 Chunsong Yang
Chunsong Yang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 03 May 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.852414
This article is part of the Research Topic Reducing the Harm of Medication - Recent Trends in Pharmacovigilance, Volume II View all 13 articles
Objective: Survey pediatricians and guardians of children with tic disorder on medication needs and choices.
Methods: We designed a cross-sectional survey for pediatricians in mainland China, Hong Kong, Macao, and Taiwan, as well as for the guardians of patients with tic disorder from West China Second University Hospital. We collected and analyzed information on clinicians’ medical behavior and medication choices and on guardians’ knowledge of tic disorder, medical treatment behaviors, and medication choices and needs.
Results: We collected responses from 242 physicians and 610 guardians. For patients with tic disorder and without comorbidities, the first-line drugs selected by physicians were tiapride (60.74%), clonidine (32.64%), haloperidol (25.62%), aripiprazole (16.53%), and sulpiride (12.4%). Physicians reported making medication choices by considerations such as clinical guidelines, clinical efficacy, a low incidence of adverse drug reactions, sufficient clinical research evidence, convenient dosage forms, and patient adherence. Guardians reported making medication choices by considerations such as a low incidence of adverse drug reactions, physician recommendations, clinical efficacy, dose, dosage forms, and the convenience and steadiness of obtaining the medication. However, guardians exhibited insufficient knowledge of tic disorder and treatment options.
Conclusions: Physicians and patient guardians differ in their considerations when selecting medications, highlighting a gap in optimizing treatment.
Tic disorder (TD) is a common childhood neuropsychiatric disorder characterized by motor or vocal twitching in one or more parts of the muscles and is sudden, involuntary, repeated, rapid, and purposeless (Yang et al., 2020). TD is categorized as transient, chronic, Tourette syndrome, or undefined (Liu et al., 2020).
The prevalence of transient TD, chronic TD, and Tourette syndrome in children has been estimated at 2.99, 1.61, and 0.77%, respectively, and appears to be more than four times higher in boys (1.06%) than in girls (0.25%) (Knight et al., 2012). In China, the prevalence of transient TD, chronic TD, and Tourette syndrome has been reported as 1.7, 1.2, and 0.3%, respectively (Yang et al., 2016).
TD patients often suffer from comorbidities that affect their physical and mental health. Approximately 30–50% of patients with TD are diagnosed with attention-deficit/hyperactivity disorder, and 10–50% of patients are estimated to have obsessive-compulsive disorder (Kurlan et al., 2002; Hirschtritt et al., 2015). Other comorbidities include sleep disorders, learning difficulties, anxiety, and depression. Patients with TD have an overall lower quality of life than children without TD (Conelea et al., 2011; Eddy et al., 2011; Evans et al., 2016).
Drug therapy is the main treatment to control the symptoms of TD in children, but medication choices vary by country and physician preferences (Waldon et al., 2013). A survey of 22 European experts (Roessner et al., 2011) recorded support for risperidone, clonidine, aripiprazole, and pimozide. A survey of Canadian physicians (Cothros et al., 2019) reported that aripiprazole, risperidone, and clonidine were the most commonly prescribed drugs for TD, but the use of risperidone was decreasing. A survey of 110 Chinese physicians (Lu et al., 2020) showed support for clonidine, aripiprazole, and tiapride as the preferred drugs for newly diagnosed TD cases with moderate chronic TD. Other surveys of drug choices for TD did not investigate factors related to medication choice and polled physicians but not patient guardians.
In addition, patient and guardian awareness of TD is important for controlling the condition, but research has rarely focused on guardian awareness of the disorder, medical treatment behaviors, medication choices, or patient needs. Therefore, we assessed these factors from the perspective of both guardians and physicians so as to improve guardian participation in treatment decision-making and the clinical outcomes.
Pediatricians from major hospitals in China who were members of child development and behavior groups of the Chinese Pediatric Society in Chinese Medical Association were included in the survey. Pediatricians were included if they were in active medical practice, without limitation of professional title or age, and if they prescribed medication for patients with TD. Interns, medical students, and trainees receiving standardized training were excluded.
Patients with TD from the outpatient department of pediatric neurology of West China Second University Hospital, Sichuan University, were included. Patients under 18 years of age who had been diagnosed with TD according to DSM-IV diagnostic criteria and whose guardians agreed to participate and sign the informed consent were included. Patients were excluded if they exhibited cerebral palsy, meningitis, motor language development lags, nail-biting, restless legs syndrome, myasthenia gravis, Brown syndrome, or other neuropsychiatric conditions.
Questionnaires for physicians collected data in three categories: basic information (sex, education level, professional title, years of medical service, and province), medical behavior (tic assessment methods, common treatment methods, and treatment goals), and prescribing behavior (preferred drugs and considerations in selecting drugs). Questionnaires for guardians collected data in three categories: basic information (patient age, disease duration, family history, type of tic, and comorbidities), guardian’s cognition of TD (understanding TD pathways, TD classification, symptoms and characteristics, pathogenic factors, common treatment methods, and treatment duration), and guardian’s medical behavior and medication choices (department of first visit, time to first treatment, treatment methods, and involvement in medication choices).
Questionnaires with incomplete contents were excluded from the analysis. The mean (± standard deviation) or median was used to describe quantitative variables. The frequency or composition ratio was used for categorical variables. Tic assessment methods, treatment goals, and treatment strategies were assigned a numeric score of 1 (“very unimportant”), 2 (“not important”), 3 (“neutral”), 4 (“important”), or 5 (“very important”). Factors in medication choice were evaluated on the same scale. Data analyses were performed in SPSS version 22 (IBM SPSS, Armonk, NY, United States).
The study protocol conformed to the Helsinki Declaration and was approved by the Office of Research Ethics Committees of West China Women’s and Children’s Hospital. All participants voluntarily took part in the study and provided informed consent.
A total of 242 questionnaires were collected, and all contained complete information (effective rate: 100%). Participating physicians were from 24 provinces in eastern, central, and western China and from Hong Kong, Macao, and Taiwan. Almost three quarters (73.55%) were female, and almost all (97%) possessed at least one university degree. Sixty percent of participating physicians had professional titles of deputy senior or above, 69% had been practicing medicine for more than 10 years, and 75.21% worked at Grade III, Level A hospitals (Table 1).
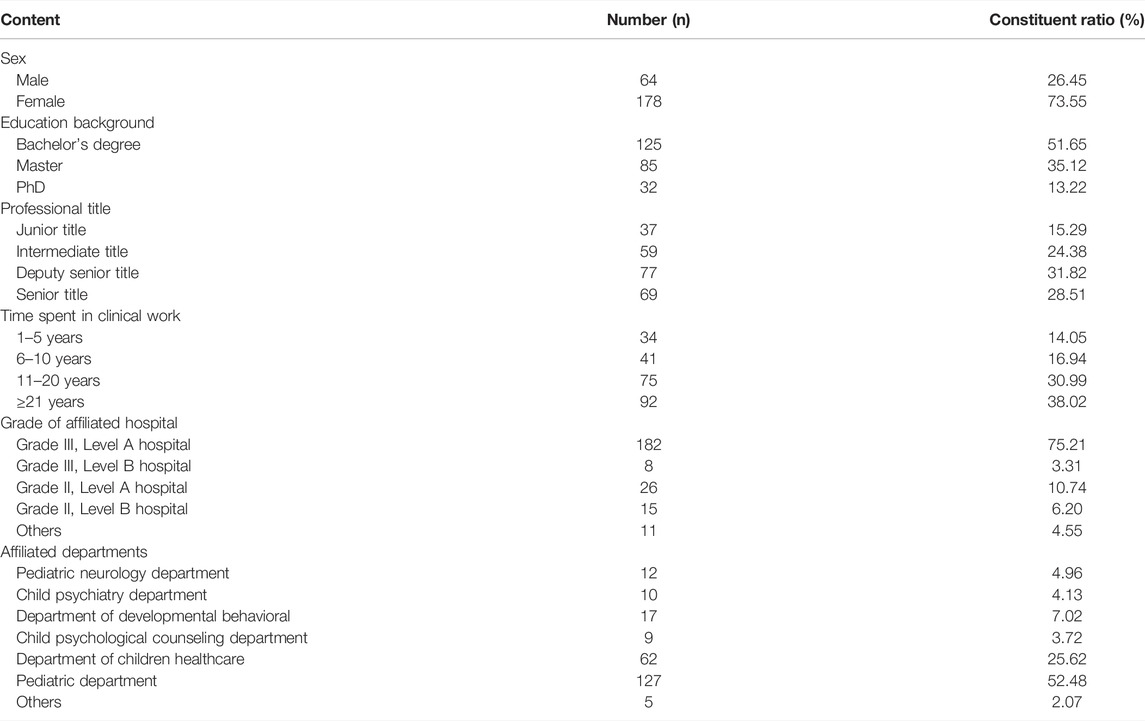
TABLE 1. Demographic information of pediatricians (N = 242).
The most common methods for evaluating tics used by pediatricians were observation of tic symptoms (4.55 points) and reference to past medical history (4.39 points), followed by the tic comorbidities scale (3.96 points), functional examinations (3.91 points), and the tic specificity scale (3.89 points). Most common treatment goals were improving overall function (4.42 points), reducing tic frequency (4.39 points), alleviating comorbidities (4.30 points), and eliminating tics (3.98 points). The most commonly used treatment tactic reported was providing strategies to help patients manage tics (4.39 points), followed by oral or written education of parents (4.33 points), drug treatment (4.13 points), and surgery (2.16 points; Table 2).

TABLE 2. Evaluation methods, treatment goals, and treatment strategies of tic (N = 242).
Preferred treatment methods for patients without comorbidities were psycho-behavioral therapy (86.36%, 209/242), educational interventions (73.97%, 179/242), and drug therapy (68.18%, 165/242). For children with TD and comorbidities, the commonly used treatment methods were drug therapy (89.26%, 216/242), psycho-behavioral therapy (85.12%, 206/242), and educational interventions (71.49%, 173/242).
For patients without comorbidities, the first-line drugs were tiapride (60.74%), clonidine (32.64%), haloperidol (25.62%), aripiprazole (16.53%), and sulpiride (12.40%). For patients with TD and attention-deficit/hyperactivity disorder, the preferred drugs were tiapride (50.83%), clonidine (32.64%), haloperidol (25.21%), Aatomoxetine (25.21%), and aripiprazole (21.49%; Table 3).
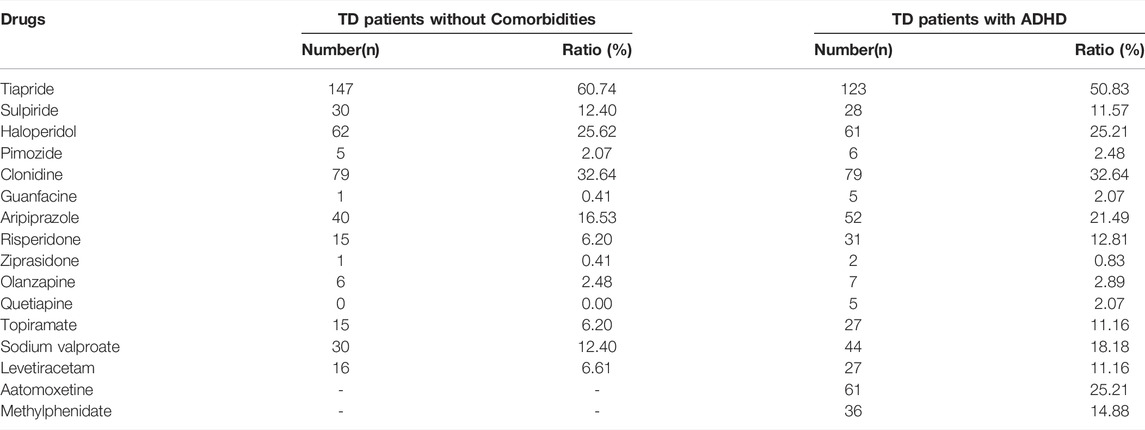
TABLE 3. Preferred drugs during treatment (N = 242).
When selecting therapeutic drugs, physicians cited the following factors as priority considerations: clinical guideline recommendations (4.55 points), better clinical efficacy (4.44 points), fewer adverse drug reactions (4.38 points), sufficient clinical evidence (4.24 points), convenient dosage forms (4.11 points), and better patient adherence (4.10 points; Table 4).
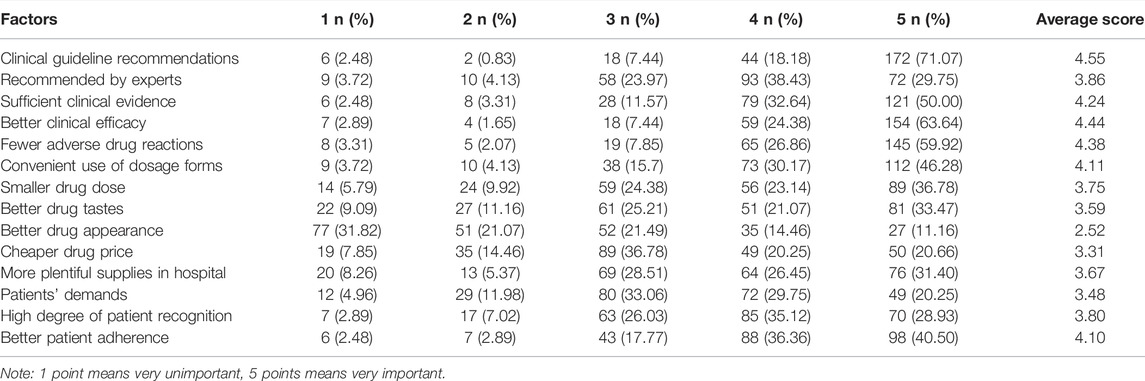
TABLE 4. Considerations of choosing in selecting drugs (N = 242).
A total of 621 questionnaires were collected, of which 610 contained complete responses (effective rate: 98.2%). Three quarters (77.90%, 475/610) of patients with TD were male. Patient age ranged from 2.20 to 15.98 years (mean: 7.86 ± 2.38 years). The mean course of TD disease was 1.44 ± 1.48 years, and 26.10% (159/610) of the patients had comorbidities. Disease types were transient TD (322/610, 52.80%), chronic TD (27.20%, 166/610), other (11.80%, 72/610), and Tourette syndrome (8.20%, 50/610).
More than half of the guardians had learned about TD through medical staff (53.60%, 327/610) and self-education (52.30%, 319/610). Most guardians (81.50%) thought that TD was a neuropsychiatric disease, while 5.10% (31/610) thought that TD was not a disease. More than 80% of the guardians believed that the cause of TD was neurotransmitter imbalance. The factors that guardians thought would aggravate tic symptoms were stress (81.10%, 495/610), shock (72.30%, 441/610), being reminded (51.60%, 315/610), fatigue (49.30%, 301/610), concentration (20.20%, 123/610), infections (1.30%, 8/610), colds (0.80%, 5/610), and watching television or using electronic devices (0.80%, 5/610). As for common treatments for TD, most guardians were aware of drug therapy (89%, 543/610) and psycho-behavioral therapy (78.20%, 477/610), but fewer knew about educational interventions (29.30%, 179/610), physical therapy (19.50%, 119/610), or surgery (1.50%, 9/610). More than half of the guardians believed that TD treatment lasted 6–12 months (Table 5).
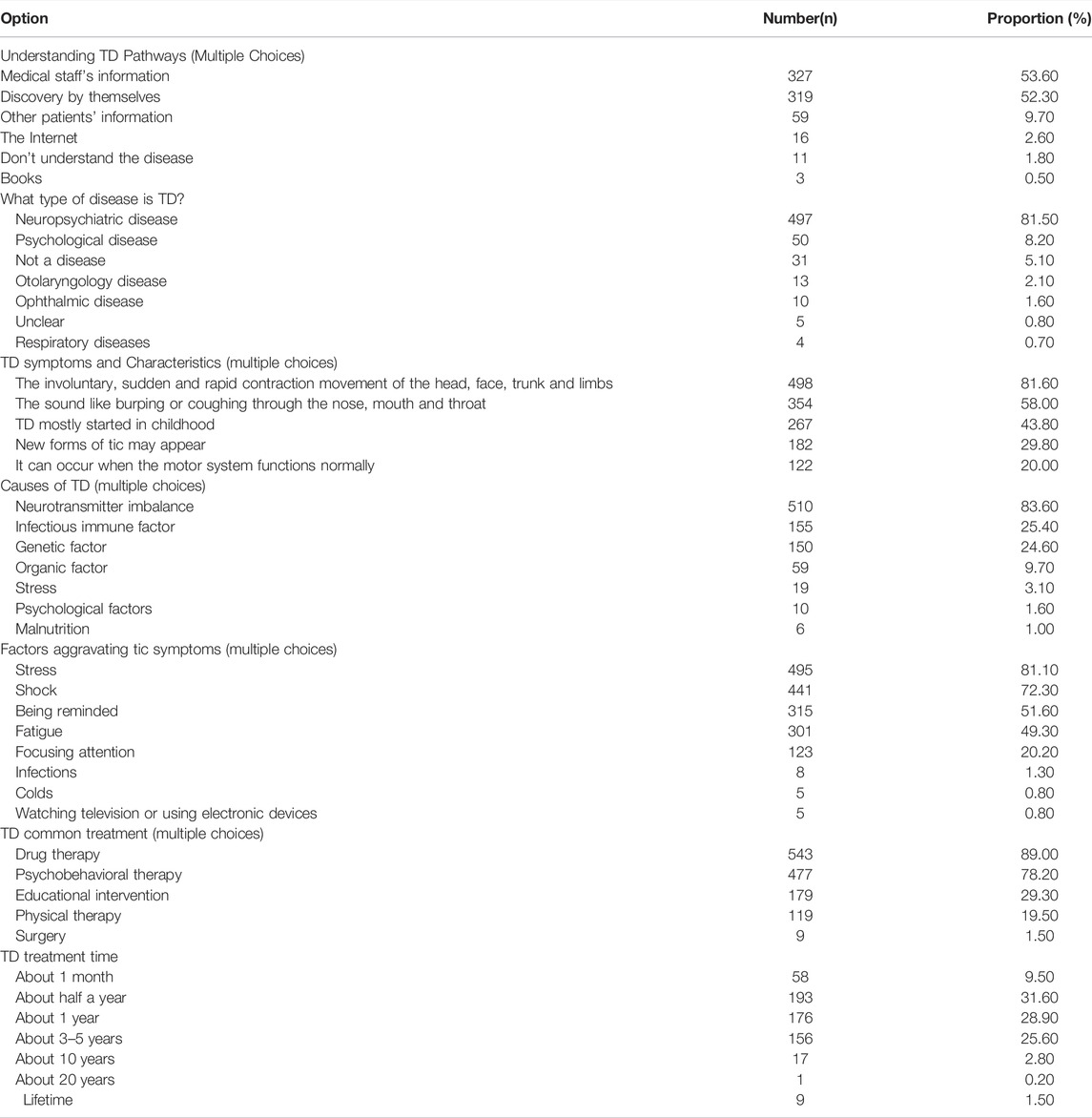
TABLE 5. Guardian’s cognition of TD (N = 610).
Only 14.10% (86/610) of patients had received medical treatment immediately after the first onset of tics, and more than half of patients first received medical treatment at a neurology department (62.10%, 379/610). Only 51.50% (314/610) of the guardians participated in medication choices: 38.90% (237/610) of the guardians had expressed their medication preferences to physicians, and 66.40% (405/610) of the guardians took their children’s medication preference into consideration. In terms of medication behavior, 67.40% (411/610) of guardians thought that medication should be taken on time and at a regular dose, 66.70% (407/610) of the guardians immediately consulted medical staff when they observed new symptoms, and 23.60% (144/610) of the guardians thought that drug use should be discontinued or reduced when symptoms were alleviated. Moreover, 9.80% (60/610) thought that medication was unnecessary because they could manage the disorder themselves, and 2.30% (14/610) thought that medication was only necessary at the onset of tics (Table 6).

TABLE 6. Guardian’s medical behavior and medication choices (N = 610).
When selecting medications, guardians placed emphasis on drugs with fewer adverse reactions (4.52 points), recommendations from physicians (4.44 points), better clinical efficacy (4.29 points), lower drug doses (4.27 points), more convenient dosage forms (4.01 points), and sufficient supplies at the hospital (3.95 points; Table 7).
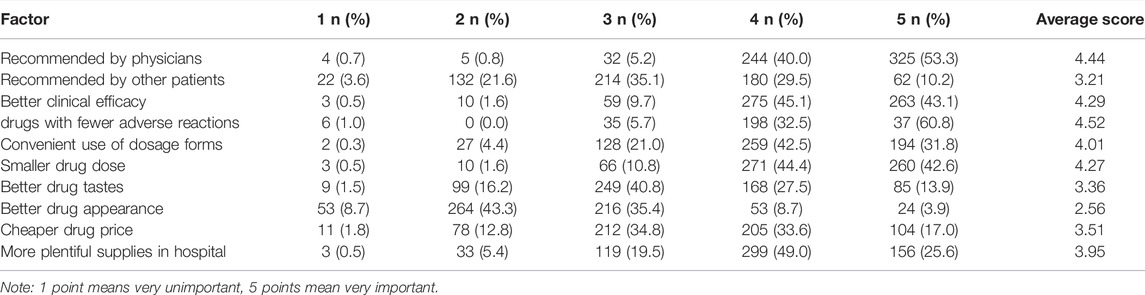
TABLE 7. Factors to consider in the medication choices of the patient’s guardian (N = 610).
The majority of physicians we polled thought that the most important treatment goals for patients with TD were to improve their overall function, reduce the frequency of tics, and control comorbidities. The most important treatment strategies include the provision of effective strategies to manage TD, oral or written education of both patients and guardians, and medication. Psycho-behavioral therapy, educational interventions, and medication are the main treatment methods. The first-line drugs include selective D2 dopamine receptor antagonists (e.g., tiapride), α-adrenergic agonists (e.g., clonidine), and antipsychotics (haloperidol and aripiprazole). Clinical guidelines, better clinical efficacy, fewer adverse drug reactions, sufficient clinical evidence, convenient dosage forms, and better patient adherence are the important factors influencing the medication choices of pediatricians. Haloperidol was used for patients with severe tics, which was recommended as a second-line drug in Chinese guideline (Liu et al., 2020), and weak recommendations are made for the use of haloperidol in Canadian guideline (Pringsheim et al., 2012), doctors also prescribed trihexyphenidyl to reduce extrapyramidal reactions caused by haloperidol in China. Chinese pediatricians’ drug choices for treating TD generally follow clinical recommendations (Pringsheim et al., 2012; Pringsheim et al., 2019; Liu et al., 2020), but they do not fully consider guardian preferences and medication prices when selecting drugs. This may reflect the heavy workload of physicians and the short time allotted to each patient visit, precluding in-depth communications between physicians and patients or guardians, further improvements and optimizations are required in future medical practice. Tiapride is not a very common medicine in western countries, but it was recommended as a first-line drug for TD in Chinese guideline (Liu et al., 2020), adequate clinical research evidence showed that the drug is effective and safe, and it is also very cheap in China, so it is widely used.
We found that guardians had a poor understanding of the disease, especially its classifications, symptoms, and characteristics, factors aggravating tic symptoms, and the length of treatment. In addition, the guardians were not sufficiently aware of educational interventions, physical therapy, or surgical options, and some guardians even misunderstood treatment needs. Because of the guardians’ poor understanding of TD, some patients did not receive timely medical attention when needed, delaying treatment. Therefore, more effective education should be provided to patients and their guardians to enhance their cognition of TD. Moreover, some guardians did not understand the nature of the drug therapy, believing that medication could be discontinued or the dose reduced when symptoms were alleviated; some even believed that medication was only required at the onset of tic. In terms of medication choices, both guardians and clinicians preferred drugs with fewer adverse effects and better clinical efficacy, but guardians also considered factors such as smaller drug dose, more convenient dosage forms, and a steady and convenient supply. However, guardians reported that most physicians did not consider patients’ treatment needs, underscoring the importance of physicians listening to guardians’ input when making medication choices.
A Japanese survey from 2019 (Yu et al., 2019) found that the most important factor considered in the decision to begin pharmacotherapy in children with TD was functional impairment caused by tic symptoms, and this finding is consistent with ours. Aripiprazole and risperidone were the first- and second-line medications for TD, as α-adrenergic agonists are seldom prescribed in Japan, although they are widely used in China. This difference in clinical practice may result from the fast-acting receptor agonist clonidine being the only α-adrenergic receptor agonist officially accepted for treatment of hypertension in Japan. In addition, Aatomoxetine was a first-line drug because the use of methylphenidate is restricted in Japan.
A cross-sectional study of TD medications prescribed in Korea between 2009 and 2016 (Choi et al., 2019) reported that aripiprazole was the most commonly prescribed drug, the use of risperidone was declining, and the number of prescriptions written increased over time. Other commonly used drugs were benzatropine and haloperidol. The widespread use of aripiprazole might be related to the mounting body of evidence that indicates that aripiprazole has good efficacy and tolerability. In China, physicians’ drug choices are similar, with the exception of benzatropine and haloperidol, which are rarely used because of the high incidence of adverse drug reactions.
Lu et al. (2020) recently surveyed 110 pediatricians in China on drug treatment of patients with newly diagnosed TD and comorbidities. Their findings were consistent with ours, although their sample was smaller and they did not report factors that influenced medication choices. Geng et al. (2016) surveyed 57 guardians on their knowledge of TD; 71.90% believed that TD was a disease, but 73.70% still adopted inappropriate measures when tics occurred, indicating that guardians had a poor understanding of TD, similar to our findings. However, the study did not investigate patients’ medication needs or factors in medication choices.
Our study has some limitations. First, we did not sample at random, but we did include physicians from 24 provinces and Hong Kong, Macao, and Taiwan. Guardians were recruited from the largest women and children’s hospital in southwestern China, so the results were of good representativeness. Second, we used a cross-sectional design to identify the factors influencing medication choices, so causal inference could not be made. Third, patient medications were reported by guardians. Although this can reflect patients’ medication needs to a certain extent, some information bias was inevitable. Fourth, this study is from a specific region, so the extrapolation has certain limitations. Future research should overcome these limitations.
We found that pediatricians in China typically follow clinical guidelines in selecting medications for TD but seldom consider guardian preferences, highlighting a gap in optimizing treatment. Moreover, patient guardians lack sufficient knowledge of TD and medication choices, requiring more physician-initiated dialogue.
The original contributions presented in the study are included in the article/Supplementary Material, and further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Office of Research Ethics Committees of West China Women’s and Children’s Hospital. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
CY and YY: designed the review, collected data, carried out analysis and interpretation of the data and wrote this study. LlZ and LiZ: designed the review, collected data, checked the data and wrote the study.
This study was funded by Sichuan Health and Wellness Committee: Evidence-based construction of clinical drug route for children with tic disorder (18PJ528).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Liwen Bianji (Edanz) (www.liwenbianji.cn/) for editing the English text of a draft of this manuscript.
TD, tic disorder.
Choi, S., Lee, H., Song, D. H., and Cheon, K. A. (2019). Population-Based Epidemiology of Pediatric Patients with Treated Tic Disorders from Real-World Evidence in Korea. J. Child. Adolesc. Psychopharmacol. 29 (10), 764–772. doi:10.1089/cap.2019.0050
Conelea, C. A., Woods, D. W., Zinner, S. H., Budman, C., Murphy, T., Scahill, L. D., et al. (2011). Exploring the Impact of Chronic Tic Disorders on Youth: Results from the Tourette Syndrome Impact Survey. Child. Psychiatry Hum. Dev. 42 (2), 219–242. doi:10.1007/s10578-010-0211-4
Cothros, N., Martino, D., McMorris, C., Stewart, D., Tehrani, A., and Pringsheim, T. (2019). Prescriptions for Alpha Agonists and Antipsychotics in Children and Youth with Tic Disorders: A Pharmacoepidemiologic Study. Tremor Other Hyperkinet Mov (N Y) 9, 9. doi:10.7916/tohm.v0.645
Eddy, C. M., Cavanna, A. E., Gulisano, M., Agodi, A., Barchitta, M., Calì, P., et al. (2011). Clinical Correlates of Quality of Life in Tourette Syndrome. Mov Disord. 26 (4), 735–738. doi:10.1002/mds.23434
Evans, J., Seri, S., and Cavanna, A. E. (2016). The effects of Gilles de la Tourette syndrome and other chronic tic disorders on quality of life across the lifespan: a systematic review. Eur. Child. Adolesc. Psychiatry 25 (9), 939–948. doi:10.1007/s00787-016-0823-8
Geng, Ni., Wang, M. F., and Li, J. Q. (2016). Research on Parents' Misunderstanding of Coping with Tic Disorder and its Influence [J]. J. Nurs. Educ. 31 (08), 688–690.
Hirschtritt, M. E., Lee, P. C., Pauls, D. L., Dion, Y., Grados, M. A., Illmann, C., et al. (2015). Lifetime Prevalence, Age of Risk, and Genetic Relationships of Comorbid Psychiatric Disorders in Tourette Syndrome. JAMA Psychiatry 72, 325–333. doi:10.1001/jamapsychiatry.2014.2650
Knight, T., Steeves, T., Day, L., Lowerison, M., Jette, N., and Pringsheim, T. (2012). Prevalence of Tic Disorders: A Systematic Review and Meta-Analysis. Pediatr. Neurol. 47 (2), 77–90. doi:10.1016/j.pediatrneurol.2012.05.002
Kurlan, R., Como, P. G., Miller, B., Palumbo, D., Deeley, C., Andresen, E. M., et al. (2002). The Behavioral Spectrum of Tic Disorders: a Community-Based Study. Neurology 59, 414–420. doi:10.1212/wnl.59.3.414
Liu, Z. S., Cui, Y. H., Sun, D., Lu, Q., Jiang, Y. W., Jiang, L., et al. (2020). Current Status, Diagnosis, and Treatment Recommendation for Tic Disorders in China. Front. Psychiatry 11, 774. doi:10.3389/fpsyt.2020.00774
Lu, Q., Cui, Y. H., Liu, Z. S., Sun, D., Fang, F., Peng, J., et al. (2020). Investigation and Analysis of Newly Diagnosed Tic Disorder and its Comorbidities in Children. Chin. J. Pediatr. 58 (11), 887–892.
Pringsheim, T., Doja, A., Gorman, D., McKinlay, D., Day, L., Billinghurst, L., et al. (2012). Canadian Guidelines for the Evidence-Based Treatment of Tic Disorders: Pharmacotherapy. Can. J. Psychiatry 57 (3), 133–143. doi:10.1177/070674371205700302
Pringsheim, T., Okun, M. S., Müller-Vahl, K., Martino, D., Jankovic, J., Cavanna, A. E., et al. (2019). Practice Guideline Recommendations Summary: Treatment of Tics in People with Tourette Syndrome and Chronic Tic Disorders. Neurology 92 (19), 896–906. doi:10.1212/WNL.0000000000007466
Roessner, V., Plessen, K. J,, Plessen, K. J., Rothenberger, A., Ludolph, A. G., Rizzo, R., et al. (2011). ESSTS Guidelines GroupEuropean Clinical Guidelines for Tourette Syndrome and Other Tic Disorders. Part II: Pharmacological Treatment. Eur. Child. Adolesc. Psychiatry 20 (4), 173–196. doi:10.1007/s00787-011-0163-7
Waldon, K., Hill, J., Termine, C., Balottin, U., and Cavanna, A. E. (2013). Trials of Pharmacological Interventions for Tourette Syndrome: a Systematic Review. Behav. Neurol. 26, 265–273. doi:10.3233/BEN-2012-120269
Yang, C., Cheng, X., Zhang, Q., Yu, D., Li, J., and Zhang, L. (2020). Interventions for Tic Disorders: An Updated Overview of Systematic Reviews and Meta Analyses. Psychiatry Res. 287, 112905. doi:10.1016/j.psychres.2020.112905
Yantg, C., Zhang, L., Zhu, P., Zhu, C., and Guo, Q. (2016). The Prevalence of Tic Disorders for Children in China: A Systematic Review and Meta-Analysis. Medicine (Baltimore) 95 (30), e4354. doi:10.1097/MD.0000000000004354
Keywords: pediatricians, aripiprazole, tiapride, doctors, dose
Citation: Yang C, Yang Y, Zhang L and Zhao L (2022) Medication Choices in Children With Tic Disorders in Mainland China, Macao, Hong Kong, and Taiwan: Perspectives of Guardians and Physicians. Front. Pharmacol. 13:852414. doi: 10.3389/fphar.2022.852414
Received: 11 January 2022; Accepted: 31 March 2022;
Published: 03 May 2022.
Edited by:
Elena Ramírez, University Hospital La Paz, SpainReviewed by:
Soumitra Das, NorthWestern Mental health, AustraliaCopyright © 2022 Yang, Yang, Zhang and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lingli Zhang, zhlingli@sina.com; Li Zhao, zhaoli@scu.edu.cn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.