 Chaoqun Song1
Chaoqun Song1 Zheng Nan
Zheng Nan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol., 05 July 2023
Sec. Ethnopharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1180751
This article is part of the Research TopicNatural Products in the Treatment of Hyperuricemia, Gout and other Metabolic DisordersView all 8 articles
Background: Diabetic nephropathy (DN) is the main cause of chronic kidney disease (CKD) and end-stage renal failure (ESRF), and the control of disease progression and adverse events during treatment needs to be improved.
Objective: This study aimed to systematically evaluate the clinical efficacy and safety of Niaoduqing granules (NDQG) in the treatment of diabetic kidney disease (DKD).
Method: Randomized controlled trials (RCTs) of NDQG for DKD from Chinese and English databases up to 31 August 2022 were included. The quality of the literature was assessed using the risk of bias tool of the Cochrane Handbook. At a 95% confidence interval (CI), relative risk (RR) and Cohen’s d were used for the categorical and continuous variables, respectively, and Stata 16.0 software was used for statistical analysis. A funnel plot and Egger’s tests were used to assess publication bias.
Result: A total of 4,006 patients were included in 52 RCTs, including 1,987 cases in the control group and 2,019 cases in the treatment group. Compared with conventional treatment (CT), combined NDQG therapy is more effective in improving clinical efficiency [RR = 1.23, 95% confidence interval (1.17, 1.29), p < 0.001, I2 = 53.17%], kidney function (urinary albumin excretion rate [SMD = −0.90, 95% CI (−1.14, −0.66), p < 0.001, I2 = 78.19%], 24hUTP levels [SMD = −0.81, 95% CI (−1.08, −0.55), p < 0.001, I2 = 87.08%], blood urea nitrogen [SMD = −0.54, 95% CI (−0.69, −0.39), p < 0.01, I2 = 77.01%], SCr [SMD = −0.68, 95% CI (−0.90, −0.45), p < 0.001, I2 = 89.97%], CCr [SMD = 0.76, 95% CI (0.10,1.42), p = 0.02, I2 = 95.97%], and Cys-C [SMD = −1.32, 95% CI (−2.25, −0.40), p = 0.01, I2 = 93.44%]), the level of glucose metabolism (fasting blood glucose [SMD = −0.18, 95% CI (−0.38, 0.03), p = 0.10, I2 = 71.18%] and HbA1c [SMD = −0.42, 95% CI (−0.86, −0.02), p = 0.06, I2 = 81.64%]), the level of lipid metabolism (total cholesterol [SMD = −0.70, 95% CI (−1.01, −0.39), p < 0.001, I2 = 86.74%] and triglyceride [SMD = −0.61, 95% CI (−0.87,−0.36), p < 0.001, I2 = 80.64%]), inflammatory factors (Hs-CRP [SMD = −1.00, 95% CI (−1.54, −0.46), p < 0.001, I2 = 86.81%], IL-18 [SMD = −1.25, 95% CI (−1.58, −0.92), p < 0.001, I2 = 0], and TNF-α [SMD = −1.28, 95% CI (−1.64, −0.91), p < 0.001, I2 = 75.73%]), and indicators of oxidative stress (malondialdehyde [SMD = −0.88, 95% CI (−1.22, −0.54), p < 0.001, I2 = 66.01%] and advanced oxidation protein products [SMD = −0.92, 95% CI (−1.85, 0.00), p < 0.001, I2 = 90.68%]). In terms of improving uric acid [SMD = −1.59, 95% CI (−3.45, 0.27), p = 0.09, I2 = 94.67%], 2hPG [SMD = −0.04, 95% CI (−0.61, 0.53), p = 0.89, I2 = 84.33%], HDL-C [SMD = 0.71, 95% CI (0.02, 1.40), p = 0.04, I2 = 87.43%], Hb [SMD = 0.11, 95% CI (−0.10, 0.32), p = 0.32, I2 = 0.00]), and superoxide dismutase [SMD = 1.32, 95% CI (0.44, 2.20), p < 0.001, I2 = 93.48%], the effect is not obvious. Adjuvant treatment with NDQG did not increase the incidence of adverse reactions in the control group [SMD = 0.98, 95% CI (0.71, 1.34), p = 0.89, I2 = 1.59%]. Obvious publication bias was detected by funnel plot and Egger’s test.
Conclusion: Our meta-analysis showed that adjuvant treatment with NDQG has more advantages than conventional treatment alone in the DKD treatment, which could improve clinical efficiency, kidney function, the level of glucose metabolism, the level of lipid metabolism, inflammatory factors, and oxidative stress indicators. At the same time, it also showed that NDQG are relatively safe. However, more high-quality studies are needed to provide more reliable evidence for clinical use.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022373726, identifier CRD42022373726.
Diabetic kidney disease (DKD) is a chronic microvascular disease secondary to diabetes. DKD is the leading cause of chronic kidney disease (CKD) and end-stage renal failure (ESRF) worldwide (Collaboration, 2020), and DKD-associated CKD or ESRF mortality is higher in patients with CKD or ESRF than in non-DKD patients (Thomas, 2019). According to the data from the International Diabetes Federation in 2021, as of 2021, there are approximately 537 million adult diabetic patients aged 20 to 79, with a prevalence of 10.5%, although only 30%–40% of diabetic patients develop DKD, but it is the main cause of ESRF in most developed countries (Sun et al., 2022). The key features of DKD include persistent proteinuria, mesangial cell proliferation and stromal expansion, glomerulosclerosis, tubulointerstitial fibrosis, podocyte epithelial–mesenchymal transdifferentiation, and autophagy and apoptosis of podocytes (Hernandez et al., 2022). The treatment of DKD is mainly symptomatic treatment such as lowering blood pressure, controlling blood sugar, lowering lipids, improving circulation, and reducing proteinuria, but this does not prevent the progression of the disease, and it is accompanied by many adverse events (Gu et al., 2019). Recently, Traditional Chinese Medicine (TCM) has presented its unique advantages in the treatment of DKD, and previous studies have shown that TCM treatment can improve the clinical symptoms and quality of life of DKD patients, maintain the stability of the condition, and reduce adverse effects (Zhou et al., 2022).
NDQG have been approved by the China State Food and Drug Administration for the treatment of CRF as a compounded Chinese patent medicine and their productive process is under the national drug supervision and administration drug standards [WS3-229 (Z-033)-2000 (Z)], consisting of 16 herbs of TCM—rhubarb (Dahuang, Rheum palmatum L.), milkvetch root (Huangqi, Astragalus mongholicus Bunge [Fabaceae]), liquorice root (Gancao, Glycyrrhiza glabra L.), Largehead Atractylodes Rhizome (Baizhu, Atractylodes macrocephala Koidz.), Poria (Fuling, Smilax glabra Roxb.), Radix Polygoni Multiflori (Heshouwu, Reynoutria multiflora (Thunb.) Moldenke), Sichuan lovage rhizome (Chuanxiong, Conioselinum anthriscoides ‘Chuanxiong’), Chrysanthemum (Juhua, Chrysanthemum indicum L.), Salviae Miltiorrhizae (Danshen, Salvia miltiorrhiza Bunge), Pinellia tuber (Banxia, Pinellia ternata (Thunb.) Makino), Pilose Asiabell root (Dang shen, Codonopsis pilosula (Franch.) Nannf.), white mulberry root-bark (Sangbaipi, Morus alba L.), Sophora japonica (Kushen, Sophora flavescens Aiton), plantain (Cheqiancao, Plantago asiatica L.), white peony root (Baishao, Paeonia lactiflora Pall.), and Chinese thorowax root (Chaihu, Bupleurum falcatum L.)—with the effects of nourishing the kidney and filling essence, strengthening the spleen and dampness, reducing turbidity, activating blood, and removing stasis (Lin and Xu, 2017). In Traditional Chinese Medicine Systems Pharmacology Database and Analysis Platform (http://tcmspw.com/tcmsp.php), the screening criteria was set to DL ≥ 0.18, OB ≥ 30%, Caco-2 ≥ −0.4, and HL ≥ 4 (Zheng et al., 2016) and the drug ingredients were inquired, the composition of which is shown in Supplementary Material S1. As a TCM compound widely used in the treatment of chronic renal failure (CRF), azotemia phase, and early uremia, NDQG has a certain effect on nephrotic syndrome, and no obvious adverse reactions to the heart, liver, intestine, and other organs have been found after long-term medication (Lu et al., 2017), and it shows good efficacy in the prevention and treatment of CKD (10).
There are many clinical studies on the treatment of DKD with NDQG, but there is a lack of evidence-based medical support. This study aimed to investigate the efficacy and safety of NDQG through evidence-based medical approaches.
This systematic review and meta-analysis is the reporting item of choice for systematic reviews and meta-analyses (PRISMA) (Moher et al., 2009) conducted and reported under the guidance of the Cochrane Manual Systematic Review of Interventions Version 6.3 (2022 update). The PRISMA 2020 checklist is provided in Supplementary Material S2. Prior to the start of the 2020 statement, this study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42022373726). Data were derived from published clinical studies.
The search period was from the establishment of the library to 31 August 2022. The three English electronic databases of PubMed, Embase, and the Cochrane Library and the three Chinese electronic databases of CNKI (China National Knowledge Infrastructure), Wanfang Data, and VIP (China Science and Technology Journal Database) were comprehensively searched for RCTs on the treatment of DKD by NDQG, and the search was conducted by combining subject words and free words. The specific search strategies are shown in Table 1.
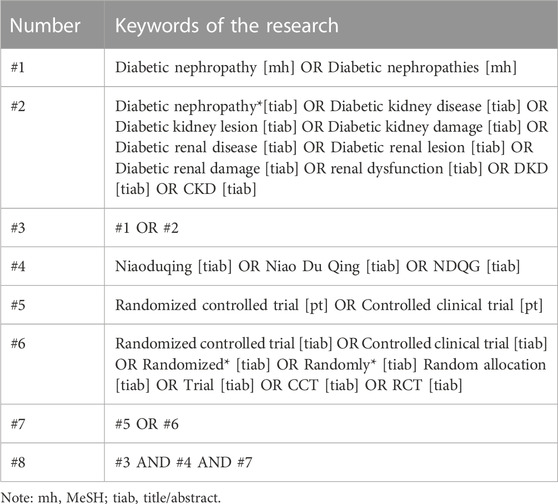
TABLE 1. Specific search strategies.
RCTs of all original studies, irrespective of source or country, published in English or Chinese language only.
Adult (at least 18 years old) patients diagnosed with DKD, regardless of age, gender, and course of the disease.
Placebo or usual treatment in the control group; the treatment group added NDQG to oral treatment on the basis of the same CT as the control group, or the treatment group added NDQG combined with CT. CT includes symptomatic treatment, diabetes health education, diet control, exercise intervention, daily monitoring of blood sugar changes, oral hypoglycemic drugs, insulin, and other classic Western medicine treatment measures.
In order to comprehensively evaluate the efficacy and safety of NDQG for DKD, the clinical efficiency, kidney function, level of glucose metabolism, level of lipid metabolism, Hb, inflammatory factors, oxidative stress indicators, and adverse events were analyzed.
1) Primary outcome: clinical effective rate, urinary albumin excretion rate (UAER), and 24-h urine protein quantification (24UTP).
2) Secondary outcomes: blood urea nitrogen (BUN), serum creatinine concentration (SCr), creatinine clearance rate (CCr), cystatin-c (Cys-C), uric acid (UA), fasting blood glucose (FBG), 2-h postprandial blood glucose (2hPG), glycosylated hemoglobin (HbA1c), total cholesterol (TC), triglyceride (TG), high-density lipid-cholesterol (HDL-C), hemoglobin (Hb), high-sensitivity C-reactive protein (Hs-CRP), interleukin-18 (IL-18), tumor necrosis factor-α (TNF-α), malondialdehyde (MDA), superoxide dismutase (SOD), and advanced oxidation protein products (AOPP).
If a study reported multiple time points, the results with the longest time point were included in the analysis. If multiple stages were included in a study report, the first stage was analyzed.
3) Safety outcome: Any adverse events that occurred during the study should be recorded, such as the incidence of hypoglycemia, the rate of adverse events, the rate of serious adverse events, and the incidence of gastrointestinal adverse reactions.
1) Non-RCT research studies, such as conference papers, animal studies, mechanism studies, clinical experience, data analysis, systematic reviews, guideline studies, retrospective studies, and data analysis and reviews.
2) If there were duplicates in the data, only the one with detailed data was selected.
3) Papers that could not be searched and authors who could not be contacted were excluded.
4) Literature from research in other fields, such as nursing, was excluded.
1) Patients on dialysis were excluded.
2) Patients with other complications clearly written in the text were excluded.
3) Patients with unclear diagnostic criteria were excluded.
Interventions included TCM methods other than oral NDQG, such as enemas, acupuncture, and other TCM medicines.
There are obvious data errors or incomplete data and lack of required indicators.
Import the search results into the EndNoteX9 software in the form of a bibliography to establish a database. YDL (Yuandong Li) and YX (Yang Xiao) independently screened the literature, extracted the data, and cross-checked according to the inclusion criteria and exclusion criteria, and if there was a discrepancy, ZYZ (Zhiyue Zhu) was consulted to assist in judgment, and the authors of the literature lacking the data were contacted by email to obtain the literature as much as possible. First, software was used to delete duplicate documents, and then they were manually checked again to delete duplicate documents. Second, preliminary screening was carried out by reading the titles and abstracts of the literature, and literature that did not meet the criteria was excluded. Literature that still did not meet the criteria was excluded by reading the full text. If there were differences, they were determined after discussion or consultation with ZYZ. YDL and YX independently extracted data from the included studies and cross-checked them based on pre-designed data extraction tables. The data extraction content mainly included the following: (Collaboration, 2020) the basic information of the included research, the research title, first author, and year of publication; (Thomas, 2019) the baseline characteristics of the study subjects, including the sample size of each group, the age, gender, and disease status of the patients; (Sun et al., 2022) specific details of the intervention; (Hernandez et al., 2022) key elements of risk of bias assessment; and (Gu et al., 2019) outcomes of interest and adverse events.
CQS (Chaoqun Song) and SLL (Shilin Liu) assessed the risk of bias of the included studies according to the Cochrane risk of bias assessment tool for RCTs. The tool assessed seven important sources of bias: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Risk of bias was assessed for each included study from these seven domains. By assessing the completeness of the study and the correctness of the methodological implementation, each aspect was assessed as “high risk,” “low risk, or “unclear risk.” The two researchers operated independently and examined each other’s results. Any disagreement on the evaluation of results was solved through discussion between LL (Le Liu) and CWW (Chunwei Wu) to make the final decision.
The meta-analysis was conducted using Stata 16.0 software, which is provided by the Cochrane Collaboration Network. Relative risk (RR) and its 95% Confidence interval (CI) were used as the combined effect size for the counted data. The mean difference (MD) and its 95% CI were used as the combined effect size for the measured data. I2 was used for heterogeneity between results. Meta-analyses were performed using a fixed-effect model when there was statistical homogeneity between results (p > 0.1, I2 < 50%), and sources of heterogeneity were analyzed if there was statistical heterogeneity between results (p < 0.1, I2 > 50%). If there was statistical heterogeneity between groups, there was no clinical heterogeneity or difference. A random-effects model was used for meta-analysis. If there was too much heterogeneity between results, descriptive analysis was performed. Funnel plots were used to assess publication bias in results involving more than 10 studies. Subgroup analysis based on prespecified assumptions explored sources of heterogeneity if necessary.
Through the search of six major Chinese and English databases, 626 relevant articles were obtained. Of these, 266 were excluded due to duplication. After reading the article titles and abstracts, 274 were excluded. By reading the full text of the remaining 86 papers, a total of 52 papers (Cao and Liu, 2005; Lv et al., 2008; Zhao et al., 2008; Wang et al., 2009; Wu et al., 2009; Xie and Feng, 2009; Yang, 2009; Zhao and Chen, 2009; Bai and Shi, 2010; Cai et al., 2010; Cai and Wang, 2010; Jia et al., 2010; Yan and Liu, 2010; Zhang et al., 2010; Chen, 2011; Liang, 2011; Wang and Zhang, 2011; Xiao et al., 2011; Zhang et al., 2011; Hu, 2012; Liu et al., 2012; Wang et al., 2012; Fan, 2013; Gong, 2013; Wang et al., 2013; Yao and Ren, 2013; Yu, 2013; Zhang, 2013; Shi et al., 2014; Hao, 2015; He and Ding, 2015; Huang, 2015; Li, 2015; Wan, 2015; Li et al., 2016; Wang, 2016; Zhang et al., 2016; Li et al., 2017; Luo and Li, 2018; Wei and Ruan, 2018; Ding and Zhang, 2019; Liu and Yang, 2020; Chen et al., 2021; Fang, 2021; He, 2021; Kou, 2021; Lan et al., 2021; Li et al., 2021; Liang et al., 2021; Wu, 2021; Xu, 2021; Li, 2022) were finally included for quantitative analysis. The study selection and identification are shown in Figure 1.
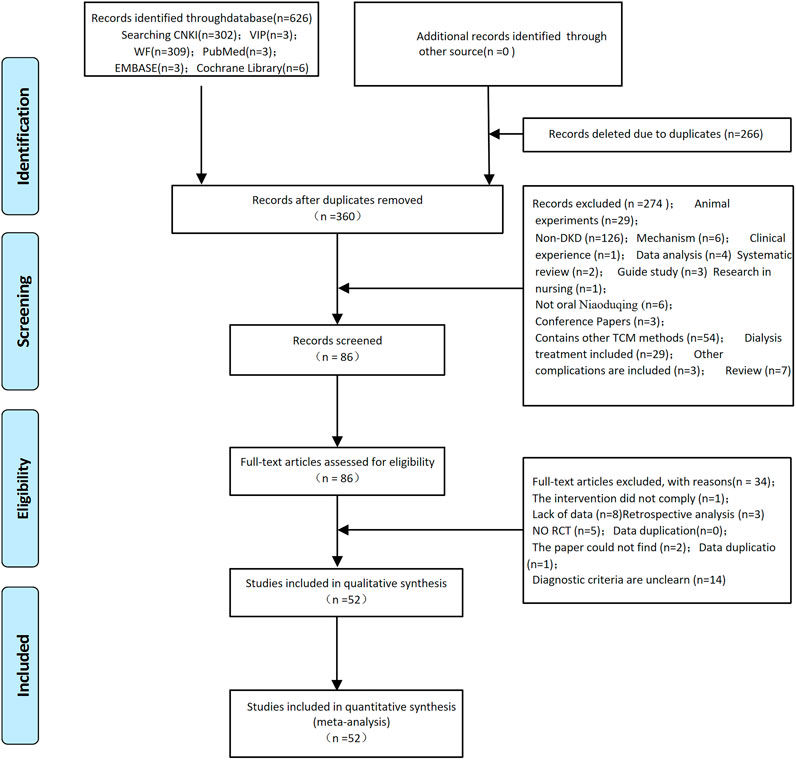
FIGURE 1. Flowchart of study selection and identification.
The total of 52 RCTs included in this study, all of which are Chinese literature, were dated between 2005 and 2022, and a total of 4,006 patients were included, including 1,987 in the control group and 2,019 in the treatment group. The WHO, ADA, Morganson, or Chinese guidelines were referred to for diagnostic criteria. The baseline characteristics for inclusion in this study are shown in Table 2.
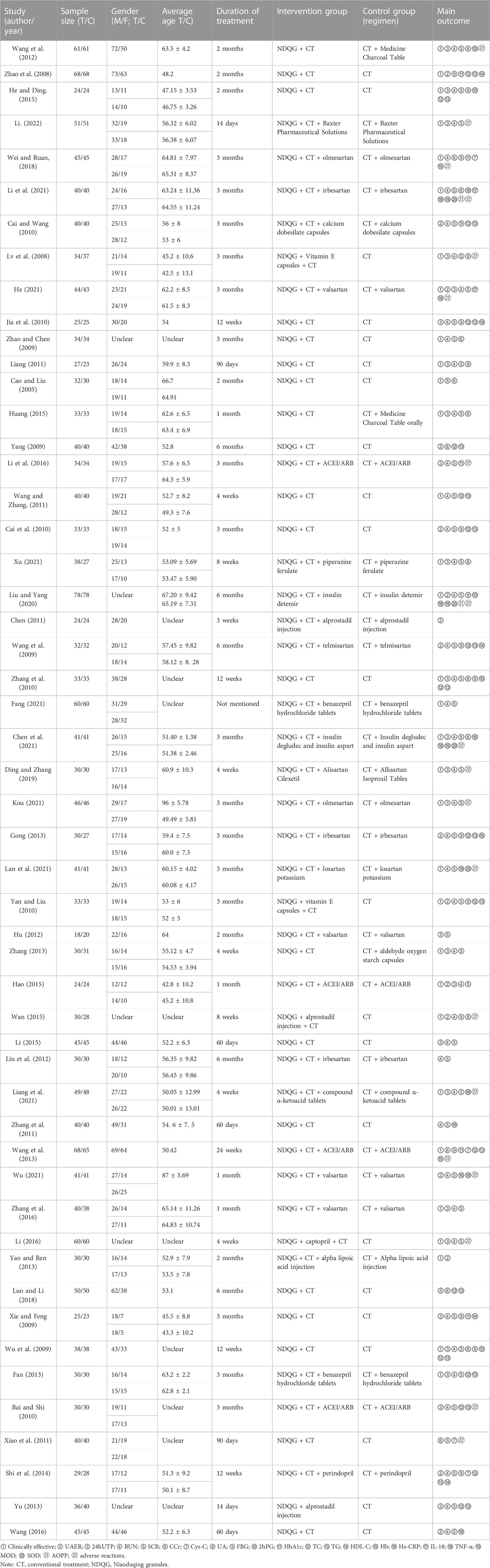
TABLE 2. Baseline characteristics for inclusion.
A total of 52 RCTs were included in this systematic review, of which 15 studies (Cai et al., 2010; Cai and Wang, 2010; Yan and Liu, 2010; Wang et al., 2013; He and Ding, 2015; Li, 2015; Wang, 2016; Zhang et al., 2016; Wei and Ruan, 2018; He, 2021; Kou, 2021; Lan et al., 2021; Liang et al., 2021; Wu, 2021; Li, 2022) used the random number table method, one study (Liu and Yang, 2020) used the random lottery method, and the remaining 36 items (Cao and Liu, 2005; Lv et al., 2008; Zhao et al., 2008; Wang et al., 2009; Wu et al., 2009; Xie and Feng, 2009; Yang, 2009; Zhao and Chen, 2009; Bai and Shi, 2010; Jia et al., 2010; Zhang et al., 2010; Chen, 2011; Liang, 2011; Wang and Zhang, 2011; Xiao et al., 2011; Zhang et al., 2011; Hu, 2012; Liu et al., 2012; Wang et al., 2012; Fan, 2013; Gong, 2013; Yao and Ren, 2013; Yu, 2013; Zhang, 2013; Shi et al., 2014; Hao, 2015; Huang, 2015; Wan, 2015; Li et al., 2016; Li et al., 2017; Luo and Li, 2018; Ding and Zhang, 2019; Chen et al., 2021; Fang, 2021; Li et al., 2021; Xu, 2021) mentioned randomization but did not describe the specific random method, and the aforementioned literature was not sufficiently blinded. In one reference (Lv et al., 2008), the results and description of the UAER did not match, and this set of data was excluded; the data of TC and TG in one paper (Jia et al., 2010) were reversed, and the results were changed back after verifying the authors; the verified results and the unit errors for CCr in one study (Liang, 2011) and 24hUTP in two studies (Chen et al., 2021; Kou, 2021) were not excluded; the 24hUTP unit was wrong in one study (Wang and Zhang, 2011), and we cannot identify or correct it, so it was excluded; the UAER unit was wrong in one study (Liu et al., 2012), and the data were excluded. Three RCTs (Lv et al., 2008; Gong, 2013; Wan, 2015) had participants of exfoliation, which were not included, and exfoliation cases were excluded. There were multiple sets of data for the same indicator in three papers (Yang, 2009; Yao and Ren, 2013; Luo and Li, 2018), and the group of data with a longer observation period was selected. Overall, the quality of the included literature was not high.
The clinical effective rate were reported in 32 studies (Cao and Liu, 2005; Lv et al., 2008; Zhao et al., 2008; Wu et al., 2009; Zhao and Chen, 2009; Yan and Liu, 2010; Zhang et al., 2010; Liang, 2011; Wang and Zhang, 2011; Wang et al., 2012; Fan, 2013; Wang et al., 2013; Yao and Ren, 2013; Zhang, 2013; Hao, 2015; He and Ding, 2015; Huang, 2015; Wan, 2015; Zhang et al., 2016; Li et al., 2017; Wei and Ruan, 2018; Ding and Zhang, 2019; Liu and Yang, 2020; Chen et al., 2021; Fang, 2021; He, 2021; Kou, 2021; Lan et al., 2021; Li et al., 2021; Liang et al., 2021; Xu, 2021; Li, 2022) involving 2,630 patients, including 1,332 in the treatment group and 1,298 in the control group. The results showed that the clinical effective rate of the treatment of the experimental group was better than that of the control group [RR = 1.23, 95% CI (1.17, 1.29), p < 0.001, I2 = 53.17%], which was statistically significant, as shown in Figure 2A. In the included literature, heterogeneity analysis showed that heterogeneity was due to the difference in the specific conventional treatment modality of the different DKD stages of the patients. L'Abbe diagrams and funnel diagrams are shown in Figures 2B, C.
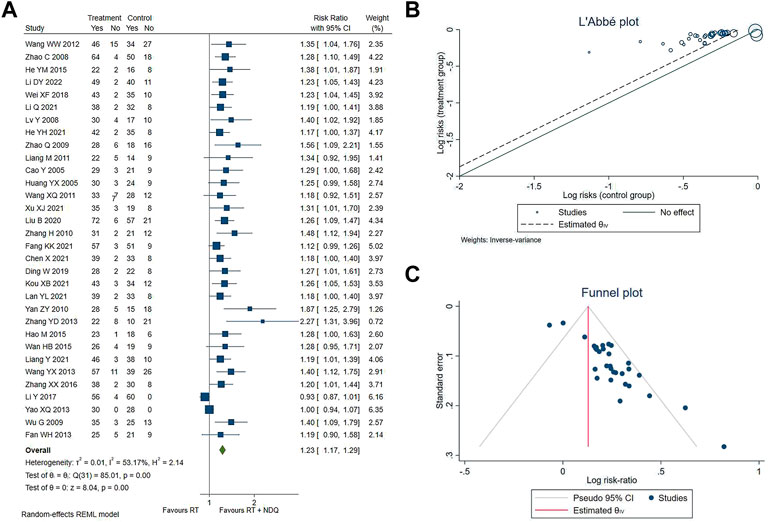
FIGURE 2. (A) Clinically effective. (B) L'Abbe plot. (C) Funnel plot.
The UAER levels were reported in 18 studies (Zhao et al., 2008; Wang et al., 2009; Yang, 2009; Cai et al., 2010; Cai and Wang, 2010; Yan and Liu, 2010; Chen, 2011; Xiao et al., 2011; Gong, 2013; Yao and Ren, 2013; Shi et al., 2014; Hao, 2015; Wan, 2015; Li et al., 2016; Luo and Li, 2018; Liu and Yang, 2020; He, 2021; Wu, 2021), including 700 patients in the treatment group and 693 patients in the control group. The results showed that the treatment group significantly outperformed the control group in reducing UAER levels [SMD = −0.90, 95% CI (−1.14, −0.66), p < 0.001, I2 = 78.19%], as shown in Figure 3.
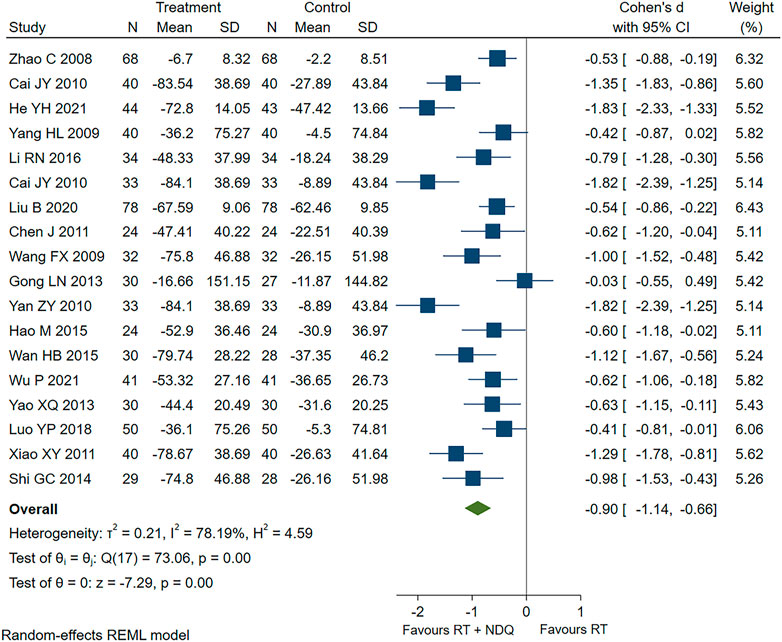
FIGURE 3. UAER forest chart.
The 24hUTP levels were reported in 27 studies (Lv et al., 2008; Wu et al., 2009; Xie and Feng, 2009; Bai and Shi, 2010; Jia et al., 2010; Zhang et al., 2010; Liang, 2011; Zhang et al., 2011; Hu, 2012; Wang et al., 2012; Fan, 2013; Yu, 2013; Zhang, 2013; Hao, 2015; He and Ding, 2015; Huang, 2015; Li, 2015; Wang, 2016; Zhang et al., 2016; Li et al., 2017; Ding and Zhang, 2019; Chen et al., 2021; He, 2021; Kou, 2021; Liang et al., 2021; Xu, 2021; Li, 2022), including 997 patients in the treatment group and 976 patients in the control group. The results showed that the treatment group was significantly better than the control group in reducing 24hUTP levels [SMD = −0.81, 95% CI (−1.08, −0.55), p < 0.001, I2 = 87.08%], and the forest chart is shown in Figure 4.
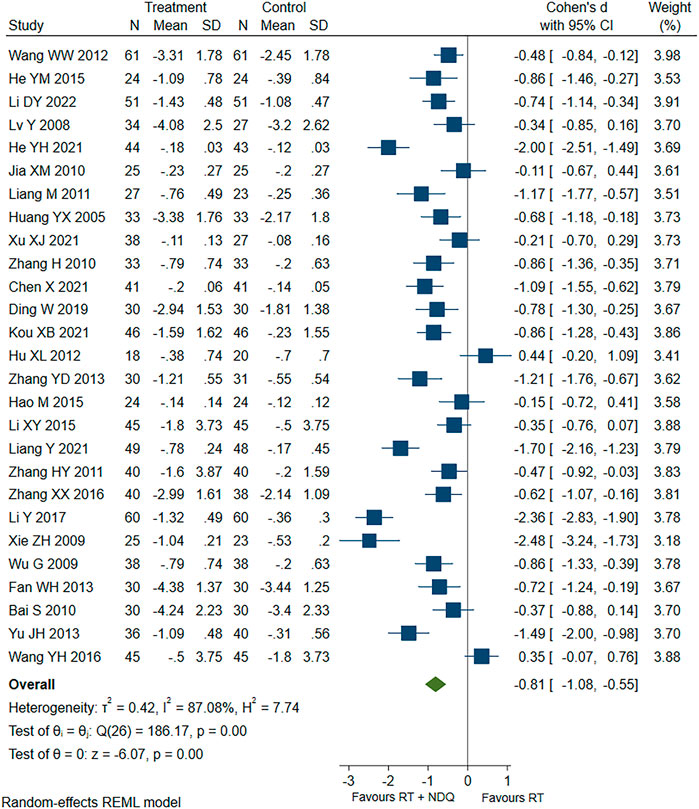
FIGURE 4. 24hUTP forest chart.
We studied 18 secondary outcomes from six aspects: kidney function, the level of glucose metabolism, the level of lipid metabolism, hemoglobin, inflammatory factors, and oxidative stress. Furthermore, safety outcomes were studied from adverse events, the specific results of which are shown in Table 3; forest charts are shown in Supplementary Materials S3–S21.
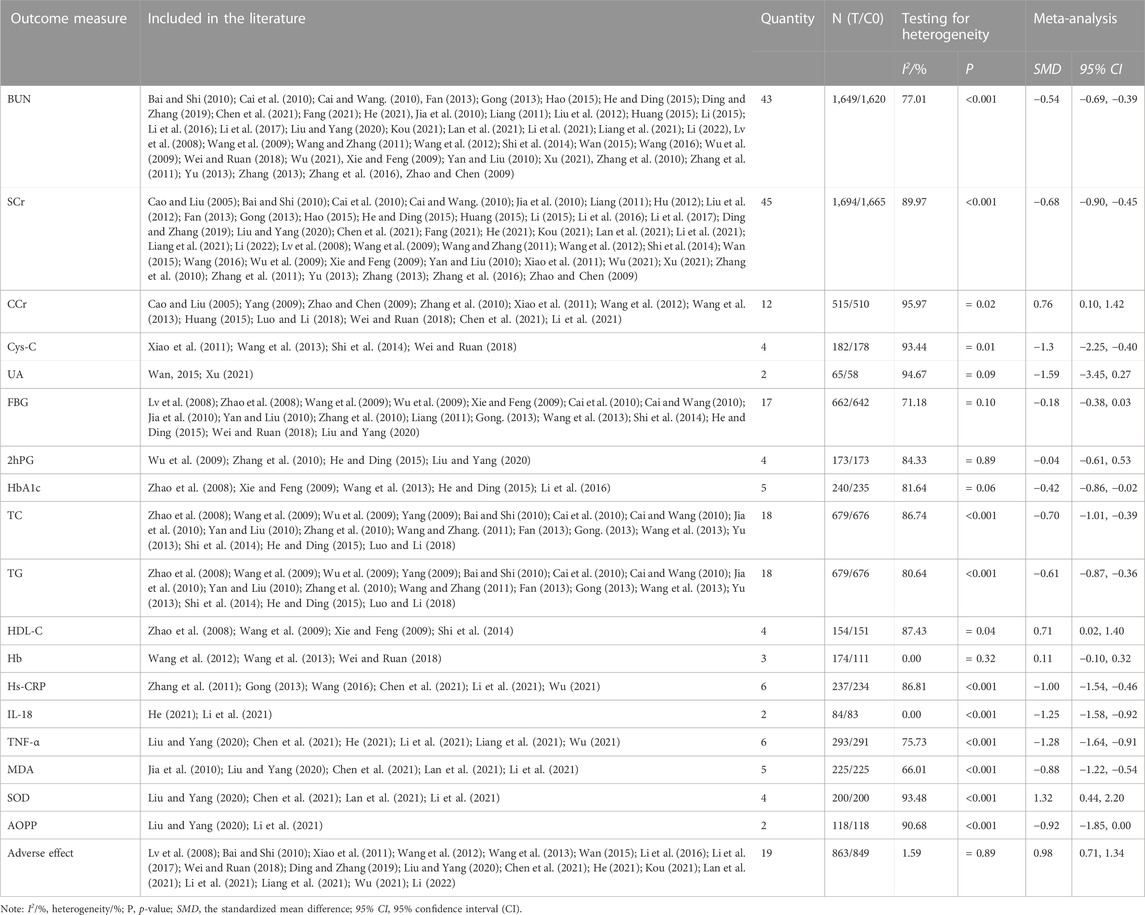
TABLE 3. Secondary outcomes and safety outcomes.
Clinical studies have shown that diabetes is more likely to cause glomerulosclerosis in affected patients leading to renal insufficiency, which leads to DKD (Li, 2016; Jing et al., 2017). Increased deposition of extracellular matrix proteins at the glomerular level, such as fibronectin and type IV (IV-C), leads to thylakoid dilation and thickening of the glomerular basement membrane, leading to progressive renal failure, which eventually develops into ESRF (Lan et al., 2010).
In this study, we analyzed the efficacy and safety of NDQG in the treatment of DKD for the first time and conducted detailed analyses of the indicators in terms of clinical effective rate, kidney function, the level of glucose metabolism, the level of lipid metabolism, Hb, inflammatory factors, oxidative stress, and adverse events. A total of 626 articles were identified, and 52 were included. The risk of bias assessment showed that the methodological quality of the included studies was low, mainly due to lack of detailed reporting of specific methods for randomization and allocation concealment and inadequate blinding.
This meta-analysis found that compared to CT alone, adjuvant with NDQG had significantly better clinical efficacy in the treatment of patients with DKD [RR = 1.23, 95% CI (1.17, 1.29), p < 0.001, I2 = 53.17%]. Therefore, the clinical use of NDQG as an adjuvant treatment of DKD is a good choice.
NDQG are generally beneficial in improving kidney function. NDQG can significantly reduce UAER levels [SMD = −0.90, 95% CI (−1.14, −0.66), p < 0.001, I2 = 78.19%], 24hUTP levels [SMD = −0.81, 95% CI (−1.08, −0.55), p < 0.001, I2 = 87.08%], BUN [SMD = −0.54, 95% CI (−0.69, −0.39), p < 0.01, I2 = 77.01%], SCr [SMD = −0.68, 95% CI (−0.90, −0.45), p < 0.001, I2 = 89.97%], and Cys-C [SMD = −1.32, 95% CI (−2.25, −0.40), p = 0.01, I2 = 93.44%] and elevate CCr [SMD = 0.76, 95% CI (0.10, 1.42), p = 0.02, I2 = 95.97%], but the reduction of UA [SMD = −1.59, 95% CI (−3.45, 0.27), p = 0.09, I2 = 94.67%] is not much different from CT. Therefore, we can think that NDQG improve kidney function by reducing UAER, 24hUTP, SCr, BUN, and Cys-C and increasing CCr but have little effect on UA. The level of estimated glomerular filtration rate (eGFR) is a common indicator used to evaluate whether the kidney function is normal (You et al., 2018). However, only one paper (Kou, 2021) observed this indicator, but it is not sufficient for pooled analysis, so eGFR is not discussed in this paper. Relevant studies have shown that NDQG can improve renal fibrosis by inhibiting TGF-β1 expression, reducing podocyte damage, inhibiting tubular epithelial cell transdifferentiation, improving the microinflammatory state, inhibiting oxidative stress, and reducing insulin resistance (Tang et al., 2008a; Tang et al., 2008b; Chen et al., 2008; Zhang et al., 2009; Hu and Ou, 2010; Qi, 2010).
NDQG are generally beneficial in improving the level of glucose metabolism. NDQG can reduce FBG [SMD = −0.18, 95% CI (−0.38, 0.03), p = 0.10, I2 = 71.18%] and HbA1c [SMD = −0.42, 95% CI (−0.86, −0.02), p = 0.06, I2 = 81.64%], but the effect on 2hPG [SMD = −0.04, 95% CI (−0.61, 0.53), p = 0.89, I2 = 84.33%] is not obvious, which suggests that NDQG in the treatment of DKD lower HbA1c by reducing FBG. In 2010, the ADA guidelines for diabetes management included glycated hemoglobin ≥6.5 percent as one of the diagnostic criteria for type 2 diabetes (T2DM) (American Diabetes Associtaion, 2010). HbA1c reflects the average blood glucose level over the past 2–3 months and is an important criterion for assessing control blood glucose. The UK Prospective Diabetes Study has shown that the risk of developing various complications in people with T2DM is strongly related to blood sugar control. For every 1% reduction in HbA1c, the risk of all diabetes-related endpoints was reduced by 21%, the risk of diabetes-related death by 21%, the risk of myocardial infarction by 14%, and the risk of microvascular complications by 37% (Stratton et al., 2000).
Adjuvant treatment with NDQG can reduce TC [SMD = −0.70, 95% CI (−1.01, −0.39), p < 0.001, I2 = 86.74%] and TG [SMD = −0.61, 95% CI (−0.87, −0.36), p < 0.001, I2 = 80.64%], which are the risk factors of DKD. However, due to the small number of included studies on HDL-C [SMD = 0.71, 95% CI (0.02, 1.40), p = 0.04, I2 = 87.43%], it is unclear whether NDQG have an improved effect on HDL-C. Dyslipidemia is a common risk factor for cardiovascular disease, which in turn is the main cause of morbimortality in CKD and T2DM (Hager et al., 2017). Abnormalities in the lipid metabolism promote progression of kidney damage (Kramer et al., 2006). According to our findings, combining NDQG with CT could be a beneficial therapy for DKD patients with abnormal TC and TG metabolisms.
In all patients with CKD, patients with DKD are more likely to develop anemia than those with non-diabetic kidney disease (NDKD) (Ito et al., 2021), so we investigated the effect of NDQG on Hb, and studies have shown that adjuvant treatments with NDQG are not much different from CT in increasing Hb [SMD = 0.11, 95% CI (−0.10, 0.32), p = 0.32, I2 = 0.00]. This is contrary to the conclusion that NDQG can improve anemia caused by kidney disease (Zhang and Lei, 2012). We think there could be two reasons for this: on the one hand, it may be due to NDQG having no benefit on kidney anemia caused by DKD; on the other hand, it may be due to the small number of included literature and the low quality of the literature, so more high-quality literature is needed to explore this indicator.
Chronic microinflammatory states are common in patients with CRF, and inflammatory factors associated with microinflammatory states include Hs-CRP, IL-6, IL-8, and TNF-α (Zhu et al., 2018). We found that NDQG have beneficial effects in reducing Hs-CRP [SMD = −1.00, 95% CI (−1.54, −0.46), p < 0.001, I2 = 86.81%], IL-18 [SMD = −1.25, 95% CI (−1.58, −0.92), p < 0.001, I2 = 0], and TNF-α [SMD = −1.28, 95% CI (−1.64, −0.91), p < 0.001, I2 = 75.73%]. It has been proven that NDQG can have a positive effect on the disease by improving the microinflammatory state of DKD.
Oxidative stress plays an important role in the development of CRF, and studies have shown that reducing oxide production or increasing the body’s antioxidant capacity can improve oxidative stress damage in renal tissue in patients with CRF (Kim and Vaziri, 2010). This analysis found that NDQG mainly improve oxidative stress in DKD by reducing MDA [SMD = −0.88, 95% CI (−1.22, −0.54), p < 0.001, I2 = 66.01%] and AOPP [SMD = −0.92, 95% CI (−1.85, 0.00), p < 0.001, I2 = 90.68%].
Of the 52 included studies, adverse events were mentioned in 24 studies (Lv et al., 2008; Bai and Shi, 2010; Xiao et al., 2011; Zhang et al., 2011; Wang et al., 2012; Gong, 2013; Wang et al., 2013; Li, 2015; Wan, 2015; Li et al., 2016; Wang, 2016; Zhang et al., 2016; Li et al., 2017; Wei and Ruan, 2018; Ding and Zhang, 2019; Liu and Yang, 2020; Chen et al., 2021; He, 2021; Kou, 2021; Lan et al., 2021; Li et al., 2021; Liang et al., 2021; Wu, 2021; Li, 2022), of which adverse events occurred in 19 studies (Lv et al., 2008; Bai and Shi, 2010; Xiao et al., 2011; Wang et al., 2012; Wang et al., 2013; Wan, 2015; Li et al., 2016; Li et al., 2017; Wei and Ruan, 2018; Ding and Zhang, 2019; Liu and Yang, 2020; Chen et al., 2021; He, 2021; Kou, 2021; Lan et al., 2021; Li et al., 2021; Liang et al., 2021; Wu, 2021; Li, 2022). Adverse events were mentioned in the remaining five studies (Zhang et al., 2011; Gong, 2013; Li, 2015; Wang, 2016; Zhang et al., 2016), but no adverse events were observed in either groups. The remaining 28 studies did not report adverse events, suggesting that these researchers did not pay enough attention to adverse events. We also found that adjuvant treatment with NDQG did not increase the incidence of adverse reactions in the control group [SMD = 0.98, 95% CI (0.71, 1.34), p = 0.89, I2 = 1.59%]. Adverse reactions include gastrointestinal reactions, dry mouth, hyperkalemia, hypoglycemia, allergies, dizziness, headache, fatigue, flushing, dry cough, fever, rash, and hypercalcemia, of which gastrointestinal reactions are the most common, appearing 17 times. None of these studies had patients withdrawn from the RCT; however, only two studies (Wang et al., 2013; Li et al., 2016) mentioned that side effects disappeared after NDQG reduction, and the rest of the literature did not treat them or did not mention how to deal with them. These results show that the proper use of NDQG has a high safety profile in clinical use.
However, the heterogeneity of the 22 indicators analyzed in this study was high (I2 > 50%), which may be caused by different disease and treatment courses.
NDQG are a pure Chinese medicine preparation composed of 16 herbs, which have the advantages of being a component and multi-target and have played a unique role in the treatment of DKD. Modern pharmacological studies have found that the main components of NDQG include rhubarb acid, matrine, astragaloside IV, peony glycoside, Salvianic acid A and protocatechin, stilbene glycoside, and salvianolic acid B (Zou and Zhou, 2009; He et al., 2011; Chen, 2015; Zhao, 2017; Zhao et al., 2022). Previous studies have shown that NDQG can reduce the expression level of the pro-inflammatory factor interleukin in the blood of DKD patients, alleviate platelet activation status, and delay renal failure (Liang et al., 2020), and the active ingredients such as isoflavones and peony glycosides can significantly improve kidney function (Zhou et al., 2020). NDQG have been widely used in clinical practice, which can effectively reduce the level of SCr and BUN, stabilize and protect residual kidney function, help discharge accumulated toxins in the body, and reduce the burden on patients’ kidneys (Layton et al., 2020). The total glycoside of white peony in NDQG can effectively improve the immune function of rats and effectively reduce inflammatory response and oxidative stress response (Yan et al., 2018); white urinary lactone I and white urinary lactone III can significantly inhibit the production of TNF-α and inhibit the activity of TNF-αmRNA; atractylenolide I has a stronger inhibitory effect than atractylenolide III (Li et al., 2007); chuanxiongzine can reduce the 24hUTP levels in rats with IgA nephropathy, inhibit the deposition of IgA in the mesangial region, and downregulate TGF-β mRNA in kidney tissue and TGF-β protein levels (Lin et al., 2013); and oxymatrine inhibits renal fibrosis (Chen and Jin, 2014).
In summary, the intrinsic reasons for NDQG to improve kidney function and regulate glycolipid metabolism may be related to factors such as the fact that its active ingredients can inhibit oxidative stress and reduce and regulate inflammatory response.
The mechanism of adverse reactions caused by NDQG is not clear. Among these 16 herbs in NDQG, rhubarb (Dahuang, Rheum palmatum L.), Radix Polygoni Multiflori (Heshouwu, Reynoutria multiflora (Thunb.) Moldenke), Pinellia tuber (Banxia, Pinellia ternata (Thunb.) Makino), and Chinese thorowax root (Chaihu, Bupleurum falcatum L.) were shown to cause adverse reactions in five studies (Yang et al., 2012; Yang, 2015; Sun et al., 2016; Wei and Liu, 2018; Yang et al., 2023). Among them, rhubarb (Dahuang, Rheum palmatum L.) contains anthraquinones, polysaccharides, tannins, and other components which cause liver toxicity, renal toxicity, and gastrointestinal toxicity in normal animals (Wei and Liu, 2018). The main material basis that can cause irritating toxicity in Pinellia tuber (Banxia, Pinellia ternata (Thunb.) Makino) is calcium oxalate needle crystals formed by the combination of calcium oxalate and protein (Yang et al., 2023), which will stimulate the mucosa to cause cell damage, release inflammatory mediators, and produce pinprick-like tingling; however, ginger–Pinellia tuber (Banxia, Pinellia ternata (Thunb.) Makino) is used in NDQG, and the Pinellia tuber (Banxia, Pinellia ternata (Thunb.) Makino) after concocting with ginger becomes soothing and spicy warm, which enhances its anti-nausea effect and can also play a role in strengthening the stomach. The main component of Radix Polygoni Multiflori (Heshouwu, Reynoutria multiflora (Thunb.) Moldenke) is stilbene, and it may cause skin itching, sweating, fever, chills, general weakness, dry mouth, and dizziness clinically (Yang, 2015). The main active ingredients of Chinese thorowax toot (Chaihu, Bupleurum falcatum L.) mainly include saponins, volatile oils, flavonoids, and polysaccharides (Yang et al., 2012), and Chinese thorowax toot (Chaihu, Bupleurum falcatum L.) shows hepatotoxicity and nephrotic properties in rats (Sun et al., 2016). We suspect that the adverse effects caused by NDQG may be caused by the aforementioned drugs. The side effects of NDQG still need further pharmacological and toxicological studies to be explored, and the mechanism of the synergistic effect has not been revealed completely and requires more investigations.
Although we efficiently carried out the standard analytical methods, this study has some limitations. First, according to Figure 2C, there was asymmetry on both sides and publication bias, possibly due to the poor methodological quality of the included studies, unclear randomization methods in most of the 52 included studies, lack of blinding, and failure to report allocation concealment. Second, some studies did not fully report the study characteristics such as disease course and treatment course, so the choice of heterogeneity analysis methods and the exploration of dominant populations were limited. Third, the included studies were single-center, small-sample studies and may not be representative. Fourth, the included studies were all Chinese literature, which may have ethnic and regional limitations.
In summary, we found that combination treatment with NDQG has more advantages than CT alone in DKD treatment, which could improve clinical efficiency, kidney function, blood glucose level, blood lipid level, inflammatory factors, and oxidative stress indicators. At the same time, we found that NDQG are also relatively safe. However, more high-quality studies are needed to provide more reliable evidence for clinical use.
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author.
CS and ZN conceived the idea and designed the study. CS, YL, YX, and SL conducted the literature search, study selection, data extraction, and methodology assessment. CS performed the meta-analysis. Disagreements were resolved by discussion with ZZ and LL. CS wrote the original manuscript. ZZ, LL, and CW revised the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the Natural Science Foundation of Jilin Province (YDZJ202201ZYTS192) and Jilin Provincial Science and Technology Department Project (20190304072YY).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1180751/full#supplementary-material
American Diabetes Associtaion (2010). Standards of medical care in diabetes-2010. Diabetes Care 33 (1), S11–S61. doi:10.2337/dc10-S011
Bai, S., and Shi, Y. S. (2010). Early efficacy of niaoduqing granules in the treatment of chronic renal failure caused by diabetic nephropathy. Chinese community doctors, 12 (2), 24. doi:10.3969/j.issn.1007-614x.2010.01.024
Cai, J. Y., Wang, Y. F., and Cao, P. (2010). Clinical study of niaoduqing granules in the treatment of early diabetic nephropathy. J. Pract. Diabetology 6 (4), 37–38.
Cai, J. Y., and Wang, Y. F. (2010). Niaoduqing particles combined with calcium dobesilate capsules for early diabetic nephropathy. J. Pract. Med. 26 (14), 2612–2614. doi:10.3969/j.issn.1006-5725.2010.14.058
Cao, Y., and Liu, X. (2005). Clinical observation of niaoduqing granules in the treatment of renal failure caused by diabetic nephropathy. J. Emerg. Traditional Chin. Med. 14 (4), 313. doi:10.3969/j.issn.1004-745X.2005.04.016
Chen, C., and Jin, Y. (2014). Experimental study on the mechanism of oxymatrine in the prevention and treatment of chronic renal fibrosis. Shaanxi Tradit. Chin. Med. 35 (1), 106–109. doi:10.3969/j.issn.1000-7369.2014.01.059
Chen, J. (2011). Clinical observation of alprostadil combined with niaoduqing granules in the treatment of early diabetic nephropathy. Journal 24 (5), 782–783. doi:10.3969/j.issn.1006-2882.2011.05.046
Chen, S. J., Chen, H. P., and Liu, Q. (2008). The protection on podocyte injury by niaoduqing in diabetes mellitus rats. Chin. J. Integr. Med. Nephrol. 9 (10), 875–878+944.
Chen, X. (2015). Determination of matrine in niaoduqing granules by HPLC. Heilongjiang Med. J. 28 (5), 1017–1019. doi:10.14035/j.cnki.hljyy.2015.05.003
Chen, X., Luo, H. Y., Gao, J., and Qi, C. (2021). Clinical efficacy of insulin degludec and insulin aspart combined with niaoduqing in treatment of patients with early diabetic nephropathy. Chin. J. Integr. Traditional West. Med. Intensive Crit. Care 28 (4), 404–408. doi:10.3969/j.issn.1008-9691.2021.04.005
Collaboration, G. B. D. C. K. D. (2020). Global, regional, and national burden of chronic kidney disease, 1990-2017: A systematic analysis for the global burden of disease study 2017. Lancet 395 (10225), 709–733. doi:10.1016/S0140-6736(20)30045-3
Ding, W., and Zhang, W. (2019). Analysis of the effect of niaoduqing granules combined with Allisartan Isoproxil Tables in the treatment of massive proteinuria in diabetic nephropathy. Yiayao Qianyan 9 (34), 99–100.
Fan, W. H. (2013). Efficacy of niaoduqing granules in the treatment of early renal failure in diabetic nephropathy. Chin. Med. Guide 11 (9), 649–650.
Fang, K. K. (2021). Therapeutic effect of the combination of Chinese and western medicine on early diabetic nephropathy. Chin. J. Urban Rural Enterp. Hyg. 36 (3), 163–165. doi:10.16286/j.1003-5052.2021.03.066
Gong, L. N. (2013). Clinical efficacy of compound niaoduqing particles and irbesartan in patients with stage - diabetic nephropathy. Yiayao Qianyan 13, 115–116. doi:10.3969/j.issn.2095-1752.2013.13.112
Gu, J. L., Guo, M., Xu, Y., and Xu, Y. H. (2019). Research progress on treatment strategies for diabetic kidney disease. Chin. J. Diabetes 11 (10), 645–678. doi:10.3760/cma.j.issn.1674-5809.2019.10.002
Hager, M. R., Narla, A. D., and Tannock, L. R. (2017). Dyslipidemia in patients with chronic kidney disease. Rev. Endocr. Metab. Disord. 18 (1), 29–40. doi:10.1007/s11154-016-9402-z
Hao, M. (2015). Efficacy analysis of niaoduqing granules combined with ARB/ACEI in the treatment of massive proteinuria in diabetic nephropathy. World Clin. Med. 9 (7), 142.
He, J. Y., Wang, R. S., and Huang, Z. S. (2011). Determination of the contentes of rhein in niaoduqing granules by HPLC. Modern hospital. 11 (6). 30–31. doi:10.3969/j.issn.1671-332X.2011.06.014
He, Y. H. (2021). Effects of niaoduqing granules combined with valsartan on renal function, inflammatory factors and immune function in patients with early diabetic nephropathy. J. New Chin. Med. 53 (10), 60–63. doi:10.13457/j.cnki.jncm.2021.10.016
He, Y. M., and Ding, X. Q. (2015). Clinical study on the effect of niaoduqing granules on inflammatory factors in patients with early and intermediate diabetic nephropathy. Pharmacol. Clin. Chin. Materia Medica 31 (6), 160–162. doi:10.13412/j.cnki.zyyl.2015.06.051
Hernandez, L. F., Eguchi, N., Whaley, D., Alexander, M., Tantisattamo, E., and Ichii, H. (2022). Anti-oxidative therapy in diabetic nephropathy. Front. Biosci. Sch. Ed. 14 (2), 14. doi:10.31083/j.fbs1402014
Hu, H. J., and Ou, Y. P. (2010). Effects of niaoduqing granule on renal function and C-reactive protein in patients with chronic renal failure. China J. Clin. Ration. Drug Use 3 (9), 70–71. doi:10.15887/j.cnki.13-1389/r.2010.09.016
Hu, X. L. (2012). Efficacy of niaoduqing granules combined with valsartan in the treatment of diabetic nephropathy. Yiayao Qianyan 2 (5), 11–112. doi:10.3969/j.issn.2095-1752.2012.05.101
Huang, Y. X. (2015). Clinical study of niaoduqing granules in the treatment of diabetic renal failure. Asia-pacific traditional medicine. 11 (18). 117–118. doi:10.11954/ytctyy.201518064
Ito, K., Yokota, S., Watanabe, M., Inoue, Y., Takahashi, K., Himuro, N., et al. (2021). Anemia in diabetic patients reflects severe tubulointerstitial injury and aids in clinically predicting a diagnosis of diabetic nephropathy. Intern Med. 60 (9), 1349–1357. doi:10.2169/internalmedicine.5455-20
Jia, X. M., Hu, Z. J., Dong, C. X., Guo, L., and Shi, Y. N. (2010). Observation of antioxidant stress of niaoduqing granules in diabetic nephropathy. Shandong Med. J. 50 (17), 56–57. doi:10.3969/j.issn.1002-266X.2010.17.024
Jing, Y. F., Hu, J. L., and Tang, S. Y. (2017). Systematic evaluation of cordyceps sinensis in the treatment of diabetic nephropathy stage III-IV tianjin pharmacy. 29 (2). 32–37.
Kim, H. J., and Vaziri, N. D. (2010). Contribution of impaired Nrf2-Keap1 pathway to oxidative stress and inflammation in chronic renal failure. Am. J. Physiol. Ren. Physiol. 298 (3), F662–F671. doi:10.1152/ajprenal.00421.2009
Kou, X. B. (2021). Observation of the effect of niaoduqing granules combined with olmesartan in the treatment of early diabetic nephropathy. J. Henan Med. Coll. Staff Work. 33 (6), 652–654. doi:10.3969/j.issn.1008-9276.2021.06.005
Kramer, H. J., Saranathan, A., Luke, A., Durazo-Arvizu, R. A., Guichan, C., Hou, S., et al. (2006). Increasing body mass index and obesity in the incident ESRD population. J. Am. Soc. Nephrol. 17 (5), 1453–1459. doi:10.1681/ASN.2005111241
Lan, T., Shen, X., Liu, P., Liu, W., Xu, S., Xie, X., et al. (2010). Berberine ameliorates renal injury in diabetic C57BL/6 mice: Involvement of suppression of SphK-S1P signaling pathway. Arch. Biochem. Biophys. 502 (2), 112–120. doi:10.1016/j.abb.2010.07.012
Lan, Y. L., Du, L., Jiang, C. Y., and Feng, F. (2021). Curative effect of niaoduqing granule combined with losartan potassium on early diabetic nephropathy and its effect on oxidative stress indicators. Chin. Archives Traditional Chin. Med. 39 (4), 56–59. doi:10.13193/j.issn.1673-7717.2021.04.015
Layton, J. B., McGrath, L. J., Sahrmann, J. M., Ma, Y., Dharnidharka, V. R., O'Neil, C., et al. (2020). Comparative safety of high-dose versus standard-dose influenza vaccination in patients with end-stage renal disease. Vaccine 38 (33), 5178–5186. doi:10.1016/j.vaccine.2020.06.020
Li, C. Q., He, L. C., and Jin, J. Q. (2007). Atractylenolide I and atractylenolide III inhibit Lipopolysaccharide-induced TNF-alpha and NO production in macrophages. Phytother. Res. 21 (4), 347–353. doi:10.1002/ptr.2040
Li, D. Y. (2022). Analysis of the effect of niaoduqing granules combined with exenatide in patients with diabetic nephropathy. J. Med. Theory Pract. 35 (12), 2039–2041. doi:10.19381/j.issn.1001-7585.2022.12.020
Li, Q., Cao, M., Li, K., and Li, J. (2021). Observation on the effect of niaoduqing granules combined with irbesartan in the treatment of early diabetic nephropathy. Med. Innovation China 18 (16), 16–20. doi:10.3969/j.issn.1674-4985.2021.16.004
Li, R. N., Lv, Q., Yang, X. L., and Chen, N. (2016). Clinical observation of niaoduqing granules in the treatment of early diabetic nephropathy. J. Med. Theory Pract. 29 (11), 1406–1407.
Li, X. Y. (2015). Changes of renal function and serum hs-CRP levels in diabetes patients with chronic renal insufficiency before and after taking niaoduqing particle. Chinese J. Pract. Med. 42 (23), 41–42. doi:10.3760/cma.j.issn.1674-4756.2015.23.021
Li, Y., Gao, J., Wang, M., Zheng, J., Hui, E. S., Wan, M., et al. (2017). Characterization of extensive microstructural variations associated with punctate white matter lesions in preterm neonates. Chronic Pathematology J. 18 (11), 1228–1234. doi:10.3174/ajnr.A5226
Li, Y. X. (2016). Effect observation of Jin shui bao in the treatment of early diabetic Nephropathy. Chinese community doctors. 32 (7). 105+7. doi:10.3969/j.issn.1007-614x.2016.7.65
Liang, M. (2011). Clinical observation of niaoduqing granules in the treatment of renal failure in diabetic nephropathy. China Pract. Med. 6 (31), 155–156. doi:10.3969/j.issn.1673-7555.2011.31.129
Liang, Y., Chen, X., Zhou, F., Xiao, Y., Cao, X., Zhang, Z., et al. (2021). Self-powered soft robot in the mariana trench. Med. Dietetics Health 19 (8), 66–71. doi:10.1038/s41586-020-03153-z
Liang, Z. G., Zhang, Z. Z., Li, B. J., Huang, J., and Zhang, J. (2020). Clinical observation of niaoduqing granule combined with valsartan capsules in treatment of diabetic nephropathy. 38 (5). 241–244. doi:10.13193/j.issn.1673-7717.2020.05.057
Lin, P., and Xu, X. L., (2017). Clinical observation of niaoduqing granules combined with western medicine in the treatment of chronic kidney disease. 38 (11), 1538–1539. doi:10.3969/j.issn.1000-7369.2017.11.024
Lin, X. C., Ye, X. H., Lin, R. X., Yang, Q., and Chen, M. G. (2013). Protective effect and mechanism of action of chuanxiongzine on podocytes in rat model of IgA nephropathy. Zhejiang Med. 35 (8), 626–629.
Liu, B., and Yang, X. L. (2020). Effect of niaoduqing combined with insulin detemir on inflammation, oxidative stress and curative effect in patients with diabetic nephropathy. Diabetes New World 23 (24), 13–17. doi:10.16658/j.cnki.1672-4062.2020.24.013
Liu, X. Q., Zhang, Z. Y., and Guan, Y. (2012). Efficacy of irbesartan combined with niaoduqing granules in the treatment of early diabetic nephropathy. J. Pract. Med. 28 (9), 1567–1568. doi:10.3969/j.issn.1006-5725.2012.09.074
Lu, W. J., Wu, S. F., and Yang, H. T. (2017). Research progress on the mechanism of niaoduqing granules in the treatment of diabetic nephropathy. Henan Tradit. Chin. Med. 37 (1), 181–184. doi:10.16367/j.issn.1003-5028.2017.01.0063
Luo, Y. P., and Li, R. (2018). Efficacy of the niaoduqing granules on diabetic nephropathy. Clin. Res. Traditional Chin. Med. 10 (16), 80–81. doi:10.3969/j.issn.1674-7860.2018.16.036
Lv, Y., Wan, H. B., and Zhang, J. (2008). The efficacy of niaoduqing granules combined with low-dose vitamin E in the treatment of diabetic nephropathy in 35 cases. J. Traditional Chin. Med. 39 (1), 3–4. doi:10.3969/j.issn.1000-338X.2008.01.002
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., and Group, P. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6 (7), e1000097. doi:10.1371/journal.pmed.1000097
Qi, G. J. (2010). Effect of niaoduqing granule on insulin resistance in patients with chronic renal failure. Chin. J. Integr. Med. Nephrol. 11 (06), 537–538.
Shi, G. C., Su, C., Cui, L., Wang, G., and Ru, D. F. (2014). Observation of the therapeutic effect of perindopril combined with niaoduqing granules on diabetic nephropathy. Clin. J. Traditional Chin. Med. 26 (7), 679–681.
Stratton, I. M., Adler, A. I., Neil, H. A., Matthews, D. R., Manley, S. E., Cull, C. A., et al. (2000). Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): Prospective observational study. BMJ 321 (7258), 405–412. doi:10.1136/bmj.321.7258.405
Sun, H., Saeedi, P., Karuranga, S., Pinkepank, M., Ogurtsova, K., Duncan, B. B., et al. (2022). IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 183, 109119. doi:10.1016/j.diabres.2021.109119
Sun, X. Q., Huang, N. N., Dou, L. W., and Li, X. Y. (2016). A study on liver fibrosis efficacy accompanied by side effects of alcohol extracts from Bupleurum chinense. World Sci. Technology/Modernization Traditional Chin. Med. Materia Medica 18 (8), 1353–1361. doi:10.11842/wst.2016.08.019
Tang, S. F., Chen, G. Y., Hong, Q. G., and Lin, X. M. (2008a). Effects of niaoduqing capsule and its ingredients on expressions of TGF-β1 mVRNA in renal Tissue of CRF rats modeled by 5/6 nephrectomy. J. Guangzhou Univ. Traditional Chin. Med. 25 (6), 537–539. doi:10.13359/j.cnki.gzxbtcm.2008.06.019
Tang, S. F., Guo, S. S., and Hong, Q. G. (2008b). Effects of niaoduqing capsule and its ingredients on expressions of TGF-β1 FNLN in renal Tissue of CRF rats modeled by 5/6 nephrectomy. Chin. Archives Traditional Chin. Med. 26 (8), 1656–1658. doi:10.13193/j.archtcm.2008.08.57.tangshf.065
Thomas, B. (2019). The global burden of diabetic kidney disease: Time trends and gender gaps. Curr. Diab Rep. 19 (4), 18. doi:10.1007/s11892-019-1133-6
Wan, H. B. (2015). Clinical observation of alprostadil combined with niaoduqing granules in the treatment of diabetic nephropathy. Yiayao Qianyan 5 (9), 291–292. doi:10.3969/j.issn.2095-1752.2015.09.242
Wang, F. X., Huang, Z. Y., and Wu, J. W. (2009). Clinical observation on therapeutic effects of combined use of niaoduqing pellet and telmisartan in treating early diabetic nephropathy. Chin. J. Clin. Ration. Drug Use 2 (6), 9–10. doi:10.3969/j.issn.1674-3296.2009.06.005
Wang, W. W., Shao, Y. Y., and Wu, Y. H. (2012). The short-term efficacy of niaoduqing granules in the adjuvant treatment of diabetic renal failure was analyzed. China foreign medical treatment 31 (7). 106–107. doi:10.3969/j.issn.1674-0742.2012.07.075
Wang, X. Q., and Zhang, C. X. (2011). Clinical observation of niaoduqing granules in the treatment of early diabetic nephropathy. China's Naturop. 19 (11), 38–39. doi:10.3969/j.issn.1007-5798.2011.11.038
Wang, Y. H. (2016). Changes in kidney function before and after analysis of serum hsCRP with diabetes and chronic renal insufficiency in patients taking niaoduqing granules levels. 19 (2). 112–114. doi:10.16658/j.cnki.1672-4062.2016.02.112
Wang, Y. X., An, Y. C., Zhao, X. J., and Shi, G. H. (2013). Clinical observation of niaoduqing granules in the treatment of early diabetic nephropathy. China pharmacy 24 (20). 1881–1883. doi:10.6039/j.issn.1001-0408.2013.20.22
Wei, L. B., and Liu, L. Y. (2018). Toxic and side effects of rhubarb and its reasonable application in kidney diseases. Chin. J. Kidney Dis. Invest. Electron. Ed. 7 (1), 13–16. doi:10.3877/cma.j.issn.2095-3216.2018.01.004
Wei, X. F., and Ruan, S. L. (2018). Efficacy of niaoduqing granules combined with olmesartan in the treatment of early diabetic nephropathy and its effect on liver and kidney function. Chin. J. Gerontology 38 (4), 874–876. doi:10.3969/j.issn.1005-9202.2018.04.045
Wu, G., Zhang, Y., and Zhang, J. (2009). Clinical observation of niaoduqing granules in the treatment of diabetic nephropathy and renal insufficiency. Shandong Med. 49 (36), 89–90. doi:10.16440/j.cnki.1674-8166.2021.03.053
Wu, P. (2021). Effect of niaoduqing granules combined with valsartan on renal function in patients with early diabetic nephropathy. Chronic Pathematology J. 22 (3), 474–475+8. doi:10.16440/j.cnki.1674-8166.2021.03.053
Xiao, X. Y., Zhou, R., and Chen, F. S. (2011). Efficacy of niaoduqing granules in the treatment of early diabetic nephropathy in 40 cases. J. New Chin. Med. 43 (8), 48–49.
Xie, Z. H., and Feng, B. (2009). Clinical observation of niaoduqing granules in the treatment of diabetic nephropathy. Chinese TCM emergency 18 (6). 896–897.
Xu, X. J. (2021). Effect of niaoduqing combined with piperazine ferulate on renal function and protein metabolism in diabetic nephropathy. Med. J. present Clin. 34 (3), 90–91. doi:10.3969/j.issn.2095-9559.2021.03.055
Yan, M. G., Zhong, F. F., Guo, J. J., and Yin, W. B. (2018). Study on the immunomodulatory mechanism of total white peony glycosides on autoimmune hepatitis rats. Chin. J. Biomed. Eng. 24 (5), 324–327.
Yan, Z. Y., and Liu, B. (2010). Clinical study of niaoduqing granules combined with vitamin E in the treatment of early diabetic nephropathy. Chin. J. Postgraduates Med. 33 (36), 43–44. doi:10.3760/cma.j.issn.1673-4904.2010.36.019
Yang, F. J., Chen, J., Li, H. D., Liu, X. J., Ge, D. D., Wu, C. W., et al. (2023). Research progress on toxic components and attenuated processing methods of Pinellia ternata. Feed Ind. Mag. 44 (7), 94–98. doi:10.13302/j.cnki.fi.2023.07.015
Yang, H. L. (2009). Efficacy of niaoduqing granules in the treatment of early diabetic nephropathy. Youjiang Med. J. 37 (2), 142–143. doi:10.3969/j.issn.1003-1383.2009.02.008
Yang, L., Wang, X. Y., Liu, C., and Jiang, H. (2012). Research progress on chemical composition and pharmacological effects of Beichaihu. Inf. Traditional Chin. Med. 29 (3), 143–145.
Yang, Y. Q. (2015). The clinical application and toxic side effects of He Shou Wu. Contemp. Med. Forum 13 (9), 22–23.
Yao, X. Q., and Ren, A. P. (2013). Niaoduqing granules combined with lipoic acid in the treatment of type 2 diabetic nephropathy. Shaanxi Tradit. Chin. Med. 34 (09), 1155–1156.
You, S., Zheng, D., Zhong, C., Wang, X., Tang, W., Sheng, L., et al. (2018). Prognostic significance of blood urea nitrogen in acute ischemic stroke. Circ. J. 82 (2), 572–578. doi:10.1253/circj.CJ-17-0485
Yu, J. H. (2013). Clinical observation of alprostadil combined with niaoduqing granules in the treatment of diabetic nephropathy fujian medicine. Journal 35 (03), 96–97.
Zhang, H., Chen, L. Q., Liu, S. H., Zhao, D., and Guo, C. F. (2010). Posterior decompression with kyphosis correction for thoracic myelopathy due to ossification of the ligamentum flavum and ossification of the posterior longitudinal ligament at the same level. J. Med. Forum 31 (17), 116–122. doi:10.3171/2010.3.SPINE09237
Zhang, H. Y., Zhang, H. X., Xiao, Y., and Feng, X. Z. (2011). Effects of niaoduqing granules on renal function and serum hs-CRP levels in patients with DN chronic renal insufficiency. Shandong Med. 51 (03), 77–78.
Zhang, Q. L., Tang, S. F., and Hong, Q. G. (2009). Niaoduqing granule human drugcontaining serum inhibition of uremic toxin serum-stimulated tubular epithelial cell proliferation-2 proliferation and transdifferentiation observation. J. Guangzhou Univ. Traditional Chin. Med. 26 (6), 550–553+8. doi:10.13359/j.cnki.gzxbtcm.2009.06.014
Zhang, W., and Lei, M. (2012). Efficacy of urine toxin granules in the treatment of renal anemia. J. Pract. Med. 28 (19), 3323–3324. doi:10.3969/j.issn.1006-5725.2012.19.069
Zhang, X. X., Ma, L., and Liu, Y. (2016). Clinical observation of niaoduqing granules combined with valsartan capsule on the treatment of diabetic nephropathy complicated with massive proteinuria. Hebei J. TCM 38 (10), 1504–1506. doi:10.3969/j.issn.1002-2619.2016.10.015
Zhang, Y. D. (2013). Clinical observation of niaoduqing granules in the treatment of type 2 diabetic nephropathy. Med. Inf. 26 (8), 410. doi:10.3969/j.issn.1006-1959.2013.08.487
Zhao, C., Ma, Z. J., Chen, Y. L., and Luo, X. L. (2008). Efficacy of niaoduqing granules in 68 cases of early diabetic nephropathy. Med. Innovation China 5 (36), 145–147. doi:10.3969/j.issn.1674-4985.2008.36.101
Zhao, L., Li, Q., Li, S., Li, B., Jia, M., Pang, B., et al. (2022). Resveratrol alleviates salivary gland dysfunction induced by ovariectomy in rats. Biochem. Biophys. Res. Commun. 19 (12), 112–117. doi:10.1016/j.bbrc.2022.09.058
Zhao, Q., and Chen, B. P. (2009). Efficacy of niaoduqing granules in the treatment of diabetic nephropathy and renal failure China pharmacist. 12 (2). 233.
Zhao, S. Y. (2017). Reversed-phase high performance liquid chromatography for the determination of niaoduqing granules (sugar-free), Danshinin Protocatechin Content. Her. Med. 36 (12), 1402–1403. doi:10.3870/j.issn.1004-0781.2017.12.018
Zheng, C., Pei, T., Huang, C., Chen, X., Bai, Y., Xue, J., et al. (2016). A novel systems pharmacology platform to dissect action mechanisms of traditional Chinese medicines for bovine viral diarrhea disease. Eur. J. Pharm. Sci. 94, 33–45. doi:10.1016/j.ejps.2016.05.018
Zhou, J. W., Wang, Z., Yang, Y. X., and Wang, Y. X. (2022). Recent advances in Chinese and western medicine treatments for diabetic kidney disease. Chin. General Pract. 25 (12), 1411–1417. doi:10.12114/j.issn.1007-9572.2021.02.117
Zhou, S., Dong, Y. J., Bai, B., and Pan, X. L. (2020). Effects of niaoduqing granules combined with compound α-ketoacid tablets on renal function and serum inflammatory factors in patients with chronic renal failure. Chinese archives of traditional Chinese medicine 38 (11). 74–77. doi:10.13193/j.issn.1673-7717.2020.11.020
Zhu, L., Lu, Q. H., Wang, Z. F., Xing, X. Z., Jiang, J. X., and Liu, G. D. (2018). Effect of niaoduqing granule on microinflammatory state in patients with chronic renal failure in early and middle stage. Chin. Archives Traditional Chin. Med. 36 (6), 1474–1477. doi:10.13193/j.issn.1673-7717.2018.06.050
Zou, J. C., and Zhou, H. B. (2009). Determination of astragaloside in niaoduqing granules by HPLC-ELSD. China Pharm. 18 (9), 27–28.
Keywords: Niaoduqing granules, diabetic kidney disease, traditional Chinese medicine, systematic reviews, meta-analysis
Citation: Song C, Zhu Z, Liu L, Liu S, Li Y, Xiao Y, Wu C and Nan Z (2023) The efficacy and safety of Niaoduqing granules in the treatment of diabetic kidney disease: a systematic review and meta-analysis. Front. Pharmacol. 14:1180751. doi: 10.3389/fphar.2023.1180751
Received: 06 March 2023; Accepted: 20 June 2023;
Published: 05 July 2023.
Edited by:
Arifullah Mohammed, Universiti Malaysia Kelantan, MalaysiaReviewed by:
Fang Zhong, Icahn School of Medicine at Mount Sinai, United StatesCopyright © 2023 Song, Zhu, Liu, Liu, Li, Xiao, Wu and Nan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zheng Nan, bmFuemhlbmcwMDFAYWxpeXVuLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.