 Fang Li1,2†
Fang Li1,2† Luming Zhang
Luming Zhang Jun Lyu
Jun Lyu Haiyan Yin
Haiyan Yin
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 05 May 2022
Sec. Respiratory Pharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.898422
This article is part of the Research Topic Drug Prevention and Control of Ventilator-Associated Pneumonia Volume II View all 12 articles
Objective: This study analyzed the association of gastric acid secretion inhibitors (GASIs) [including proton pump inhibitors (PPIs) and histamine 2 receptor antagonists (H2RAs)] with the occurrence of ventilator-associated pneumonia (VAP) and in-hospital mortality in patients who received invasive mechanical ventilation (IMV).
Method: Patients who received IMV and used GASI were included based on records in the MIMIC-IV database. The relationships of GASIs with VAP and the in-hospital mortality were determined using univariate and multivariate logistic regression analyses. Also, the effects of GASIs in some subgroups of the population were further analyzed.
Results: A total of 18,669 patients were enrolled, including 9191 patients on H2RAs only, 6921 patients on PPIs only, and 2557 were on a combination of the two drugs. Applying logistic regression to the univariate and multivariate models revealed that compared with H2RAs, PPIs had no significant effect on the incidence of VAP, and the combination of H2RAs and PPIs was a risk factor for VAP. Compared with H2RAs, univariate logistic regression revealed that, PPIs and combine the two drugs were both risk factors for in-hospital mortality, but multivariate logistic regression showed that they were not significantly associated with in-hospital mortality. In subgroup analysis, there were interaction in different subgroups of age, PCO2, myocardial infarct, congestive heart failure (P for interaction<0.05).
Conclusion: Compared with H2RAs, PPIs did not have a significant association with either VAP or in-hospital mortality; the combination of H2RAs and PPIs was risk factor for VAP, but did not have a significantly associated with in-hospital mortality.
Invasive mechanical ventilation (IMV) is commonly used in critically ill patients in intensive care units (ICUs) to maintain airway patency, prevent aspiration, and improve oxygenation. A critical complication is ventilator-associated pneumonia (VAP). Patients who received IMV had pulmonary infections mostly caused by pathogens present in the hospital environment (Timsit et al., 1000). A meta-analysis estimated that the incidence density of VAP/1000 ventilator days was 15.1%, with higher incidence rates in low-income countries (Bonell et al., 2019). VAP increases hospital stays, mortality, and treatment costs (Koenig and Truwit, 2006; Fadda and Ahmad, 2022).
Patients with IMV are often associated with stress ulcer risk, and preventive application of gastric acid secretion inhibitors (GASIs) can significantly reduce gastrointestinal bleeding (Zhou et al., 2019). The most commonly used drugs are proton pump inhibitors (PPIs) and histamine 2 receptor antagonists (H2RAs). H2RAs were thought to inhibit gastric acid secretion by blocking histamine receptors, PPIs work by inhibiting the final stages of gastric acid production (Toews et al., 2018). On the one hand, these drugs can improve the pH gastric juice and allow excessive bacterial growth (Buendgens et al., 2016); on the other hand, they can reduce reflux, and prevent bacteria movement to the pharynx and lungs. The purpose of this study was to determine the effects of two different GASIs on VAP incidence and in-hospital mortality among patients with IMV.
The Beth Israel Deaconess Medical Center (BIDMC), Massachusetts General Hospital, and the Massachusetts Institute of Technology jointly developed the Medical Information Mart for Intensive Care (MIMIC) in 2003. The project was funded by the National Institutes of Health (Yang et al., 2020). The MIMIC-IV database provides information on more than 70,000 patients admitted to the ICU of BIDMC from 2008 to 2019, and it is freely available to researchers. All patients were re-identification under the Safe harbor provisions of and Health Insurance Portability and Accountability Act, thereby waiving the need to obtain informed consent (Wu et al., 2021).
Patients were searched for in the MIMIC-IV database. The inclusion criteria identified 25,031 patients who used IMV. The exclusion criteria were 1) not the first ICU admission (2,495 patients), 2) ICU stay of less than 24 h (1379 patients), 3) >5% missing data (141 patients), and 4) not used PPIs or H2RAs (2444 patients).
Baseline characteristics during ICU admission were obtained using Structured Query Language, and if there were multiple values, the worst values for that period were recorded. Information was collected on demographic characteristics (year of admission, sex, body weight, and age), disease severity [Acute Physiology Score III (APSIII), Sequential Organ Failure Assessment scores (SOFA), laboratory examination results white blood cells (WBC), hemoglobin (HB), platelets (PLT)], [partial pressure of carbon dioxide (PCO2), partial pressure of oxygen (PO2), lactate, anion gap, blood urea nitrogen (BUN), blood sugar (GLU), international normalized ratio (INR), and total bilirubin (TBIL)], commodities (myocardial infarction, congestive heart failure, peptic ulcer disease, diabetes, cerebrovascular disease, renal disease, liver disease, and sepsis), treatment regimens [renal replacement therapy (RRT) vasopressors use, PPIs, H2RAs, and IMV duration], hospital length of stay (LOS), and ICU LOS. PPIs included esomeprazole, lansoprazole, omeprazole, and pantoprazole; and H2RAs included famotidine, ranitidine, and cimetidine.
End points were a VAP diagnosis and all-cause in-hospital mortality. According to the standard VAP diagnostic criteria of the Centers for Disease Control and Prevention, the specific diagnostic criteria used in this study are listed in Table 1 (American Thoracic Society and Infectious Diseases Society of America, 2005; Klompas et al., 2012).
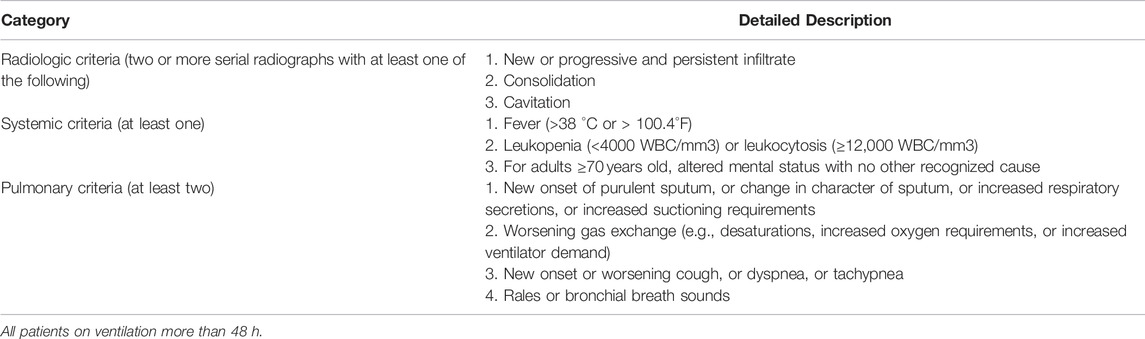
TABLE 1. Centers for Disease Control and Prevention’s clinical surveillance definition for VAP.
Data were collated and outliers were deleted. If a variable had >20% missing data, it was discarded; otherwise, the 10-degree interpolation method was applied. Categorical data were expressed as frequencies or percentages. Continuous variables were expressed as medians and interquartile ranges. Chi-square and Kruskal–Wallis H tests were used to identify significant differences between the groups.
Logistic regression was used to analyze the relationships of PPIs, H2RAs, and the combination of PPIs and H2RAs with VAP and in-hospital mortality. These results were expressed as odds ratios (ORs) and 95% confidence intervals (CIs). The logistic regression presupposes a linear relationship between the continuous independent variables and logit(P), so we first performed the boxTidwell test (Brescia et al., 2021).p values for the variables age, weight, PLT, AG, INR, and TBIL were all greater than 0.05 (Supplementary Table S1) consistent with a linear relationship with logit(P), and the remaining continuous variables were converted to categorical variables based on clinical significance or inter-quartile spacing. Univariate and multivariate models were established for each end point. In the multivariate model, we adjusted for patients’ general information age, sex, weight; disease severity score APSIII, SOFA score; routine hematological tests WBC, HB, PLT; patients’ liver and kidney functions: BUN, TBIL, INR; indicators reflecting patients’ internal environment PO2, PCO2, anion gap, GLU, lactate and patients’ major comorbidities myocardial infarction, congestive heart failure, cerebrovascular disease, peptic ulcer disease, liver disease, diabetes, renal disease, sepsis were adjusted. In addition, whether patients were on RRT after ICU admission, vasopressors use, and IMV duration were also used for adjustment. The variance inflation factor showed no multicollinearity between these variables (Supplementary Table S2).
The relationships of PPIs, H2RAs, and the combination of PPIs and H2RAs with VAP were assessed using subgroup analyses. The subgroups were classified according to age, sex, APSIII, SOFA score, PO2, PCO2, HB, WBC, PLT, anion gap, BUN, INR, body weight, GLU, TBIL, lactate, myocardial infarct, congestive heart failure, cerebrovascular disease, peptic ulcer disease, liver disease, diabetes, renal disease, sepsis, RRT, vasopressors use, and IMV duration.
R software (http://www.R-project.org) and SPSS software (version 27.0, IBM, United States) were used for all statistical analyses. All probability values were bilateral, and p < 0.05 was considered indicative of statistical significance.
This study enrolled 18,669 ICU patients with IMV and GASIs (see flowchart in Figure 1). There were 9191 patients in the H2RAs group, 6,921 patients in the PPIs group, 2,557 patients in the combination of PPIs and H2RAs group. H2RAs group were more male (p < 0.05). PPIs group were older (p < 0.05). The combination of PPIs and H2RAs group had higher APSIII, SOFA scores; more vasopressors and RRT use; longer IMV duration, hospital LOS and ICU LOS (p < 0.05). In comorbidity, patients in the three groups were most complicated with sepsis (67.7%, 76.2% and 84.8%, respectively).More detailed characteristics of the remaining participants stratified by different GASIs can be seen in Table 2.
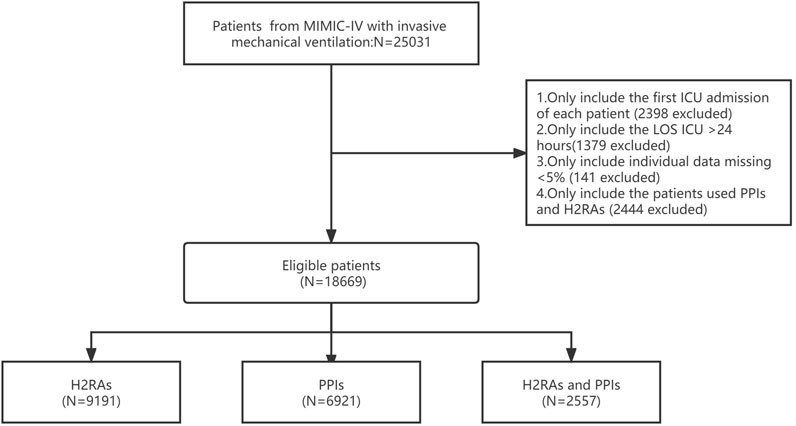
FIGURE 1. Illustration of exclusion and inclusion criteria.
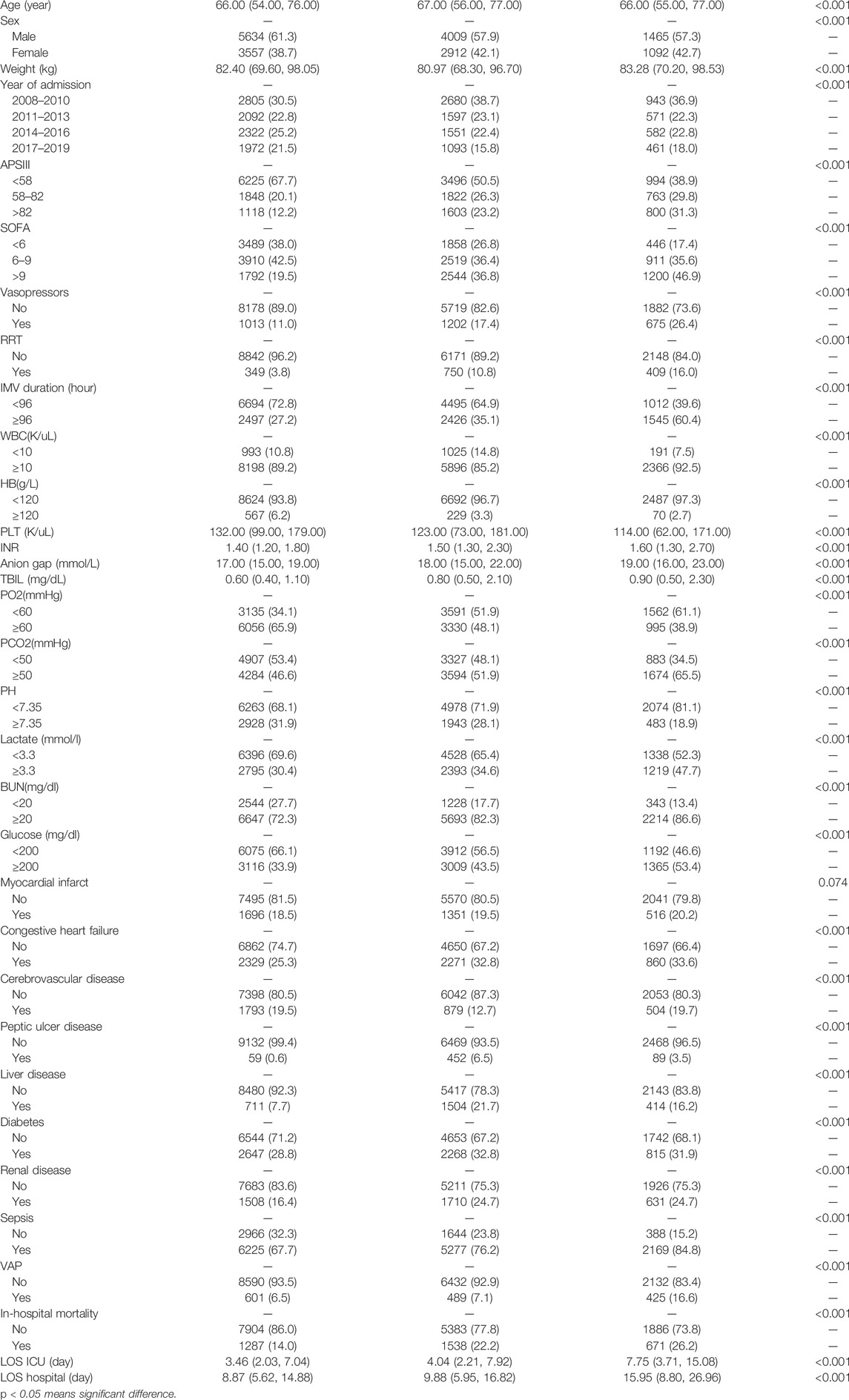
TABLE 2. Characteristics of patients with GASIs.
The distribution of GASIs in different years was shown in Figure 2. The proportion of H2RAs increased year by year, and the comparison among all groups was significant, and the highest in 2017–2019 group (55.93%) (p < 0.05). The proportion of PPIs decreased year by year, except that there was no statistical difference between 2011–2013 group and 2014–2016 group (p > 0.05), other groups had statistical differences, the lowest in 2017–2019 group (31.00%) (p < 0.05). There was no statistical difference in the combination of PPIs and H2RAs among all groups (p > 0.05).
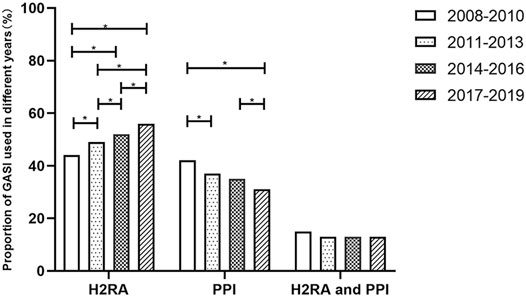
FIGURE 2. Comparison of distribution proportion between GASIs in different years.
Applying logistic regression revealed that compared with H2RAs group, the combination of PPIs and H2RAs group was a risk factor for VAP in the univariate and multivariate models (p < 0.05), whereas PPIs group was not significantly associated with VAP (p > 0.05). Compared with H2RAs, univariate logistic regression revealed that, PPIs and the combination of H2RAs and PPIs were both risk factors for in-hospital mortality, but multivariate logistic regression revealed that PPIs and the combination of H2RAs and PPIs were not significantly associated with in-hospital mortality (p > 0.05) (Table 3).
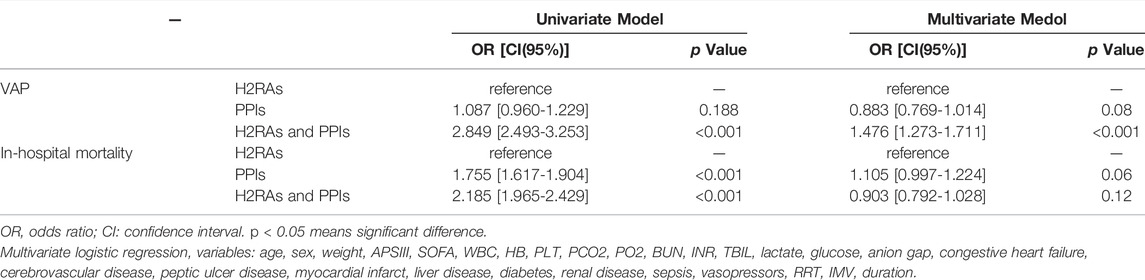
TABLE 3. Logistic regression analysis of GASIs to VAP and in hospital mortality for both models.
Subgroup analyses were performed on various covariate, most of which presented no obvious interaction (Table 4, p > 0.05). There were interactions in different subgroups of age, PCO2, myocardial infarct, congestive heart failure (P for interaction<0.05). PPIs was a protect factor for VAP in the subgroup of age <65 years, APSIII <58, PCO2<50 mmHg, IMV duration≥96 h, without used vasopressors, without myocardial infarct, without congestive heart failure, without liver disease, without diabetes, without renal disease. (p < 0.05).
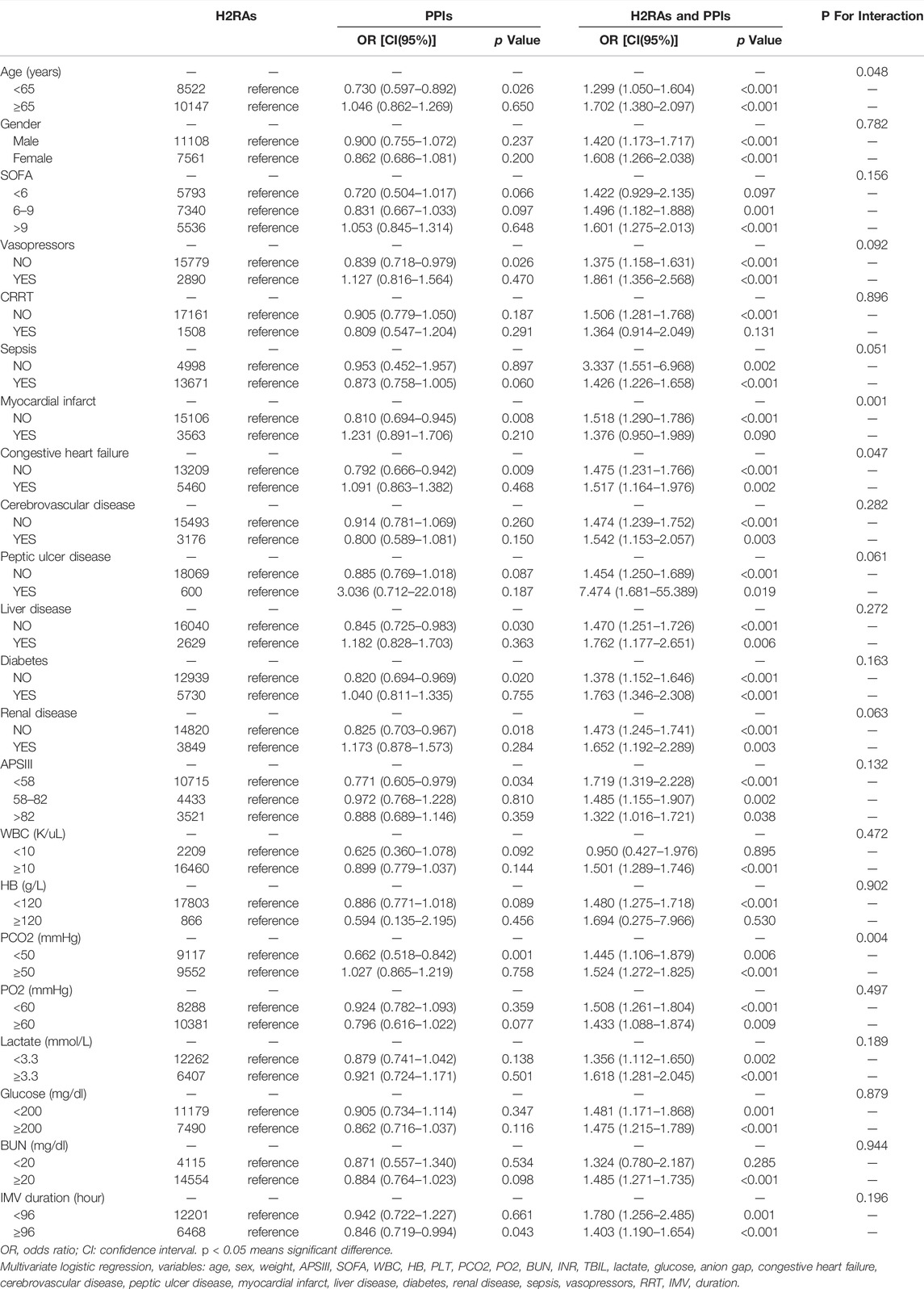
TABLE 4. Subgroup analysis of the associations between GASIs and VAP.
The patients who received IMV in the ICU had severe diseases that were often accompanied by stress ulcers, resulting in inadequate nutritional supplies, and further digestive tract hemorrhage, gastrointestinal perforation, and life-threatening conditions in serious cases. Stress ulcer treatment guidelines for gastrointestinal bleeding prevention in critically ill patients recommend using PPIs (or H2RAs as a reasonable alternative), but sucralfate is not recommended (Ye et al., 2020). Previous research has linked stress ulcer medication use to an increased VAP risk. Our current study showed that 18,669 patients had received GASIs while on IMV therapy, and 1,515 (8.12%) of them developed VAP, which is a relatively high rate. Moreover, we found that the utilization rate of H2RAs increased year by year compared with PPIs, and the proportion of patients using only H2RAs reached 55.93% from 2017 to 2019. To investigate the prognostic impact of specific GASIs, this study investigated the effect of PPI, H2RAs and their combination on VAP and in-hospital mortality. The results showed that compared to H2RAs, PPIs was found no significant effect on VAP or in-hospital mortality, but their combination was risk factors for VAP whereas no significant effect on in-hospital mortality.
Aspiration is an important factor in hospital acquired pneumonia (HAP) and VAP pathogenesis. By inhibiting acid production, PPIs and H2RAs increase nosocomial pathogen colonization in the oropharynx and trachea, while delaying gastric emptying, greatly increasing the risk of infection from aspiration (Tablan et al., 2004). The flora analysis of VAP also supported this, and the pathogenic bacteria of patients who received PPIs and H2RAs were mostly pseudomonas, Gram-negative bacteria, and methicillin-resistant Staphylococcus aureus, which may be caused by gastric alkalinization (Grindlinger et al., 2016). In critically ill patients, there was no difference in pneumonia incidence between H2RAs and PPIs, but PPIs significantly reduced GIB incidence (Deliwala et al., 2021), and H2RAs had a lower cost and higher survival rate (MacLaren and Campbell, 2014). Both of them have advantages and disadvantages. However, some studies have suggested the presence of a difference in VAP incidence between the two GASIs. Miano et al. reported that pantoprazole was associated with a higher HAP incidence than was ranitidine (Miano et al., 2009). A meta-analysis also found that PPIs are more effective than H2RAs, but may also increase the risk of VAP (Alquraini et al., 2017). Zhou et al. believed that for high-risk critically ill patients, PPIs and H2RAs can significantly reduce gastrointestinal bleeding, with both potentially increasing the pneumonia incidence (Zhou et al., 2019). Other studies had shown that there was no difference in the effect of PPI on VAP compared with H2RAs, but PPI had a better anti-gastrointestinal bleeding effect (Arriola et al., 2016). Some studies had pointed out that PPIs and H2RAs had no effect on the risk of death or extubation in critically ill patients (Li et al., 2020). The effect of PPIs and H2RAs on VAP, the results of previous studies were inconsistent.
In this study, PPIs compared with H2RAs had no difference in VAP and in hospital mortality. The combination of PPIs and H2RAs would lead to a higher incidence of VAP, but did not have a beneficial effect on in hospital mortality, which reminds us not to use the two drugs to inhibit gastric acid secretion at the same time. We hypothesized that the combination of the two drugs meant that the dose was increased, the inhibition of gastric acid secretion was stronger, and the gastric alkalization was more serious. On the one hand, the incidence of VAP was increased, and on the other hand, the treatment effect of stress ulcer was better, thus having the impact on mortality. Further confirmation is certainly needed.
This study found that PPIs compared with H2RAs was a protect factor for VAP in subgroup of age<65 years, APSIII <58, PCO2<50 mmHg, without used vasopressors, without myocardial infarct, without congestive heart failure, without liver disease, without diabetes, without renal disease. The effect of PPIs on VAP was more beneficial in mild, young patients without chronic heart, renal and liver disease. Therefore, we still suggest that more consideration should be given to the use of PPIs after the evaluation of patients with IMV, and PPIs was also the preferred drug for stress ulcer in the guidelines. Studies have shown that compared with the using H2RAs, PPIs prophylaxis was the most effective preventive strategy in patients at high risk of developing stress ulcer bleeding (Barkun et al., 2013). However, in recent years, the proportion of H2RAs had increased rapidly, and the reasons affecting doctors’ decision-making need to be further discussed.
In clinical practice, it is necessary to measure VAP incidence and the efficiency of stress ulcer prevention and treatment, and select appropriate drugs according to the situation of each patient. In this study, the combination of PPIs and H2RAs is not recommended, which increases the risk of VAP. In patients with less severe disease, younger and with fewer comorbidities, PPIs was associated with a lower incidence of VAP compared to H2RAs. However, no matter how GASIs was selected, it had no significant impact on in hospital mortality.
This study analyzed a big-data sample spanning 12 years, but there were some limitations. First, it uses a retrospective single-center design, which has some uncontrolled confounding bias. Second, there was no comparison of the effects of the drugs on gastrointestinal bleeding to determine their therapeutic effects. Third, logistic regression presupposes a linear relationship between continuous independent variables and logit(P), but in some machine learning methods such as ensemble modeling, non-linearity can be handled automatically without prior specification, and the application of this method can be tried in future research (Zhang et al., 2022). Finally, due to some limitations in the database, the total dose and duration of the drug could not be accurately calculated in this study, and these factors could be taken into account in the design of future studies.
Compared with H2RAs, PPIs did not have a significant association with either VAP or in-hospital mortality; the combination of H2RAs and PPIs was risk factor for VAP, but did not have a significantly associated with in-hospital mortality.
APSIII, Acute physiology score III; BUN, Blood Urea Nitrogen; GASIs, Gastric acid secretion inhibitors; H2RAs, Histamine 2 receptor antagonist; INR, international normalized ratio; IMV, Invasive mechanical ventilation; PPIs: Proton pump inhibitors; PO2, Partial pressure of blood oxygen; PCO2, Partial Pressure of Carbon Dioxide; RRT, Renal replacement therapy; SOFA, Sequential organ failure assessment; VAP, ventilator-associated pneumonia; WBC, White Blood Cell.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: The data were available on the MIMIC-IV website at https://mimic-iv.mit.edu.
FL, HL and LZ contributed equally to this work. FL extracted the data from the MIMIC-IV database. HL and LZ participated in data analysis and interpretation. FL and LZ wrote the first draft of the paper. XH and YL planned the analyses, and BL and CX guided the literature review. HY and JL conceptualized the research aims. All author approves the final manuscript.
This work was supported by The National Social Science Foundation of China (grant/award no. 16BGL183), The National Natural Science Foundation of China (No. 82072232; 81871585), The Natural Science Foundation of Guangdong Province (No. 2018A030313058), Technology and Innovation Commission of Guangzhou Science, China (No.201804010308).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the Massachusetts Institute of Technology, the Beth Israel Deaconess Medical Center for the MIMIC project, and Guangdong Provincial Key Laboratory of Traditional Chinese Medicine Informatization (2021B1212040007), Guangzhou, Guangdong, China.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.898422/full#supplementary-material
Alquraini, M., Alshamsi, F., Møller, M. H., Belley-Cote, E., Almenawer, S., Jaeschke, R., et al. (2017). Sucralfate versus Histamine 2 Receptor Antagonists for Stress Ulcer Prophylaxis in Adult Critically Ill Patients: A Meta-Analysis and Trial Sequential Analysis of Randomized Trials. J. Crit. Care 40, 21–30. doi:10.1016/j.jcrc.2017.03.005
American Thoracic SocietyInfectious Diseases Society of America (2005). Guidelines for the Management of Adults with Hospital-Acquired, Ventilator-Associated, and Healthcare-Associated Pneumonia. Am. J. Respir. Crit. Care Med. 171(4): p. 388–416.doi:10.1164/rccm.200405-644ST
Arriola, V., Tischendorf, J., Musuuza, J., Barker, A., Rozelle, J. W., and Safdar, N. (2016). Assessing the Risk of Hospital-Acquired Clostridium Difficile Infection with Proton Pump Inhibitor Use: A Meta-Analysis. Infect. Control Hosp. Epidemiol. 37 (12), 1408–1417. doi:10.1017/ice.2016.194
Barkun, A. N., Adam, V., Martel, M., and Bardou, M. (2013). Cost-effectiveness Analysis: Stress Ulcer Bleeding Prophylaxis with Proton Pump Inhibitors, H2 Receptor Antagonists. Value Health 16 (1), 14–22. doi:10.1016/j.jval.2012.08.2213
Bonell, A., Azarrafiy, R., Huong, V. T. L., Viet, T. L., Phu, V. D., Dat, V. Q., et al. (2019). A Systematic Review and Meta-Analysis of Ventilator-Associated Pneumonia in Adults in Asia: An Analysis of National Income Level on Incidence and Etiology. Clin. Infect. Dis. 68 (3), 511–518. doi:10.1093/cid/ciy543
Brescia, A. V., Bensi, C., Di Gennaro, G., Monda, M., and Docimo, R. (2021). Impact of Lockdown on Children's Lifestyle and Their Collaboration during Dental Sessions. Eur. J. Paediatr. Dent. 22 (1), 61–65. doi:10.23804/ejpd.2021.22.01.11
Buendgens, L., Koch, A., and Tacke, F. (2016). Prevention of Stress-Related Ulcer Bleeding at the Intensive Care Unit: Risks and Benefits of Stress Ulcer Prophylaxis. World J. Crit. Care Med. 5 (1), 57–64. doi:10.5492/wjccm.v5.i1.57
Deliwala, S. S., Hamid, K, Goyal, H, Ponnapalli, A, Zayed, Y, Bala, A, et al. (2021). Proton Pump Inhibitors versus Histamine-2-Receptor Antagonists for Stress Ulcer Prophylaxis in Critically Ill Patients: A Meta-Analysis and Trial Sequential Analysis. J. Clin. Gastroenterol. 56 (3), 204–217. doi:10.1097/MCG.0000000000001562
Fadda, R. A., and Ahmad, M. (2022). Investigating Patient Outcomes and Healthcare Costs Associated with Ventilator-Associated Pneumonia. Nurs. Manag. (Harrow) 29 (1), 32–40. doi:10.7748/nm.2021.e1986
Grindlinger, G. A., Cairo, S. B., and Duperre, C. B. (2016). Pneumonia Prevention in Intubated Patients Given Sucralfate versus Proton-Pump Inhibitors And/or Histamine II Receptor Blockers. J. Surg. Res. 206 (2), 398–404. doi:10.1016/j.jss.2016.08.028
Klompas, M., Magill, S., Robicsek, A., Strymish, J. M., Kleinman, K., Evans, R. S., et al. (2012). Objective Surveillance Definitions for Ventilator-Associated Pneumonia. Crit. Care Med. 40 (12), 3154–3161. doi:10.1097/CCM.0b013e318260c6d9
Koenig, S. M., and Truwit, J. D. (2006). Ventilator-associated Pneumonia: Diagnosis, Treatment, and Prevention. Clin. Microbiol. Rev. 19 (4), 637–657. doi:10.1128/CMR.00051-05
Li, X., Klompas, M., Menchaca, J. T., and Young, J. G. (2020). Effects of Daily Treatment with Acid Suppressants for Stress Ulcer Prophylaxis on Risk of Ventilator-Associated Events. Infect. Control Hosp. Epidemiol. 41 (2), 187–193. doi:10.1017/ice.2019.323
MacLaren, R., and Campbell, J. (2014). Cost-effectiveness of Histamine Receptor-2 Antagonist versus Proton Pump Inhibitor for Stress Ulcer Prophylaxis in Critically Ill Patients*. Crit. Care Med. 42 (4), 809–815. doi:10.1097/CCM.0000000000000032
Miano, T. A., Reichert, M. G., Houle, T. T., MacGregor, D. A., Kincaid, E. H., and Bowton, D. L. (2009). Nosocomial Pneumonia Risk and Stress Ulcer Prophylaxis: a Comparison of Pantoprazole vs Ranitidine in Cardiothoracic Surgery Patients. Chest 136 (2), 440–447. doi:10.1378/chest.08-1634
Tablan, O. C., Anderson, L. J., Besser, R., Bridges, C., and Hajjeh, R. (2004). Guidelines for Preventing Health-Care-Aassociated Pneumonia, 2003: Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR Recomm. Rep. 53 (RR-3), 1–36.
Timsit, J. F., Esaied, W., Neuville, M., Bouadma, L., and Mourvllier, B. (10002017). Update on Ventilator-Associated Pneumonia. F1000Res 6, 2061. doi:10.12688/f1000research.12222.1
Toews, I., George, A. T., Peter, J. V., Kirubakaran, R., Fontes, L. E. S., Ezekiel, J. P. B., et al. (2018). Interventions for Preventing Upper Gastrointestinal Bleeding in People Admitted to Intensive Care Units. Cochrane Database Syst. Rev. 6, CD008687. doi:10.1002/14651858.CD008687.pub2
Wu, W. T., Li, Y. J., Feng, A. Z., Li, L., Huang, T., Xu, A. D., et al. (2021). Data Mining in Clinical Big Data: the Frequently Used Databases, Steps, and Methodological Models. Mil. Med. Res. 8 (1), 44. doi:10.1186/s40779-021-00338-z
Yang, J., Li, Y., Liu, Q., Li, L., Feng, A., Wang, T., et al. (2020). Brief Introduction of Medical Database and Data Mining Technology in Big Data Era. J. Evid. Based Med. 13 (1), 57–69. doi:10.1111/jebm.12373
Ye, Z., Reintam Blaser, A., Lytvyn, L., Wang, Y., Guyatt, G. H., Mikita, J. S., et al. (2020). Gastrointestinal Bleeding Prophylaxis for Critically Ill Patients: a Clinical Practice Guideline. BMJ 368, l6722. doi:10.1136/bmj.l6722
Zhang, Z., Chen, L., Xu, P., and Hong, Y. (2022). Predictive Analytics with Ensemble Modeling in Laparoscopic Surgery: A Technical Note. Laparosc. Endosc. Robotic Surg. 5 (1), 25–34. doi:10.1016/j.lers.2021.12.003
Zhou, X., Fang, H., Xu, J., Chen, P., Hu, X., Chen, B., et al. (2019). Stress Ulcer Prophylaxis with Proton Pump Inhibitors or Histamine 2 Receptor Antagonists in Critically Ill Adults - a Meta-Analysis of Randomized Controlled Trials with Trial Sequential Analysis. BMC Gastroenterol. 19 (1), 193. doi:10.1186/s12876-019-1105-y
Keywords: ventilator-associated pneumonia, mortality, proton pump inhibitor, histamine 2 receptor antagonist, gastric acid secretion inhibitors
Citation: Li F, Liu H, Zhang L, Huang X, Liu Y, Li B, Xu C, Lyu J and Yin H (2022) Effects of Gastric Acid Secretion Inhibitors for Ventilator-Associated Pneumonia. Front. Pharmacol. 13:898422. doi: 10.3389/fphar.2022.898422
Received: 17 March 2022; Accepted: 20 April 2022;
Published: 05 May 2022.
Edited by:
Zhi Mao, People’s Liberation Army General Hospital, ChinaReviewed by:
Yuli Huang, Shunde Hospital, Southern Medical University, ChinaCopyright © 2022 Li, Liu, Zhang, Huang, Liu, Li, Xu, Lyu and Yin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jun Lyu, bHl1anVuMjAyMEBqbnUuZWR1LmNu; Haiyan Yin, eWluaGFpeWFuMTg2N0AxMjYuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.