
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pharmacol. , 08 August 2023
Sec. Gastrointestinal and Hepatic Pharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1160949
This article is part of the Research Topic Advances in Novel Drugs and Targets for Hepatic and Gastrointestinal Diseases View all 33 articles
 Shilin Huang1†
Shilin Huang1† Jiazhou Ye2†
Jiazhou Ye2† Xing Gao1Xi Huang1Julu Huang2
Xing Gao1Xi Huang1Julu Huang2 Lu Lu1Cheng Lu2Yongqiang Li1Min Luo1Mingzhi Xie1
Lu Lu1Cheng Lu2Yongqiang Li1Min Luo1Mingzhi Xie1 Yan Lin1*‡
Yan Lin1*‡ Rong Liang1*
Rong Liang1*Colorectal cancer (CRC) is one of the most common malignancies, accounting for approximately 10% of global cancer incidence and mortality. Approximately 20% of patients with CRC present metastatic disease (mCRC) at the time of diagnosis. Moreover, up to 50% of patients with localized disease eventually metastasize. mCRC encompasses a complex cascade of reactions involving multiple factors and processes, leading to a diverse array of molecular mechanisms. Improved comprehension of the pathways underlying cancer cell development and proliferation, coupled with the accessibility of relevant targeted agents, has propelled advancements in CRC treatment, ultimately leading to enhanced survival rates. Mutations in various pathways and location of the primary tumor in CRC influences the efficacy of targeted agents. This review summarizes available targeted agents for different CRC pathways, with a focus on recent advances in anti-angiogenic and anti-epidermal growth factor receptor agents, BRAF mutations, and human epidermal growth factor receptor 2-associated targeted agents.
Colorectal cancer (CRC) is the third most common cancer and the third leading cause of cancer-related death worldwide. The onset of CRC is subtle and challenging to detect in early stages, underscoring the importance of timely screening. Moreover, approximately 22% of patients are diagnosed with metastatic disease at the outset. The 5-year metastatic CRC (mCRC) survival rate is approximately 15% (Howlader N et al., 2020). Therefore, precise treatment of mCRC using appropriate drugs based on relevant molecular biosignatures is essential to prolong the survival time of patients.
The main treatment strategies for mCRC are chemotherapy using cytotoxic agents, molecular-targeted therapy, and immunotherapy. Combination chemotherapy regimens frequently involve the use of fluorouracil (5-FU)-based drugs together with oxaliplatin or irinotecan. These combinations have demonstrated significant improvements in patient survival, with survival durations exceeding 20 months (Tournigand et al., 2004; Van Cutsem et al., 2014; García-Alfonso et al., 2021; Glimelius et al., 2021). Rapid and significant advancement in the development of targeted agents for CRC has been observed since the approval of cetuximab for mCRC treatment in 2004 (Figure 1) Currently, more than 10 agents have been approved for mCRC treatment. Combined treatments utilizing targeted drugs and chemotherapy have been reported to increase the 5-year survival rate from 9% to 15% and survival to more than 30 months in mCRC patients (Van Cutsem et al., 2016; Siegel et al., 2022). As distant metastasis is the main cause of death in CRC, relevant review that comprehensively explores and summarizes the efficacy of molecularly targeted drugs in CRC and associated latest research progress does not exist, and this review highlights these. This review focuses on progress of research on targeted agents for treating mCRC patients, providing a reference for clinicians for precise treatment of CRC.
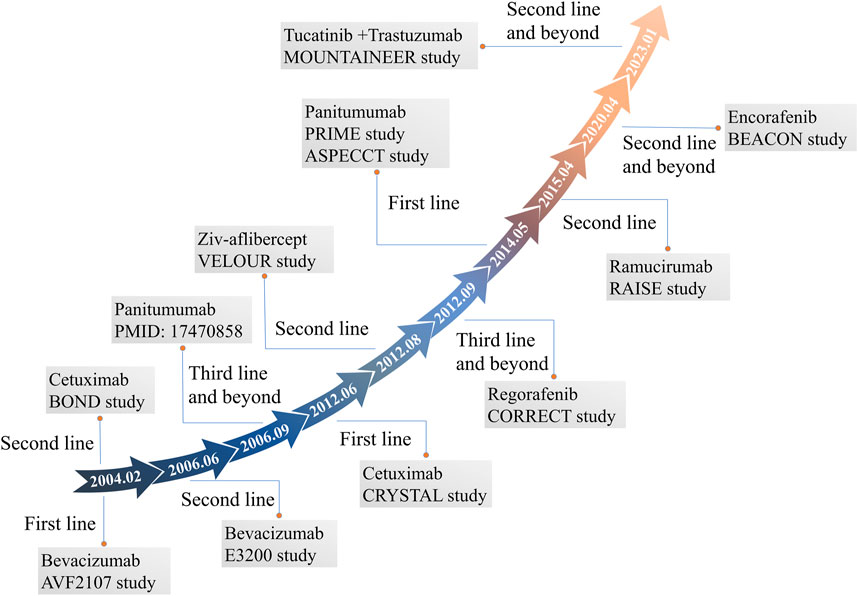
FIGURE 1. FDA-approved molecular targeted agents for mCRC and their associated clinical studies.
VEGF family includes VEGFA–D, VEGF receptor (VEGFR), and placental growth factor. VEGFA, commonly known as VEGF or vascular permeability factor, is the main angiogenic feature of the VEGF family. The role of VEGFB in tumor angiogenesis has not yet been elucidated; however, VEGFC and VEGFD mainly regulate lymphatic endothelial cell growth (Dvorak, 2002; Karkkainen et al., 2002; Ferrara et al., 2003; Bry et al., 2014). VEGFR includes VEGFR1–3, with VEGFA capable of binding to VEGFR1 and 2, and VEGFC and VEGFD binding to VEGFR2 and 3, respectively. VEGFR activation can promote cell proliferation, migration, and growth via the mitogen-activated protein kinase (MAPK) and phosphoinositide 3-kinases (PI3K) pathways, leading to angiogenesis and tumor angiogenesis (Ivy et al., 2009). VEGF inhibitors used in CRC treatment include monoclonal antibodies (mAbs) like bevacizumab, ramucirumab, Ziv-aflibercept, as well as tyrosine kinase inhibitors (TKIs), such as sunitinib, sorafenib, fruquintinib, and regorafenib. These drugs target the VEGF pathway to inhibit angiogenesis and tumor growth (Figure 2).
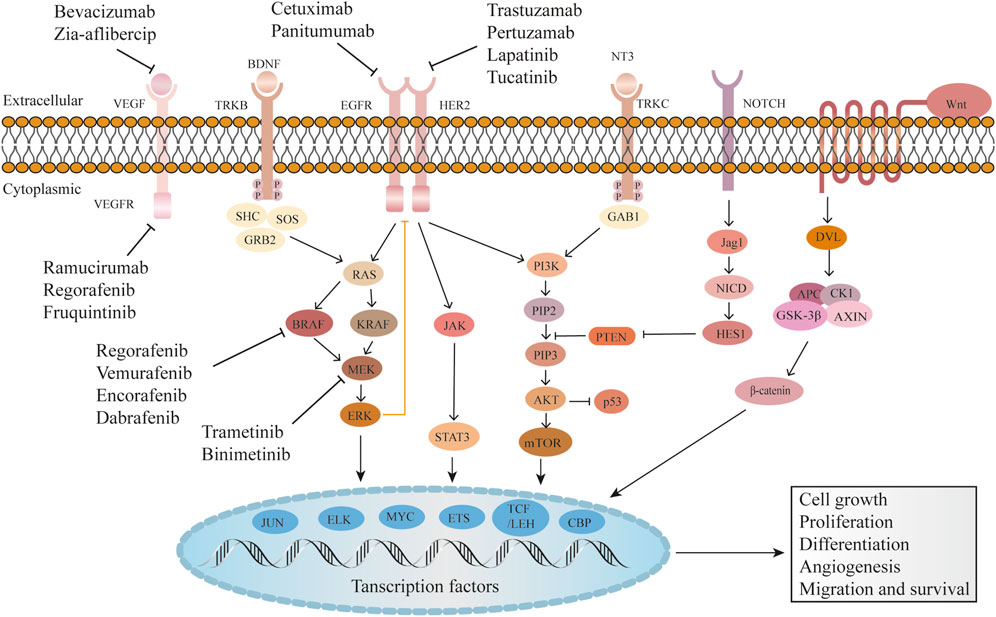
FIGURE 2. Common molecular targets and their mechanisms of action in CRC.
Epidermal growth factor receptor (EGFR), also known as ERBB1 or human epidermal growth factor receptor (HER) 1, is a member of the HER family, which also includes HER2–4. EGFR promotes tumor cell proliferation, differentiation, growth, and distant metastasis by activating downstream signaling pathways, such as PI3K and MAPK (Roskoski, 2014; Kumagai et al., 2021). EGFR activation induces the secretion of angiogenic factors, such as VEGF, which stimulate the formation of new blood vessels. Increased angiogenesis ensures sufficient blood supply to the tumor, facilitating its expansion and providing nutrients for sustained growth. Additionally, EGFR signaling provides anti-apoptotic signals through the activation of AKT, which inhibits apoptosis by inactivating pro-apoptotic proteins (De Luca et al., 2008). This allows cancer cells to evade programmed cell death and survive in unfavorable conditions. Furthermore, HER2 overexpression, as a member of the EGFR family, inhibits the tumor suppressor gene, p53 (Ménard et al., 2003). Common EGFR inhibitors used in cancer treatment include anti-EGFR mAbs, such as cetuximab and panitumumab, EGFR TKIs like gefitinib, erlotinib, and afatinib, as well as HER2 mAbs trastuzumab and pertuzumab, and HER2 TKI lapatinib. The inhibitors target EGFR and HER2, blocking their signaling pathways and inhibiting tumor growth and progression.
The RAS/RAF/MEK/ERK signaling cascade (MAPK) pathway is one of the downstream EGFR pathways, which mainly regulates cell proliferation and differentiation. RAS family members include KRAS, NRAS, and HRAS (Karnoub and Weinberg, 2008). KRAS mutation (MT) accounts for approximately 32%–40% of CRC cases, and BRAF V600E MT accounts for 5%–15% (De Roock et al., 2011; Pakneshan et al., 2013). MEK, or MAPK/ERK kinase, plays a pivotal role as a mediator in the downstream signaling of the MAPK pathway. ERK, also known as extracellular signal-regulated kinase, is a critical component of this pathway (Downward, 2003). Studies have confirmed that MEK/ERK inhibitors significantly enhance the treatment efficacy in patients with KRAS/BRAF-mutant tumors (Hatzivassiliou et al., 2013; Morris et al., 2013). Available inhibitors targeting the RAS/RAF/MEK/ERK pathway include dabrafenib and vemurafenib as BRAF inhibitors, and trametinib and encorafenib as MEK inhibitors. Additionally, there are ERK inhibitors such as ulixertinib and temuterkib.
PI3K is an enzyme that plays a crucial role in cellular signaling pathways involved in cell growth, survival, and metabolism. It functions by phosphorylating the lipid phosphatidylinositol 4,5-bisphosphate (PIP2) to generate phosphatidylinositol 3,4,5-trisphosphate (PIP3), which in turn activates downstream signaling pathways. PIP3 acts as a docking site for AKT, facilitating its activation through phosphorylation. Notably, one of the significant downstream AKT targets the mammalian target of rapamycin (mTOR), which plays a critical role in protein synthesis, cellular growth, and metabolic regulation. Aberrant activation of PI3K can occur through various mechanisms, including genetic mutations, PI3K genes amplification, or upstream receptors activation such as EGFR. Dysregulation of the PI3K/AKT/mTOR pathway has been implicated in various diseases, including cancer, highlighting its significance as a therapeutic target for intervention and treatment strategies (Fruman and Rommel, 2014; Polivka and Janku, 2014; Janku et al., 2018). Several inhibitors have been developed to target the PI3K/AKT/mTOR pathway. These include PI3K inhibitors such as buparlisib and sonolisib, which specifically target the PI3K enzyme and AKT inhibitors like MK-2206 and ipatasertib that block the activity of the AKT protein, a downstream effector of PI3K. Sirolimus and everolimus are targeted towards mTOR, a key component of the pathway. Additionally, dual PI3K/mTOR inhibitors such as dactolisib and apitolisib simultaneously target PI3K and mTOR.
NOTCH signaling involves the activation of NOTCH receptors by ligands such as JAG1, resulting in the release of the Notch intracellular domain (NICD). The NICD then translocates to the nucleus and forms a complex with transcriptional regulators to activate target genes, including the hairy and enhancer of split (HES) family genes. This signaling pathway plays a crucial role in cell fate determination, differentiation, and various cellular processes (Siebel and Lendahl, 2017; Li et al., 2023). NOTCH receptors mAbs such as tarextumab and demcizumab, have been developed and tested in preclinical and clinical studies.
The Wnt signaling pathway plays a critical role in various biological processes, including embryonic development, tissue homeostasis, and cell proliferation. Dysregulation of this pathway has been implicated in several diseases, particularly cancer. Recruitment and activation of Disheveled (Dvl) are initiated by the activation of the Wnt signaling pathway. Subsequently, a complex involving Adenomatous Polyposis Coli (APC), glycogen synthase kinase 3β (GSK-3β), Casein kinase 1 (CK1), and Axin forms, leading to phosphorylation and inhibition of GSK3β (Duchartre et al., 2016; Zhang and Wang, 2020). This, in turn, results in increased levels of β-catenin, a pivotal component of the Wnt signaling pathway, which drives cancer cell proliferation. WNT974 and CGX1321, inhibitors targeting the Wnt ligand/receptor interface, have shown promising efficacy in preclinical studies (Rodon et al., 2021a; Rodon et al., 2021b).
The tropomyosin receptor kinase (TRK) family comprises TRK A–C, which is encoded by neurotrophic TRK (NTRK)1–3. NTRK gene fusion occurs when the 3′region of the NTRK gene and 5′end of the fusion chaperone gene are connected by intra-chromosome or inter-chromosome rearrangement. The protein encoded by the fusion gene can bind to TRK and activate the downstream PI3K and MAPK pathways, resulting in tumor growth, proliferation, and differentiation. NTRK gene fusion was first identified in patients with CRC and then in those with other tumors (Martin-Zanca et al., 1986; Vaishnavi et al., 2015; Amatu et al., 2019; Solomon et al., 2019). Entrectinib, which targets the NTRK fusion gene, has been shown to be highly therapeutic for patients with NTRK. (2019).
Bevacizumab specifically binds to VEGF, blocking its interaction with the receptor, degrading existing tumor blood vessels, normalizing surviving ones, and inhibiting tumor neovascularization to exert antitumor effects.
The QUASAR 2 study showed that CRC patients treated with capecitabine (Cap) + bevacizumab or only Cap after radical (R0) resection had 3-year disease-free survival (DFS) rates of 75.4% and 78.4%, respectively (Kerr et al., 2016). Similarly, the NSABP protocol C-08 and other studies (Allegra et al., 2011; de Gramont et al., 2012; André et al., 2020) confirmed that neoadjuvant chemotherapy with bevacizumab in combination with oxaliplatin did not increase DFS in patients compared to that in patients treated with chemotherapy alone. Overall, none of these trials showed a significant survival benefit for CRC patients treated with adjuvant bevacizumab; therefore, none of the current guidelines recommend the use of bevacizumab as adjuvant therapy. Adjuvant and neoadjuvant treatment trials in mCRC are summarized in Table 1.
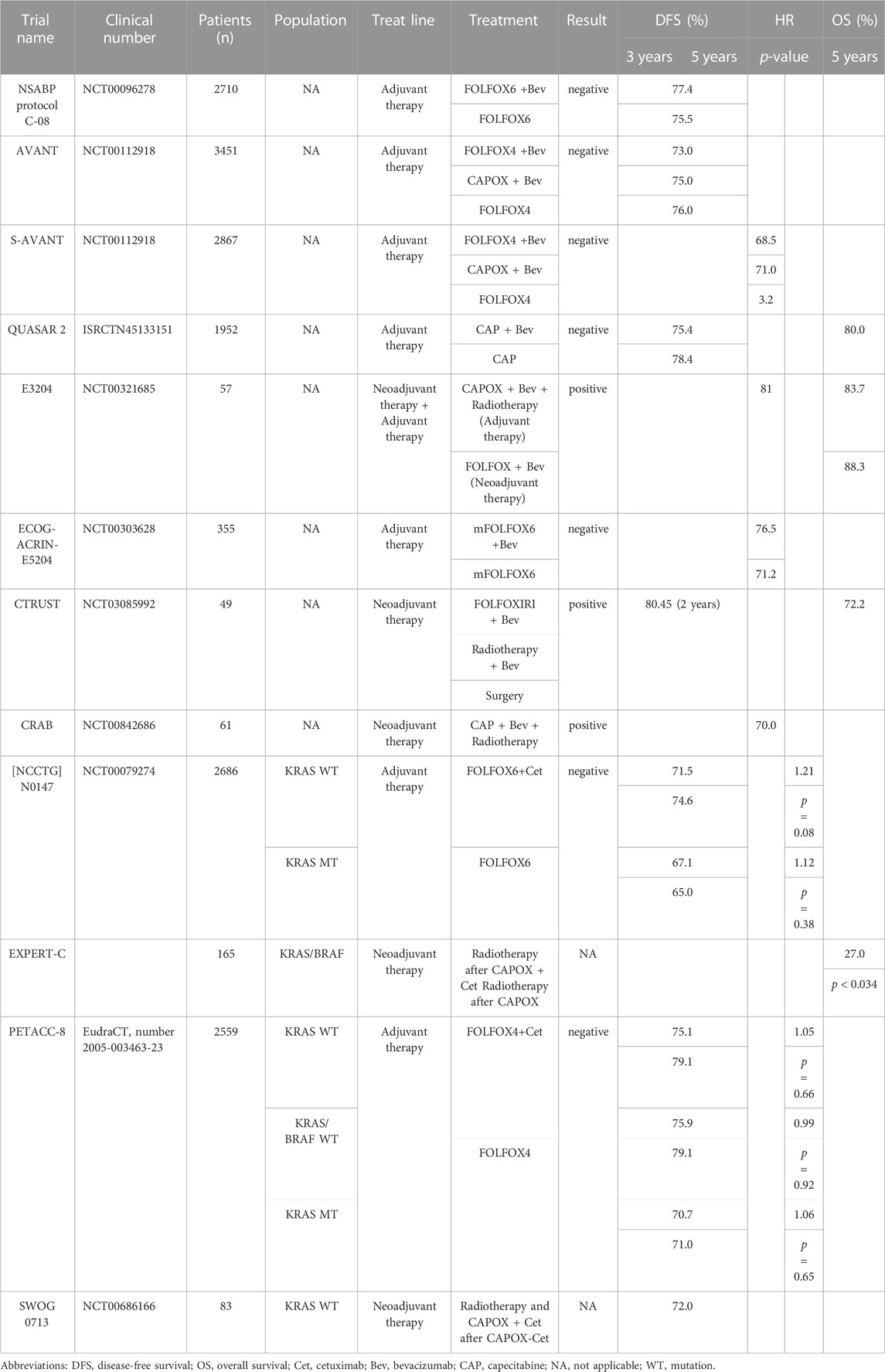
TABLE 1. Adjuvant and neoadjuvant treatment trials in mCRC.
A previous study showed that six cycles of bevacizumab in combination with chemotherapy, followed by chemoradiotherapy (CRT) achieved an objective response rate (ORR) of 88.9% in locally advanced colorectal patients with T4 or high-risk T3, with R0 resection rate of 97.8% (Masi et al., 2019). Similarly, the CRAB study reported a 95% R0 resection rate in patients with stage II/III rectal cancer treated with neoadjuvant bevacizumab + CRT (Velenik et al., 2020). Although these studies reported positive outcomes, available evidence is insufficient to support the adoption of bevacizumab as a standard neoadjuvant (Table 1).
The AVF2107 study showed the administration of FOLFIRI + bevacizumab as a first-line treatment significantly improved (p < 0.001) the median overall survival (mOS; 20.3 vs. 15.6 months) and median progression-free survival (mPFS; 10.6 vs. 6.2 months) of mCRC patients compared to those of the mCRC patients treated with chemotherapy alone (Hurwitz et al., 2004). This finding facilitated the approval of bevacizumab by the United States Food and Drug Administration (FDA) as a first-line mCRC treatment in 2004. Additionally, the administration of bevacizumab + chemotherapy significantly increased (p = 0.0023) the mPFS of patients compared to that of the patients treated with chemotherapy alone (9.4 vs. 8.0 months) but did not affect mOS (Saltz et al., 2008). Moreover, both the MAVERICC (Parikh et al., 2019) and ARIES studies (Bendell et al., 2012) confirmed that FOLFIRI or FOLFOX + bevacizumab had similar PFS and OS.
However, the TRIBE2 study (Cremolini et al., 2020) showed that FOLFOXIRI + bevacizumab achieved higher mOS (27.4 vs. 22.5 months) and mPFS (19.2 vs. 16.4 months) than mFOLFOX6 + bevacizumab. The treatment benefit was independent of RAS and BRAF mutation status but was better in patients with right-sided tumors, and the same benefit was achieved in patients who progressed after treatment with FOLFOXIRI + bevacizumab (Loupakis et al., 2015; Cremolini et al., 2018b). Moreover, both the AVEX (Cunningham et al., 2013) and PRODIGE20 (Aparicio et al., 2018a) studies confirmed that bevacizumab provided increased treatment benefits in elderly patients and did not induce adverse events. Key trials of anti-VEGF agents in the treatment of mCRC are illustrated in Table 2.
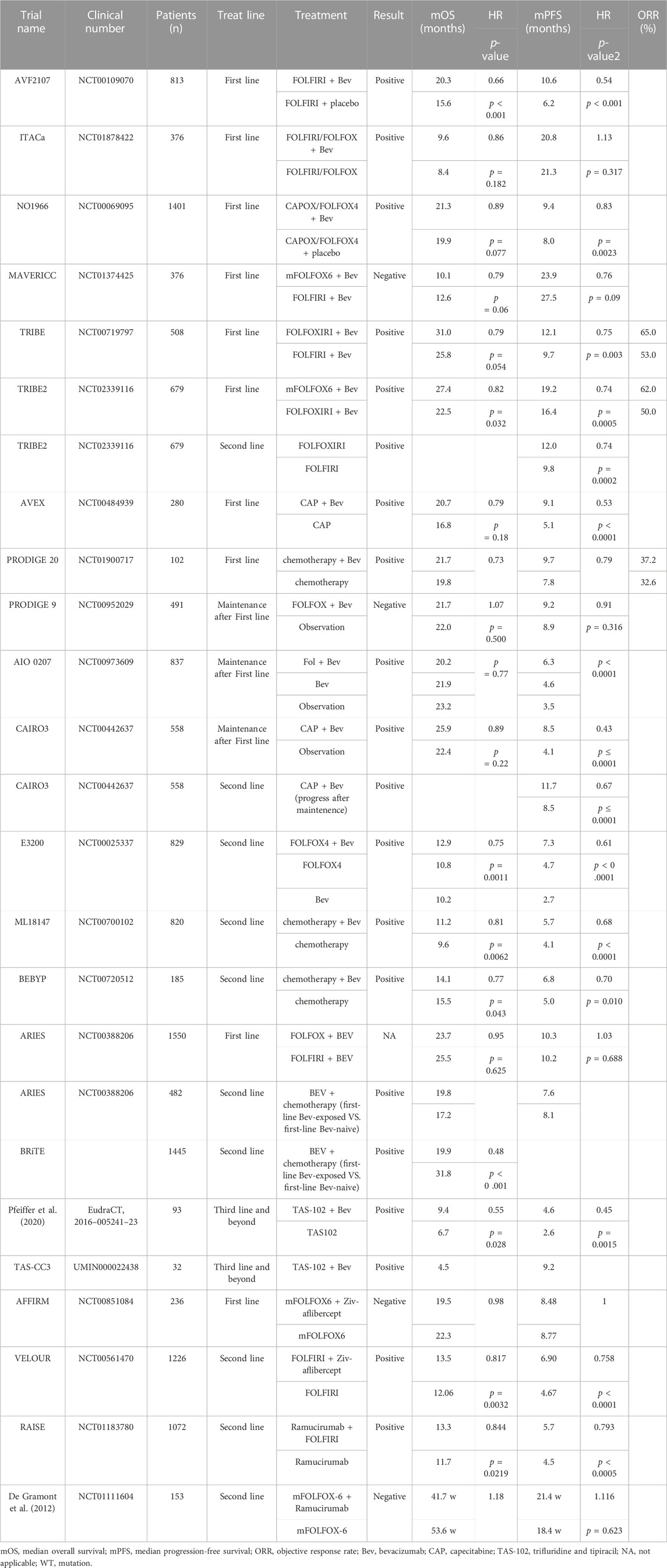
TABLE 2. Key trials of anti-VEGF agents in the treatment of mCRC.
In the CAIRO3 study (Simkens et al., 2015), bevacizumab + Cap was used as maintenance treatment for mCRC patients after first-line treatment with chemotherapy + bevacizumab that led to improved mPFS (8.5 vs. 4.1 months, p < 0.0001); however, the maintenance treatment did not affect OS. Similarly, both the PRODIGE9 (Aparicio et al., 2018b) and AIO0207 (Hegewisch-Becker et al., 2015) studies confirmed bevacizumab-induced improvement in PFS after induction chemotherapy. Moreover, the 2016 ESMO guidelines state that Cap + bevacizumab can be used for maintenance therapy after first-line treatment, but bevacizumab alone is not recommended for maintenance therapy. Additionally, the National Comprehensive Cancer Network (NCCN) guidelines do not recommend bevacizumab as maintenance therapy.
The E3200 study (Giantonio et al., 2007) showed that the administration of bevacizumab as a second-line treatment in mCRC patients achieved mOS of 12.9, 10.2, and 10.8 months and mPFS of 7.3, 2.7, and 4.7 months in patients subjected to FOLFOX + bevacizumab, bevacizumab only, or chemotherapy only first-line therapies, respectively. Thus, bevacizumab was approved in 2006 as a second-line treatment for patients with mCRC. Additionally, the ML18147 study showed that the administration of chemotherapy + bevacizumab or chemotherapy only as a second-line treatment achieved mOS of 11.2 vs. 9.6 months (p = 0.0062) and mPFS of 5.7 vs. 4.1 months (p < 0.0001), respectively, in mCRC patients subjected to bevacizumab as a first-line therapy (Bennouna et al., 2013). Moreover, the ML18147 and several other studies confirmed that retreatment with bevacizumab-containing regimens exerted significant therapeutic effects in mCRC patients who received bevacizumab-containing regimens as first-line therapy (Grothey et al., 2008; Hurwitz et al., 2014). Based on these findings, the FDA approved bevacizumab as a cross-line therapy in 2013.
A previous study showed that trifluridine and tipiracil (TAS-102) + bevacizumab was more effective than TAS-102 alone as a third-line treatment in patients with anti-EGFR positive and chemotherapy-resistant mCRC, with considerable increase in mOS (9.4 vs. 6.7 months, p = 0.028) and mPFS (4.6 vs. 2.6 months, p = 0.0010) (Pfeiffer et al., 2020). Similarly, the TAS-CC3 study confirmed the positive effects of TAS-102 + bevacizumab as a third-line treatment in Asian patients with mCRC (Yoshida et al., 2021). Accordingly, the NCCN guidelines recommend the use bevacizumab in combination with TAS-102 as a third-line treatment in patients with mCRC (Table 2).
Ziv-aflibercept is an anti-VEGF agent that inhibits neovascularization by tightly binding to VEGF and reducing vascular permeability. The AFFIRM study showed (Folprecht et al., 2016) that abatacept did not achieve promising outcomes as a first-line treatment for mCRC. However, considerable therapeutic benefit was obtained with Ziv-aflibercept as a second-line treatment (Van Cutsem et al., 2012). Notably, FOLFIRI + Ziv-aflibercept was more effective than FOLFIRI only as a second-line treatment in mCRC patients, with improved mOS (13.5 vs. 12.06 months, p = 0.0032) and mPFS (6.90 vs. 4.67 months, p < 0.0001). Accordingly, Ziv-aflibercept was approved by the FDA as a second-line treatment for mCRC patients who progressed or were resistant to first-line oxaliplatin therapy in 2012 (Table 2).
Cetuximab binds specifically to EGFR and competitively blocks VEGF and other receptors, inhibiting intracellular signaling pathways, thereby suppressing the proliferation of cancer cells and inducing apoptosis.
In the N0147 [NCCTG] study (Alberts et al., 2012), mFOLFOX + cetuximab did not show significant health-promoting effects as an adjuvant compared to those of chemotherapy alone, with no statistical difference in 3-year DFS in patients with KRAS wild-type (WT). Moreover, the PETACC-8 (Taieb et al., 2014) study confirmed that cetuximab adjuvant therapy had no survival benefit in patients with KRAS WT. Current guidelines do not recommend the use of cetuximab as an adjuvant therapy (Table 1).
The EXPERT-C study (Dewdney et al., 2012) showed that CAPOX + cetuximab was more effective than CAPOX only (four cycles each) in neoadjuvant therapy, with significantly higher response rate (RR) and OS in the cetuximab group. However, some studies, including the COIN study (Maughan et al., 2011; Tveit et al., 2012), showed that cetuximab treatment did not improve patient survival; in contrast, the TAILOR study (Qin et al., 2018) confirmed cetuximab OS benefit. The 2012 NCCN guidelines do not recommend cetuximab as a neoadjuvant therapy because of insufficient evidence (Table 1).
The CRYSTAL study (Van Cutsem et al., 2009) showed that treatment with FOLFIRI + cetuximab significantly increased mOS (24.9 vs. 21.0 months) and mPFS (9.9 vs. 8.7 months) in patients with KRAS WT mCRC compared to those in patients with KRAS WT treated with FOLFIRI treatment alone. Accordingly, cetuximab was approved by the FDA in 2012 as a first-line treatment in patients with KRAS WT mCRC. In contrast, the COIN (Maughan et al., 2011) and NORDIC-VII (Tveit et al., 2012) studies showed insignificant differences in OS and PFS between oxaliplatin + cetuximab and oxaliplatin treated patients with KRAS WT mCRC. However, the TAILOR study (Qin et al., 2018) showed that cetuximab + FOLFOX increased mPFS (9.2 vs. 7.4 months, p = 0.004) and mOS (20.7 vs. 17.8 months, p = 0.02) in patients with RAS WT mCRC compared to those in FOLFOX alone treated patients with RAS WT mCRC. Moreover, previous studies have shown that cetuximab was as effective as bevacizumab in patients with RAS WT (Heinemann et al., 2014; Venook et al., 2017). Additionally, the NCT00208546 study showed insignificant difference in efficacy between cetuximab + bevacizumab and cetuximab only (Tol et al., 2009); therefore, cetuximab + bevacizumab is not recommended for patients with mCRC.
The CALGB/SWOG80405 (Alliance) study (Venook et al., 2017) found that cetuximab achieved significantly higher OS and PFS in patients with left-sided primary tumors than in those with right-sided primary tumors. Several studies confirmed that anti-EGFR antibody in combination with chemotherapy exerted the best effects in patients with left-sided primary tumors and RAS WT mCRC (Arnold et al., 2017; Tejpar et al., 2017). Pivotal trials of anti-EGFR monoclonal antibody treatment in mCRC are summarized in Table 3.
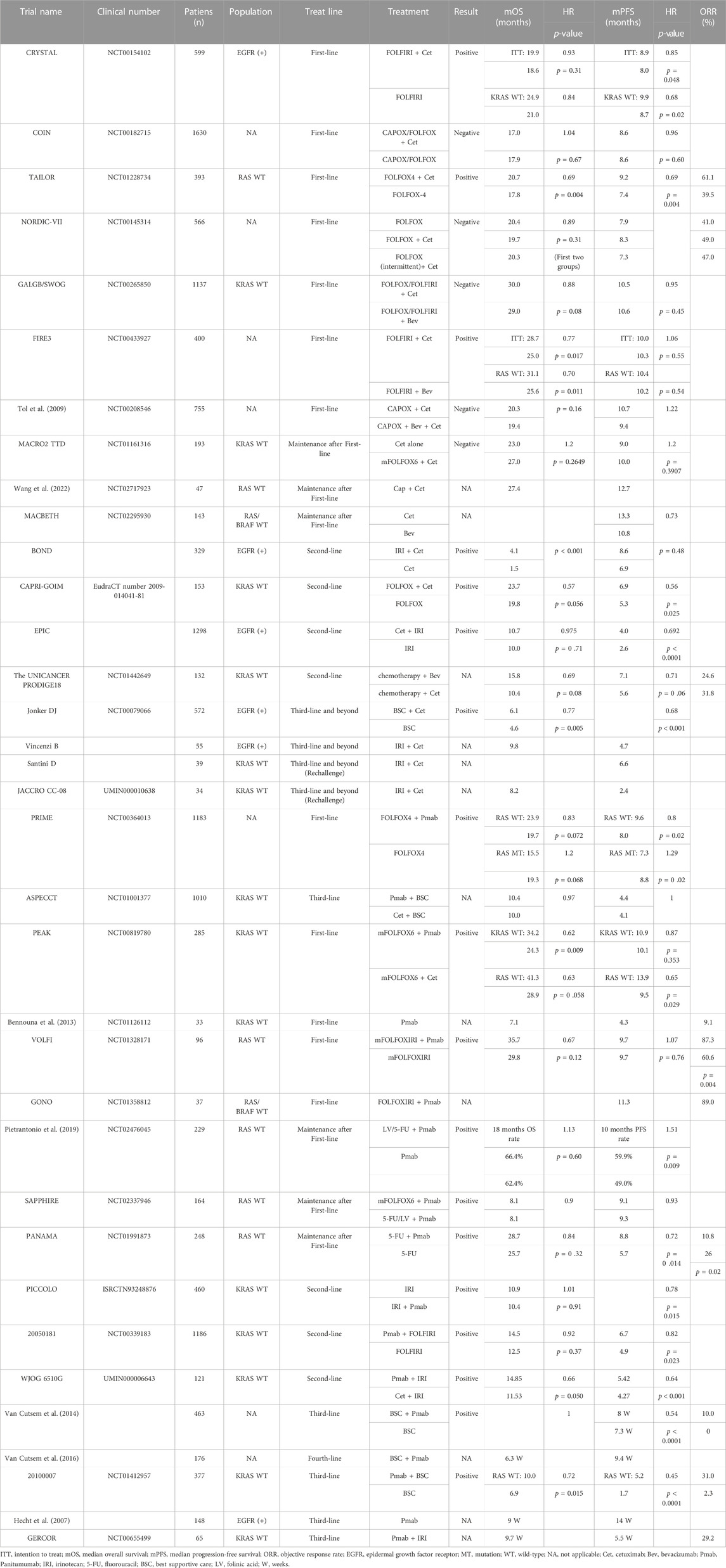
TABLE 3. Pivotal trials of anti-EGFR mAbs treatment in mCRC.
The MACRO2TTD study (Aranda et al., 2018) confirmed insignificant differences in mPFS and mOS between continuation of the original regimen and maintenance treatment with cetuximab alone after induction therapy with mFOLFOX + cetuximab. Moreover, the MACBETH study (Cremolini et al., 2018a) suggested that cetuximab could be used for maintenance therapy in patients with RAS/RAF WT mCRC. However, current guidelines do not recommend the use of cetuximab for maintenance therapy.
The BOND study (Cunningham et al., 2004) confirmed that cetuximab in combination with chemotherapy achieved a better therapeutic benefit than cetuximab alone in mCRC treatment, with increase in mOS (8.6 vs. 6.9 months, p = 0.48) and mPFS (4.1 vs. 1.5 months, p < 0.001). Cetuximab was approved by the FDA in 2004 as a second-line treatment for patients with mCRC. Subsequent studies (Sobrero et al., 2008; Ciardiello et al., 2016) have confirmed the therapeutic benefit of cetuximab in combination with chemotherapy over chemotherapy alone. Moreover, the UNICANCERPRODIGE18 study (Bennouna et al., 2019) showed that cetuximab had therapeutic benefits comparable to those of bevacizumab as second-line treatment.
The NCT00079066 study (Jonker et al., 2007) demonstrated that cetuximab monotherapy resulted in higher OS and PFS in patients with refractory mCRC than the best supportive care (BSC) alone. Vincenzi et al. (2006) treated patients with mCRC using cetuximab + irinotecan as third-line chemotherapy, with an mPFS of 4.7 months and mOS of 9.8 months.
Rechallenge therapy means the reintroduction of targeted agent to which a tumor has already proven to be resistant (Tonini et al., 2013). Santini et al. (2012) performed cetuximab rechallenge as a third-line treatment for refractory mCRC and achieved promising results, with ORR of 53.8% [partial response (PR), 48.7%; complete response (CR), 5.1%] and mPFS of 6.6 months. Similarly, patients with KRAS WT mCRC rechallenged with cetuximab as third-line treatment exhibited positive results, with mPFS and OS of 2.4 and 8.2 months, respectively (Masuishi et al., 2020). A meta-analysis conducted by Mauri et al. (2019) showed that anti-EGFR rechallenge therapy yielded better therapeutic benefits than sequential and dose escalation therapies. Therefore, cetuximab could be used as a third-line treatment (Table 3).
Panitumumab is an IgG2 monoclonal antibody that binds to EGFR, blocking the binding of VEGFR and VEGF and inhibiting cancer cell growth.
The PRIME study (Douillard et al., 2010) showed that treatment with FOLFOX4 + panitumumab significantly improved mPFS in patients with KRAS WT mCRC compared to that in patients with KRAS WT mCRC treated with FOLFOX4 alone (9.6 vs. 8.0 months, p = 0.02) but did not affect OS and was not significant in patients with KRAS MT. Moreover, the ASPECCT trial (Price et al., 2014) confirmed that panitumumab achieved results comparable to those of cetuximab in patients with KRAS WT mCRC. Based on these findings, panitumumab was approved by the FDA as a first-line treatment for patients with KRAS WT mCRC in 2014. A retrospective analysis of the PRIME study (Douillard et al., 2013) showed that all patients with RAS WT benefited from panitumumab treatment. Interestingly, the PEAK study (Schwartzberg et al., 2014) showed that panitumumab had better efficacy than bevacizumab in patients with KRAS/NRAS WT mCRC. Therefore, the FDA included NRAS WT mCRC as an indication for panitumumab treatment in 2017. Additionally, studies (Arnold et al., 2017; Boeckx et al., 2017; Peeters et al., 2018) have shown that panitumumab was more effective against RAS WT tumors located on the left side than those on the right side.
Furthermore, although treatment with mFOLFOXIRI + panitumumab did not significantly affect mOS and mPFS in patients with RAS WT mCRC, there was a significant increase (p = 0.004) in ORR (87.3% vs. 60.6%, p = 0.004) and metastasis resection-free recurrence survival (7.9 vs. 4.0 months) in the mFOLFOXIRI + panitumumab group compared to those in the mFOLFOXIRI group (Modest et al., 2019a). Similar results were found in the GONO study (Fornaro et al., 2013). Overall, panitumumab + FOLFOXIRI could be used for patients with RAS WT mCRC with metastases that require surgical resection.
The NCT02476045 study (Pietrantonio et al., 2019) showed that 5-Fu + panitumumab was more effective than 5-Fu only as maintenance treatment in patients with RAS WT mCRC, with 10-month PFS of 59.9% and 49.0% (p = 0.01) in the 5-Fu + panitumumab and 5-Fu groups, respectively. Additionally, there were no significant differences in PFS, OS, and RR between panitumumab + mFOLFOX6-and 5-Fu + panitumumab-treated patients with RAS WT mCRC (Munemoto et al., 2019). Moreover, the PANAMA study (Modest et al., 2022) confirmed that 5-Fu + panitumumab was a better maintenance treatment than 5-Fu alone. A retrospective analysis of the PRIME and PEAK studies confirmed that panitumumab was comparable to bevacizumab as a maintenance therapy (Modest et al., 2019b), indicating that panitumumab could be combined with other agents as a maintenance therapy for patients with RAS WT mCRC.
The PICCOLO study (Seymour et al., 2013) showed that irinotecan + panitumumab was effective as a second-line treatment against KRAS WT mCRC than irinotecan only, as evidenced by a significant increase in PFS and RR in the panitumumab group; however, the OS was not significantly affected. Moreover, panitumumab had limited effects on patients with RAS MT. Similar results were obtained in the 20050181 study (Peeters et al., 2010; Peeters et al., 2014); therefore, panitumumab and cetuximab are sometimes used interchangeably as second-line treatments.
Cutsem Eric Van Cutsem et al. (2007) reported that panitumumab monotherapy as a third-line treatment significantly increased (p < 0.0001) mPFS to 8 weeks in patients with mCRC compared to that in patients with mCRC treated with BSC only (7.3 weeks) but did not affect OS. Accordingly, panitumumab was approved by the FDA as a third-line treatment for patients with EGFR-positive mCRC in 2006. Similar results were observed in patients retreated with panitumumab + BSC (Van Cutsem et al., 2008). Overall, several studies have confirmed the efficacy of panitumumab monotherapy as a third-line treatment for mCRC (Hecht et al., 2007; Kim et al., 2016; Kim et al., 2018). Moreover, the GERCOR (André et al., 2013) and WJOG6510G (Sakai et al., 2020) studies both confirmed that panitumumab + irinotecan improved PFS in patients with KRAS WT mCRC but did not affect OS (Table 3).
Ramucirumab exerts its antitumor effects by specifically binding to VEGFR-2 and inhibiting tumor angiogenesis. The RAISE study (Tabernero et al., 2015) showed that treatment with FOLFIRI + ramucirumab increased mOS (p = 0.0219) and mPFS (p < 0.0005) to 13.3 and 5.7 months, respectively, compared with 11.7 and 4.5 months, respectively, in FOLFIRI-treated patients. Moreover, the treatment benefit of ramucirumab was superior to chemotherapy-only for both OS and PFS in any subgroup. Ramucirumab was approved as a second-line treatment for patients with mCRC by the FDA in 2015 (Table 3).
Fruquintinib is a VEGFR inhibitor that blocks neointimal growth associated with tumor proliferation and is a potent and highly selective small-molecule inhibitor of VEGFR1–3. The FRESCO study (Li et al., 2018) showed that fruquintinib + BSC treatment achieved considerable therapeutic effects in mCRC patients, irrespective of whether the patients were previously treated with anti-VEGF or anti-EGFR drugs, as evidenced by an increase (p < 0.001) in mOS (9.3 months) and mPFS (3.7 months) compared to those in mCRC patients treated with the BSC only (mOS, 6.6 months; mPFS, 1.8 months). Accordingly, fruquintinib was approved by the China National Medical Products Administration as a third-line treatment for patients with mCRC in 2018; however, fruquintinib has not been approved for use in other countries. Similarly, the results of FRESCO-2 study showed that fruquintinib treatment significantly improved (p < 0.001) mOS (7.4 months) and mPFS (3.7 months) compared to those of BSC treatment (mOS, 4.8 months; mFPS, 1.8 months) (Dasari et al., 2022). Key trials of HER2 targeted agents and TKIs in mCRC are summarized in Table 4.
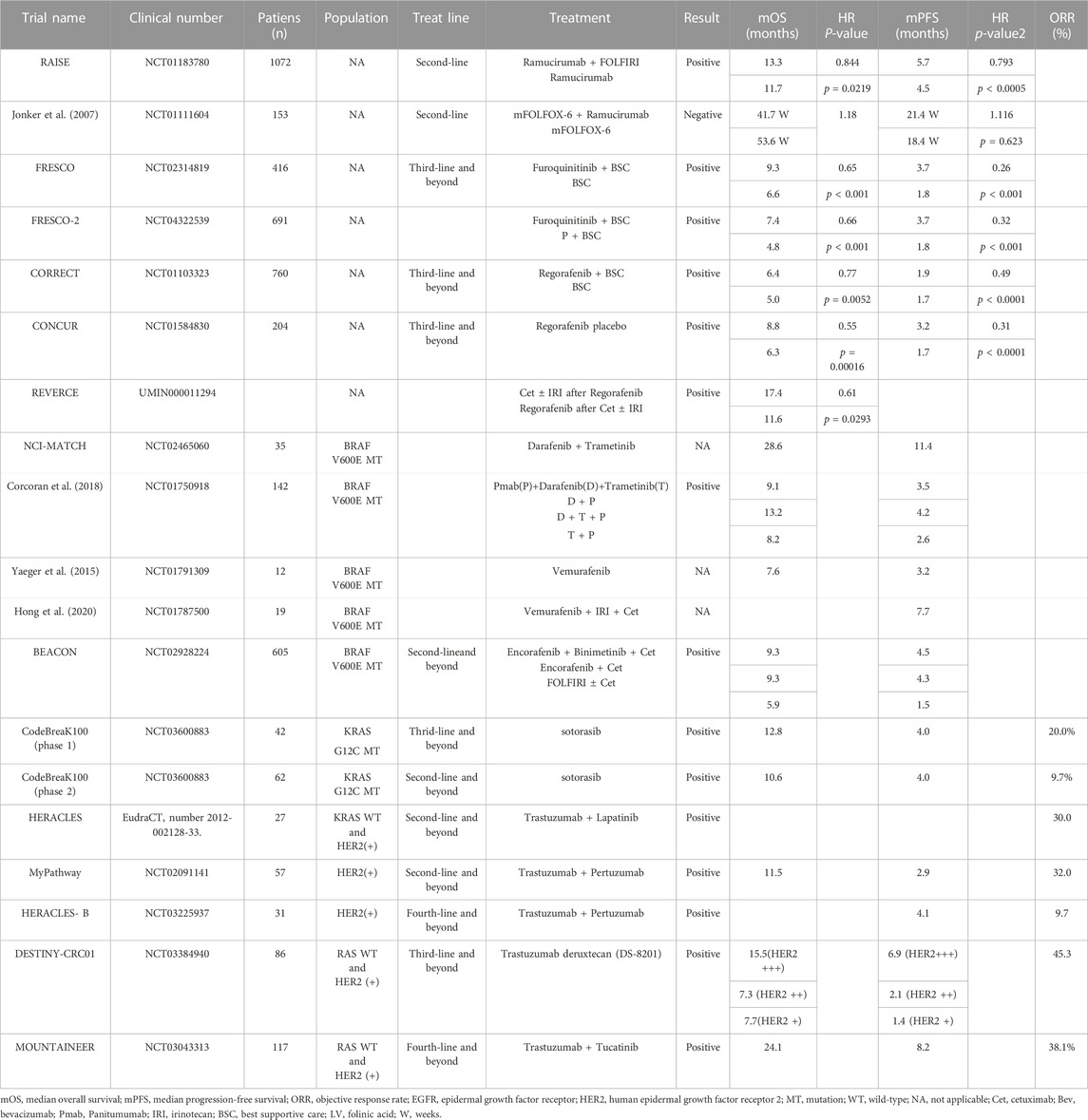
TABLE 4. Major trials of HER2 mAbs and all TKIs in mCRC.
Regorafenib is a TKI that acts on multiple targets, such as VEGFR and BRAF V600E. The CORRECT study (Grothey et al., 2013) showed that regorafenib + BSC improved mOS (6.4 months) and mPFS (1.9 months) in patients with mCRC compared to patients with mCRC treated with BSC only (mOS, 5 months; mPFS, 1.7 months). Accordingly, regorafenib was approved as a third-line treatment for patients with mCRC by the FDA in 2012. The CONCUR study (Li et al., 2015) demonstrated the benefits of regorafenib in Asian population. Regorafenib is the only monotherapy recommended by the NCCN guidelines for third-line therapy and further treatment (Table 4).
Encorafenib primarily targets the BRAFV600E MT, which is commonly found in certain types of cancer. Additionally, it has inhibitory effects on JNK1–3, LIMK1–4, and STK36. The BEACON study (Kopetz et al., 2019) showed that encorafenib + binimetinib + cetuximab triple-agent treatment exerted considerable therapeutic effects in mCRC patients compared to those in the mCRC patients treated with FOLFIRI + cetuximab (control). However, subsequent studies showed insignificant differences in OS and mPFS between encorafenib + binimetinib + cetuximab and encorafenib + cetuximab groups (Tabernero et al., 2021). Accordingly, the NCCN guidelines recommend the use of encorafenib in combination with anti-EGFR as a second-line treatment in patients with BRAFV600E MT mCRC (Table 4).
Dabrafenib specifically targets BRAF mutations (V600E and V600K), while trametinib selectively inhibits MEK1 and MEK2, key components of the RAS/RAF/MEK/ERK signaling pathway, resulting in the tumor growth suppression. The NCT01072175 study (Corcoran et al., 2015) showed that combined second-line treatment with dabrafenib (BRAF inhibitor) and trametinib (MEK inhibitor) increased mPFS to 3.5 months in patients with BRAF V600E MT mCRC, with PR observed in 12% of the patients and CR in one patient. Similarly, the NCT01750918 study (Corcoran et al., 2018) showed that panitumumab + dabrafenib + trametinib treatment increased RR (21%), mPFS (4.2 months), and mOS (13.2 months) in patients with BRAFV600E MT mCRC compared to those in patients with BRAFV600E MT mCRC treated with panitumumab + dabrafenib or panitumumab + trametinib. Therefore, the 2020 NCCN guidelines recommend that dabrafenib + trametinib could be combined with cetuximab or panitumumab as a second-line treatment for BRAFV600E MT mCRC. However, the 2021 and 2022 NCCN guidelines do not include dabrafenib and trametinib in combination with anti-EGFR for mCRC treatment (Table 4).
Vemurafenib is a targeted therapy that specifically inhibits the mutated BRAF form, BRAFV600E. A combination of vemurafenib and panitumumab has been shown to have a 100% tumor shrinkage rate, mPFS of 3.2 months, and mOS of 7.6 months in patients with BRAFV600E MT mCRC (Yaeger et al., 2015). Similarly, RR of 35% and mPFS of 7.7 months was obtained in patients with BRAFV600E MT mCRC treated with a combination of irinotecan, vemurafenib, and cetuximab (Hong et al., 2016). Additionally, the SWOGS1406 study (Kopetz et al., 2021) showed that irinotecan + cetuximab + vemurafenib treatment significantly increased PFS in patients with BRAFV600E MT mCRC compared to patients with BRAFV600E MT mCRC administered treatment regimens without vemurafenib. Moreover, FOLFIRI + cetuximab + vemurafenib treatment achieved an ORR of 81%, mPFS of 9.7 months, and mOS of 15.4 months in patients with BRAFV600E MT mCRC (Wang et al., 2022). Overall, these results confirmed that vemurafenib plus anti-EGFR can achieve significant efficacy in patients with BRAF MT mCRC; however, vemurafenib is yet to be approved for use in mCRC patients owing to shortage of relevant trials and limited number of enrolled patients (Table 4).
Sotorasib and adagrasib are potent inhibitors of KRASG12C, specifically designed to target this mutation and act as antineoplastic agents. These agents selectively bind to and inhibit the mutant KRASG12C protein, offering potential therapeutic options for patients with KRASG12C MT cancers. In the phase 1 CodeBreaK100 study (Fakih et al., 2022) involving KRASG12C MT solid tumors, sotorasib treatment resulted in a median mPFS of 4.0 months and an ORR of 7.1% in the mCRC group. In the phase 2 study specifically conducted with mCRC patients, the ORR was 12.9%, with a mOS of 10.6 months and mPFS of 4.0 months (Hong et al., 2020). MRTX849 study (Klempner et al., 2022) showed that adagrasib + cetuximab mPFS was 6.9 vs. 5.6 months in adagrasib only group, and ORR was 46% vs. 19. The aforementioned studies have provided evidence of sotorasib and adagrasib efficacy in the treatment of mCRC. Nevertheless, additional clinical validation is required to further substantiate their practical clinical application.
Trastuzumab and pertuzumab are monoclonal antibodies that specifically bind to different epitopes of the HER2 receptor, inhibiting HER2 signaling and enhancing immune-mediated destruction of tumor cells. In contrast, lapatinib is a TKI that targets both HER2 and EGFR receptors, effectively blocking their activation and downstream signaling pathways. The HERACLES study (Sartore-Bianchi et al., 2016) showed that trastuzumab + lapatinib treatment achieved an ORR of 30% in patients with KRAS WT and HER2-positive mCRC who previously underwent anti-EGFR therapy. Moreover, trastuzumab + pertuzumab treatment (HER2 antibodies) achieved an ORR of 32%, mPFS of 2.9 months, and mOS of 1.5 months in patients with HER2 positive mCRC (Meric-Bernstam et al., 2019) and an mPFS of 5.3 months in RAS WT subgroup. The HERACLES-B study (Sartore-Bianchi et al., 2020) showed that trastuzumab + panitumumab treatment achieved an ORR of 9.7% and mPFS of 4.1 months in patients with RAS WT and HER2-positive mCRC who had previously been treated with a third-line regimen.
Trastuzumab deruxtecan (DS-8201) is a novel antibody-drug conjugate with a humanized anti-HER2 antibody, cleavable peptide linker, and potent topoisomerase I inhibitor payload that has been confirmed to be effective in multiple solid tumors, including CRC (Tsurutani et al., 2020). The DESTINY-CRC01 study (Siena et al., 2021; Yoshino et al., 2023) treated HER2-positive mCRC patients with DS-8201 after two or more prior regimens. The patients were divided into three cohorts based on HER2 expression levels: cohort A (HER2-positive, IHC 3+ or IHC 2+/ISH+), cohort B (HER2 IHC 2+/ISH-), and cohort C (HER2 IHC 1+). The mOS in cohorts A, B, and C was 15.5, 7.3, and 7.7 months, respectively, while the mPFS was 6.9, 2.1, and 1.4 months, respectively. Notably, the ORR was observed only in cohort A, with a rate of 24%.
Tucatinib blocks proliferation and the phosphorylation of HER2 and its downstream effector, which is a TKI. MOUNTAINEER Trial (Strickler et al., 2022) rolled mCRC patients with RAS WT and HER2-positive which was treatment before but without anti-HER2, mOS was 24.1 months and mPFS was 8.2 months in the tucatinib + trastuzumab. As a result of the remarkable breakthrough in this study, the FDA granted accelerated approval in 2023 for the use of tucatinib + trastuzumab as a second-line treatment in HER2+ and RAS WT mCRC patients.
In light of the research findings mentioned above, the NCCN guidelines recommend trastuzumab in combination with either pertuzumab, lapatinib, tucatinib, or DS-8201 as second-line and beyond treatment options for patients with mCRC who have RAS WT and HER2-positive (Table 4).
Recent years have witnessed remarkable advancements in tumor research, driven by breakthroughs in sequencing technologies. These advancements have enhanced our understanding of tumors, including their genetic and genomic alterations. The knowledge provided a basis for personalized treatments, identification of new therapeutic targets, and improved diagnostic methods for different types of cancer. Particularly, the rapid progress in single-cell sequencing technology has revolutionized the field by enabling investigations at individual tumor cell level. This approach has provided unprecedented insights into tumor heterogeneity, allowing us to gain a better understanding of the diverse cellular composition within tumors and identify potential therapeutic targets. Furthermore, it has enhanced our understanding of the tumor microenvironment, including the distinct subpopulations and functions of different cells, as well as their intricate interactions. These advancements have particularly highlighted the crucial role of the tumor microenvironment in studying mechanisms of drug resistance.
In the context of targeted therapy for tumors, significant improvements have been made in terms of CRC survival rates. The current strategies for targeted therapy in mCRC are summarized in Figure 3. However, several challenges remain. Drug resistance remains an inescapable obstacle, as the development of resistance in patients often goes unnoticed until disease progression occurs. Additionally, economic costs pose a major concern, as the need for testing multiple target markers further amplifies the financial burden on patients. Moreover, adverse drug reactions are a significant consideration, especially among vulnerable populations such as the elderly and children, given the varying tolerances to drug dosages. Striking a balance between achieving optimal efficacy and minimizing adverse effects remains an ongoing area of research.
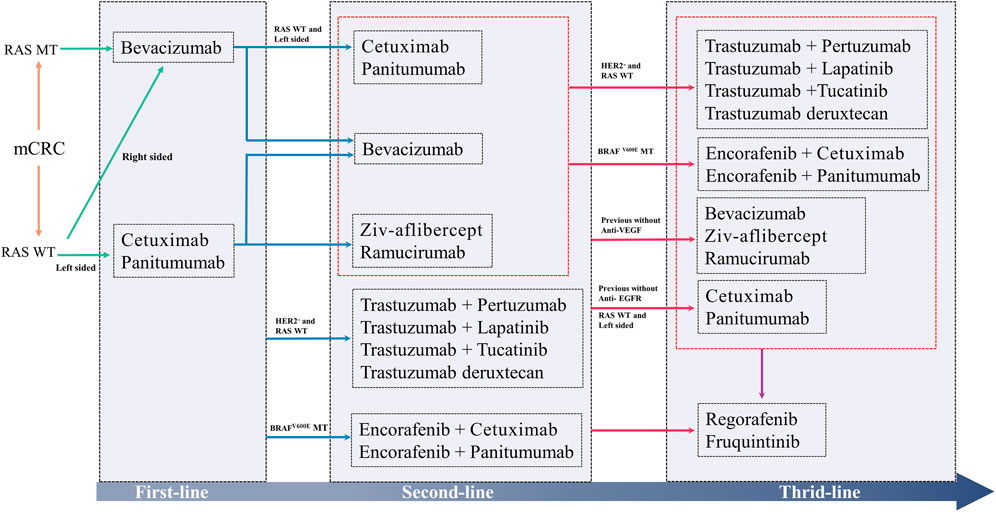
FIGURE 3. The current strategies for molecular targeted therapy in mCRC.
Furthermore, the integration of immunotherapy and molecular targeted therapy has shown potential for further improvement of the survival rates of patients with tumors, including those with mCRC. However, combination of these therapies presents its own set of challenges requiring careful consideration. Co-administration of multiple drugs can potentially intensify adverse reactions, underscoring the importance of identifying the most effective combination regimen through thorough evaluation.
In summary, scientific progress has significantly enhanced our ability to combat CRC and other tumors. While obstacles and unanswered questions remain, the field of targeted therapy continues to advance, and it is anticipated that future clinical trials and research efforts will yield major breakthroughs, further increasing the survival rates and overall outcomes for cancer patients.
SH and JY drafted the manuscript, tables and figures. XG, XH, CL assisted the literature search. RL and YaL assisted the revision. ML, LL, YoL, and JH advised on the manuscript. YaL and RL supervised and finalized the work. All authors contributed to the article and approved the submitted version.
This research was supported by Guangxi Key Research and Development Program (NO. GUIKEAB19245002), National Natural Science Foundation of China (NO.82103297, NO.82060427), Advanced Innovation Teams and Xinghu Scholars Program of Guangxi Medical University, Guangxi Medical and health key cultivation discipline construction project, Training Program for Thousands of Young and Middle-aged Backbone Teachers in Guangxi Colleges and Universities, Guangxi Medical University Outstanding Young Talents Training Program, Nanning Qingxiu District Science and Technology Project (NO. 2020037, NO. 2020038, NO. 2021007, NO. 2021010, NO. 2021012), Guangxi Medical and health key discipline construction project.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
BSC, best supportive care; CRC, colorectal cancer; CRT, chemoradiotherapy; CR, complete response; Cap, capecitabine; DFS, disease-free survival; EGFR, epidermal growth factor receptor; FDA, United States Food and Drug Administration; HES, hairy and enhancer of split; HER, human epidermal growth factor receptor; mAbs, monoclonal antibodies; MAPK, mitogen-activated protein kinase; mCRC, metastasis colorectal cancer; mOS, median overall survival; mPFS, median progression-free survival; MT, mutation; mTOR, mammalian target of rapamycin; NCCN, National Comprehensive Cancer Network; NICD, Notch intracellular domain; ORR, objective response rate; OS, overall survival; PR, partial response; PI3K, phosphoinositide 3-kinases; RR, response rate; TKI, tyrosine kinase inhibitor; TRK, tropomyosin receptor kinase; TRK, tropomyosin receptor kinase; VEGF, vascular endothelial growth factor; WT, wild-Type; 5-FU, fluorouracil.
Alberts, S. R., Sargent, D. J., Nair, S., Mahoney, M. R., Mooney, M., Thibodeau, S. N., et al. (2012). Effect of oxaliplatin, fluorouracil, and leucovorin with or without cetuximab on survival among patients with resected stage III colon cancer: A randomized trial. JAMA 307, 1383–1393. doi:10.1001/jama.2012.385
Allegra, C. J., Yothers, G., O'connell, M. J., Sharif, S., Petrelli, N. J., Colangelo, L. H., et al. (2011). Phase III trial assessing bevacizumab in stages II and III carcinoma of the colon: Results of NSABP protocol C-08. J. Clin. Oncol. 29, 11–16. doi:10.1200/JCO.2010.30.0855
Amatu, A., Sartore-Bianchi, A., Bencardino, K., Pizzutilo, E. G., Tosi, F., and Siena, S. (2019). Tropomyosin receptor kinase (TRK) biology and the role of NTRK gene fusions in cancer. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 30, viii5–viii15. doi:10.1093/annonc/mdz383
André, T., Blons, H., Mabro, M., Chibaudel, B., Bachet, J. B., Tournigand, C., et al. (2013). Panitumumab combined with irinotecan for patients with KRAS wild-type metastatic colorectal cancer refractory to standard chemotherapy: A GERCOR efficacy, tolerance, and translational molecular study. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 24, 412–419. doi:10.1093/annonc/mds465
André, T., Vernerey, D., Im, S. A., Bodoky, G., Buzzoni, R., Reingold, S., et al. (2020). Bevacizumab as adjuvant treatment of colon cancer: Updated results from the S-avant phase III study by the GERCOR group. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 31, 246–256. doi:10.1016/j.annonc.2019.12.006
Aparicio, T., Bouché, O., Taieb, J., Maillard, E., Kirscher, S., Etienne, P. L., et al. (2018a). Bevacizumab+chemotherapy versus chemotherapy alone in elderly patients with untreated metastatic colorectal cancer: A randomized phase II trial-PRODIGE 20 study results. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 29, 2270–3138. doi:10.1093/annonc/mdx808
Aparicio, T., Ghiringhelli, F., Boige, V., Le Malicot, K., Taieb, J., Bouché, O., et al. (2018b). Bevacizumab maintenance versus No maintenance during chemotherapy-free intervals in metastatic colorectal cancer: A randomized phase III trial (PRODIGE 9). J. Clin. Oncol. official J. Am. Soc. Clin. Oncol. 36, 674–681. doi:10.1200/JCO.2017.75.2931
Aranda, E., Garcia-Alfonso, P., Benavides, M., Sanchez Ruiz, A., Guillen-Ponce, C., Safont, M. J., et al. (2018). First-line mFOLFOX plus cetuximab followed by mFOLFOX plus cetuximab or single-agent cetuximab as maintenance therapy in patients with metastatic colorectal cancer: Phase II randomised MACRO2 TTD study. Eur. J. Cancer 101, 263–272. doi:10.1016/j.ejca.2018.06.024
Arnold, D., Lueza, B., Douillard, J. Y., Peeters, M., Lenz, H. J., Venook, A., et al. (2017). Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 28, 1713–1729. doi:10.1093/annonc/mdx175
Bendell, J. C., Bekaii-Saab, T. S., Cohn, A. L., Hurwitz, H. I., Kozloff, M., Tezcan, H., et al. (2012). Treatment patterns and clinical outcomes in patients with metastatic colorectal cancer initially treated with FOLFOX–bevacizumab or FOLFIRI–bevacizumab: Results from ARIES, a bevacizumab observational cohort study. Oncol. 17, 1486–1495. doi:10.1634/theoncologist.2012-0190
Bennouna, J., Hiret, S., Bertaut, A., Bouche, O., Deplanque, G., Borel, C., et al. (2019). Continuation of bevacizumab vs cetuximab plus chemotherapy after first progression in KRAS wild-type metastatic colorectal cancer: The UNICANCER PRODIGE18 randomized clinical trial. JAMA Oncol. 5, 83–90. doi:10.1001/jamaoncol.2018.4465
Bennouna, J., Sastre, J., Arnold, D., Österlund, P., Greil, R., Van Cutsem, E., et al. (2013). Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML18147): A randomised phase 3 trial. Lancet Oncol. 14, 29–37. doi:10.1016/S1470-2045(12)70477-1
Boeckx, N., Koukakis, R., Op De Beeck, K., Rolfo, C., Van Camp, G., Siena, S., et al. (2017). Primary tumor sidedness has an impact on prognosis and treatment outcome in metastatic colorectal cancer: Results from two randomized first-line panitumumab studies. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 28, 1862–1868. doi:10.1093/annonc/mdx119
Bry, M., Kivelä, R., Leppänen, V.-M., and Alitalo, K. (2014). Vascular endothelial growth factor-B in physiology and disease. Physiol. Rev. 94, 779–794. doi:10.1152/physrev.00028.2013
Ciardiello, F., Normanno, N., Martinelli, E., Troiani, T., Pisconti, S., Cardone, C., et al. (2016). Cetuximab continuation after first progression in metastatic colorectal cancer (CAPRI-GOIM): A randomized phase II trial of FOLFOX plus cetuximab versus FOLFOX. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 27, 1055–1061. doi:10.1093/annonc/mdw136
Corcoran, R. B., Andre, T., Atreya, C. E., Schellens, J. H. M., Yoshino, T., Bendell, J. C., et al. (2018). Combined BRAF, EGFR, and MEK inhibition in patients with BRAF(V600e)-mutant colorectal cancer. Cancer Discov. 8, 428–443. doi:10.1158/2159-8290.CD-17-1226
Corcoran, R. B., Atreya, C. E., Falchook, G. S., Kwak, E. L., Ryan, D. P., Bendell, J. C., et al. (2015). Combined BRAF and MEK inhibition with dabrafenib and trametinib in BRAF V600-mutant colorectal cancer. J. Clin. Oncol. 33, 4023–4031. doi:10.1200/JCO.2015.63.2471
Cremolini, C., Antoniotti, C., Lonardi, S., Aprile, G., Bergamo, F., Masi, G., et al. (2018a). Activity and safety of cetuximab plus modified FOLFOXIRI followed by maintenance with cetuximab or bevacizumab for RAS and BRAF wild-type metastatic colorectal cancer: A randomized phase 2 clinical trial. JAMA Oncol. 4, 529–536. doi:10.1001/jamaoncol.2017.5314
Cremolini, C., Antoniotti, C., Lonardi, S., Bergamo, F., Cortesi, E., Tomasello, G., et al. (2018b). Primary tumor sidedness and benefit from FOLFOXIRI plus bevacizumab as initial therapy for metastatic colorectal cancer. Retrospective analysis of the TRIBE trial by GONO. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 29, 1528–1534. doi:10.1093/annonc/mdy140
Cremolini, C., Antoniotti, C., Rossini, D., Lonardi, S., Loupakis, F., Pietrantonio, F., et al. (2020). Upfront FOLFOXIRI plus bevacizumab and reintroduction after progression versus mFOLFOX6 plus bevacizumab followed by FOLFIRI plus bevacizumab in the treatment of patients with metastatic colorectal cancer (TRIBE2): A multicentre, open-label, phase 3, randomised, controlled trial. Lancet. Oncol. 21, 497–507. doi:10.1016/S1470-2045(19)30862-9
Cunningham, D., Humblet, Y., Siena, S., Khayat, D., Bleiberg, H., Santoro, A., et al. (2004). Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N. Engl. J. Med. 351, 337–345. doi:10.1056/NEJMoa033025
Cunningham, D., Lang, I., Marcuello, E., Lorusso, V., Ocvirk, J., Shin, D. B., et al. (2013). Bevacizumab plus capecitabine versus capecitabine alone in elderly patients with previously untreated metastatic colorectal cancer (AVEX): An open-label, randomised phase 3 trial. Lancet. Oncol. 14, 1077–1085. doi:10.1016/S1470-2045(13)70154-2
Dasari, N. A., Lonardi, S., Garcia-Carbonero, R., Fernandez, M. E. E., Yoshino, T., Sobrero, A. F., et al. (2022). LBA25 FRESCO-2: A global phase III multiregional clinical trial (mrct) evaluating the efficacy and safety of fruquintinib in patients with refractory metastatic colorectal cancer. Ann. Oncol. 33, S1391–S1392. doi:10.1016/j.annonc.2022.08.021
De Gramont, A., Van Cutsem, E., Schmoll, H.-J., Tabernero, J., Clarke, S., Moore, M. J., et al. (2012). Bevacizumab plus oxaliplatin-based chemotherapy as adjuvant treatment for colon cancer (AVANT): A phase 3 randomised controlled trial. Lancet. Oncol. 13, 1225–1233. doi:10.1016/S1470-2045(12)70509-0
De Luca, A., Carotenuto, A., Rachiglio, A., Gallo, M., Maiello, M. R., Aldinucci, D., et al. (2008). The role of the EGFR signaling in tumor microenvironment. J. Cell. Physiology 214, 559–567. doi:10.1002/jcp.21260
De Roock, W., De Vriendt, V., Normanno, N., Ciardiello, F., and Tejpar, S. (2011). KRAS, BRAF, PIK3CA, and PTEN mutations: Implications for targeted therapies in metastatic colorectal cancer. Lancet. Oncol. 12, 594–603. doi:10.1016/S1470-2045(10)70209-6
Dewdney, A., Cunningham, D., Tabernero, J., Capdevila, J., Glimelius, B., Cervantes, A., et al. (2012). Multicenter randomized phase II clinical trial comparing neoadjuvant oxaliplatin, capecitabine, and preoperative radiotherapy with or without cetuximab followed by total mesorectal excision in patients with high-risk rectal cancer (EXPERT-C). J. Clin. Oncol. official J. Am. Soc. Clin. Oncol. 30, 1620–1627. doi:10.1200/JCO.2011.39.6036
Douillard, J. Y., Oliner, K. S., Siena, S., Tabernero, J., Burkes, R., Barugel, M., et al. (2013). Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N. Engl. J. Med. 369, 1023–1034. doi:10.1056/NEJMoa1305275
Douillard, J. Y., Siena, S., Cassidy, J., Tabernero, J., Burkes, R., Barugel, M., et al. (2010). Randomized, phase III trial of panitumumab with infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX4) versus FOLFOX4 alone as first-line treatment in patients with previously untreated metastatic colorectal cancer: The PRIME study. J. Clin. Oncol. 28, 4697–4705. doi:10.1200/JCO.2009.27.4860
Downward, J. (2003). Targeting RAS signalling pathways in cancer therapy. Nat. Rev. Cancer 3, 11–22. doi:10.1038/nrc969
Duchartre, Y., Kim, Y.-M., and Kahn, M. (2016). The Wnt signaling pathway in cancer. Crit. Rev. Oncology/hematology 99, 141–149. doi:10.1016/j.critrevonc.2015.12.005
Dvorak, H. F. (2002). Vascular permeability factor/vascular endothelial growth factor: A critical cytokine in tumor angiogenesis and a potential target for diagnosis and therapy. J. Clin. Oncol. official J. Am. Soc. Clin. Oncol. 20, 4368–4380. doi:10.1200/JCO.2002.10.088
Fakih, M. G., Kopetz, S., Kuboki, Y., Kim, T. W., Munster, P. N., Krauss, J. C., et al. (2022). Sotorasib for previously treated colorectal cancers with KRASG12C mutation (CodeBreaK100): A prespecified analysis of a single-arm, phase 2 trial. Lancet. Oncol. 23, 115–124. doi:10.1016/S1470-2045(21)00605-7
Ferrara, N., Gerber, H.-P., and Lecouter, J. (2003). The biology of VEGF and its receptors. Nat. Med. 9, 669–676. doi:10.1038/nm0603-669
Folprecht, G., Pericay, C., Saunders, M. P., Thomas, A., Lopez Lopez, R., Roh, J. K., et al. (2016). Oxaliplatin and 5-FU/folinic acid (modified FOLFOX6) with or without aflibercept in first-line treatment of patients with metastatic colorectal cancer: The AFFIRM study. Ann. Oncol. 27, 1273–1279. doi:10.1093/annonc/mdw176
Fornaro, L., Lonardi, S., Masi, G., Loupakis, F., Bergamo, F., Salvatore, L., et al. (2013). FOLFOXIRI in combination with panitumumab as first-line treatment in quadruple wild-type (KRAS, NRAS, HRAS, BRAF) metastatic colorectal cancer patients: A phase II trial by the gruppo oncologico nord ovest (GONO). Ann. Oncol. official J. Eur. Soc. Med. Oncol. 24, 2062–2067. doi:10.1093/annonc/mdt165
Fruman, D. A., and Rommel, C. (2014). PI3K and cancer: Lessons, challenges and opportunities. Nat. Rev. Drug Discov. 13, 140–156. doi:10.1038/nrd4204
García-Alfonso, P., Muñoz Martín, A. J., Ortega Morán, L., Soto Alsar, J., Torres Pérez-Solero, G., Blanco Codesido, M., et al. (2021). Oral drugs in the treatment of metastatic colorectal cancer. Ther. Adv. Med. Oncol. 13, 17588359211009001. doi:10.1177/17588359211009001
Giantonio, B. J., Catalano, P. J., Meropol, N. J., O'dwyer, P. J., Mitchell, E. P., Alberts, S. R., et al. (2007). Bevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: Results from the eastern cooperative oncology group study E3200. J. Clin. Oncol. 25, 1539–1544. doi:10.1200/JCO.2006.09.6305
Glimelius, B., Stintzing, S., Marshall, J., Yoshino, T., and De Gramont, A. (2021). Metastatic colorectal cancer: Advances in the folate-fluoropyrimidine chemotherapy backbone. Cancer Treat. Rev. 98, 102218. doi:10.1016/j.ctrv.2021.102218
Grothey, A., Cutsem, E. V., Sobrero, A., Siena, S., Falcone, A., Ychou, M., et al. (2013). Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 381, 303–312. doi:10.1016/S0140-6736(12)61900-X
Grothey, A., Sugrue, M. M., Purdie, D. M., Dong, W., Sargent, D., Hedrick, E., et al. (2008). Bevacizumab beyond first progression is associated with prolonged overall survival in metastatic colorectal cancer: Results from a large observational cohort study (BRiTE). J. Clin. Oncol. Official J. Am. Soc. Clin. Oncol. 26, 5326–5334. doi:10.1200/JCO.2008.16.3212
Hatzivassiliou, G., Haling, J. R., Chen, H., Song, K., Price, S., Heald, R., et al. (2013). Mechanism of MEK inhibition determines efficacy in mutant KRAS- versus BRAF-driven cancers. Nature 501, 232–236. doi:10.1038/nature12441
Hecht, J. R., Patnaik, A., Berlin, J., Venook, A., Malik, I., Tchekmedyian, S., et al. (2007). Panitumumab monotherapy in patients with previously treated metastatic colorectal cancer. Cancer 110, 980–988. doi:10.1002/cncr.22915
Hegewisch-Becker, S., Graeven, U., Lerchenmüller, C. A., Killing, B., Depenbusch, R., Steffens, C.-C., et al. (2015). Maintenance strategies after first-line oxaliplatin plus fluoropyrimidine plus bevacizumab for patients with metastatic colorectal cancer (AIO 0207): A randomised, non-inferiority, open-label, phase 3 trial. Lancet Oncol. 16, 1355–1369. doi:10.1016/S1470-2045(15)00042-X
Heinemann, V., Von Weikersthal, L. F., Decker, T., Kiani, A., Vehling-Kaiser, U., Al-Batran, S.-E., et al. (2014). FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): A randomised, open-label, phase 3 trial. Lancet Oncol. 15, 1065–1075. doi:10.1016/S1470-2045(14)70330-4
Hong, D. S., Fakih, M. G., Strickler, J. H., Desai, J., Durm, G. A., Shapiro, G. I., et al. (2020). KRASG12C inhibition with sotorasib in advanced solid tumors. N. Engl. J. Med. 383, 1207–1217. doi:10.1056/NEJMoa1917239
Hong, D. S., Morris, V. K., El Osta, B., Sorokin, A. V., Janku, F., Fu, S., et al. (2016). Phase IB study of vemurafenib in combination with irinotecan and cetuximab in patients with metastatic colorectal cancer with BRAFV600E mutation. Cancer Discov. 6, 1352–1365. doi:10.1158/2159-8290.CD-16-0050
Howlader N, N. A., and Krapcho, M., Miller, D., Brest, A, , Yu, M., Ruhl, J., et al. (2020). SEER cancer Statistics review (Bethesda, MD: National Cancer Institute). https://seer.cancer.gov/csr/1975_2018/.based on November 2020 SEER data submission, posted to the SEER web site, April 2021. [Online]. [Accessed]
Hurwitz, H., Fehrenbacher, L., Novotny, W., Cartwright, T., Hainsworth, J., Heim, W., et al. (2004). Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N. Engl. J. Med. 350, 2335–2342. doi:10.1056/NEJMoa032691
Hurwitz, H. I., Bekaii-Saab, T. S., Bendell, J. C., Cohn, A. L., Kozloff, M., Roach, N., et al. (2014). Safety and effectiveness of bevacizumab treatment for metastatic colorectal cancer: Final results from the Avastin® registry – investigation of effectiveness and safety (ARIES) observational cohort study. Clin. Oncol. 26, 323–332. doi:10.1016/j.clon.2014.03.001
Ivy, S. P., Wick, J. Y., and Kaufman, B. M. (2009). An overview of small-molecule inhibitors of VEGFR signaling. Nat. Rev. Clin. Oncol. 6, 569–579. doi:10.1038/nrclinonc.2009.130
Janku, F., Yap, T. A., and Meric-Bernstam, F. (2018). Targeting the PI3K pathway in cancer: Are we making headway? Nat. Rev. Clin. Oncol. 15, 273–291. doi:10.1038/nrclinonc.2018.28
Jonker, D. J., O'callaghan, C. J., Karapetis, C. S., Zalcberg, J. R., Tu, D., Au, H.-J., et al. (2007). Cetuximab for the treatment of colorectal cancer. N. Engl. J. Med. 357, 2040–2048. doi:10.1056/NEJMoa071834
Karkkainen, M. J., Mäkinen, T., and Alitalo, K. (2002). Lymphatic endothelium: A new frontier of metastasis research. Nat. Cell Biol. 4, E2–E5. doi:10.1038/ncb0102-e2
Karnoub, A. E., and Weinberg, R. A. (2008). Ras oncogenes: Split personalities. Nat. Rev. Mol. cell Biol. 9, 517–531. doi:10.1038/nrm2438
Kerr, R. S., Love, S., Segelov, E., Johnstone, E., Falcon, B., Hewett, P., et al. (2016). Adjuvant capecitabine plus bevacizumab versus capecitabine alone in patients with colorectal cancer (QUASAR 2): An open-label, randomised phase 3 trial. Lancet. Oncol. 17, 1543–1557. doi:10.1016/S1470-2045(16)30172-3
Kim, T. W., Elme, A., Kusic, Z., Park, J. O., Udrea, A. A., Kim, S. Y., et al. (2016). A phase 3 trial evaluating panitumumab plus best supportive care vs best supportive care in chemorefractory wild-type KRAS or RAS metastatic colorectal cancer. Br. J. Cancer 115, 1206–1214. doi:10.1038/bjc.2016.309
Kim, T. W., Elme, A., Park, J. O., Udrea, A. A., Kim, S. Y., Ahn, J. B., et al. (2018). Final analysis of outcomes and RAS/BRAF status in a randomized phase 3 study of panitumumab and best supportive care in chemorefractory wild type KRAS metastatic colorectal cancer. Clin. Colorectal Cancer 17, 206–214. doi:10.1016/j.clcc.2018.03.008
Klempner, S. J., Weiss, J., Pelster, M., Spira, A., Barve, M., Ou, S. H. I., et al. (2022). LBA24 KRYSTAL-1: Updated efficacy and safety of adagrasib (MRTX849) with or without cetuximab in patients with advanced colorectal cancer (CRC) harboring a KRASG12C mutation. Ann. Oncol. 33, S1391. doi:10.1016/j.annonc.2022.08.020
Kopetz, S., Grothey, A., Yaeger, R., Van Cutsem, E., Desai, J., Yoshino, T., et al. (2019). Encorafenib, binimetinib, and cetuximab in BRAF V600e-mutated colorectal cancer. N. Engl. J. Med. 381, 1632–1643. doi:10.1056/NEJMoa1908075
Kopetz, S., Guthrie, K. A., Morris, V. K., Lenz, H.-J., Magliocco, A. M., Maru, D., et al. (2021). Randomized trial of irinotecan and cetuximab with or without vemurafenib in BRAF-mutant metastatic colorectal cancer (SWOG S1406). J. Clin. Oncol. Official J. Am. Soc. Clin. Oncol. 39, 285–294. doi:10.1200/JCO.20.01994
Kumagai, S., Koyama, S., and Nishikawa, H. (2021). Antitumour immunity regulated by aberrant ERBB family signalling. Nat. Rev. Cancer 21, 181–197. doi:10.1038/s41568-020-00322-0
Li, J., Qin, S., Xu, R. H., Shen, L., Xu, J., Bai, Y., et al. (2018). Effect of fruquintinib vs placebo on overall survival in patients with previously treated metastatic colorectal cancer: The FRESCO randomized clinical trial. JAMA 319, 2486–2496. doi:10.1001/jama.2018.7855
Li, J., Qin, S., Xu, R., Yau, T. C. C., Ma, B., Pan, H., et al. (2015). Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 16, 619–629. doi:10.1016/S1470-2045(15)70156-7
Li, X., Yan, X., Wang, Y., Kaur, B., Han, H., and Yu, J. (2023). The Notch signaling pathway: A potential target for cancer immunotherapy. J. Hematol. Oncol. 16, 45. doi:10.1186/s13045-023-01439-z
Loupakis, F., Cremolini, C., Antoniotti, C., Lonardi, S., Ronzoni, M., Zaniboni, A., et al. (2015). FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as initial treatment for metastatic colorectal cancer (TRIBE study): Updated survival results and final molecular subgroups analyses. J. Clin. Oncol. 33, 3510. doi:10.1200/jco.2015.33.15_suppl.3510
Martin-Zanca, D., Hughes, S. H., and Barbacid, M. (1986). A human oncogene formed by the fusion of truncated tropomyosin and protein tyrosine kinase sequences. Nature 319, 743–748. doi:10.1038/319743a0
Masi, G., Vivaldi, C., Fornaro, L., Lonardi, S., Buccianti, P., Sainato, A., et al. (2019). Total neoadjuvant approach with FOLFOXIRI plus bevacizumab followed by chemoradiotherapy plus bevacizumab in locally advanced rectal cancer: The TRUST trial. Eur. J. Cancer 110, 32–41. doi:10.1016/j.ejca.2019.01.006
Masuishi, T., Tsuji, A., Kotaka, M., Nakamura, M., Kochi, M., Takagane, A., et al. (2020). Phase 2 study of irinotecan plus cetuximab rechallenge as third-line treatment in KRAS wild-type metastatic colorectal cancer: JACCRO CC-08. Br. J. Cancer 123, 1490–1495. doi:10.1038/s41416-020-01042-w
Maughan, T. S., Adams, R. A., Smith, C. G., Meade, A. M., Seymour, M. T., Wilson, R. H., et al. (2011). Addition of cetuximab to oxaliplatin-based first-line combination chemotherapy for treatment of advanced colorectal cancer: Results of the randomised phase 3 MRC COIN trial. Lancet 377, 2103–2114. doi:10.1016/S0140-6736(11)60613-2
Mauri, G., Pizzutilo, E. G., Amatu, A., Bencardino, K., Palmeri, L., Bonazzina, E. F., et al. (2019). Retreatment with anti-EGFR monoclonal antibodies in metastatic colorectal cancer: Systematic review of different strategies. Cancer Treat. Rev. 73, 41–53. doi:10.1016/j.ctrv.2018.12.006
Ménard, S., Pupa, S. M., Campiglio, M., and Tagliabue, E. (2003). Biologic and therapeutic role of HER2 in cancer. Oncogene 22, 6570–6578. doi:10.1038/sj.onc.1206779
Meric-Bernstam, F., Hurwitz, H., Raghav, K. P. S., Mcwilliams, R. R., Fakih, M., Vanderwalde, A., et al. (2019). Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): An updated report from a multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 20, 518–530. doi:10.1016/S1470-2045(18)30904-5
Modest, D. P., Karthaus, M., Fruehauf, S., Graeven, U., Müller, L., König, A. O., et al. (2022). Panitumumab plus fluorouracil and folinic acid versus fluorouracil and folinic acid alone as maintenance therapy in RAS wild-type metastatic colorectal cancer: The randomized Panama trial (AIO KRK 0212). J. Clin. Oncol. 40, 72–82. doi:10.1200/JCO.21.01332
Modest, D. P., Martens, U. M., Riera-Knorrenschild, J., Greeve, J., Florschütz, A., Wessendorf, S., et al. (2019a). FOLFOXIRI plus panitumumab as first-line treatment of RAS wild-type metastatic colorectal cancer: The randomized, open-label, phase II VOLFI study (AIO KRK0109). J. Clin. Oncol. 37, 3401–3411. doi:10.1200/JCO.19.01340
Modest, D. P., Rivera, F., Bachet, J.-B., De Braud, F., Pietrantonio, F., Koukakis, R., et al. (2019b). Panitumumab-based maintenance after oxaliplatin discontinuation in metastatic colorectal cancer: A retrospective analysis of two randomised trials. Int. J. cancer 145, 576–585. doi:10.1002/ijc.32110
Morris, E. J., Jha, S., Restaino, C. R., Dayananth, P., Zhu, H., Cooper, A., et al. (2013). Discovery of a novel ERK inhibitor with activity in models of acquired resistance to BRAF and MEK inhibitors. Cancer Discov. 3, 742–750. doi:10.1158/2159-8290.CD-13-0070
Munemoto, Y., Nakamura, M., Takahashi, M., Kotaka, M., Kuroda, H., Kato, T., et al. (2019). Sapphire: A randomised phase II study of planned discontinuation or continuous treatment of oxaliplatin after six cycles of modified FOLFOX6 plus panitumumab in patients with colorectal cancer. Eur. J. Cancer (Oxford, Engl. 1990) 119, 158–167. doi:10.1016/j.ejca.2019.07.006
NTRK (2019). Entrectinib effective across NTRK fusion-positive cancers. Cancer Discov. 9, OF4. doi:10.1158/2159-8290.CD-NB2018-156
Pakneshan, S., Salajegheh, A., Smith, R. A., and Lam, A. K.-Y. (2013). Clinicopathological relevance of BRAF mutations in human cancer. Pathology 45, 346–356. doi:10.1097/PAT.0b013e328360b61d
Parikh, A. R., Lee, F.-C., Yau, L., Koh, H., Knost, J., Mitchell, E. P., et al. (2019). MAVERICC, a randomized, Biomarker-stratified, phase II study of mFOLFOX6-bevacizumab versus FOLFIRI-bevacizumab as first-line chemotherapy in metastatic colorectal cancer. Clin. cancer Res. official J. Am. Assoc. Cancer Res. 25, 2988–2995. doi:10.1158/1078-0432.CCR-18-1221
Peeters, M., Price, T. J., Cervantes, A., Sobrero, A. F., Ducreux, M., Hotko, Y., et al. (2014). Final results from a randomized phase 3 study of FOLFIRI {+/-} panitumumab for second-line treatment of metastatic colorectal cancer. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 25, 107–116. doi:10.1093/annonc/mdt523
Peeters, M., Price, T. J., Cervantes, A., Sobrero, A. F., Ducreux, M., Hotko, Y., et al. (2010). Randomized phase III study of panitumumab with fluorouracil, leucovorin, and irinotecan (FOLFIRI) compared with FOLFIRI alone as second-line treatment in patients with metastatic colorectal cancer. J. Clin. Oncol. 28, 4706–4713. doi:10.1200/JCO.2009.27.6055
Peeters, M., Price, T., Taieb, J., Geissler, M., Rivera, F., Canon, J.-L., et al. (2018). Relationships between tumour response and primary tumour location, and predictors of long-term survival, in patients with RAS wild-type metastatic colorectal cancer receiving first-line panitumumab therapy: Retrospective analyses of the PRIME and PEAK clinical trials. Br. J. cancer 119, 303–312. doi:10.1038/s41416-018-0165-z
Pfeiffer, P., Yilmaz, M., Möller, S., Zitnjak, D., Krogh, M., Petersen, L. N., et al. (2020). TAS-102 with or without bevacizumab in patients with chemorefractory metastatic colorectal cancer: An investigator-initiated, open-label, randomised, phase 2 trial. Lancet Oncol. 21, 412–420. doi:10.1016/S1470-2045(19)30827-7
Pietrantonio, F., Morano, F., Corallo, S., Miceli, R., Lonardi, S., Raimondi, A., et al. (2019). Maintenance therapy with panitumumab alone vs panitumumab plus fluorouracil-leucovorin in patients with RAS wild-type metastatic colorectal cancer: A phase 2 randomized clinical trial. JAMA Oncol. 5, 1268–1275. doi:10.1001/jamaoncol.2019.1467
Polivka, J., and Janku, F. (2014). Molecular targets for cancer therapy in the PI3K/AKT/mTOR pathway. Pharmacol. Ther. 142, 164–175. doi:10.1016/j.pharmthera.2013.12.004
Price, T. J., Peeters, M., Kim, T. W., Li, J., Cascinu, S., Ruff, P., et al. (2014). Panitumumab versus cetuximab in patients with chemotherapy-refractory wild-type KRAS exon 2 metastatic colorectal cancer (ASPECCT): A randomised, multicentre, open-label, non-inferiority phase 3 study. Lancet Oncol. 15, 569–579. doi:10.1016/S1470-2045(14)70118-4
Qin, S., Li, J., Wang, L., Xu, J., Cheng, Y., Bai, Y., et al. (2018). Efficacy and Tolerability of first-line cetuximab plus leucovorin, fluorouracil, and oxaliplatin (FOLFOX-4) versus FOLFOX-4 in patients with RAS wild-type metastatic colorectal cancer: The open-label, randomized, phase III TAILOR trial. J. Clin. Oncol. official J. Am. Soc. Clin. Oncol. 36, 3031–3039. doi:10.1200/JCO.2018.78.3183
Rodon, J., Argilés, G., Connolly, R. M., Vaishampayan, U., De Jonge, M., Garralda, E., et al. (2021a). Phase 1 study of single-agent WNT974, a first-in-class Porcupine inhibitor, in patients with advanced solid tumours. Br. J. Cancer 125, 28–37. doi:10.1038/s41416-021-01389-8
Rodon, J., Argilés, G., Connolly, R. M., Vaishampayan, U., De Jonge, M., Garralda, E., et al. (2021b). Phase 1 study of single-agent WNT974, a first-in-class Porcupine inhibitor, in patients with advanced solid tumours. Br. J. Cancer 125, 28–37. doi:10.1038/s41416-021-01389-8
Roskoski, R. (2014). The ErbB/HER family of protein-tyrosine kinases and cancer. Pharmacol. Res. 79, 34–74. doi:10.1016/j.phrs.2013.11.002
Sakai, D., Taniguchi, H., Sugimoto, N., Tamura, T., Nishina, T., Hara, H., et al. (2020). Randomised phase II study of panitumumab plus irinotecan versus cetuximab plus irinotecan in patients with KRAS wild-type metastatic colorectal cancer refractory to fluoropyrimidine, irinotecan and oxaliplatin (WJOG 6510G). Eur. J. cancer 135, 11–21. doi:10.1016/j.ejca.2020.04.014
Saltz, L. B., Clarke, S., Diaz-Rubio, E., Scheithauer, W., Figer, A., Wong, R., et al. (2008). Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: A randomized phase III study. J. Clin. Oncol. 26, 2013–2019. doi:10.1200/JCO.2007.14.9930
Santini, D., Vincenzi, B., Addeo, R., Garufi, C., Masi, G., Scartozzi, M., et al. (2012). Cetuximab rechallenge in metastatic colorectal cancer patients: How to come away from acquired resistance? Ann. Oncol. 23, 2313–2318. doi:10.1093/annonc/mdr623
Sartore-Bianchi, A., Lonardi, S., Martino, C., Fenocchio, E., Tosi, F., Ghezzi, S., et al. (2020). Pertuzumab and trastuzumab emtansine in patients with HER2-amplified metastatic colorectal cancer: The phase II HERACLES-B trial. ESMO Open 5, e000911. doi:10.1136/esmoopen-2020-000911
Sartore-Bianchi, A., Trusolino, L., Martino, C., Bencardino, K., Lonardi, S., Bergamo, F., et al. (2016). Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): A proof-of-concept, multicentre, open-label, phase 2 trial. Lancet Oncol. 17, 738–746. doi:10.1016/S1470-2045(16)00150-9
Schwartzberg, L. S., Rivera, F., Karthaus, M., Fasola, G., Canon, J. L., Hecht, J. R., et al. (2014). Peak: A randomized, multicenter phase II study of panitumumab plus modified fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) or bevacizumab plus mFOLFOX6 in patients with previously untreated, unresectable, wild-type KRAS exon 2 metastatic colorectal cancer. J. Clin. Oncol. 32, 2240–2247. doi:10.1200/JCO.2013.53.2473
Seymour, M. T., Brown, S. R., Middleton, G., Maughan, T., Richman, S., Gwyther, S., et al. (2013). Panitumumab and irinotecan versus irinotecan alone for patients with KRAS wild-type, fluorouracil-resistant advanced colorectal cancer (PICCOLO): A prospectively stratified randomised trial. Lancet Oncol. 14, 749–759. doi:10.1016/S1470-2045(13)70163-3
Siebel, C., and Lendahl, U. (2017). Notch signaling in development, tissue homeostasis, and disease. Physiol. Rev. 97, 1235–1294. doi:10.1152/physrev.00005.2017
Siegel, R. L., Miller, K. D., Fuchs, H. E., and Jemal, A. (2022). Cancer statistics, 2022. A Cancer J. Clin. 72, 7–33. doi:10.3322/caac.21708
Siena, S., Di Bartolomeo, M., Raghav, K., Masuishi, T., Loupakis, F., Kawakami, H., et al. (2021). Trastuzumab deruxtecan (DS-8201) in patients with HER2-expressing metastatic colorectal cancer (DESTINY-CRC01): A multicentre, open-label, phase 2 trial. Lancet Oncol. 22, 779–789. doi:10.1016/S1470-2045(21)00086-3
Simkens, L. H. J., Van Tinteren, H., May, A., Ten Tije, A. J., Creemers, G.-J. M., Loosveld, O. J. L., et al. (2015). Maintenance treatment with capecitabine and bevacizumab in metastatic colorectal cancer (CAIRO3): A phase 3 randomised controlled trial of the Dutch colorectal cancer group. Lancet 385, 1843–1852. doi:10.1016/S0140-6736(14)62004-3
Sobrero, A. F., Maurel, J., Fehrenbacher, L., Scheithauer, W., Abubakr, Y. A., Lutz, M. P., et al. (2008). Epic: Phase III trial of cetuximab plus irinotecan after fluoropyrimidine and oxaliplatin failure in patients with metastatic colorectal cancer. J. Clin. Oncol. 26, 2311–2319. doi:10.1200/JCO.2007.13.1193
Solomon, J. P., Benayed, R., Hechtman, J. F., and Ladanyi, M. (2019). Identifying patients with NTRK fusion cancer. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 30, viii16–viii22. doi:10.1093/annonc/mdz384
Strickler, J., Cercek, A., Siena, S., André, T., Ng, K., Van Cutsem, E., et al. (2022). LBA-2 primary analysis of MOUNTAINEER: A phase 2 study of tucatinib and trastuzumab for HER2-positive mCRC. Ann. Oncol. 33, S375–S376. doi:10.1016/j.annonc.2022.04.440
Tabernero, J., Grothey, A., Van Cutsem, E., Yaeger, R., Wasan, H., Yoshino, T., et al. (2021). Encorafenib plus cetuximab as a new standard of care for previously treated BRAF V600e-mutant metastatic colorectal cancer: Updated survival results and Subgroup analyses from the BEACON study. J. Clin. Oncol. official J. Am. Soc. Clin. Oncol. 39, 273–284. doi:10.1200/JCO.20.02088
Tabernero, J., Yoshino, T., Cohn, A. L., Obermannova, R., Bodoky, G., Garcia-Carbonero, R., et al. (2015). Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine (RAISE): A randomised, double-blind, multicentre, phase 3 study. Lancet Oncol. 16, 499–508. doi:10.1016/S1470-2045(15)70127-0
Taieb, J., Tabernero, J., Mini, E., Subtil, F., Folprecht, G., Van Laethem, J.-L., et al. (2014). Oxaliplatin, fluorouracil, and leucovorin with or without cetuximab in patients with resected stage III colon cancer (PETACC-8): An open-label, randomised phase 3 trial. Lancet Oncol. 15, 862–873. doi:10.1016/S1470-2045(14)70227-X
Tejpar, S., Stintzing, S., Ciardiello, F., Tabernero, J., Van Cutsem, E., Beier, F., et al. (2017). Prognostic and predictive relevance of primary tumor location in patients with RAS wild-type metastatic colorectal cancer: Retrospective analyses of the CRYSTAL and FIRE-3 trials. JAMA Oncol. 3, 194–201. doi:10.1001/jamaoncol.2016.3797
Tol, J., Koopman, M., Cats, A., Rodenburg, C. J., Creemers, G. J. M., Schrama, J. G., et al. (2009). Chemotherapy, bevacizumab, and cetuximab in metastatic colorectal cancer. N. Engl. J. Med. 360, 563–572. doi:10.1056/NEJMoa0808268
Tonini, G., Imperatori, M., Vincenzi, B., Frezza, A. M., and Santini, D. (2013). Rechallenge therapy and treatment holiday: Different strategies in management of metastatic colorectal cancer. J. Exp. Clin. cancer Res. CR 32, 92. doi:10.1186/1756-9966-32-92
Tournigand, C., André, T., Achille, E., Lledo, G., Flesh, M., Mery-Mignard, D., et al. (2004). FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: A randomized GERCOR study. J. Clin. Oncol. 22, 229–237. doi:10.1200/JCO.2004.05.113
Tsurutani, J., Iwata, H., Krop, I., Janne, P. A., Doi, T., Takahashi, S., et al. (2020). Targeting HER2 with trastuzumab deruxtecan: A dose-expansion, phase I study in multiple advanced solid tumors. Cancer Discov. 10, 688–701. doi:10.1158/2159-8290.CD-19-1014
Tveit, K. M., Guren, T., Glimelius, B., Pfeiffer, P., Sorbye, H., Pyrhonen, S., et al. (2012). Phase III trial of cetuximab with continuous or intermittent fluorouracil, leucovorin, and oxaliplatin (nordic FLOX) versus FLOX alone in first-line treatment of metastatic colorectal cancer: The NORDIC-VII study. J. Clin. Oncol. 30, 1755–1762. doi:10.1200/JCO.2011.38.0915
Vaishnavi, A., Le, A. T., and Doebele, R. C. (2015). TRKing down an old oncogene in a new era of targeted therapy. Cancer Discov. 5, 25–34. doi:10.1158/2159-8290.CD-14-0765
Van Cutsem, E., Cervantes, A., Adam, R., Sobrero, A., Van Krieken, J. H., Aderka, D., et al. (2016). ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. Official J. Eur. Soc. Med. Oncol. 27, 1386–1422. doi:10.1093/annonc/mdw235
Van Cutsem, E., Cervantes, A., Nordlinger, B., and Arnold, D. (2014). Metastatic colorectal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 25, iii1–iii9. doi:10.1093/annonc/mdu260
Van Cutsem, E., Köhne, C.-H., Hitre, E., Zaluski, J., Chang Chien, C.-R., Makhson, A., et al. (2009). Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N. Engl. J. Med. 360, 1408–1417. doi:10.1056/NEJMoa0805019
Van Cutsem, E., Peeters, M., Siena, S., Humblet, Y., Hendlisz, A., Neyns, B., et al. (2007). Open-label phase III trial of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy-refractory metastatic colorectal cancer. J. Clin. Oncol. 25, 1658–1664. doi:10.1200/JCO.2006.08.1620
Van Cutsem, E., Siena, S., Humblet, Y., Canon, J. L., Maurel, J., Bajetta, E., et al. (2008). An open-label, single-arm study assessing safety and efficacy of panitumumab in patients with metastatic colorectal cancer refractory to standard chemotherapy. Ann. Oncol. official J. Eur. Soc. Med. Oncol. 19, 92–98. doi:10.1093/annonc/mdm399
Van Cutsem, E., Tabernero, J., Lakomy, R., Prenen, H., Prausova, J., Macarulla, T., et al. (2012). Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J. Clin. Oncol. 30, 3499–3506. doi:10.1200/JCO.2012.42.8201
Velenik, V., Zadnik, V., Omejc, M., Grosek, J., and Tuta, M. (2020). Influence of concurrent capecitabine based chemoradiotherapy with bevacizumab on the survival rate, late toxicity and health-related quality of life in locally advanced rectal cancer: A prospective phase II CRAB trial. Radiol. Oncol. 54, 461–469. doi:10.2478/raon-2020-0043
Venook, A. P., Niedzwiecki, D., Lenz, H. J., Innocenti, F., Fruth, B., Meyerhardt, J. A., et al. (2017). Effect of first-line chemotherapy combined with cetuximab or bevacizumab on overall survival in patients with KRAS wild-type advanced or metastatic colorectal cancer: A randomized clinical trial. JAMA 317, 2392–2401. doi:10.1001/jama.2017.7105
Vincenzi, B., Santini, D., Rabitti, C., Coppola, R., Beomonte Zobel, B., Trodella, L., et al. (2006). Cetuximab and irinotecan as third-line therapy in advanced colorectal cancer patients: A single centre phase II trial. Br. J. Cancer 94, 792–797. doi:10.1038/sj.bjc.6603018
Wang, Z., Qin, B. D., Ye, C. Y., Wang, M. M., Yuan, L. Y., Dai, W. P., et al. (2022). Cetuximab and vemurafenib plus FOLFIRI (5-fluorouracil/leucovorin/irinotecan) for BRAF V600E-mutated advanced colorectal cancer (IMPROVEMENT): An open-label, single-arm, phase II trial. Eur. J. Cancer 163, 152–162. doi:10.1016/j.ejca.2021.12.028
Yaeger, R., Cercek, A., O'reilly, E. M., Reidy, D. L., Kemeny, N., Wolinsky, T., et al. (2015). Pilot trial of combined BRAF and EGFR inhibition in BRAF-mutant metastatic colorectal cancer patients. Clin. Cancer Res. 21, 1313–1320. doi:10.1158/1078-0432.CCR-14-2779
Yoshida, Y., Yamada, T., Kamiyama, H., Kosugi, C., Ishibashi, K., Yoshida, H., et al. (2021). Combination of TAS-102 and bevacizumab as third-line treatment for metastatic colorectal cancer: TAS-CC3 study. Int. J. Clin. Oncol. 26, 111–117. doi:10.1007/s10147-020-01794-8
Yoshino, T., Di Bartolomeo, M., Raghav, K., Masuishi, T., Loupakis, F., Kawakami, H., et al. (2023). Final results of DESTINY-CRC01 investigating trastuzumab deruxtecan in patients with HER2-expressing metastatic colorectal cancer. Nat. Commun. 14, 3332. doi:10.1038/s41467-023-38032-4
Keywords: colorectal cancer, EGFR, HER2, BRAF, anti-angiogenic
Citation: Huang S, Ye J, Gao X, Huang X, Huang J, Lu L, Lu C, Li Y, Luo M, Xie M, Lin Y and Liang R (2023) Progress of research on molecular targeted therapies for colorectal cancer. Front. Pharmacol. 14:1160949. doi: 10.3389/fphar.2023.1160949
Received: 07 February 2023; Accepted: 26 July 2023;
Published: 08 August 2023.
Edited by:
Yong Gao, Guangzhou University of Chinese Medicine, ChinaReviewed by:
Fan He, Washington University in St. Louis, United StatesCopyright © 2023 Huang, Ye, Gao, Huang, Huang, Lu, Lu, Li, Luo, Xie, Lin and Liang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yan Lin, bGlueWFuQGd4bXUuZWR1LmNu; Rong Liang, bGlhbmdyb25nQGd4bXUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship
‡Lead Contact
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.