 Kay Khine Soe1
Kay Khine Soe1 Thanachit Krikeerati2
Thanachit Krikeerati2 Chatkamol Pheerapanyawaranun3
Chatkamol Pheerapanyawaranun3 Suvimol Niyomnaitham1
Suvimol Niyomnaitham1 Phichayut Phinyo4,5,6
Phichayut Phinyo4,5,6 Torpong Thongngarm2*
Torpong Thongngarm2*- 1Department of Pharmacology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
- 2Division of Allergy and Clinical Immunology, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
- 3Siriraj Institute of Clinical Research, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
- 4Center for Clinical Epidemiology and Clinical Statistics, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
- 5Department of Family Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
- 6Musculoskeletal Science and Translational Research (MSTR), Chiang Mai University, Chiang Mai, Thailand
No evidence shows that one intranasal corticosteroid (INCS) is better than another for treating moderate-to-severe allergic rhinitis (AR). This network meta-analysis assessed the comparative efficacy and acceptability of licensed dose aqueous INCSs. PubMed/MEDLINE, Scopus, EMBASE, and the Cochrane Central Register of Controlled Trials were searched until 31 March 2022. Eligible studies included randomized controlled trials comparing INCSs with placebo or other types of INCSs in patients with moderate-to-severe allergic rhinitis. Two reviewers independently screened and extracted data following the Preferred Reporting Items in Systematic Reviews and Meta-analysis guideline. A random-effects model was used for data pooling. Continuous outcomes were expressed as standardized mean difference (SMD). The primary outcomes were the efficacy in improving total nasal symptom score (TNSS) and treatment acceptability (the study dropout). We included 26 studies, 13 with 5,134 seasonal AR patients and 13 with 4,393 perennial AR patients. Most placebo-controlled studies had a moderate quality of evidence. In seasonal AR, mometasone furoate (MF) was ranked the highest efficacy, followed by fluticasone furoate (FF), ciclesonide (CIC), fluticasone propionate and triamcinolone acetonide (TAA) (SMD −0.47, 95% CI: −0.63 to −0.31; −0.46, 95% CI: −0.59 to −0.33; −0.44, 95% CI: −0.75 to −0.13; −0.42, 95% CI: −0.67 to −0.17 and −0.41, 95% CI: −0.81 to −0.00), In perennial AR, budesonide was ranked the highest efficacy, followed by FF, TAA, CIC, and MF (SMD −0.43, 95% CI: −0.75 to −0.11; −0.36, 95% CI: −0.53 to −0.19; −0.32, 95% CI: −0.54 to −0.10; −0.29, 95% CI: −0.48 to −0.11; and −0.28, 95% CI: −0.55 to −0.01). The acceptability of all included INCSs was not inferior to the placebo. According to our indirect comparison, some INCSs have superior efficacy to others with moderate quality of evidence in most placebo-controlled studies for treating moderate-to-severe AR.
1 Introduction
The introduction of intranasal corticosteroid (INCS) spray in the early 1970s (Mygind, 1973) was a crucial advanced step for treating allergic rhinitis (AR). INCS is more effective than antihistamines, both oral and intranasal routes, and anti-leukotrienes and is currently the mainstay of treatment in patients with moderate-to-severe AR in both children and adults (Bousquet et al., 2020; Dykewicz et al., 2020).
Eight INCS in an aqueous nasal spray are approved for AR management: beclomethasone dipropionate (BDP), budesonide (BUD), flunisolide, triamcinolone acetonide (TAA), ciclesonide (CIC), fluticasone propionate (FP), mometasone furoate (MF), and fluticasone furoate (FF). Newer INCS, including FF, MF, and FP, have higher glucocorticoid receptor (GR) binding affinities and very low systemic bioavailability compared to older ones, such as BDP, BUD, and TAA (Derendorf and Meltzer, 2008). Although the pharmacological profiles of newer agents are close to desired criteria of an ideal INCS, well-designed head-to-head randomized controlled trials (RCTs) comparing the efficacy among INCSs are limited. Moreover, differences in types and severity of AR population, study duration, and outcome assessment of those RCTs also hamper the comparison among INCSs.
Therefore, identifying the preferred INCS with the most remarkable efficacy remains challenging. This systematic review (SR) and network meta-analysis (NMA) aims to assess the comparative efficacy and treatment acceptability (the study dropout) across all licensed-dose aqueous INCSs for moderate-to-severe AR.
2 Materials and methods
We followed the Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (Chaimani et al., 2019) in conducting this SR and NMA. The reporting of this review complied with the Preferred Reporting Items for Systematic Reviews and Meta-analyses statement extension for NMA (Hutton et al., 2015). The review protocol was registered in the International prospective register of systematic reviews (PROSPERO CRD42022336687).
2.1 Eligibility criteria
The study inclusion criteria comprised: 1) RCTs; 2) Participants: patients of all ages with moderate-to-severe AR, defined by the baseline total nasal symptom score (TNSS) of at least 6 of 0–12 scale, 3) Intervetion: a licensed dose of aqueous INCSs for at least 2 weeks for seasonal AR (SAR) and at least 4 weeks for perennial AR (PAR) (United States Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER), 2018); 4) Comparators: placebo or other types of aqueous INCSs. Exclusion criteria are patients with non-allergic rhinitis, rhinosinusitis, INCS in a formulation other than aqueous, studies with no abstract or available full-text, and duplicated published studies.
The primary outcomes were efficacy measured by TNSS changes from baseline and treatment acceptability (defined by the study dropout for any reason). The secondary outcomes were efficacy in improving ocular symptoms measured by the changes from baseline in total ocular symptom score (TOSS). All the outcomes were measured at week 2 for seasonal AR and week 4 for perennial AR after randomized assignments.
2.2 Search strategy
Electronic medical databases included PubMed/MEDLINE, Scopus, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL). A search strategy for each database is provided in Supplementary Table S1. A prespecified search strategy was used to search for relevant literature from its inception to the end of 31 March 2022. The authors also reviewed previous references from previously reported SR and/or meta-analyses on the same topic.
2.3 Study selection
Two review authors (KS and TK) independently screened titles and abstracts of all retrieved records from database searching to determine the eligible studies. These two authors retrieved and screened the full-text articles according to the prespecified inclusion and exclusion criteria. All studies chosen to be excluded were discussed, and the reasons for the exclusion were recorded. Any disagreement during this selection process was resolved by consulting a clinical expert in allergy (TT) and a clinical methodologist (PP).
2.4 Data extraction
Two reviewers (KS and CP) independently extracted the data: study and patient characteristics, including baseline symptom or severity score, definition or description of intervention and control treatments, factors with potential effect modification, and the outcomes of interest. All the extracted data was cross-checked and confirmed with the lead investigator (TT). To assess the plausibility of conducting NMA, we tabulated the study and clinical characteristics, including potential effect modifiers, to evaluate the transitivity assumptions to ensure systematic differences among all available treatment comparisons do not exist (Salanti, 2012; Rouse et al., 2017).
We extracted the exact mean change values and their standard deviations (SD) for each treatment arm from each study for continuous outcomes. However, for studies that did not directly report these values, we employed the methods suggested by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2019) and other relevant literature (Wan et al., 2014; Luo et al., 2018) to estimate the mean and SD values. For categorical outcomes, the total number of patients and events in each treatment arm were collected. If no events were identified, we imputed the zero value with 0.5 (Friedrich et al., 2007).
2.5 Risk of bias assessment
The internal validity of the included RCTs was evaluated using Risk-of-Bias 2 assessment tools (Sterne et al., 2019). Two authors (KS and TK) independently assessed the risk of bias. Any discrepancy during the assessment was resolved through discussion with PP and TT.
2.6 Grading quality of evidence
Two reviewers (KS and TK) independently graded the certainty evidence for each outcome using the Grading of Recommended Assessment, Development, and Evaluation (GRADE) approach (Puhan et al., 2014). All pairwise comparisons were rated based on their risk of bias, imprecision, inconsistency, and indirectness into four levels of evidence quality: high, moderate, low, and very low. Any disagreement was resolved through discussion with the clinical methodologist (PP).
2.7 Statistical analysis
Before conducting the meta-analysis, both clinical and methodological heterogeneity of each study were assessed to examine transitivity and trial homogeneity. Heterogeneity was assessed by Cochran’s Q test and Higgin’s I2 statistic, respectively (Higgins et al., 2003).
A pairwise meta-analysis was performed using a random-effects model by DerSimonian and Laird (DerSimonian and Laird, 1986). A random-effects NMA was performed using a frequentist approach to estimate the comparative efficacy among all available treatments (Lu and Ades, 2004; Rucker and Schwarzer, 2015). We planned to express the continuous outcomes using mean difference. As the TNSS and TOSS were continuous data with varying scales of measurements, standardized mean difference (SMD) was used. The interpretation of SMD was as follows: 0.2 for small, 0.5 for medium, and 0.8 for large effect (Cohen, 1988). In this study, we determined the cutoff for minimal clinically important difference at an SMD of 0.2 (Lemieux et al., 2007). For categorical outcomes, the odds ratio (OR) was used.
To ensure valid NMA estimates, we evaluated the consistency assumption using the global test, the loop-specific approach, and the node-splitting approach (Mills et al., 2013; Veroniki et al., 2013; Chaimani et al., 2017; Rouse et al., 2017). Treatment ranking for each outcome was based on the mean surface under the cumulative ranking (SUCRA). Rankograms and league tables are presented separately for each outcome. A hierarchical clustering analysis was conducted using two-dimensional plots to group treatments according to their underlying SUCRA on efficacy and acceptability (Chaimani et al., 2013). Publication bias was evaluated using a comparison-adjusted funnel plot of treatments (Chaimani and Salanti, 2012).
Sensitivity analyses were performed by excluding studies involving children, studies with a high risk of bias, studies published prior to 2000, and studies with small sample sizes (sample size less than the 10th percentile). We also conducted a leave-one-out sensitivity analysis in which we omitted one study from each round of analysis.
All statistical analyses were performed using Stata 17 (StataCorp, College Station, TX). Except for a p-value less than .10 for the heterogeneity test, a 2-tailed p-value less than .05 was considered statistical significance.
3 Results
3.1 Study selection and characteristics
The systematic literature search details are provided in Figure 1. Screening titles and abstracts retrieved 121 full texts of potentially relevant studies. After screening those full texts, 89 studies were excluded, as shown in Supplementary Table S2. Thirty-two RCTs involving patients with moderate-to-severe AR were included for qualitative synthesis, as described in Table 1. Six studies had insufficient outcome data for quantitative synthesis (Ratner et al., 1992; van Bavel et al., 1994; Bronsky et al., 1996; Gross et al., 2002; Lumry et al., 2003; Meltzer et al., 2004). Therefore, only 26 studies, 13 with 5,134 SAR patients (Meltzer et al., 1998; Berger et al., 2003; Gawchik et al., 2003; Ratner et al., 2006; Fokkens et al., 2007; Kaiser et al., 2007; Andrews et al., 2009; Jacobs et al., 2009; Okubo et al., 2009; Prenner et al., 2010; Meltzer et al., 2011; Igarashi et al., 2012; Ratner et al., 2015) and 13 with 4,393 PAR patients (Kobayashi et al., 1995; Fokkens et al., 2002; Tai and Wang, 2003; Chervinsky et al., 2007; Meltzer et al., 2007; Rosenblut et al., 2007; Nathan et al., 2008; Vasar et al., 2008; Weinstein et al., 2009; Baena-Cagnani and Patel, 2010; Given et al., 2010; Meltzer et al., 2010; Karaulov et al., 2019), were included in NMA. Of 26 studies, 3 (Fokkens et al., 2002; Weinstein et al., 2009; Baena-Cagnani and Patel, 2010) were conducted in children and 23 in adults and adolescents. Three studies (Berger et al., 2003; Tai and Wang, 2003; Karaulov et al., 2019) compared active drug VS active drug, 1 (Okubo et al., 2009) compared 2 active drugs VS placebo, and 22 compared active drug VS placebo.
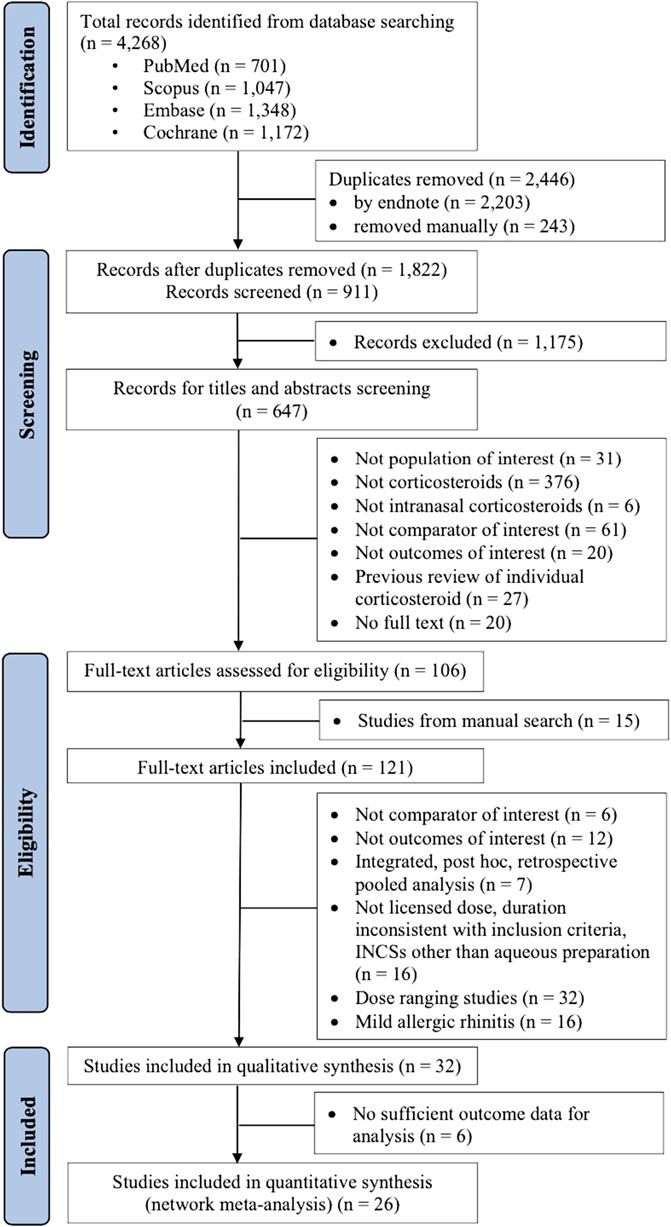
FIGURE 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of included and excluded studies.
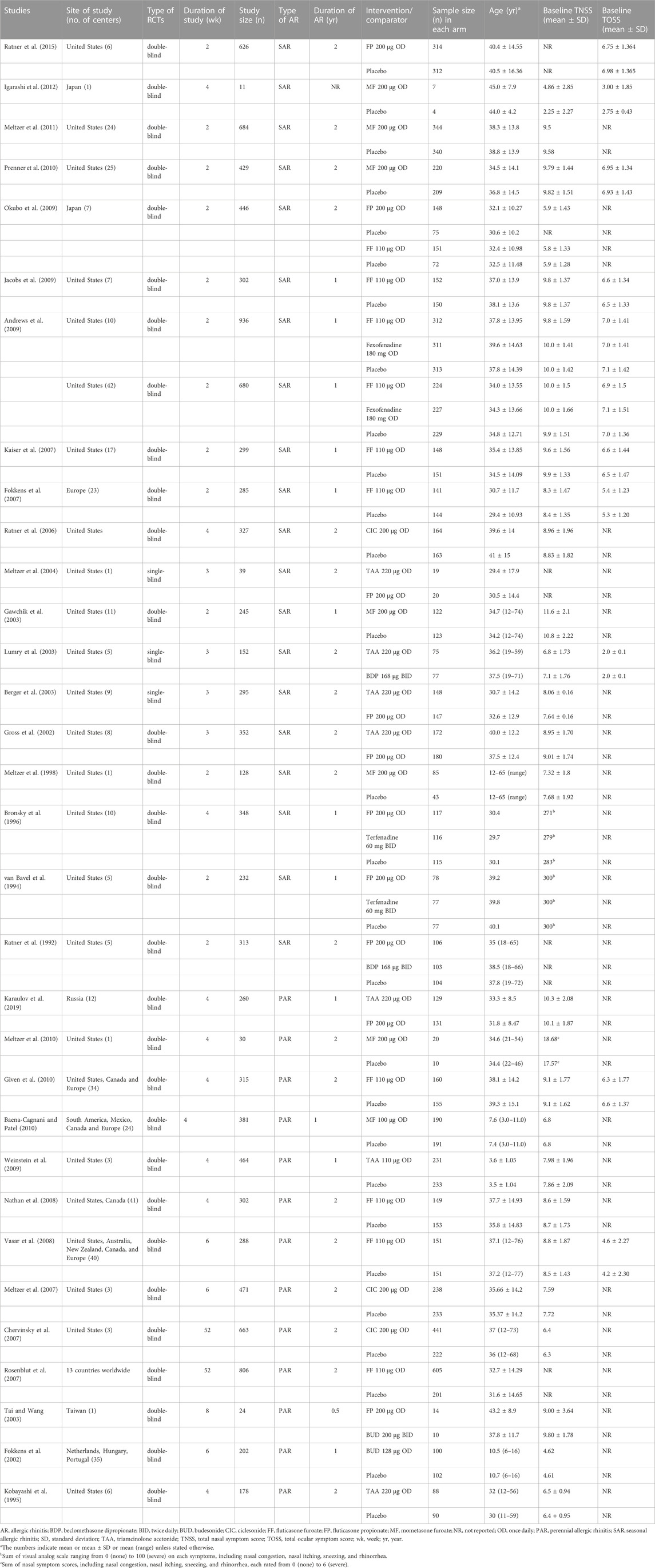
TABLE 1. Characteristics of included studies.
The network diagrams of available comparison pairs for both efficacy and acceptability outcomes are illustrated in Figure 2. Details on the inclusion criteria, exclusion criteria, number, and reasons for withdrawals of each study are shown in Supplementary Table S3. Details on the outcome of interest, point of outcome measurements, and definitions of outcomes are shown in Supplementary Table S4.
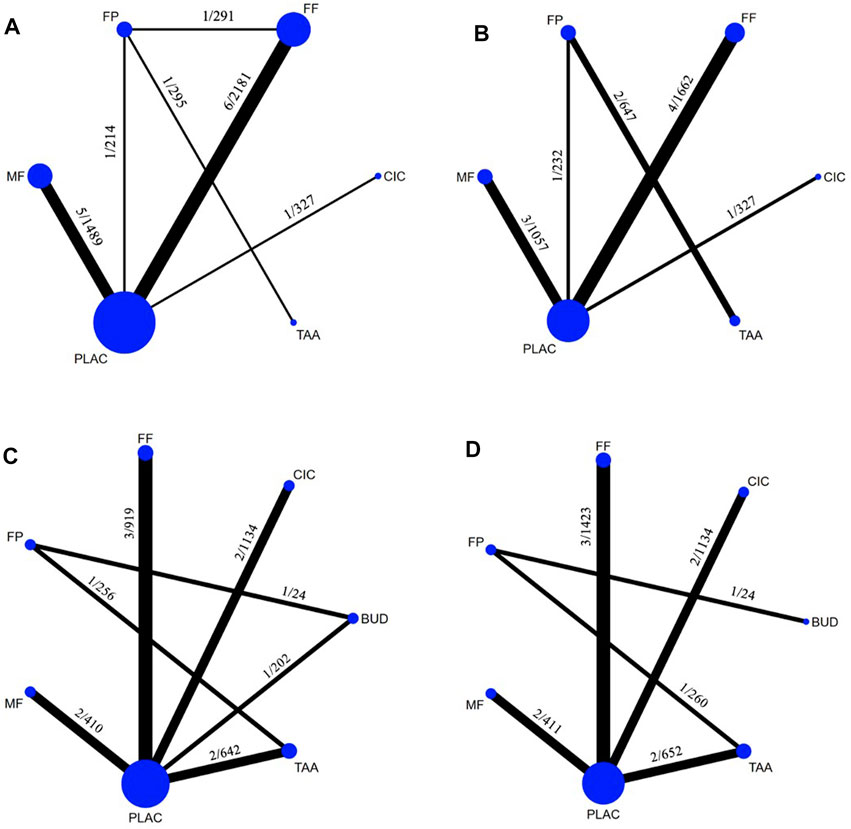
FIGURE 2. Networks of treatment comparisons according to the outcomes measured: (A), Total nasal symptom score changes from baseline (12 studies, 15 treatment pairs, 4,508 patients) and (B), Acceptability (10 studies, 11 treatment pairs, 3,925 patients) in seasonal allergic rhinitis; (C), Total nasal symptom score changes from baseline (12 studies, 12 treatment pairs, 3,587 patients) and (D), Acceptability (11 studies, 11 treatment pairs, 3,904 patients) in perennial allergic rhinitis. The thickness of the lines is proportional to the number of trials comparing each pair of treatments. The labels on each line represent the number of studies/the total number of patients involved in the comparison. The size of each circle is proportional to the number of randomly assigned participants. BUD, budesonide; CIC, ciclesonide; FF, fluticasone furoate; FP, fluticasone propionate; MF, mometasone furoate; TAA, triamcinolone acetonide.
3.2 Assessment of risk of bias
Regarding the quality of the studies, 26 studies were rated to have a low risk of bias, 4 studies had a high risk of bias, and 2 studies had some concerns (Supplementary Figure S1 and Supplementary Figure S2). Details of the risk-of-bias evaluation of each included study are shown in Supplementary Table S5.
3.3 Changes from baseline in total nasal symptom score in seasonal allergic rhinitis
The TNSS outcome was available in 12 SAR studies involving 5 INCSs (Figure 2A). MF, FF, CIC, FP, and TAA, significantly had superior efficacy to placebo with small treatment effects [SMD −0.47 (95% CI: −0.63 to −0.31), −0.46 (95% CI: −0.59 to −0.33), −0.44 (95% CI: −0.75 to −0.13), −0.42 (95% CI: −0.67 to −0.17), and −0.41 (95% CI: −0.81 to −0.00), respectively] (Table 2; Figure 3A). Based on SUCRA, MF was ranked the highest efficacy, followed by FF, CIC, FP, and TAA, respectively (Supplementary Figure S3A).
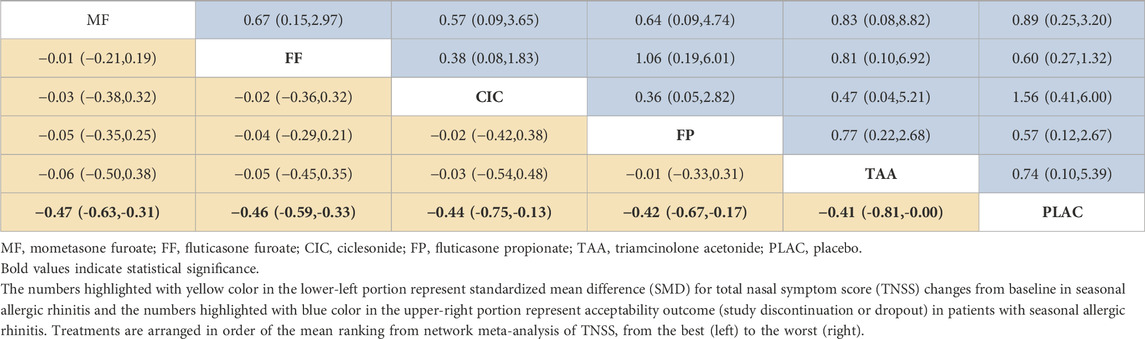
TABLE 2. League table of efficacy measured by standardized mean difference for total nasal symptom score changes from baseline and acceptability outcome in patients with seasonal allergic rhinitis.
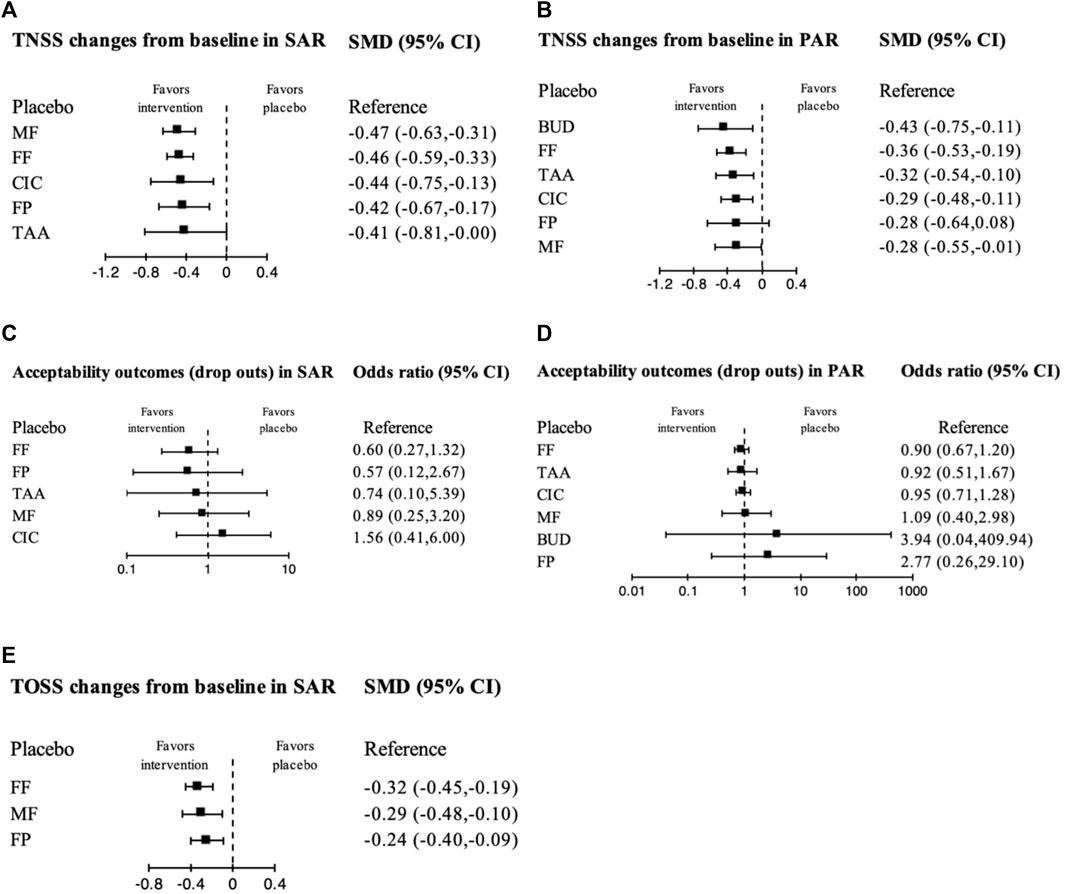
FIGURE 3. Forest plot showing network meta-analysis results of all treatment options compared with placebo using randomized controlled trials. The following figures show the effect sizes (standardized mean difference, SMD) of each treatment compared to the placebo and are presented separately according to the measured outcomes. (A), Total nasal symptom score (TNSS) changes from baseline in seasonal allergic rhinitis (SAR); (B), TNSS changes from baseline in perennial allergic rhinitis (PAR); (C), Acceptability in SAR; (D), Acceptability in PAR; (E), Total ocular symptom score (TOSS) changes from baseline in SAR. CI, Confidence interval; BUD, budesonide; CIC, ciclesonide; FF, fluticasone furoate; FP, fluticasone propionate; MF, mometasone furoate; TAA, triamcinolone acetonide.
3.4 Changes from baseline in total nasal symptom score in perennial allergic rhinitis
The TNSS outcome was available in 12 PAR studies involving 6 INCSs (Figure 2C). BUD, FF, TAA, CIC, and MF, significantly had superior efficacy to placebo with small treatment effects [SMD −0.43 (95% CI: −0.75 to −0.11), −0.36 (95% CI: −0.53 to −0.19), −0.32 (95% CI: −0.54 to −0.10), −0.29 (95% CI: −0.48 to −0.11), and −0.28 (95% CI: −0.55 to −0.01), respectively], while FP had no significant treatment effect compared with placebo [SMD-0.28 (95% CI: −0.64 to 0.08)] (Table 3; Figure 3B). Based on SUCRA, BUD was ranked the highest efficacy, followed by FF, TAA, CIC, and MF (Supplementary Figure S3B).
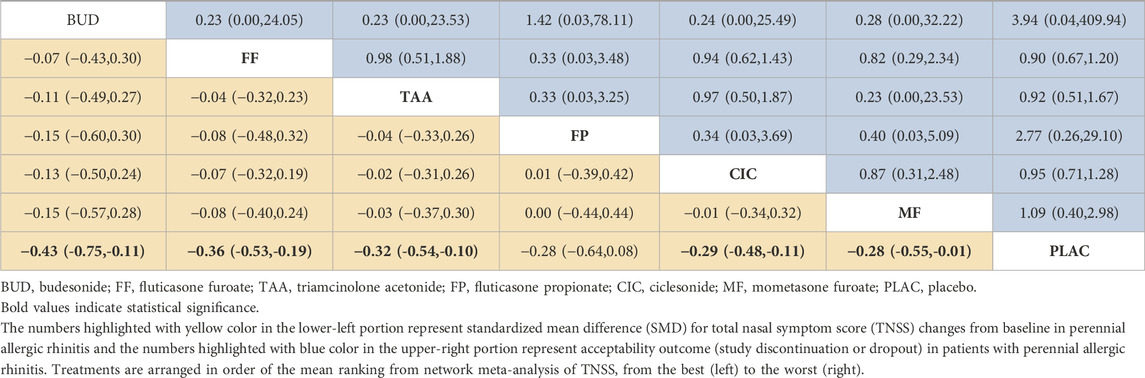
TABLE 3. League table of efficacy measured by standardized mean difference for total nasal symptom score changes from baseline and acceptability outcome in patients with perennial allergic rhinitis.
3.5 Changes from baseline in total ocular symptom score
Six SAR studies (Fokkens et al., 2007; Kaiser et al., 2007; Jacobs et al., 2009; Prenner et al., 2010; Igarashi et al., 2012; Ratner et al., 2015) involving 3 INCSs provided TOSS outcomes for NMA (Supplementary Figure S4A). FF, MF, and FP significantly improved TOSS with small treatment effects compared with the placebo [SMD -0.32 (95% CI: −0.45 to −0.19), −0.29 (95% CI: −0.48 to −0.10), and −0.24 (95% CI: −0.40 to −0.09), respectively] (Supplementary Table S6 and Figure 3E). Based on SUCRA, FF was ranked the highest efficacy, followed by MF and FP (Figure 3E and Supplementary Figure S4B).
3.6 Acceptability of treatments
Networks for acceptability outcomes in SAR and PAR are illustrated in Figures 2B, D. An assessment of 10 SAR studies (Bronsky et al., 1996; Meltzer et al., 1998; Gross et al., 2002; Berger et al., 2003; Gawchik et al., 2003; Ratner et al., 2006; Fokkens et al., 2007; Kaiser et al., 2007; Andrews et al., 2009; Meltzer et al., 2011) and 11 PAR studies (Kobayashi et al., 1995; Tai and Wang, 2003; Chervinsky et al., 2007; Meltzer et al., 2007; Rosenblut et al., 2007; Vasar et al., 2008; Weinstein et al., 2009; Baena-Cagnani and Patel, 2010; Given et al., 2010; Meltzer et al., 2010; Karaulov et al., 2019) for the acceptability of treatments found that all INCSs were comparable to placebo in acceptability outcome without statistical significance (Table 2; Table 3; Figures 3C, D). Based on SUCRA, The ranking in treatment acceptability in SAR and PAR is shown in Supplementary Figure S3C and Supplementary Figure S3D, respectively.
3.7 Hierarchical cluster analysis
The SUCRA values for treatment efficacy in improving the TNSS, TOSS, and acceptability by the patient were used in the hierarchical cluster analysis. Regarding SAR (Figure 4A), FF, FP, MF, and TAA were classified into groups with high efficacy and acceptability, with FF and FP being equivalent in both outcomes. CIC had high efficacy but the lowest acceptability. Regarding PAR (Figure 4B), CIC, FF, MF, and TAA were classified into groups with high efficacy and acceptability. FP also had high efficacy but low acceptability. BUD had the highest efficacy in PAR but had low acceptability, with FP being the lowest SUCRA for acceptability. Regarding TOSS (Supplementary Figure S4B), FF, FP, and MF had high efficacy and high acceptability, with FF being the highest in both outcomes.
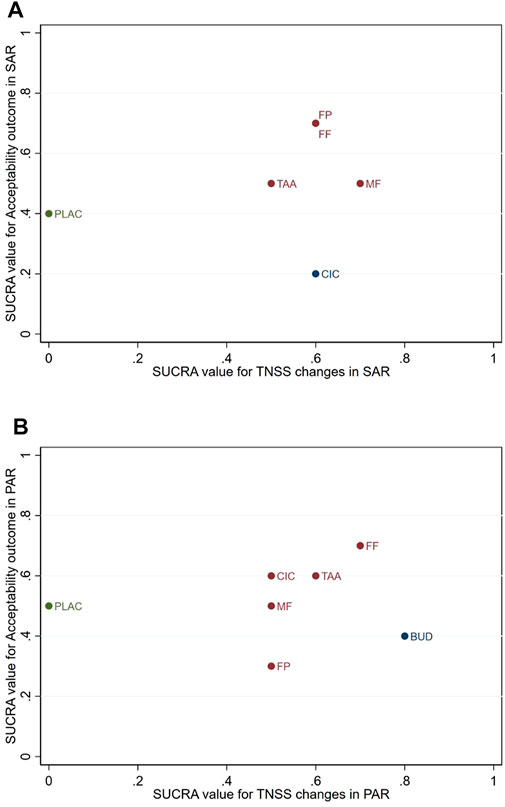
FIGURE 4. Cluster ranking based on the surface under the cumulative ranking (SUCRA) for changes in the total nasal symptom score (TNSS) from baseline and acceptability outcome via any cause of dropout in patients with (A), seasonal allergic rhinitis (SAR), and (B), perennial allergic rhinitis (PAR). BUD, budesonide; CIC, ciclesonide; FF, fluticasone furoate; FP, fluticasone propionate; MF, mometasone furoate; PLAC, placebo; TAA, triamcinolone acetonide.
3.8 Subgroup analyses and sensitivity analyses
The results of the sensitivity analyses are shown in Supplementary Table S7. Concerning the TNSS changes in SAR, MF was ranked with the highest efficacy, followed by FF in the primary analysis of 12 studies. By excluding one study (n = 11) with a small sample size and a significant risk of bias (Igarashi et al., 2012), both MF and FF became the first rank. In contrast, by excluding one study with SD imputation (Meltzer et al., 2011), FF became the highest efficacy, followed by MF. The results in the leave-one-out sensitivity analysis also went in the same direction and magnitude of effect estimates.
Regarding the TNSS changes in PAR, BUD was ranked with the highest efficacy, followed by FF and TAA in the primary analysis of 12 studies. By excluding two with a significant risk of bias (Chervinsky et al., 2007; Vasar et al., 2008), and two studies with a small sample size (Tai and Wang, 2003; Meltzer et al., 2010), BUD remained in the first rank. In contrast, by excluding three studies in children (Fokkens et al., 2002; Weinstein et al., 2009; Baena-Cagnani and Patel, 2010), MF became the first rank, followed by TAA. However, the leave-one-out sensitivity analysis results were consistent with the primary analysis.
Concerning the TOSS changes in SAR, FF was ranked with the highest efficacy, followed by MF and FP in the primary analysis of 6 studies. The results remained consistent with the primary analysis by excluding one study with a small sample size (Igarashi et al., 2012).
3.9 Heterogeneity, inconsistency, transitivity, publication bias, and strength of evidence
From the results of the pairwise meta-analysis, there was some evidence of moderate-to-high statistical heterogeneity among included studies, especially in the treatment outcomes of TNSS and TOSS changes (Supplementary Table S8 and Supplementary Table S9). Evidence of inconsistency between direct and indirect evidence was not identified from the global design-by-treatment interaction model and 2 loops of treatment efficacy (Supplementary Table S10A, B). No significant evidence of asymmetry was found in the analysis of comparison-adjusted funnel plots (Supplementary Figure S5). We graded the strength of evidence for the synthesized NMA estimates by considering all relevant domains and assumptions. Most placebo-controlled studies were rated as having a moderate quality of evidence, while active-controlled studies were rated as having very low to low quality of evidence for the TNSS outcomes in SAR and PAR. The grading summary is provided separately for placebo-controlled and active-controlled comparisons in Supplementary Table S11 and Supplementary Table S12.
4 Discussion
4.1 Summary of main findings
The present NMA included 26 studies, 13 with 5,134 SAR patients and 13 with 4,393 PAR patients. Most studies were placebo-controlled trials with moderate quality of evidence. In SAR, MF was ranked the highest efficacy in improving TNSS, followed by FF, CIC, FP, and TAA. In PAR, BUD was ranked the highest efficacy in improving TNSS, followed by FF, TAA, CIC, and MF. FF was ranked the highest efficacy in improving TOSS in SAR, followed by MF and FP. The acceptability of all included INCSs was not inferior to the placebo.
Some INCSs were missing in this NMA because no BDP studies in PAR, BUD studies in SAR, and flunisolide studies in both SAR and PAR met our inclusion criteria. Two BDP studies in SAR were included in the qualitative analysis, but there was no sufficient data for NMA (Ratner et al., 1992; Lumry et al., 2003). However, those 2 studies showed that BDP was as effective as FP and TAA. Our methodology requires a 2-week and 4-week study duration for SAR and PAR to be consistent with the USFDA guidance for conducting INCS trials (United States Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER), 2018). Including patients with moderate-to-severe AR corresponds to an indication of INCS recommended by the standard guideline (United States Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER), 2018; Bousquet et al., 2020; Dykewicz et al., 2020). Excluding patients with mild AR would help distinguish the efficacy among INCSs since any INCSs may be effective in AR with mild severity, irrespective of their pharmacological profiles. Although the visual analog scale has recently become popular for grading AR severity, it was clearly shown to correlate well with TNSS used in our study (Klimek et al., 2017). These robust prespecified criteria allowed us to assure the transitivity of the network, minimize heterogeneity and enhance the applicability of the results to clinical practice.
Concerning the comparative efficacy, all INCSs were superior to placebo in either SAR or PAR or both. However, those INCSs showed an improvement in TNSS and TOSS with a small treatment effect compared with placebo, reflecting their similar efficacy. In addition, 8 out of 32 studies comparing FF VS FP (Okubo et al., 2009), FP VS TAA (Gross et al., 2002; Berger et al., 2003; Meltzer et al., 2004; Karaulov et al., 2019), BDP VS TAA (Lumry et al., 2003), BDP VS FP (Ratner et al., 1992), and BUD VS FP (Tai and Wang, 2003) demonstrated the equivalent efficacy between each paired comparison. These findings suggest that the licensed dose of any INCSs is sufficient to control allergic inflammation, irrespective of their different pharmacological profiles. Nevertheless, in our NMA, FP failed to show superior efficacy to placebo in PAR because no placebo-controlled FP studies agreed with our prespecified inclusion criteria. The indirect comparison results came from two active-controlled studies comparing FP VS TAA (n = 260) (Karaulov et al., 2019) and FP VS BUD (n = 24) (Tai and Wang, 2003) in PAR. Although FP was as efficacious as its comparators in those two studies, a limited number of studies with insufficient sample size may, at least in part, account for its insignificant efficacy compared with a placebo.
Apart from efficacy, safety is also crucial for choosing an INCS. Using standard-dose INCSs is usually safe for the adult population (Donaldson et al., 2020). In contrast, some INCSs, including BDP, TAA, and FF, had evidence of long-term effects on growth retardation in children (Skoner et al., 2000; Lee et al., 2014; Skoner et al., 2015). Another factor concerning INCS selection is patient preference and satisfaction, which could be affected by odor, taste, types of delivery devices, and cost (Sher and Ross, 2014). Patient-physician interaction to understand the differences among INCS products is essential to accomplish the treatment of AR.
4.2 Strengths and limitations
The primary strength of our study was the use of strict inclusion criteria in scoping the domain of patients and the timing of outcome measurement to ensure that all included RCTs were homogeneous enough to address our specific clinical questions. However, our study carries some limitations. First, a limited number of RCTs were included for each specific outcome. Some studies could not be included due to the stringent inclusion criteria. Thus, statistical significance among head-to-head comparisons could not be demonstrated, and the ranking sequence might be alternated by chance. We suggested that the interpretation of results should not be weighted entirely on the statistical significance and SUCRA but on the magnitude of the effect estimates and the certainty of evidence, which takes into account multiple aspects affecting the credibility of the results (e.g., the heterogeneity between each pairwise comparison, the imprecision of the estimates, and the inconsistency between the direct and indirect evidence) (Brignardello-Petersen et al., 2018). Second, there was an insufficient number of studies in each comparative pair to evaluate the source of heterogeneity using meta-regression or subgroup analysis. Third, new evidence after concluding the database search in March 2022 might have been reported so far.
Conclusion
According to our NMA, MF was ranked the highest efficacy in improving TNSS in SAR, followed by FF, CIC, FP, and TAA. BUD was ranked the highest efficacy in improving TNSS in PAR, followed by FF, TAA, CIC, and MF. FF was ranked the highest efficacy in improving TOSS in SAR, followed by MF and FP. In addition to efficacy, other factors, including safety, cost, patient preference, and education, should be considered to improve long-term adherence and achieve AR control.
Author contributions
TT conceived the original concept of the project. PP is an essentially intellectual contributor of this manuscript. KS, SN, PP, and TT designed and drafted the study protocol. KS and TK screened all retrieved records from database searching to determine the eligible studies. KS and CP extracted data, and KS and TK assessed the risk of bias from included studies. PP and TT supervised the data extraction and risk-of-bias assessment. KS and PP performed the statistical analyses. KS, PP, and TT drafted the manuscript. TT had the final decision to submit for publication. TT attests that all listed authors meet authorship criteria, and none meeting the criteria have been omitted. All authors contributed to the article and approved the submitted version.
Funding
This study was partially supported by the Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand, and the Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
Conflict of interest
KS, TK, CP, SN, and PP: None. TT: received honoraria for scientific lectures from A. Menarini, Astra-Zeneca, GSK, Novartis, P&G, Sanofi, Takeda, and Viatris; research supports from Abbott, Sanofi, and Viatris; served on the advisory board for Sanofi and Viatris.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1184552/full#supplementary-material
References
Andrews, C. P., Martin, B. G., Jacobs, R. L., Mohar, D. E., Diaz, J. D., Amar, N. J., et al. (2009). Fluticasone furoate nasal spray is more effective than fexofenadine for nighttime symptoms of seasonal allergy. Allergy Asthma Proc. 30 (2), 128–138. doi:10.2500/aap.2009.30.3204
Baena-Cagnani, C. E., and Patel, P. (2010). Efficacy and long-term safety of mometasone furoate nasal spray in children with perennial allergic rhinitis. Curr. Med. Res. Opin. 26 (9), 2047–2055. doi:10.1185/03007995.2010.487661
Berger, W. E., Kaiser, H., Gawchik, S. M., Tillinghast, J., Woodworth, T. H., Dupclay, L., et al. (2003). Triamcinolone acetonide aqueous nasal spray and fluticasone propionate are equally effective for relief of nasal symptoms in patients with seasonal allergic rhinitis. Otolaryngol. Head. Neck Surg. 129 (1), 16–23. doi:10.1016/s0194-5998(03)00526-6
Bousquet, J., Schunemann, H. J., Togias, A., Bachert, C., Erhola, M., Hellings, P. W., et al. (2020). Next-generation allergic rhinitis and its impact on asthma (ARIA) guidelines for allergic rhinitis based on grading of recommendations assessment, development and evaluation (GRADE) and real-world evidence. J. Allergy Clin. Immunol. 145 (1), 70–80.e3. doi:10.1016/j.jaci.2019.06.049
Brignardello-Petersen, R., Johnston, B. C., Jadad, A. R., and Tomlinson, G. (2018). Using decision thresholds for ranking treatments in network meta-analysis results in more informative rankings. J. Clin. Epidemiol. 98, 62–69. doi:10.1016/j.jclinepi.2018.02.008
Bronsky, E. A., Dockhorn, R. J., Meltzer, E. O., Shapiro, G., Boltansky, H., LaForce, C., et al. (1996). Fluticasone propionate aqueous nasal spray compared with terfenadine tablets in the treatment of seasonal allergic rhinitis. J. Allergy Clin. Immunol. 97 (4), 915–921. doi:10.1016/s0091-6749(96)80065-0
Chaimani, A., Caldwell, D. M., Li, T., Higgins, J. P. T., and Salanti, G. (2019). “Chapter 11: Undertaking network meta-analyses,” in Cochrane Handbook for systematic reviews of interventions. Editors J. P. T. Higgins, J. Thomas, J. Chandler, M. Cumpston, T. Li, M. J. Pageet al. (Chichester, UK: John Wiley & Sons).
Chaimani, A., Higgins, J. P., Mavridis, D., Spyridonos, P., and Salanti, G. (2013). Graphical tools for network meta-analysis in STATA. PLoS One 8 (10), e76654. doi:10.1371/journal.pone.0076654
Chaimani, A., and Salanti, G. (2012). Using network meta-analysis to evaluate the existence of small-study effects in a network of interventions. Res. Synth. Methods 3 (2), 161–176. doi:10.1002/jrsm.57
Chaimani, A., Salanti, G., Leucht, S., Geddes, J. R., and Cipriani, A. (2017). Common pitfalls and mistakes in the set-up, analysis and interpretation of results in network meta-analysis: What clinicians should look for in a published article. Evid. Based Ment. Health 20 (3), 88–94. doi:10.1136/eb-2017-102753
Chervinsky, P., Kunjibettu, S., Miller, D. L., Prenner, B. M., Raphael, G., Hall, N., et al. (2007). Long-term safety and efficacy of intranasal ciclesonide in adult and adolescent patients with perennial allergic rhinitis. Ann. Allergy Asthma Immunol. 99 (1), 69–76. doi:10.1016/S1081-1206(10)60624-2
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. 2nd ed. New York, NY: Routledge.
Derendorf, H., and Meltzer, E. O. (2008). Molecular and clinical pharmacology of intranasal corticosteroids: Clinical and therapeutic implications. Allergy 63 (10), 1292–1300. doi:10.1111/j.1398-9995.2008.01750.x
DerSimonian, R., and Laird, N. (1986). Meta-analysis in clinical trials. Control Clin. Trials 7 (3), 177–188. doi:10.1016/0197-2456(86)90046-2
Donaldson, A. M., Choby, G., Kim, D. H., Marks, L. A., and Lal, D. (2020). Intranasal corticosteroid therapy: Systematic review and meta-analysis of reported safety and adverse effects in adults. Otolaryngol. Head. Neck Surg. 163 (6), 1097–1108. doi:10.1177/0194599820931455
Dykewicz, M. S., Wallace, D. V., Amrol, D. J., Baroody, F. M., Bernstein, J. A., Craig, T. J., et al. (2020). Rhinitis 2020: A practice parameter update. J. Allergy Clin. Immunol. 146 (4), 721–767. doi:10.1016/j.jaci.2020.07.007
Fokkens, W. J., Cserhati, E., dos Santos, J. M., Praca, F., van Zanten, M., Schade, A., et al. (2002). Budesonide aqueous nasal spray is an effective treatment in children with perennial allergic rhinitis, with an onset of action within 12 hours. Ann. Allergy Asthma Immunol. 89 (3), 279–284. doi:10.1016/s1081-1206(10)61955-2
Fokkens, W. J., Jogi, R., Reinartz, S., Sidorenko, I., Sitkauskiene, B., van Oene, C., et al. (2007). Once daily fluticasone furoate nasal spray is effective in seasonal allergic rhinitis caused by grass pollen. Allergy 62 (9), 1078–1084. doi:10.1111/j.1398-9995.2007.01522.x
Friedrich, J. O., Adhikari, N. K., and Beyene, J. (2007). Inclusion of zero total event trials in meta-analyses maintains analytic consistency and incorporates all available data. BMC Med. Res. Methodol. 7, 5. doi:10.1186/1471-2288-7-5
Gawchik, S., Goldstein, S., Prenner, B., and John, A. (2003). Relief of cough and nasal symptoms associated with allergic rhinitis by mometasone furoate nasal spray. Ann. Allergy Asthma Immunol. 90 (4), 416–421. doi:10.1016/S1081-1206(10)61826-1
Given, J. T., Cheema, A. S., Dreykluft, T., Stillerman, A., Silvey, M., Wu, W., et al. (2010). Fluticasone furoate nasal spray is effective and well tolerated for perennial allergic rhinitis in adolescents and adults. Am. J. Rhinol. Allergy 24 (6), 444–450. doi:10.2500/ajra.2010.24.3534
Gross, G., Jacobs, R. L., Woodworth, T. H., Georges, G. C., and Lim, J. C. (2002). Comparative efficacy, safety, and effect on quality of life of triamcinolone acetonide and fluticasone propionate aqueous nasal sprays in patients with fall seasonal allergic rhinitis. Ann. Allergy Asthma Immunol. 89 (1), 56–62. doi:10.1016/S1081-1206(10)61911-4
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327 (7414), 557–560. doi:10.1136/bmj.327.7414.557
Higgins, J. P. T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2019) 2nd ed (Chichester: Wiley).Cochrane handbook for systematic reviews of interventions
Hutton, B., Salanti, G., Caldwell, D. M., Chaimani, A., Schmid, C. H., Cameron, C., et al. (2015). The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern Med. 162 (11), 777–784. doi:10.7326/M14-2385
Igarashi, T., Nakazato, Y., Kunishige, T., Fujita, M., Yamada, Y., Fujimoto, C., et al. (2012). Mometasone furoate nasal spray relieves the ocular symptoms of seasonal allergic rhinoconjunctivitis. J. Nippon. Med. Sch. 79 (3), 182–189. doi:10.1272/jnms.79.182
Jacobs, R., Martin, B., Hampel, F., Toler, W., Ellsworth, A., and Philpot, E. (2009). Effectiveness of fluticasone furoate 110 microg once daily in the treatment of nasal and ocular symptoms of seasonal allergic rhinitis in adults and adolescents sensitized to mountain cedar pollen. Curr. Med. Res. Opin. 25 (6), 1393–1401. doi:10.1185/03007990902890512
Kaiser, H. B., Naclerio, R. M., Given, J., Toler, T. N., Ellsworth, A., and Philpot, E. E. (2007). Fluticasone furoate nasal spray: A single treatment option for the symptoms of seasonal allergic rhinitis. J. Allergy Clin. Immunol. 119 (6), 1430–1437. doi:10.1016/j.jaci.2007.02.022
Karaulov, A. V., Vylegzhanina, T., Ovchinnikov, A., Chernikova, M., and Nenasheva, N. (2019). Triamcinolone acetonide versus fluticasone propionate in the treatment of perennial allergic rhinitis: A randomized, parallel-group trial. Int. Arch. Allergy Immunol. 179 (2), 142–151. doi:10.1159/000497160
Klimek, L., Bergmann, K. C., Biedermann, T., Bousquet, J., Hellings, P., Jung, K., et al. (2017). Visual analogue scales (VAS): Measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care: Position paper of the German society of allergology (AeDA) and the German society of allergy and clinical immunology (DGAKI), ENT section, in collaboration with the working group on clinical immunology, allergology and environmental medicine of the German society of otorhinolaryngology, head and neck surgery (DGHNOKHC). Allergo J. Int. 26 (1), 16–24. doi:10.1007/s40629-016-0006-7
Kobayashi, R. H., Beaucher, W. N., Koepke, J. W., Luskin, A., Ransom, J. H., Rosen, J. P., et al. (1995). Triamcinolone acetonide aqueous nasal spray for the treatment of patients with perennial allergic rhinitis: A multicenter, randomized, double-blind, placebo-controlled study. Clin. Ther. 17 (3), 503–513. doi:10.1016/0149-2918(95)80115-4
Lee, L. A., Sterling, R., Maspero, J., Clements, D., Ellsworth, A., and Pedersen, S. (2014). Growth velocity reduced with once-daily fluticasone furoate nasal spray in prepubescent children with perennial allergic rhinitis. J. Allergy Clin. Immunol. Pract. 2 (4), 421–427. doi:10.1016/j.jaip.2014.04.008
Lemieux, J., Beaton, D. E., Hogg-Johnson, S., Bordeleau, L. J., and Goodwin, P. J. (2007). Three methods for minimally important difference: No relationship was found with the net proportion of patients improving. J. Clin. Epidemiol. 60 (5), 448–455. doi:10.1016/j.jclinepi.2006.08.006
Lu, G., and Ades, A. E. (2004). Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 23 (20), 3105–3124. doi:10.1002/sim.1875
Lumry, W., Hampel, F., LaForce, C., Kiechel, F., and el-Akkad, T. (2003). A comparison of once-daily triamcinolone acetonide aqueous and twice-daily beclomethasone dipropionate aqueous nasal sprays in the treatment of seasonal allergic rhinitis. Allergy Asthma Proc. 24 (3), 203–210.
Luo, D., Wan, X., Liu, J., and Tong, T. (2018). Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 27 (6), 1785–1805. doi:10.1177/0962280216669183
Meltzer, E. O., Gallet, C. L., Jalowayski, A. A., Garcia, J., Diener, P., Liao, Y., et al. (2004). Triamcinolone acetonide and fluticasone propionate aqueous nasal sprays significantly improve nasal airflow in patients with seasonal allergic rhinitis. Allergy Asthma Proc. 25 (1), 53–58.
Meltzer, E. O., Jalowayski, A. A., Orgel, H. A., and Harris, A. G. (1998). Subjective and objective assessments in patients with seasonal allergic rhinitis: Effects of therapy with mometasone furoate nasal spray. J. Allergy Clin. Immunol. 102 (1), 39–49. doi:10.1016/s0091-6749(98)70053-3
Meltzer, E. O., Kunjibettu, S., Hall, N., Wingertzahn, M. A., Murcia, C., Berger, W., et al. (2007). Efficacy and safety of ciclesonide, 200 microg once daily, for the treatment of perennial allergic rhinitis. Ann. Allergy Asthma Immunol. 98 (2), 175–181. doi:10.1016/s1081-1206(10)60693-x
Meltzer, E. O., Munafo, D. A., Chung, W., Gopalan, G., and Varghese, S. T. (2010). Intranasal mometasone furoate therapy for allergic rhinitis symptoms and rhinitis-disturbed sleep. Ann. Allergy Asthma Immunol. 105 (1), 65–74. doi:10.1016/j.anai.2010.04.020
Meltzer, E. O., Shekar, T., and Teper, A. A. (2011). Mometasone furoate nasal spray for moderate-to-severe nasal congestion in subjects with seasonal allergic rhinitis. Allergy Asthma Proc. 32 (2), 159–167. doi:10.2500/aap.2011.32.3424
Mills, E. J., Thorlund, K., and Ioannidis, J. P. (2013). Demystifying trial networks and network meta-analysis. BMJ 346, f2914. doi:10.1136/bmj.f2914
Mygind, N. (1973). Local effect of intranasal beclomethasone dipropionate aerosol in hay fever. Br. Med. J. 4 (5890), 464–466. doi:10.1136/bmj.4.5890.464
Nathan, R. A., Berger, W., Yang, W., Cheema, A., Silvey, M., Wu, W., et al. (2008). Effect of once-daily fluticasone furoate nasal spray on nasal symptoms in adults and adolescents with perennial allergic rhinitis. Ann. Allergy Asthma Immunol. 100 (5), 497–505. doi:10.1016/S1081-1206(10)60477-2
Okubo, K., Nakashima, M., Miyake, N., Komatsubara, M., and Okuda, M. (2009). Comparison of fluticasone furoate and fluticasone propionate for the treatment of Japanese cedar pollinosis. Allergy Asthma Proc. 30 (1), 84–94. doi:10.2500/aap.2009.30.3182
Prenner, B. M., Lanier, B. Q., Bernstein, D. I., Shekar, T., and Teper, A. (2010). Mometasone furoate nasal spray reduces the ocular symptoms of seasonal allergic rhinitis. J. Allergy Clin. Immunol. 125 (6), 1247–1253. doi:10.1016/j.jaci.2010.03.004
Puhan, M. A., Schunemann, H. J., Murad, M. H., Li, T., Brignardello-Petersen, R., Singh, J. A., et al. (2014). A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 349, g5630. doi:10.1136/bmj.g5630
Ratner, P. H., Paull, B. R., Findlay, S. R., Hampel, F., Martin, B., Kral, K. M., et al. (1992). Fluticasone propionate given once daily is as effective for seasonal allergic rhinitis as beclomethasone dipropionate given twice daily. J. Allergy Clin. Immunol. 90 (3), 285–291. doi:10.1016/s0091-6749(05)80005-3
Ratner, P. H., Wingertzahn, M. A., van Bavel, J. H., Hampel, F., Darken, P. F., and Shah, T. (2006). Efficacy and safety of ciclesonide nasal spray for the treatment of seasonal allergic rhinitis. J. Allergy Clin. Immunol. 118 (5), 1142–1148. doi:10.1016/j.jaci.2006.07.050
Ratner, P., Van Bavel, J., Mohar, D., Jacobs, R. L., Hampel, F., Howland, W., et al. (2015). Efficacy of daily intranasal fluticasone propionate on ocular symptoms associated with seasonal allergic rhinitis. Ann. Allergy Asthma Immunol. 114 (2), 141–147. doi:10.1016/j.anai.2014.11.012
Rosenblut, A., Bardin, P. G., Muller, B., Faris, M. A., Wu, W. W., Caldwell, M. F., et al. (2007). Long-term safety of fluticasone furoate nasal spray in adults and adolescents with perennial allergic rhinitis. Allergy 62 (9), 1071–1077. doi:10.1111/j.1398-9995.2007.01521.x
Rouse, B., Chaimani, A., and Li, T. (2017). Network meta-analysis: An introduction for clinicians. Intern Emerg. Med. 12 (1), 103–111. doi:10.1007/s11739-016-1583-7
Rucker, G., and Schwarzer, G. (2015). Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med. Res. Methodol. 15, 58. doi:10.1186/s12874-015-0060-8
Sterne, J. A. C., Savovic, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., et al. (2019). RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898. doi:10.1136/bmj.l4898
Salanti, G. (2012). Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: Many names, many benefits, many concerns for the next generation evidence synthesis tool. Res. Synth. Methods 3 (2), 80–97. doi:10.1002/jrsm.1037
Sher, E. R., and Ross, J. A. (2014). Intranasal corticosteroids: The role of patient preference and satisfaction. Allergy Asthma Proc. 35 (1), 24–33. doi:10.2500/aap.2014.35.3725
Skoner, D. P., Berger, W. E., Gawchik, S. M., Akbary, A., and Qiu, C. (2015). Intranasal triamcinolone and growth velocity. Pediatrics 135 (2), e348–e356. doi:10.1542/peds.2014-1641
Skoner, D. P., Rachelefsky, G. S., Meltzer, E. O., Chervinsky, P., Morris, R. M., Seltzer, J. M., et al. (2000). Detection of growth suppression in children during treatment with intranasal beclomethasone dipropionate. Pediatrics 105 (2), E23. doi:10.1542/peds.105.2.e23
Tai, C. J., and Wang, P. C. (2003). Comparisons of two intranasal corticosteroid preparations in treating allergic rhinitis. Otolaryngol. Head. Neck Surg. 129 (5), 518–525. doi:10.1016/s0194-5998(03)01449-9
U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER) (2018). Allergic rhinitis: Developing drug products for treatment guidance for industry. Maryland. Available at: https://www.fda.gov/files/drugs/published/Allergic-Rhinitis–Developing-Drug-Products-for-Treatment-Guidance-for-Industry.pdf (Accessed September 6, 2022).
van Bavel, J., Findlay, S. R., Hampel, F. C., Martin, B. G., Ratner, P., and Field, E. (1994). Intranasal fluticasone propionate is more effective than terfenadine tablets for seasonal allergic rhinitis. Arch. Intern Med. 154 (23), 2699–2704. doi:10.1001/archinte.1994.00420230086010
Vasar, M., Houle, P. A., Douglass, J. A., Meltzer, E. O., Silvey, M., Wu, W., et al. (2008). Fluticasone furoate nasal spray: Effective monotherapy for symptoms of perennial allergic rhinitis in adults/adolescents. Allergy Asthma Proc. 29 (3), 313–321. doi:10.2500/aap.2008.29.3126
Veroniki, A. A., Vasiliadis, H. S., Higgins, J. P., and Salanti, G. (2013). Evaluation of inconsistency in networks of interventions. Int. J. Epidemiol. 42 (1), 332–345. doi:10.1093/ije/dys222
Wan, X., Wang, W., Liu, J., and Tong, T. (2014). Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 14, 135. doi:10.1186/1471-2288-14-135
Weinstein, S., Qaqundah, P., Georges, G., and Nayak, A. (2009). Efficacy and safety of triamcinolone acetonide aqueous nasal spray in children aged 2 to 5 years with perennial allergic rhinitis: A randomized, double-blind, placebo-controlled study with an open-label extension. Ann. Allergy Asthma Immunol. 102 (4), 339–347. doi:10.1016/S1081-1206(10)60340-7
Keywords: acceptability, allergic rhinitis, efficacy, intranasal corticosteroid, meta-analysis, systematic review, total nasal symptom score, total ocular symptom score
Citation: Soe KK, Krikeerati T, Pheerapanyawaranun C, Niyomnaitham S, Phinyo P and Thongngarm T (2023) Comparative efficacy and acceptability of licensed dose intranasal corticosteroids for moderate-to-severe allergic rhinitis: a systematic review and network meta-analysis. Front. Pharmacol. 14:1184552. doi: 10.3389/fphar.2023.1184552
Received: 12 March 2023; Accepted: 09 May 2023;
Published: 23 May 2023.
Edited by:
Mauro Maniscalco, Fondazione Salvatore Maugeri (IRCCS), ItalyReviewed by:
Corrado Pelaia, Magna Græcia University, ItalyClaudio Candia, University of Naples Federico II, Italy
Antonio Molino, University of Naples Federico II, Italy
Copyright © 2023 Soe, Krikeerati, Pheerapanyawaranun, Niyomnaitham, Phinyo and Thongngarm. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Torpong Thongngarm, dG9yYWxsZXJneUBnbWFpbC5jb20=