 Koki Kato1
Koki Kato1 Tomohiro Mizuno1*Takenao Koseki1
Tomohiro Mizuno1*Takenao Koseki1 Yoshimasa Ito2Kazuo Takahashi3
Yoshimasa Ito2Kazuo Takahashi3 Naotake Tsuboi2Shigeki Yamada1
Naotake Tsuboi2Shigeki Yamada1- 1Department of Clinical Pharmacy, Fujita Health University School of Medicine, Toyoake, Japan
- 2Department of Nephrology, Fujita Health University School of Medicine, Toyoake, Japan
- 3Department of Biomedical Molecular Sciences, Fujita Health University School of Medicine, Toyoake, Japan
Information on immune checkpoint inhibitor-induced vasculitides is limited, and predictors for this condition have not been identified. Therefore, we have examined the frequency of immune checkpoint inhibitor-induced vasculitides by analyzing the data recorded in the Japanese Adverse Drug Event Report database. Data from April 2004 to March 2020 were extracted, and vasculitides as an immune-related adverse event was defined according to the 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Adverse event signals were recognized as significant when the reporting odds ratio estimates and lower limits of the corresponding 95% confidence intervals exceeded 1. The use of nivolumab showed a significant signal for vasculitides. Furthermore, significant signals of polymyalgia rheumatica were found when the patients were treated with nivolumab, pembrolizumab, and ipilimumab. In addition, the frequencies of nivolumab- and pembrolizumab-induced polymyalgia rheumatica were higher in patients aged ≥70 years and female patients, respectively. Polymyalgia rheumatica was reported in 38 patients treated with nivolumab; 31 (82%) of these were either in recovery or in remission. Further, polymyalgia rheumatica was reported in 17 patients treated with pembrolizumab; 13 (76%) of these were in recovery or remission, while three (18%) were not. Polymyalgia rheumatica was reported in 12 patients treated with ipilimumab; seven (58%) of these were in recovery or remission. Our study highlights that careful monitoring for the symptom of PMR (e.g., bilateral pain in shoulder and pelvic girdles) is required when the patients are aged >70 years and have been treated with nivolumab and when the patients are women and have been treated with pembrolizumab.
Introduction
Immune checkpoint inhibitors (ICPIs) are used for chemotherapy in various types of cancers (Hodi et al., 2010; Brahmer et al., 2012; Borghaei et al., 2015; Robert et al., 2015b; Motzer et al., 2015). The pharmacological mechanisms of ICPIs include blockade of programmed cell death 1 (PD-1)/PD ligand 1 (PD-L1) signaling (Brahmer et al., 2010; Herbst et al., 2014) and cytotoxic T-lymphocyte antigen 4 (CTLA-4) signaling (Melero et al., 2007) to activate T cell-mediated antitumor immunity. ICPIs induce immune-related adverse events (irAEs) such as skin disorders (Robert et al., 2015a), gastrointestinal disorders (Robert et al., 2015b), thyroid dysfunction (Robert et al., 2015b; Tie et al., 2017), type 1 diabetes mellitus (DM) (Robert et al., 2015b), lupus nephritis (Fadel et al., 2009), and vasculitides (Daxini et al., 2018). These irAEs are effectively treated by temporary administration of glucocorticoids or additional immunosuppressants in severe cases (Postow et al., 2018; Mamlouk et al., 2020). In addition, an anti-PD-1 therapy can improve the prognosis of patients with severe irAEs induced by ipilimumab (Brunot et al., 2020). However, these therapeutic interventions may decrease the efficacy of chemotherapy, and the use of immunosuppressive agents can lead to some irAEs (Postow et al., 2018).
Identification of the risk factors of irAEs can facilitate their prevention after ICPI chemotherapy. Changes in the composition of the gastrointestinal microflora (Sivan et al., 2015; Vétizou et al., 2015; Chaput et al., 2017), a high body mass index (Guzman-Prado et al., 2021), female sex, and a history of melanoma (Takada et al., 2020) have been identified as risk factors of irAEs. As the frequency of vasculitides is lower than that of other irAEs, identifying the predictors of vasculitides requires analyses based on large-scale databases. The Japanese Adverse Drug Event Report (JADER) database is an open-access repository of adverse drug events (ADEs) that has been maintained by the Pharmaceuticals and Medical Devices Agency since 2012. The JADER database is used to identify predictors of irAEs. For instance, female sex and a history of melanoma have been identified as the risk factors of type 1 diabetes mellitus after ICPI chemotherapy using this database (Takada et al., 2020).
Vasculitides are a group of heterogeneous autoimmune inflammatory diseases that often result in organ injuries. Because the frequency of vasculitides induced by ICPIs is lower than that of other irAEs, they have not been described extensively before (Daxini et al., 2018). Although the previous report suggested that pre-existed giant cell arteritis (GCA) was associated with irAEs (Leonardi et al., 2018; Klavdianou et al., 2021), the information on vasculitides is limited and the predictors of ICPI-induced vasculitides have not been identified. In the present study, we aimed to identify these predictors using the JADER database and to broaden our knowledge of the underlying risk factors and frequency of ICPI-induced vasculitides.
Materials and Methods
Data Source and Study Design
Data deposited between April 2004 and March 2020 were extracted from the JADER database. The database comprises three data tables, namely DEMO, DRUG, and REAC. The DEMO file contains data on parameters such as sex and age; the DRUG file contains data on the generic name and route or dates of administration; and the REAC file contains data on the ADEs, their date of occurrence, and outcomes (recovery, remission, no recovery, death, after-effects, and unknown). Based on their contribution to the ADEs, the medications administered were classified into three categories, namely “suspected medicine,” “concomitant medicine,” and “interaction.” The “suspected medicine” category was defined as having caused the ADEs in the present study. Duplicate data from the DRUG and REAC tables were removed, and the DEMO table was linked to the DRUG and REAC tables by using each case identified in the data tables.
Cases without data on the sex or age in the DEMO table were excluded from the dataset. To analyze the association with patients classified in 10-years age intervals, we defined “older adults” as those in their 70, 80, 90, and 100 s according to a previous report (Sugawara et al., 2019). Nivolumab, pembrolizumab, ipilimumab, atezolizumab, durvalumab, and avelumab were selected as the suspected drugs for vasculitides.
Definition of Patients With Cancer
The primary disease in the HIST tables extracted from the JADER database was defined based on the preferred terms (PTs) in the Medical Dictionary for Regulatory Activities (MedDRA) version 23.1. MedDRA is an internationally used set of terms relating to medical conditions. Essentially, these PTs define the medical condition of the patient. Cancer as primary disease was defined by the PTs after removing duplicate data (see Supplementary Table S1). Cancers that appeared as primary diseases but were not included in Supplementary Table S1 were classified as others/uncertain.
Definition of Immune Checkpoint Inhibitors and Vasculitides as irAEs
The ADEs in the REAC table were coded according to the PTs in the MedDRA. Vasculitides as irAEs were defined according to the recommendations of the 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides (Sunderkötter et al., 2018). The PTs for vasculitides are listed in Table 1. When there were multiple occurrences of different vasculitides in same patients, we counted the each events. We counted the onset day of vasculitides since the first exposure of ICPIs.
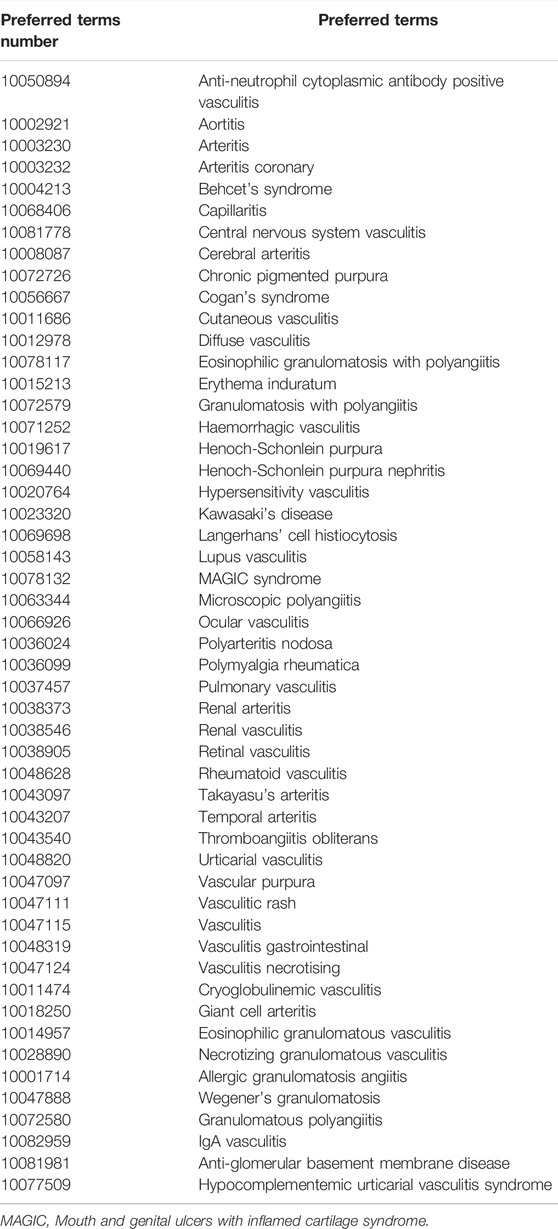
TABLE 1. Preferred terms of vasculitides.
Statistical Analysis
The reporting odds ratio (ROR), which evaluates the AE signals, was calculated using the following formula (Sugawara et al., 2019):
where a represents number of cases with an ADE related to the use of the suspected drugs; b, number of cases with an ADE related to the use of all other drug; c, number of cases with all other ADEs related to the use of the suspected drug; and d, number of cases with all other ADEs related to the use of all other drugs.
AE signals were considered significant when the ROR estimates and the lower limits of the corresponding 95% confidence interval (CI) exceeded 1. RORs were calculated using Excel for Microsoft 365 (Microsoft Corporation, Redmond, WA, United States).
As polymyalgia rheumatica (PMR) was the most frequent in this study, a chi-square test as univariate analysis and multiple logistic regression analysis were performed to identify the predictors of PMR in patients treated with nivolumab, pembrolizumab, and ipilimumab. Sex and age (≥70 years) were used as variables in the univariate and multivariate analyses. The Hosmer–Lemeshow statistical test was used for testing the goodness of fit for the logistic regression models. A two-sided p-value lower than 0.05 was considered statistically significant. The chi-square test, Mann-Whitney U test, multiple logistic regression analysis, and Hosmer–Lemeshow statistical test were performed using SPSS version 22.0 (SPSS, Inc., Chicago, IL, United States).
Ethics Approval and Consent to Participate
As this study involved an open-access database, ethics approval and consent to participate were not required.
Results
Patient Characteristics and the Reporting Odds Ratio Estimates
A total of 573,316 cases were included in the dataset table (Figure 1). Of these, 8,705, 5,202, 2,362, 1,039, 876, and 17 cases had the use of nivolumab, pembrolizumab, ipilimumab, atezolizumab, durvalumab, and avelumab, respectively (Table 2). Characteritics of patients with vasculitides and PMR were shown in Table 3 and Table 4, respectively. The nivolumab, pembrolizumab, atezolizumab, and durvalumab groups predominantly included patients with lung cancer, whereas the ipilimumab group mostly included patients with melanoma (Table 2). ADE signals of vasculitides were detected in the nivolumab, pembrolizumab, ipilimumab, atezolizumab, and durvalumab groups. The use of nivolumab showed a significant signal for vasculitides [ROR (95% CI): 1.498 (1.12–2.00)] (Table 5). The pembrolizumab, ipilimumab, atezolizumab, and durvalumab groups also showed ADE signals for vasculitides, although these were not significant (Table 5). Moreover, the avelumab group showed no ADE signals for vasculitides because of the small sample size.
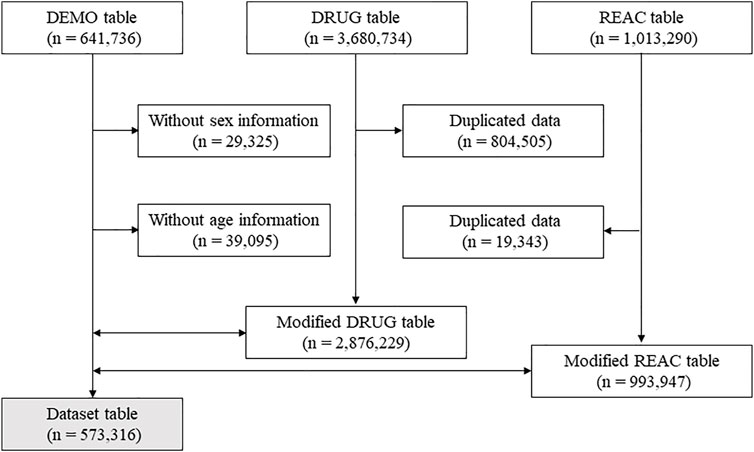
FIGURE 1. Flow diagram of the study. Dotted arrow and double arrow show data exclusion and combination, respectively.
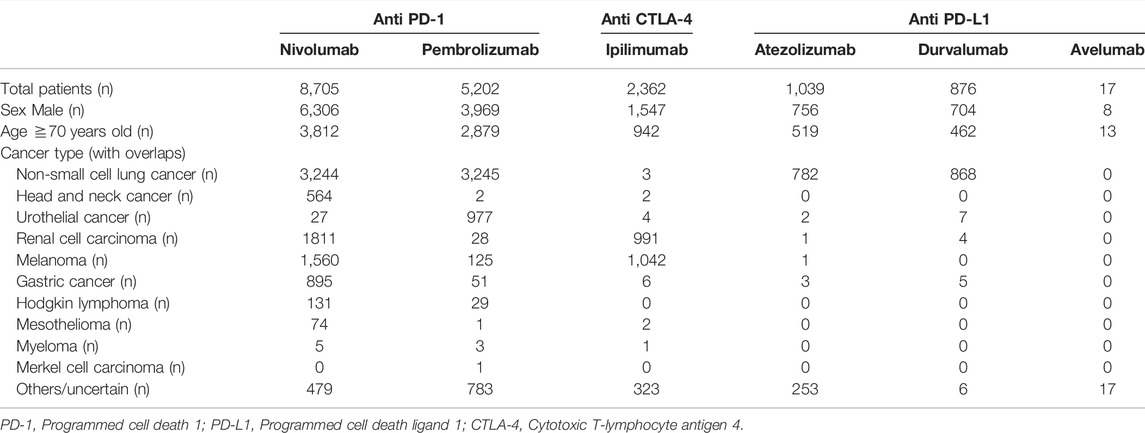
TABLE 2. Patient characteristics.

TABLE 3. Characteristics of patient with vasculitides.
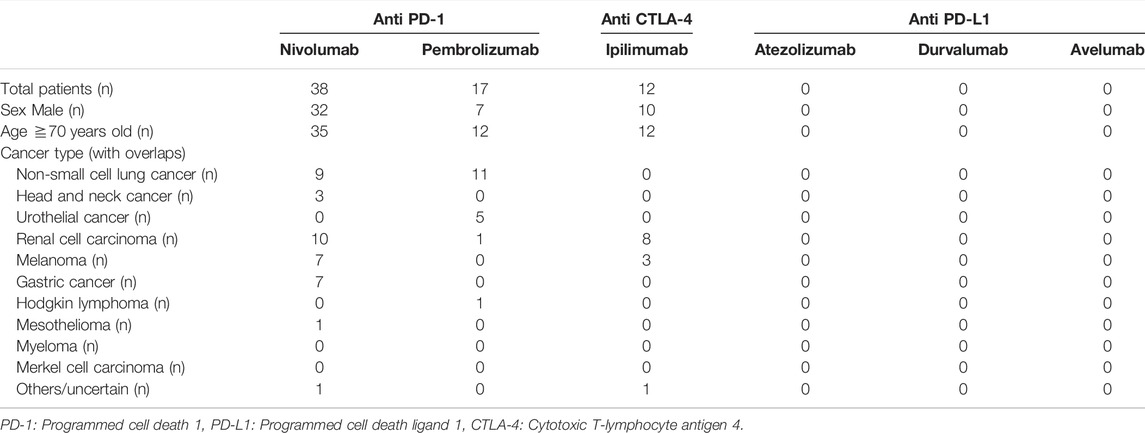
TABLE 4. Characteristics of patient with polymyalgia rheumatic.
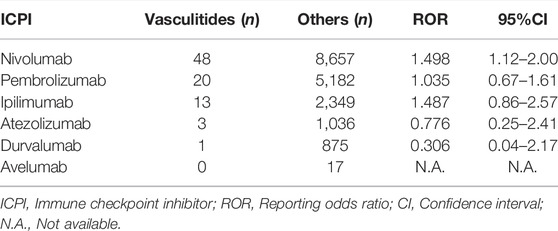
TABLE 5. Reporting odds ratios for vasculitides.
The number of cases with PMR was the highest among all cases with ICPI-induced vasculitides (PMR: 67 cases, vasculitis: 8 cases, Henoch–Schönlein purpura: 3 cases, temporal arteritis: 2 cases, anti-neutrophil cytoplasmic antibody-positive vasculitis: 1 case, aortitis: 1 case, eosinophilic granulomatosis with polyangiitis: 1 case, Henoch–Schönlein purpura nephritis: 1 case, and retinal vasculitis: 1 case). To avoid the overlooks of PMR cases associated with vasculitides in spontaneous reports, the JADER database classifies PMR cases to the category of vasculitides. Therefore, these cases were detected as vasculitides-related PMR. Although physicians reported all cases to JADER database according to classification of MedDRA, some cases could not be categorized to typical vasculitides. These cases were detected as “vasculitis.” The use of nivolumab, pembrolizumab, and ipilimumab showed significant signals for PMR [ROR (95% CI); nivolumab: 28.78 (19.64–42.17), pembrolizumab: 17.40 (10.43–29.06), and ipilimumab: 26.03 (14.33–47.27)]. There were no reports of PMR in patients treated with atezolizumab, durvalumab, and avelumab. A significant signal of retinal vasculitis after the use of pembrolizumab was also identified [ROR (95% CI): 13.65 (1.71–109.1)]. No significant signals were obtained for other vasculitides (Table 6). To evaluate whether an unknown factor have induced a variation in the occurrence of vasculitis, we compared the numbers of vasculitides from 2004 to 2013 and from 2014 to 2019. There were no significant differences between two groups (Supplementary Figure S1).
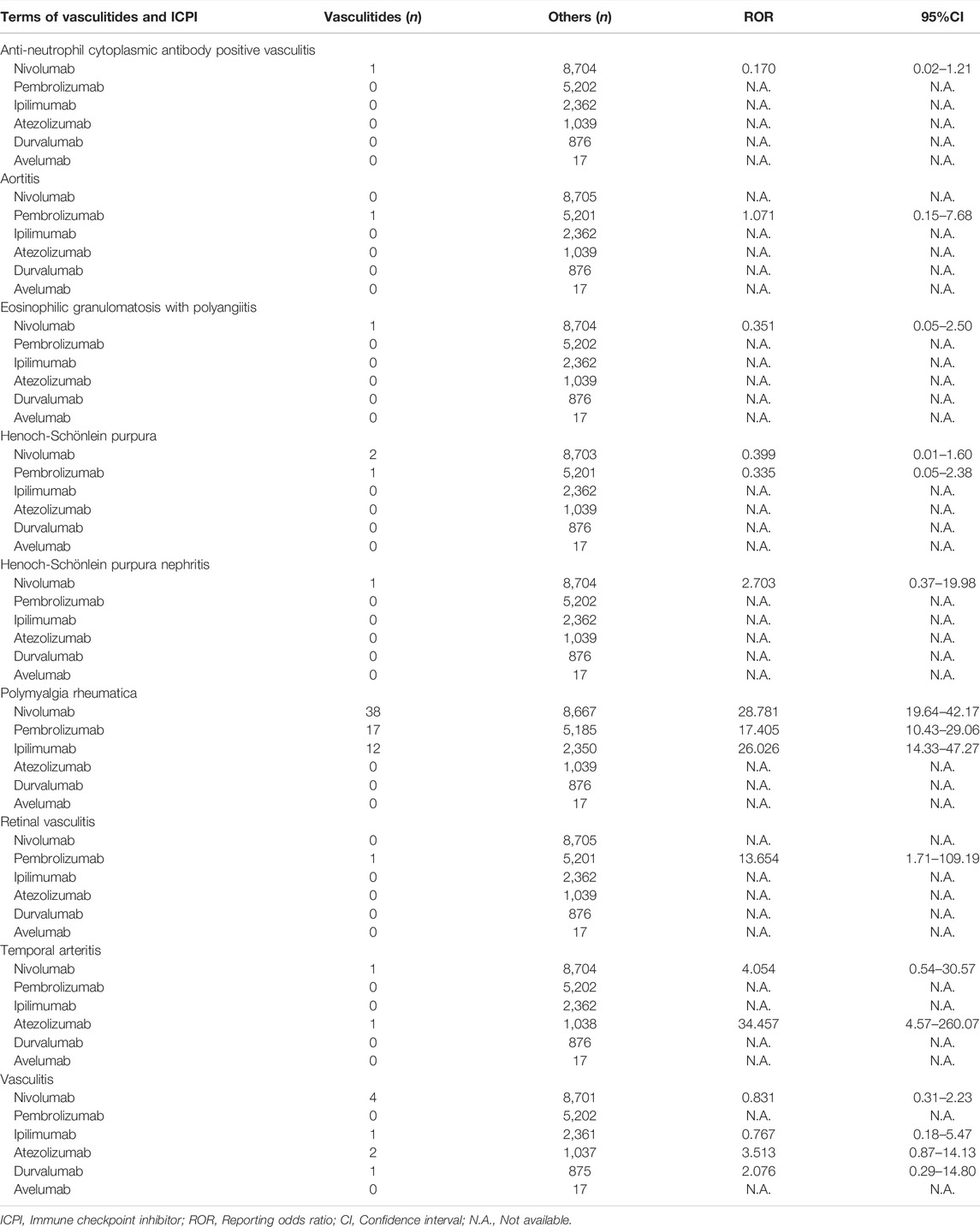
TABLE 6. Reporting odds ratios for the types of vasculitides.
Predictors of Immune Checkpoint Inhibitors-Induced Polymyalgia Rheumatica
Univariate analysis revealed that the frequency of nivolumab-induced PMR was significantly higher in patients aged ≥70 years (older adults) than in patients aged <70 years [OR (95% CI): 15.11 (4.642–49.15), p < 0.001]. The frequency of pembrolizumab-induced PMR was significantly lower in male patients than in female patients [OR (95% CI): 0.216 (0.082–0.569), p = 0.001]. Multivariate analysis confirmed the results of the univariate analysis. The frequency of nivolumab-induced PMR was significantly higher in older adults (aged ≥70 years) than in those aged <70 years [OR (95% CI): 15.02 (4.615–48.87), p < 0.001; Hosmer–Lemeshow test, p = 0.711], while the frequency of pembrolizumab-induced PMR was significantly lower in male patients than in female patients [OR (95% CI): 0.214 (0.081–0.564), p = 0.002; Hosmer–Lemeshow test, p = 0.548] (Table 7). Because only one case of retinal vasculitis was available, multivariate analysis could not be performed for all variables.
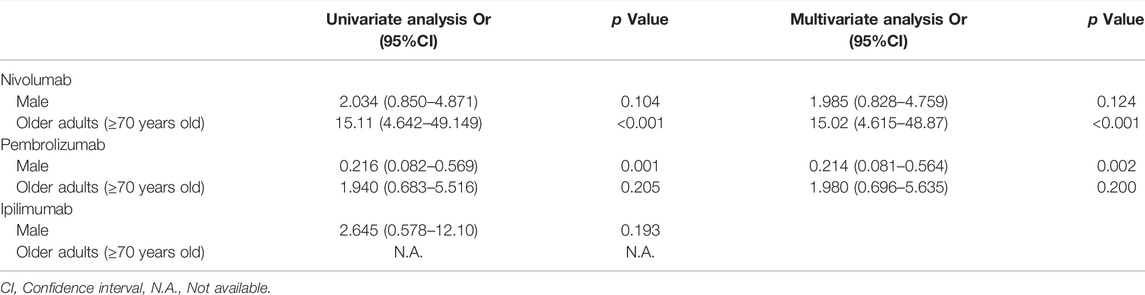
TABLE 7. Univariate and multivariate analysis for predictors of ICPI-induced polymyalgia rheumatica.
Time of Occurrence and Outcomes of Polymyalgia Rheumatica
PMR was reported in 38 patients treated with nivolumab; among these, 12 (32%) experienced the onset within 60 days from the exposure to nivolumab. The date of occurrence was unknown for the remaining 16 (42%) cases. In addition, 31 (82%) cases were in recovery or remission (Table 8). PMR was also reported in 17 patients treated with pembrolizumab; six (35%) of these experienced the onset within 60 days from the exposure to pembrolizumab, whereas two (12%) experienced the onset at over 121 days after the exposure. The date of occurrence was unknown in nine (53%) cases. Furthermore, 13 (76%) cases were in recovery or remission, while three (18%) were not (Table 8). Finally, PMR was reported in 12 patients treated with ipilimumab; of these, four (33%) experienced the onset within 7 days from the exposure to ipilimumab. The date of occurrence was unknown in six (50%) cases, while seven (58%) cases were in recovery or remission (Table 8).
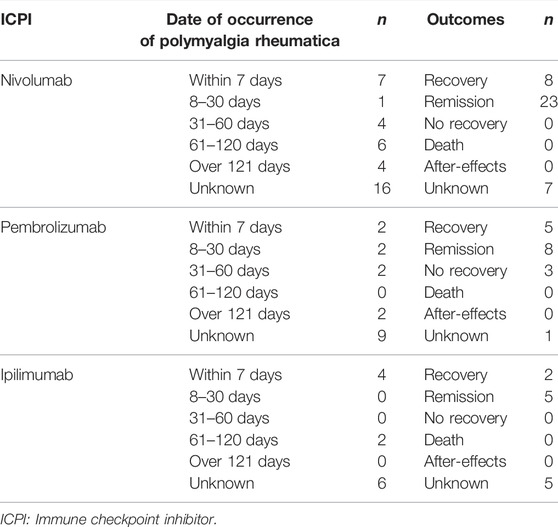
TABLE 8. Time-to-onset and outcomes of occurrence of polymyalgia rheumatica.
Discussion
The frequency of vasculitides induced by ICPIs is much lower than that of other irAEs. Although the mortality associated with vasculitides is high (Isobe et al., 2020), the mechanism underlying the development of ICPI-induced vasculitides remains elusive. Determining the underlying molecular mechanisms and identifying the predictors of ICPI-induced vasculitides may improve the prognosis of such patients. Herein, we investigated the predictors of ICPI-induced vasculitides by analyzing real-world data obtained from the JADER database. The use of nivolumab was found to increase the frequency of vasculitides, and PMR was the most frequently reported vasculitis among patients treated with nivolumab, pembrolizumab, and ipilimumab.
PMR is characterized by GCA and inflammatory symptoms, such as aching and morning stiffness in the cervical region (Salvarani et al., 2002). Prednisone treatment at a dose of 12.5–25 mg/day is typically recommended for patients with PMR (Hernández-Rodríguez et al., 2009; Dejaco et al., 2015). However, specific diagnostic markers for PMR are currently lacking, making it difficult to distinguish PMR from similar inflammatory diseases, such as myositis and rheumatoid arthritis. The European League Against Rheumatism/American College of Rheumatology guidelines state that other diagnoses should be excluded at the discretion of the physician. They recommend extensive serological tests, such as tests for anti-nuclear antibodies, anti-cytoplasmic neutrophil antibodies, and tuberculosis, to enable an accurate diagnosis (Dejaco et al., 2015). Because diagnosing PMR is a time-consuming process, withdrawal of drugs suspected to have caused it and diagnostic treatment are commenced in some cases to improve outcomes. Angelopoulou et al. (2021) reviewed clinical studies and case series and reported the frequency of ICPI-induced irAEs. The prevalence rate of musculoskeletal events was reported to be 6.13%, wherein PMR accounted for 12.12% of these events. In addition, the rate of patients who discontinued the treatment because of musculoskeletal conditions reached 19%. Therefore, to prevent discontinuation of ICPI or additional treatments (e.g., steroids and disease modifying anti-rheumatic drugs), the risk factors for musculoskeletal events, including PMR, must be identified.
PD-1 regulates Tcell-mediated autoimmune diseases, and hence, disruption of the PD-1/PD-L1 or PD-L2 axis can trigger PMR. The expression of PD-1 is low in Asian patients with rheumatoid arthritis (Kong et al., 2005; Li et al., 2014). In addition, ICPI-induced PMR has been described in some case reports (Belkhir et al., 2017; Bernier et al., 2017; Nakamagoe et al., 2017; Betrains and Blockmans, 2019; Imai et al., 2019; Lobo et al., 2020; Kita et al., 2021) and clinical reviews (Benfaremo et al., 2018; Angelopoulou et al., 2021). Our findings indicated that blockade of PD-1 or CTLA-4 increases the risk of PMR; this is in line with the reports of previous studies. Because the type of vasculitis more prevalent in patients treated with ICPIs is vaguely understood, the present study provides a new strategy for preventing irAEs in such patients. In addition, older and female patients experienced higher frequencies of nivolumab- and pembrolizumab-induced PMR, respectively. A previous report indicated that the mean age at which ICPI-associated PMR occurred was 75 years, and the frequency of PMR was higher in men than in women (Salem et al., 2018). Because the risk of PMR for each ICPI has not been determined, we could not compare the previous results with ours. However, both our study and the above-mentioned previous study suggest that the frequency of PMR is higher in older patients; further studies are needed to clarify the reasons underlying sex-based differences.
The incidence of PMA peaks at around 70 years of age, and two-thirds of the patients are women (Matteson and Dejaco, 2017). Thus, our findings suggest that the risk factors for PMR are the same as those for PMR unrelated to ICIPs. Belkhir et al. (2017) reported four cases of ICPI-induced PMR. Among these, two experienced PMR onset after treatment with nivolumab or a combination of nivolumab and ipilimumab, while one experienced onset after pembrolizumab treatment. In all three cases, the onset occurred within 120 days from the anti-PD-1 or anti-CTLA-4 therapy. In addition, all cases responded to corticosteroids (Belkhir et al., 2017). Although none of the cases experienced an onset of PMR after an anti-PD-L1 therapy, these findings support our results. In the current study, three patients with pembrolizumab-induced PMR did not recover, suggesting that patients treated with pembrolizumab are at a risk of severe PMR. Because we used databases reporting spontaneous ADEs, the detailed clinical background of these three cases was not available. In order to investigate the mortality and response rate to corticosteroids in patients with pembrolizumab-induced PMR, further clinical studies are required. The monitoring for PMR events after ICPIs therapy should be needed in patients with pre-existed PMR (Menzies et al., 2017).
The present study has some limitations. First, because the JADER database is a large spontaneous reporting system, it is subject to various biases, including under- or over-reporting and confounders caused by comorbidities (Abe et al., 2016; Hara et al., 2017; Hasegawa et al., 2017; Hosoya et al., 2017; Sugawara et al., 2019; Takada et al., 2020). Therefore, we could not elucidate whether ICPIs-induced PMR is the idiopathic form of the disease, or whether it should be considered as a new entity. This limitation has been raised in the previous report (Manzo et al., 2020). In addition, pharmacovigilance studies based solely on the JADER database could create the hypothesis for prospective studies. Second, the ADE signals of vasculitides induced by some ICPIs were weak or not detected because of the small sample size. In Japan, nivolumab was approved in 2014, whereas pembrolizumab, ipilimumab, atezolizumab, and durvalumab were approved in 2016, 2015, 2018, and 2018, respectively. As some of these drugs have been recently approved, studies to evaluate the ADE signals between the events of rare vasculitides and the usage of other ICPIs are currently scanty. Third, the characteristics used in the univariate and multivariate analyses were limited because of missing data. However, this large-scale database provided information on infrequent ADEs. Fourth, some patients with PMR have concomitant GCA; however, its incidence is around 20% (Salvarani et al., 1995). Because the Medical Dictionary for Regulatory Activities has included the term “PMR” within the category of vasculitis, we could not classify PMR as with or without GCA. However, it is possible that the physician reported cases of ICPI-induced PMR, because PMR is under the category of vasculitis in the JADER database. To eliminate this limitation, further studies using real world data are required.
In conclusion, based on the predictors of ICPI-induced PMR identified, it is suggested that careful monitoring for the symptom of PMR (e.g., bilateral pain in shoulder and pelvic girdles) is required in patients over 70 years of age treated with nivolumab and female patients treated with pembrolizumab.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found here: https://www.info.pmda.go.jp/fukusayoudb/CsvDownload.jsp.
Author Contributions
KK, TM, YI, and NT designed the study. KK and TK surveyed the JADER database. KK, TM, and TK performed the statistical analyses. KK, TM, YI, KT, SY, and NT drafted the manuscript. All authors approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank Editage (https://www.editage.com/) for the English language editing and reviewing of this manuscript.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.803706/full#supplementary-material
Abbreviations
ICPI, immune checkpoint inhibitor; PD-1, programmed cell death 1; PD-L1, programmed cell death ligand 1; CTLA-4, cytotoxic T-lymphocyte antigen 4; irAE, immune-related adverse event; ADEs, adverse drug events; PT, preferred term; ROR, reporting odds ratio; CI, confidence interval; PMR, polymyalgia rheumatica; GCA, giant cell arteritis.
References
Abe, J., Umetsu, R., Mataki, K., Kato, Y., Ueda, N., Nakayama, Y., et al. (2016). Analysis of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Using the Japanese Adverse Drug Event Report Database. J. Pharm. Health Care Sci. 2, 14. doi:10.1186/s40780-016-0048-5
Angelopoulou, F., Bogdanos, D., Dimitroulas, T., Sakkas, L., and Daoussis, D. (2021). Immune Checkpoint Inhibitor-Induced Musculoskeletal Manifestations. Rheumatol. Int. 41 (1), 33–42. doi:10.1007/s00296-020-04665-7
Belkhir, R., Burel, S. L., Dunogeant, L., Marabelle, A., Hollebecque, A., Besse, B., et al. (2017). Rheumatoid Arthritis and Polymyalgia Rheumatica Occurring after Immune Checkpoint Inhibitor Treatment. Ann. Rheum. Dis. 76 (10), 1747–1750. doi:10.1136/annrheumdis-2017-211216
Benfaremo, D., Manfredi, L., Luchetti, M. M., and Gabrielli, A. (2018). Musculoskeletal and Rheumatic Diseases Induced by Immune Checkpoint Inhibitors: A Review of the Literature. Curr. Drug Saf. 13 (3), 150–164. doi:10.2174/1574886313666180508122332
Bernier, M., Guillaume, C., Leon, N., Alexandre, J., Hamel-Senecal, L., Chretien, B., et al. (2017). Nivolumab Causing a Polymyalgia Rheumatica in a Patient with a Squamous Non-small Cell Lung Cancer. J. Immunother. 40 (4), 129–131. doi:10.1097/cji.0000000000000163
Betrains, A. E., and Blockmans, D. E. (2019). Immune Checkpoint Inhibitor-Associated Polymyalgia Rheumatica/Giant Cell Arteritis Occurring in a Patient after Treatment with Nivolumab. J. Clin. Rheumatol. 27, S555–S556. doi:10.1097/rhu.0000000000001012
Borghaei, H., Paz-Ares, L., Horn, L., Spigel, D. R., Steins, M., Ready, N. E., et al. (2015). Nivolumab versus Docetaxel in Advanced Nonsquamous Non-small-cell Lung Cancer. N. Engl. J. Med. 373 (17), 1627–1639. doi:10.1056/NEJMoa1507643
Brahmer, J. R., Drake, C. G., Wollner, I., Powderly, J. D., Picus, J., Sharfman, W. H., et al. (2010). Phase I Study of Single-Agent Anti-programmed Death-1 (MDX-1106) in Refractory Solid Tumors: Safety, Clinical Activity, Pharmacodynamics, and Immunologic Correlates. J. Clin. Oncol. 28 (19), 3167–3175. doi:10.1200/jco.2009.26.7609
Brahmer, J. R., Tykodi, S. S., Chow, L. Q., Hwu, W. J., Topalian, S. L., Hwu, P., et al. (2012). Safety and Activity of Anti-PD-L1 Antibody in Patients with Advanced Cancer. N. Engl. J. Med. 366 (26), 2455–2465. doi:10.1056/NEJMoa1200694
Brunot, A., Grob, J.-J., Jeudy, G., Grange, F., Guillot, B., Kramkimel, N., et al. (2020). Association of Anti-programmed Cell Death 1 Antibody Treatment with Risk of Recurrence of Toxic Effects after Immune-Related Adverse Events of Ipilimumab in Patients with Metastatic Melanoma. JAMA Dermatol. 156, 982. doi:10.1001/jamadermatol.2020.2149
Chaput, N., Lepage, P., Coutzac, C., Soularue, E., Le Roux, K., Monot, C., et al. (2017). Baseline Gut Microbiota Predicts Clinical Response and Colitis in Metastatic Melanoma Patients Treated with Ipilimumab. Ann. Oncol. 28 (6), 1368–1379. doi:10.1093/annonc/mdx108
Daxini, A., Cronin, K., and Sreih, A. G. (2018). Vasculitis Associated with Immune Checkpoint Inhibitors-A Systematic Review. Clin. Rheumatol. 37 (9), 2579–2584. doi:10.1007/s10067-018-4177-0
Dejaco, C., Singh, Y. P., Perel, P., Hutchings, A., Camellino, D., Mackie, S., et al. (2015). 2015 Recommendations for the Management of Polymyalgia Rheumatica: a European League against Rheumatism/American College of Rheumatology Collaborative Initiative. Ann. Rheum. Dis. 74 (10), 1799–1807. doi:10.1136/annrheumdis-2015-207492
Fadel, F., El Karoui, K., and Knebelmann, B. (2009). Anti-CTLA4 Antibody-Induced Lupus Nephritis. N. Engl. J. Med. 361 (2), 211–212. doi:10.1056/NEJMc0904283
Guzman-Prado, Y., Ben Shimol, J., and Samson, O. (2021). Body Mass index and Immune-Related Adverse Events in Patients on Immune Checkpoint Inhibitor Therapies: a Systematic Review and Meta-Analysis. Cancer Immunol. Immunother. 70 (1), 89–100. doi:10.1007/s00262-020-02663-z
Hara, A., Matsumoto, K., Yokoyama, Y., and Kizu, J. (2017). Factorial Analysis of Hepatitis B Virus Reactivation-Induced Hepatitis B Using JADER. Biol. Pharm. Bull. 40 (6), 782–788. doi:10.1248/bpb.b16-00765
Hasegawa, S., Matsui, T., Hane, Y., Abe, J., Hatahira, H., Motooka, Y., et al. (2017). Thromboembolic Adverse Event Study of Combined Estrogen-Progestin Preparations Using Japanese Adverse Drug Event Report Database. PLoS One 12 (7), e0182045. doi:10.1371/journal.pone.0182045
Herbst, R. S., Soria, J. C., Kowanetz, M., Fine, G. D., Hamid, O., Gordon, M. S., et al. (2014). Predictive Correlates of Response to the Anti-PD-L1 Antibody MPDL3280A in Cancer Patients. Nature 515 (7528), 563–567. doi:10.1038/nature14011
Hernández-Rodríguez, J., Cid, M. C., López-Soto, A., Espigol-Frigolé, G., and Bosch, X. (2009). Treatment of Polymyalgia Rheumatica: a Systematic Review. Arch. Intern. Med. 169 (20), 1839–1850. doi:10.1001/archinternmed.2009.352
Hodi, F. S., O'Day, S. J., McDermott, D. F., Weber, R. W., Sosman, J. A., Haanen, J. B., et al. (2010). Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 363 (8), 711–723. doi:10.1056/NEJMoa1003466
Hosoya, R., Uesawa, Y., Ishii-Nozawa, R., and Kagaya, H. (2017). Analysis of Factors Associated with Hiccups Based on the Japanese Adverse Drug Event Report Database. PLoS One 12 (2), e0172057. doi:10.1371/journal.pone.0172057
Imai, Y., Tanaka, M., Fujii, R., Uchitani, K., and Okazaki, K. (2019). Effectiveness of a Low-Dose Corticosteroid in a Patient with Polymyalgia Rheumatica Associated with Nivolumab Treatment. Yakugaku Zasshi 139 (3), 491–495. doi:10.1248/yakushi.18-00161
Isobe, M., Amano, K., Arimura, Y., Ishizu, A., Ito, S., Kaname, S., et al. (2020). JCS 2017 Guideline on Management of Vasculitis Syndrome - Digest Version. Circ. J. 84 (2), 299–359. doi:10.1253/circj.CJ-19-0773
Kita, T., Araya, T., Sakai, T., Uchida, Y., Matsuoka, H., and Kasahara, K. (2021). Nivolumab-induced Polymyalgia Rheumatica in a Patient with Lung Adenocarcinoma. Am. J. Med. Sci. 362, 321–323. doi:10.1016/j.amjms.2021.04.010
Klavdianou, K., Melissaropoulos, K., and Daoussis, A. D. (2021). Should We Be Afraid of Immune Check Point Inhibitors in Cancer Patients with Pre-existing Rheumatic Diseases? Immunotherapy in Pre-existing Rheumatic Diseases. Mediterr. J. Rheumatol. 32 (3), 218–226. doi:10.31138/mjr.32.3.218
Kong, E. K., Prokunina-Olsson, L., Wong, W. H., Lau, C. S., Chan, T. M., Alarcón-Riquelme, M., et al. (2005). A New Haplotype of PDCD1 Is Associated with Rheumatoid Arthritis in Hong Kong Chinese. Arthritis Rheum. 52 (4), 1058–1062. doi:10.1002/art.20966
Leonardi, G. C., Gainor, J. F., Altan, M., Kravets, S., Dahlberg, S. E., Gedmintas, L., et al. (2018). Safety of Programmed Death-1 Pathway Inhibitors Among Patients with Non-small-cell Lung Cancer and Preexisting Autoimmune Disorders. J. Clin. Oncol. 36 (19), 1905–1912. doi:10.1200/jco.2017.77.0305
Li, S., Liao, W., Chen, M., Shan, S., Song, Y., Zhang, S., et al. (2014). Expression of Programmed Death-1 (PD-1) on CD4+ and CD8+ T Cells in Rheumatoid Arthritis. Inflammation 37 (1), 116–121. doi:10.1007/s10753-013-9718-8
Lobo, Y., Good, P., and Murphy, F. (2020). Polymyalgia Rheumatica in a Melanoma Patient 11 Months after Completion of Immunotherapy with Nivolumab. Cancer Rep. (Hoboken) 3 (3), e1244. doi:10.1002/cnr2.1244
Mamlouk, O., Lin, J. S., Abdelrahim, M., Tchakarov, A. S., Glass, W. F., Selamet, U., et al. (2020). Checkpoint Inhibitor-Related Renal Vasculitis and Use of Rituximab. J. Immunother. Cancer 8 (2), e000750. doi:10.1136/jitc-2020-000750
Manzo, C., Isetta, M., Natale, M., and Castagna, A. (2020). Identification and Classification of Polymyalgia Rheumatica (PMR) and PMR-like Syndromes Following Immune Checkpoint Inhibitors (ICIs) Therapy: Discussion Points and Grey Areas Emerging from a Systematic Review of Published Literature. Medicines (Basel) 7 (11), 68. doi:10.3390/medicines7110068
Matteson, E. L., and Dejaco, C. (2017). Polymyalgia Rheumatica. Ann. Intern. Med. 166 (9), Itc65–itc80. doi:10.7326/aitc201705020
Melero, I., Hervas-Stubbs, S., Glennie, M., Pardoll, D. M., and Chen, L. (2007). Immunostimulatory Monoclonal Antibodies for Cancer Therapy. Nat. Rev. Cancer 7 (2), 95–106. doi:10.1038/nrc2051
Menzies, A. M., Johnson, D. B., Ramanujam, S., Atkinson, V. G., Wong, A. N. M., Park, J. J., et al. (2017). Anti-PD-1 Therapy in Patients with Advanced Melanoma and Preexisting Autoimmune Disorders or Major Toxicity with Ipilimumab. Ann. Oncol. 28 (2), 368–376. doi:10.1093/annonc/mdw443
Motzer, R. J., Escudier, B., McDermott, D. F., George, S., Hammers, H. J., Srinivas, S., et al. (2015). Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 373 (19), 1803–1813. doi:10.1056/NEJMoa1510665
Nakamagoe, K., Moriyama, T., Maruyama, H., Yokosawa, M., Hara, T., Tanaka, S., et al. (2017). Polymyalgia Rheumatica in a Melanoma Patient Due to Nivolumab Treatment. J. Cancer Res. Clin. Oncol. 143 (7), 1357–1358. doi:10.1007/s00432-017-2410-x
Postow, M. A., Sidlow, R., and Hellmann, M. D. (2018). Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 378 (2), 158–168. doi:10.1056/NEJMra1703481
Robert, C., Long, G. V., Brady, B., Dutriaux, C., Maio, M., Mortier, L., et al. (2015a). Nivolumab in Previously Untreated Melanoma without BRAF Mutation. N. Engl. J. Med. 372 (4), 320–330. doi:10.1056/NEJMoa1412082
Robert, C., Schachter, J., Long, G. V., Arance, A., Grob, J. J., Mortier, L., et al. (2015b). Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 372 (26), 2521–2532. doi:10.1056/NEJMoa1503093
Salem, J. E., Manouchehri, A., Moey, M., Lebrun-Vignes, B., Bastarache, L., Pariente, A., et al. (2018). Cardiovascular Toxicities Associated with Immune Checkpoint Inhibitors: an Observational, Retrospective, Pharmacovigilance Study. Lancet Oncol. 19 (12), 1579–1589. doi:10.1016/s1470-2045(18)30608-9
Salvarani, C., Cantini, F., Boiardi, L., and Hunder, G. G. (2002). Polymyalgia Rheumatica and Giant-Cell Arteritis. N. Engl. J. Med. 347 (4), 261–271. doi:10.1056/NEJMra011913
Salvarani, C., Gabriel, S. E., O'Fallon, W. M., and Hunder, G. G. (1995). Epidemiology of Polymyalgia Rheumatica in Olmsted County, Minnesota, 1970-1991. Arthritis Rheum. 38 (3), 369–373. doi:10.1002/art.1780380311
Sivan, A., Corrales, L., Hubert, N., Williams, J. B., Aquino-Michaels, K., Earley, Z. M., et al. (2015). Commensal Bifidobacterium Promotes Antitumor Immunity and Facilitates Anti-PD-L1 Efficacy. Science 350 (6264), 1084–1089. doi:10.1126/science.aac4255
Sugawara, H., Uchida, M., Suzuki, S., Suga, Y., Uesawa, Y., Nakagawa, T., et al. (2019). Analyses of Respiratory Depression Associated with Opioids in Cancer Patients Based on the Japanese Adverse Drug Event Report Database. Biol. Pharm. Bull. 42 (7), 1185–1191. doi:10.1248/bpb.b19-00105
Sunderkötter, C. H., Zelger, B., Chen, K. R., Requena, L., Piette, W., Carlson, J. A., et al. (2018). Nomenclature of Cutaneous Vasculitis: Dermatologic Addendum to the 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheumatol. 70 (2), 171–184. doi:10.1002/art.40375
Takada, S., Hirokazu, H., Yamagishi, K., Hideki, S., and Masayuki, E. (2020). Predictors of the Onset of Type 1 Diabetes Obtained from Real-World Data Analysis in Cancer Patients Treated with Immune Checkpoint Inhibitors. Asian Pac. J. Cancer Prev. 21 (6), 1697–1699. doi:10.31557/apjcp.2020.21.6.1697
Tie, Y., Ma, X., Zhu, C., Mao, Y., Shen, K., Wei, X., et al. (2017). Safety and Efficacy of Nivolumab in the Treatment of Cancers: A Meta-Analysis of 27 Prospective Clinical Trials. Int. J. Cancer 140 (4), 948–958. doi:10.1002/ijc.30501
Keywords: immune checkpoint inhibitor, polymyalgia rheumatica (PMR), Japanese adverse drug event report (JADER), adults, vasculitides
Citation: Kato K, Mizuno T, Koseki T, Ito Y, Takahashi K, Tsuboi N and Yamada S (2022) Frequency of Immune Checkpoint Inhibitor-Induced Vasculitides: An Observational Study Using Data From the Japanese Adverse Drug Event Report Database. Front. Pharmacol. 13:803706. doi: 10.3389/fphar.2022.803706
Received: 28 October 2021; Accepted: 28 January 2022;
Published: 25 March 2022.
Edited by:
Lin Zhang, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaReviewed by:
Marc Henri De Longueville, UCB Pharma, BelgiumTheodoros Dimitroulas, Aristotle University of Thessaloniki, Greece
Copyright © 2022 Kato, Mizuno, Koseki, Ito, Takahashi, Tsuboi and Yamada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tomohiro Mizuno, dG9tb2hpcm8ubWl6dW5vQGZ1aml0YS1odS5hYy5qcA==