
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 08 April 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.802334
 María Luz Ruiz-Falcó Rojas1*
María Luz Ruiz-Falcó Rojas1* Martha Feucht2
Martha Feucht2 Alfons Macaya3Bernd Wilken4
Alfons Macaya3Bernd Wilken4 Andreas Hahn5
Andreas Hahn5 Ricardo Maamari6Yulia Hirschberg6Antonia Ridolfi7
Ricardo Maamari6Yulia Hirschberg6Antonia Ridolfi7 John Chris Kingswood8
John Chris Kingswood8The TuberOus SClerosis registry to increase disease Awareness (TOSCA) Post-Authorization Safety Study (PASS) was a non-interventional, multicenter, safety substudy that assessed the long-term safety of everolimus in patients with tuberous sclerosis complex (TSC) receiving everolimus for its licensed indications in the European Union (EU). This substudy also aimed to address TSC-associated neuropsychiatric disorders (TAND), sexual development, and male infertility. Eligible patients were enrolled from 39 sites across 11 countries in the EU. Outcomes of interest included the incidence of adverse events (AEs), serious adverse events (SAEs), treatment-related AEs (TRAEs), AEs leading to everolimus discontinuation, AEs of special interest (AESIs), the observed relationship between everolimus blood levels and incidence of AESIs, TAND, and reproductive clinical features. Herein, we present the final analysis results from this substudy (data cutoff date: 22 January 2020). At data cutoff, 179 patients were enrolled (female, 59.2%; age ≥18 years, 65.9%), of which the majority completed the study (76%). Overall, 121 patients (67.6%) had AEs regardless of causality. The most frequent TRAEs (≥5%) were stomatitis (7.8%), aphthous ulcer (6.7%), and hypercholesterolemia (6.1%). The most common treatment-related SAEs (>1%) were pneumonia (3.4%), influenza, pyelonephritis, aphthous ulcer, stomatitis, dyslipidemia, and hypercholesterolemia (1.1% each). Ten patients (5.6%) reported AEs leading to everolimus discontinuation. The common psychiatric disorders (N = 179) were autism spectrum disorder (21.8%), anxiety disorder (12.8%), “other” psychiatric disorders (8.9%), attention-deficit hyperactivity disorder, and depressive disorder (7.8% each). Of 179 patients, 88 (49.2%) had ≥1 behavioral problem. Of these (n = 88), the most common (>20%) were sleep difficulties (47.7%), anxiety (43.2%), mood swings (37.5%), depression mood (35.2%), impulsivity (30.7%), severe aggression (23.9%), and overactivity (22.7%). Of 179 patients, four (2.2%) reported abnormal puberty onset, and three (1.7%) reported other reproductive disorders. Of 106 females, 23 (21.7%) reported menstrual cycle disorders and 10 (9.4%) reported amenorrhea. Available data did not show delays in sexual maturation or an association between sexual development and infertility. The results demonstrate that everolimus has a manageable long-term safety profile in the TSC treatment setting. No new safety signals emerged. This substudy also contributed to the mapping of TAND and reproductive clinical features in patients with TSC.
Tuberous sclerosis complex (TSC) is a rare, multisystem, autosomal dominant disorder characterized by the growth of benign tumors (hamartomas) in various organs, including the brain, kidneys, lungs, liver, heart, and skin (Crino et al., 2006; Curatolo et al., 2008). TSC is caused by inactivating mutations in the TSC1 or TSC2 genes (Dabora et al., 2001; Crino et al., 2006; Curatolo et al., 2008; Huang and Manning, 2008; Tyburczy et al., 2015). These mutations lead to a hyperactivation of the mammalian target of rapamycin (mTOR) pathway with subsequent abnormal cell proliferation/differentiation, which in turn results in the development of hamartomatous lesions characteristic of TSC (Zhang et al., 2003; Kwiatkowski and Manning, 2005; Jozwiak et al., 2008; Borkowska et al., 2011).
Patients with TSC experience a wide spectrum of clinical manifestations with varying degrees of severity as well as age-related onset and expression patterns (Józwiak et al., 2000; Crino et al., 2006; Curatolo et al., 2008; Franz et al., 2010; Kingswood et al., 2014; Curatolo et al., 2015). Central nervous system (CNS) manifestations, such as cortical tubers, subependymal nodules, and subependymal giant cell astrocytoma (SEGA), are common in TSC and cause significant disease burden (Curatolo et al., 2008; Franz et al., 2010; Curatolo and Maria, 2013; Curatolo et al., 2015). The majority of patients develop epilepsy that is often refractory (Franz et al., 2010; Kingswood et al., 2014). In addition, TSC-associated neuropsychiatric disorders (TAND) significantly impact quality of life (Krueger and Northrup, 2013; Curatolo et al., 2015); TAND features comprise a wide range of manifestations, such as intellectual disability, academic/scholastic difficulties, autism spectrum disorders and other neurodevelopmental and psychiatric disorders, and various behavioral problems (Prather and de Vries, 2004; Krueger and Northrup, 2013; de Vries et al., 2015).
Targeting the mTOR pathway has emerged as a promising therapeutic strategy for TSC (Davies et al., 2011; McCormack et al., 2011; Krueger and Northrup, 2013; Tran and Zupanc, 2015; Capal and Franz, 2016; Franz and Krueger, 2018; Annear et al., 2019). Everolimus is a selective and orally bioavailable mTOR inhibitor approved for the treatment of adult and pediatric patients aged ≥1 year who have TSC-associated SEGA that requires therapeutic intervention but is not amenable to surgery. Everolimus is also approved for the treatment of adults with TSC-related renal angiomyolipoma not requiring immediate surgery. Since 2017, everolimus has been approved as an adjunctive treatment for patients with TSC aged ≥2 years who have refractory partial-onset seizures, with or without secondary generalization (US Food and Drug Administration, 2018; European Medicines Agency, 2020). The approvals were based on the results from the EXIST-1 (Franz et al., 2013; Franz et al., 2014; Franz et al., 2016), EXIST 2 (Bissler et al., 2013; Bissler et al., 2016; Bissler et al., 2017), and EXIST 3 (French et al., 2016; Franz et al., 2018) phase 3, randomized, double-blind, placebo-controlled clinical trials, which demonstrated the efficacy and safety of everolimus in these indications. Furthermore, results from the long-term follow-up of patients in these randomized clinical trials showed that everolimus had a manageable long-term safety and tolerability profile. Stomatitis was the most frequently reported treatment-related adverse event (TRAE) (Franz et al., 2016; Bissler et al., 2017; Franz et al., 2018).
There is limited real-world evidence of the long-term safety of everolimus for its licensed indications in the TSC treatment setting. The TuberOus SClerosis registry to increase disease Awareness (TOSCA) was a global registry primarily established to address gaps in understanding the course of various TSC manifestations, therapeutic interventions and their outcomes, and quality of life (Kingswood et al., 2014; Jansen et al., 2020). The registry aimed at collecting data from patients with TSC to further inform treatment standards and promote research in TSC (Kingswood et al., 2014; Kingswood et al., 2017).
The TOSCA Post-Authorization Safety Study (PASS) was a non-interventional, multicenter, safety substudy that was initiated based on a request from the European Medicines Agency (EMA) (Kingswood et al., 2014). The purpose of this safety substudy was to prospectively collect data on the long-term safety profile of everolimus prescribed for TSC-related licensed indications in a real-world setting in the European Union (EU) (Kingswood et al., 2014). The TOSCA PASS also aimed to address TAND, sexual development, and male infertility.
Results of a prior interim analysis from TOSCA PASS (data cutoff: 10 August 2017) showed that everolimus had a manageable safety profile in patients with TSC who received everolimus for the licensed indications (Kingswood et al., 2021). Furthermore, data on reproductive clinical features indicated age-appropriate sexual maturation in these patients (Kingswood et al., 2021).
Herein, we present final analysis results from TOSCA PASS that include cumulative data from the PASS first patient first visit (FPFV, 7 March 2013) to the last date of study data collection (data cutoff date: 22 January 2020). The focus of this report will be on the long-term safety of everolimus and TAND features.
The TOSCA PASS (EU PAS Register Number ENCePP/SDPP/3247) enrolled patients with TSC from 39 sites across 11 countries in the EU. The participating countries were Austria, Czech Republic, Denmark, France, Germany, Netherlands, Poland, Slovenia, Spain, Sweden, and the United Kingdom. Patients receiving everolimus prescribed for its licensed indications were eligible. No clinical, instrumental, or laboratory assessments/interventions were performed in this study other than those required for disease management, according to local best practice, or required to monitor any treatment as per locally approved summary of product characteristics. Due to the observational nature of this study, no specific visit schedules were mandated, and only available data from routine clinical management of patients were collected at patients’ visits to their site. Patients could be withdrawn from the study if any of the following occurred: death, lost to follow-up by the site, voluntary withdrawal of consent, or at physician discretion. The period of observation in this study ended before the start of the COVID-19 pandemic in Europe.
This study was designed, implemented, and reported in accordance with the Guidelines for Good Pharmacoepidemiology Practices (GPP) of the International Society for Pharmacoepidemiology (ISPE 2008), the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, and the ethical principles in the Declaration of Helsinki. The protocol and the proposed informed consent form were reviewed and approved by constituted Institutional Review Boards/Independent Ethics Committees/Research Ethics Boards (IRB/IEC/REB). Patients (or parent/guardian as applicable) had to sign the TOSCA PASS informed consent form before any data or information were provided for this study.
The main objective of the TOSCA PASS was to document the long-term safety and tolerability profile of everolimus prescribed for the licensed indications in patients with TSC residing in the EU (Kingswood et al., 2014). The corresponding endpoints included the incidence of adverse events (AEs), serious adverse events (SAEs), TRAEs, AEs leading to everolimus discontinuation, and the incidence of AEs of special interest (AESIs) (Kingswood et al., 2014); AESIs were those events of special clinical interest that were explored in relation to everolimus treatment (Supplementary Table S2), and these events have also been listed in the prior interim analysis report (Kingswood et al., 2021). The other objective was to collect everolimus Therapeutic Drug Monitoring data, and the corresponding endpoint was everolimus blood concentration, where available (Kingswood et al., 2014). The relationship among everolimus blood levels, the incidence of AESIs, and the intake of concomitant antiepileptic drugs (AEDs) was also explored. In addition, the TOSCA PASS aimed to address TAND, sexual development, and male infertility.
The start of data collection was 7 March 2013 (PASS FPFV). The recommended frequency of data collection was 3-monthly intervals, with a minimum of once-yearly follow-up visits (10 ± 2 months interval) for each patient to ensure an ongoing data stream. Disease evaluation could be performed more frequently, if needed. For reporting purposes, the baseline visit defined each subsequent follow-up window (FU1, FU2, FU3, FU4, and FU5, etc). All events occurring during the 12 months on or after the baseline visit were reported as baseline; all events in the next 12-month period were reported as follow-up 1, and so forth. This was derived for each patient regardless of the actual dates of the visits. A follow-up observation period of up to five years was foreseen for PASS patients aged >16 years for females or >17 years for males, or at Tanner stage V. Follow-up visits were scheduled according to the standard practice of each site and as per the treating physician’s judgment. For pediatric patients, the follow-up period was extended until they reached Tanner stage V, or until age 16 for females or 17 for males, regardless of the end of treatment, to collect long-term data on safety, sexual maturation, and fertility. Patients who chose to withdraw consent were not contacted for follow-up information.
An interim analysis from this study was submitted to the EMA every year. In agreement with the EMA, the TOSCA PASS was terminated early since no new safety signals were identified, and due to the observational nature of the study, further data collection was not expected to provide meaningful data to draw new conclusions.
Variables of interest were summarized descriptively either for the overall population and by age ranges or at baseline and by follow-up year. In this manuscript, data by follow-up included only those reported for follow-up year 1–6, while the data from follow-up year 7 were not reported, owing to very few patients. AEs were assessed according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. The incidence of various AEs was summarized by preferred terms using the Medical Dictionary for Regulatory Activities (MedDRA) version 22.1.
Overall, 179 patients from 11 European countries participating in the TOSCA registry were enrolled in the TOSCA PASS. Of these, the majority (n = 136, 76%) completed the study, while 43 (24%) discontinued. The primary reasons for discontinuation were registry termination by the sponsor (n = 25, 14%), loss to follow-up (n = 12, 6.7%), death (n = 3, 1.7%), investigator’s decision to stop the study at site due to lack of resources (n = 2, 1.1%), and physician’s decision (n = 1, 0.6%). The patient disposition is presented in Figure 1.
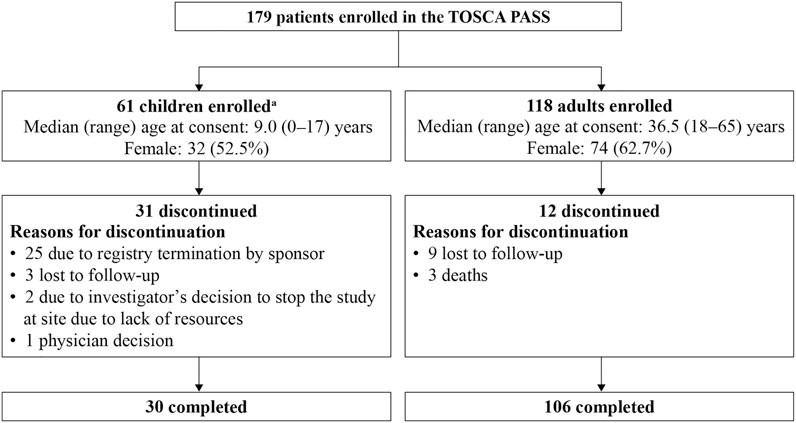
FIGURE 1. Patient disposition in the TOSCA PASS.PASS, Post-Authorization Safety Study.aChildren within different age groups at registry entry were as follows: ≤2 years (n = 7), >2 to ≤9 years (n = 27), and >9 to <18 years (n = 27).
Of 179 enrolled patients, 106 (59.2%) were female. The mean age at consent was 27.1 years, and the median age was 27.0 years (range, 0–65 years). Patients within different age groups at registry entry were as follows: ≤2 years (n = 7); >2 to ≤9 years (n = 27); >9 to <18 years (n = 27); and ≥18 years (n = 118). The proportion of adults (≥18 years) was numerically higher than the proportion of pediatric patients (n = 118, 65.9% vs. n = 61, 34.1%). Detailed disease characteristics of the enrolled patients have been previously published (Kingswood et al., 2021). Of the 179 patients enrolled, 100 (55.9%) had SEGA, 149 (83.2%) had renal angiomyolipoma, and 151 (84.4%) had epilepsy (Kingswood et al., 2021).
Table 1 presents everolimus dosage, exposure, and safety in the overall population (N = 179), by sex, and across age groups. Most patients took the tablet formulation (n = 172, 96.1%). The most commonly administered dosage was 5 mg (n = 156, 87.2%). The average (standard deviation [SD]) daily dose was 7.3 mg (3.1 mg), and the median duration of exposure was 1026.0 days (range, 36–2652 days). Everolimus dose changes were reported in 116 patients (64.8%); dose interruptions in 69 (38.5%), dose increases in 98 (54.7%), and dose reductions in 57 (31.8%) patients. In 78 patients (43.6%), the reason for dose changes was listed as “other”, with no additional specific details. In 50 patients (27.9%), the reason for dose changes was side effects.
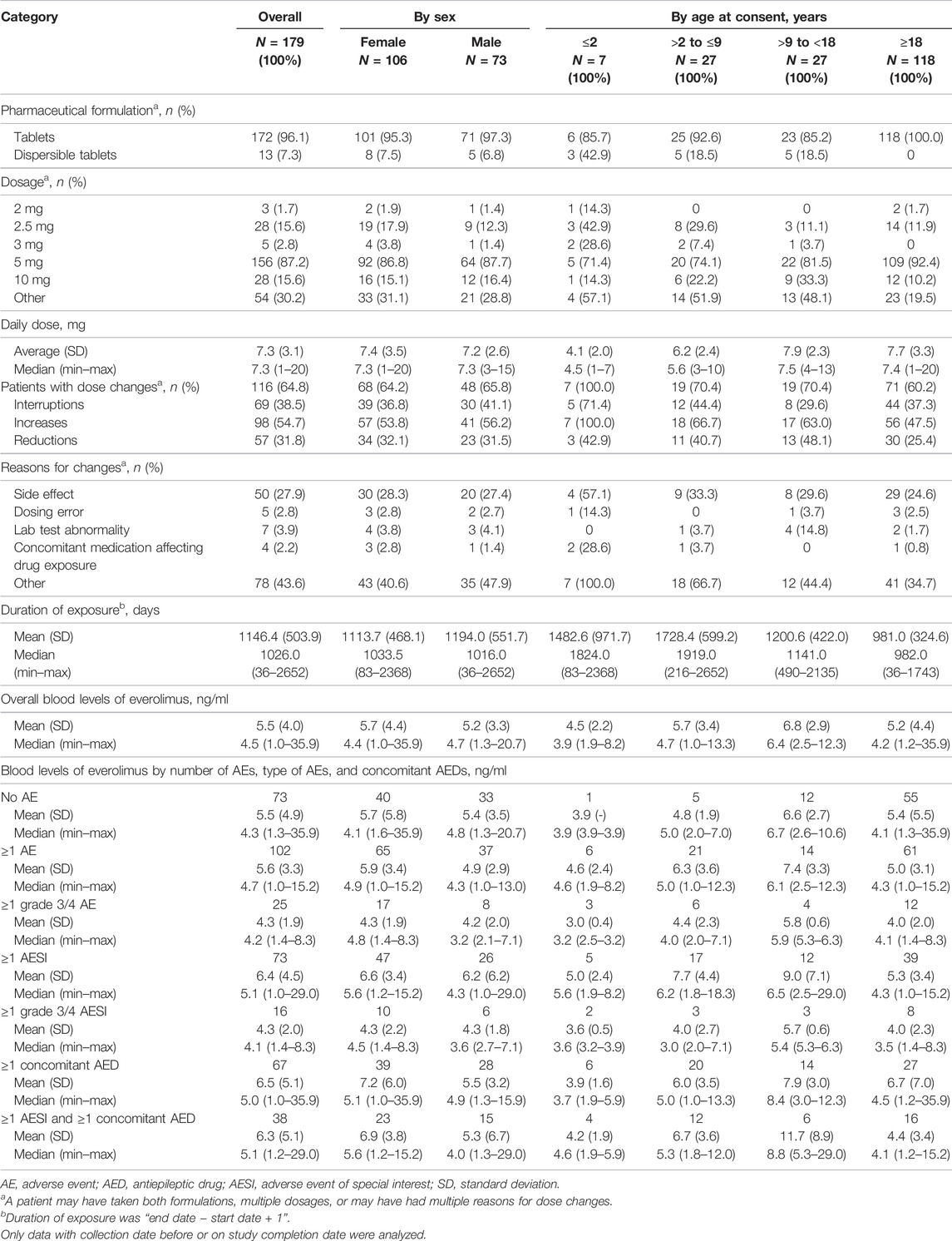
TABLE 1. Everolimus dosage, exposure, and safety for the overall population, by sex, and across age groups.
The overall mean (SD) blood level of everolimus (n = 175) was 5.5 ng/ml (4.0 ng/ml). The mean (SD) blood levels of everolimus (in ng/ml) in patients who experienced no AE, ≥1 AE, ≥1 grade 3/4 AE, ≥1 AESI, and ≥1 grade 3/4 AESI were 5.5 (4.9), 5.6 (3.3), 4.3 (1.9), 6.4 (4.5), and 4.3 (2.0), respectively. In patients who had ≥1 AESI and were treated with ≥1 concomitant AED, the mean (SD) blood level of everolimus was 6.3 ng/ml (5.1 ng/ml) (Table 1).
There were no differences in everolimus dosing or blood levels between males and females. Everolimus blood levels were not different between age groups, but there was a trend to an increased mean/median dose in adults vs. children (Table 1).
Of 179 patients, 120 (67.0%) received concomitant medications or significant non-drug therapies. The most frequently administered concomitant medications were nervous system medications (n = 95, 53.1%) including vigabatrin (n = 32, 17.9%), lamotrigine (n = 29, 16.2%), levetiracetam (n = 25, 14.0%), valproate sodium (n = 20, 11.2%), and oxcarbazepine (n = 19, 10.6%); medications belonging to the alimentary tract and metabolism class (n = 60, 33.5%) including colecalciferol (n = 25, 14.0%); and systemic antiinfectives (n = 38, 21.2%) including cefuroxime (n = 10, 5.6%). Sirolimus (0.1% and 0.25%) was used topically for angiofibroma in one patient (not related to AE), and sirolimus (6-mg dose) was also used for anemia in another patient (not related to AE).
Overall, 121 patients (67.6%) had AEs regardless of causality; 44 patients (24.6%) had grade 1, 32 (17.9%) had grade 2, 36 (20.1%) had grade 3, and nine (5.0%) had grade 4 AEs. Supplementary Table S1 presents frequent AEs (>3% overall) regardless of causality. The most frequent AE regardless of causality was stomatitis (n = 16, 8.9%).
Overall, AEs suspected to be everolimus-related (TRAEs) were reported in 81 patients (45.3%). The rate of TRAEs was numerically higher in children vs. adults (n/N = 42/61, 68.9% vs. n/N = 39/118, 33.1%). Frequent TRAEs (>3% overall) were reported in 49 patients (grade 1 [n = 27, 15.1%], grade 2 [n = 15, 8.4%], grade 3 [n = 7, 3.9%]) (Table 2). The most frequent (>5%) were stomatitis (n = 14, 7.8%), aphthous ulcer (n = 12, 6.7%), and hypercholesterolemia (n = 11, 6.1%) (Table 2). The rates of frequent TRAEs were comparable between females and males (Table 2).
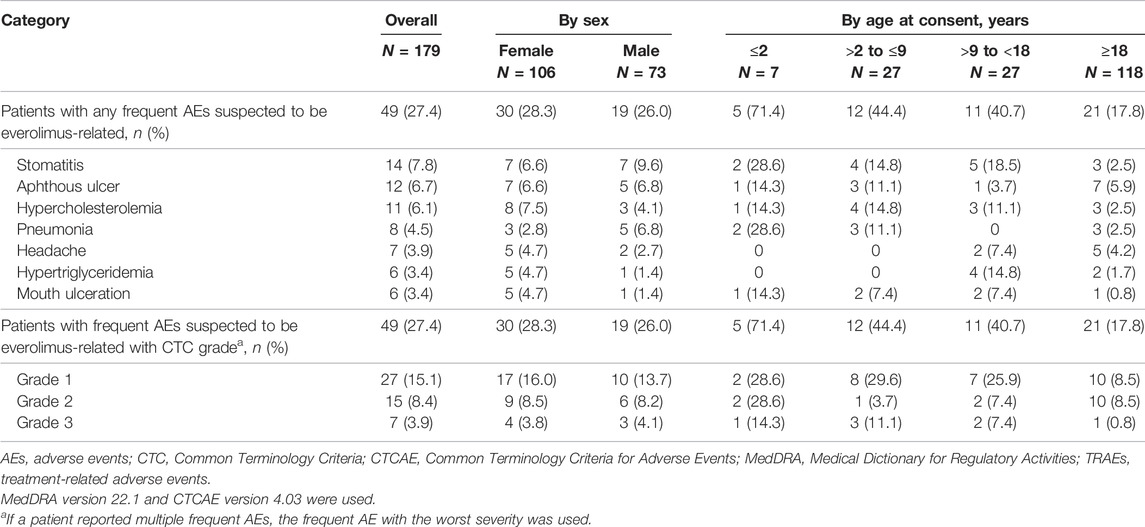
TABLE 2. Frequent TRAEs (>3%, overall) in the overall population, by sex, and across age groups.
SAEs regardless of causality were reported in 59 patients (33.0%); 58 (32.4%) had SAEs with Common Terminology Criteria (CTC) grade reported (grade 1 [n = 7, 3.9%], grade 2 [n = 11, 6.1%], grade 3 [n = 31, 17.3%], grade 4 [n = 9, 5.0%]). The most frequent SAEs regardless of causality (>3% overall) were pneumonia (n = 8, 4.5%) and epilepsy (n = 7, 3.9%).
SAEs suspected to be everolimus-related were reported in 25 patients (14%); four patients (2.2%) had grade 1, six (3.4%) had grade 2, 13 (7.3%) had grade 3, and two (1.1%) had grade 4 SAEs. The most common SAEs (>1% overall) suspected to be everolimus-related were pneumonia (n = 6, 3.4%), influenza, pyelonephritis, aphthous ulcer, stomatitis, dyslipidemia, and hypercholesterolemia (n = 2, 1.1% each).
AEs leading to everolimus discontinuation were reported in 10 patients (5.6%); four patients (2.2%) had grade 1, and two (1.1%) each had grade 2, grade 3, and grade 4 AEs. The AEs leading to study drug discontinuation were fatigue, amenorrhea (n = 2, 1.1% each), anemia, mouth ulceration, drug ineffective, empyema, pneumonia, hyperglycemia, type I diabetes mellitus, flank pain, intestinal adenocarcinoma, seizure, and alopecia (n = 1, 0.6% each). AEs leading to everolimus dose adjustments were reported in 60 patients (grade 1 [n = 23, 12.8%], grade 2 [n = 17, 9.5%], grade 3 [n = 19, 10.6%], grade 4 [n = 1, 0.6%]). The most frequent (>2% overall) were diarrhea, aphthous ulcer (n = 6, 3.4% each), pneumonia (n = 5, 2.8%), stomatitis, nasopharyngitis, and urinary tract infection (n = 4, 2.2% each).
Overall, AESIs were reported in 91 patients (50.8%). The most frequent AESI by safety topic of interest was severe infections (n = 64, 35.8%); the events occurring in >2% of patients were nasopharyngitis (n = 11, 6.1%), pneumonia, urinary tract infection (n = 10, 5.6% each), bronchitis (n = 7, 3.9%), influenza (n = 6, 3.4%), ear infection, gastroenteritis, oral candidiasis, pharyngitis, and rhinitis (n = 4, 2.2% each) (Supplementary Table S2). Increased creatinine or proteinuria or renal failure was observed in three patients (1.7%); the events included increased blood creatinine (n = 1, 0.6%) and proteinuria (n = 3, 1.7%).
With longer follow-up in this study, the number of deaths remained unchanged relative to that reported in the prior interim analysis (Kingswood et al., 2021). A total of three deaths were reported, and none were related to everolimus treatment. Detailed narratives for these deaths have been published previously (Kingswood et al., 2021).
Of 179 TOSCA PASS patients, information related to everolimus exposure was available for 150 patients at the baseline visit, while 29 entered the PASS after the baseline visit. Of these 150 patients, the majority did not experience AESIs (n = 101, 67.3%); 49 (32.7%) experienced AESIs, and in 37 (24.7%), these AESIs were suspected to be everolimus-related. Similar trends were observed at follow-up 1–4 (Table 3).
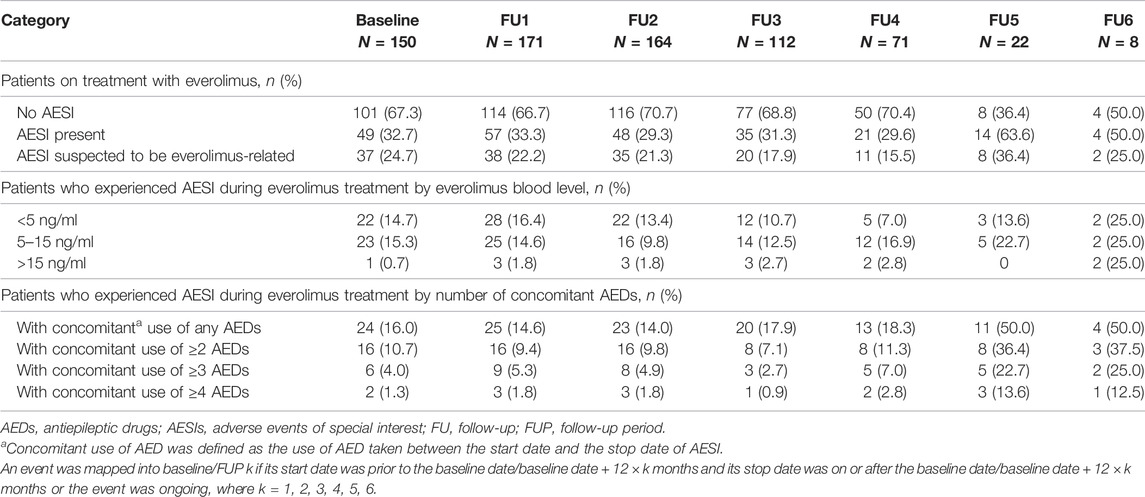
TABLE 3. AESIs and incidence by everolimus blood levels and number of concomitant AEDs at baseline and by follow-up year.
Among patients who experienced AESIs during everolimus treatment, 22 (14.7%) had everolimus blood levels <5 ng/ml, 23 (15.3%) had everolimus blood levels in the range of 5–15 ng/ml, and one (0.7%) had everolimus blood levels >15 ng/ml. Similar proportions were observed in follow-up 1–4 (Table 3).
The proportion of patients who experienced AESIs during everolimus treatment and with concomitant AED use at baseline and follow-up 1–6 is shown in Table 3.
Overall, investigator-reported data for TAND features were scarce compared to those for other TSC manifestations. In general, TAND features presented at varying frequencies across different age groups (Table 4).
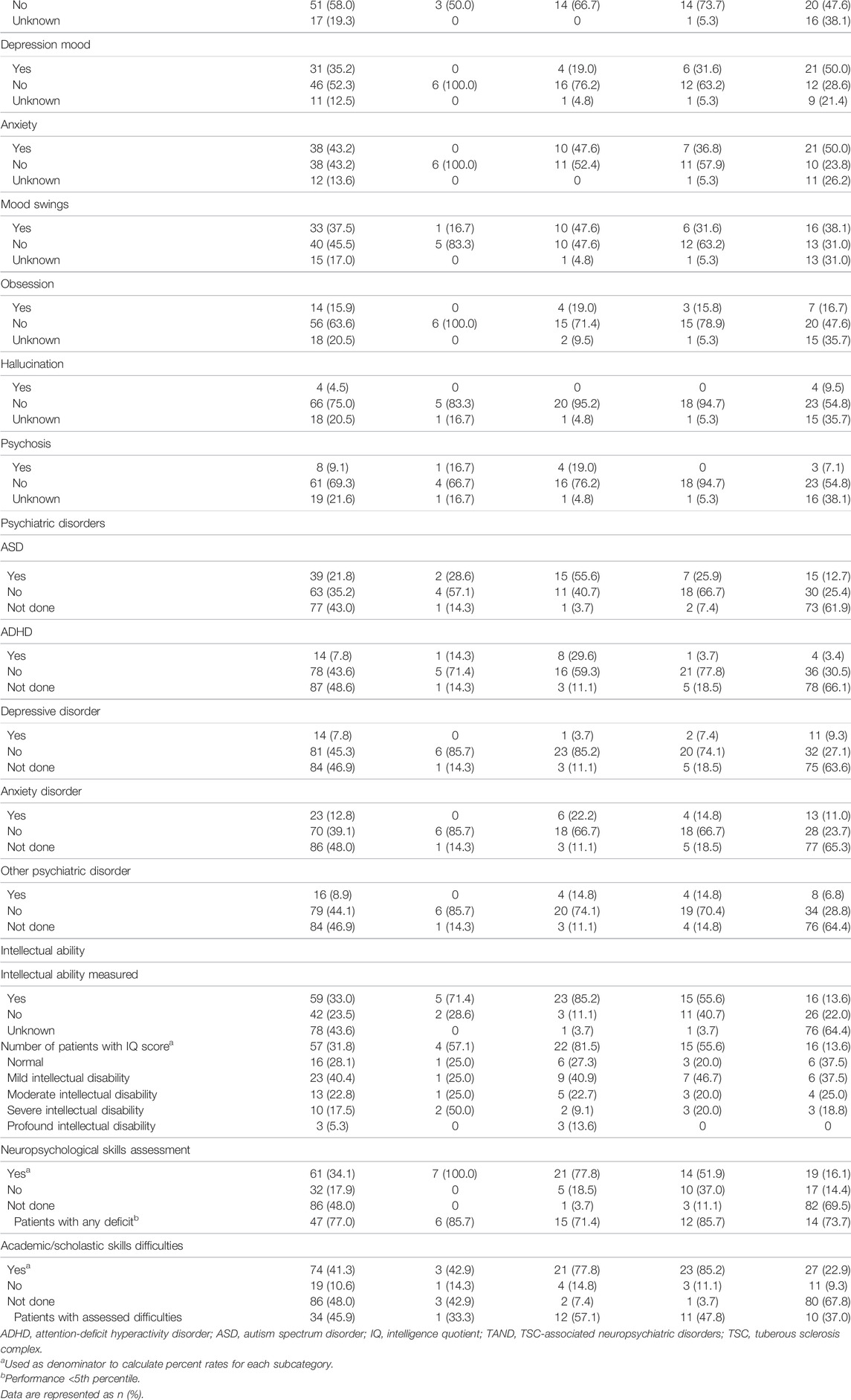
TABLE 4. TAND by age group.
At the psychiatric level, the common psychiatric disorders reported (Table 4) were autism spectrum disorder (n/N = 39/179, 21.8%), anxiety disorder (n/N = 23/179, 12.8%), “other” psychiatric disorders (n/N = 16/179, 8.9%), attention-deficit hyperactivity disorder, and depressive disorder (n/N = 14/179, 7.8% each).
At the behavioral level, of 179 patients, 88 (49.2%) had at least one behavioral problem (Table 4). Of these, the most common (reported in >20%) were sleep difficulties (n/N = 42/88, 47.7%), anxiety (n/N = 38/88, 43.2%), mood swings (n/N = 33/88, 37.5%), depression mood (n/N = 31/88, 35.2%), impulsivity (n/N = 27/88, 30.7%), severe aggression (n/N = 21/88, 23.9%), and overactivity (n/N = 20/88, 22.7%).
At the intellectual level, an intelligence quotient (IQ) score was available for 57 of 179 patients (31.8%). Of these, 16/57 (28.1%) had normal intellectual ability, while mild, moderate, severe, and profound intellectual disabilities were observed in 23/57 (40.4%), 13/57 (22.8%), 10/57 (17.5%), and 3/57 (5.3%), respectively, (Table 4).
At the academic/scholastic level, 74 of 179 patients (41.3%) reported having had difficulties in school subjects, of which 34/74 (45.9%) had assessed difficulties. At the neuropsychological level, neuropsychological skills were formally assessed in 61 of 179 patients (34.1%). Of those assessed, neuropsychological deficits (performance <5th percentile) were identified in 47/61 (77%) (Table 4).
Reproductive clinical features for the overall population and by age group are presented in Supplementary Table S3. Of 179 patients, four (2.2%) reported abnormal puberty onset (one male and three females). Menstrual cycle disorders (n/N = 23/106, 21.7%) and amenorrhea (n/N = 10/106, 9.4%) were reported in a low percentage of females aged ≥10 years. Other abnormal reproductive conditions were reported in three of 179 patients (1.7%).
Tanner staging was performed in 34 of 179 patients (19.0%; six males and 28 females). Male patients had genitalia stages 3 (n/N = 1/6, 16.7%), 4 (n/N = 3/6, 50.0%), and 5 (n/N = 2/6, 33.3%) and pubic hair stages 4 and 5 (n/N = 3/6, 50% each). Female patients mostly had breast stage 5 (n/N = 16/25, 64.0%) and pubic hair stage 5 (n/N = 18/26, 69.2%).
Of 106 females, a small proportion used contraception (n = 19, 17.9%), mostly hormone-based contraception (n/N = 16/19, 84.2%). Of 179 patients, five (2.8%) used external sex hormones and three (1.7%) underwent ovariectomy.
Overall, 39 of 179 patients (21.8%) underwent hormone tests (Supplementary Table S3); hormone tests were performed for 26 patients (14.6%) at baseline (N = 178), 19 (10.7%) at follow-up 1 (N = 178), 15 (8.5%) at follow-up 2 (N = 176), 11 (6.8%) at follow-up 3 (N = 161), two (2.2%) at follow-up 4 (N = 89), two (3.3%) at follow-up 5 (N = 61), and for none of the patients at follow-up 6 (N = 16).
The results of this final analysis from the TOSCA PASS demonstrated that everolimus had a manageable long-term safety and tolerability profile in patients with TSC. The safety profile of everolimus in this study was largely consistent with that previously reported in the TSC treatment setting (Krueger et al., 2013; Franz et al., 2014; Bissler et al., 2016; Franz et al., 2016; Bissler et al., 2017). Overall, AEs regardless of causality were reported in about two-thirds of patients, with most AEs of modest severity. The events were treatable with dose adjustments and/or use of concomitant medications. AEs leading to everolimus discontinuation were reported in a low percentage of patients in this study (5.6%), which was numerically lower compared with the rates of discontinuation due to AEs observed in the EXIST-1 (n/N = 11/111; 9.9%), EXIST-2 (n/N = 10/112; 8.9%), and EXIST-3 trials (n/N = 47/361; 13%) reporting on the long-term safety of everolimus (Franz et al., 2016; Bissler et al., 2017; Franz et al., 2018). One possible explanation for this is that clinicians in real life practice routinely commence everolimus at a lower dose than that used initially in the registration trials (Iqbal et al., 2017). The original starting dose chosen for everolimus in the EXIST-2 study (10 mg/day) was based on the fact that 10 mg was found to be tolerated by most adults in oncology trials (Davies et al., 2017). During the EXIST-2 study, it was found that 71.4% of patients had dose interruptions/reductions and after one year on everolimus, 35% received everolimus 5 mg/day. However, continued therapeutic benefits were still observed (Bissler et al., 2016; Davies et al., 2017; Northrup et al., 2021). Over the next five years in clinical practice, it was found that starting with 5 mg caused less side effects, was clinically effective, and very few patients needed a higher dose (Davies et al., 2017). A starting dose of 5 mg daily of everolimus in adults has become the almost universal practice of all experienced prescribers, as evidenced by the data in TOSCA.
In this substudy, numerically higher rates of TRAEs were observed in children vs. adults. We could speculate that some children may have needed a lower dose of everolimus than the one recommended, and thus, a higher exposure could have been achieved. Another explanation could be that pediatric patients may have been more thoroughly monitored for side effects compared with adult patients or may have had more frequent visits to the doctors’ offices and were therefore more closely followed up by their treating physicians. Nevertheless, due to the observational nature of this study, we cannot rule out the underreporting of AEs in the adult population. The most likely reason for this is that TOSCA is a non-interventional study, and as such, the reporting of AEs was done as per real-world practice, which might differ from randomized controlled studies (Franz et al., 2016; French et al., 2016; Bissler et al., 2017).
The results from this PASS also indicate that there was no cumulative toxicity (or new safety issues) observed with prolonged use of everolimus. Consistent with the long-term safety reports from the EXIST 1-3 clinical trials (Franz et al., 2016; Bissler et al., 2017; Franz et al., 2018), stomatitis was the most commonly reported (7.8%) TRAE in this substudy. Stomatitis-related AEs are a known identified risk associated with everolimus in patients with TSC, which are usually effectively managed to minimize their occurrence and severity (Kingswood et al., 2021). Severe infections, an identified risk with everolimus (Krueger et al., 2013; Trelinska et al., 2015; Bissler et al., 2017), were reported in 35.8% of patients in this substudy, mostly nasopharyngitis followed by pneumonia, urinary tract infection, bronchitis, and influenza. In the EXIST-2 trial report of the long-term safety of everolimus following four years of follow-up, infections were reported in 91.1% of patients, mostly those of the upper respiratory tract (Bissler et al., 2017). In this substudy, no conclusions could be drawn regarding the observed relationship between everolimus blood levels and AESI. The average blood levels of everolimus were not different in patients who did or who did not have AEs.
Consistent with prior TAND findings from the TOSCA study (Kingswood et al., 2017; de Vries et al., 2018), the results of this analysis from TOSCA PASS showed low reporting rates of TAND evaluation and reporting in patients with TSC in the EU, thus emphasizing the need for a more cautious evaluation of TAND by clinicians. The high rates of missing data limit the interpretability of the results of TAND features and, overall, are suggestive of underdiagnosis/undertreatment of TAND features in the clinical setting. In general, low rates of psychiatric disorders and behavioral difficulties were observed in this substudy. This finding is largely in line with the previously reported TAND findings from the TOSCA study (Kingswood et al., 2017; de Vries et al., 2018). At the neuropsychological level, of those who had neuropsychological skills assessed, 77% (n/N = 47/61) reported performance <5th percentile in this substudy compared with 55.7% (n/N = 314/564) in a prior TAND report from TOSCA (de Vries et al., 2018). At the academic level, of those who reported difficulties in school subjects or academic performance, the rates of individuals with assessed difficulties was 45.9% (n/N = 34/74) in this substudy vs. 48.8% (n/N = 359/735) in the prior TAND report from TOSCA (de Vries et al., 2018). In this study, 31.8% of patients had IQ scores, and among these, the rates of severe or profound intellectual disability were low.
With longer follow-up in this study, the rates of various reproductive clinical features remained either unchanged or numerically similar to those reported in the prior interim analysis (Kingswood et al., 2021). In general, limited data were collected for sexual maturation and hormone levels for patients in TOSCA PASS. Although the number of patients with reproductive hormonal testing performed decreased through the study, precluding a proper longitudinal evaluation and conclusion, overall, a low incidence of abnormal puberty onset, other abnormal reproductive conditions, amenorrhea, and menstrual cycle disorders was observed in this study. Overall, the available data did not suggest any delay in sexual maturation. A relationship between sexual development and male infertility could not be established.
Some limitations of the TOSCA PASS warrant discussion. Firstly, given the observational nature of the study, an important limitation was the high rates of missing data due to different reasons such as data not being reported, unknown data, or data not assessed by investigators. Of note, the missing data for the assessment and reporting of TAND likely reflect the limited use of this evaluation in the medical community. Secondly, the limited data on reproductive clinical features, in particular Tanner staging, possibly reflect gaps in the current medical practice for the reporting and/or assessment of reproductive clinical features in most European countries. Tanner staging is not routinely done as a standard practice as reproductive clinical features are not always considered a priority by the treating physicians, since patients with TSC experience multiple comorbidities. Moreover, Tanner stage evaluation assesses physical measurements of development based on external primary and secondary sex characteristics. Although an individual can reach the final Tanner stage (mature), this might not necessarily predict a final outcome on male or female infertility. Any impact on fertility would be observed when an individual tries to generate an offspring. Finally, considering the disease complexity, a patient was not always followed for all disease manifestations over follow-up periods by the site(s). Given the observational nature of the study, only data already available from clinical practice were collected.
In conclusion, TOSCA PASS provided a detailed picture of the TSC population in Europe. Results from this substudy show that everolimus has a well-characterized and acceptable long-term safety profile for its licensed indications in patients with TSC. No new safety signals were identified. AEs were common, but rarely needed withdrawal. This implies that everolimus treatment was considered valuable enough to continue despite AEs, and physicians therefore managed these events with a combination of dose interruptions and/or dose changes. The results from this study also suggest that physicians judge that the TSC indication is controlled on fairly low blood levels of everolimus. The observed occurrence of AEs did not seem to be influenced by everolimus blood levels. Although monitoring of renal function was not systematic, there were no strong indicators of any renal function-related issues in patients who were monitored. The results from this PASS showed inadequate monitoring and/or reporting of TAND in patients with TSC in the EU. Therefore, the effect of everolimus on TAND could not be interpreted from the collected data. However, despite some unavailable data, differences in local clinical practice, and the inconsistent application of international guidelines for TSC diagnosis, the TOSCA PASS did contribute to the mapping of TAND and reproductive clinical features in patients with TSC.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by constituted Institutional Review Boards/Independent Ethics Committees/Research Ethics Boards (IRB/IEC/REB): National Hospital Organization Central Ethics Committee; Gazi University Clinical Research Ethics Committee; Independent Multidisciplinary Committee on Ethical Review of Clinical Trials; Peking Union Medical College Hospital; Commissie Medische Ethiek UZ Brussel; CNIL (Commission National de l'Informatique et des Libertés), CCTIRS (Comité Consultatif sur le traitement de l’information en matière de recherche dans le domaine de la santé); Comité Etico Investigación Clínica de Euskadi (CEIC-E); Consejeria de Salud y Bienestar Social, Dirección General de Calidad, Investigación, Desarrollo e Innovación, Comité Coordinador de Ética de la Investigación Biomédica de Andalucía; Research Ethics Committee of the University of Tartu (UT REC); Ethikkommission der Medizinischen Universität Graz; North Wales REC–West; Regionala Etikprövningsnämnden i Göteborg; REK–Regionale komiteer for medisinsk og helsefaglig forskningsetikk; Komisja Bioetyczna przy Instytucie Pomnik Centrum Zdrowia Dziecka; Ethikkommission bei der Ludwig-Maximilians-Universitat München; Hokkaido University Hospital Independent clinical research Institutional Ethics Committee; Medical Juntendo University Institutional Ethics Committee; National Center for Chile Health and Deveropment of IRB; Osaka University Hospital of IRB; Ethics Committee at Moscow Institute of Pediatrics and Pediatric Surgery; Peking University First Hospital; Sanbo Brain Hospital Capital Medical University; Tianjin Children’s Hospital; Childrens Hospital Of Fudan University; Zhongshan Hospital Fudan University; Fudan University Shanghai Cancer Center; The Second Affiliated Hospital of Guangzhou Medical University; The First Affiliated Hospital, Sun Yan-Sen University; The First Affiliated Hospital Of Guangzhou Medical University; Shenzhen Children’s Hospital; West China Hospital, Sichuan University; Xijing Hospital; Children’s Hospital of Chongqing Medical University; Wuhan Children’s Hospital; The second affiliated hospital of Xi’an jiaotong university; Guangdong 999 brain hospital; Seoul National University Hospital Institutional Review Board; National Taiwan University Hospital (NTUH) Research Ethics Committee (REC); Institutional Review Board of the Taichung Veterans General Hospital; Institutional Review Board of Chung Shan Medical University Hospital; Institutional Review Board, Tungs’ Taichung MetroHarbor Hospital; Institutional Review Board of National Cheng Kung University Hospital; Metro South Human Research Ethics Committee; Sydney Children’s Hospital Network Human Research Ethics Committee; St Vincents Hospital Human Research Ethics Committee; Royal Melbourne Hospital Human Research Ethics Committee; Siriraj Institutional Review Board; The Institutional Review board, Faculty of Medicine, Chulalongkorn University, 3rd Floor, Ananthamahidol Building, King Chulalongkorn Memorial Hospital; The committee on Human Rights Related to Research Involving Human Subjects; Institutional Review board, Royal Thai Army Medical Department IRB RTA, 5th Floor, Phramongkutklaowejvitya Building, Phramongkutklao College of Medicine; Research Ethics Committee, Faculty of Medicine, Chiang Mai University; Research and Development, Queen Sirikit National Institute of Child Health; Human Research Ethics Committee, Faculty of Health Sciences, University of Cape Town; Shaare Zedek Meidcla center Helsinki comittee; Sheba Medical center Helsinki comittee; Tel Aviv Sourasly Medical center Helsinki comittee; General University Hospital of Patras Ethics Committee; Pendeli Children’s Hospital Ethics Committee; General University Hospital of Athens “G. Gennimatas” Ethics Committee; Evaggelismos General Hospital Ethics Committee; General University Hospital of Thessaloniki AHEPA Ethics Committee; General University Hospital of Ionnina Ethics Committee; METC UMC Utrecht; Direcció General de Regulació, Planificació i Recursos Sanitaris; Comité Ético de Investigación Clínica del Hospital Universitario Vall d'Hebron de Barcelona, Generalitat de Catalunya. Departament de Salut; Comité Ético de Investigación Clínica Hospital Universitario La Paz; Dirección General de Ordenación e Inspección, Consejería de Sanidad Comunidad de Madrid, Servicios de Control Farmacéutico y Productos Sanitarios; Comité Etico Investigación Clínica del Hospital Universitario y Politécnico de La Fe; Dirección General de Farmàcia i Productes Sanitaris, Generalitat de Valencia; Comité de Ética de la Investigación de Centro de Granada; Instituto Aragonés de Ciencias de la Salud (IACS); Comité Etico Investigación Clínica Regional del Principado de Asturias; Comité Etico Investigación Clínica Hospital 12 de Octubre; Comité Etico Investigación Clínica Hospital Universitario Virgen de la Arrixaca; Sección de Ordenación e Inspección Farmacéutica Departamento de Salud; Comité Ético de Investigación Clínica del Hospital Universitario del Río Hortega de Valladolid; Comissão de Ética para a Saúde (CES), Centro Hospitalar de Lisboa Ocidental, EPE; Comissão de Ética para a Saúde (CES), Centro Hospitalar do Porto, EPE; Comissão de Ética para a Saúde (CES), Centro Hospitalar Lisboa Central, EPE; Comissão de Ética para a Saúde (CES), Hospital Garcia de Orta, EPE; Comissão de Ética para a Saúde (CES), Centro Hospitalar de São João, EPE; Comissão de Ética para a Saúde (CES), Hospital Professor Doutor Fernando Fonseca, EPE; Comissão de Ética para a Saúde (CES), Centro Hospitalar do Algarve, EPE (Unidade de Faro); LUHS Kaunas Regional Biomedical Research Ethics Committee; Paula Stradina kliniskās universitātes slimnicas, Attīstības biedrības Klīniskās izpētes Ētika Etikas komiteja, Ethics Committee for Clinical Research; Komisija Republike Slovenije za medicinsko etiko; Comitato Etico Indipendente Presso La Fondazione Ptv Policlinico Tor Vergata Di Roma; Comitato Etico Regione Calabria Sezione Centro c/o A.O.U. Mater Domini Di Catanzaro; Comitato Etico Azienda Ospedaliera Universitaria Di Cagliari; Comitato Etico Cardarelli-Santobono c/o Ao Cardarelli; Comitato Etico Per La Sperimentazione Clinica Delle Province Di Verona E Rovigo, Presso Aoui Verona; Eticka Komise Fn Brno; Eticka Komisia Dfnsp Bratislava; Eticka Komisia Pri Dfn Kosice; Eticka Komisia Bratislavskeho Samospravneho Kraja; Comisia Naţională de Bioetică a Medicamentului şi a Dispozitivelor Medicale; Comitato Etico Milano area 1 c/o ASST FBF Sacco-P.O. L. Sacco; Comité de Ética de la Investigación de Centro Hospital Universitario Virgen del Rocío; Comité Ético de Investigación Clínica Fundació Sant Joan de Déu Generalitat de Catalunya. Departament de Salut; Comité Ético de Investigación Clínica Hospital Infantil Universitario Niño Jesús; Consejería de Sanidad Dirección General de Salus Pública Junta de Castilla León; Dirección General de Asistencia Sanitaria, Consejería de Sanidad Gobierno del Principado de Asturias; Dirección General de Planificación, Ordenación Sanitaria y Farmacéutica e Investigación, Consejeria de Sanidad y Política Social Región de Murcia; Ethics Committee at Moscow Institute of Pediatrics and Pediatric Surgery; Paula Stradina kliniskās universitātes slimnicas, Attistibas biedribas Kliniskās izpētes Etikas komiteja, Ethics Committee for Clinical Research; The First Affiliated Hospital of The Fourth Military Medical University; Zhongshan hospital fudan university. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
MR-FR, MF, AM, and JK: designing the study, collection of data, data interpretation, drafting, revising, final review, and approval of the manuscript. AH and BW: collection of data, data interpretation, drafting, revising, final review, and approval of the manuscript. RM and YH: data analysis, data interpretation, drafting, revising, final review, and approval of the manuscript. AR: designing the study, data analysis, data interpretation, drafting, revising, final review, and approval of the manuscript.
This study was funded by Novartis Pharmaceuticals Corporation.
Authors RM and YH are employees at Novartis and report stock ownership at Novartis. Author AR is an employee at Novartis.
MF reports consulting fees for being part of the scientific advisory board and TOSCA working committee; received speaker honoraria, support for travel, and payment for expert testimony from Novartis; and reports leadership or fiduciary role in the following: ILAE task force epilepsy surgery, ERN EpiCARE, ÖGKN, and ÖGfE. AM received honoraria and support for travel from Novartis. BW reports honoraria for a lecture from Takeda. JK received honoraria, support for travel, and research grant from Novartis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the patients and their families, investigators, and staff from all participating sites. The authors thank all the TOSCA PASS Investigators who contributed to this study. The authors thank Gowri Natarajan (Novartis Healthcare Pvt Ltd.) for providing medical writing support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.802334/full#supplementary-material
Annear, N. M. P., Appleton, R. E., Bassi, Z., Bhatt, R., Bolton, P. F., Crawford, P., et al. (2019). Tuberous Sclerosis Complex (TSC): Expert Recommendations for Provision of Coordinated Care. Front. Neurol. 10, 1116. doi:10.3389/fneur.2019.01116
Bissler, J. J., Kingswood, J. C., Radzikowska, E., Zonnenberg, B. A., Belousova, E., Frost, M. D., et al. (2017). Everolimus Long-Term Use in Patients with Tuberous Sclerosis Complex: Four-Year Update of the EXIST-2 Study. PLoS One 12 (8), e0180939. doi:10.1371/journal.pone.0180939
Bissler, J. J., Kingswood, J. C., Radzikowska, E., Zonnenberg, B. A., Frost, M., Belousova, E., et al. (2016). Everolimus for Renal Angiomyolipoma in Patients with Tuberous Sclerosis Complex or Sporadic Lymphangioleiomyomatosis: Extension of a Randomized Controlled Trial. Nephrol. Dial. Transpl. 31 (1), 111–119. doi:10.1093/ndt/gfv249
Bissler, J. J., Kingswood, J. C., Radzikowska, E., Zonnenberg, B. A., Frost, M., Belousova, E., et al. (2013). Everolimus for Angiomyolipoma Associated with Tuberous Sclerosis Complex or Sporadic Lymphangioleiomyomatosis (EXIST-2): a Multicentre, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 381 (9869), 817–824. doi:10.1016/S0140-6736(12)61767-X
Borkowska, J., Schwartz, R. A., Kotulska, K., and Jozwiak, S. (2011). Tuberous Sclerosis Complex: Tumors and Tumorigenesis. Int. J. Dermatol. 50 (1), 13–20. doi:10.1111/j.1365-4632.2010.04727.x
Capal, J. K., and Franz, D. N. (2016). Profile of Everolimus in the Treatment of Tuberous Sclerosis Complex: an Evidence-Based Review of its Place in Therapy. Neuropsychiatr. Dis. Treat. 12, 2165–2172. doi:10.2147/NDT.S91248
Crino, P. B., Nathanson, K. L., and Henske, E. P. (2006). The Tuberous Sclerosis Complex. N. Engl. J. Med. 355 (13), 1345–1356. doi:10.1056/NEJMra055323
Curatolo, P., Bombardieri, R., and Jozwiak, S. (2008). Tuberous Sclerosis. Lancet 372 (9639), 657–668. doi:10.1016/S0140-6736(08)61279-9
Curatolo, P., and Maria, B. L. (2013). Tuberous Sclerosis. Handb Clin. Neurol. 111, 323–331. doi:10.1016/B978-0-444-52891-9.00038-5
Curatolo, P., Moavero, R., and de Vries, P. J. (2015). Neurological and Neuropsychiatric Aspects of Tuberous Sclerosis Complex. Lancet Neurol. 14 (7), 733–745. doi:10.1016/S1474-4422(15)00069-1
Dabora, S. L., Jozwiak, S., Franz, D. N., Roberts, P. S., Nieto, A., Chung, J., et al. (2001). Mutational Analysis in a Cohort of 224 Tuberous Sclerosis Patients Indicates Increased Severity of TSC2, Compared with TSC1, Disease in Multiple Organs. Am. J. Hum. Genet. 68 (1), 64–80. doi:10.1086/316951
Davies, D. M., de Vries, P. J., Johnson, S. R., McCartney, D. L., Cox, J. A., Serra, A. L., et al. (2011). Sirolimus Therapy for Angiomyolipoma in Tuberous Sclerosis and Sporadic Lymphangioleiomyomatosis: a Phase 2 Trial. Clin. Cancer Res. 17 (12), 4071–4081. doi:10.1158/1078-0432.CCR-11-0445
Davies, M., Saxena, A., and Kingswood, J. C. (2017). Management of Everolimus-Associated Adverse Events in Patients with Tuberous Sclerosis Complex: a Practical Guide. Orphanet J. Rare Dis. 12 (1), 35. doi:10.1186/s13023-017-0581-9
de Vries, P. J., Belousova, E., Benedik, M. P., Carter, T., Cottin, V., Curatolo, P., et al. (2018). TSC-associated Neuropsychiatric Disorders (TAND): Findings from the TOSCA Natural History Study. Orphanet J. Rare Dis. 13 (1), 157. doi:10.1186/s13023-018-0901-8
de Vries, P. J., Whittemore, V. H., Leclezio, L., Byars, A. W., Dunn, D., Ess, K. C., et al. (2015). Tuberous Sclerosis Associated Neuropsychiatric Disorders (TAND) and the TAND Checklist. Pediatr. Neurol. 52 (1), 25–35. doi:10.1016/j.pediatrneurol.2014.10.004
Franz, D. N., Belousova, E., Sparagana, S., Bebin, E. M., Frost, M., Kuperman, R., et al. (2014). Everolimus for Subependymal Giant Cell Astrocytoma in Patients with Tuberous Sclerosis Complex: 2-year Open-Label Extension of the Randomised EXIST-1 Study. Lancet Oncol. 15 (13), 1513–1520. doi:10.1016/S1470-2045(14)70489-9
Franz, D. N., Belousova, E., Sparagana, S., Bebin, E. M., Frost, M., Kuperman, R., et al. (2013). Efficacy and Safety of Everolimus for Subependymal Giant Cell Astrocytomas Associated with Tuberous Sclerosis Complex (EXIST-1): a Multicentre, Randomised, Placebo-Controlled Phase 3 Trial. Lancet 381 (9861), 125–132. doi:10.1016/S0140-6736(12)61134-9
Franz, D. N., Belousova, E., Sparagana, S., Bebin, E. M., Frost, M. D., Kuperman, R., et al. (2016). Long-Term Use of Everolimus in Patients with Tuberous Sclerosis Complex: Final Results from the EXIST-1 Study. PLoS One 11 (6), e0158476. doi:10.1371/journal.pone.0158476
Franz, D. N., Bissler, J. J., and McCormack, F. X. (2010). Tuberous Sclerosis Complex: Neurological, Renal and Pulmonary Manifestations. Neuropediatrics 41 (5), 199–208. doi:10.1055/s-0030-1269906
Franz, D. N., and Krueger, D. A. (2018). mTOR Inhibitor Therapy as a Disease Modifying Therapy for Tuberous Sclerosis Complex. Am. J. Med. Genet. C Semin. Med. Genet. 178 (3), 365–373. doi:10.1002/ajmg.c.31655
Franz, D. N., Lawson, J. A., Yapici, Z., Ikeda, H., Polster, T., Nabbout, R., et al. (2018). Everolimus for Treatment-Refractory Seizures in TSC: Extension of a Randomized Controlled Trial. Neurol. Clin. Pract. 8 (5), 412–420. doi:10.1212/CPJ.0000000000000514
French, J. A., Lawson, J. A., Yapici, Z., Ikeda, H., Polster, T., Nabbout, R., et al. (2016). Adjunctive Everolimus Therapy for Treatment-Resistant Focal-Onset Seizures Associated with Tuberous Sclerosis (EXIST-3): a Phase 3, Randomised, Double-Blind, Placebo-Controlled Study. Lancet 388 (10056), 2153–2163. doi:10.1016/S0140-6736(16)31419-2
Huang, J., and Manning, B. D. (2008). The TSC1-TSC2 Complex: a Molecular Switchboard Controlling Cell Growth. Biochem. J. 412 (2), 179–190. doi:10.1042/BJ20080281
Iqbal, Z., Kingswood, J. C., and Sayer, J. A. (2017). Tuberous Sclerosis Complex and Renal Angiomyolipomas. Br. J. Ren. Med. 22 (1), 25–29.
Jansen, A. C., Vanclooster, S., de Vries, P. J., Fladrowski, C., Beaure d'Augères, G., Carter, T., et al. (2020). Burden of Illness and Quality of Life in Tuberous Sclerosis Complex: Findings from the TOSCA Study. Front. Neurol. 11, 904. doi:10.3389/fneur.2020.00904
Jozwiak, J., Jozwiak, S., and Wlodarski, P. (2008). Possible Mechanisms of Disease Development in Tuberous Sclerosis. Lancet Oncol. 9 (1), 73–79. doi:10.1016/S1470-2045(07)70411-4
Józwiak, S., Schwartz, R. A., Janniger, C. K., and Bielicka-Cymerman, J. (2000). Usefulness of Diagnostic Criteria of Tuberous Sclerosis Complex in Pediatric Patients. J. Child. Neurol. 15 (10), 652–659. doi:10.1177/088307380001501003
Kingswood, J. C., Bruzzi, P., Curatolo, P., de Vries, P. J., Fladrowski, C., Hertzberg, C., et al. (2014). TOSCA - First International Registry to Address Knowledge Gaps in the Natural History and Management of Tuberous Sclerosis Complex. Orphanet J. Rare Dis. 9, 182. doi:10.1186/s13023-014-0182-9
Kingswood, J. C., d'Augères, G. B., Belousova, E., Ferreira, J. C., Carter, T., Castellana, R., et al. (2017). TuberOus SClerosis Registry to Increase Disease Awareness (TOSCA) - Baseline Data on 2093 Patients. Orphanet J. Rare Dis. 12 (1), 2. doi:10.1186/s13023-016-0553-5
Kingswood, J. C., Belousova, E., Benedik, M. P., Budde, K., Carter, T., Cottin, V., et al. (2021). TuberOus SClerosis Registry to increAse Disease Awareness (TOSCA) Post-Authorisation Safety Study of Everolimus in Patients with Tuberous Sclerosis Complex. Front. Neurol. 12 (228), 12. doi:10.3389/fneur.2021.630378
Krueger, D. A., Care, M. M., Agricola, K., Tudor, C., Mays, M., and Franz, D. N. (2013). Everolimus Long-Term Safety and Efficacy in Subependymal Giant Cell Astrocytoma. Neurology 80 (6), 574–580. doi:10.1212/WNL.0b013e3182815428
Krueger, D. A., and Northrup, H. (2013). Tuberous Sclerosis Complex Surveillance and Management: Recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr. Neurol. 49 (4), 255–265. doi:10.1016/j.pediatrneurol.2013.08.002
Kwiatkowski, D. J., and Manning, B. D. (2005). Tuberous Sclerosis: a GAP at the Crossroads of Multiple Signaling Pathways. Hum. Mol. Genet. 14 (2), R251–R258. doi:10.1093/hmg/ddi260
McCormack, F. X., Inoue, Y., Moss, J., Singer, L. G., Strange, C., Nakata, K., et al. (2011). Efficacy and Safety of Sirolimus in Lymphangioleiomyomatosis. N. Engl. J. Med. 364 (17), 1595–1606. doi:10.1056/NEJMoa1100391
Northrup, H., Aronow, M. E., Bebin, E. M., Bissler, J., Darling, T. N., de Vries, P. J., et al. (2021). Updated International Tuberous Sclerosis Complex Diagnostic Criteria and Surveillance and Management Recommendations. Pediatr. Neurol. 123, 50–66. doi:10.1016/j.pediatrneurol.2021.07.011
Prather, P., and de Vries, P. J. (2004). Behavioral and Cognitive Aspects of Tuberous Sclerosis Complex. J. Child. Neurol. 19 (9), 666–674. doi:10.1177/08830738040190090601
Tran, L. H., and Zupanc, M. L. (2015). Long-Term Everolimus Treatment in Individuals with Tuberous Sclerosis Complex: A Review of the Current Literature. Pediatr. Neurol. 53 (1), 23–30. doi:10.1016/j.pediatrneurol.2014.10.024
Trelinska, J., Dachowska, I., Kotulska, K., Fendler, W., Jozwiak, S., and Mlynarski, W. (2015). Complications of Mammalian Target of Rapamycin Inhibitor Anticancer Treatment Among Patients with Tuberous Sclerosis Complex Are Common and Occasionally Life-Threatening. Anticancer Drugs 26 (4), 437–442. doi:10.1097/CAD.0000000000000207
Tyburczy, M. E., Dies, K. A., Glass, J., Camposano, S., Chekaluk, Y., Thorner, A. R., et al. (2015). Mosaic and Intronic Mutations in TSC1/TSC2 Explain the Majority of TSC Patients with No Mutation Identified by Conventional Testing. Plos Genet. 11 (11), e1005637. doi:10.1371/journal.pgen.1005637
Keywords: tuberous sclerosis complex (TSC), everolimus, TOSCA, post-authorization safety study (PASS), real-world evidence (RWE)
Citation: Ruiz-Falcó Rojas ML, Feucht M, Macaya A, Wilken B, Hahn A, Maamari R, Hirschberg Y, Ridolfi A and Kingswood JC (2022) Real-World Evidence Study on the Long-Term Safety of Everolimus in Patients With Tuberous Sclerosis Complex: Final Analysis Results. Front. Pharmacol. 13:802334. doi: 10.3389/fphar.2022.802334
Received: 01 November 2021; Accepted: 07 March 2022;
Published: 08 April 2022.
Edited by:
Elham Rahme, McGill University, CanadaReviewed by:
Luca Gallelli, University of Catanzaro, ItalyCopyright © 2022 Ruiz-Falcó Rojas, Feucht, Macaya, Wilken, Hahn, Maamari, Hirschberg, Ridolfi and Kingswood. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Luz Ruiz-Falcó Rojas, bWFyaWx1ekBydWl6LWZhbGNvLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.