 Shouyuan Sun1†
Shouyuan Sun1† Liang Zhao
Liang Zhao Zongzhi Xie
Zongzhi Xie Yawen Pan
Yawen Pan
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 09 February 2023
Sec. Ethnopharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1047650
Objective: The aim of this study is to critically appraise whether published systematic reviews/meta-analyses of traditional Chinese medicine for adults with ischemic stroke are of sufficient quality and to rate the quality of evidence using the Grading of Recommendations, Assessment, Development, and Evaluation approach.
Method: A literature search was performed in the Cochrane Library, PubMed, Chinese National Knowledge Infrastructure, and SinoMed databases by March 2022. The inclusion criteria were systematic reviews/meta-analyses of traditional Chinese medicine in adults who suffered from ischemic stroke. A Measurement Tool to Access Systematic Reviews 2 (AMSTAR-2) and Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Abstract (PRISMA-A) statements were used to assess the methodological and reporting quality of the included reviews. The Grading of Recommendations, Assessment, Development, and Evaluation system was utilized to assess each report’s evidence level.
Results: Of the 1,908 titles and abstracts, 83 reviews met the inclusion criteria. These studies were published between 2005 and 2022. The results of AMSTAR-2 showed that 51.4% of the items were reported, but the registration, reasons for the inclusion of study design, the list of excluded studies, and funding information were ignored in the majority of the reviews. The results of PRISMA-A showed that 33.9% of items were reported, and the information on registration, limitation, and funding was not available in many publications. The assessment of the evidence with the Grading of Recommendations, Assessment, Development, and Evaluation showed that more than half (52/83) of the included studies had either low or very low levels of evidence.
Conclusion: The reporting quality in the abstract of systematic reviews/meta-analyses on traditional Chinese medicine for ischemic stroke is poor and does not facilitate timely access to valid information for clinical practitioners. Although the methodological quality is of a medium level, this evidence lacks certainty, especially with a high risk of bias in individual studies.
Stroke, a medical disorder in which poor blood flow to the brain leads to cell death, can result in lasting brain injury, long-term disability, and even death. It is the second leading cause of death and the third leading cause of disability-adjusted life-years (DALYs) lost in the world (Feigin et al., 2022). There are two types of stroke, namely, ischemic stroke (due to insufficient blood flow) and hemorrhagic stroke (due to bleeding). Approximately 87% of all strokes are ischemic strokes, where blood flow to the brain is blocked (Tsao et al., 2022). Globally, there are over 77 million prevalent ischemic strokes, 7.6 million new cases, 3.3 million deaths from ischemic stroke, and over 63 million DALYs due to ischemic stroke as of 2019 (GBD 2019 Stroke Collaborators, 2021). The financial burden of ischemic stroke on health services and societies is enormous, and the average lifetime cost is $67,900 (Strilciuc et al., 2021). Reperfusion therapy is considered the standard management and is globally approved for ischemic stroke; however, it is urgent and high-risk (Campbell et al., 2019). Although many drugs have proven to be neuroprotective in preclinical studies, most of them have failed in clinical trials (Gaire, 2018; Campbell et al., 2019).
In recent years, several systematic reviews have been published on the efficacy and safety of traditional Chinese medicine (TCM). It has been suggested that TCM may improve cerebral microcirculation in the brain (Gong and Sucher, 1999), protect against ischemic reperfusion injury (Lee et al., 2005; Wang et al., 2005), reduce oxidative stress reaction (Bi et al., 2012), possess neuroprotective properties, and inhibit apoptosis (Kim, 2005).
High-quality systematic reviews/meta-analyses can provide a more valuable reference for clinical practices than individual studies (Schalken and Rietbergen, 2017; Vrieze, 2018); however, some studies have indicated that the reporting and methodological quality of systematic reviews on TCM are low, which may disturb and even mislead clinical practices or scientific research (Ma et al., 2011; Wang Y. et al., 2016; Zhou et al., 2016). Therefore, the present review aims to evaluate the methodological and reporting quality of systematic reviews/meta-analyses of randomized controlled trials (RCTs) on TCM for ischemic stroke with PRISMA-A (Page et al., 2021) and AMSTAR-2 (Shea et al., 2017). Additionally, the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system was used to rate each report’s evidence level to provide evidence to practitioners and researchers when they make clinical decisions.
A literature search was performed in PubMed and the Cochrane Library using the keywords “ischemic stroke,” “Chinese medicine,” “systematic review,” and “meta-analysis.” Considering the interventions of Chinese medicine, we conducted additional searches in the Chinese National Knowledge Infrastructure (CNKI) and China Biomedical Literature Service System (SinoMed) with the same keywords (the search strategy is shown in Table 1). We also scanned the reference list mentioned in the related reviews to ensure that our search did not miss any important potential studies on the Chinese medical treatment for ischemic stroke. The deadline for database searching was 1 March 2022. Two steps were adopted for selection. First, the titles and abstracts of the literature were scanned to screen all related studies, and this process was conducted with an online tool known as Rayyan (https://rayyan.ai/), a web and mobile app that was developed specifically to expedite the initial screening of abstracts and titles using a process of semi-automation (Ouzzani et al., 2016). Before the formal screening, the first three authors conducted two rounds of pilot trials for selection with 100 records until the consistency was over 90%. In the formal stage, the first two authors screened all the titles and abstracts independently with the blind function on. When they completed all the records, the blind function turned on, and any disagreements were solved by a discussion with the third author. Then, they located and screened the full texts to identify the reports which met all inclusion criteria in Excel software. The results of the literature search and the selection of articles based on the PRISMA flow diagram are shown in Figure 1.
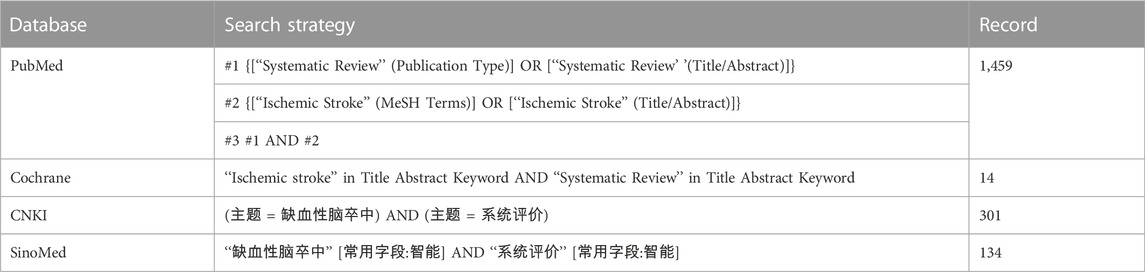
TABLE 1. Search strategy of each database.
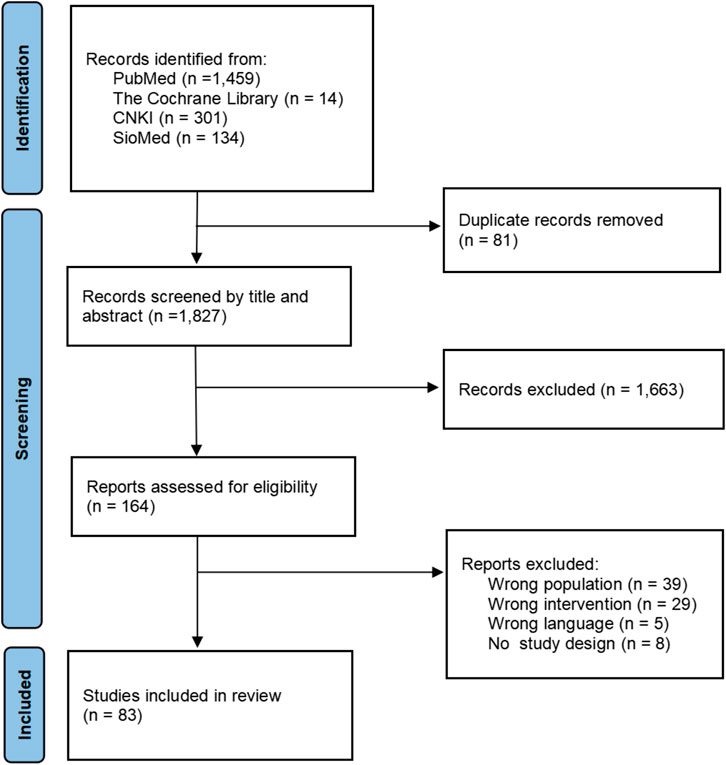
FIGURE 1. Process of literature selection.
To be included in our review, a review had to meet the following criteria: 1) the patients included were adults who experienced ischemic stroke. The transient ischemic attack and hemorrhagic stroke were also excluded; 2) the interventions included were the Chinese medical treatment, where acupuncture and massage were excluded. Single TCM treatments, integrated TCM treatments, and integrated TCM and Western medicine treatments were included, and animal experiments were excluded; 3) the comparisons were of TCM, Western medicine treatment, placebo, or no treatment; 4) the outcome without limitations; 5) the study design included was the systematic review or meta-analysis. The overview of systematic reviews, mixed-method review, qualitative review, integrative review, rapid review, and evidence synthesis were beyond the inclusion; 6) published in English and Chinese; and 7) there was no restriction on the time framework of the studies.
The information extraction and coding were designed with Excel software, and two rounds of pilots were carried out before the formal extraction and coding to make sure the extractors have an accurate and consistent understanding of what to extract. When the consistency reaches 100%, the formal data extraction and coding process begins. There were four parts of information: (Feigin et al., 2022) general information, including title, author, language, the year of publication, database, number of included studies, number of patients, type of interventions and comparisons, and outcomes; (Tsao et al., 2022) information of 12 items in PRISMA-A; (GBD 2019 Stroke Collaborators, 2021) information of 16 items in AMSTAR-2; and (Strilciuc et al., 2021) information of five domains in GRADE. The PRISMA-A and AMSTAR-2 were coded into “Yes,” “Partial Yes,” or “No” depending on how well each item was reported. The fourth part was rated as “Not serious,” “Serious,” “Very serious,” or “No information,” according to the risk bias in each domain. “High,” “Moderate,” “Low,” and “Very Low” were applied to rate the overall level of risks of bias. The process of data extraction and coding was performed by two authors independently, and any disagreements were solved by the third author.
We used the PRISMA-A guideline to reflect the abstract quality of systematic reviews/meta-analyses, and descriptive statistics (frequencies and percentages) was used to describe the reporting characteristics. We adopted AMSTAR-2 to evaluate the methodological quality of reviews, and the results were shown with percentages for each item. We also applied GRADE to rate the overall quality of evidence, and the ratio of each grade was analyzed (high, moderate, low, and critically low). In addition, regression analysis with the year of publication and the percentage of “Yes” in PRISMA-A and AMSTAR-2 was performed to explore the changes in quality, and subgroup analysis was adopted to compare the difference depending on the publication language. All these analyses were conducted in Excel software and SPSS 22.0.
Of 1,908 records, 1,827 titles and abstracts were screened with Rayyan after removing the duplications, 52 studies with disagreements were resolved by the third author (the consistency is 97.2%), 164 were located with full text, and 83 systematic reviews/meta-analyses on the TCM for ischemic stroke were included which were published between 2005 and 2022. The PRISMA flow diagram is shown in Figure 1. Among them, 61 (73.5%) were published in Chinese, 81 (97.6%) were conducted in China, 1 (1.2%) in Malaysia, and 1 (1.2%) in Korea. The number of included primary studies in these reviews ranged from two to 107. A total of 43 (51.8%) were focused on acute ischemic stroke (AIS). The number of patients involved in the reports ranged from 161 to 13,073. The characteristics of included studies are shown in Table 2.

TABLE 2. Characteristics of included studies.
Based on the PRISMA-A statement, two reviewers discussed the different coding items with the third author, and finally unified the coding data. The results showed that among 83 abstracts that were accessed, the overall total report (percentage of “Yes”) was 33.9% and the partial report (percentage of “Partial Yes”) was 13.2%. Most reviews (96.6%) clearly described the publication type and all of them reported the objectives of the reviews, while only information sources were reported by over half reviews in the methods section. All reviews demonstrated the results (84.3% in the main outcome) and discussion (97.6% in interpretation), but the limitations of evidence were ignored by many publications (30.1% reported). In addition, other information such as funding and registration were mentioned by 1.2% and 6.0%, respectively. The completion of a single item is shown in Figure 2, and the results of each item are shown in the Supplementary material.
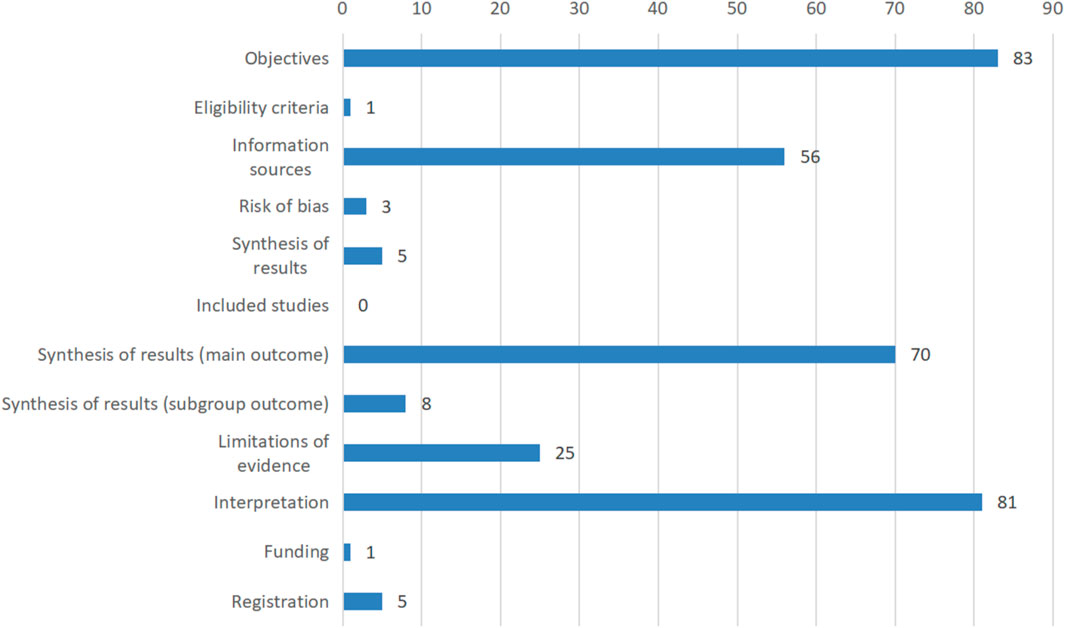
FIGURE 2. Reporting quality of abstracts based on PRISMA-A.
The methodological quality of reviews was accessed by the AMSTAR-2, including 16 items. The results showed that the average report completeness was 51.4%, and eight items (items 1, 5, 6, 8, 9, 11, 13, and 15) were higher than 70% (71.1%–98.9%). However, fewer papers included in the evaluation fully reported the registration (item 2: 7.2%), the reasonableness of the inclusion criteria of the study design (item 3: 1.2%), the list of excluded studies (item 7: 6.0%), information on the funding (item 10: 4.8%), and the explanation of heterogeneity (item 14: 30.1%), which directly affects the openness and transparency of systematic reviews and results in the inability of follow-up researchers to repeat and update (Figure 3). The results of each item are shown in the Supplementary material.
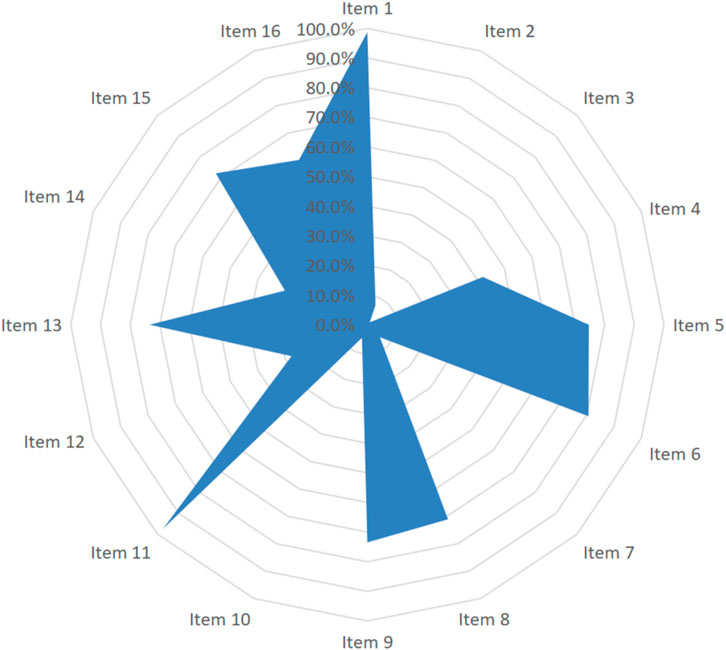
FIGURE 3. Methodological quality of systematic reviews based on AMSTAR-2.
We adopted the GRADE system to evaluate the overall evidence quality, and the results showed that there were only 15.7% of included studies in high certainty, 21.7% in moderate, 30.1% in low, and 32.5% in very low certainty. Notably, 49.4% of included reviews had a very serious risk of bias, in which more than one-third of them had serious publication bias and inconsistency, and 9.6% had a serious risk of imprecision (Figure 4). The results of each item are shown in the Supplementary material.
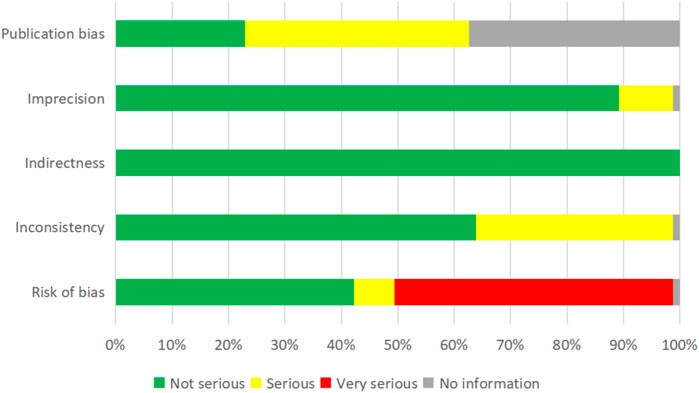
FIGURE 4. Evidence certainty based on the GRADE system.
Table 3 shows that the reporting quality and certainty of meta-analyses on TCM for ischemic stroke had no obvious improvement after PRISMA and AMSTAR-2 were released in 2009, but the methodological quality showed an upward trend, especially in the inclusion/exclusion criteria (item 7, χ2 = 13.3, and p < 0.01) and risk of bias assessment (item 12, χ2 = 7.7, and p < 0.01).

TABLE 3. Results of the subgroup analysis.
52 (62.7%) reviews included TCM for ischemic stroke, and 29 (34.9%) included TCM with WM. Table 3 shows that the reviews focused on TCM with WM are the most frequently adopted selection in duplicate (item 5 in AMSTAR-2: χ2 = 6.4, and p < 0.01) and reported potential sources of conflict of interest (item 16 in AMSTAR-2: χ2 = 8.6, and p < 0.01). However, they had a higher risk of inconsistency (χ2 = 6.1 and p < 0.01).
We included both Chinese (61, 73.5%) and English studies (22, 26.5%) and analyzed the variety of reporting and methodological quality depending on the publication language. The results showed that reviews published in Chinese rarely reported the protocol (item 2 in AMSTAR-2: χ2 = 17.9, and p < 0.01). However, studies published in English had a higher risk of bias (χ2 = 6.6 and p < 0.05) and imprecision (χ2 = 9.0 and p < 0.05) than those with Chinese studies. The details are shown in Table 3.
Due to the advantages of TCM for ischemic stroke, numerous meta-analyses were conducted to evaluate its efficacy and safety. The present review included 83 reviews to evaluate the methodological, reporting, and evidence certainty of systematic reviews and meta-analysis of TCM for ischemic stroke. The results showed that the reporting quality for abstract was in the low level (33.9% of items were reported) and methodological quality was in the middle level (51.4% of items were reported). However, only 15.7% of included studies were in high certainty. In addition, 49.4% of reviews had a very serious risk of bias, 37.1% had serious publication bias, and 34.9% had inconsistency risk, which may affect the evidence confidence and even mislead the clinical decision.
Although the PRISMA and AMSTAR were developed to improve the reporting and methodological quality of systematic review/meta-analysis (Moher et al., 1999; Moher et al., 2009; Shea et al., 2009; Sharma and Oremus, 2018; Page et al., 2021), there was no obvious persistent improvement in the reviews of the TCM for ischemic stroke. Li et al. (2009) introduced the PRISMA in China and translated it to a Chinese vision, but it was interpreted systematically since 2015 (Tian et al., 2015; Zhang et al., 2015; Sun et al., 2018). The majority (item 81: 97.6%) of reviews included in this study were conducted in China, and the delayed promotion of PRISMA in China may be the main reason for this result.
In addition, it was rare that Chinese medicine journals recommended the PRISMA guideline when the authors conducted and submitted their manuscripts to the journal. For example, the Journal of Traditional Chinese Medicine, an open-access journal that aims to publish evidence-based, scientifically justified original articles, and review papers in all aspects of Chinese medicine, only suggested that authors should refer to the CONSORT 2010 Statement for reports of RCTs. Even the American Journal of Chinese Medicine, an international journal of comparative eastern and western medicine, did not mention the reporting requirement for systematic reviews in the submission guidelines. Therefore, it is necessary for editors to highly recommend the reporting items of systematic reviews in their submission guidelines to promote the repeatability and transparency of Chinese medicine studies.
Differing from Western medicine, most of the principles of TCM were derived from a philosophical basis instead of biological mechanisms, such as the dynamic balance between Yin and Yang, and the majority of treatments aimed to expel or suppress the cause of disharmony and restore balance (Tang et al., 2008). Moreover, the same disease in Western medicine can be categorized into different syndromes (called Zhengs) in TCM. Thus, patients with the same “diagnosis” in Western medicine can be treated differently in TCM, and even the treatments of TCM in the same patient vary over time. Although there were several reporting guidelines for systematic reviews, such as the CONSORT and PRISMA guidelines, the uniqueness of TCM was not considered in the present guidelines (Wang G. et al., 2016; Hu et al., 2019; Yu et al., 2019). For example, in addition to patients, interventions, comparisons, and outcomes, the symptoms, time points, formula, and dosage of Chinese medicine should be recorded in detail. More researchers had focused on this and built a tailed reporting guideline for TCM, such as the extension of PRISMA for acupuncture (Liu et al., 2014; Li et al., 2017). Meanwhile, it is also essential to create a series of standards and guidelines for TCM to improve its evidence quality in clinical practices and research.
As mentioned previously, treatments from TCM are dialectical and emphasize individual therapy based on the time, place, and patient. When designing a clinical study, it is difficult to conduct large-sample, multi-center, double-blind RCTs due to differences in the treatment form, method, and nature (duration and intensity), and may introduce higher bias and risk (Xie and Leung, 2009). However, by ignoring the diversities of TCM in a systematic review, the evidence cannot be translated into practice effectively. Thus, researchers are suggested to minimize the random error using rigorous, transparent, and standardized design and to also reduce the system error using statistical methods when conducting small sample clinical trials and are advised to report both quantitative and qualitative results of primary studies and systematic reviews.
In addition, we found that the reviews published in Chinese rarely provided information about their protocol. A published or documented detailed plan could promote consistency between the authors’ plan and action when implementing the research, ensure clear responsibility, and enhance the openness, transparency, and repeatability of evidence (Liu et al., 2021). It also helps to reduce the authors’ bias when selecting and extracting (Moher et al., 2009). However, there is no registration platform for TCM yet, which will also be an important issue in the future.
The reporting quality in the abstracts of systematic reviews/meta-analyses about TCM for ischemic stroke is poor and does not facilitate rapid access to valid information for clinical practitioners. The methodological quality is of a medium level, but this evidence lacks certainty, especially with a high risk of bias in individual studies.
In addition, rare reviews reported the process of protocol registration and the list of excluded studies, which increases the repetitive crisis. Although TCM has its advantages for ischemic stroke, it is necessary to develop target guidelines to improve its evidence quality.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
SS, LZ, and YP participated in the study design, data analysis, and article writing. XZ, XL, BZ, LZ, and SS contributed to the literature search, screening, and extraction of data. ZX, JR, and YP proofread the manuscript. All authors contributed to the article and approved the submitted version.
This study was funded by the Science and Technology Program of Gansu Province (21YF11FA003), the Youth Innovation and Entrepreneurship Talent Project of Longyuan (2022LQTD31), the Science and Technology Program of Lanzhou Chengguan District (2021SHFZ0028), and the Health Industry Scientific Research Program of Gansu Province (GSWSKY 2017-58). The funders had no role in the design and conduct of the study; management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1047650/full#supplementary-material
Bi, Q., Wang, T., and Zhang, W. (2012). Frequency and etiological diagnosis of ischemic stroke in Chinese young adults. Neurol. Res. 34, 354–358. doi:10.1179/1743132812Y.0000000023
Campbell, B. C. V., De Silva, D. A., Macleod, M. R., Coutts, S. B., Schwamm, L. H., Davis, S. M., et al. (2019). Ischaemic stroke. Nat. Rev. Dis. Prim. 5, 70. doi:10.1038/s41572-019-0118-8
Feigin, V. L., Brainin, M., Norrving, B., Martins, S., Sacco, R. L., Hacke, W., et al. (2022). World stroke organization (WSO): Global stroke fact sheet 2022. Int. J. Stroke 17, 18–29. doi:10.1177/17474930211065917
Gaire, B. P. (2018). Herbal medicine in ischemic stroke: Challenges and prospective. Chin. J. Integr. Med. 24, 243–246. doi:10.1007/s11655-018-2828-2
GBD 2019 Stroke Collaborators (2021). Global, regional, and national burden of stroke and its risk factors, 1990-2019: A systematic analysis for the global burden of disease study 2019. Lancet Neurol. 20, 795–820. doi:10.1016/S1474-4422(21)00252-0
Gong, X., and Sucher, N. J. (1999). Stroke therapy in traditional Chinese medicine (TCM): Prospects for drug discovery and development. Trends Pharmacol. Sci. 20, 191–196. doi:10.1016/s0165-6147(98)01276-0
Hu, R., Wen, L., Yu, M., Ren, Y., Cao, H., Gao, J., et al. (2019). Literature analysis of present situation and reporting quality in TCM safety systematic reviews based on PRISMA harms checklist. CJPV 16, 231–238. doi:10.3969/j.issn.1672-8629.2019.04.010
Kim, H. (2005). Neuroprotective herbs for stroke therapy in traditional eastern medicine. Neurol. Res. 27, 287–301. doi:10.1179/016164105X25234
Lee, I. Y., Lee, C. C., Chang, C. K., Chien, C. H., and Lin, M. T. (2005). Sheng mai san, a Chinese herbal medicine, protects against renal ischaemic injury during heat stroke in the rat. Clin. Exp. Pharmacol. Physiol. 32 (9), 742–748. doi:10.1111/j.1440-1681.2005.04259.x
Li, X., Cao, H., and Liu, J. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement (Chinese edition). Chin. J. Integr. Med. 7, 889–896. doi:10.3736/jcim20090918
Li, X., Wang, R., Shi, X., Su, J., Pan, Y., Tian, J., et al. (2017). Reporting characteristics and quality of systematic reviews of acupuncture analgesia. Pain Pract. 17, 1066–1074. doi:10.1111/papr.12555
Liu, Y., Chen, S., Fan, F., Di, X., Fan, H., Feng, C., et al. (2021). A standardized checklist on meta-analysis reporting in the open science era. Sci. Sin. Vitae 51, 764–778. doi:10.1360/ssv-2021-0009
Liu, Y., Zhang, R., Huang, J., Zhao, X., Liu, D., Sun, W., et al. (2014). Reporting quality of systematic reviews/meta-analyses of acupuncture. PLoS One 9, e113172. doi:10.1371/journal.pone.0113172
Ma, B., Guo, J., Qi, G., Li, H., Peng, J., Zhang, Y., et al. (2011). Epidemiology, quality and reporting characteristics of systematic reviews of traditional Chinese medicine interventions published in Chinese journals. PLoS One 6, e20185. doi:10.1371/journal.pone.0020185
Moher, D., Cook, D. J., Eastwood, S., Olkin, I., Rennie, D., and Stroup, D. F. (1999). Improving the quality of reports of meta-analyses of randomised controlled trials: The QUOROM statement. Quality of reporting of meta-analyses. Lancet 354, 1896–1900. doi:10.1016/s0140-6736(99)04149-5
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G.PRISMA Group (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 339, b2535. doi:10.1136/bmj.b2535
Ouzzani, M., Hammady, H., Fedorowicz, Z., and Elmagarmid, A. (2016). Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 5, 210. doi:10.1186/s13643-016-0384-4
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 372, n160. doi:10.1136/bmj.n160
Schalken, N., and Rietbergen, C. (2017). The reporting quality of systematic reviews and meta-analyses in industrial and organizational psychology: A systematic review. Front. Psychol. 8, 1395. doi:10.3389/fpsyg.2017.01395
Sharma, S., and Oremus, M. (2018). PRISMA and AMSTAR show systematic reviews on health literacy and cancer screening are of good quality. J. Clin. Epidemiol. 99, 123–131. doi:10.1016/j.jclinepi.2018.03.012
Shea, B. J., Hamel, C., Wells, G. A., Bouter, L. M., Kristjansson, E., Grimshaw, J., et al. (2009). AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epidemiol. 62, 1013–1020. doi:10.1016/j.jclinepi.2008.10.009
Shea, B. J., Reeves, B. C., Wells, G., Thuku, M., Hamel, C., Moran, J., et al. (2017). Amstar 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358, j4008. doi:10.1136/bmj.j4008
Strilciuc, S., Grad, D. A., Radu, C., Chira, D., Stan, A., Ungureanu, M., et al. (2021). The economic burden of stroke: A systematic review of cost of illness studies. J. Med. Life 14, 606–619. doi:10.25122/jml-2021-0361
Sun, X., Zhou, X., Yu, Y., and Liu, H. (2018). Exploring reporting quality of systematic reviews and Meta-analyses on nursing interventions in patients with Alzheimer’s disease before and after PRISMA introduction. BMC Med. Res. Methodol. 18, 154. doi:10.1186/s12874-018-0622-7
Tang, J. L., Liu, B. Y., and Ma, K. W. (2008). Traditional Chinese medicine. Lancet 372, 1938–1940. doi:10.1016/S0140-6736(08)61354-9
Tian, J., Ge, L., Zhao, Y., Zhang, J., Su, X., Liu, A., et al. (2015). An introduction to PRISMA extension statement for network meta-analysis. Chin. J. Drug Eval. 32, 266–272. doi:10.3969/j.issn.2095-3593.2015.05.003
Tsao, C. W., Aday, A. W., Almarzooq, Z. I., Alonso, A., Beaton, A. Z., Bittencourt, M. S., et al. (2022). Heart disease and stroke statistics-2022 update: A report from the American heart association. Circulation 145, e153–e639. doi:10.1161/CIR.0000000000001052
Wang, G., Jin, Y., Zhang, L., Wang, X., Zhang, Y., Li, Q., et al. (2016). Reporting and methodological quality of systematic reviews and meta-analyses in TCM nursing. J. Nurs. S. C. 31, 98–102. doi:10.3870/j.issn.1001-4152.2016.01.098
Wang, N. L., Liou, Y. L., Lin, M. T., Lin, C. L., and Chang, C. K. (2005). Chinese herbal medicine, Shengmai San, is effective for improving circulatory shock and oxidative damage in the brain during heatstroke. J. Pharmacol. Sci. 97, 253–265. doi:10.1254/jphs.fp0040793
Wang, Y., Liu, Q., Zhang, H., Wang, Y., and Liu, G. (2016). Quality evaluation of systematic review/meta analysis papers on stroke treated with promoting blood circulation for removing blood stasis method: Adopting PRISMA declaration. J. Tradit. Chin. Med. 57, 660–664. doi:10.13288/j.11-2166/r.2016.08.009
Xie, P. S., and Leung, A. Y. (2009). Understanding the traditional aspect of Chinese medicine in order to achieve meaningful quality control of Chinese materia medica. J. Chromatogr. A 1216, 1933–1940. doi:10.1016/j.chroma.2008.08.045
Yu, F., Liu, J., Xin, M., Liu, N., and Liu, H. (2019). Systematic review of TCM intervention for acute myocardial infarction and meta analysis on quality of literature. West Chin. Med. 32, 56–60. doi:10.3969/j.issn.1004-6852.2019.03.015
Zhang, J., Ge, L., Zhao, Y., Wang, Y., Zhang, J., Tian, J., et al. (2015). An introduction to a series of PRISMA statement for systematic review and meta-analysis. Chin. J. Drug Eval. 32, 257–261. doi:10.3969/j.issn.2095-3593.2015.05.001
Keywords: ischemic stroke, traditional Chinese medicine, systematic reviews, meta-analysis, quality
Citation: Sun S, Zhao L, Zhou X, Liu X, Xie Z, Ren J, Zhou B and Pan Y (2023) Methodological, reporting, and evidence quality of systematic reviews of traditional Chinese medicine for ischemic stroke. Front. Pharmacol. 14:1047650. doi: 10.3389/fphar.2023.1047650
Received: 18 September 2022; Accepted: 23 January 2023;
Published: 09 February 2023.
Edited by:
Michael Heinrich, University College London, United KingdomReviewed by:
Chi-Jung Tai, Kaohsiung Medical University, TaiwanCopyright © 2023 Sun, Zhao, Zhou, Liu, Xie, Ren, Zhou and Pan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yawen Pan, cHl3QGx6dS5lZHUuY24=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.