 Su Bin Park
Su Bin Park Jee-Hyun Yoon
Jee-Hyun Yoon Eun Hye Kim
Eun Hye Kim Hayun Jin
Hayun Jin Seong Woo Yoon
Seong Woo Yoon- 1Department of Korean Internal Medicine, Kyung Hee University Hospital at Gangdong, Seoul, Republic of Korea
- 2Department of Clinical Korean Medicine, Graduate School, Kyung Hee University, Seoul, Republic of Korea
Background: The purpose of this systematic review and meta-analysis was to evaluate the efficacy and safety of traditional herbal medicine (THM) for improving anorexia in patients with cancer.
Methods: We searched for randomized controlled trials (RCTs) that evaluated orally administered THM for cancer-related anorexia using 10 databases from the inception to 1 August 2021. The primary outcome was an improvement in anorexia, measured with the total effective rate (TER) or visual analog scale (VAS). The secondary outcomes were the changes in body weight, the Karnofsky performance scale, acylated ghrelin, and adverse events. We used the Cochrane risk of bias assessment tool and the Grading of Recommendations Assessment, Development, and Evaluation method to assess the quality of the studies and the quality of the evidence.
Results: A total of 26 RCTs were included, of which 23 were subjected to quantitative analysis. THM showed a significant improvement in anorexia measured with the TER [risk ratio (RR) 1.12, 95% confidence intervals (CI) 1.04–1.20] than appetite stimulants with moderate quality evidence and in the Karnofsky performance scale (RR 1.38, 95% CI 1.12–1.70) with low quality evidence but not in body weight gain (RR 0.98, 95% CI 0.80–1.20). THM showed a significant improvement in anorexia measured with the TER (RR 1.74, 95% CI 1.23–2.48) compared with usual care with low-quality evidence but did not significantly improve the VAS score (mean difference 0.72, 95% CI 0.00–1.43) or the level of acylated ghrelin (mean difference 0.94, 95% CI 1.08–2.97). There were no serious adverse events.
Conclusion: This review suggests that THM may be considered a safe alternative therapeutic option for improving anorexia in patients with cancer. Nonetheless, more rigorous RCTs are needed due to methodological limitations.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero, identifier CRD42021276508.
1 Introduction
Anorexia, a common cancer-related symptom, is defined as a loss of appetite leading to a reduced food intake (Laviano et al., 2017). It occurs in 50% of patients with new cancer diagnoses and 70% of patients with advanced cancer (Yu, 2015; Zhang et al., 2018) and is often accompanied by cachexia, which causes weight loss, tissue wasting, poor quality of life, low response to cancer treatment, and poor survival rates (Trajkovic-Vidakovic et al., 2012; Tarricone et al., 2016; Laviano et al., 2017).
The multifactorial etiology of anorexia in patients with cancer is not fully understood, but systematic inflammation and abnormal neurohormonal responses due to tumor-induced changes in host metabolism are likely to play a major role. Additionally, cancer-related symptoms such as pain, depression, taste disorders, and anti-cancer therapies can contribute to anorexia in these patients (Wiffen et al., 2014; Ezeoke and Morley, 2015; Mattox, 2017). Pharmacological interventions such as progesterone analogs and corticosteroids are recommended for patients with cancer-related anorexia (Roeland et al., 2020). Megestrol acetate, one of the progesterone analogs, improves appetite and increases body weight. However, it can cause thromboembolic events, edema, dyspnea, and adrenal suppression, and increase the risk of deaths especially in higher doses (Garcia et al., 2013). Medroxyprogesterone acetate has shown similar side effects (Roeland et al., 2020). Corticosteroids also improve appetite and quality of life, but they should only be used for a short period of time due to the toxicities such as gastrointestinal bleeding and proximal myopathy and decreased efficacy during long-term use (Miller et al., 2014; Roeland et al., 2020).
Complementary and alternative medicine (CAM) is commonly used in patients with cancer. From 25% to 80% of patients in western countries have used some form of CAM, and 32.2% of them used herbal medicine (Judson et al., 2017; Alsharif F, 2021). Traditional herbal medicine (THM) in East Asian countries is one of the important components of CAM, which includes traditional Korean medicine, traditional Chinese medicine, and traditional Japanese medicine (Kampo). It has been widely used to enhance the efficacy and manage the side effects of standard cancer treatment and to improve cancer-related symptoms (McQuade et al., 2012; Chung et al., 2016; Yoon et al., 2021). A recent study suggested that THM could be used to enhance the effect of immunotherapy and reduce immune-related adverse events by having an impact on both immunological stimulation and immunological suppression (Zhang and Xiao, 2021).
In East Asian countries, 44.6%–83% of patients with cancer had used THM (Iwase et al., 2012; McQuade et al., 2012). 37.8%–64.3% of physicians prescribed THM to manage cancer-related symptoms, of which 16.9%–36% were prescribed for anorexia and weight loss (Iwase et al., 2012; McQuade et al., 2012; Yoon et al., 2021). Other CAM interventions such as auricular acupuncture, acupuncture, and moxibustion are feasible to improve appetite and maintain weight in patients with cancer, but the evidence is insufficient to make a definitive conclusion (Sun et al., 2020; Liu et al., 2021). Preclinical studies have shown that THM ameliorates cancer-related anorexia and cachexia through anti-inflammation, regulation of the neuroendocrine pathway, and modulation of the ubiquitin-proteasome system or protein synthesis (Park et al., 2019). A systematic review and meta-analysis on cancer cachexia reported that THM and acupuncture improve appetite, cachexia-related symptoms, and quality of life in patients with cancer cachexia while also being safe (Xu et al., 2021). Earlier systematic reviews and meta-analyses have demonstrated the therapeutic potential of THM for improving anorexia in palliative cancer care (Chung et al., 2016; Lee et al., 2017; Chen et al., 2021). However, there are shortcomings. Chung et al. discussed overall cancer and cancer treatment-related symptoms rather than focusing on anorexia and included just two randomized controlled trials (RCTs) (Chung et al., 2016). Also reviewed overall chemotherapy-induced gastrointestinal toxicity and only included colorectal cancer patients (Chen et al., 2021). Lee et al. systematically reviewed RCTs published between 2000 and 2015 focused on cancer-related anorexia, but a meta-analysis was not conducted (Lee et al., 2017). More robust clinical evidence of THM focusing on cancer-related anorexia is needed. Therefore, this systematic review and meta-analysis of randomized controlled trials aimed to evaluate the efficacy and safety of THM for anorexia in patients with cancer.
2 Materials and methods
2.1 Search strategy
Ten electronic databases including PubMed, Cochrane Library, EMBASE, China National Knowledge Infrastructure (CNKI), Japanese databases (CiNii and JSOM), and Korean databases (KMBASE, KISS, NDSL, and OASIS) from their inception date to 1 August 2021 were searched independently by two investigators (SBP and EHK) without any restriction on publication language, region, or date. The search keywords included cancer, neoplasm, anorexia, cachexia, traditional Korean medicine, traditional Chinese medicine, herbal medicine, and Kampo medicine. The search terms were adjusted for the different databases using a highly sensitive search strategy created by the Cochrane Collaboration. The details of the search strategies are provided in Supplementary Material S1.
The systematic review and meta-analysis were conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis checklist (Page et al., 2021). The protocol for this study had been registered with the International Prospective Register of Systematic Review (PROSPERO) with the registration number CRD42021276508. Since all materials used in this research are published studies, ethical approval was not required.
2.2 Study selection
Two investigators independently assessed the eligibility of citations based on the title and abstract. Relevant studies were obtained as full text and screened against the following inclusion criteria: (1) RCTs (parallel or crossover studies); (2) studies involving adult patients (age ≥18 years); (3) studies of patients with cancer who have anorexia, cachexia, or both; (4) studies that used oral administration of THM as an interventional group; and (5) studies that used conventional treatment, appetite stimulants, usual care or routine care, a placebo, or no treatment as a control group. Studies were excluded if they met any of the following criteria: (1) studies on THM administered intravenously or externally; (2) studies that were irrelevant to anorexia; and (3) studies that involved other interventions such as acupuncture and moxibustion. Disagreements were resolved through discussion between the reviewers or arbitrated by a third investigator (SWY) if necessary.
2.3 Outcome measures
The primary outcome was to assess the improvement in clinical symptoms of anorexia after the intervention, as measured by changes in food intake or anorexia score using tools such as the total effective rate (TER) or visual analog scale (VAS). The TER is calculated as the percentage of participants who were cured, markedly effective, or improved out of the total number enrolled. The secondary outcomes included the change in body weight, the quality of life measured using the Karnofsky performance scale, the plasma level of acylated ghrelin, and any adverse events that occurred during the treatment period.
2.4 Data extraction
Two investigators independently assessed the literature and extracted data using a standardized form. The following data were recorded: name of the first author, publication year, sample size, patient characteristics, cancer type, cancer stage, intervention, comparison, outcomes, and adverse events. Disagreements were resolved through discussion or by consulting a third investigator. If any data were missing, the corresponding author of that respective study was contacted if contact information was available.
2.5 Quality assessment
The Cochrane risk of bias tool from the Cochrane handbook version 5.2 was used to evaluate the methodological quality of the included RCTs across seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome, selective reporting, and other bias (Higgins et al., 2017). Each domain was assessed as having a low (“L”), uncertain (“U”), or high (“H”) risk of bias. If baseline characteristics were different, other bias was assessed as high risk. Two investigators independently conducted the risk of bias assessment, and disagreements were resolved by consulting a third investigator.
2.6 Statistical analysis
Statistical analyses were performed by the RevMan software (Version 5.4, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). The mean difference (MD) with 95% confidence intervals (CI) was used for continuous outcomes and the risk ratios (RR) with 95% CI for dichotomous outcomes (Higgins et al., 2017). If less than five studies were included in the comparison and the outcome measurements were consistent across all of the studies, a fixed-effects model was used; otherwise, a random-effects model was used (Tufanaru et al., 2015). The Cochrane chi-square test, with a significance threshold set at 0.10, and the I2 statistic were used to measure the heterogeneity between studies. A value of I2 > 50% suggests significant heterogeneity. A funnel plot was used to examine any potential publication bias if there were more than 10 trials in a single outcome.
The quality of the evidence for the results was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system. Based on the risk of bias, inconsistency, indirectness, impression, and publication bias, each outcome was classified as “high,” “moderate,” “low,” or “very low” quality (Schünemann et al., 2013).
3 Results
3.1 Selection
The search of electronic databases identified 812 studies, of which 58 duplicates were removed. After screening titles and abstracts, 591 studies were excluded, and one study was excluded because the full text was unavailable. The remaining 162 full-text articles were assessed for eligibility, and 136 studies were excluded for the following reasons: not RCTs (n = 50); different interventions (n = 45); not related to anorexia (n = 37); protocol studies (n = 3); and duplicated publication (n = 1). Finally, a total of 26 studies were included in the systematic review (Deng, 1997; Zhang, 2000; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Cheon et al., 2017; Ohnishi et al., 2017; Wang et al., 2018; Hamai et al., 2019; Yoshiya et al., 2020; Zhang and Wang, 2020; Ko M. H. et al., 2021). A meta-analysis was conducted using the data from 23 studies (Deng, 1997; Zhang, 2000; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Yu, 2015; Yi, 2016; Ohnishi et al., 2017; Wang et al., 2018; Hamai et al., 2019; Yoshiya et al., 2020; Ko S. J. et al., 2021). The detailed study selection process is shown in Figure 1.
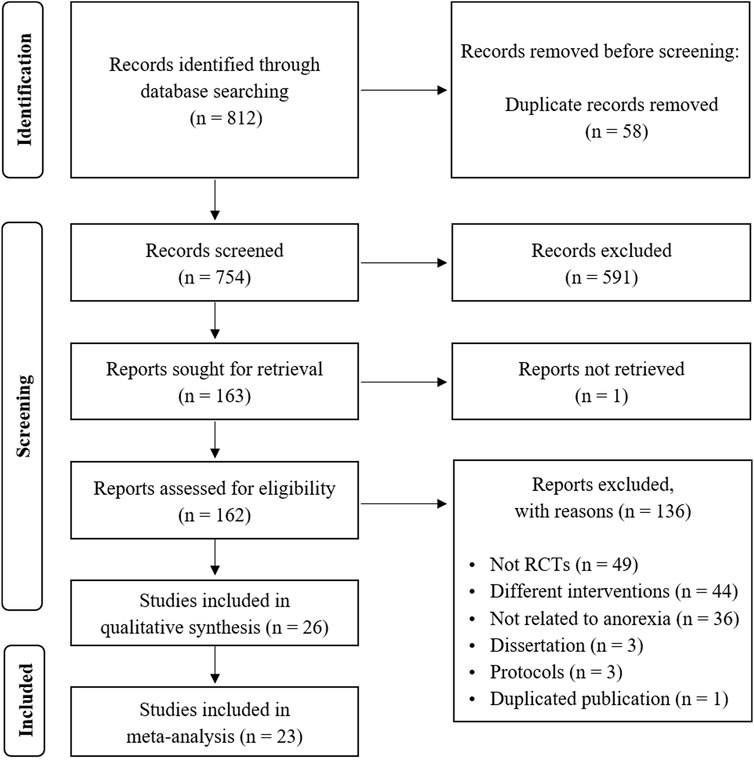
FIGURE 1. PRISMA flowchart of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
3.2 Study characteristics
The characteristics of the included studies are summarized in Table 1. Twenty-six RCTs were published from 1997 to 2021, with most studies conducted in China (n = 20) (Deng, 1997; Zhang, 2000; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Wang et al., 2018; Zhang and Wang, 2020), followed by Japan (n = 4) (Ohno et al., 2011; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020), and Korea (n = 2) (Cheon et al., 2017; Ko M. H. et al., 2021). The sample size varied from 10 to 195, with a mean patient age ranging from 43.1 to 69 years old. Seventeen RCTs included various cancer types (Zhang, 2000; Cai et al., 2003; He et al., 2007; Li and Li, 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Cheon et al., 2017; Wang et al., 2018; Zhang and Wang, 2020; Ko S. J. et al., 2021), and three studies did not specify the cancer type (Deng, 1997; Chen, 2007; Yi, 2016). Other studies included specific cancer types such as lung (He et al., 2007; Kuang et al., 2009; Yoshiya et al., 2020), esophageal (Hamai et al., 2019), gastric (Ohno et al., 2011), and cervical (Ohnishi et al., 2017) cancers. Fifteen RCTs did not mention the cancer stage (Deng, 1997; Cai et al., 2003; He et al., 2007; Li and Li, 2011; Wang et al., 2013b; Qiu and Zhang, 2013; Huang et al., 2015; Yu, 2015; Yi, 2016; Cheon et al., 2017; Ohnishi et al., 2017; Wang et al., 2018; Yoshiya et al., 2020; Zhang and Wang, 2020; Ko M. H. et al., 2021), while the remaining 10 studies enrolled patients with cancer stages III or IV (Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Zhang and Wang, 2020). Eight studies enrolled patients undergoing chemotherapy (He et al., 2007; Ohno et al., 2011; Qiu and Zhang, 2013; Huang et al., 2015; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020) or radiotherapy (Deng, 1997), and eleven studies included patients diagnosed with cancer and cachexia-anorexia syndrome (Zhang, 2000; Cai et al., 2003; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Yan et al., 2012; Wang et al., 2013a; Zhang et al., 2014; Yu, 2015; Wang et al., 2018).
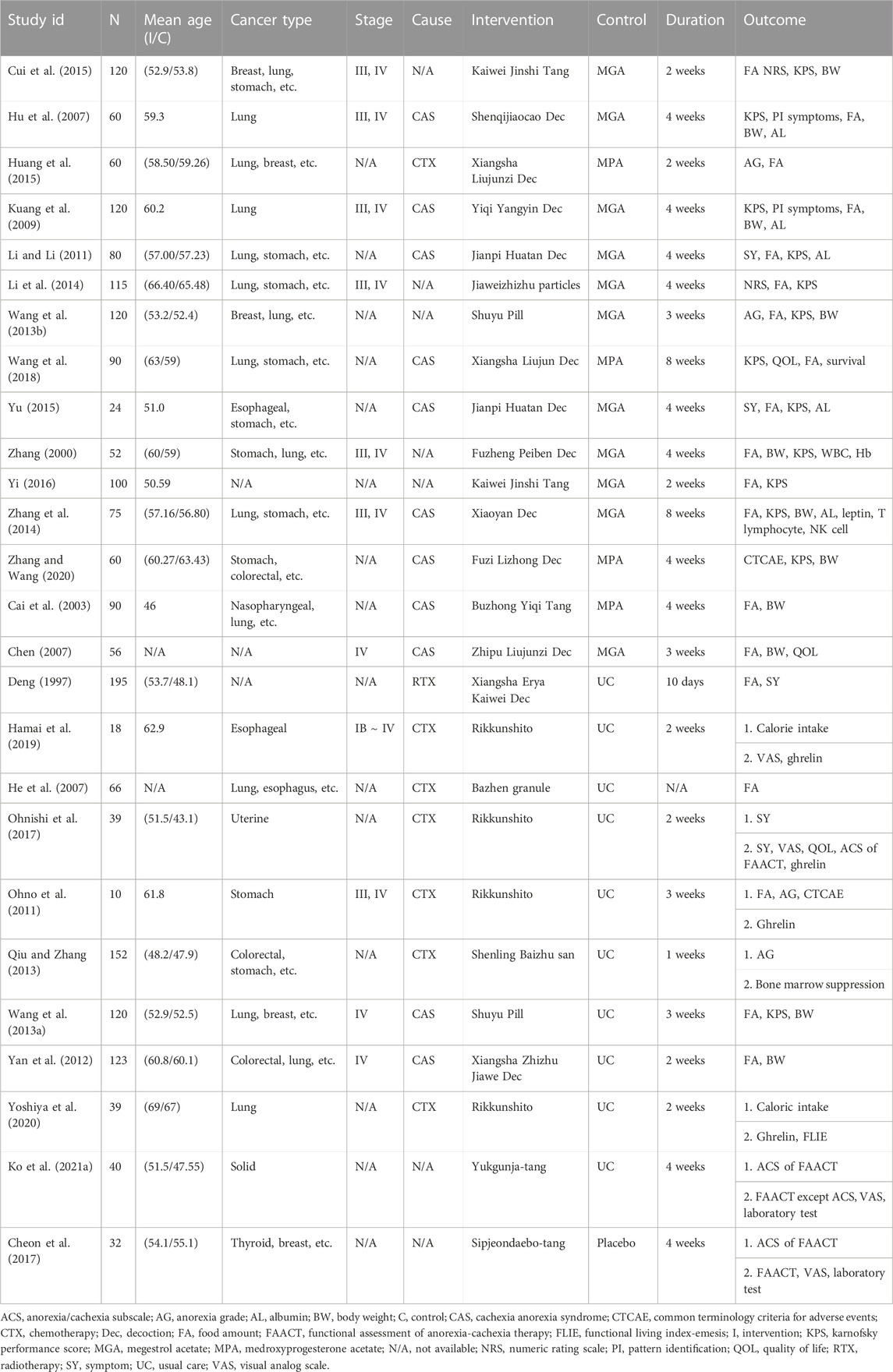
TABLE 1. Basic characteristics of included studies.
Eight studies included patients with anorexia correlated with particular pattern identification (Hu et al., 2007; Kuang et al., 2009; Qiu and Zhang, 2013; Li et al., 2014; Cui et al., 2015; Cheon et al., 2017; Wang et al., 2018; Zhang and Wang, 2020). Spleen-stomach deficiency (n = 5) (Qiu and Zhang, 2013; Li et al., 2014; Cui et al., 2015; Wang et al., 2018; Zhang and Wang, 2020), Qi-blood deficiency (n = 2) (Hu et al., 2007; Cheon et al., 2017), and Qi-yin deficiency (n = 1) (Kuang et al., 2009) were the three pattern identification categories (not shown in Table 1). For Spleen-stomach deficiency, Jiaweizhizhu particles (Li et al., 2014), Kaiwei Jinshi Tang (Cui et al., 2015), Xiangsha Liujun decoction (Wang et al., 2018), Fuzi Lizhong decoction (Zhang and Wang, 2020), and Shenling Baizhu San (Qiu and Zhang, 2013) were prescribed. Sipjeondaebo-Tang (Cheon et al., 2017) and Shenqijiaocao decoction (Hu et al., 2007) were used to treat Qi-blood deficiency, and Yiqi Yangyin decoction (Kuang et al., 2009) was used to treat Qi-yin deficiency.
Various types of herbal formulas were used in the included RCTs, with Yukgunja-tang (YGJT) (Rikkunshito in Japanese or Liujunzi decoction in Chinese) (Ohno et al., 2011; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020; Ko S. J. et al., 2021) or modified YGJT (Chen, 2007; Huang et al., 2015; Wang et al., 2018) being the most frequently used THM. Citrus aurantium L. (C. aurantium) was the most frequently used herb in the included RCTs and the details of THM prescriptions and the frequency of herbs are shown in Supplementary Materials S2–S4.
The control group was treated with appetite stimulants such as megestrol acetate (Zhang, 2000; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Wang et al., 2013b; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Yu, 2015; Yi, 2016) and medroxyprogesterone (Cai et al., 2003; Huang et al., 2015; Wang et al., 2018; Zhang and Wang, 2020), or usual care such as digestive medicine (Deng, 1997; He et al., 2007; Yan et al., 2012), antiemetics (Ohno et al., 2011; Qiu and Zhang, 2013; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020), parenteral nutrition (He et al., 2007), nutritional counseling (Ko M. H. et al., 2021), the best supportive care (Wang et al., 2013a), or a placebo (Cheon et al., 2017).
The primary outcome was reported with the TER of improvement in anorexia (Deng, 1997; Zhang, 2000; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Yu, 2015; Yi, 2016; Wang et al., 2018), the VAS score of anorexia (Cheon et al., 2017; Ohnishi et al., 2017; Hamai et al., 2019; Ko S. J. et al., 2021), or other measures (Ohno et al., 2011; Huang et al., 2015; Yoshiya et al., 2020; Zhang and Wang, 2020). The secondary outcomes were reported with the TER of improvement in the Karnofsky performance scale (Zhang, 2000; Hu et al., 2007; Kuang et al., 2009; Wang et al., 2013a; Wang et al., 2013b; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Yi, 2016), the TER of body weight gain (Zhang, 2000; Cai et al., 2003; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Yan et al., 2012; Wang et al., 2013b; Zhang et al., 2014), the level of acylated ghrelin (Ohno et al., 2011; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020), or other measures (Li and Li, 2011; Wang et al., 2013a; Cui et al., 2015; Yu, 2015; Zhang and Wang, 2020).
3.3 Risk of bias in the included studies
The risk of bias in the included studies is shown in Figure 2. Most studies properly described random sequence generation, although one study had a high selection bias (Huang et al., 2015). In terms of allocation concealment, five studies reported a detailed allocation procedure (Zhang et al., 2014; Cheon et al., 2017; Ohnishi et al., 2017; Wang et al., 2018; Ko M. H. et al., 2021), while the remaining 21 studies had an unclear bias (Deng, 1997; Zhang, 2000; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Hamai et al., 2019; Yoshiya et al., 2020; Zhang and Wang, 2020). Blinding of participants and personnel was not performed in 25 studies (Deng, 1997; Zhang, 2000; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Ohnishi et al., 2017; Wang et al., 2018; Hamai et al., 2019; Yoshiya et al., 2020; Zhang and Wang, 2020; Ko S. J. et al., 2021), but one study using a placebo was graded as having low-performance bias (Cheon et al., 2017). Blinding of outcome assessment was presented in one study (Cheon et al., 2017), whereas other studies with no such data were determined to be unclear (Deng, 1997; Zhang, 2000; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Ohnishi et al., 2017; Wang et al., 2018; Hamai et al., 2019; Yoshiya et al., 2020; Zhang and Wang, 2020; Ko M. H. et al., 2021). In terms of incomplete outcome data, two studies were unclear (Zhang, 2000; Wang et al., 2018), and the other studies were assessed as having a low risk of bias (Deng, 1997; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Cheon et al., 2017; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020; Zhang and Wang, 2020; Ko S. J. et al., 2021). Two studies were unclear in reporting bias (Li and Li, 2011; Li et al., 2014), whereas the other 24 studies were evaluated as low risk (Deng, 1997; Zhang, 2000; Cai et al., 2003; Chen, 2007; He et al., 2007; Hu et al., 2007; Kuang et al., 2009; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Cheon et al., 2017; Ohnishi et al., 2017; Wang et al., 2018; Hamai et al., 2019; Yoshiya et al., 2020; Zhang and Wang, 2020; Ko M. H. et al., 2021). Except for five studies (Cai et al., 2003; He et al., 2007; Ohno et al., 2011; Hamai et al., 2019; Yoshiya et al., 2020), the other 21 studies were considered to have a low risk of other biases because there were no differences in baseline between the intervention and control groups (Deng, 1997; Zhang, 2000; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Yan et al., 2012; Wang et al., 2013a; Wang et al., 2013b; Qiu and Zhang, 2013; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Cheon et al., 2017; Ohnishi et al., 2017; Wang et al., 2018; Zhang and Wang, 2020; Ko M. H. et al., 2021).
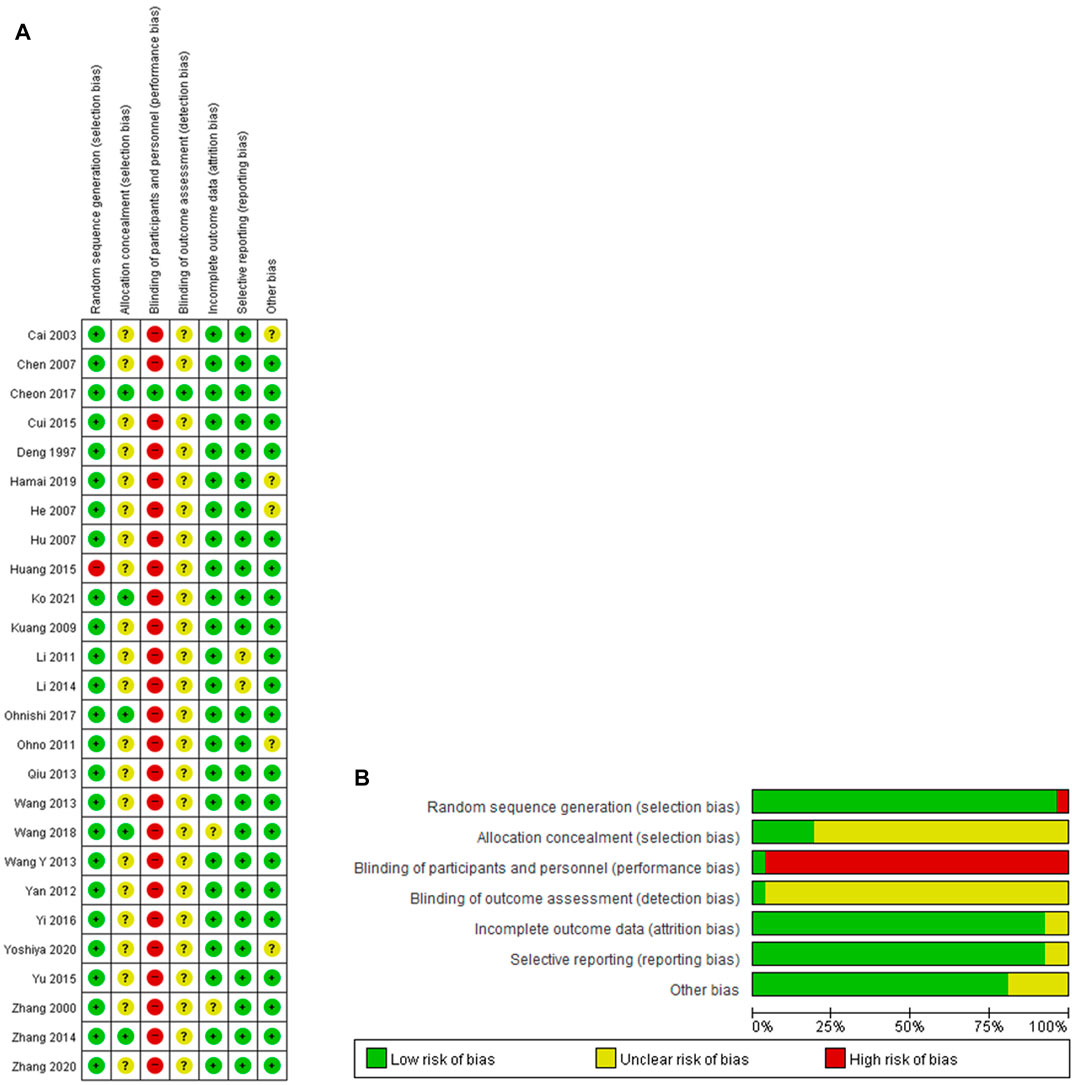
FIGURE 2. (A) Risk of bias summary. (B) Risk of bias graph. +, low risk of bias; ?, unclear of bias; -, high risk of bias.
3.4 THM versus appetite stimulants
Fifteen studies compared THM with appetite stimulants (Zhang, 2000; Cai et al., 2003; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Wang et al., 2013b; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Yi, 2016; Wang et al., 2018; Zhang and Wang, 2020), and the treatment duration of THM ranged from two to 8 weeks. Eleven studies included various cancer types (Zhang, 2000; Cai et al., 2003; Li and Li, 2011; Wang et al., 2013b; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Huang et al., 2015; Yu, 2015; Wang et al., 2018; Zhang and Wang, 2020); two included lung cancer (Hu et al., 2007; Kuang et al., 2009); and the remaining two did not indicate the cancer type (Chen, 2007; Yi, 2016). Anorexia was induced by cachexia-anorexia syndrome in nine studies (Cai et al., 2003; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Zhang et al., 2014; Yu, 2015; Wang et al., 2018; Zhang and Wang, 2020), chemotherapy in one study (Huang et al., 2015), and an unknown etiology in five studies (Zhang, 2000; Wang et al., 2013b; Li et al., 2014; Cui et al., 2015; Yi, 2016).
3.4.1 Anorexia
Thirteen RCTs with a total of 1,009 patients reported the TER of THM versus appetite stimulants for improving anorexia and were included in the meta-analysis (Figure 3) (Zhang, 2000; Cai et al., 2003; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Wang et al., 2013b; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Yu, 2015; Yi, 2016; Wang et al., 2018). Overall, THM showed a statistically significant improvement in anorexia compared to appetite stimulants (RR 1.12, 95% CI 1.04 to 1.20, p = 0.001) with a low grade of heterogeneity (I2 = 12%). In subgroup analysis according to herbal formula, Kaiwei Jinshi Tang (Cui et al., 2015; Yi, 2016) showed significant improvement in anorexia compared to appetite stimulants (RR 1.30, 95% CI 1.05 to 1.60, p = 0.02), whereas Liujunzi decoction (Chen, 2007; Wang et al., 2018) did not (RR 0.92, 95% CI 0.59 to 1.45, p = 0.73). The remaining THM (Zhang, 2000; Cai et al., 2003; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Wang et al., 2013b; Li et al., 2014; Zhang et al., 2014; Yu, 2015) showed a significant improvement in anorexia compared to appetite stimulants (RR 1.10, 95% CI 1.03 to 1.18, p = 0.008). Based on the GRADE profile, the TER of THM compared to appetite stimulants has a moderate quality of evidence due to methodological limitations, as shown in Table 2.

FIGURE 3. Forest plot of the total effective rate of THM versus AS for anorexia. THM, traditional herbal medicine; AS, appetite stimulants; LJZ, Liujunzi decoction; KWJS, kaiweijinshi tang; CI, confidence intervals.
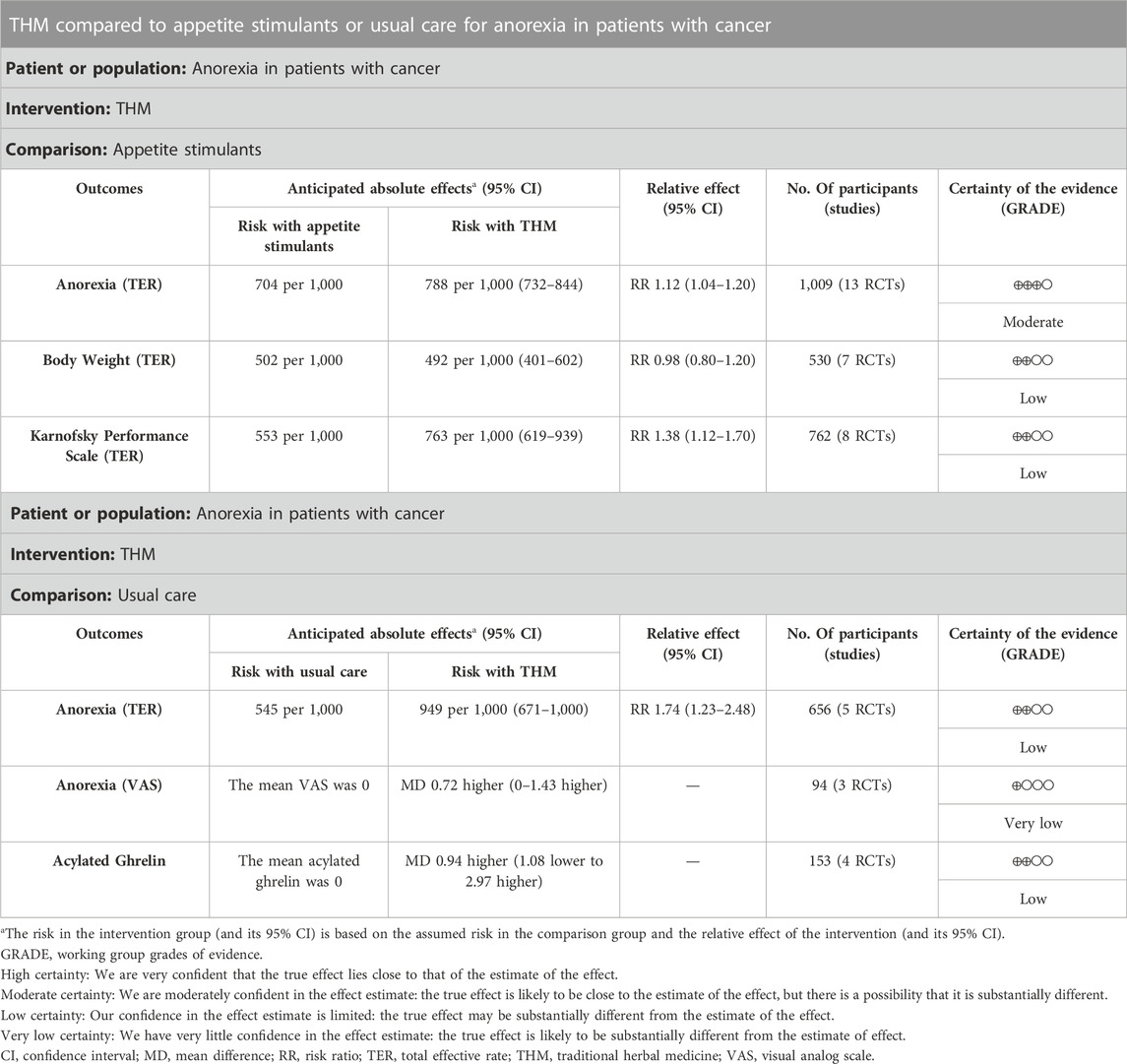
TABLE 2. Summary of findings.
3.4.2 Body weight
Seven RCTs with a total of 530 patients reported the TER of THM versus appetite stimulants for body weight gain and were included in the meta-analysis (Figure 4) (Zhang, 2000; Cai et al., 2003; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Wang et al., 2013b; Zhang et al., 2014). THM did not show significance in body weight gain compared to appetite stimulants (RR 0.98, 95% CI 0.80 to 1.20, p = 0.83) with a low grade of heterogeneity (I2 = 35%). Based on the GRADE profile, the TER of THM compared to appetite stimulants for body weight gain has a low quality of evidence due to methodological limitations and imprecisions (Table 2).
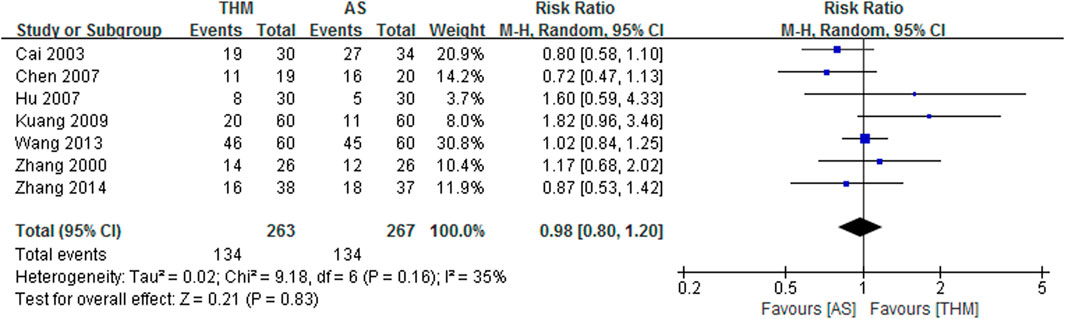
FIGURE 4. Forest plot of the total effective rate of THM versus AS for body weight. THM, traditional herbal medicine; AS, appetite stimulants; CI, confidence intervals.
3.4.3 Karnofsky performance scale
Eight RCTs involving 762 patients were included in the meta-analysis to compare the TER of THM versus appetite stimulants for improving the Karnofsky performance scale, as depicted in Figure 5 (Zhang, 2000; Hu et al., 2007; Kuang et al., 2009; Wang et al., 2013b; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Yi, 2016). The results showed that THM had a statistically significant improvement in the Karnofsky performance scale compared to appetite stimulants (RR 1.38, 95% CI 1.12 to 1.70, p = 0.002) with a high grade of heterogeneity (I2 = 79%). Based on the GRADE profile, the TER of THM versus appetite stimulant for improving the Karnofsky performance scale has a low quality of evidence due to methodological limitations and inconsistencies (Table 2).
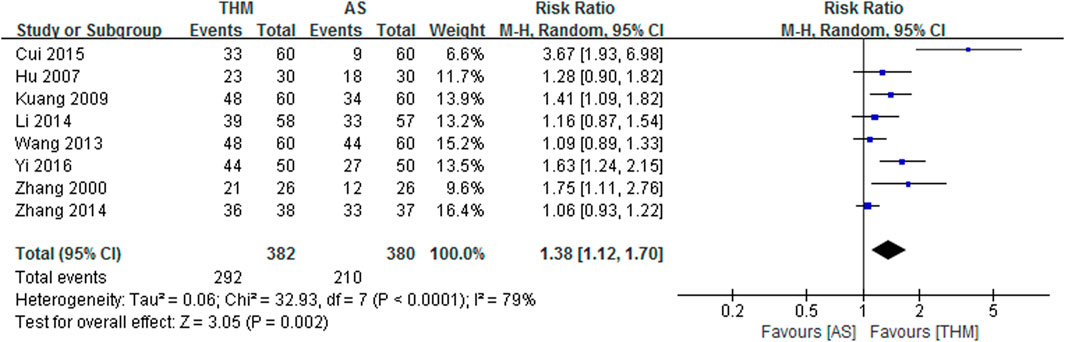
FIGURE 5. Forest plot of the total effective rate of THM versus AS for the Karnofsky performance scale. THM, traditional herbal medicine; AS, appetite stimulants; CI, confidence intervals.
3.5 THM versus usual care
Ten studies compared THM with usual care (Deng, 1997; He et al., 2007; Ohno et al., 2011; Yan et al., 2012; Wang et al., 2013a; Qiu and Zhang, 2013; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020; Ko S. J. et al., 2021), with treatment durations of THM ranging from one to 4 weeks. Four of these studies included various cancer types (He et al., 2007; Yan et al., 2012; Wang et al., 2013a; Qiu and Zhang, 2013), and the other four studies included esophageal (Hamai et al., 2019), uterine (Ohnishi et al., 2017), stomach (Ohno et al., 2011), and lung (Yoshiya et al., 2020) cancers, whereas the remaining two studies did not state the cancer type (Deng, 1997; Ko M. H. et al., 2021). Anorexia was induced by chemotherapy in six studies (He et al., 2007; Ohno et al., 2011; Qiu and Zhang, 2013; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020), cachexia-anorexia syndrome in two studies (Yan et al., 2012; Wang et al., 2013a), radiotherapy in one study (Deng, 1997), and unknown etiology in one study (Ko S. J. et al., 2021).
3.5.1 Anorexia
Five RCTs with a total of 656 patients were included in the meta-analysis to compare the TER of THM versus usual care for improving anorexia, as shown in Figure 6 (Deng, 1997; He et al., 2007; Yan et al., 2012; Wang et al., 2013a; Qiu and Zhang, 2013). The results showed that THM had a statistically significant improvement in anorexia compared to usual care (RR 1.74, 95% CI 1.23 to 2.48, p = 0.002), with a high grade of heterogeneity (I2 = 91%). Based on the GRADE profile, the TER of THM versus usual care for improving anorexia has a low quality of evidence due to methodological limitations and inconsistencies (Table 2).
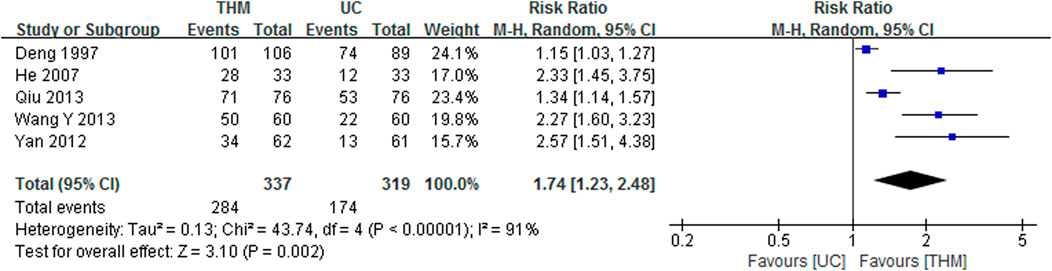
FIGURE 6. Forest plot of the total effective rate of THM versus UC for anorexia. THM, traditional herbal medicine; UC, usual care; CI, confidence intervals.
Three RCTs with a total of 94 patients were included in the meta-analysis to compare the VAS score of THM versus usual care for improving anorexia, as depicted in Figure 7 (Ohnishi et al., 2017; Hamai et al., 2019; Ko M. H. et al., 2021). All three included RCTs used YGJT as a THM intervention. The results showed that THM did not have a statistically significant improvement in anorexia compared to usual care (MD 0.72, 95% CI 0.00 to 1.43, p = 0.05), with a moderate grade of heterogeneity (I2 = 60%). However, based on the GRADE profile, the VAS score of THM compared to usual care for improving anorexia has a very low quality of evidence due to methodological limitations, imprecisions, and inconsistencies (Table 2).

FIGURE 7. Forest plot of the visual analog scale of THM versus UC for anorexia. THM, traditional herbal medicine; UC, usual care; CI, confidence intervals.
3.5.2 Acylated ghrelin
Four RCTs with a total of 153 patients reporting the plasma or serum level of acylated ghrelin in THM versus usual care were included in the meta-analysis, as shown in Figure 8 (Ohno et al., 2011; Ohnishi et al., 2017; Hamai et al., 2019; Yoshiya et al., 2020). All of them compared Rikkunshito with usual care for anorexia in patients with cancer treated with cisplatin-based chemotherapy. THM did not show a statistically significantly higher level of acylated ghrelin compared to usual care (MD 0.94, 95% CI 1.08 to 2.97, p = 0.36), with a low grade of heterogeneity (I2 = 0%). However, based on the GRADE profile, the quality of the evidence for the level of acylated ghrelin in THM compared to usual care was low due to methodological limitations and imprecisions (Table 2).
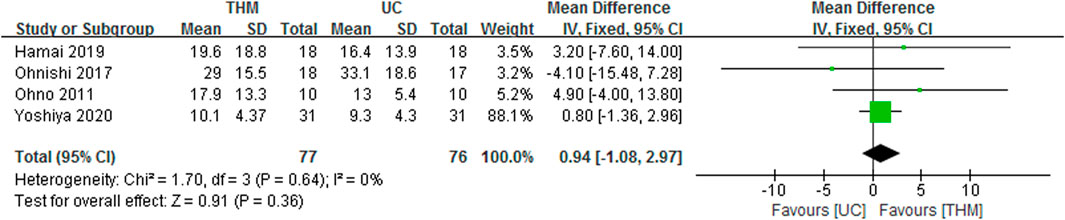
FIGURE 8. Forest plot of the level of acylated ghrelin in THM versus UC. THM, traditional herbal medicine; UC, usual care; CI, confidence intervals.
3.6 Adverse events
Out of 26 included studies, 13 studies reported adverse events. In 11 out of 13 studies, there were no adverse events related to THM (Chen, 2007; Hu et al., 2007; Ohno et al., 2011; Wang et al., 2013a; Cui et al., 2015; Cheon et al., 2017; Ohnishi et al., 2017; Wang et al., 2018; Hamai et al., 2019; Yoshiya et al., 2020; Zhang and Wang, 2020). Two studies (Zhang, 2000; Ko M. H. et al., 2021) reported mild epigastric bloating, upper respiratory inflammation, and heartburn with no serious THM-related adverse events.
3.7 Publication bias
A funnel plot analysis of the 13 RCTs reporting the TER of THM versus appetite stimulants for improvement in anorexia was generated to identify the presence of publication bias (Zhang, 2000; Cai et al., 2003; Chen, 2007; Hu et al., 2007; Kuang et al., 2009; Li and Li, 2011; Wang et al., 2013b; Li et al., 2014; Zhang et al., 2014; Cui et al., 2015; Yu, 2015; Yi, 2016; Wang et al., 2018). Significant asymmetry was not detected, indicating that there was no noticeable publication bias, as shown in Figure 9.
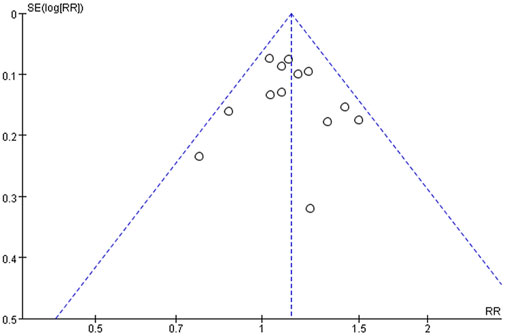
FIGURE 9. Funnel plot of primary outcome. RR, risk ratio; SE, standard error.
4 Discussion
The purpose of this systematic review and meta-analysis was to examine the efficacy and safety of THM in improving anorexia in patients with cancer. This study reviewed 26 studies involving 2,056 patients with cancer suffering from anorexia, of which 23 studies were analyzed quantitatively. The main finding of this study is that THM significantly improved anorexia in patients with cancer compared to appetite stimulants and usual care with moderate and low quality evidence, respectively. Additionally, THM significantly improved the Karnofsky performance scale compared to appetite stimulants, although the quality of the evidence was low. No serious adverse events were reported in the studies evaluating the safety of THM.
Twenty three out of 26 RCTs mentioned the type of cancer, and 3 RCTs did not. There was no relationship between the type of cancer and the THM used to treat cancer-related anorexia. The duration of the THM treatment varies from 1 week to 8 weeks, and 4 weeks was the most common. Although the average treatment period of megestrol acetate and corticosteroids was 8 weeks, the optimal duration of pharmacological treatment remains unknown and long-term use is not recommended (Garcia et al., 2013; Miller et al., 2014; Roeland et al., 2020). Compared to pharmaceutical interventions, the duration of the THM treatment in this study is relatively short, but further research is needed to determine the optimal treatment time because there has been no study comparing the effects of THM depending on the treatment duration.
A previous meta-analysis showed that in children, THM was significantly superior to placebo and active controls such as dietary supplements or conventional medications in improving anorexia symptoms and some biological markers related to appetite (Lee et al., 2022). It also indicated that THM reduces the recurrence rate of anorexia and the incidence of adverse events. Xingpi Yanger granule was the most frequently used herbal formula, and Crataegus pinnatifida Bunge, Atractylodes macrocephala Koidz, Poria cocos (Schw.) Wolf, C. aurantium, Glycyrrhiza uralensis Fisch. ex DC., and Hordeum vulgare L. were frequently used herbs (Lee et al., 2022). These findings are consistent with the results of our study, which also observed that THM improved anorexia in patients with cancer and included commonly used herbs.
In this study, the most frequently used THM prescriptions were YGJT or modified YGJT, which is known as Rikkunshito in Japanese or Liujunzi decoction in Chinese. It is widely used to treat upper gastrointestinal symptoms, including anorexia (Mogami and Hattori, 2014). A previous preclinical study demonstrated that the hesperidin in YGJT improved gastrointestinal motor activities and food intake in rats by inducing endogenous ghrelin secretion through the antagonism of 5-hydroxytryptamine (HT) 2b and 5-HT2c receptors (Fujitsuka et al., 2009). YGJT and its components (10-gingerol) increased plasma levels of acylated ghrelin by inhibiting ghrelin-degrading enzymes in rats treated with cisplatin (Sadakane et al., 2011). YGJT also antagonizes the 5-HT3 receptor (Tominaga et al., 2011). It significantly increased the plasma level of acylated ghrelin in mice and healthy people and upregulated the expression of ghrelin mRNA in the mouse stomach (Matsumura et al., 2010). In clinical studies, YGJT has shown efficacy in improving the symptoms of GERD and functional and drug-associated dyspepsia through its effects on upper gastrointestinal functions and ghrelin secretion signaling. A systematic review and meta-analysis reported that YGJT showed a significantly higher total clinical efficacy rate, higher reduction of total dyspepsia symptom scale, more improved gastric emptying rate and lower recurrence 6 months after treatment in patients with functional dyspepsia compared with western medicine (Ko M. H. et al., 2021). A prior RCT showed that YGJT improved gastrointestinal symptoms and increased plasma ghrelin levels compared to domperidone in patients with FD (Arai et al., 2012). Another RCT demonstrated the efficacy of YGJT against nausea and vomiting caused by selective serotonin reuptake inhibitors (Oka et al., 2007). Although these findings suggest that YGJT has strong evidence for improving anorexia through multiple pathways, our study did not show a statistically significant difference between YGJT and appetite stimulants in treating anorexia or using usual care in the level of acylated ghrelin. These differences may be attributed to concurrent treatment with chemotherapy and a small number of inclusions in the study.
The most frequently used herb in the included RCTs was C. aurantium. The dried peel of C. aurantium was found to have dual effects by inhibiting the strain of intestinal smooth muscle and increasing gastric emptying and small bowel peristalsis activity (Zhang et al., 2012). It effectively relieves the symptoms induced by reserpine in rats, including poor digestion and absorption capacity, and increases the level of gastrin while lowering motilin and cholecystokinin-8 levels (Zheng et al., 2020). Hesperidin in C. aurantium increases the levels of gastrin and decreases the levels of acetylcholine, substance P, motilin, and vasoactive intestinal peptide, while synephrine increases the levels of acetylcholine and motilin and decreases the levels of vasoactive intestinal peptide and substance P (Song et al., 2017). In this study, some RCTs included patients with anorexia who correlated with a specific pattern identification based on the theory of THM (Hu et al., 2007; Kuang et al., 2009; Qiu and Zhang, 2013; Li et al., 2014; Cui et al., 2015; Cheon et al., 2017; Wang et al., 2018; Zhang and Wang, 2020). Most of the pattern identifications were related to deficiency syndromes, including Qi-Blood deficiency, Qi-Yin deficiency, and Spleen-Stomach deficiency. Spleen-Stomach deficiency is a pathological change that leads to a decrease in spleen and stomach activities related to food intake and digestion (World Health Organization Western Pacific Regional Office, 2007). The majority of the herbal formulas in these RCTs have effects that fortify the spleen and promote digestion (Li et al., 2014; Cui et al., 2015), tonify Qi and fortify the spleen (Hu et al., 2007; Qiu and Zhang, 2013; Wang et al., 2018), or tonify Qi and Blood or Yin (Kuang et al., 2009; Cheon et al., 2017). An earlier systematic review reported that invigorating the spleen and regulating Qi therapy is more effective in alleviating symptoms of functional dyspepsia than conventional treatment (Ye et al., 2019). Therefore, it can be assumed that THM, which strengthens the function of the spleen and stomach, encourages digestion, and relieves deficiencies, may be effective for patients with cancer who have anorexia.
Most of the studies that mentioned adverse events reported that there were no adverse events related to THM. Two studies reported mild epigastric bloating, upper respiratory inflammation, and heartburn as THM-related adverse events, and they were not serious (Zhang, 2000; Ko M. H. et al., 2021). Considering that megestrol acetate can cause thromboembolic events, dyspnea, and increased risk of death, and that corticosteroids can be used only for a short period of time due to the adverse events, THM may be considered a safe alternative treatment option (Garcia et al., 2013; Miller et al., 2014; Roeland et al., 2020).
This study has some limitations. First, each study used different outcome measurements, making it difficult to compare and generalize the results. Anorexia was assessed using various scales and indicators, such as the numeric rating scale, the VAS, and food intake. Although food intake and the TER of anorexia were measured, the definitions of efficacy were not consistent across the studies. Second, significant heterogeneity was observed due to differences in treatment duration, doses of appetite stimulants, and the lack of standardization of herbal ingredients. Third, the methodological quality of the included studies was generally limited, with the majority of the studies being graded as having a high or unclear risk of bias due to limited data. In terms of allocation concealment, 21 studies of 26 RCTs did not report the detailed allocation procedure. Blinding of participants and personnel, and blinding of outcome assessment were not performed in 25 studies. As most RCTs in the included studies used positive control such as appetite stimulant or usual care, blinding of participants and personnel could not be performed. Fourth, the long-term effect of THM on cancer-related anorexia could not be determined as most studies had short treatment durations (less than 4 weeks) and did not have a follow-up after treatment. Finally, since the majority of the studies were conducted in Asian countries, it is difficult to generalize these results to broader populations with cancer.
Therefore, large-sample, double-blind RCTs with rigorous methodological evidence are needed. Future studies need to compare the effects of THM depending on the treatment duration to determine the optimal duration. To confirm the long-term effect of THM, follow-up after treatment is also considered. Finally, they should consider a generalized population, standardized herbal ingredients, and standardized outcome measurements to generalize the results to broad populations with cancer.
Nonetheless, this systematic review and meta-analysis is the first attempt to focus on the potential appetite-improving effect of orally administered THM in treating anorexia in patients with cancer. It adhered to rigorous methodologies such as the Preferred Reporting Items for Systematic Reviews and Meta-Analysis and the Cochrane handbook, and addressed the quality of evidence using the GRADE profile. Furthermore, the protocol of this study was registered with the International Prospective Register of Systematic Review, and a search was carried out in various databases without publication language or country restrictions.
5 Conclusion
Moderate to low quality of evidence suggests that THM is more effective than appetite stimulants or usual care in improving anorexia in patients with cancer. The administration of THM was not related to serious adverse events. However, large-sample, double-blind RCTs with rigorous methodological evidence are required to fully define the efficacy and safety of THM in treating cancer-related anorexia. Future studies with a generalized population, standardized herbal ingredients, and an appropriate follow-up duration are recommended.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
SBP contributed to the study concept, design, and drafting of the manuscript. SBP and EHK searched database, determined which studies should be included, and extracted data. J-HY and HJ performed the statistical analysis. SWY proofread, revised, and guided through all stages. All authors contributed to the article and approved the submitted version.
Funding
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (HF20C0038).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1203137/full#supplementary-material
References
Alsharif, F. (2021). Discovering the use of complementary and alternative medicine in oncology patients: A systematic literature review. Evid. Based Complement. Altern. Med. eCAM 2021, 6619243. doi:10.1155/2021/6619243
Arai, M., Matsumura, T., Tsuchiya, N., Sadakane, C., Inami, R., Suzuki, T., et al. (2012). Rikkunshito improves the symptoms in patients with functional dyspepsia, accompanied by an increase in the level of plasma ghrelin. Hepato-gastroenterology 59 (113), 62–66. doi:10.5754/hge11246
Cai, H. B., Luo, K. C., Yang, C. B., Pan, C., Zuo, Q., and Wang, Y. G. (2003). Buzhong Yiqi tang for carcinomatous anorexia - cachexia syndrome: A clinical observation of 30 cases. New J. Traditional Chin. Med. 35 (03), 25–26. doi:10.13457/j.cnki.jncm.2003.03.014
Chen, J. (2007). Treatment of 56 cases of cancer anorexia cachexia syndrome with modified Zhipu Liujunzi Decoction. Shaanxi J. Traditional Chin. Med. (09), 1182–1183.
Chen, Y., Cheng, C. S., Tan, H. Y., Tam, C. W., Wang, N., and Feng, Y. (2021). Efficacy of herbal medicines intervention for colorectal cancer patients with chemotherapy-induced gastrointestinal toxicity—A systematic review and meta-analysis. Front. Oncol. 11, 629132. doi:10.3389/fonc.2021.629132
Cheon, C., Yoo, J. E., Yoo, H. S., Cho, C. K., Kang, S., Kim, M., et al. (2017). Efficacy and safety of sipjeondaebo-tang for anorexia in patients with cancer: A pilot, randomized, double-blind, placebo-controlled trial. Evid. Based Complement. Altern. Med. 2017, 8780325. doi:10.1155/2017/8780325
Chung, V. C., Wu, X., Lu, P., Hui, E. P., Zhang, Y., Zhang, A. L., et al. (2016). Chinese herbal medicine for symptom management in cancer palliative care: Systematic review and meta-analysis. Medicine 95 (7), e2793. doi:10.1097/md.0000000000002793
Cui, Y. X., Zhang, Y., Ren, F., Wang, H. M., Feng, Y., and Li, S. (2015). Clinical study on Kaiwei Jinshi Tang in the treatment of anorexia associated with malignant tumor. Beijing J. Traditional Chin. Med. 34 (05), 353–355. doi:10.16025/j.1674-1307.2015.05.003
Deng, G. (1997). Xiangsha Erya Kaiwei Decoction for the treatment of anorexia in cancer patients during radiotherapy. Sichuan J. Traditional Chin. Med. (09), 32.
Ezeoke, C. C., and Morley, J. E. (2015). Pathophysiology of anorexia in the cancer cachexia syndrome. J. Cachexia Sarcopenia Muscle 6 (4), 287–302. doi:10.1002/jcsm.12059
Fu, D. Z. (2006). Improvement of anorexia and weight reducing in patients with lung cancer by integrated Chinese and Western medicine. Zhejiang J. Intergrative Traditional Chin. West. Med. 16, 471–472.
Fujitsuka, N., Asakawa, A., Hayashi, M., Sameshima, M., Amitani, H., Kojima, S., et al. (2009). Selective serotonin reuptake inhibitors modify physiological gastrointestinal motor activities via 5-HT2c receptor and acyl ghrelin. Biol. Psychiatry 65 (9), 748–759. doi:10.1016/j.biopsych.2008.10.031
Garcia, V. R., López-Briz, E., Sanchis, R. C., Perales, J. L. G., and Bort-Martí, S. (2013). Megestrol acetate for treatment of anorexia-cachexia syndrome. Cochrane Database Syst. Rev. 2013 (3), Cd004310. doi:10.1002/14651858.CD004310.pub3
Hamai, Y., Yoshiya, T., Hihara, J., Emi, M., Furukawa, T., Yamakita, I., et al. (2019). Traditional Japanese herbal medicine rikkunshito increases food intake and plasma acylated ghrelin levels in patients with esophageal cancer treated by cisplatin-based chemotherapy. J. Thorac. Dis. 11 (6), 2470–2478. doi:10.21037/jtd.2019.05.67
He, Y., Jiang, H., Wang, S., and Yang, X. (2007). Clinical observation on Bazhen granule in treating anorexia after chemotherapy. Hainan Med. J. 11, 87. CNKI:SUN:HAIN.0.2007-11-053.
Higgins, J. P. T., Churchill, R., Chandler, J., and Cumpston, M. S. (2017). Cochrane handbook for systematic reviews of interventions. Available at: http://www.training.cochrane.org/handbook (Accessed April 24, 2021).
Hu, W., Wang, J., and Lin, S. (2007). The short-time effect of Shenqijiaocao decoction in treating 30 cases of advanced lung cancer cachexia. J. Zhejiang Univ. Traditional Chin. Med. (02), 194–195. doi:10.16466/j.issn1005-5509.2007.02.029
Huang, J., Lin, Q., Chen, Y., and Chen, J. (2015). Clinical study on the curative effect of additive Xiangsha Liujunzi decoction on anorexia from Chemotherapy in patients with malignant tumor. Clin. J. Chin. Med. 7 (08), 64–66. doi:10.3969/j.issn.1674-7860.2015.8.035
Iwase, S., Yamaguchi, T., Miyaji, T., Terawaki, K., Inui, A., and Uezono, Y. (2012). The clinical use of kampo medicines (traditional Japanese herbal treatments) for controlling cancer patients' symptoms in Japan: A national cross-sectional survey. BMC complementary Altern. Med. 12, 222. doi:10.1186/1472-6882-12-222
Judson, P. L., Abdallah, R., Xiong, Y., Ebbert, J., and Lancaster, J. M. (2017). Complementary and alternative medicine use in individuals presenting for care at a comprehensive cancer center. Integr. cancer Ther. 16 (1), 96–103. doi:10.1177/1534735416660384
Ko, M. H., Song, S. Y., Ha, S. J., Lee, J. Y., Yoon, S. W., Park, J. H., et al. (2021a). Efficacy and safety of yukgunja-tang for patients with cancer-related anorexia: A randomized, controlled trial, pilot study. Integr. Cancer Ther. 20, 15347354211019107. doi:10.1177/15347354211019107
Ko, S. J., Park, J., Kim, M. J., Kim, J., and Park, J. W. (2021b). Effects of the herbal medicine rikkunshito, for functional dyspepsia: A systematic review and meta-analysis. J. gastroenterology hepatology 36 (1), 64–74. doi:10.1111/jgh.15208
Kuang, T., Liu, Y., and Yao, Y. (2009). Clinical observation on 60 cases of advanced lung cancer cachexia treated with Yiqi Yangyin Decoction. Zhejiang J. Traditional Chin. Med. 44 (06), 421–422.
Laviano, A., Koverech, A., and Seelaender, M. (2017). Assessing pathophysiology of cancer anorexia. Curr. Opin. Clin. Nutr. Metab. Care 20 (5), 340–345. doi:10.1097/MCO.0000000000000394
Lee, B., Kwon, C.-Y., Lee, S. H., and Chang, G. T. (2022). Herbal medicine for the treatment of anorexia in children: A systematic review and meta-analysis. Front. Pharmacol. 13, 839668. doi:10.3389/fphar.2022.839668
Lee, J. H., Bae, K., Yoo, H. S., Kim, M. N., and Cho, J. H. (2017). Difference of auditory brainstem responses by stimulating to round and oval window in animal experiments. J. Korean Med. 38 (1), 8–13. doi:10.1080/21655979.2016.1226662
Li, J. R., Wang, H. W., Jia, M., Li, X., and Du, H. T. (2014). Jiaweizhizhu particles improved cancerous tumor patients clinical observation of anorexia. Chin. J. Clin. 42 (09), 24–26.
Li, Y., and Li, C. (2011). 40 cases of cancer cachexia treated with Jianpi Huatan Decoction. Traditional Chin. Med. Res. 24 (10), 29–31.
Liu, W., Lopez, G., Narayanan, S., Qdaisat, A., Geng, Y., Zhou, S., et al. (2021). Acupuncture for cancer-related anorexia: A review of the current evidence. Curr. Oncol. Rep. 23 (7), 82. doi:10.1007/s11912-021-01067-1
Matsumura, T., Arai, M., Yonemitsu, Y., Maruoka, D., Tanaka, T., Suzuki, T., et al. (2010). The traditional Japanese medicine Rikkunshito increases the plasma level of ghrelin in humans and mice. J. Gastroenterol. 45 (3), 300–307. doi:10.1007/s00535-009-0166-z
Mattox, T. W. (2017). Cancer cachexia: Cause, diagnosis, and treatment. Nutr. Clin. Pract. 32 (5), 599–606. doi:10.1177/0884533617722986
McQuade, J. L., Meng, Z., Chen, Z., Wei, Q., Zhang, Y., Bei, W., et al. (2012). Utilization of and attitudes towards traditional Chinese medicine therapies in a Chinese cancer hospital: A survey of patients and physicians. Evidence-based complementary Altern. Med. eCAM, 2012, 504507. doi:10.1155/2012/504507
Miller, S., McNutt, L., McCann, M. A., and McCorry, N. (2014). Use of corticosteroids for anorexia in palliative medicine: A systematic review. J. Palliat. Med. 17 (4), 482–485. doi:10.1089/jpm.2013.0324
Mogami, S., and Hattori, T. (2014). Beneficial effects of rikkunshito, a Japanese kampo medicine, on gastrointestinal dysfunction and anorexia in combination with western drug: A systematic review. Evid. Based Complement. Altern. Med. 2014, 519035. doi:10.1155/2014/519035
Ohnishi, S., Watari, H., Kanno, M., Ohba, Y., Takeuchi, S., Miyaji, T., et al. (2017). Additive effect of rikkunshito, an herbal medicine, on chemotherapy-induced nausea, vomiting, and anorexia in uterine cervical or corpus cancer patients treated with cisplatin and paclitaxel: Results of a randomized phase II study (JORTC KMP-02). J. Gynecol. Oncol. 28 (5), e44. doi:10.3802/jgo.2017.28.e44
Ohno, T., Yanai, M., Ando, H., Toyomasu, Y., Ogawa, A., Morita, H., et al. (2011). Rikkunshito, a traditional Japanese medicine, suppresses cisplatin-induced anorexia in humans. Clin. Exp. Gastroenterol. 4, 291–296. doi:10.2147/ceg.S26297
Oka, T., Tamagawa, Y., Hayashida, S., Kaneda, Y., Kodama, N., and Tsuji, S. (2007). Rikkunshi-to attenuates adverse gastrointestinal symptoms induced by fluvoxamine. Biopsychosoc. Med. 1, 21. doi:10.1186/1751-0759-1-21
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj 372, n71. doi:10.1136/bmj.n71
Park, B., You, S., Cho, W., Choi, J. Y., and Lee, M. S. (2019). A systematic review of herbal medicines for the treatment of cancer cachexia in animal models. J. Zhejiang University-Science B 20 (1), 9–22. doi:10.1631/jzus.B1800171
Qiu, W., and Zhang, X. (2013). Modified shenling Baizhu powder for reducing anorexia caused by chemotherapy: A report of 76 cases. Fujian J. Traditional Chin. Med. 44 (04), 11–12. doi:10.13260/j.cnki.jfjtcm.010589
Roeland, E. J., Bohlke, K., Baracos, V. E., Bruera, E., Del Fabbro, E., Dixon, S., et al. (2020). Management of cancer cachexia: ASCO guideline. J. Clin. Oncol. 38 (21), 2438–2453. doi:10.1200/JCO.20.00611
Sadakane, C., Muto, S., Nakagawa, K., Ohnishi, S., Saegusa, Y., Nahata, M., et al. (2011). 10-Gingerol, a component of rikkunshito, improves cisplatin-induced anorexia by inhibiting acylated ghrelin degradation. Biochem. Biophys. Res. Commun. 412 (3), 506–511. doi:10.1016/j.bbrc.2011.08.002
Schünemann, H., Brożek, J., Guyatt, G., and Oxman, A. (2013). GRADE handbook for grading quality of evidence and strength of recommendations [Online]. The grade Working group. Available: guidelinedevelopment.org/handbook [Accessed].
Song, Y. P., Chen, H. F., Hu, Y. X., Shum, T. S., and Quan, L. X. (2017). Effect of Pericarpium Citri Reticulatae and its main active ingredients on gastrin in serum, acetylcholine, motilin, substance P and vasoactive intestinal peptide in plasma of rats. Pharmacol. Clin. Chin. Materia Medica 33 (3), 79–83. doi:10.13412/j.cnki.zyyl.2017.03.023
Sun, L., Mao, J. J., Liu, Q., Yang, Y., and He, B. (2020). Effects of auricular acupuncture on appetite in patients with advanced cancer: A pilot randomized controlled trial. Ann. Palliat. Med. 9 (4), 1804–1811. doi:10.21037/apm.2020.04.24
Tarricone, R., Ricca, G., Nyanzi-Wakholi, B., and Medina-Lara, A. (2016). Impact of cancer anorexia-cachexia syndrome on health-related quality of life and resource utilisation: A systematic review. Crit. Rev. Oncol. Hematol. 99, 49–62. doi:10.1016/j.critrevonc.2015.12.008
Tominaga, K., Kido, T., Ochi, M., Sadakane, C., Mase, A., Okazaki, H., et al. (2011). The traditional Japanese medicine rikkunshito promotes gastric emptying via the antagonistic action of the 5-HT3 receptor pathway in rats. Evid. Based Complement. Altern. Med. 2011, 248481. doi:10.1093/ecam/nep173
Trajkovic-Vidakovic, M., de Graeff, A., Voest, E. E., and Teunissen, S. C. (2012). Symptoms tell it all: A systematic review of the value of symptom assessment to predict survival in advanced cancer patients. Crit. Rev. Oncol. Hematol. 84 (1), 130–148. doi:10.1016/j.critrevonc.2012.02.011
Tufanaru, C., Munn, Z., Stephenson, M., and Aromataris, E. (2015). Fixed or random effects meta-analysis? Common methodological issues in systematic reviews of effectiveness. Int. J. Evid. Based Healthc. 13 (3), 196–207. doi:10.1097/XEB.0000000000000065
Wang, L., Zou, X., and Liu, S.-L. (2018). Clinical research on modified Xiangsha Liujun decoctin combined with medroxyprogesterone in treating cancer-related anorexia and cachexia syndrome. Chin. J. Integr. Traditional West. Med. 38 (08), 927–931. doi:10.7661/j.cjim.20180623.182
Wang, Y., Zhang, X., An, F., Zhao, W., Wang, H., and Gu, R. (2013a). Randomized controlled study of shuyu pill combined with the best supportive treating patients suffering from cancer anorexia. J. Pract. Traditional Chin. Intern. Med. 27 (08), 99–101.
Wang, Y., Zhu, M., Zhao, W., and Zhang, X. (2013b). Effect of Dioscorea Pill on tumor related anorexia. Clin. J. Traditional Chin. Med. 25 (10), 850–852. doi:10.16448/j.cjtcm.2013.10.033
Wiffen, P. J., Derry, S., and Moore, R. A. (2014). Impact of morphine, fentanyl, oxycodone or codeine on patient consciousness, appetite and thirst when used to treat cancer pain. Cochrane Database Syst. Rev. 2014 (5), CD011056. doi:10.1002/14651858.CD011056.pub2
World Health Organization Western Pacific Regional Office (2007). WHO international standard terminologies on traditional medicine in the western pacific region. Manila: World Health Organization.
Xu, B., Cheng, Q., and So, W. K. W. (2021). Review of the effects and safety of traditional Chinese medicine in the treatment of cancer cachexia. Asia-Pacific J. Oncol. Nurs. 8 (5), 471–486. doi:10.4103/apjon.apjon-2130
Yan, W., Huang, J., and Chen, J. (2012). Clinical observation on Xiangsha Zhizhu Jiawe Decoction in improving correlation anorexia of tumor. China Mod. Med. 19 (32), 120–121.
Ye, J. T., Dai, Y. K., Li, D. Y., Zhang, Y. Z., Huang, M. X., Chen, W. J., et al. (2019). Efficacy of jianpi liqi therapy for functional dyspepsia: A meta-analysis of randomized, positive medicine-controlled trials. Medicine 98(33), e16607. doi:10.1097/MD.0000000000016607
Yi, Y. (2016). Clinical effect of kaiweiyitang on anorexia associated with malignant tumor. Asia-Pacific Tradit. Med. 12 (22), 138–139. doi:10.11954/ytctyy.201622061
Yoon, J. H., Park, S. B., Kim, E. H., Lee, J. Y., and Yoon, S. W. (2021). A survey on clinical practice patterns of patients with cancer at Korean medical hospitals for Korean medicine cancer registry. J. Korean Traditional Oncol. 26 (1), 17–27. doi:10.15432/JKTO.2021.26.1.017
Yoshiya, T., Mimae, T., Ito, M., Sasada, S., Tsutani, Y., Satoh, K., et al. (2020). Prospective, randomized, cross-over pilot study of the effects of Rikkunshito, a Japanese traditional herbal medicine, on anorexia and plasma-acylated ghrelin levels in lung cancer patients undergoing cisplatin-based chemotherapy. Investig. New Drugs 38 (2), 485–492. doi:10.1007/s10637-019-00836-x
Yu, G. (2015). Curative effect of jianpi huatan decoction on cancer cachexia. J. Clin. Med. Literature 2 (18), 3712–3713. doi:10.16281/j.cnki.jocml.2015.18.086
Zhang, F., Shen, A., Jin, Y., and Qiang, W. (2018). The management strategies of cancer-associated anorexia: A critical appraisal of systematic reviews. BMC Complement. Altern. Med. 18 (1), 236. doi:10.1186/s12906-018-2304-8
Zhang, J. (2000). Effect of traditional Chinese medicine on cachexia of cancer patients. Chin. J. Integr. Traditional West. Med. (11), 871. CNKI:SUN:ZZXJ.0.2000-11-038.
Zhang, M., and Wang, Y. (2020). Treatment of 60 cases of tumor related anorexia with Fuzi Lizhong Decoction. Jiangxi J. Traditional Chin. Med. 51 (06), 47–49.
Zhang, N., and Xiao, X. H. (2021). Integrative medicine in the era of cancer immunotherapy: Challenges and opportunities. J. Integr. Med. 19 (4), 291–294. doi:10.1016/j.joim.2021.03.005
Zhang, X., Ji, Z., Zhao, C., Ma, B., Du, G., Yue, J., et al. (2012). Identification of putative biomarkers for the serodiagnosis of drug-resistant Mycobacterium tuberculosis. J. Henan Univ. Med. Sci. 31 (1), 12–14. doi:10.1186/1477-5956-10-12
Zhang, Y. C., Jia, Y. J., Lu, N., Yang, P. Y., Zhang, X., Zhu, J. L., et al. (2014). Effect of “xiaoyan Decoction”on cancer cachexia: On the basis of leptin-feeding-immune network. Shanghai J. Traditional Chin. Med. 48 (04), 29–31.
Keywords: cancer, anorexia, traditional herbal medicine, systematic review, meta-analysis
Citation: Park SB, Yoon J-H, Kim EH, Jin H and Yoon SW (2023) Traditional herbal medicine for anorexia in patients with cancer: a systematic review and meta-analysis of randomized controlled trials. Front. Pharmacol. 14:1203137. doi: 10.3389/fphar.2023.1203137
Received: 10 April 2023; Accepted: 19 June 2023;
Published: 27 June 2023.
Edited by:
Chen Ling, Fudan University, ChinaReviewed by:
Hisayoshi Norimoto, PuraPharm International (H. K) Ltd., Hong Kong SAR, ChinaDalinda Isabel Sánchez-Vidaña, Hong Kong Polytechnic University, Hong Kong SAR, China
Hongyun Chen, Shanghai University of Traditional Chinese Medicine, China
Copyright © 2023 Park, Yoon, Kim, Jin and Yoon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Seong Woo Yoon, c3RlcGFubzIxMkBoYW5tYWlsLm5ldA==