic medications such as antidepressants are subject to a co-payment of between 0% and 10%, up to a maximum of €4.24 per package (Spanish Ministry of Health, 2015). In our study, out-of-pocket costs accounted for 6% of total antidepressant expenditures, with a median value of €2.78/patient/year. However, a high percentage of non-adherence was observed for fluoxetine, the medicine with the lowest cost/DDD of all antidepressants. The study was not without several limitations. An indirect method based on MPR was used, considering filling as a proxy for medication taking. A cut-off of 80% in the MPR was used, but it is not a universal score (Baumgartner et al., 2018). However, MPR may overestimate adherence compared with more conservative measures such as the proportion of days covered (PDC) (Gelzer et al., 2019). In this sense, PDC provides a more accurate measure of medication adherence and has been recommended by several institutions, including the Pharmacy Quality Alliance, to measure adherence in polymedicated patients (Canfield et al., 2019). Despite significant limitations, MPR is widely used to measure adherence in chronic diseases because of its ease of calculation and low cost (Boulet et al., 2012). Furthermore, data on antidepressant use in hospital and private prescriptions are not accessible through our data source, CONCYLIA. However, due to the sample size and the fact that antidepressants covered are prescription medicines, the biases introduced by the use of dispensing data are not considered relevant (Pedrosa-Naudín et al., 2022) within the free public health system in Spain. In addition, caution should be exercised when comparing figures from other countries, especially outside the European Union, because of possible differences in the costs of antidepressant medication. This real-world study provides a comprehensive view of the population covered by the free Spanish National public health system. In conclusion, escitalopram was the most used antidepressant, while citalopram was associated with the lowest rate of non-adherence. In addition, fluoxetine was the least expensive antidepressant and, surprisingly, the one with the highest percentage of costs associated with non-adherent patients. Antidepressants differ about the non-adherence and their cost, and this should be considered when prescribing this medication.
Reducing non-adherence to antidepressants is critical to improving clinical and economic outcomes (Ho et al., 2016). Thus, there is an urgent need to implement strategies such as the integration of measures for the early detection of non-adherence. MPR could serve as a tool for healthcare providers and clinicians to identify non-adherent patients for close monitoring and intervention as needed.
Lastly, in this sense, previous research conducted by our group concluded that MPR should serve as the physician’s preferred indicator of antidepressant non-adherence (Pedrosa-Naudín et al., 2022). However, the role of the pharmacist as a key figure in patient care should not be ignored (Lallemand et al., 2023). Spain has an extensive network of more than 22,000 community pharmacies (Amador-Fernández et al., 2023), making it easier for pharmacists to build trusting relationships with their patients (Pousinho et al., 2016). As part of their pharmaceutical care, community pharmacists should provide patients with personalized strategies to achieve optimal adherence to prescribed medications (Jairoun et al., 2023). In fact, there are numerous examples in the literature of successful adherence improvement through community pharmacy initiatives (Nogueira et al., 2020; Jairoun et al., 2023; Lallemand et al., 2023; Sáez-Benito et al., 2023).
The data analyzed in this study is subject to the following licenses/restrictions: Restrictions apply to the availability of these data. Data were obtained from regional health authorities (Gerencia Regional de Salud (GRS)) and may be requested from conciertofco@saludcastillayleon.es. Requests to access these datasets should be directed to conciertofco@saludcastillayleon.es.
The studies involving humans were approved by CEIm Area de Salud Valladolid Este, PI-22-2622. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participant’s legal guardians/next of kin in accordance with the national legislation and institutional requirements.
EG-A: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Methodology, Project administration, Resources, Software, Writing–original draft, Writing–review and editing. MP-N: Conceptualization, Formal Analysis, Investigation, Software, Validation, Writing–original draft, Writing–review and editing. DF-L: Formal Analysis, Investigation, Methodology, Writing–original draft, Writing–review and editing. FJ: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by Gerencia Regional de Salud de Castilla y León, Spain, grant number GRS 2589/B/22.
The authors thank the Pharmacy Directorate (Castilla y León Health Council) for access to Concylia database. The funders have no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the funder and collaborating institutions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Amador-Fernández, N., Gastelurrutia, M. Á., and García-Cárdenas, V. (2023). Development of self-care in Spanish community pharmacies. Explor Res. Clin. Soc. Pharm. 12, 100337. doi:10.1016/j.rcsop.2023.100337
Andrade, S. E., Kahler, K. H., Frech, F., and Chan, K. A. (2006). Methods for evaluation of medication adherence and persistence using automated databases. Pharmacoepidemiol Drug Saf. 15, 565–574. discussion 575-577. doi:10.1002/pds.1230
Baeza-Velasco, C., Olié, E., Béziat, S., Guillaume, S., and Courtet, P. (2019). Determinants of suboptimal medication adherence in patients with a major depressive episode. Depress Anxiety 36, 244–251. doi:10.1002/da.22852
Baumgartner, P. C., Haynes, R. B., Hersberger, K. E., and Arnet, I. (2018). A systematic review of medication adherence thresholds dependent of clinical outcomes. Front. Pharmacol. 9, 1290. doi:10.3389/fphar.2018.01290
Boulet, L.-P., Vervloet, D., Magar, Y., and Foster, J. M. (2012). Adherence: the goal to control asthma. Clin. Chest Med. 33, 405–417. doi:10.1016/j.ccm.2012.06.002
Canfield, S. L., Zuckerman, A., Anguiano, R. H., Jolly, J. A., DeClercq, J., Wascher, M., et al. (2019). Navigating the wild west of medication adherence reporting in specialty pharmacy. J. Manag. Care Spec. Pharm. 25, 1073–1077. doi:10.18553/jmcp.2019.25.10.1073
COVID-19 Mental Disorders Collaborators (2021). Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 398, 1700–1712. doi:10.1016/S0140-6736(21)02143-7
Cutler, R. L., Fernandez-Llimos, F., Frommer, M., Benrimoj, C., and Garcia-Cardenas, V. (2018). Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open 8, e016982. doi:10.1136/bmjopen-2017-016982
EMA (2022). European medicines agency. Available at: https://www.ema.europa.eu/en (Accessed May 20, 2022).
GBD 2019 Mental Disorders Collaborators (2022). Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 9, 137–150. doi:10.1016/S2215-0366(21)00395-3
Gelzer, A. D., Gao, W., Keleti, D., Donia, T., Megargell, L., Kreitman, J., et al. (2019). Multifaceted interventions improve medication adherence and reduce acute hospitalization rates in medicaid patients prescribed asthma controllers. J. Asthma 56, 190–199. doi:10.1080/02770903.2018.1439954
Goldman, D. P., Joyce, G. F., Escarce, J. J., Pace, J. E., Solomon, M. D., Laouri, M., et al. (2004). Pharmacy benefits and the use of drugs by the chronically ill. JAMA 291, 2344–2350. doi:10.1001/jama.291.19.2344
González López-Valcárcel, B., Librero, J., García-Sempere, A., Peña, L. M., Bauer, S., Puig-Junoy, J., et al. (2017). Effect of cost sharing on adherence to evidence-based medications in patients with acute coronary syndrome. Heart 103, 1082–1088. doi:10.1136/heartjnl-2016-310610
Greenberg, P. E., Fournier, A.-A., Sisitsky, T., Simes, M., Berman, R., Koenigsberg, S. H., et al. (2021). The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics 39, 653–665. doi:10.1007/s40273-021-01019-4
Gutiérrez-Abejón, E., Herrera-Gómez, F., Criado-Espegel, P., and Alvarez, F. J. (2017). Use of driving-impairing medicines by a Spanish population: a population-based registry study. BMJ Open 7, e017618. doi:10.1136/bmjopen-2017-017618
Gutiérrez-Abejón, E., Herrera-Gómez, F., Criado-Espegel, P., and Álvarez, F. J. (2020). Trends in antidepressants use in Spain between 2015 and 2018: analyses from a population-based registry study with reference to driving. Pharm. (Basel) 13, E61. doi:10.3390/ph13040061
Ho, S. C., Chong, H. Y., Chaiyakunapruk, N., Tangiisuran, B., and Jacob, S. A. (2016). Clinical and economic impact of non-adherence to antidepressants in major depressive disorder: a systematic review. J. Affect Disord. 193, 1–10. doi:10.1016/j.jad.2015.12.029
Husereau, D., Drummond, M., Augustovski, F., de Bekker-Grob, E., Briggs, A. H., Carswell, C., et al. (2022). Consolidated health economic evaluation reporting standards (CHEERS) 2022 explanation and elaboration: a report of the ispor CHEERS II good practices task force. Value Health 25, 10–31. doi:10.1016/j.jval.2021.10.008
Jacob, L., and Kostev, K. (2016). Impact of comorbidities on the cost of depression drug therapy in general practices in Germany. J. Psychiatr. Res. 83, 130–136. doi:10.1016/j.jpsychires.2016.08.017
Jairoun, A. A., Al-Himyari, S. S., Shahwan, M., Al Ani, M., Habeb, M., Jairoun, M., et al. (2023). Community pharmacists’ perspectives on cardiovascular disease pharmaceutical care in the United Arab Emirates: a questionnaire survey-based analysis. Front. Pharmacol. 14, 1237717. doi:10.3389/fphar.2023.1237717
Kales, H. C., Kavanagh, J., Chiang, C., Kim, H. M., Bishop, T., Valenstein, M., et al. (2016). Predictors of antidepressant nonadherence among older veterans with depression. Psychiatr. Serv. 67, 728–734. doi:10.1176/appi.ps.201500120
Khoo, A. L., Zhou, H. J., Teng, M., Lin, L., Zhao, Y. J., Soh, L. B., et al. (2015). Network meta-analysis and cost-effectiveness analysis of new generation antidepressants. CNS Drugs 29, 695–712. doi:10.1007/s40263-015-0267-6
Lalji, H. M., McGrogan, A., and Bailey, S. J. (2021). An analysis of antidepressant prescribing trends in England 2015-2019. J. Affect Disord. Rep. 6, 100205. doi:10.1016/j.jadr.2021.100205
Lallemand, A., Verrue, C., Santi, A., Delhaye, N., Willaert, M., Attipoe, A., et al. (2023). Evaluation of community pharmacist follow-up supported by the use of healthcare technology for type 2 diabetes patients. Explor Res. Clin. Soc. Pharm. 12, 100330. doi:10.1016/j.rcsop.2023.100330
Linnet, K., Halldórsson, M., Thengilsdóttir, G., Einarsson, Ó. B., Jónsson, K., and Almarsdóttir, A. B. (2013). Primary non-adherence to prescribed medication in general practice: lack of influence of moderate increases in patient copayment. Fam. Pract. 30, 69–75. doi:10.1093/fampra/cms049
Liu, Y., Söderberg, J., and Chao, J. (2022). Adherence to and persistence with adalimumab therapy among Swedish patients with crohn’s disease. Pharm. (Basel) 10, 87. doi:10.3390/pharmacy10040087
Luiza, V. L., Chaves, L. A., Silva, R. M., Emmerick, I. C. M., Chaves, G. C., Fonseca de Araújo, S. C., et al. (2015). Pharmaceutical policies: effects of cap and co-payment on rational use of medicines. Cochrane Database Syst. Rev. 2015, CD007017. doi:10.1002/14651858.CD007017.pub2
Nogueira, M., Otuyama, L. J., Rocha, P. A., and Pinto, V. B. (2020). Pharmaceutical care-based interventions in type 2 diabetes mellitus: a systematic review and meta-analysis of randomized clinical trials. Einstein (Sao Paulo) 18, eRW4686. doi:10.31744/einstein_journal/2020RW4686
Ong, M., Catalano, R., and Hartig, T. (2003). A time-series analysis of the effect of increased copayments on the prescription of antidepressants, anxiolytics, and sedatives in Sweden from 1990 to 1999. Clin. Ther. 25, 1262–1275. doi:10.1016/s0149-2918(03)80082-6
Párraga Martínez, I., López-Torres Hidalgo, J., del Campo del Campo, J. M., Villena Ferrer, A., Morena Rayo, S., Escobar Rabadán, F., et al. (2014). Seguimiento de la adherencia al tratamiento antidepresivo en pacientes que inician su consumo. Aten. Primaria 46, 357–366. doi:10.1016/j.aprim.2013.11.003
Pedrosa-Naudín, M. A., Gutiérrez-Abejón, E., Herrera-Gómez, F., Fernández-Lázaro, D., and Álvarez, F. J. (2022). Non-adherence to antidepressant treatment and related factors in a region of Spain: a population-based registry study. Pharmaceutics 14, 2696. doi:10.3390/pharmaceutics14122696
Pousinho, S., Morgado, M., Falcão, A., and Alves, G. (2016). Pharmacist interventions in the management of type 2 diabetes mellitus: a systematic review of randomized controlled trials. J. Manag. Care Spec. Pharm. 22, 493–515. doi:10.18553/jmcp.2016.22.5.493
Sáez-Benito, A., Berenguer, N., Magallón, R., Oliván, B., Ezquerra, L., and Sáez-Benito, L. (2023). Clinical, economic, and humanistic impact of a multidisciplinary medication review with follow-up for anticoagulated patients treated with vitamin K antagonists in primary care: a cluster randomised controlled trial. Res. Soc. Adm. Pharm. 19, 1570–1578. doi:10.1016/j.sapharm.2023.08.007
Schneeweiss, S., Patrick, A. R., Maclure, M., Dormuth, C. R., and Glynn, R. J. (2007). Adherence to statin therapy under drug cost sharing in patients with and without acute myocardial infarction: a population-based natural experiment. Circulation 115, 2128–2135. doi:10.1161/CIRCULATIONAHA.106.665992
Sinnott, S.-J., Normand, C., Byrne, S., Woods, N., and Whelton, H. (2016). Copayments for prescription medicines on a public health insurance scheme in Ireland. Pharmacoepidemiol Drug Saf. 25, 695–704. doi:10.1002/pds.3917
Spanish Ministry of Health (2015). Royal legislative decree 1/2015, of july 24, 2015, approving the revised text of the law on guarantees and rational use of medicines and medical devices. Available at: https://www.boe.es/diario_boe/txt.php?id=BOE-A-2015-8343 (Accessed May 20, 2022).
WHO (2003). Adherence to long-term therapies: evidence for action/[edited by Eduardo Sabaté]. World Health Organization. Available at: https://apps.who.int/iris/handle/10665/42682 (Accessed May 20, 2022).
WHO Collaborating Centre for Drug Statistics Methodology (2020). ATC/DDD index. Available at: https://www.whocc.no/atc_ddd_index/(Accessed August 12, 2020).
Keywords: antidepressant, medication adherence, drug utilization, depression, anxiety, mental disorders, psychotropic drugs
Citation: Gutiérrez-Abejón E, Pedrosa-Naudín MA, Fernández-Lázaro D and Alvarez FJ (2023) Medication economic burden of antidepressant non-adherence in Spain. Front. Pharmacol. 14:1266034. doi: 10.3389/fphar.2023.1266034
Received: 24 July 2023; Accepted: 30 October 2023;
Published: 14 November 2023.
Edited by:
André Coelho, Instituto Politécnico de Lisboa, PortugalReviewed by:
Ângelo Jesus, Polytechnic Institute of porto, PortugalCopyright © 2023 Gutiérrez-Abejón, Pedrosa-Naudín, Fernández-Lázaro and Alvarez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo Gutiérrez-Abejón, ZWd1dGllcnJlemFAc2FsdWRjYXN0aWxsYXlsZW9uLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.