 Jiayi Deng
Jiayi Deng Fanglin Li
Fanglin Li Ningjie Zhang
Ningjie Zhang Yanjun Zhong
Yanjun Zhong
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pharmacol. , 19 October 2022
Sec. Respiratory Pharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.945892
This article is part of the Research Topic Drug Prevention and Control of Ventilator-Associated Pneumonia Volume II View all 12 articles
Ventilator-associated pneumonia (VAP) is the most common acquired infection in the intensive care unit. Recent studies showed that the critical COVID-19 patients with invasive mechanical ventilation have a high risk of developing VAP, which result in a worse outcome and an increasing economic burden. With the development of critical care medicine, the morbidity and mortality of VAP remains high. Especially since the outbreak of COVID-19, the healthcare system is facing unprecedented challenges. Therefore, many efforts have been made in effective prevention, early diagnosis, and early treatment of VAP. This review focuses on the treatment and prevention drugs of VAP in COVID-19 patients. In general, prevention is more important than treatment for VAP. Prevention of VAP is based on minimizing exposure to mechanical ventilation and encouraging early release. There is little difference in drug prophylaxis from non-COVID-19. In term of treatment of VAP, empirical antibiotics is the main treatment, special attention should be paid to the antimicrobial spectrum and duration of antibiotics because of the existence of drug-resistant bacteria. Further studies with well-designed and large sample size were needed to demonstrate the prevention and treatment of ventilator-associated pneumonia in COVID-19 based on the specificity of COVID-19.
Ventilator-associated pneumonia (VAP) is usually regarded as a pneumonia phenomenon that occurs within 48 h after mechanical ventilation to 48 h after extubation, and is the main type of hospital-acquired pneumonia. The risk of VAP in patients with invasive mechanical ventilation is approximately 5%–40%, and has been reported to be different depending on the country, the type of intensive care unit (ICU), and the criteria of VAP identification (American Thoracic and Infectious Diseases Society of, 2005; Seguin et al., 2014). Not only does VAP have a significant attributable mortality rate (4.6%), and VAP remains an integral part of the spectrum of adverse events such as acute respiratory distress syndrome (ARDS) (Spalding et al., 2017). VAP may place a longer hospital course and a greater financial burden on patients (Kalil et al., 2016), with a VAP-related cost of $40,144 (95% CI $36,286–44,220) reported in a survey in the United States in 2013 (Zimlichman et al., 2013). Although our knowledge of VAP has increased, its incidence has not decreased (Wang et al., 2014). Since the outbreak of COVID-19, Earth shaking changes have taken place in global medical care. COVID-19 patients had a high incidence of severe ARDS, many of whom require invasive ventilation and are at a high risk of VAP (Razazi et al., 2020; Maes et al., 2021; Fumagalli et al., 2022; Gosangi et al., 2022), which can make the state of COVID-19 patients more complicated and more strenuous to manage. Besides, COVID-19-associated VAP shows novel characters compared to non-COVID-19 disease (Wicky et al., 2021). Thus, a literature search on the PubMed and Web of Science was done for this review, using the following keywords from 2005 to 2022: “ventilator associated pneumonia” or “ventilator-associated pneumonia” or “ventilator-acquired pneumonia” or “VAP”, “COVID-19” or “SARS-CoV-2”. We aim to review the characteristics, diagnosis, drug prevention and therapy for the management of VAP in COVID-19 patients.
During the COVID-19 pandemic, severe COVID-19 patients were admitted to ICUs, received mechanical ventilation (Chang et al., 2021; COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators, 2021), and have a high incidence of VAP (Ippolito et al., 2021; Wicky et al., 2022).
VAP is thought to be the most common fatal nosocomial infections in ICU (Kalanuria et al., 2014; Haque et al., 2018; Papazian et al., 2020). The reported incidence of VAP varies widely in COVID-19 patients, but was different from studies. We summarized these studies in Table 1. Some studies have shown a higher VAP risk in COVID-19 ARDS patients than in non-COVID-19 ARDS patients (Maes et al., 2021; Nseir et al., 2021; Rouzé et al., 2021; Vacheron et al., 2022a). It has been reported that VAP may bring poor prognosis to patients, with prolonged durations of both mechanical ventilation and ICU stay, and even a high mortality (Papazian et al., 2020). Similarly, the association of VAP with some relevant poor outcomes was also reported in COVID-19 patients in recent studies. Compared with non-COVID-19 patients, VAP in COVID-19 cases was significantly related with 28-day mortality, shock, VAP recurrence, and polymicrobial culture, as well as a significantly longer mechanical ventilation time (Razazi et al., 2020; Maes et al., 2021; Nseir et al., 2021; Rouyer et al., 2021). Meanwhile, compared with the influenza or non-virus infection group, no significant difference in the relationship between VAP with mortality was found in the COVID-19 group (Nseir et al., 2021).
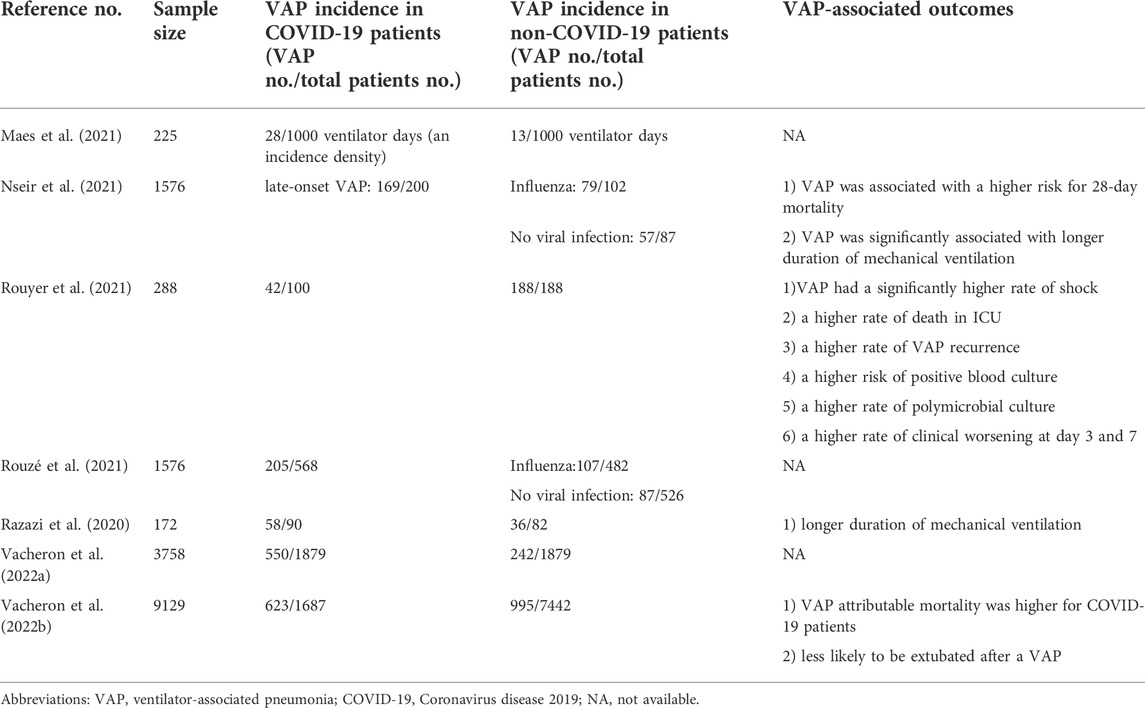
TABLE 1. The characteristics of studies reported ventilator-associated pneumonia in COVID-19.
Potential causes for the increased incidence of VAP include prolonged mechanical ventilation and hospital stay, viral immunomodulation, steroids use, sedating and neuromuscular blocking agents use, vasopressor use, ARDS, prone positioning, applications of extracorporeal mechanical oxygenation, shortages of healthcare workers and inadequate protective equipment corresponding to the increased medical resource demands (Fumagalli et al., 2022). The number of patients requiring invasive ventilation has significantly increased during the COVID-19 pandemic, which has overwhelmed the medical resources (Nacoti et al., 2021).
The prolonged mechanical ventilation was thought to be the most relevant risk factor of VAP (Kalil and Cawcutt, 2022). The patients treated with invasive mechanical ventilation who were accompanied with COVID-19 tend to present a delayed mechanical ventilation and a higher incidence of ARDS than without COVID-19, which are both recognized as risk factors for VAP (Razazi et al., 2020; Blonz et al., 2021; Nseir et al., 2021; Rouzé et al., 2021). It has been suggested that in COVID-19 patients the use of immunomodulatory drugs may promote the development of VAP (Martínez-Martínez et al., 2021). What is more, there are also studies indicating that dexamethasone could accelerate the process of the VAP occurrence (Cour et al., 2021; Gragueb-Chatti et al., 2021). In addition, the prone position, widely applied in the treatment of COVID-19, is associated with an elevated risk of microaspiration (Ayzac et al., 2016), thereby leading to the occurrence of VAP.
The kind of microorganisms responsible for VAP reported is various, which may be explained by the duration of invasive mechanical ventilation, length of hospital and ICU stays before VAP episode, the local ecology, and cumulative exposure and timing to antimicrobials (Papazian et al., 2020). Some studies suggested that gram-negative bacteria were the predominant microorganisms (primarily Pseudomonas aerginosa, Enterobacter spp., Klebsiella spp.) followed by gram-positives (mainly Staphylococcus aureus) responsible for VAP in patients with COVID-19 (Grasselli et al., 2021; Rouzé et al., 2021). Furthermore, there is an increased occurrence of multidrug-resistant (MDR) bacterial strains in patients with COVID-19, one of the reasons may be that most cases of COVID-19-related VAP were diagnosed when invasive mechanical ventilation had been initiated for more than 7 days (late VAP) (Fumagalli et al., 2022). It is reported that multiple drug resistance of Klebsiella pneumoniae and Pseudomonas aeruginosa were isolated from COVID-19 patients (Gregorova et al., 2020; Baba et al., 2021; Ghanizadeh et al., 2021). In addition, a monocenter retrospective study involving 172 patients suggested that compared with non-COVID-19 patients, COVID-19 cases were more likely to develop MDR-related VAP (Razazi et al., 2020). Besides, COVID-19 could lead to severe organ dysfunction and prone to secondary bacterial infections, and then even facilitate the emergence of infectious diseases caused by rare microorganisms. There are also studies of VAP contributed by the rare bacteria Hafnia alvei (Cutuli et al., 2021; Méndez et al., 2021).
It is worth noting that bacteria are not the only cause of VAP. Secondary causes of fungal infection have been reported from first noticed in China, to become a clear manifestation as indicated in European in severe COVID-19 patients (Marr et al., 2021). A clinical study showed that all 134/134 (100%) patients with VAP caused by fungal were already receiving the treatment of corticosteroids and tocilizumab (Meawed et al., 2021). Current studies have shown a higher prevalence of Aspergillus pneumoniae in critical COVID-19 patients compared with the other patients in ICUs. In addition, patients affected by COVID-19 associated invasive pulmonary aspergillosis have a high mortality rate (Lahmer et al., 2021). Moreover, COVID-19 patients can also develop virus-related VAP. Herpesvirade (HSV) activation was also numerically more frequent among COVID-19 than non-COVID-19 cases (Maes et al., 2021). HSV-1 reactivation was related to the increased risks of VAP and mortality in critical COVID-19 patients (Meyer et al., 2021).
Diagnosing VAP in patients with COVID-19 is an appreciable challenge, since substantial overlap exists between the basic clinical symptoms and signs of COVID-19 with secondary infection (Fumagalli et al., 2022). It is considered traditionally that the diagnosis of VAP should be based on three criteria followed: clinical suspicion, new or progressive radiographic infiltrates, and microbiological diagnosis meaning positive microbiological cultures from the lower respiratory tract (Papazian et al., 2020).
We should realize that it is time to consider whether there exists VAP when new clinical signs of respiratory deterioration potentially attributed by infection appear (Papazian et al., 2020). The clinical presentation of COVID-19 includes high fever, severe hypoxemia, hyperleukocytosis, biological inflammatory syndrome, and extensive bilateral radiologic infiltrates in detail. These symptoms overlap highly with VAP, making traditionally clinic diagnosis criteria for VAP invalid in the critical population with COVID-19 (Francois et al., 2020). While discovering new infiltrations in patients based on baseline infiltrations is arduous, the conventional assessment of VAP, chest X-ray or computed tomography imaging, are not suitable for real-time measurement in critical patients. Hence, lung ultrasound has been widely used as a real-time monitoring tool to monitor VAP for critically ill patients in recent years (Kameda et al., 2001; Dargent et al., 2020; Dargent et al., 2021). It must be stated that confirmed diagnosis of VAP depends on the identification of the pathogen. Regardless of the technique used (endotracheal aspiration or bronchoscopy-guided bronchoalveolar lavage), a challenge in diagnosing VAP is reducing the time from sampling to pathogen identification (Papazian et al., 2020).
The widespread use of new molecular technology effectively alleviates this problem and contributes to the increasing incidence of VAP. Tools based on multiplex polymerase chain reaction make it possible to diagnose early VAP and identify VAP usually underdiagnosed by conventional culture-based methods (Cohen et al., 2021; Wicky et al., 2022). It has been reported in the literature, the combination of sequential PCR and electrospray ionization mass spectrometry was a potential rapid technique to diagnose VAP within 6 h (Hou et al., 2020). In addition, the next-generation sequencing (NGS) and even metagenomic NGS (mNGS) are in some distance more effective and rapid for pathogen detections (Toma et al., 2014; He et al., 2022). NGS-based methods and mNGS-based methods can help clinicians to make accurate and precise diagnosis, leading to targeted antimicrobial therapy and improve the prognosis of patients in time.
It is reported that procalcitonin (PCT) can help distinguish virus from bacterial pathogens in patients with VAP, and typical bacteria tend to present higher procalcitonin levels than atypical bacteria or viruses (Self et al., 2017; Modi and Kovacs, 2020). The data of a clinical study suggested that the patients whose PCT was over 0.975 ng/ml were more likely to have VAP, showing that PCT may be an applicable biomarker for VAP diagnosis (Côrtes et al., 2021). In addition, immature granulocytes (IGs) was considered that the threshold was 18% or 2 g/L, and the sensitivity and specificity to identify patients with ventilator-associated pneumonia were 100%, supporting IGs could be a biomarker to help identify pulmonary bacterial infections in this population (Daix et al., 2021).
Intravenous antimicrobial therapy is the cornerstone for drug treatment of VAP. It must be stressed that the emergence of antimicrobial resistance and determining the appropriate type, timing and duration of antibiotics is worthy of attention.
COVID-19 patients on mechanical ventilation have a very high risk of exposure to extensive antibiotic treatment. During their hospitalization, most patients were prescribed several different classes of antibiotics, of which broad-spectrum coverage was commonly used. Cefepime and vancomycin have been reported to be the most commonly used antibiotics, with an average duration of 1 week. (Risa et al., 2021). It is generally recommended that the empirical treatment plan should be based on the local distribution of VAP-related pathogens and their antimicrobial susceptibility, and resistance rates vary widely among countries, regions, and hospitals. Guideline-based empirical antibiotic management results in antibiotic overuse (Pickens et al., 2021). Inappropriate empiric antibiotic use may lead to the emergence of more resistant bacteria.
Antimicrobial resistance is not only a global crisis but also a global problem that attracts the attention of governments and society. Multiple studies showed that drug-resistant and even multidrug-resistant frequently occurred in COVID-19 patients with VAP. Since the outbreak of COVID-19, antibiotic resistance is increasing. The resistance to the ceftazidime and levofloxacin for P. aeruginosa strains was significantly increased, as well as A. baumannii strains (Bahçe et al., 2022). Therefore, drugs for multidrug resistant bacteria infection of VAP, such as polymyxins, ceftazidime avibatan et al. were used to improve the outcomes of COVID-19 patients. Moreover, recent researches suggested that PBT2 may act as a drug resistance inhibitor to rescue the efficacy of commonly used tetracycline antibiotics in the treatment of multidrug-resistant baumannii infection (De Oliveira and Walker, 2022).
The best way to determine a specific antibiotic depends on the evidence of pathogen culture from bronchoalveolar lavage or endotracheal aspiration of the lower airways (Fumagalli et al., 2022). New antimicrobials are undergoing rapid development, aiming to keep pace with the development of multidrug resistance (Cusack et al., 2022). We expect more target drugs to be developed earlier in the future, to implement more precise etiological treatment.
An observational study found that it may be a reasonable therapeutic option to decrease the intubation rate in COVID-19 patients (Mushtaq et al., 2022). Compared with high-dose dexamethasone, tocilizumab seemed to be a much better and safer for controlling the cytokine storm in COVID-19 patients with moderate to severe ARDS (Naik et al., 2021). In contrast to this study, tocilizumab was reported to increase the incidence of VAP in critical COVID-19 patients (Ceccarelli et al., 2021). In addition, it is reported that combination therapy of tocilizumab and steroids is likely to be conducive to managing COVID-19-associated cytokine release syndrome (Dravid et al., 2021). While another research suggested that adding tocilizumab to methylprednisolone did not improve outcomes significantly (Hamed et al., 2021). Further, interferon gamma is proved to have a plausible efficacy in the treatment of recurrent VAP by recovering monocyte activation (Nguyen et al., 2021).
VAP is difficult to manage and it will complicate existing diseases, so we should pay attention to its prevention which is thought to be more important than the treatment of VAP. It is generally believed that the main way to prevent VAP is to reduce the timing of invasive mechanical ventilation, and this part focuses on the pharmacological prevention of VAP.
Ventilated patients usually need to use proton pump inhibitors (PPI) and gastric mucosal protective agent prophylactically because of the risk of stress ulcers. These acid suppressive medications inhibit gastric acid secretion, increase the hydrogen of the gastric juice, and promote bacterial growth (Buendgens et al., 2016). It may be a reason of stress ulcer prophylaxis was reported to be associated with higher VAP rates (Alhazzani et al., 2018; Huang et al., 2018). There were a lot of researches focused on the association of PPI use with COVID-19 (Almario et al., 2020; Elmunzer et al., 2021; Fan et al., 2021; Lee et al., 2021; Ramachandran et al., 2022), and the results showed that PPI use was associated with the increased susceptibility of COVID-19 infection and poor outcome including disease severity and mortality (Fatima et al., 2022). However, the relationship between PPI use and VAP in COVID-19 patients still needs to be demonstrated. A meta-analysis suggested that sucralfate, a gastric mucosal protective agent, could significantly decrease the occurrence of VAP, but cannot affect the days on ventilator, duration of ICU stay, and ICU mortality (He et al., 2014). Hence, sucralfate would be a good choice to prevent stress ulcers in critical ill patients with invasive mechanical ventilation.
Selective digestive decontamination (SDD) is demonstrated to be effective in reducing the occurrence of VAP in non-COVID-19 patients (Liberati et al., 2009; Minozzi et al., 2021; van der Meer et al., 2021). In COVID-19 patients, a retrospective observational study that included 178 subjects on invasive mechanical ventilation more than 2 days, showed that the use of SDD significantly reduced the incidence of VAP (Luque-Paz et al., 2022). But, the evidence level of this study limited the reliability for its retrospective and observational design. Therefore, SDD deserves more consideration to use in critical COVID-19 patients.
Chlorhexidine, a drug used in oral hygiene care for over 2 decades, can reduce oral colonization, and prevent the occurrence of VAP (Zand et al., 2017). Besides, the combination of chlorhexidine with toothbrushing was more satisfactory in preventing VAP in patients on mechanical ventilation, compared with chlorhexidine alone (Silva et al., 2021). However, several studies were questioning the efficacy and safety of oral chlorhexidine. It has been reported in some studies that the use of chlorhexidine oral care may increase mortality, owing to the occurrence of acute lung injury resulting from aspirating the anticorrosive composition of chlorhexidine (Klompas et al., 2014a; Klompas, 2017; Deschepper et al., 2018; Harris et al., 2018). In COVID-19 patients, Chlorhexidine was reported to be effective in reducing SARS-CoV-2 load in the oral cavity (Costa et al., 2021). More research is needed in the future to clarify the safety and efficacy of chlorhexidine in preventing VAP for COVID-19 patients.
The microbiota plays an important role in the risk of intestinal complications and the disease severity of COVID-19 patients (Zanza et al., 2021). Probiotics may be an attractive intervention for preventing VAP in adult hospitalized patients by modulating the intestinal microbiome and reducing the colonization of pathogens (Papazian et al., 2020; Su et al., 2020; Kullar et al., 2021). Systematic reviews also support the protective role of probiotics in preventing VAP (Rozga et al., 2021). But the evidence levels of these included studies were low and existing significant heterogeneity, the use of probiotics for preventing VAP in COVID-19 patients remains controversial.
Early enteral nutrition is recommended to prevent VAP in critically ill non-COVID-19 patients (Klompas et al., 2014b) and critical COVID-19 patients (Haines et al., 2022). A study of real-world clinical practice showed that early enteral nutrition within 3 days after invasive mechanical ventilation can shorten the time of invasive mechanical ventilation and improve the outcome of COVID-19 patients (Haines et al., 2022). The mechanisms of early enteral nutrition in preventing VAP may involve reducing pathogen colonization and bacterial translocation through facilitating intestinal peristalsis and maintaining intestinal mucosal structure and barrier function. However, a large number of patients failed to initiate early enteral nutrition for hemodynamic instability, fear of aspiration, and significant gastrointestinal complications.
A narrative literature review proved that selenium supplementation could reduce the incidence of VAP, shorten the length of hospital stay, and decrease mortality through decreasing the inflammatory cytokines (Mahmoodpoor et al., 2018; Oliveira et al., 2022). In COVID-19 patients, a higher prevalence of selenium deficiencies was found, especially in older cases (Voelkle et al., 2022). However, direct evidence of selenium supplementation in preventing VAP is needed in further research.
As mentioned above, during the COVID-19 era, VAP has drawn more attention than before due to its high incidence and high mortality. Patients who develop ARDS and require invasive mechanical ventilation after SARS-CoV-2 infection are at a higher risk to experience VAP episodes than non-COVID-19 ARDS patients. Despite extensive research, the diagnosis, prevention and treatment of VAP remain a challenge. At present, strict hospital management measures and standardized procedures to prevent VAP. As for clinical treatment, the application of antibiotics remains recommended, especially the resistance of antibacterial drugs is a serious problem, attracting people’s attention. Further studies with well-designed and large sample size were needed to demonstrate the prevention and treatment of ventilator-associated pneumonia in COVID-19 based on the specificity of COVID-19.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alhazzani, W., Alshamsi, F., Belley-Cote, E., Heels-Ansdell, D., Brignardello-Petersen, R., Alquraini, M., et al. (2018). Efficacy and safety of stress ulcer prophylaxis in critically ill patients: A network meta-analysis of randomized trials. Intensive Care Med. 44, 1–11. doi:10.1007/s00134-017-5005-8
Almario, C. V., Chey, W. D., and Spiegel, B. M. R. (2020). Increased risk of COVID-19 among users of proton pump inhibitors. Am. J. Gastroenterol. 115, 1707–1715. doi:10.14309/ajg.0000000000000798
American Thoracic, S., and Infectious Diseases Society of, A. (2005). Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 171, 388–416. doi:10.1164/rccm.200405-644ST
Ayzac, L., Girard, R., Baboi, L., Beuret, P., Rabilloud, M., Richard, J. C., et al. (2016). Ventilator-associated pneumonia in ARDS patients: The impact of prone positioning. A secondary analysis of the proseva trial. Intensive Care Med. 42, 871–878. doi:10.1007/s00134-015-4167-5
Baba, H., Kanamori, H., Seike, I., Niitsuma-Sugaya, I., Takei, K., Oshima, K., et al. (2021). Multiple secondary healthcare-associated infections due to carbapenem-resistant organisms in a critically ill COVID-19 patient on extensively prolonged venovenous extracorporeal membrane oxygenation support-A case report. Microorganisms 10, 19. doi:10.3390/microorganisms10010019
Bahçe, Y. G., Acer, Ö., and Özüdoğru, O. (2022). Evaluation of bacterial agents isolated from endotracheal aspirate cultures of Covid-19 general intensive care patients and their antibiotic resistance profiles compared to pre-pandemic conditions. Microb. Pathog. 164, 105409. doi:10.1016/j.micpath.2022.105409
Blonz, G., Kouatchet, A., Chudeau, N., Pontis, E., Lorber, J., Lemeur, A., et al. (2021). Epidemiology and microbiology of ventilator-associated pneumonia in COVID-19 patients: A multicenter retrospective study in 188 patients in an un-inundated French region. Crit. Care (Houten). 25, 72. doi:10.1186/s13054-021-03493-w
Buendgens, L., Koch, A., and Tacke, F. (2016). Prevention of stress-related ulcer bleeding at the intensive care unit: Risks and benefits of stress ulcer prophylaxis. World J. Crit. Care Med. 5, 57–64. doi:10.5492/wjccm.v5.i1.57
Ceccarelli, G., Alessandri, F., Oliva, A., Dell'Isola, S., Rocco, M., Ruberto, F., et al. (2021). Superinfections in patients treated with Teicoplanin as anti-SARS-CoV-2 agent. Eur. J. Clin. Invest. 51, e13418. doi:10.1111/eci.13418
Chang, R., Elhusseiny, K. M., Yeh, Y. C., and Sun, W. Z. (2021). COVID-19 ICU and mechanical ventilation patient characteristics and outcomes-A systematic review and meta-analysis. PLoS One 16, e0246318. doi:10.1371/journal.pone.0246318
Cohen, R., Babushkin, F., Finn, T., Geller, K., Alexander, H., Datnow, C., et al. (2021). High rates of bacterial pulmonary Co-infections and superinfections identified by multiplex PCR among critically ill COVID-19 patients. Microorganisms 9, 2483. doi:10.3390/microorganisms9122483
Côrtes, M. F., de Almeida, B. L., Espinoza, E. P. S., Campos, A. F., do Nascimento Moura, M. L., Salomão, M. C., et al. (2021). Procalcitonin as a biomarker for ventilator associated pneumonia in COVID-19 patients: Is it an useful stewardship tool? Diagn. Microbiol. Infect. Dis. 101, 115698. doi:10.1016/j.diagmicrobio.2022.115698
Costa, D. D., Brites, C., Vaz, S. N., de Santana, D. S., Dos Santos, J. N., and Cury, P. R. (2021). Chlorhexidine mouthwash reduces the salivary viral load of SARS-CoV-2: A randomized clinical trial. Oral Dis. doi:10.1111/odi.14086
COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators (2021). Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: A prospective cohort study. Intensive Care Med. 47, 60–73. doi:10.1007/s00134-020-06294-x
Cour, M., Simon, M., Argaud, L., Monneret, G., and Venet, F. (2021). Effects of dexamethasone on immune dysfunction and ventilator-associated pneumonia in COVID-19 acute respiratory distress syndrome: An observational study. J. Intensive Care 9, 64. doi:10.1186/s40560-021-00580-6
Cusack, R., Garduno, A., Elkholy, K., and Martín-Loeches, I. (2022). Novel investigational treatments for ventilator-associated pneumonia and critically ill patients in the intensive care unit. Expert Opin. Investig. Drugs 31, 173–192. doi:10.1080/13543784.2022.2030312
Cutuli, S. L., De Maio, F., De Pascale, G., Grieco, D. L., Monzo, F. R., Carelli, S., et al. (2021). COVID-19 influences lung microbiota dynamics and favors the emergence of rare infectious diseases: A case report of Hafnia alvei pneumonia. J. Crit. Care 64, 173–175. doi:10.1016/j.jcrc.2021.04.008
Daix, T., Jeannet, R., Hernandez Padilla, A. C., Vignon, P., Feuillard, J., and François, B. (2021). Immature granulocytes can help the diagnosis of pulmonary bacterial infections in patients with severe COVID-19 pneumonia. J. intensive care 9, 58. doi:10.1186/s40560-021-00575-3
Dargent, A., Chatelain, E., Kreitmann, L., Quenot, J. P., Cour, M., Argaud, L., et al. (2020). Lung ultrasound score to monitor COVID-19 pneumonia progression in patients with ARDS. PLoS One 15, e0236312. doi:10.1371/journal.pone.0236312
Dargent, A., Chatelain, E., Si-Mohamed, S., Simon, M., Baudry, T., Kreitmann, L., et al. (2021). Lung ultrasound score as a tool to monitor disease progression and detect ventilator-associated pneumonia during COVID-19-associated ARDS. Heart Lung. 50, 700–705. doi:10.1016/j.hrtlng.2021.05.003
De Oliveira, D. M. P., and Walker, M. J. (2022). An ionophore breaks the multi-drug-resistance of Acinetobacter baumannii. Microb. Cell. 9, 69–71. doi:10.15698/mic2022.03.772
Deschepper, M., Waegeman, W., Eeckloo, K., Vogelaers, D., and Blot, S. (2018). Effects of chlorhexidine gluconate oral care on hospital mortality: A hospital-wide, observational cohort study. Intensive Care Med. 44, 1017–1026. doi:10.1007/s00134-018-5171-3
Dravid, A., Kashiva, R., Khan, Z., Memon, D., Kodre, A., Potdar, P., et al. (2021). Combination therapy of tocilizumab and steroid for management of COVID-19 associated cytokine release syndrome: A single center experience from pune, western India. Med. Baltim. 100, e26705. doi:10.1097/MD.0000000000026705
Elmunzer, B. J., Wolf, B. J., Scheiman, J. M., Tierney, W. M., Taylor, J. R., and North, C. (2021). American alliance for the study of digestive manifestations of, association between preadmission acid suppressive medication exposure and severity of illness in patients hospitalized with COVID-19. Gastroenterology 160, 1417–1422 e14.
Fan, X., Liu, Z., Miyata, T., Dasarathy, S., Rotroff, D. M., Wu, X., et al. (2021). Effect of acid suppressants on the risk of COVID-19: A propensity score-matched study using UK biobank. Gastroenterology 160, 455–458 e5. doi:10.1053/j.gastro.2020.09.028
Fatima, K., Almas, T., Lakhani, S., Jahangir, A., Ahmed, A., Siddiqui, A., et al. (2022). The use of proton pump inhibitors and COVID-19: A systematic review and meta-analysis. Trop. Med. Infect. Dis. 7, 37. doi:10.3390/tropicalmed7030037
Francois, B., Laterre, P. F., Luyt, C. E., and Chastre, J. (2020). The challenge of ventilator-associated pneumonia diagnosis in COVID-19 patients. Crit. Care 24, 289. doi:10.1186/s13054-020-03013-2
Fumagalli, J., Panigada, M., Klompas, M., and Berra, L. (2022). Ventilator-associated pneumonia among SARS-CoV-2 acute respiratory distress syndrome patients. Curr. Opin. Crit. Care 28, 74–82. doi:10.1097/MCC.0000000000000908
Ghanizadeh, A., Najafizade, M., Rashki, S., Marzhoseyni, Z., and Motallebi, M. (2021). Genetic diversity, antimicrobial resistance pattern, and biofilm formation in Klebsiella pneumoniae isolated from patients with coronavirus disease 2019 (COVID-19) and ventilator-associated pneumonia. Biomed. Res. Int. 2021, 2347872. doi:10.1155/2021/2347872
Gosangi, B., Rubinowitz, A. N., Irugu, D., Gange, C., Bader, A., and Cortopassi, I. (2022). COVID-19 ARDS: A review of imaging features and overview of mechanical ventilation and its complications. Emerg. Radiol. 29, 23–34. doi:10.1007/s10140-021-01976-5
Gragueb-Chatti, I., Lopez, A., Hamidi, D., Guervilly, C., Loundou, A., Daviet, F., et al. (2021). Impact of dexamethasone on the incidence of ventilator-associated pneumonia and blood stream infections in COVID-19 patients requiring invasive mechanical ventilation: A multicenter retrospective study. Ann. Intensive Care 11, 87. doi:10.1186/s13613-021-00876-8
Grasselli, G., Scaravilli, V., Mangioni, D., Scudeller, L., Alagna, L., Bartoletti, M., et al. (2021). Hospital-acquired infections in critically ill patients with COVID-19. Chest 160, 454–465. doi:10.1016/j.chest.2021.04.002
Gregorova, M., Morse, D., Brignoli, T., Steventon, J., Hamilton, F., Albur, M., et al. (2020). Post-acute COVID-19 associated with evidence of bystander T-cell activation and a recurring antibiotic-resistant bacterial pneumonia. Elife 9. doi:10.7554/elife.63430
Haines, K., Parker, V., Ohnuma, T., Krishnamoorthy, V., Raghunathan, K., Sulo, S., et al. (2022). Role of early enteral nutrition in mechanically ventilated COVID-19 patients. Crit. Care Explor. 4, e0683. doi:10.1097/CCE.0000000000000683
Hamed, D. M., Belhoul, K. M., Al Maazmi, N. A., Ghayoor, F., Moin, M., Al Suwaidi, M., et al. (2021). Intravenous methylprednisolone with or without tocilizumab in patients with severe COVID-19 pneumonia requiring oxygen support: A prospective comparison. J. Infect. Public Health 14, 985–989. doi:10.1016/j.jiph.2021.06.003
Haque, M., Sartelli, M., McKimm, J., and Abu Bakar, M. B. (2018). Health care-associated infections - an overview. Infect. Drug Resist. 11, 2321–2333. doi:10.2147/IDR.S177247
Harris, B. D., Thomas, G. A., Greene, M. H., Spires, S. S., and Talbot, T. R. (2018). Ventilator bundle compliance and risk of ventilator-associated events. Infect. Control Hosp. Epidemiol. 39, 637–643. doi:10.1017/ice.2018.30
He, H., Hu, S., Chen, Q., Liu, L., Huang, Y., Yang, Y., et al. (2014). Effects of sucralfate and acid-suppressive drugs on preventing ventilator- associated pneumonia of mechanically ventilated patients: A meta-analysis. Zhonghua Nei Ke Za Zhi 53, 48–54.
He, Y., Fang, K., Shi, X., Yang, D., Zhao, L., Yu, W., et al. (2022). Enhanced DNA and RNA pathogen detection via metagenomic sequencing in patients with pneumonia. J. Transl. Med. 20, 195. doi:10.1186/s12967-022-03397-5
Hou, D., Ju, M., Wang, Y., Zhang, D., Zhu, D., Zhong, M., et al. (2020). PCR coupled to electrospray ionization mass spectrometry for microbiological diagnosis and surveillance of ventilator-associated pneumonia. Exp. Ther. Med. 20, 3587–3594. doi:10.3892/etm.2020.9103
Huang, H. B., Jiang, W., Wang, C. Y., Qin, H. Y., and Du, B. (2018). Stress ulcer prophylaxis in intensive care unit patients receiving enteral nutrition: A systematic review and meta-analysis. Crit. Care 22, 20. doi:10.1186/s13054-017-1937-1
Ippolito, M., Misseri, G., Catalisano, G., Marino, C., Ingoglia, G., Alessi, M., et al. (2021). Ventilator-associated pneumonia in patients with COVID-19: A systematic review and meta-analysis. Antibiot. (Basel) 10, 545. doi:10.3390/antibiotics10050545
Kalanuria, A., Zai, W., and Mirski, M. (2014). Ventilator-associated pneumonia in the ICU. Crit. Care 18, 208. doi:10.1186/cc13775
Kalil, A. C., and Cawcutt, K. A. (2022). Is ventilator-associated pneumonia more frequent in patients with coronavirus disease 2019? Crit. Care Med. 50, 522–524. doi:10.1097/CCM.0000000000005389
Kalil, A. C., Metersky, M. L., Klompas, M., Muscedere, J., Sweeney, D. A., Palmer, L. B., et al. (2016). Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American thoracic society. Clin. Infect. Dis. 63, e61–e111. doi:10.1093/cid/ciw353
Kameda, T., Mizuma, Y., Taniguchi, H., Fujita, M., and Taniguchi, N. (2001). Point-of-care lung ultrasound for the assessment of pneumonia: A narrative review in the COVID-19 era. J. Med. Ultrason. 48 (2021), 31–43. doi:10.1007/s10396-020-01074-y
Klompas, M., Branson, R., Eichenwald, E. C., Greene, L. R., Howell, M. D., Lee, G., et al. (2014). Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect. Control Hosp. Epidemiol. 35, S133–S154. doi:10.1017/s0899823x00193894
Klompas, M. (2017). Oropharyngeal decontamination with antiseptics to prevent ventilator-associated pneumonia: Rethinking the benefits of chlorhexidine. Semin. Respir. Crit. Care Med. 38, 381–390. doi:10.1055/s-0037-1602584
Klompas, M., Speck, K., Howell, M. D., Greene, L. R., and Berenholtz, S. M. (2014). Reappraisal of routine oral care with chlorhexidine gluconate for patients receiving mechanical ventilation: Systematic review and meta-analysis. JAMA Intern. Med. 174, 751–761. doi:10.1001/jamainternmed.2014.359
Kullar, R., Johnson, S., McFarland, L. V., and Goldstein, E. J. C. (2021). Potential roles for probiotics in the treatment of COVID-19 patients and prevention of complications associated with increased antibiotic use. Antibiot. (Basel) 10, 408. doi:10.3390/antibiotics10040408
Lahmer, T., Kriescher, S., Herner, A., Rothe, K., Spinner, C. D., Schneider, J., et al. (2021). Invasive pulmonary aspergillosis in critically ill patients with severe COVID-19 pneumonia: Results from the prospective AspCOVID-19 study. PLoS One 16, e0238825. doi:10.1371/journal.pone.0238825
Lee, S. W., Ha, E. K., Yeniova, A. O., Moon, S. Y., Kim, S. Y., Koh, H. Y., et al. (2021). Severe clinical outcomes of COVID-19 associated with proton pump inhibitors: A nationwide cohort study with propensity score matching. Gut 70, 76–84. doi:10.1136/gutjnl-2020-322248
Liberati, A., D'Amico, R., Pifferi, S., Torri, V., Brazzi, L., and Parmelli, E. (2009). Antibiotic prophylaxis to reduce respiratory tract infections and mortality in adults receiving intensive care. Cochrane Database Syst. Rev. 2009, CD000022. doi:10.1002/14651858.CD000022.pub3
Luque-Paz, D., Tattevin, P., Jaubert, P., Reizine, F., Kouatchet, A., and Camus, C. (2022). Selective digestive decontamination to reduce the high rate of ventilator-associated pneumonia in critical COVID-19. Anaesth. Crit. Care Pain Med. 41, 100987. doi:10.1016/j.accpm.2021.100987
Maes, M., Higginson, E., Pereira-Dias, J., Curran, M. D., Parmar, S., Khokhar, F., et al. (2021). Ventilator-associated pneumonia in critically ill patients with COVID-19. Crit. Care (Houten). 25, 25. doi:10.1186/s13054-021-03460-5
Mahmoodpoor, A., Hamishehkar, H., Sanaie, S., Behruzizad, N., Iranpour, A., Koleini, E., et al. (2018). Antioxidant reserve of the lungs and ventilator-associated pneumonia: A clinical trial of high dose selenium in critically ill patients. J. Crit. Care 44, 357–362. doi:10.1016/j.jcrc.2017.12.016
Marr, K. A., Platt, A., Tornheim, J. A., Zhang, S. X., Datta, K., Cardozo, C., et al. (2021). Aspergillosis complicating severe coronavirus disease. Emerg. Infect. Dis. 27, 18–25. doi:10.3201/eid2701.202896
Martínez-Martínez, M., Plata-Menchaca, E. P., Nuvials, F. X., Roca, O., and Ferrer, R. (2021). Risk factors and outcomes of ventilator-associated pneumonia in COVID-19 patients: A propensity score matched analysis. Crit. Care 25, 235. doi:10.1186/s13054-021-03654-x
Meawed, T. E., Ahmed, S. M., Mowafy, S. M. S., Samir, G. M., and Anis, R. H. (2021). Bacterial and fungal ventilator associated pneumonia in critically ill COVID-19 patients during the second wave. J. Infect. Public Health 14, 1375–1380. doi:10.1016/j.jiph.2021.08.003
Méndez, L., Ferreira, J., and Caneiras, C. (2021). Hafnia alvei pneumonia: A rare cause of infection in a patient with COVID-19. Microorganisms 9, 2369. doi:10.3390/microorganisms9112369
Meyer, A., Buetti, N., Houhou-Fidouh, N., Patrier, J., Abdel-Nabey, M., Jaquet, P., et al. (2021). HSV-1 reactivation is associated with an increased risk of mortality and pneumonia in critically ill COVID-19 patients. Crit. Care 25, 417. doi:10.1186/s13054-021-03843-8
Minozzi, S., Pifferi, S., Brazzi, L., Pecoraro, V., Montrucchio, G., and D'Amico, R. (2021). Topical antibiotic prophylaxis to reduce respiratory tract infections and mortality in adults receiving mechanical ventilation. Cochrane Database Syst. Rev. 1, CD000022. doi:10.1002/14651858.CD000022.pub4
Modi, A. R., and Kovacs, C. S. (2020). Hospital-acquired and ventilator-associated pneumonia: Diagnosis, management, and prevention. Cleve. Clin. J. Med. 87, 633–639. doi:10.3949/ccjm.87a.19117
Mushtaq, M. Z., Mahmood, S. B. Z., Almas, A., Ather Wasti, S., and Ahsan Ali, S. (2022). Tocilizumab in critically ill COVID-19 patients: An observational study. Int. Immunopharmacol. 102, 108384. doi:10.1016/j.intimp.2021.108384
Nacoti, M., Ciocca, A., Brambillasca, P., Fazzi, F., Pisano, M., Giupponi, M., et al. (2021). A community-based model to the COVID-19 humanitarian crisis. Front. Cell. Infect. Microbiol. 11, 639579. doi:10.3389/fcimb.2021.639579
Naik, N. B., Puri, G. D., Kajal, K., Mahajan, V., Bhalla, A., Kataria, S., et al. (2021). High-dose dexamethasone versus tocilizumab in moderate to severe COVID-19 pneumonia: A randomized controlled trial. Cureus 13, e20353. doi:10.7759/cureus.20353
Nguyen, L. S., Ait Hamou, Z., Gastli, N., Chapuis, N., and Pène, F. (2021). Potential role for interferon gamma in the treatment of recurrent ventilator-acquired pneumonia in patients with COVID-19: A hypothesis. Intensive Care Med. 47, 619–621. doi:10.1007/s00134-021-06377-3
Nseir, S., Martin-Loeches, I., Povoa, P., Metzelard, M., Du Cheyron, D., Lambiotte, F., et al. (2021). Relationship between ventilator-associated pneumonia and mortality in COVID-19 patients: A planned ancillary analysis of the coVAPid cohort. Crit. Care 25, 177. doi:10.1186/s13054-021-03588-4
Oliveira, C. R., Viana, E. T., Gonçalves, T. F., Mateus-Silva, J. R., and Vieira, R. P. (2022). Therapeutic use of intravenous selenium in respiratory and immunological diseases: A narrative review. Adv. Respir. Med. 90, 134–142. doi:10.5603/ARM.a2022.0018
Papazian, L., Klompas, M., and Luyt, C. E. (2020). Ventilator-associated pneumonia in adults: A narrative review. Intensive Care Med. 46, 888–906. doi:10.1007/s00134-020-05980-0
Pickens, C. O., Gao, C. A., Cuttica, M. J., Smith, S. B., Pesce, L. L., Grant, R. A., et al. (2021). Bacterial superinfection pneumonia in patients mechanically ventilated for COVID-19 pneumonia. Am. J. Respir. Crit. Care Med. 204, 921–932. doi:10.1164/rccm.202106-1354OC
Ramachandran, P., Perisetti, A., Gajendran, M., Jean-Louis, F., Bansal, P., Dwivedi, A. K., et al. (2022). Pre-hospitalization proton pump inhibitor use and clinical outcomes in COVID-19. Eur. J. Gastroenterol. Hepatol. 34, 137–141. doi:10.1097/MEG.0000000000002013
Razazi, K., Arrestier, R., Haudebourg, A. F., Benelli, B., Carteaux, G., Decousser, J. W., et al. (2020). Risks of ventilator-associated pneumonia and invasive pulmonary aspergillosis in patients with viral acute respiratory distress syndrome related or not to Coronavirus 19 disease. Crit. Care 24, 699. doi:10.1186/s13054-020-03417-0
Risa, E., Roach, D., Budak, J. Z., Hebert, C., Chan, J. D., Mani, N. S., et al. (2021). Characterization of secondary bacterial infections and antibiotic use in mechanically ventilated patients with COVID-19 induced acute respiratory distress syndrome. J. Intensive Care Med. 36, 1167–1175. doi:10.1177/08850666211021745
Rouyer, M., Strazzulla, A., Youbong, T., Tarteret, P., Pitsch, A., de Pontfarcy, A., et al. (2021). Ventilator-associated pneumonia in COVID-19 patients: A retrospective cohort study. Antibiot. (Basel) 10, 988. doi:10.3390/antibiotics10080988
Rouzé, A., Martin-Loeches, I., Povoa, P., Makris, D., Artigas, A., Bouchereau, M., et al. (2021). Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: A European multicenter cohort study. Intensive Care Med. 47, 188–198. doi:10.1007/s00134-020-06323-9
Rozga, M., Cheng, F. W., and Handu, D. (2021). Effects of probiotics in conditions or infections similar to COVID-19 on health outcomes: An evidence analysis center scoping review. J. Acad. Nutr. Diet. 121, 1841–1854. doi:10.1016/j.jand.2020.07.016
Seguin, P., Laviolle, B., Dahyot-Fizelier, C., Dumont, R., Veber, B., Gergaud, S., et al. (2014). Effect of oropharyngeal povidone-iodine preventive oral care on ventilator-associated pneumonia in severely brain-injured or cerebral hemorrhage patients: A multicenter, randomized controlled trial. Crit. Care Med. 42, 1–8. doi:10.1097/CCM.0b013e3182a2770f
Self, W. H., Balk, R. A., Grijalva, C. G., Williams, D. J., Zhu, Y., Anderson, E. J., et al. (2017). Procalcitonin as a marker of etiology in adults hospitalized with community-acquired pneumonia. Clin. Infect. Dis. 65, 183–190. doi:10.1093/cid/cix317
Silva, P. U. J., Paranhos, L. R., Meneses-Santos, D., Blumenberg, C., Macedo, D. R., and Cardoso, S. V. (2021). Combination of toothbrushing and chlorhexidine compared with exclusive use of chlorhexidine to reduce the risk of ventilator-associated pneumonia: A systematic review with meta-analysis. Clin. (Sao Paulo) 76, e2659. doi:10.6061/clinics/2021/e2659
Spalding, M. C., Cripps, M. W., and Minshall, C. T. (2017). Ventilator-associated pneumonia: New definitions. Crit. Care Clin. 33, 277–292. doi:10.1016/j.ccc.2016.12.009
Su, M., Jia, Y., Li, Y., Zhou, D., and Jia, J. (2020). Probiotics for the prevention of ventilator-associated pneumonia: A meta-analysis of randomized controlled trials. Respir. Care 65, 673–685. doi:10.4187/respcare.07097
Toma, I., Siegel, M. O., Keiser, J., Yakovleva, A., Kim, A., Davenport, L., et al. (2014). Single-molecule long-read 16S sequencing to characterize the lung microbiome from mechanically ventilated patients with suspected pneumonia. J. Clin. Microbiol. 52, 3913–3921. doi:10.1128/JCM.01678-14
Vacheron, C. H., Lepape, A., Savey, A., Machut, A., Timsit, J. F., Comparot, S., et al. (2022). Attributable mortality of ventilator-associated pneumonia among patients with COVID-19. Am. J. Respir. Crit. Care Med. 206, 161–169. doi:10.1164/rccm.202202-0357OC
Vacheron, C. H., Lepape, A., Savey, A., Machut, A., Timsit, J. F., Vanhems, P., et al. (2022). Increased incidence of ventilator-acquired pneumonia in coronavirus disease 2019 patients: A multicentric cohort study. Crit. Care Med. 50, 449–459. doi:10.1097/CCM.0000000000005297
van der Meer, S. B., Figaroa, G., van der Voort, P. H. J., Nijsten, M. W., and Pillay, J. (2021). Ventilator-associated pneumonia in critically-ill patients with COVID-19 in a setting of selective decontamination of the digestive tract. Crit. Care (Houten). 25, 445. doi:10.1186/s13054-021-03869-y
Voelkle, M., Gregoriano, C., Neyer, P., Koch, D., Kutz, A., Bernasconi, L., et al. (2022). Prevalence of micronutrient deficiencies in patients hospitalized with COVID-19: An observational cohort study. Nutrients 14, 1862. doi:10.3390/nu14091862
Wang, Y., Eldridge, N., Metersky, M. L., Verzier, N. R., Meehan, T. P., Pandolfi, M. M., et al. (2014). National trends in patient safety for four common conditions, 2005-2011. N. Engl. J. Med. 370, 341–351. doi:10.1056/NEJMsa1300991
Wicky, P. H., d'Humières, C., and Timsit, J. F. (2022). How common is ventilator-associated pneumonia after coronavirus disease 2019? Curr. Opin. Infect. Dis. 35, 170–175. doi:10.1097/QCO.0000000000000817
Wicky, P. H., Niedermann, M. S., and Timsit, J. F. (2021). Ventilator-associated pneumonia in the era of COVID-19 pandemic: How common and what is the impact? Crit. Care 25, 153. doi:10.1186/s13054-021-03571-z
Zand, F., Zahed, L., Mansouri, P., Dehghanrad, F., Bahrani, M., and Ghorbani, M. (2017). The effects of oral rinse with 0.2% and 2% chlorhexidine on oropharyngeal colonization and ventilator associated pneumonia in adults' intensive care units. J. Crit. Care 40, 318–322. doi:10.1016/j.jcrc.2017.02.029
Zanza, C., Romenskaya, T., Thangathurai, D., Ojetti, V., Saviano, A., Abenavoli, L., et al. (2021). Microbiome in critical care: An unconventional and unknown ally. Curr. Med. Chem. 29, 3179–3188. doi:10.2174/0929867328666210915115056
Keywords: ventilator-associated pneumonia, COVID-19, SARS-CoV-2, nosocomial infection, antibiotic, acute respiratory distress syndrome, ARDS
Citation: Deng J, Li F, Zhang N and Zhong Y (2022) Prevention and treatment of ventilator-associated pneumonia in COVID-19. Front. Pharmacol. 13:945892. doi: 10.3389/fphar.2022.945892
Received: 17 May 2022; Accepted: 07 October 2022;
Published: 19 October 2022.
Edited by:
Zhi Mao, People’s Liberation Army General Hospital, ChinaReviewed by:
Dmytro Dmytriiev, National Pirogov Memorial Medical University, UkraineCopyright © 2022 Deng, Li, Zhang and Zhong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ningjie Zhang, em5qXzEyMzE4OEBjc3UuZWR1LmNu; Yanjun Zhong, emhvbmd5YW5qdW5AY3N1LmVkdS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.