
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 04 July 2022
Sec. Pharmacology of Infectious Diseases
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.863587
 Miguel Cervero1*
Miguel Cervero1* Daniel López-Wolf2
Daniel López-Wolf2 Guiomar Casado3Maria Novella-Mena4Pablo Ryan-Murua5María Luisa Taboada-Martínez6
Guiomar Casado3Maria Novella-Mena4Pablo Ryan-Murua5María Luisa Taboada-Martínez6 Sara Rodríguez-Mora3
Sara Rodríguez-Mora3 Lorena Vigón3
Lorena Vigón3 Mayte Coiras3*
Mayte Coiras3* Montserrat Torres3* Multidisciplinary Group of Study of COVID-19 (MGS-COVID)
Montserrat Torres3* Multidisciplinary Group of Study of COVID-19 (MGS-COVID)There is now sufficient evidence to support that vitamin D deficiency may predispose to SARS-CoV-2 infection and increase COVID-19 severity and mortality. It has been suggested that vitamin D3 supplementation may be used prophylactically as an affordable and safe strategy that could be added to the existing COVID-19 standard treatment. This multicenter, single-blinded, prospective randomized pilot clinical trial aimed to evaluate the safety, tolerability, and effectiveness of 10,000 IU/day in comparison with 2000 IU/day of cholecalciferol supplementation for 14 days to reduce the duration and severity of COVID-19 in 85 hospitalized individuals. The median age of the participants was 65 years (Interquartile range (IQR): 53–74), most of them (71%) were men and the mean baseline of 25-hydroxyvitamin D (25(OH)D) in serum was 15 ng/ml (standard deviation (SD):6). After 14 days of supplementation, serum 25(OH)D levels were significantly increased in the group who received 10,000IU/day (p < 0.0001) (n = 44) in comparison with the 2,000IU/day group (n = 41), especially in overweight and obese participants, and the higher dose was well tolerated. A fraction of the individuals in our cohort (10/85) developed acute respiratory distress syndrome (ARDS). The median length of hospital stay in these patients with ARDS was significantly different in the participants assigned to the 10,000IU/day group (n = 4; 7 days; IQR: 4–13) and the 2,000IU/day group (n = 6; 27 days; IQR: 12–45) (p = 0.04). Moreover, the inspired oxygen fraction was reduced 7.6-fold in the high dose group (p = 0.049). In terms of blood parameters, we did not identify overall significant improvements, although the platelet count showed a modest but significant difference in those patients who were supplemented with the higher dose (p = 0.0492). In conclusion, the administration of 10,000IU/day of vitamin D3 for 14 days in association with the standard clinical care during hospitalization for COVID-19 was safe, tolerable, and beneficial, thereby helping to improve the prognosis during the recovery process.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is an enveloped positive-sense RNA betacoronavirus that appeared in Wuhan (China) in December 2019 and is the cause of coronavirus disease 2019 (COVID-19). COVID-19 has a variable clinical presentation from asymptomatic to milder symptoms or, far more seriously, as a severe and often deadly respiratory disease (Chen et al., 2020). The initial symptoms of COVID-19 mainly include fever, cough, myalgia, or fatigue and some patients develop gastrointestinal problems, such as diarrhoea and vomiting. In the later stages of the disease may occur dyspnea, hypoxia, confusion, or chest pain and gradually progress into complications such as acute respiratory distress syndrome (ARDS), which may result in lung injury, decreased oxygen saturation, and widespread tissue damage, thus, causing a multiple organ system failure, unfavourable prognosis, and even death (Hu et al., 2021, 2020).
The main cause of COVID-19 disease severity and death in patients is the extreme inflammatory response caused when the damaged cells trigger lung inflammation, largely mediated by proinflammatory macrophages and granulocytes, along with severe lymphopenia, neutrophil activation, thrombosis, and massive mononuclear cell infiltration in multiple organs (Merad and Martin, 2020). Accordingly, severe or fatal cases of COVID-19 disease are associated with elevated levels of interleukin-6 (IL-6), IL-7 and reduced levels of cytokines related to T-cell antiviral activity, such as IL-2, IL-12 or interferon (IFN)-γ (Vigón et al., 2021), as well as other laboratory abnormalities that include elevated levels of urea, creatinine, tissue markers (adipose tissue, kidney and muscle), ferritin, C-reactive protein (CRP), lower counts of lymphocytes (<1,000/µL), and platelets (<100 × 109/L), as well as reduced levels of albumin (Goyal et al., 2020; Malik et al., 2021).
For a long time, no evidence-based or clinically demonstrated strategy was shown for the treatment of COVID-19 (Mishra and Tripathi, 2021). Different drugs, designed for treating other diseases, have been used to limit the adverse effects of viral pathogenesis, such as antivirals (e.g., remdesivir), IL-6 inhibitors (e.g., tocilizumab), Janus kinase (JAK) inhibitors (e.g., baricitinib), or corticosteroids (e.g., dexamethasone, methylprednisolone). The excessive immune response and inflammation in severe COVID-19 patients have prompted many clinical studies to use a combination of different drugs (Esposito et al., 2020). As a consequence, FDA recently authorized the simultaneous administration of nirmatrelvir and ritonavir for the treatment of mild-to-moderate COVID-19 in children and adults, as well as oral molnupiravir for adults, but this authorization has only been issued in case of emergency for those individuals with high risk to progress to severe disease (Couzin-Frankel, 2021; Parums, 2022).
Risk factors such as older age, cardiovascular disease, diabetes mellitus, chronic respiratory disease, arterial hypertension, and cancer are associated with a higher probability to develop a severe form of COVID-19 (Huang et al., 2020; Jordan et al., 2020; Yang et al., 2020). In addition, there is now sufficient evidence to indicate that pre-existing conditions such as vitamin D deficiency may also predispose to SARS-CoV-2 infection and increase COVID-19 severity (Bergman, 2021; Rhodes et al., 2021; Seal et al., 2022). Vitamin D is widely known for its role in calcium and phosphate balance but supports also key functions in many organs, including the brain, muscle and the immune system (Carlberg and Muñoz, 2022; Holick, 2022). Its immunomodulatory role promotes the development of an anti-inflammatory and antiviral environment and consequently, its deficiency seems to contribute to airway and gastrointestinal infectious illnesses (Ilie et al., 2020; Watkins, 2020). It has been suggested that vitamin D3 supplementation may be used prophylactically as an affordable and safe treatment strategy that could be added to existing COVID-19 protocols. However, there is still no clear evidence that vitamin D3 supplementation can prevent the severity and/or mortality of COVID-19.
Accordingly, the main objective of this study was to evaluate the safety, tolerability and effectiveness of vitamin D3 supplementation to reduce the duration and severity of COVID-19 in hospitalized individuals who were recruited for a randomized pilot clinical trial to receive the moderate dose of 2000 International Units (IU)/daily of cholecalciferol or a higher dose of 10,000 IU/daily for 14 days, in combination with the standard drug therapeutic regimen.
This is a multicenter, single-blinded, prospective randomized pilot clinical trial (RCT) to evaluate the safety, tolerability, and effectiveness of the administration of daily oral supplementation of a high dose of cholecalciferol (vitamin D3) (10,000 IU/day) in comparison with a moderate dose of cholecalciferol (2000 IU/day) and in combination with the standard drug regimen therapeutic. Due to the potential effectiveness of vitamin D3 supplementation, and following the ethical tenet of beneficence, this pilot clinical trial did not include a placebo arm. The moderate (2000 IU/day) dose was selected following the Endocrine Society Practice Guidelines on Vitamin D which recommends the intake of 1,500–2,000 IU/day of vitamin D2 or D3 for adults over 18 year-old to achieve an optimal blood concentration of 25(OH)D in the range of 75–100 nmol/L (30–40 ng/ml) (Holick et al., 2011). The high dose (10,000 IU) was selected because the amount of vitamin D3 made in the skin after Sun exposure has been estimated within a range from 10,000 to 25,000 IU/day (Stamp et al., 1977; Holick and Chen, 2008; McCullough et al., 2019) and also because the daily intake of 10,000 IU/day for 5 months has been considered safe in a healthy population, without reporting events of hypercalcaemia or an increase in the urinary calcium excretion (Heaney et al., 2003; Holick and Chen, 2008). This study was sponsored by Hospital Universitario Severo Ochoa (Madrid, Spain) and was conducted between June 2020 and March 2021 in this hospital and other four Tertiary Care Hospitals located in Spain: Hospital Universitario Infanta Leonor (Madrid), Hospital Universitario Fundación Alcorcón (Alcorcón, Madrid), Hospital Universitario Príncipe de Asturias (Alcalá de Henares, Madrid), and Hospital Universitario de Cabueñes (Gijón, Asturias).
The eligible participants were patients aged 18 years or older diagnosed with COVID-19 pneumonia based on clinical-radiological criteria and positive for SARS-CoV-2 infection confirmed by laboratory detection (RT-PCR), with values of oxygen saturation <94% and levels of 25(OH)D in serum <30 ng/ml. The exclusion criteria were pregnancy or to be lactating, patients who were participating in other clinical trials with drugs with potential antiviral action for COVID-19, on treatment with digoxin, with evidence of Multiple Organ Dysfunction Syndrome (MODS), or who were requiring mechanical ventilation at the time of inclusion. Patients who had hypersensitivity to cholecalciferol or the excipient refined olive oil, had hypercalcemia or hypercalciuria, were diagnosed with hereditary fructose intolerance, sarcoidosis or hyperparathyroidism, had glucose-galactose malabsorption, sucrose insufficiency or chronic kidney disease (stage 4; estimated glomerular filtration rate (eGFR) < 30), or who were expected to be transferred to another hospital in the following 96 h or to die in the next 24–48 h were also excluded.
This pilot clinical trial (protocol ID 01052020) was previously reviewed and approved by the Spanish Agency for Medicines and Health Products (AEMPS) (EudraCT Number 2020–002312–43) and by the Drug Research Ethics Committee of the Hospital Universitario Severo Ochoa (Madrid, Spain) (https://reec.aemps.es/reec/estudio/2020-002312-43). The study was conducted under the recommendations for Clinical Studies and Drug Evaluation in Humans, contained in the latest version of the Declaration of Helsinki, and the Spanish and European Legislation on Clinical Studies (Real Decreto 1090/2015; European Regulation 536/2014). Written or oral informed consent was obtained from all patients.
Following eligibility screening (visit 1), patients were randomized according to a computer-generated process by blocks series sizes of 5 (STATA 14.2 software; StataCorp LLC, College Station, TX) to receive 10,000 IU or 2000 IU of cholecalciferol (1:1) once daily for 14 days. Study medication was presented as an oral solution containing 25,000 IU/2.5 ml of cholecalciferol (Grupo Italfarmaco, Madrid, Spain) (National Code 7188605; ATC code A11CC05). This medication was provided by the pharmacy of each hospital, where the batches of the vials were registered, and administrated by a nurse according to the medical prescription. Throughout the study, all patients received any concomitant medication deemed necessary to provide adequate standard care, according to local recommendations. On-treatment, the visits occurred at seven (visit 2, day 7) and fourteen (visit 3, day 14) days. After 14 days of the end of the treatment, a safety follow-up visit (visit 4, day 28) occurred. At baseline and each visit, patients underwent a physical examination (including vital signs), a chest X-ray or imaging test, an electrocardiogram, and a blood sample collection. Data of the study were collected and recorded using the Research Electronic Data Capture tool (REDCap) online platform (https://e-clinicos.com/redcap/; Vanderbilt University, Nashville, TN), including the following data: age, sex, ethnicity, body mass index (BMI), main coexisting comorbidities (chronic heart/pulmonary/inflammatory/kidney disease, arterial hypertension, asthma, cirrhosis, neoplasia, HIV-1 infection/AIDS, obesity, dementia, malnutrition, smoker), respiratory status (respiratory rate, oxygen flow, ventilatory support), radiological score (number of affected zones of lung parenchyma), vital signs (body temperature, heart rate, breath rate, systolic blood pressure, diastolic blood pressure), symptoms (fever, malaise, upper respiratory tract symptoms, dyspnea, chest pain, cough, expectoration, hemoptysis, myalgia, headache, confusion, seizures, abdominal pain, nausea, vomiting, diarrhea, rash, anosmia), biochemical parameters (leucocytes, neutrophils and lymphocytes count, haemoglobin, platelets, D-Dimer, aPTT, fibrinogen, glucose, creatinine kinase, sodium, potassium, albumin, bilirubin, alanine aminotransferase (ALT/GPT), aspartate aminotransferase (AST/GOT), C-reactive protein (CRP), lactate dehydrogenase (LDH), procalcitonin, ferritin, calcium, phosphate, iPTH and vitamin D), treatments administered during admission (corticosteroids, tocilizumab, remdesivir, ceftriaxone, azithromycin, heparin), together with their previous or indicated treatments. Data were also collected on safety, adverse effects, symptom onset, length of hospital stay (LOS), the occurrence of ARDS, defined by the ratio arterial oxygen pressure/inspired oxygen fraction (PaO2/FiO2) <300 mm Hg, the admission at the Intensive Care Unit (ICU), and mortality.
The quantification of the level of 25(OH)D (ng/ml) in serum samples was performed with the automated immunoassays Liaison 25(OH) Vitamin D Total assay DiaSorin Liaison XL (DiaSorin, Italy) in the participating hospitals, according to the manufacturer’s instructions.
The primary outcome measure was to reach a serum 25(OH)D concentration ≥30 ng/ml (75 nmol/L) after 14 days of supplementation without the presence of any adverse effects. The secondary outcomes were the LOS, defined as the days that participants remained hospitalized from admission until the hospital discharge or death, as well as the development and evolution of blood biomarkers of inflammation. Other pre-specified clinical outcomes were the need for high-flow oxygen, ICU admission and mortality. The criteria for patient discharge were no requirement for supplemental oxygen, absence of fever, and oxygen saturation >94%.
The safety assessment was carried out according to the scheme that included a detailed medical history, a physical examination and a biochemical and blood examination at each visit. Any adverse event that occurred during the study was recorded.
The primary analyses used the intention to treat (ITT) analysis set. The data were evaluated for normality using the Kolmogorov-Smirnov test, and mean ± SD was calculated to represent data following a normal Gaussian pattern, and median and interquartile range for skewed data. Categorical data were expressed as percentages. Group comparisons were done using Mann-Whitney U-test, t-student test or Wilcoxon signed-rank test for numerical data and Chi-square (χ2) or Fisher’s exact test for categorical data. Predictors related to the LOS were identified using multiple linear regression analysis. Predictors related to the ARDS were identified using multiple logistic regression analysis. A two-factor mixed factorial split-plot design was used, with an intersubject factor (2000 IU/day vs. 10,000 IU/day) and an intrasubject factor (baseline, visit 2, and visit 3) using a mixed ANOVA and multiple comparisons between the three-time periods (Repeated Measures Analysis with Stata, n. d.). The statistical analyses and graphics were performed using STATA 14.2 software. p-values lower than 0.05 (two-tailed) were considered to be statistically significant.
A total of 87 participants were enrolled in the study. Of them, two participants that were randomized to the 10,000 IU/day group refused to participate and withdrew consent without having taken the study medication. Finally, 44 participants were assigned to take 2000 IU/day (moderate dose) of cholecalciferol and 41 participants 10,000 IU/day (high dose) of cholecalciferol (Figure 1). A summary of the characteristics of the participants assigned to each treatment group is shown in Table 1. The median time from the onset of the symptoms before admission was 7 days (IQR: 6–10). Median age of the participants was 65 years (IQR: 53–74), 71% of them were male and 54% were obese. The main conditions were hypertension (48%), dyslipidaemia (36%), and diabetes (22%), and at least one of these coexisting diseases were described in 34% of the participants. Most of the participants (86%) showed bilateral pneumonia at chest x-rays. According to the ventilatory support, 85% of the participants received oxygen with nasal goggles (between 1 and 5 L/min) and 15% of them with reservoir (between 6 and 15 L/min). Mean serum 25(OH)D basal levels were 14.8 ng/ml (SD: 6.2). The treatments administered included corticosteroids such as dexamethasone and methylprednisolone (87%), ceftriaxone (59%), azithromycin (44%), IL-6 antagonists such as tocilizumab (25%), and remdesivir (15%). There were no differences between groups at baseline regarding the demographic characteristics, symptoms, vital signs, blood biochemistry data, or treatments, although the level of haemoglobin was significantly higher (p = 0.006) in the group of participants assigned to the 10,000 IU/day group (Supplementary Table S1).

FIGURE 1. Flowchart of the study design. ITT: intention to treat.
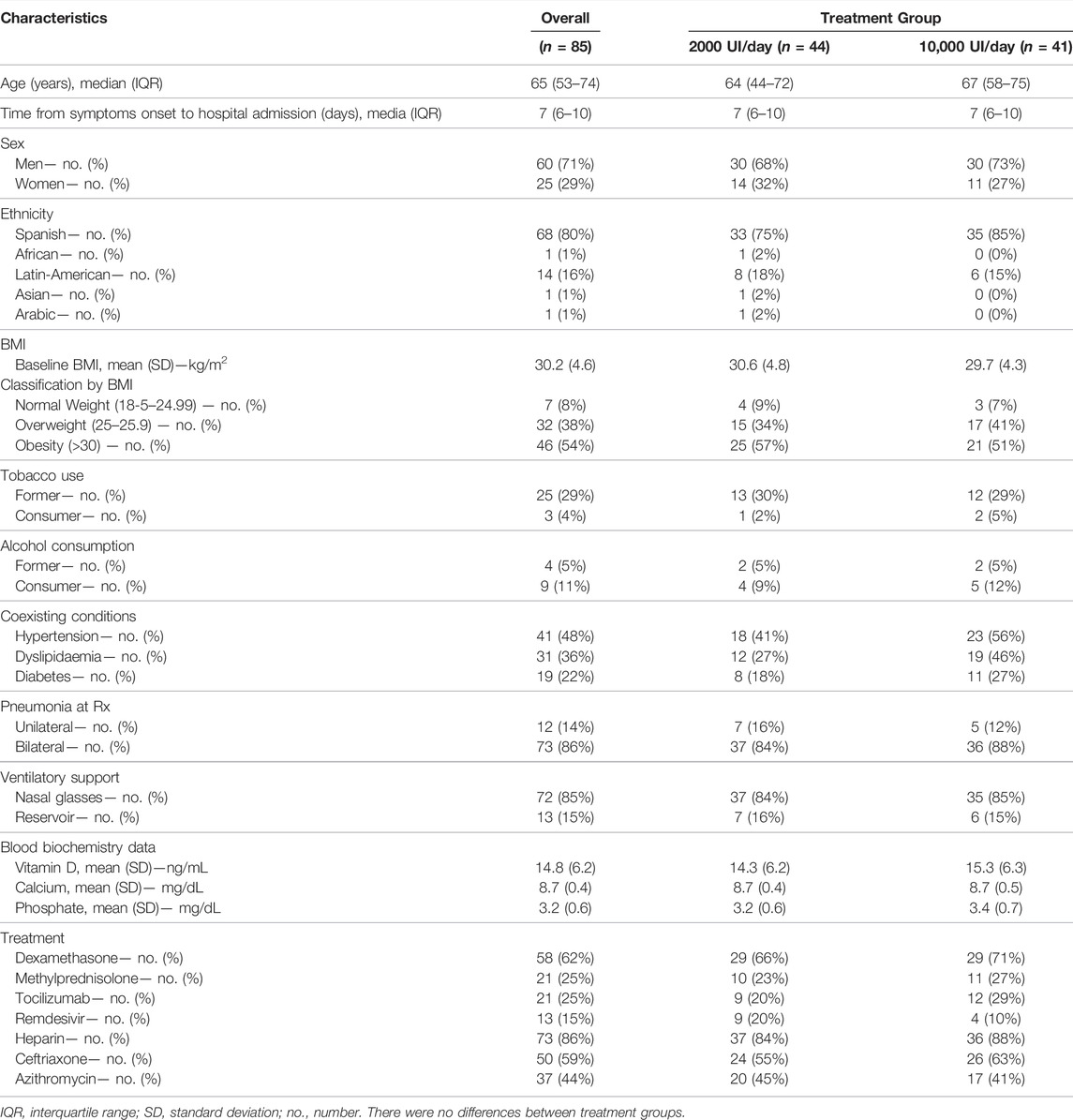
TABLE 1. Baseline clinical and biochemical characteristics in hospitalized patients with COVID-19 who received 2000 IU/day and 10,000IU/day of cholecalciferol.
At the entry in the study, mean serum 25(OH)D levels were very similar in both treatment group (Table 1). After supplementation, target serum 25(OH)D level (≥30 ng/ml) was reached by 7 (16%) participants in the moderate dose group and 20 (49%) in the high dose group (p = 0.0021). The mixed-design ANOVA showed a statistically significant interaction between measurement times and treatment groups: F2.162 = 25.02, p < 0.001 and time: F2.162 = 106.21, p < 0.001 in the serum 25(OH)D levels (Figure 2A).
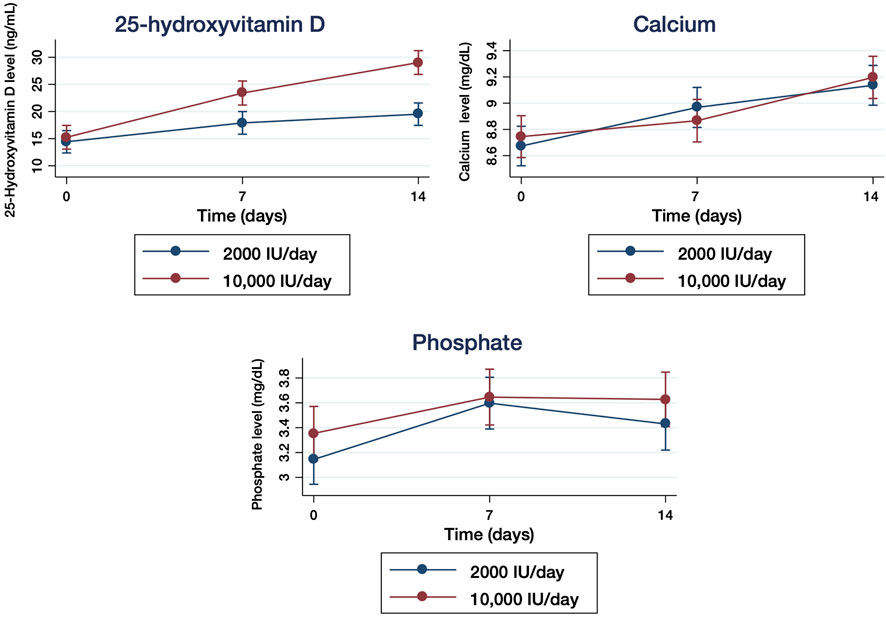
FIGURE 2. Quantification of serum 25-hydroxyvitamin D (25(OH)D) levels (mg/ml) (A), calcium level (mg/dl) (B), and phosphate level (mg/dl) (C) in hospitalized patients with COVID-19 who received 2000 IU/day and 10,000IU/day of cholecalciferol measured at baseline (day 0) and after 7 and 14 days of treatment. The results are presented as means ±95% of confidence intervals.
Basal calcium levels were 8.7 mg/dl (SD: 0.4) in the moderate dose group and 8.7 mg/dl (SD: 0.5) in the high dose group (Table 1). Basal phosphate levels were 3.2 mg/dl (SD: 0.6) in the 2000 IU/day group and 3.4 mg/dl (SD: 0.7) in the 10,000 IU/day group (Table 1). The mixed-design ANOVA did not identify statistically significant interaction between measurement times and treatment groups in serum calcium: F2.160 = 1.52, p = 0.22 (Figure 2B) or phosphate: F2.158 = 0.24, p = 0.79 (Figure 2C) levels, respectively. No episodes of hypercalcemia, hypercalciuria or hyperphosphatemia occurred among the participants in either group as a consequence of the treatment with cholecalciferol.
LOS was similar in both groups, 7 days (IQR: 4–9) among the participants who received 2000 IU/day and 7 days (IQR: 4–8) in those who received 10,000 IU/day, without significant differences between groups (Table 2). Multivariable analysis of predictors associated with the LOS is shown in Table 3. We identified that only supplementation with 10,000 IU/day of vitamin D versus 2000 IU/day (p = 0.01) was associated with a decrease in the LOS, while factors such as age (p < 0.001), male gender (p = 0.01), high oxygen needs at admission (p = 0.001), development of ARDS (p < 0.001) and the treatment with corticosteroids (p = 0.002) were correlated with a significant increase in the LOS. During the study, 10 (12%) participants developed ARDS. Of them, 6 (14%) participants had been randomly assigned to the 2000 IU/day group and 4 (10%) patients to the 10,000 IU/day group (Table 2). The analysis of the predictors related to the development of ARDS showed that female gender (p = 0.049), high oxygen requirements on admission (p = 0.001) and D-dimer levels >0.5 μg/ml at entry (p = 0.047) were associated with significant risk (Table 4). According to ARDS, LOS was significantly different in the groups of vitamin D3 supplementation. Those patients who received 2000 IU/day and developed ARDS stayed at the hospital a median of 27 days (IQR: 12–45), whereas the participants who received 10,000 IU/day stayed 7 days (IQR: 4–13) (p = 0.04) (Table 5). In those participants who developed ARDS, the analysis of the needs for non-invasive mechanical ventilation (NIV) between the groups was not significantly different (n = 3 in 2000 IU/day group vs. n = 1 in 10,000 IU/day group). Similarly, there were no significant differences among these participants in the ICU admission rate (n = 5 in the 2000 IU/day group vs. n = 1 in the 10,000 IU/day group) (Table 5).

TABLE 2. Clinical characteristics in hospitalized patients with COVID-19 who received 2000 IU/day and 10,000IU/day of cholecalciferol.
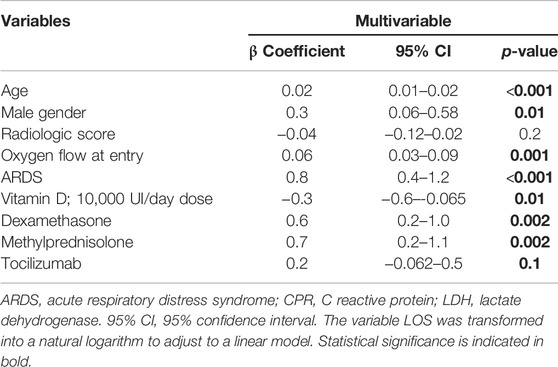
TABLE 3. Multivariable analysis predicting factors associated with the length of hospital stay (LOS) in hospitalized patients with COVID-19.

TABLE 4. Predictive factors related to acute respiratory distress syndrome (ARDS) in hospitalized patients with COVID-19.

TABLE 5. Clinical characteristics in hospitalized patients with COVID-19 who developed acute respiratory distress syndrome (ARDS) during treatment with 2000 IU/day or 10,000IU/day of cholecalciferol.
At the beginning of the study, all participants required supplemental oxygen. Of them, 37 (84%) participants in the 2000 IU/day group and 35 (85%) participants in the 10,000 IU/day needed nasal prongs, whereas 7 (16%) participants in the 2000 IU/day group and 6 (15%) in the 10,000 IU/day group needed reservoir masks (Table 1). During the study, the supplemental oxygen therapy varied from NIV, high-flow nasal cannulae, reservoir masks, or nasal goggles to participants without oxygen requirements, although there were no significant differences between the groups after 7 or 14 days (Table 6). The analysis of the oxygen requirements after 14 days, measured by FiO2, was significantly reduced 7.6-fold in the high dose group compared to the moderate dose group (p = 0.049).
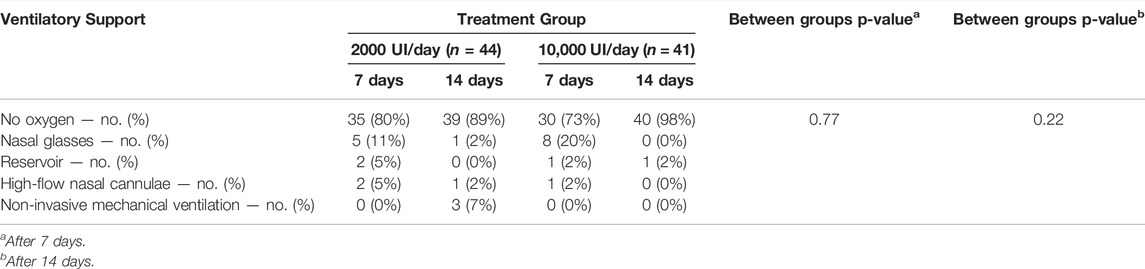
TABLE 6. Oxygen therapies in hospitalized patients with COVID-19 after 7 and 14 days of treatment with 2000 IU/day or 10,000IU/day of cholecalciferol.
In the group of participants who received 2000 IU/day, mean BMI was 30.6 (SD: 4.8) and overweight (OW) was identified in 40 patients, of whom 25 (57%) were obese. Among the participants who received 10,000 IU/day, mean BMI was 29.7 (SD: 4.3) and OW was found in 38 participants, being 21 (51%) classified as obese (Table 1). After 7 days of supplementation, there was a non-significant trend between the moderate dose group and the high dose group both normal-weight (Figure 3A) and obese (Figure 3C) participants. In contrast, the vitamin D levels of OW participants in the high dose group were significantly higher compared to participants of the moderate group (p = 0.005) (Figure 3B). At the end of supplementation (14 days), serum vitamin D levels in normal-weight participants remained with a non-significant trend between treatment groups (Figure 3A) and significantly increased in OW (p < 0.0001) and obese (p < 0.0001) participants (Figures 3B,C). The mixed-design ANOVA showed a statistically significant interaction between measurement times and treatment groups: F2.162 = 25.02, p < 0.001 and time: F2.162 = 106.21, p < 0.001 in the serum 25(OH)D levels (Figure 2A).
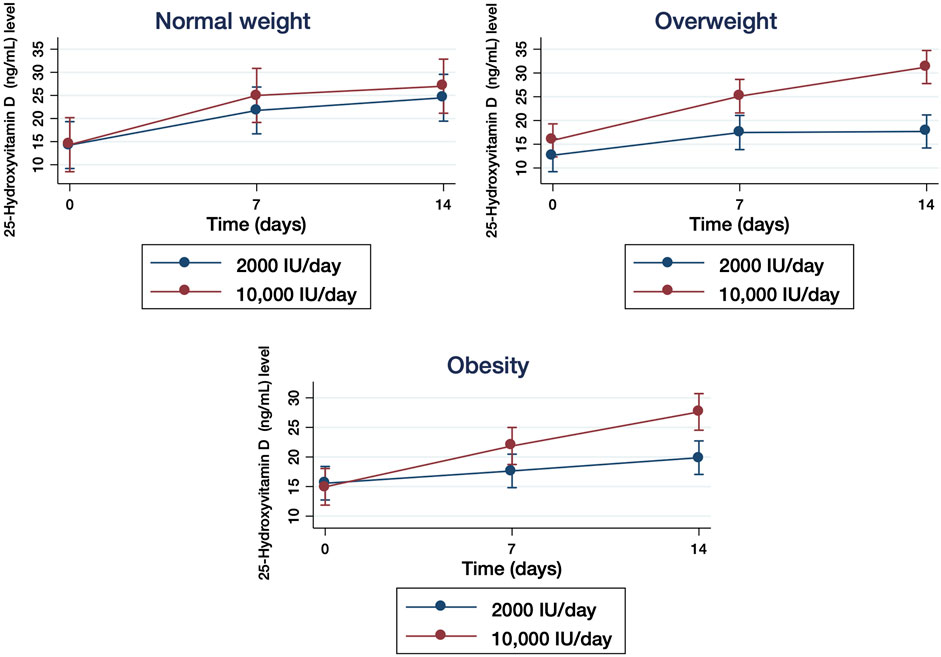
FIGURE 3. Quantification of serum 25-hydroxyvitamin D (25(OH)D) levels in hospitalized patients with COVID-19 who received 2000 IU/day and 10,000IU/day of cholecalciferol classified by the body mass index in normal-weight (BMI:18-5–24.99), overweight (BMI: 25.0–29.9) and obese (BMI ≥30) participants measured at baseline (day 0) and after 7 and 14 days of treatment. The results are presented as means ±95% of confidence intervals.
We analyzed the serological biomarkers related to inflammation and considered them as prognostic factors for COVID-19 severity. LDH levels decreased significantly 1.18- (p = 0.0023) and 1.29- (p < 0.0001) fold in the moderate group after 7 and 14 days, respectively (Figure 4A). Similarly, in the high dose group, LDH levels were significantly reduced 1.23-fold (p < 0.0001) and 1.34-fold (p < 0.0001) after 7 and 14 days, respectively. Ferritin levels also showed a significant reduction of 1.39-fold after 7 days of treatment (p = 0.0013) and 1.96-fold (p < 0.0001) after 14 days of treatment in the moderate dose group, whereas it was reduced 1.15-fold (p = 0.0033) and 1.66-fold (p < 0.0001) in the high dose group after 7 and 14 days of treatment, respectively (Figure 4B).
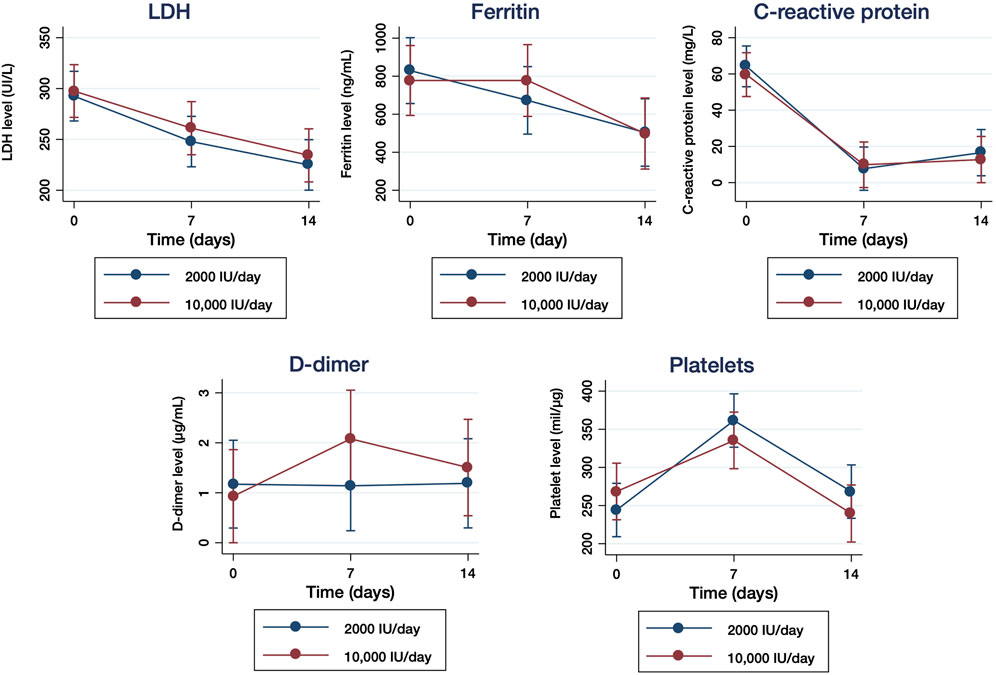
FIGURE 4. Serological biomarkers related to the inflammation in samples of hospitalized patients with COVID-19 who received 2000 IU/day and 10,000IU/day of cholecalciferol. Levels (U/L) of lactate dehydrogenase (LDH) (A), levels (ng/ml) of ferritin (B), levels (mg/L) of C-reactive protein [CRP] (C), levels (µL/ml) of D-Dimer (D) and platelet count (mil/µl) (E) were quantified at baseline (day 0), 7 and 14 days of treatment. The results are presented as means ±95% of confidence intervals.
CRP levels were significantly reduced 8.20-fold (p < 0.0001) after 7 days and 8.34-fold (p < 0.0001) after 14 days in the 2000 IU/day group, whereas they were reduced 7.47- (p < 0.0001) and 6.96- (p < 0.0001) fold in the 10,000 IU/day group after 7 and 14 days, respectively (Figure 4C). D-Dimer levels remained unchanged in the moderate dose group after 7 days of treatment and increased slightly after 14 days, but without statistical significance, whereas in the high dose group D-dimer remained unchanged after 7 and 14 days (Figure 4D). In the case of platelet count, the levels detected increased significantly after 7 days of treatment (p < 0.0001) in both groups, but decreased to basal levels in both moderate and high dose groups after 14 days of treatment, without statistical significance (Figure 4E). The analysis of the comparisons over time did not show significant differences in LDH, ferritin, CPR or D-dimer serum levels, although it was significantly different for the platelet count (p = 0.049).
Thirteen different adverse events were documented in the study participants during the study: 7 adverse events occurred in the 2000 IU/day group and 8 in the 10,000 IU/day group, although none of them was directly attributed to the administration of cholecalciferol (Table 7). The total number of participants experiencing adverse events was 17 in both groups, being 9 (20%) in the moderate dose group and 8 (20%) in the high dose group, without statistically significant differences between groups. The most frequent adverse events recorded were pulmonary embolism (n = 3; 4%) and urinary tract infections (n = 3; 4%), which were diagnosed after hospital discharge.
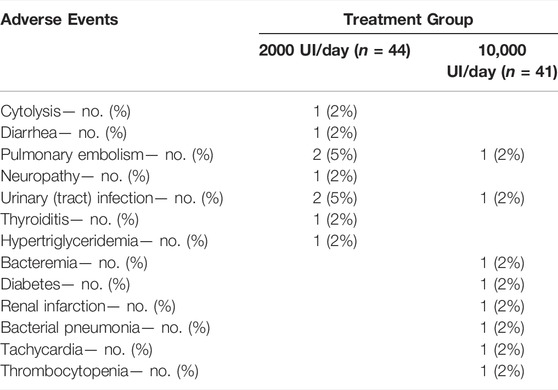
TABLE 7. Adverse events in hospitalized patients with COVID-19 who received 2000 IU/day and 10,000IU/day of cholecalciferol.
Vitamin D is a fat-soluble secosteroid hormone with a well-defined spectrum of immunomodulatory, anti-inflammatory, and antioxidant actions (Ebadi and Montano-Loza, 2020). Its deficiency is considered a public health issue that has been identified in over half of the population worldwide in people of all age groups (Rubin, 2021). Vitamin D deficiency has been associated not only with non-communicable diseases but also with increased susceptibility to infectious diseases; especially, upper respiratory tract infections (RTI) (Cannell et al., 2006; Ginde et al., 2009) and higher risk of community-acquired pneumonia (Zdrenghea et al., 2017; Zhou et al., 2019). Similarly, there is now sufficient evidence to support that vitamin D deficiency may predispose to SARS-CoV-2 infection and increase COVID-19 severity and mortality (Rhodes et al., 2021; Seal et al., 2022; Wang et al., 2022) due to several mechanisms: first, vitamin D reduces lung permeability by modulating the renin-angiotensin system (RAS) pathway and angiotensin converting enzyme 2 (ACE2) expression; second, it promotes the production of antimicrobial peptides in the epithelium of the respiratory tract, thereby reducing the possibility of virus infection and COVID-19 symptoms; third, vitamin D favours an anti-inflammatory environment, mostly by reducing the concentration of pro-inflammatory cytokines such as tumor necrosis factor (TNF)-α and IFNγ and by increasing the expression of anti-inflammatory cytokines by macrophages; and finally, vitamin D stabilizes the physical barriers by contributing to the maintenance of functional tight junctions, gap junctions and adherence junctions (Pedersen et al., 2009; Baeke et al., 2010). On the other hand, COVID-19 is characterized by the dysregulation of the inflammatory response, especially the RAS pathway. Consequently, the degree of immune overactivation has been associated with a poorer prognosis (Hu et al., 2021). Accordingly, the use of anti-inflammatory drugs during COVID-19 has been proved to be beneficial, as occurs with corticosteroids (Recovery Collaborative Group et al., 2021).
Vitamin D deficiency has been linked to geographical differences in ARDS and COVID-19 mortality (Marik et al., 2020). Therefore, vitamin D3 supplementation could be used prophylactically to reduce the severity of COVID-19, especially in those regions where hypovitaminosis D is frequent (Panarese and Shahini, 2020). Despite Spain is a country with an adequate amount of daily sunlight, the overall vitamin D intake is lower than the recommended levels of 10 µg/day and consequently, the prevalence of deficient 25(OH)D levels among the Spanish population is high (González-Rodríguez et al., 2013; Olza et al., 2017). Indeed, 78.8% of the participants recruited for our study showed basal 25(OH)D serum levels <20 ng/ml (50 nmol/L). A similar study that was performed in adults who were hospitalized for mild to moderate COVID-19 and were supplemented with a 5,000 IU/day dose of vitamin D3 during the same time (14 days), serum 25(OH)D levels raised to sufficiency (≥30 ng/ml) (Sabico et al., 2021). However, these individuals were younger than our cohort and showed median baseline serum 25(OH)D levels that were substantially higher. Accordingly, we decided to provide a higher dose of cholecalciferol (10,000 IU) that was administered daily due to the protective effects are expected to be higher when the individuals received daily or weekly doses versus high dose boluses (Martineau et al., 2019). After the daily supplementation of 10,000 IU cholecalciferol for 14 days, 93% of the participants achieved an increase of serum 25(OH)D levels ≥20 ng/ml versus 32% of the individuals who received the 2000 IU/day dose. Although there was a significant 1.5-fold increase of serum 25(OH)D levels that were close to sufficiency in those participants who received the higher dose of cholecalciferol (29 ng/ml; IQR: 25–34) in comparison to those participants that received the moderate dose (17 ng/ml; IQR: 14–23), the primary outcome of a serum 25(OH)D concentration ≥30 ng/ml after 14 days of treatment was not achieved. This could be due to 25 [OH]D is a negative component of the acute phase response (Waldron et al., 2013; Silva and Furlanetto, 2015) and it is usually reduced during acute inflammatory procedures such as COVID-19 (Antonelli and Kushner, 2021). In fact, the deficiency of vitamin D at hospital admission in individuals with COVID-19 has been appointed as a potential prognostic marker of disease severity that would indicate the progression to the inflammatory form of the disease (Chiodini et al., 2021; Seal et al., 2022). Accordingly, the achievement of the primary endpoint of >30 ng/ml of 25 [OH]D in individuals with COVID-19 may be impaired due to the inflammatory process, even with the higher dose of 10,000 IU/day. However, we determined that the administration of the higher dose of 10,000 IU/day was safe and well tolerated by all the participants in the study as we did not observe episodes of hypercalcemia, hypercalciuria, or hyperphosphatemia that are considered to be the initial signs of vitamin D intoxication, or any other related adverse events.
Previous data from other intervention trials showed a preventive effect of vitamin D3 supplementation in acute RTIs that was increased in patients with vitamin D deficiency (Martineau et al., 2017; Jolliffe et al., 2021). However, in individuals hospitalized with COVID-19, the clinical effects of the use of vitamin D3 supplementation have yielded mixed results. A Spanish population-based study concluded that patients on cholecalciferol treatment had a lower risk of SARS-CoV2 infection, lower risk of severe COVID-19 and lower COVID-19 mortality than unsupplemented 25(OH)D-deficient patients (Oristrell et al., 2022), and a case-series study in COVID-19 patients who received 50,000 IU/day for 5 days showed a reduction in the inflammatory markers and time for recovery in comparison to those who received 1,000 IU/day (Ohaegbulam et al., 2020). Similarly, a previous RCT in Spain demonstrated that the administration of a high dose (0.532 mg) of calcifediol (25(OH)D3) significantly reduced the need for ICU admission (Entrenas Castillo et al., 2020), and a placebo-controlled, double-blinded clinical trial reported that in 106 hospitalized patients, those who received vitamin D had a lower trend for hospitalization, ICU duration, need for ventilator assistance and mortality (Maghbooli et al., 2021). On the contrary, data from previous studies and a systematic review evaluating vitamin D3 supplementation found low to moderate certainty evidence that a single high dose of vitamin D3 is effective to reduce mortality, LOS, ICU admissions, and D-dimer or CRP levels (da Rocha et al., 2021; Murai et al., 2021). Our results did not report a reduction in the LOS or the ICU admissions when the administration of a high dose of vitamin D3 for 14 days was compared with the administration of a moderate dose. However, the oxygen requirements measured by FiO2 were significantly reduced in those patients assigned to the high dose group, thereby confirming previous reports (Ohaegbulam et al., 2020). Interestingly, those participants with ARDS from our cohort who received the higher dose of vitamin D3 showed a significant reduction in the LOS of 23.5 days on average in comparison with those patients who received the moderate dose. Despite the small number of patients who accelerated their recovery, these results achieved statistical significance and they were in accordance with previous studies that support that a higher vitamin D3 status is associated with a significant reduction in infectivity, morbidity and mortality from SARS-CoV-2 infection (Seal et al., 2022; Wang et al., 2022) and also that treatment with vitamin D3 during COVID-19 may also shorten the hospital stay and decrease mortality (Gönen et al., 2021). Moreover, according to previous observations in animal models (Yang et al., 2016), the higher dose of vitamin D3 in patients with ARDS would increase the expression levels of ACE2, inducing moderate lung changes that might contribute to reduce the symptoms of this syndrome. In our study, the potential positive effect of vitamin D3 could be related to the early administration just after hospitalization, as the accelerated improvement of 25(OH)D3 levels may develop an anti-inflammatory environment, thereby helping to reduce the length of stay, ICU admission, and mortality in COVID-19 patients (Holick, 2022). Finally, the biochemical inflammatory parameters related to poor prognosis improved mainly during the first week, regardless of the dose of vitamin D administered, as we did not observe significant changes in the serum levels of LDH, ferritin, CRP, or D-dimer serum levels between the two groups. Although the platelet count showed a modest but significant difference in those patients who were supplemented with the higher dose, these changes may not be clinically meaningful.
On the other hand, a high prevalence of vitamin D deficiency has been described in obese and OW patients (Pereira-Santos et al., 2015), likely caused by a dilution into the greater volumes of fat, serum, liver, and muscle that are present in obese individuals (Vranić et al., 2019), although other mechanisms, such as the sequestration of vitamin D by the adipose tissue may not be completely discarded (Wortsman et al., 2000). Due to risk factors such as excess visceral fat or high BMI have been associated with a higher probability to develop more severe forms of COVID-19 (Zhou et al., 2019), a possible link may exists between COVID-19 severity, vitamin D deficiency and BMI. In our study, significant increases in serum 25(OH)D levels were observed among obese and OW participants who received the highest dose in comparison with those who received the moderate dose, while the serum levels in normal weight participants were not different between the groups. However, most of our participants were either OW or obese, as these factors are related to a higher probability to develop severe COVID-19. Therefore, we may not rule out that this imbalance in the BMI between the participants might be affecting the results. Accordingly, the effectiveness of vitamin D3 supplementation in these individuals with high BMI to positively influence the clinical recovery from COVID-19 needs to be further analyzed by interventional studies.
This study presents two potential limitations. First, our study was not designed as a double-blinded RCT due to the Pharmacy services of the different hospitals needed to change the commercial medication into non-commercial syringes to be supplied to the participants that had been assigned to each treatment group, which made necessary that both the Pharmacy service and the Researchers knew the treatment group to which the participant had been assigned. Therefore, we cannot rule out that the single-blinded RCT design might have biased the assessment of more subjective parameters (e.g chest X-ray) in favour of those participants who received the high dose. On the other hand, the beneficial effect of vitamin D3 supplementation over the reduction of the LOS in individuals who developed ARDS have been described in a small fraction of the participants (10/85), and although these results reached statistical significance, they need to be considered with caution until confirmation in a larger cohort.
In conclusion, the supplementation of a high dose of 10,000 IU/day of cholecalciferol for 14 days in hospitalized patients with COVID-19 was well tolerated and did not cause significant adverse events in comparison with the moderate dose of 2000 IU/day. The higher dose was more effective than the moderate dose to induce a significant increase of 25(OH)D levels in serum, especially in OW and obese individuals, although the participants did not achieve the target level (≥30 ng/ml). Moreover, the results obtained in our cohort supported that a higher dose of vitamin D3 supplementation in association with the standard clinical care may be effective to improve the oxygen requirements during hospitalization by COVID-19 and to reduce the LOS in those individuals who developed ARDS. Although this study supports the notion that vitamin D3 supplementation during COVID-19 may be safe, tolerable and beneficial, more randomized clinical trials are needed to determine the true efficacy of vitamin D supplementation as part of the therapeutic arsenal used against COVID-19 disease.
David Alonso-Menchén (Hospital Universitario Príncipe de Asturias), Adriana Álvarez Jusdado (Hospital Universitario Severo Ochoa), Daniel Barranco Maroto (Hospital Universitario Severo Ochoa), Ytsel Bello Pastor (Hospital Universitario Severo Ochoa), Cristina Córdoba Chicote (Hospital Universitario Severo Ochoa), Guillermo Cuevas Tascón (Hospital Universitario Infanta Leonor), Víctor Díez Viñas (Hospital Universitario Infanta Leonor), Inés Dorado Manzanares (Hospital Universitario Severo Ochoa), Ismael Escobar Rodríguez (Hospital Universitario Infanta Leonor), Eva Fonseca Aizpuri (Hospital Universitario de Cabueñes), Rosa María Galán Zuheros (Hospital Universitario Severo Ochoa), Concepción García Lacalle (Hospital Universitario Severo Ochoa), Mario García Peña (Hospital Universitario Severo Ochoa), Sebastiano Garotti (Hospital Universitario Severo Ochoa), Marta Gómez Sanz (Hospital Universitario Severo Ochoa), Tamara Gómez Zuil (Hospital Universitario Severo Ochoa), María González Pozuelo (Hospital Universitario Infanta Leonor), Cristina Helguera Amezua (Hospital Universitario de Cabueñes), María del Carmen Herrero Alonso (Hospital Universitario Fundación Alcorcón), Javier Marcos Arias (Hospital Universitario Fundación Alcorcón), Emilio José Martínez Martín (Hospital Universitario Fundación Alcorcón), Javier Montoya Adarraga (Hospital Universitario Infanta Leonor), Patricia Moreira Escrich (Hospital Universitario Severo Ochoa), María Jesús Moro Álvarez (Hospital Universitario Infanta Leonor), Paula Novo González (Hospital Universitario Severo Ochoa), Raquel Paz Peño (Hospital Universitario Severo Ochoa), Alejandro Pérez Cachaldora (Hospital Universitario Severo Ochoa), Miriam Rodríguez Fernández (Hospital Universitario Severo Ochoa), María del Carmen Romero Pérez (Hospital Universitario Severo Ochoa), José Sanz-Moreno (Hospital Universitario Príncipe de Asturias), Mercedes Toral Leiva (Hospital Universitario Severo Ochoa), Nuria Toro Moreno (Hospital Universitario Severo Ochoa), Rafael Torres Perea (Hospital Universitario Severo Ochoa), María Velasco Arribas (Hospital Universitario Fundación Alcorcón), Gema Vico Díaz-Parreño (Hospital Universitario Severo Ochoa), Ana Villanueva Fernández-Ardavín (Hospital Universitario Fundación Alcorcón), Rocío Minaya Carrero (Hospital Universitario Severo Ochoa), Monserrat Rodríguez Miguel (Hospital Universitario Severo Ochoa).
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Spanish Agency for Medicines and Health Products (AEMPS) (EudraCT Number 2020-002312-43) adn the Drug Research Ethics Committee of the Hospital Universitario Severo Ochoa (Madrid, Spain) (https://reec.aemps.es/reec/estudio/2020-002312-43). The patients/participants provided their written informed consent to participate in this study.
MCe, MT and MCo conceptualized the project. MT wrote the manuscript. DL-W, MN-M, PR-M, MLT-M and MCe identified, selected, recruited the patients, and collected the samples. GC, LV, and SR-M processed samples. MT and MCe collected and analyzed the clinical data. All co-authors read and approved the final version of the manuscript.
This work was supported by Fundación Universidad Alfonso X el Sabio (FUAX, Madrid, Spain; ID Project: 1.012.010; ID Project EQA: 925.280); the Coordinated Research Activities at the National Center of Microbiology (Instituto de Salud Carlos III) (COV20_00679) to promote an integrated response against SARS-CoV-2 in Spain (Spanish Ministry of Science and Innovation) that is coordinated by Dr. Inmaculada Casas (WHO National Influenza Center of the CNM); a generous donation provided by Chiesi España, S.A.U. (Barcelona, Spain). The work of Montserrat Torres was financed by the Coordinated Research Activities at the CNM (Instituto de Salud Carlos III) (COV20_00679). The work of Lorena Vigón was supported by a pre-doctoral grant from Instituto de Salud Carlos III (FIS PI16CIII/00034-ISCIII-FEDER). The work of Sara Rodríguez-Mora was financed by NIH grant R01AI143567.
Drug Cholecalciferol (vitamin D) used in this study was donated by Italfarmaco Group (Cholecalciferol 25,000IU/2.5 ml oral solution). Italfarmaco Group had no role in the design and conduct of the study, in the collection, management, analysis, and interpretation of the data, or the preparation, review, or approval of the manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We greatly appreciate all the patients for their participation in this study. We thank Dr Amanda Fernández and Dr Verónica Briz from the National Center of Microbiology (Instituto de Salud Carlos III, Majadahonda) for their help and support for the statistical analysis of the clinical data presented in this manuscript, and María C. de la Cruz at the Central Support Unit for Clinical Research and Clinical Trials (Health Research Institute Gregorio Marañon; IiSGM) for her advice and assistance related to clinical research with medicines.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.863587/full#supplementary-material
Antonelli, M., and Kushner, I. (2021). Low Serum Levels of 25-Hydroxyvitamin D Accompany Severe COVID-19 Because it Is a Negative Acute Phase Reactant. Am. J. Med. Sci. 362, 333–335. doi:10.1016/j.amjms.2021.06.005
Baeke, F., Takiishi, T., Korf, H., Gysemans, C., and Mathieu, C. (2010). Vitamin D: Modulator of the Immune System. Curr. Opin. Pharmacol. 10, 482–496. doi:10.1016/j.coph.2010.04.001
Bergman, P. (2021). The Link between Vitamin D and COVID-19: Distinguishing Facts from Fiction. J. Intern. Med. 289, 131–133. doi:10.1111/joim.13158
Cannell, J. J., Vieth, R., Umhau, J. C., Holick, M. F., Grant, W. B., Madronich, S., et al. (2006). Epidemic Influenza and Vitamin D. Epidemiol. Infect. 134, 1129–1140. doi:10.1017/S0950268806007175
Carlberg, C., and Muñoz, A. (2022). An Update on Vitamin D Signaling and Cancer. Semin. Cancer Biol. 79, 217–230. doi:10.1016/j.semcancer.2020.05.018
Chen, N., Zhou, M., Dong, X., Qu, J., Gong, F., Han, Y., et al. (2020). Epidemiological and Clinical Characteristics of 99 Cases of 2019 Novel Coronavirus Pneumonia in Wuhan, China: a Descriptive Study. Lancet 395, 507–513. doi:10.1016/S0140-6736(20)30211-7
Chiodini, I., Gatti, D., Soranna, D., Merlotti, D., Mingiano, C., Fassio, A., et al. (2021). Vitamin D Status and SARS-CoV-2 Infection and COVID-19 Clinical Outcomes. Front. Public Health 9, 736665. doi:10.3389/fpubh.2021.736665
Couzin-Frankel, J. (2021). Antiviral Pills Could Change Pandemic's Course. Science 374, 799–800. doi:10.1126/science.acx9605
Ebadi, M., and Montano-Loza, A. J. (2020). Perspective: Improving Vitamin D Status in the Management of COVID-19. Eur. J. Clin. Nutr. 74, 856–859. doi:10.1038/s41430-020-0661-0
Entrenas Castillo, M., Entrenas Costa, L. M., Vaquero Barrios, J. M., Alcalá Díaz, J. F., López Miranda, J., Bouillon, R., et al. (2020). "Effect of Calcifediol Treatment and Best Available Therapy versus Best Available Therapy on Intensive Care Unit Admission and Mortality Among Patients Hospitalized for COVID-19: A Pilot Randomized Clinical Study". J. Steroid Biochem. Mol. Biol. 203, 105751. doi:10.1016/j.jsbmb.2020.105751
Esposito, S., Gnocchi, M., Gagliardi, M., Affanni, P., Veronesi, L., Colucci, M. E., et al. (2020). Therapeutic Strategies against COVID-19. Acta Biomed. 91, e2020038. doi:10.23750/abm.v91i3.10450
Ginde, A. A., Mansbach, J. M., and Camargo, C. A. (2009). Association between Serum 25-Hydroxyvitamin D Level and Upper Respiratory Tract Infection in the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 169, 384–390. doi:10.1001/archinternmed.2008.560
Gönen, M. S., Alaylıoğlu, M., Durcan, E., Özdemir, Y., Şahin, S., Konukoğlu, D., et al. (2021). Rapid and Effective Vitamin D Supplementation May Present Better Clinical Outcomes in COVID-19 (SARS-CoV-2) Patients by Altering Serum INOS1, IL1B, IFNg, Cathelicidin-LL37, and ICAM1. Nutrients 13, 4047. doi:10.3390/nu13114047
González-Rodríguez, L. G., Estaire, P., Peñas-Ruiz, C., and Ortega, R. M. (2013). Vitamin D Intake and Dietary Sources in a Representative Sample of Spanish Adults. J. Hum. Nutr. Diet. 26 Suppl 1, 64–72. doi:10.1111/jhn.12061
Goyal, P., Choi, J. J., Pinheiro, L. C., Schenck, E. J., Chen, R., Jabri, A., et al. (2020). Clinical Characteristics of Covid-19 in New York City. N. Engl. J. Med. 382, 2372–2374. doi:10.1056/NEJMc2010419
Heaney, R. P., Davies, K. M., Chen, T. C., Holick, M. F., and Barger-Lux, M. J. (2003). Human Serum 25-hydroxycholecalciferol Response to Extended Oral Dosing with Cholecalciferol. Am. J. Clin. Nutr. 77, 204–210. doi:10.1093/ajcn/77.1.204
Holick, M. F., Binkley, N. C., Bischoff-Ferrari, H. A., Gordon, C. M., Hanley, D. A., Heaney, R. P., et al. (2011). Evaluation, Treatment, and Prevention of Vitamin D Deficiency: an Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 96, 1911–1930. doi:10.1210/jc.2011-0385
Holick, M. F., and Chen, T. C. (2008). Vitamin D Deficiency: a Worldwide Problem with Health Consequences. Am. J. Clin. Nutr. 87, 1080S–6S. doi:10.1093/ajcn/87.4.1080S
Holick, M. F. (2022). The CO-VID D-Lemma: A Call for Action. Nutrients 14, 963. doi:10.3390/nu14050963
Hu, B., Guo, H., Zhou, P., and Shi, Z. L. (2020). Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 19, 1–14. doi:10.1038/s41579-020-00459-7
Hu, B., Huang, S., and Yin, L. (2021). The Cytokine Storm and COVID-19. J. Med. Virol. 93, 250–256. doi:10.1002/jmv.26232
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., et al. (2020). Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 395, 497–506. doi:10.1016/S0140-6736(20)30183-5
Ilie, P. C., Stefanescu, S., and Smith, L. (2020). The Role of Vitamin D in the Prevention of Coronavirus Disease 2019 Infection and Mortality. Aging Clin. Exp. Res. 32, 1195–1198. doi:10.1007/s40520-020-01570-8
Jolliffe, D. A., Camargo, C. A., Sluyter, J. D., Aglipay, M., Aloia, J. F., Ganmaa, D., et al. (2021). Vitamin D Supplementation to Prevent Acute Respiratory Infections: a Systematic Review and Meta-Analysis of Aggregate Data from Randomised Controlled Trials. Lancet Diabetes Endocrinol. 9, 276–292. doi:10.1016/S2213-8587(21)00051-6
Jordan, R. E., Adab, P., and Cheng, K. K. (2020). Covid-19: Risk Factors for Severe Disease and Death. BMJ 368, m1198. doi:10.1136/bmj.m1198
Maghbooli, Z., Sahraian, M. A., Jamalimoghadamsiahkali, S., Asadi, A., Zarei, A., Zendehdel, A., et al. (2021). Treatment with 25-Hydroxyvitamin D3 (Calcifediol) Is Associated with a Reduction in the Blood Neutrophil-To-Lymphocyte Ratio Marker of Disease Severity in Hospitalized Patients with COVID-19: A Pilot Multicenter, Randomized, Placebo-Controlled, Double-Blinded Clinical Trial. Endocr. Pract. 27, 1242–1251. doi:10.1016/j.eprac.2021.09.016
Malik, P., Patel, U., Mehta, D., Patel, N., Kelkar, R., Akrmah, M., et al. (2021). Biomarkers and Outcomes of COVID-19 Hospitalisations: Systematic Review and Meta-Analysis. BMJ Evid. Based Med. 26, 107–108. doi:10.1136/bmjebm-2020-111536
Marik, P. E., Kory, P., and Varon, J. (2020). Does Vitamin D Status Impact Mortality from SARS-CoV-2 Infection? Med. Drug Discov. 6, 100041. doi:10.1016/j.medidd.2020.100041
Martineau, A. R., Jolliffe, D. A., Hooper, R. L., Greenberg, L., Aloia, J. F., Bergman, P., et al. (2017). Vitamin D Supplementation to Prevent Acute Respiratory Tract Infections: Systematic Review and Meta-Analysis of Individual Participant Data. BMJ 356, i6583. doi:10.1136/bmj.i6583
Martineau, A. R., Thummel, K. E., Wang, Z., Jolliffe, D. A., Boucher, B. J., Griffin, S. J., et al. (2019). Differential Effects of Oral Boluses of Vitamin D2 vs Vitamin D3 on Vitamin D Metabolism: A Randomized Controlled Trial. J. Clin. Endocrinol. Metab. 104, 5831–5839. doi:10.1210/jc.2019-00207
McCullough, P. J., Lehrer, D. S., and Amend, J. (2019). Daily Oral Dosing of Vitamin D3 Using 5000 TO 50,000 International Units a Day in Long-Term Hospitalized Patients: Insights from a Seven Year Experience. J. Steroid Biochem. Mol. Biol. 189, 228–239. doi:10.1016/j.jsbmb.2018.12.010
Merad, M., and Martin, J. C. (2020). Pathological Inflammation in Patients with COVID-19: a Key Role for Monocytes and Macrophages. Nat. Rev. Immunol. 20, 355–362. doi:10.1038/s41577-020-0331-4
Mishra, S. K., and Tripathi, T. (2021). One Year Update on the COVID-19 Pandemic: Where Are We Now? Acta Trop. 214, 105778. doi:10.1016/j.actatropica.2020.105778
Murai, I. H., Fernandes, A. L., Sales, L. P., Pinto, A. J., Goessler, K. F., Duran, C. S. C., et al. (2021). Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients with Moderate to Severe COVID-19: A Randomized Clinical Trial. JAMA 325, 1053–1060. doi:10.1001/jama.2020.26848
Ohaegbulam, K. C., Swalih, M., Patel, P., Smith, M. A., and Perrin, R. (2020). Vitamin D Supplementation in COVID-19 Patients: A Clinical Case Series. Am. J. Ther. 27, e485–e490. doi:10.1097/MJT.0000000000001222
Olza, J., Aranceta-Bartrina, J., González-Gross, M., Ortega, R. M., Serra-Majem, L., Varela-Moreiras, G., et al. (2017). Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study. Nutrients 9, 168. doi:10.3390/nu9020168
Oristrell, J., Oliva, J. C., Casado, E., Subirana, I., Domínguez, D., Toloba, A., et al. (2022). Vitamin D Supplementation and COVID-19 Risk: a Population-Based, Cohort Study. J. Endocrinol. Invest. 45, 167–179. doi:10.1007/s40618-021-01639-9
Panarese, A., and Shahini, E. (2020). Letter: Covid-19, and Vitamin D. Aliment. Pharmacol. Ther. 51, 993–995. doi:10.1111/apt.15752
Parums, D. V. (2022). Editorial: Current Status of Oral Antiviral Drug Treatments for SARS-CoV-2 Infection in Non-hospitalized Patients. Med. Sci. Monit. 28, e935952. doi:10.12659/MSM.935952
Pedersen, A. W., Holmstrøm, K., Jensen, S. S., Fuchs, D., Rasmussen, S., Kvistborg, P., et al. (2009). Phenotypic and Functional Markers for 1alpha,25-Dihydroxyvitamin D(3)-modified Regulatory Dendritic Cells. Clin. Exp. Immunol. 157, 48–59. doi:10.1111/j.1365-2249.2009.03961.x
Pereira-Santos, M., Costa, P. R., Assis, A. M., Santos, C. A., and Santos, D. B. (2015). Obesity and Vitamin D Deficiency: a Systematic Review and Meta-Analysis. Obes. Rev. 16, 341–349. doi:10.1111/obr.12239
Repeated Measures Analysis with Stata (2022). Repeated Measures Analysis with Stata. [WWW Document], n.d. URL https://stats.oarc.ucla.edu/stata/seminars/repeated-measures-analysis-with-stata/(accessed 12 5, 2022).
Recovery Collaborative Group, Horby, P., Lim, W. S., Emberson, J. R., Mafham, M., Bell, J. L., et al. (2021). Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 384, 693–704. doi:10.1056/NEJMoa2021436
Rhodes, J. M., Subramanian, S., Laird, E., Griffin, G., and Kenny, R. A. (2021). Perspective: Vitamin D Deficiency and COVID-19 Severity - Plausibly Linked by Latitude, Ethnicity, Impacts on Cytokines, ACE2 and Thrombosis. J. Intern. Med. 289, 97–115. doi:10.1111/joim.13149
Rocha, A. P., Atallah, A. N., Aldrighi, J. M., Pires, A. L. R., Santos Puga, M. E., and Pinto, A. C. P. N. (2021). Insufficient Evidence for Vitamin D Use in COVID‐19: A Rapid Systematic Review. Int. J. Clin. Pract. 75, e14649. doi:10.1111/ijcp.14649
Rubin, R. (2021). Sorting Out whether Vitamin D Deficiency Raises COVID-19 Risk. JAMA 325, 329–330. doi:10.1001/jama.2020.24127
Sabico, S., Enani, M. A., Sheshah, E., Aljohani, N. J., Aldisi, D. A., Alotaibi, N. H., et al. (2021). Effects of a 2-Week 5000 IU versus 1000 IU Vitamin D3 Supplementation on Recovery of Symptoms in Patients with Mild to Moderate Covid-19: A Randomized Clinical Trial. Nutrients 13, 2170. doi:10.3390/nu13072170
Seal, K. H., Bertenthal, D., Carey, E., Grunfeld, C., Bikle, D. D., and Lu, C. M. (2022). Association of Vitamin D Status and COVID-19-Related Hospitalization and Mortality. J. Gen. Intern. Med. 37, 853–861. doi:10.1007/s11606-021-07170-0
Silva, M. C., and Furlanetto, T. W. (2015). Does Serum 25-hydroxyvitamin D Decrease during Acute-phase Response? A Systematic Review. Nutr. Res. 35, 91–96. doi:10.1016/j.nutres.2014.12.008
Stamp, T. C., Haddad, J. G., and Twigg, C. A. (1977). Comparison of Oral 25-hydroxycholecalciferol, Vitamin D, and Ultraviolet Light as Determinants of Circulating 25-hydroxyvitamin D. Lancet 1, 1341–1343. doi:10.1016/s0140-6736(77)92553-3
Vigón, L., Fuertes, D., García-Pérez, J., Torres, M., Rodríguez-Mora, S., Mateos, E., et al. (2021). Impaired Cytotoxic Response in PBMCs from Patients with COVID-19 Admitted to the ICU: Biomarkers to Predict Disease Severity. Front. Immunol. 12, 1901. doi:10.3389/fimmu.2021.665329
Vranić, L., Mikolašević, I., and Milić, S. (2019). Vitamin D Deficiency: Consequence or Cause of Obesity? Medicina 55, 541. doi:10.3390/medicina55090541
Waldron, J. L., Ashby, H. L., Cornes, M. P., Bechervaise, J., Razavi, C., Thomas, O. L., et al. (2013). Vitamin D: a Negative Acute Phase Reactant. J. Clin. Pathol. 66, 620–622. doi:10.1136/jclinpath-2012-201301
Wang, Z., Joshi, A., Leopold, K., Jackson, S., Christensen, S., Nayfeh, T., et al. (2022). Association of Vitamin D Deficiency with COVID-19 Infection Severity: Systematic Review and Meta-Analysis. Clin. Endocrinol. (Oxf) 96, 281–287. doi:10.1111/cen.14540
Wortsman, J., Matsuoka, L. Y., Chen, T. C., Lu, Z., and Holick, M. F. (2000). Decreased Bioavailability of Vitamin D in Obesity. Am. J. Clin. Nutr. 72, 690–693. doi:10.1093/ajcn/72.3.690
Yang, J., Zhang, H., and Xu, J. (2016). Effect of Vitamin D on ACE2 and Vitamin D Receptor Expression in Rats with LPS-Induced Acute Lung Injury. Chin. J. Emerg. Med. 25, 1284–1289. doi:10.3760/cma.j.issn.1671-0282.2016.12.016
Yang, X., Yu, Y., Xu, J., Shu, H., Xia, J., Liu, H., et al. (2020). Clinical Course and Outcomes of Critically Ill Patients with SARS-CoV-2 Pneumonia in Wuhan, China: a Single-Centered, Retrospective, Observational Study. Lancet Respir. Med. 8, 475–481. doi:10.1016/S2213-2600(20)30079-5
Zdrenghea, M. T., Makrinioti, H., Bagacean, C., Bush, A., Johnston, S. L., and Stanciu, L. A. (2017). Vitamin D Modulation of Innate Immune Responses to Respiratory Viral Infections. Rev. Med. Virol. 27, e1909. doi:10.1002/rmv.1909
Keywords: COVID-19, SARS-CoV-2, vitamin D3 supplementation, biochemical parameters, risk factors
Citation: Cervero M, López-Wolf D, Casado G, Novella-Mena M, Ryan-Murua P, Taboada-Martínez ML, Rodríguez-Mora S, Vigón L, Coiras M and Torres M (2022) Beneficial Effect of Short-Term Supplementation of High Dose of Vitamin D3 in Hospitalized Patients With COVID-19: A Multicenter, Single-Blinded, Prospective Randomized Pilot Clinical Trial. Front. Pharmacol. 13:863587. doi: 10.3389/fphar.2022.863587
Received: 27 January 2022; Accepted: 06 June 2022;
Published: 04 July 2022.
Edited by:
Kai Hilpert, St George’s, University of London, United KingdomReviewed by:
Igor Murai, University of São Paulo, BrazilCopyright © 2022 Cervero, López-Wolf, Casado, Novella-Mena, Ryan-Murua, Taboada-Martínez, Rodríguez-Mora, Vigón, Coiras and Torres. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miguel Cervero, bWNlcnZlcm9qQG1lLmNvbQ==; Mayte Coiras, bWNvaXJhc0Bpc2NpaWkuZXM=; Montserrat Torres, bS50b3JyZXNAaXNjaWlpLmVz
†Contributing members of the Multidisciplinary Group of Study of COVID-19 (in alphabetical order)
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.