 Pu Ge
Pu Ge Ning Wan
Ning Wan Xiao Han
Xiao Han Xinpei Wang
Xinpei Wang Jinzi Zhang
Jinzi Zhang Xiaoyi Long
Xiaoyi Long Xiaonan Wang
Xiaonan Wang Ying Bian
Ying Bian
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 30 August 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.914683
Background: Metastatic colorectal cancer (mCRC) imposes a heavy tumor burden worldwide due to limited availability of therapeutic drugs. Aflibercept, a kind of recombinant protein of the anti-vascular endothelial growth factor (VEGF) family, has been approved in clinical application among mCRC patients since 2012. A comprehensive analysis of the efficacy, safety, and cost-effectiveness of aflibercept in mCRC treatment is necessary.
Objective: To evaluate the efficacy, safety, and cost-effectiveness of aflibercept for the treatment of mCRC in order to provide a decision-making reference for the selection of targeted drugs for second-line treatment of mCRC in Hong Kong, Macao, and Taiwan regions of China and the selection of new drugs for medical institutions in these regions.
Methods: A systematic retrieve on databases including PubMed, Embase, Cochrane Library, China National Knowledge Infrastructure (CNKI), Wanfang, and Weipu, as well as relevant websites and databases of health technology assessment including the National Institute of Health and Clinical Optimization, Centre for Evaluation and Communication at the University of York, and the Canadian Agency for Medicines and Health Technology, was conducted. The literature was screened according to the inclusion and exclusion criteria, and data were extracted and analyzed by two authors, while the quality of the literature was assessed.
Results: Finally, we included two HTA reports, 11 systematic reviews/meta-analyses, and two cost-effectiveness studies in the rapid health technology assessment. For mCRC patients receiving second-line treatment, aflibercept combined with FOLFIRI significantly increased progression-free survival (PFS) and overall survival (OS) and the objective response rate (ORR) also improved, compared with folinic acid + fluorouracil + irinotecan (FOLFIRI). In terms of safety, mCRC patients who received aflibercept combined with FOLFIRI therapy had a higher incidence of grade 3–4 adverse events than those who received FOLFIRI alone, including anti-VEGF–related adverse events (hypertension, hemorrhagic events, and proteinuria) and chemotherapy-related adverse events (diarrhea, weakness, stomatitis, hand-foot syndrome, neutropenia, and thrombocytopenia). In terms of cost-effectiveness, two economic studies conducted in the United Kingdom and Japan, respectively, found that compared with FOLFIRI, aflibercept combined with FOLFIRI had no cost-effectiveness advantage in mCRC patients receiving second-line treatment.
Conclusion: Compared with FOLFIRI treatment, aflibercept combined with FOLFIRI for the second-line treatment of mCRC patients has better efficacy, worse safety, and is not cost-effective. More high-quality clinical studies are required for further exploration of aflibercept’s clinical value. Medical institutions in Hong Kong, Macao, and Taiwan regions of China should be cautious when using or introducing aflibercept plus FOLFIRI as a mCRC treatment.
Colorectal cancer, as one of the most common gastrointestinal malignancies, features high incidence, high death rate, and low cure rate and seriously threatens human health. The 2020 data showed that the incidence and mortality rate of colorectal cancer in the world, respectively, ranked third and second of all cancers, of which 1.932 million were new cases and 935,000 deaths (Sung et al., 2021). Patients with early colorectal cancer show lack of specific symptoms, and the screening for it is not commonly performed in most parts of the world (Halama and Haberkorn, 2020). All of these reasons make early diagnosis of colorectal cancer difficult; therefore, most patients are diagnosed in the middle or late stages and may even have metastatic colorectal cancer (mCRC). According to the anatomy of the splenic flexure, colorectal cancer can be divided into left colon cancer and right colon cancer, with approximate incidence of 69.6% and 30.3%, respectively (Broman et al., 2019). About 50% of patients with colorectal cancer have wild-type RAS genes (Yaeger et al., 2015). At present, the clinical treatment of mCRC is mainly based on radiotherapy, chemotherapy, and combination targeted therapy (Glynne-Jones et al., 2017; Modest et al., 2019; You et al., 2020). As a macromolecular monoclonal antibody–targeted drug, aflibercept can inhibit the growth, invasion, and metastasis of cancer cells by blocking the vascular endothelial growth factor (VEGF) (Holash et al., 2002; Saif, 2013). Based on the results of the randomized controlled trial VELOUR, the drug was approved by the FDA in 2012 in combination with FOLFIRI for second-line treatment of mCRC (FDA approves aflibercept, 2012; Li et al., 2018). Later, the therapy was approved in Japan and the European Union. On 13 February 2018, Bayer announced that the China Food and Drug Administration has approved the marketing application of aflibercept intraocular injection solution for the treatment of adult diabetic macular edema (DME) (Zhou et al., 2022). However, in mainland China, there is no aflibercept preparation for mCRC on the market; in other words, in mainland China, it has not yet been used for mCRC treatment. Situation differs in Hong Kong, Macau, and Taiwan regions of China, where aflibercept has already got approval for mCRC treatment in 2013–2014 (Yaozhi Data, 2014; Pharnexcloud, 2021; SSM, 2021).
Health technology assessment (HTA) can systematically evaluate the technical characteristics, effectiveness, safety, and socioeconomic attributes of health technologies, providing decision makers of health and healthcare and medical personnel with scientific information and an evidence-based basis for the rational choice of health technologies (Chen et al., 2018). It takes a lot of time and resources to carry out a comprehensive health technology assessment; when time and conditions are limited, through rapid assessment, the existing main evidence is sorted out and analyzed relatively efficiently, which can provide certain information support for decision makers in the clinical environment. The therapy has been approved for nearly a decade, and data on its efficacy, safety, and cost-effectiveness have been accumulating through this time. A certain number of secondary literature and economic studies on clinical efficacy and safety have been accumulated around aflibercept, which provide an evidence basis for rapid evaluation. The objective of this study is to evaluate the efficacy, safety, and cost-effectiveness of aflibercept in the treatment of mCRC in order to provide a decision-making reference for the selection of targeted drugs for second-line treatment of mCRC in Hong Kong, Macao, and Taiwan regions of China and the selection of new drugs for medical institutions in these regions.
We included published HTA reports, systematic reviews (SR) or meta-analyses, and pharmacoeconomic studies.
Patients diagnosed with mCRC were of any gender, ethnicity, onset, and origin, but all the patients should be adults. Considering the current status of antineoplastic drug research and the clinical characteristics of adverse events, for safety, a wider range of tumor patients were included for a more comprehensive assessment.
The trial group consisted of aflibercept monotherapy or chemotherapy (CT), and the control group was CT with or without other positive controls or the best supportive care. Both the experimental group and the control group were second-line treatments for mCRC, with unlimited doses and courses of treatments.
Efficacy measures include overall survival (OS), progression-free survival (PFS), objective response rate (ORR), complete response (CR), partial response (PR), and disease control rate (DCR). Safety indicators include the incidence of overall adverse events (AE), incidence of serious adverse events, and incidence of various types of adverse events. Economic indicator includes the incremental cost-effectiveness ratio (ICER).
The exclusion criteria include (1) repeated publications, (2) literature with lack of data or inability to obtain the full text, and (3) non-Chinese and English literature.
We searched databases including PubMed, Embase, the Cochrane Library, CNKI, Wanfang, and Weipu, as well as the official websites and related databases including the National Institute of Health and Clinical Optimization, Centre for Evaluation and Communication at the University of York, and Canadian Agency for Medicines and Health Technology, and included HTA reports. SR or meta-analysis and pharmacoeconomic studies on aflibercept for metastatic colorectal cancer were searched in full text with aflibercept, systematic review, Meta-analysis, economics, cost, economics, and health technology assessment as keywords in English and Chinese, respectively, with a search time frame from the date of database creation to 11 November 2021. In addition, as a supplement, a manual search of references of included studies was conducted. The search strategy for PubMed, as an example, was as Table 1. The search strategies for other databases can be found in Supplementary Table S1.

TABLE 1. Search strategy for PubMed.
After the literature was deduplicated, two researchers (Pu Ge and Xiaonan Wang) screened and cross-checked by reading the title, abstract, and full text according to the inclusion and exclusion criteria, and if there was any disagreement, they would negotiate with the third researcher (Xiao Han).
The basic data were independently extracted by two researchers according to the pre-designed data extraction table, including first author, publication year, intervention/control measures, and outcome indicators. If the included literature was incomplete, we would contact the original author to obtain it.
Here, two investigators used different tools to evaluate the quality of all included literature. For HTA, the HTA checklist (Hailey and Topfer, 2003) was used for quality evaluation, which was an initiative of the International Network of Agencies for Health Technology Assessment (INAHTA); for systematic reviews/meta-analyses, the AMSTAR-2 scale (Shea et al., 2017) was used for quality evaluation; and for economic studies, the CHEERS scale (Husereau et al., 2013) was used for quality evaluation.
Because of the high heterogeneity of study types, this study used descriptive methods to assess outcomes. Qualitative profiling methods were used to classify, compare, and analyze the results of the included studies according to the study design, patient population, and intervention/control measures of each study.
Figure 1 shows the flow chart of study selection. In the initial search, 2397 relevant research works were identified (290 research works from PubMed, 1055 from EMBASE, 149 from Cochrane Library, 877 from CNKI, 15 from Wanfang, five from Weipu, one from Center for Reviews and Dissemination of York University, and two from National Institute for Health Research of United Kingdom). After the exclusion of seven duplicate studies, 2390 studies underwent a title and abstract review. A total of 2344 studies were excluded at the initial screening stage. For the remaining 46 studies, the full text was reviewed, and 29 of them were excluded for following reasons: language is not Chinese or English (n = 1), duplication of research findings (n = 2), intervention method not eligible (n = 13), required outcomes not reported (n = 1), research type not eligible (n = 1), study population not eligible (n = 1), and research purpose fail to meet the requirements (n = 10). The 15 remaining studies fulfilled the eligibility criteria and were included in the rapid assessment, including two HTA reports, 11 SR/meta-analysis, and two cost-effectiveness research works.
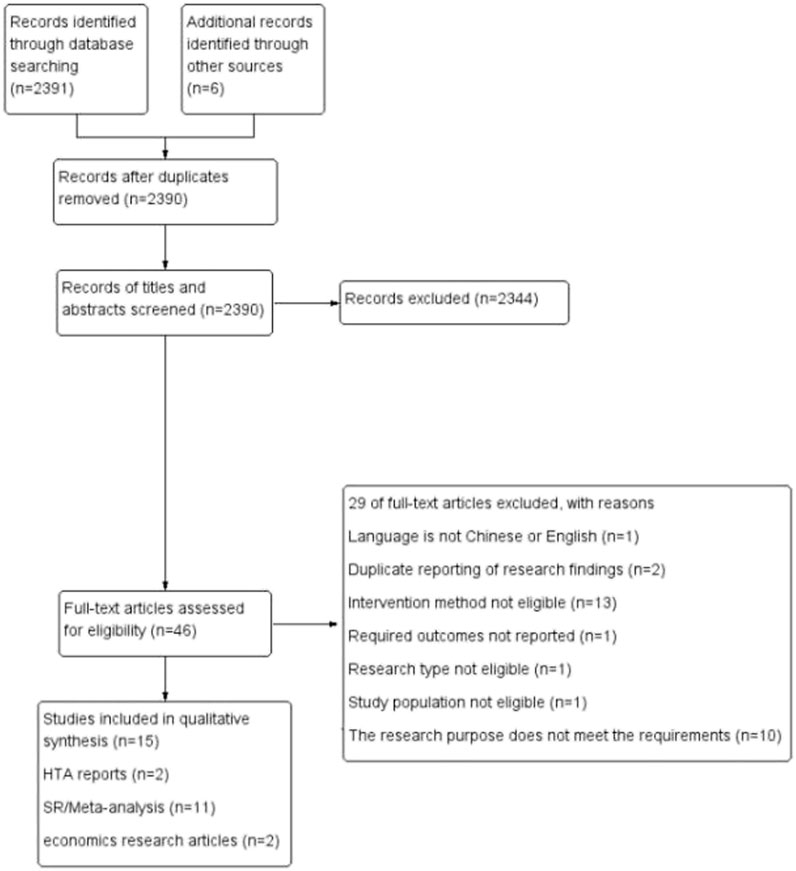
FIGURE 1. Flow chart of literature screening.
The main characteristics of the included HTA reports, SR/meta-analyses, and economics studies are reported in Tables 2-4. The overall quality of the literature was moderate for HTA reports, low for SR/meta-analyses, and high for economics studies.
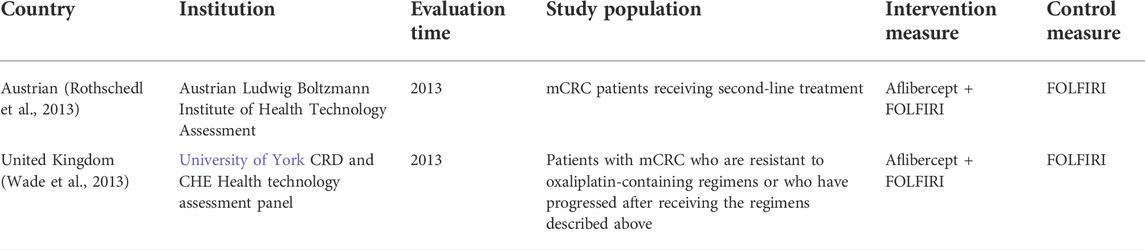
TABLE 2. Basic characteristics of included HTAs.
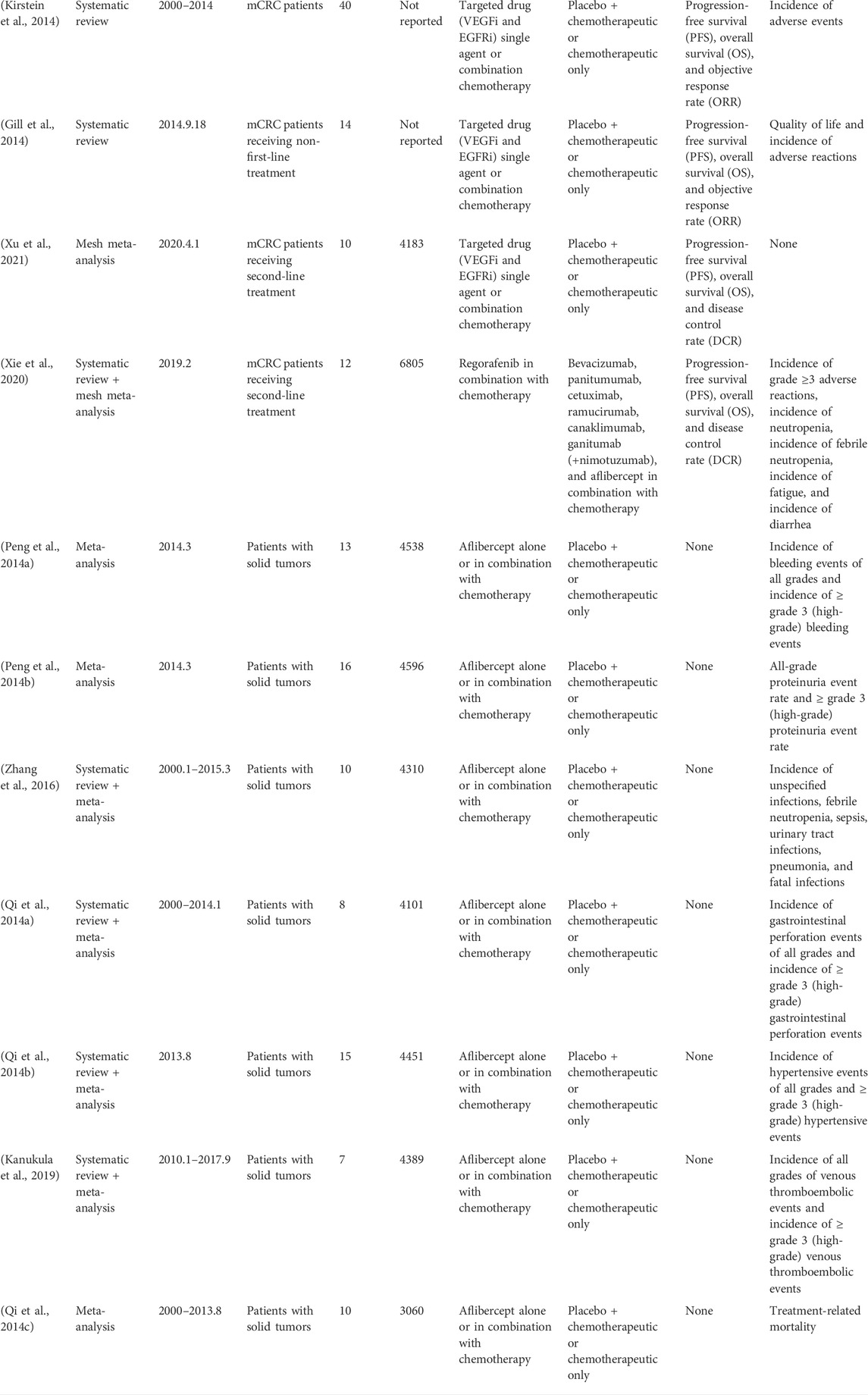
TABLE 3. Data extraction of included SRs/meta-analyses.
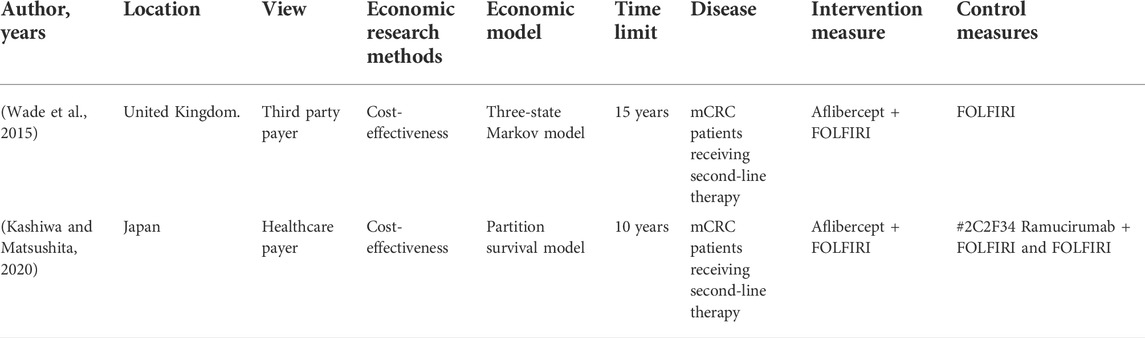
TABLE 4. Summary of included pharmacoeconomic studies.
The quality evaluation results of HTA are shown in Table 5. It can be seen from Table 4 that the HTA reports included in this study are of high quality.
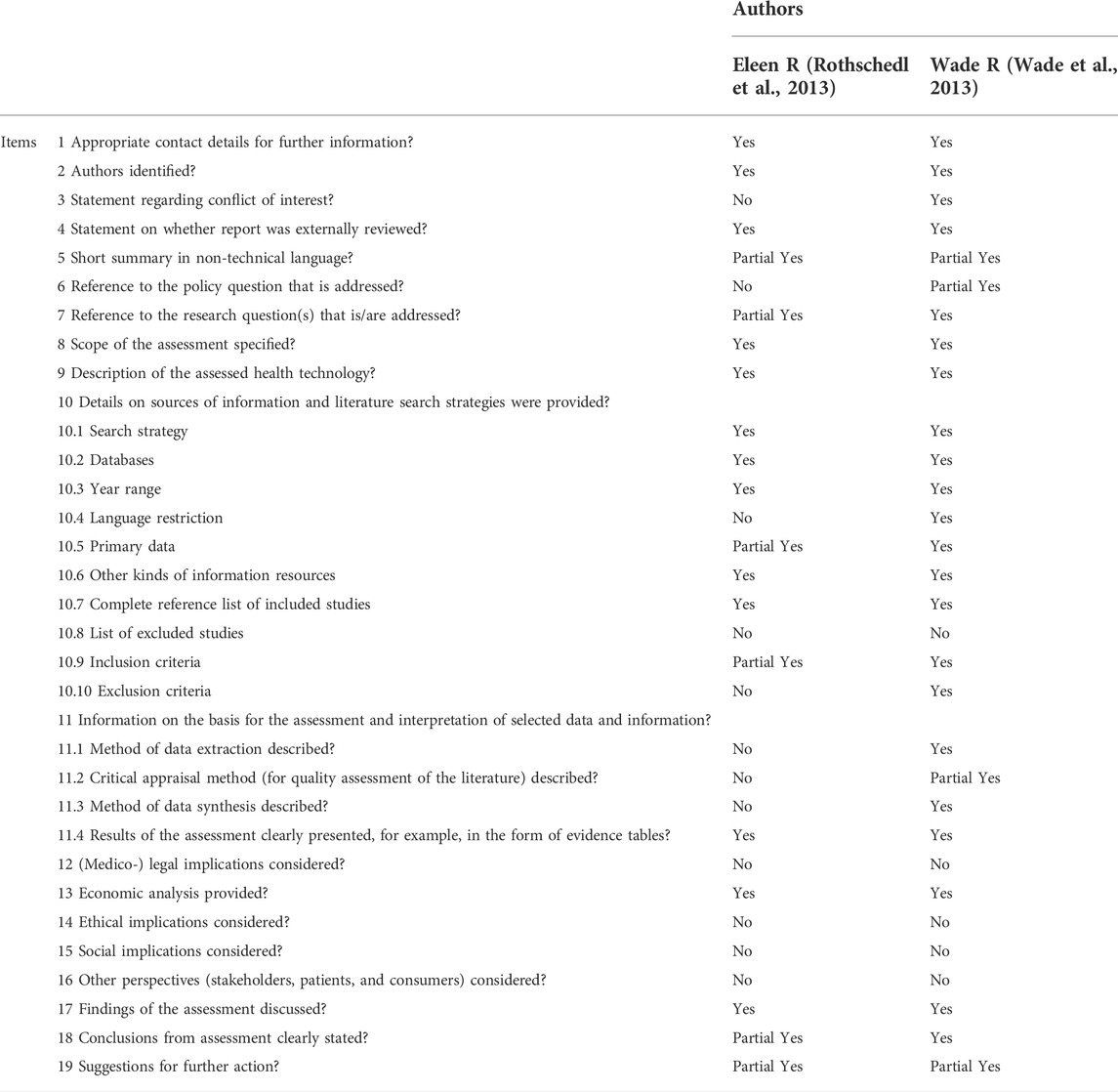
TABLE 5. Quality evaluation of included HTA.
The quality evaluation results of the SR/Meta-analysis are shown in Table 6. Table 7 shows that the quality of the SR/meta-analysis included in this study is relatively low. Studies excluding Xiaoyu Xie (Peng et al., 2014a; Qi et al., 2014a; Peng et al., 2014b; Qi et al., 2014b; Qi et al., 2014c; Gill et al., 2014; Kirstein et al., 2014; Zhang et al., 2016; Kanukula et al., 2019; Xie et al., 2020; Xu et al., 2021) had defects in “Item 2”. This item required the author to write a research plan and register or publish it before conducting a systematic review, but none of the studies mentions the existence of the plan. “Item seven” required a list of excluded studies and reasons for exclusion, but none of the included studies (Peng et al., 2014a; Qi et al., 2014a; Peng et al., 2014b; Qi et al., 2014b; Qi et al., 2014c; Gill et al., 2014; Kirstein et al., 2014; Zhang et al., 2016; Kanukula et al., 2019; Xie et al., 2020; Xu et al., 2021) provided a detailed list of excluded studies. The aforementioned two items were important areas of the quality evaluation, so the quality evaluation results of SR/meta-analysis were relatively low.
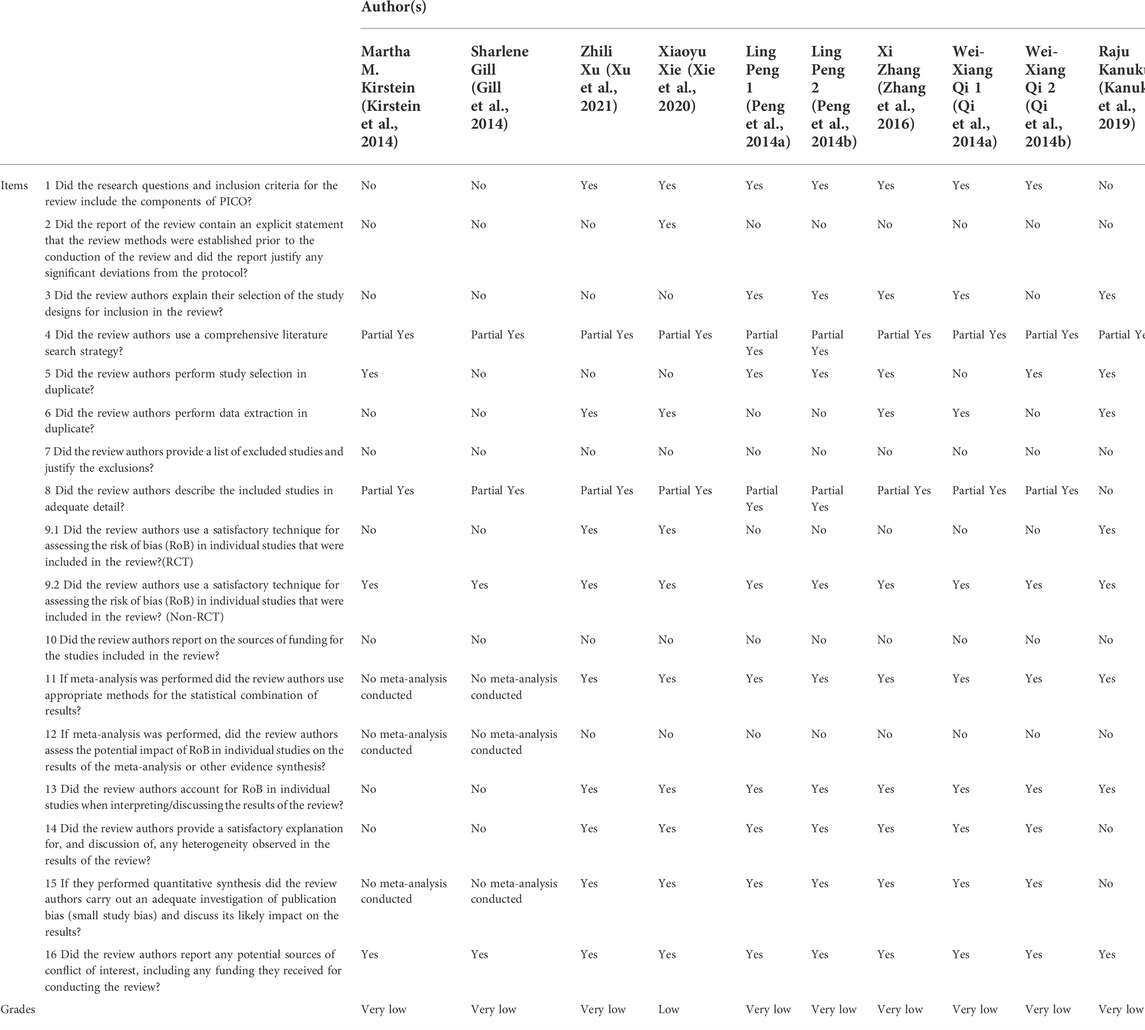
TABLE 6. Quality evaluation of included SR/meta-analysis.
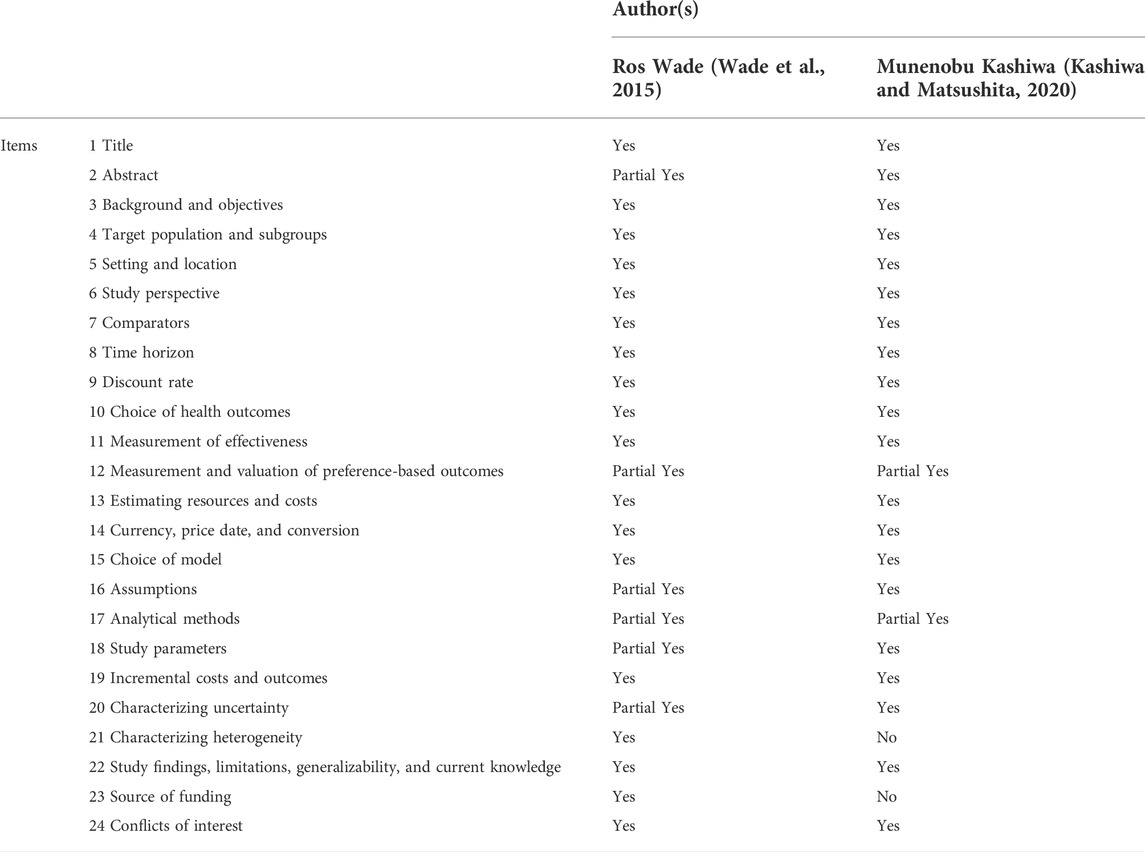
TABLE 7. Quality evaluation of included pharmacoeconomic studies.
The quality evaluation results of economic research are shown in Table 7. According to Table 6, in Wade et al. (2015), the complete coincidence rate of each item on the CHEERS scale was 75% and the total coincidence rate was 100%, while in Kashiwa and Matsushita (2020), the complete coincidence rate of each item on the CHEERS scale was 83.33% and the total coincidence rate was 91.67%, both of which were relatively high. The quality of economic research included was relatively high.
The HTA report (Rothschedl et al., 2013) from the Ludwig Boltzmann Institute for Health Technology Assessment in Austria reported the results of a phase II clinical trial of aflibercept monotherapy in metastatic colorectal cancer (Tang et al., 2012). The study was conducted at seven Canadian clinical research centers and one American research center. In this study, patients were divided into two arms according to whether they had received bevacizumab before: the arm that had not received bevacizumab before (arm 1) (n = 24) and the arm that had received bevacizumab before (arm 2) (n = 50). Among the 24 patients who had not received bevacizumab before, eight (33.33%) patients had stable disease for 8 weeks, and five (20.83%) patients had stable disease for over 16 weeks. Median PFS was 2 months (95% CI 1.7–8.6 months) for the arm not received bevacizumab before and 2.4 months (95% CI 1.9–3.7 months) for the arm that received bevacizumab before, respectively. Also, median OS was 10.4 months (95% CI 7.6–15.5 months) and 8.5 months (95% CI 6.2–10.6 months), respectively.
A total of two HTA reports (Rothschedl et al., 2013; Wade et al., 2013) and four SR/meta-analyses (Gill et al., 2014; Kirstein et al., 2014; Xie et al., 2020; Xu et al., 2021) reported the effectiveness of aflibercept in combination with FOLFIRI for mCRC. Among them, there were two HTA reports and three SR/meta-analyses (Rothschedl et al., 2013; Wade et al., 2013; Gill et al., 2014; Kirstein et al., 2014; Xie et al., 2020) that included VELOUR (a randomized controlled trial), and one SR/meta-analysis (Xu et al., 2021) included VELOUR and another randomized controlled trial.
VELOUR (Qi et al., 2014b) is a prospective, multinational, randomized, double-blind, parallel phase III randomized clinical study conducted in 176 clinical research centers in 28 countries. In this study, patients with metastatic colorectal cancer previously treated with oxaliplatin-based chemotherapy regimens were randomized into two arms: the experimental group (n = 612) treated with aflibercept plus FOLFIRI and the control group (n = 614) treated with placebo plus FOLFIRI. The objective response rate was 19.8% in the experimental group and 11.1% in the control group. Results show a significant difference between the experimental group and the control group (p < 0.001). The median PFS of the experimental group was 6.90 months (95% CI 6.51–7.2 months) and that of the control group was 4.67 months (95% CI 4.21–5.36 months); the HR of the experimental group to the control group was 0.758 (95% CI 0.661–0.869, p < 0.0001). The median OS of the experimental group was 13.50 months (95% CI 12.517–14.949 months) and that of the control group was 12.06 months (95% CI 11.072–13.109 months); the HR of the experimental group to the control group was 0.817 (95% CI 0.713–0.937, p = 0.0032). There were significant differences in median PFS and median OS between the experimental and control groups. The study also found that the efficacy of aflibercept was not related to previous bevacizumab treatment. This study provides crucial evidence for the approval of aflibercept combined with FOLFIRI for second-line treatment in patients with metastatic colorectal cancer who progressed or were resistant to oxaliplatin after oxaliplatin treatment.
Xu et al. (2021) conducted a network meta-analysis to compare the efficacy of second-line treatment for metastatic colorectal cancer. In total, two randomized controlled trials with aflibercept were included in the study. The experimental group was aflibercept plus chemotherapy, and the control group was placebo plus chemotherapy. In these two trials, compared with the control group, the HR of OS was 0.81 (95% CI 0.72–0.92) and that of PFS was 0.69 (95% CI 0.54–0.88). At the same time, the researchers compared the OS and PFS of the aflibercept plus chemotherapy group with other second-line therapies, such as bevacizumab plus chemotherapy, cetuximab plus chemotherapy, ramucirumab plus chemotherapy, and panitumumab plus chemotherapy, but no significant difference was found.
Xie et al. (2020) conducted a mesh meta-analysis to compare the efficacy of regorafenib plus chemotherapy with other second-line regimens for metastatic colorectal cancer. In this study, aflibercept plus chemotherapy and regorafenib plus chemotherapy were indirectly compared, with HR 0.81 for OS (95% CI 0.55–1.18), 1.04 for PFS (95% CI 0.73–1.47), and OR 0.988 for ORR (95% CI 0.413–2.18). There was no significant difference in the efficacy between aflibercept plus chemotherapy and regorafenib plus chemotherapy in this study.
In total, two HTA and nine SR/meta-analyses (Rothschedl et al., 2013; Wade et al., 2013; Peng et al., 2014a; Qi et al., 2014a; Peng et al., 2014b; Qi et al., 2014b; Qi et al., 2014c; Gill et al., 2014; Kirstein et al., 2014; Zhang et al., 2016; Kanukula et al., 2019) reported the safety of the VELOUR test. In the VELOUR test (Van Cutsem et al., 2012), the incidence of all-grade adverse events in the experimental group (aflibercept plus FOLFIRI) was 99.2%, grade 3 was 62.0%, and grade 4 was 21.4%. In the control group (placebo plus FOLFIRI), the incidence of all-grade adverse events was 97.9%, grade 3 was 45.1%, and grade 4 was 17.4%. The incidence of anti-VEGF–related adverse events (hypertension, hemorrhagic, thromboembolism, and proteinuria) and chemotherapy-related adverse events (diarrhea, weakness, stomatitis, palmar-plantar erythrodysesthesia syndrome, grade 3/4 neutropenia, and thrombocytopenia) in the experimental group was also higher than those in the control group.
A total of seven meta-analyses examined the incidence of different adverse events in patients with solid tumors treated with aflibercept. The results of six meta-analyses showed that patients with solid tumors treated with aflibercept had a higher rate of all-grade (RR = 2.63, 95% CI 2.07–3.34) and high-grade hemorrhagic events (RR = 2.45, 95% CI 1.62–3.72), all-grade (RR = 1.41, 95% CI 1.13–1.77) and high-grade proteinuria (RR = 6.79, 95% CI 3.10–14.89), high-grade (RR = 1.87, 95% CI 1.52–2.30) and fatal infection (OR = 2.16, 95% CI 1.14–4.11), all-grade (OR = 3.76, 95% CI 1.94–7.25) and high-grade gastrointestinal perforation (OR = 4.14, 95% CI 2.12–8.06), all-grade (OR = 4.47, 95% CI 3.84–5.22) and high-grade hypertension (OR = 4.97, 95% CI 3.95–6.27), and the risk of treatment-related death (OR = 1.81, 95% CI 1.20–2.72) than those in the control group which was only treated with chemotherapy. In contrast, the results of a meta-analysis (Peng et al., 2014b) showed that in the mCRC population, there was no significant difference in the risk of all-grade (RR = 1.00 95% CI 0.67–1.51) and high-grade venous thromboembolism (RR = 1.08 95% CI 0.67–1.73) in the experimental group (with aflibercept) compared to the control group.
In total, two pharmacoeconomic studies (Wade et al., 2015; Kashiwa and Matsushita, 2020) included cost-effectiveness analysis: one conducted in the United Kingdom and the other in Japan. Qi et al. (2014a) compared the cost-effectiveness of aflibercept combined with FOLFIRI and FOLFIRI alone. Kashiwa and Matsushita (2020) compared the cost-effectiveness of aflibercept combined with FOLFIRI, ramucirumab combined with FOLFIRI, and FOLFIRI alone.
Wade et al. (2015) described the manufacturer’s cost-effectiveness analysis of aflibercept FOLFIRI for second-line treatment of mCRC and the review of the manufacturer’s cost-effectiveness analysis results by the Evidence Review Group (ERG). The manufacturer used the three-state Markov model to simulate the cost-effectiveness after 15 years of treatment with aflibercept plus FOLFIRI. The cost included drug cost, adverse event treatment cost, and follow-up treatment cost. The manufacturer’s cost-effectiveness results showed that the ICER per QALY (quality-adjusted life year) of aflibercept combined with FOLFIRI is £ 36,294/QALY compared with FOLFIRI. The ERG believed that the manufacturer’s estimate of the efficacy of aflibercept + FOLFIRI was too optimistic. The manufacturer did not fully consider the cost of drug infusion and management. In addition, the patient group in the manufacturer’s model was younger than the actual population. After the preliminary review by the ERG, the manufacturer revised the model to include an additional cost of £ 15 for the infusion of aflibercept and £ 45 for additional dosing time and re-estimated the efficacy of aflibercept + FOLFIRI. In the revised model, compared with FOLFIRI, the ICER of aflibercept combined with FOLFIRI was £ 42,242/QALY. The ERG believed that the ICER estimation of each QALY of aflibercept combined with FOLFIRI in the revised model was still too low and did not correspond to the actual situation. The ERG estimated that the ICER of aflibercept combined with FOLFIRI was between £ 50,991/QALY and £ 55,139/QALY compared with FOLFIRI. Based on the cost-effectiveness analysis results provided by the manufacturer and the analysis of the evidence review team, the evidence review team believed that aflibercept combined with FOLFIRI had no cost-effectiveness advantage in the treatment of MCRC compared with FOLFIRI. Finally, NICE issued guidance based on the available findings that abciximab in combination with FOLFIRI was not recommended for the treatment of mCRC progressed or was resistant to oxaliplatin after oxaliplatin treatment.
Kashiwa and Matsushita (2020), based on the perspective of medical insurance payers, using partitioned survival analysis, simulated the cost-effectiveness of mCRC patients after 10 years of treatment with aflibercept plus FOLFIRI, ramucirumab plus FOLFIRI, or FOLFIRI treatment. Drug costs (targeted drugs, chemotherapy drugs, and other drugs) and other costs (various testing costs, contrast agent costs, prescription costs, dispensing costs, follow-up costs, and chemotherapy management costs) were considered. The analysis showed that in Japan, the combination of aflibercept or ramucirumab with FOLFIRI was not cost-effective compared with FOLFIRI treatment, although it could improve the efficacy. Compared with FOLFIRI, the ICER of aflibercept or ramucirumab combined with FOLFIRI was $31010/QALY and $52229/QALY, respectively. It was more cost-effective to add aflibercept than to add ramucirumab.
According to the rapid health technology assessment, for mCRC patients who were resistant or progressing after first-line oxaliplatin treatment, aflibercept combined with FOLFIRI could improve PFS, OS, and ORR compared with FOLFIRI alone. Somehow, a clinical study (Tang et al., 2012) included in the HTA from Austria showed that aflibercept as a single agent for the second-line treatment of mCRC had no significant therapeutic effect. Furthermore, two studies of network meta-analysis (Xie et al., 2020; Xu et al., 2021) compared the efficacy of aflibercept plus FOLFIRI with other second-line therapies (regorafenib plus FOLFIRI, bevacizumab plus chemotherapy, cetuximab plus chemotherapy, ramucirumab plus chemotherapy, and panitumumab plus chemotherapy) in the mCRC treatment, but no significant difference in efficacy was found among aflibercept plus FOLFIRI and other included second-line therapies.
However, compared with FOLFIRI, aflibercept plus FOLFIRI had a higher incidence of high-grade adverse events in mCRC treatment (Van Cutsem et al., 2012; Peng et al., 2014a; Qi et al., 2014a; Peng et al., 2014b; Qi et al., 2014b; Qi et al., 2014c; Zhang et al., 2016). Adverse events in patients treated with aflibercept plus FOLFIRI were divided into two categories: one was anti-VEGF–related adverse events, such as hypertension, hemorrhagic events, thromboembolism, and proteinuria, and the other was chemotherapy-related adverse events, such as diarrhea, weakness, stomatitis, hand-foot syndrome, neutropenia, and thrombocytopenia. The application of aflibercept increased the incidence of these two categories of adverse events, which caused many patients to stop treatment, and a large number of patients had to bear additional adverse reaction management costs for this, which would also increase their financial burden. Several studies (Peng et al., 2014a; Peng et al., 2014b; Gill et al., 2014; Zhang et al., 2016) compared the risk of adverse events in patients with cancer treated with aflibercept or bevacizumab and found that the overall risk of high-grade adverse events in patients receiving aflibercept was higher than that of patients receiving bevacizumab. The risks of several types of adverse events such as high-grade bleeding, proteinuria, and infections in patients receiving aflibercept were also significantly higher than those in patients receiving bevacizumab.
In total, two cost-effectiveness analysis studies (Wade et al., 2015; Kashiwa and Matsushita, 2020) showed that, compared with FOLFIRI, aflibercept combined with FOLFIRI had higher ICER in mCRC patients in the United Kingdom and Japan, and the ICER was also higher than the willingness to pay threshold of their country. Manufacturers should further improve the production process, and relevant agencies in various countries should actively negotiate with manufacturers to work together to reduce the price of the drug and increase its availability.
Among the clinical studies of aflibercept combined with chemotherapy in mCRC, only one RCT was conducted in several study sites including China (including mainland China, Hong Kong, and Taiwan), which is AFLAME by Li et al. (2018). This was a prospective, multicenter, multinational, randomized, double-blind, parallel group, phase III study carried out at 37 active sites in mainland China, Hong Kong, Japan, Singapore, and Taiwan. Patients aged 18 years or older with histologically or cytologically proven adenocarcinoma of the colon or rectum that was metastatic and not amenable to potentially curative treatment (i.e., inoperable) were eligible. Patients were randomly assigned (2:1) to aflibercept plus FOLFIRI or placebo plus FOLFIRI centrally via an interactive voice response system (IVRS) using permuted-block randomization, stratified according to baseline ECOG performance status (0 vs. 1) and prior bevacizumab (yes vs. no). Between 27 July 2012 and 19 March 2014, 332 patients were enrolled and randomly assigned to treatment groups: 223 to aflibercept plus FOLFIRI and 109 to placebo plus FOLFIRI. But in this clinical study, some problems arose. Due to the clinical supply misallocation, 198 (60%) of 332 patients received at least one cycle of misallocated treatment (aflibercept or placebo, all still received FOLFIRI): 122 of 223 in the aflibercept plus FOLFIRI group and 76 of 109 in the placebo plus FOLFIRI group. Finally, 111 patients received aflibercept plus FOLFIRI, 188 patients received mixed administration, and 33 patients received placebo plus FOLFIRI. The Data Monitoring Committee did not stop the study despite the misallocation. Ultimately, the researchers concluded that despite the misallocation, the study demonstrated that the addition of aflibercept to FOLFIRI chemotherapy improved PFS, overall survival, and response rate in patients from the Asia-Pacific region with oxaliplatin-pretreated mCRC. No new safety concerns were identified in this patient population. Together, these data suggest a favorable benefit–risk ratio for the aflibercept plus FOLFIRI combination in this setting. This study provides some evidence for the launch of aflibercept in combination with FOLFIRI in the treatment of mCRC in China, but due to the limitations of this study, the results of this study should be treated with caution.
At present, the guidelines for mCRC in France, the United States, and Japan (Aparicio et al., 2020; Hashiguchi et al., 2020; Benson et al., 2021) recommend that aflibercept can be combined with FOLFIRI for the second-line treatment of mCRC. However, the US NCCN guidelines (Benson et al., 2021) also pointed out that bevacizumab has a higher priority than aflibercept in the second-line treatment of mCRC, which was in contrast to the relatively higher price and relatively higher adverse effect rate of aflibercept. However, if the patient was resistant to bevacizumab, aflibercept was a viable option for second-line treatment. In clinical work, doctors should evaluate the health and physical strength of patients in various aspects, improve examinations, and select drugs based on the actual conditions of the patients.
This study has several advantages. It comprehensively summarizes the secondary evidence of aflibercept combined with chemotherapy for the treatment of mCRC and comprehensively analyzes the efficacy, safety, and cost-effectiveness of the therapy, which provides not only some evidence-based evidence for the clinical application of this therapy but also evidence for its drug selection decision in Hong Kong, Macao, and Taiwan regions of China.
This study also has some limitations. First, it focused on the analysis of the efficacy of aflibercept combined with FOLFIRI in the second-line treatment of mCRC. Due to the lack of direct head-to-head studies, the subgroup data of the network meta-analysis included was partially adopted. The quality of the evidence may be lower than direct research. The results might be affected by publication bias. Second, this study was a rapid assessment, with mainly qualitative analysis as well as potentially limited result.
Compared with FOLFIRI, aflibercept combined with FOLFIRI in the second-line mCRC treatment had better efficacy, but it was less safe and did not have a cost-effectiveness advantage. In the future, randomized controlled trials should be further carried out to clarify the effectiveness and safety of this therapy, and its effectiveness and safety should be compared with other second-line therapies such as bevacizumab, cetuximab, and regorfenib. Medical institutions in Hong Kong, Macao, and Taiwan regions of China should be cautious when using or introducing aflibercept plus FOLFIRI as mCRC treatment.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
PG and YB: conceptualization. PG, NW, XH, and X-NW: investigation. PG: project administration. YB: supervision. PG, NW, XH, X-PW, and X-YL: original draft. NW, XH, J-ZZ, X-PW, and YB: writing—review and editing. All authors have read and agreed to the published version of the manuscript. All authors read and approved the final manuscript.
This study was supported by the research funds provided to Ying Bian from the University of Macau (project no. MYRG 2019-00044-ICMS and project no. QRCM-IRG2022-001).
The author would like to thank all the teachers and students who put forward suggestions on methods and article revision. In addition, we thank Yu-yao Niu from University of Macau for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.914683/full#supplementary-material
Aparicio, T., Canouï-Poitrine, F., and Caillet, P. (2020). Treatment guidelines of metastatic colorectal cancer in older patients from the French Society of Geriatric Oncology (SoFOG). Digestive and liver disease. official J. Italian Soc. Gastroenterology Italian Assoc. Study Liver 52 (5), 493–505. doi:10.1016/j.dld.2019.12.145
Benson, A. B., Venook, A. P., Al-Hawary, M. M., Arain, M. A., Chen, Y. J., Ciombor, K. K., et al. (2021). Colon cancer, version 2.2021, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 19 (3), 329–359. doi:10.6004/jnccn.2021.0012
Broman, K., Bailey, C. E., and ParikH, A. A. (2019). . Sidedness of colorectal cancer impacts risk of second primary gastrointestinal malignancy. Ann. Surg. Oncol. 26 (7), 2037–2043. doi:10.1245/s10434-019-07326-7
Chen, Y., He, Y., Chi, X., Wei, Y., and Shi, L. (2018). Development of health technology assessment in China: New challenges. Biosci. Trends 12 (2), 102–108. doi:10.5582/bst.2018.01038
FDA approves aflibercept (2012). FDA approves aflibercept (Zaltrap) for metastatic colorectal cancer. Oncol. Willist. Park 26 (9), 842–873.
Gill, S., Dowden, S., Colwell, B., Collins, L. L., and Berry, S. (2014). Navigating later lines of treatment for advanced colorectal cancer - optimizing targeted biological therapies to improve outcomes. Cancer Treat. Rev. 40 (10), 1171–1181. doi:10.1016/j.ctrv.2014.10.002
Glynne-Jones, R., Wyrwicz, L., Tiret, E., Brown, G., Rödel, C., Cervantes, A., et al. (2017). Rectal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 28 (4), iv22–iv40. doi:10.1093/annonc/mdx224
Hailey, D., and Topfer, L. A. (2003). Toward transparency in health technology assessment: A checklist for HTA reports. Int. J. Technol. Assess. Health Care 19 (1), 1–7. doi:10.1017/s0266462303000011
Halama, N., and Haberkorn, U. (2020). The unmet needs of the diagnosis, staging, and treatment of gastrointestinal tumors. Semin. Nucl. Med. 50 (5), 389–398. doi:10.1053/j.semnuclmed.2020.06.003
Hashiguchi, Y., Muro, K., Saito, Y., Ajioka, Y., and Hamaguchi, T. (2020). Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 25 (1), 1–42. doi:10.1007/s10147-019-01485-z
Holash, J., Davis, S., Papadopoulos, N., Croll, S. D., Ho, L., Russell, M., et al. (2002). VEGF-trap: A VEGF blocker with potent antitumor effects. Proc. Natl. Acad. Sci. U. S. A. 99 (17), 11393–11398. doi:10.1073/pnas.172398299
Husereau, D., Drummond, M., Petrou, S., Carswell, C., Moher, D., Greenberg, D., et al. (2013). Consolidated health economic evaluation reporting standards (CHEERS)-explanation and elaboration: A report of the ISPOR health economic evaluation publication guidelines good reporting practices task force. Value Health. 16 (2), 231–250. doi:10.1016/j.jval.2013.02.002
Kanukula, R., Ganta, S., Sirumalla, Y., Salam, A., Baddam, R., and Pasupuleti, B. C. (2019). Risk of venous thromboembolic events in patients with cancer treated with aflibercept: A systematic review and meta-analysis of randomized controlled trials. Am. J. Ther. 26 (4), e549–e552. doi:10.1097/MJT.0000000000000805
Kashiwa, M., and Matsushita, R. (2020). Comparative cost-effectiveness of aflibercept and ramucirumab in combination with irinotecan and fluorouracil-based therapy for the second-line treatment of metastatic colorectal cancer in Japan. Clin. Ther. 42 (7), 1361–1375. doi:10.1016/j.clinthera.2020.05.013
Kirstein, M. M., Lange, A., Prenzler, A., Manns, M. P., Kubicka, S., and Vogel, A. (2014). Targeted therapies in metastatic colorectal cancer: A systematic review and assessment of currently available data. Oncologist 19 (11), 1156–1168. doi:10.1634/theoncologist.2014-0032
Li, J., Xu, R., Qin, S., Liu, T., and Pan, H. (2018). Aflibercept plus FOLFIRI in asian patients with pretreated metastatic colorectal cancer: A randomized phase III study. Future Oncol. 14 (20), 2031–2044. doi:10.2217/fon-2017-0669
Modest, D. P., Pant, S., and Sartore-Bianchi, A. (2019). Treatment sequencing in metastatic colorectal cancer. Eur. J. Cancer 109, 70–83. doi:10.1016/j.ejca.2018.12.019
Peng, L., Bu, Z., Zhou, Y., Ye, X., Liu, J., and Zhao, Q. (2014). Hemorrhagic events in cancer patients treated with aflibercept: A meta-analysis. Tumour Biol. 35 (9), 9419–9427. doi:10.1007/s13277-014-2189-1
Peng, L., Zhao, Q., Ye, X., Zhou, Y., Hu, D., and Zheng, S. (2014). Incidence and risk of proteinuria with aflibercept in cancer patients: A meta-analysis. PLoS One 9 (11), e111839. doi:10.1371/journal.pone.0111839
Pharnexcloud (2021). Pharnexcloud. Availableat: https://www.pharnexcloud.com/database/7/table/59?q=aflibercept.
Qi, W. X., Shen, F., Qing, Z., and Xiao-Mao, G. (2014). Risk of gastrointestinal perforation in cancer patients treated with aflibercept: A systematic review and meta-analysis. Tumour Biol. 35 (11), 10715–10722. doi:10.1007/s13277-014-2369-z
Qi, W. X., Shen, Z., Tang, L. N., and Yao, Y. (2014). Risk of hypertension in cancer patients treated with aflibercept: A systematic review and meta-analysis. Clin. Drug Investig. 34 (4), 231–240. doi:10.1007/s40261-014-0174-5
Qi, W. X., Tang, L. N., Shen, Z., and Yao, Y. (2014). Treatment-related mortality with aflibercept in cancer patients: A meta-analysis. Eur. J. Clin. Pharmacol. 70 (4), 461–467. doi:10.1007/s00228-013-1633-2
Rothschedl, E., Anna, N., Breuer, J., Borner, M., Onkologie, C., and Spitalzentrum, B. (2013). Aflibercept (Zaltrap®) in addition to FOLFIRI for the 2nd line therapy of metastatic colorectal cancer. Vienna, Austria: Institute for Health Technology Assessment, Ludwig Boltzmann Gesellschaft.
Saif, M. W. (2013). Anti-VEGF agents in metastatic colorectal cancer (mCRC): Are they all alike? Cancer Manag. Res. 5, 103–115. doi:10.2147/cmar.S45193
Shea, B. J., Reeves, B. C., Wells, G., Thuku, M., Hamel, C., Moran, J., et al. (2017). Amstar 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 358, j4008. doi:10.1136/bmj.j4008
SSM (2021). Drug information inquiry in Macao SAR. Availableat: https://www.ssm.gov.mo/dafweb/dafweb.htm.
Sung, H., Ferlay, J., Siegel, R. L., Laversanne, M., Soerjomataram, I., Jemal, A., et al. (2021). Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca. Cancer J. Clin. 71 (3), 209–249. doi:10.3322/caac.21660
Tang, P. A., Cohen, S. J., Kollmannsberger, C., Bjarnason, G., Virik, K., MacKenzie, M. J., et al. (2012). Phase II clinical and pharmacokinetic study of aflibercept in patients with previously treated metastatic colorectal cancer. Clin. Cancer Res. 18 (21), 6023–6031. doi:10.1158/1078-0432.CCR-11-3252
Van Cutsem, E., Tabernero, J., Lakomy, R., Prenen, H., Prausova, J., Macarulla, T., et al. (2012). Addition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimen. J. Clin. Oncol. 30 (28), 3499–3506. doi:10.1200/jco.2012.42.8201
Wade, R., Duarte, A., Simmonds, M., Rodriguez-Lopez, R., Duffy, S., Spackman, E., et al. (2013). Aflibercept in combination with irinotecan and fluorouracil-based therapy for the treatment of metastatic colorectal cancer which has progressed following prior oxaliplatin-based chemotherapy: A single technology appraisal. York, England: CRD and CHE Technology Assessment Group.
Wade, R., Duarte, A., Simmonds, M., Rodriguez-Lopez, R., Duffy, S., Woolacott, N., et al. (2015). The clinical and cost effectiveness of aflibercept in combination with irinotecan and fluorouracil-based therapy (FOLFIRI) for the treatment of metastatic colorectal cancer which has progressed following prior oxaliplatin-based chemotherapy: A critique of the evidence. Pharmacoeconomics 33 (5), 457–466. doi:10.1007/s40273-015-0257-z
Xie, X., Zhang, J., Hu, H., Cai, Y., Wu, Z., Ling, J., et al. (2020). Efficacy and safety of regorafenib in combination with chemotherapy as second-line treatment in patients with metastatic colorectal cancer: A network meta-analysis and systematic literature review. Adv. Ther. 37 (10), 4233–4248. doi:10.1007/s12325-020-01447-2
Xu, Z., Peng, X., Kong, Y., Cui, Y., Li, Y., and Guo, Y. (2021). The best strategy for metastatic colorectal cancer (mCRC) patients in second-line treatment: A network meta-analysis. Cancer Treat. Res. Commun. 29, 100455. doi:10.1016/j.ctarc.2021.100455
Yaeger, R., Cowell, E., Chou, J. F., Gewirtz, A. N., Borsu, L., Vakiani, E., et al. (2015). RAS mutations affect pattern of metastatic spread and increase propensity for brain metastasis in colorectal cancer. Cancer 121 (8), 1195–1203. doi:10.1002/cncr.29196
Yaozhi Data (2014). Yaozhi data. Availableat: https://db.yaozh.com/hk/17347.html.
You, Y. N., Hardiman, K. M., Bafford, A., Poylin, V., Francone, T. D., Davis, K., et al. (2020). The American society of colon and rectal surgeons clinical practice guidelines for the management of rectal cancer. Dis. Colon Rectum 63 (9), 1191–1222. doi:10.1097/DCR.0000000000001762
Zhang, X., Ran, Y., Shao, Y., Wang, K., and Zhu, Y. (2016). Incidence and risk of severe infections associated with aflibercept in cancer patients: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 81 (1), 33–40. doi:10.1111/bcp.12758
Keywords: metastatic colorectal cancer, aflibercept, rapid health technology assessment, targeted drugs, cost-effectiveness analysis, pharmacoeconomics
Citation: Ge P, Wan N, Han X, Wang X, Zhang J, Long X, Wang X and Bian Y (2022) Efficacy, safety, and cost-effectiveness analysis of aflibercept in metastatic colorectal cancer: A rapid health technology assessment. Front. Pharmacol. 13:914683. doi: 10.3389/fphar.2022.914683
Received: 07 April 2022; Accepted: 25 July 2022;
Published: 30 August 2022.
Edited by:
Yuhan Bao, Changzhou Institute of Technology, ChinaReviewed by:
Peng Men, Peking University Third Hospital, ChinaCopyright © 2022 Ge, Wan, Han, Wang, Zhang, Long, Wang and Bian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying Bian, Ymlhbnlpbmd1bUAxNjMuY29t
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.