 Zhigang Guo
Zhigang Guo Liguang Zheng
Liguang Zheng Mengyuan Fu
Mengyuan Fu Huangqianyu Li
Huangqianyu Li Lin Bai
Lin Bai Xiaodong Guan
Xiaodong Guan Luwen Shi
Luwen Shi
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 03 February 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.802219
This article is part of the Research Topic Mitigating Implicit Bias and promoting Compassionate Behavior in Public Health/Healthcare Professionals: Implications for Treatment Outcomes View all 7 articles
The full coverage policy for essential medicines (FCPEMs) was proposed and implemented in Taizhou city of Zhejiang Province, China, to promote equal access and adherence to medicines. This study aimed to examine the effects of FCPEMs on the income-related inequality in medication adherence among local patients with hypertension or diabetes. We collected electronic health records of patients with hypertension or diabetes of three districts of Taizhou from 2011 to 2016. As the implementation schedule of the FCPEMs varied across districts, we applied a retrospective longitudinal study design and assigned records from 1 year before to 3 years following the implementation of FCPEMs as baseline and follow-up data. We thus generated a dataset with 4-year longitudinal data. The concentration index (CI) and its decomposition method were employed to measure factors contributing to inequality in medication adherence and the role played by FCPEMs. The sample size rose from 264,836 at the baseline to 315,677, 340,512, and 355,676 by each follow-up year, and the proportion of patients taking free medicines rose from 17.6 to 25.0 and 29.8% after FCPEMs implementation. The proportion of patients with high adherence increased from 39.9% at baseline to 51.6, 57.2, and 60.5%, while CI decreased from 0.073 to −0.011, −0.029, and −0.035. The contribution of FCPEMs ranked at 2nd/13, 7th/13, and 2nd/13 after the implementation of FCPEMs. Changes in CI of medication adherence for every 2 years were −0.084, −0.018, and −0.006, and the contribution of FCPEMs was −0.006, 0.006, and 0.007, ranking at 2nd/13, 2nd/13, and 1st/13, respectively. Most changes in CI of medication adherence can be attributed to FCPEMs. The medication adherence of patients with hypertension or diabetes improved after the implementation FCPEMs in Taizhou, although inequality did not improve consistently. In general, FCPEMs could be a protective factor against income-related inequalities in access and adherence to medicines. Future research is needed to investigate the change mechanism and the optimal design of similar interventions.
Unequal access to medicines is a universal problem for health-care system reforms (Kolasa and Kowalczyk, 2016). It exacerbates a phenomenon well documented in the literature that people from lower income and minority groups experience higher health risks and are more vulnerable to medication costs (Fu et al., 2020; Pinto et al., 2020). The full coverage policy for medicines (FCPMs) is a policy strategy to promote equal access and adherence to medicines. Depending on specific contexts, FCPMs may also be known as “free,” “full reimbursement,” or “fee exemption” medicine policy. According to the Pharmaceutical Country Profiles by the World Health Organization, all 105 listed countries had implemented FCPMs to some extent. Among these countries, 54 had full coverage programs for any essential medicines (Wang et al., 2019). FCPMs is also increasingly studied and implemented in hypertension and diabetes interventions in the United States (Zheng et al., 2017; Ross-Degnan et al., 2020), Canada (Laba et al., 2020), Brazil (Emmerick et al., 2020), Spain (Puig-Junoy et al., 2016; Gonzalez et al., 2017), Madagascar (Garchitorena et al., 2017), India (Bose and Dutta, 2018), and Burkina Faso (Yaogo, 2017).
China has adopted FCPMs for antihypertensive and hypoglycemic medicines. By the end of 2020, 16 provinces had selected at least one district/county as the pilot area(s) to explore various policy strategies to manage hypertension and diabetes (Yu et al., 2013; Chen and Pan, 2019; Wang et al., 2019; Gong et al., 2020). In 2011, Taizhou, Zhejiang, was among the first cities to implement the full coverage policy for essential medicines (FCPEMs). The policy was set out to be as follows: 1) all nine districts/counties administered by Taizhou city were required to develop a full-coverage medication catalog between 2012 and 2013, specifying what medicines for hypertension and diabetes listed in the National Essential Medicines List of China (version 2012) would be covered in full. 2) Eligible patients could access medicines listed in this catalog without any costs, including drug, prescription, and related medical costs, at any primary care or designated facilities. 3) Physicians at primary care and designated facilities were responsible for evaluating selected medicines’ clinical benefits and appropriateness for patients, and adjusting the medication plan if clinical outcomes were poor. 4) As part of the basic public health services, China had been establishing health records and providing free chronic disease management services for every patient with hypertension and diabetes from the new healthcare reform in 2009 (Li et al., 2017; Lai et al., 2021). All hypertension and diabetes patients using medicines covered must be enrolled in chronic disease management services and have their medication and disease management plan incorporated into health records.
Studies indicated that FCPMs and FCPEMs could reduce medicine-related costs for patients, improve affordability and accessibility of covered medicines, and promote medication adherence (Choudhry et al., 2011; Kolasa and Kowalczyk, 2016; Wang et al., 2019). It can also help with disease prevention and control (Yu et al., 2013) and help in achieving more economical benefits for the society (Ito et al., 2015). There is emerging evidence that implementation of FCPMs and FCPEMs would favorably benefit vulnerable populations in accessing medications (Yu et al., 2013; Kolasa and Kowalczyk, 2016; Gonzalez et al., 2017; Yaogo, 2017), though this is better supported by further investigations. Therefore, we aimed to analyze the change in medication adherence before and after the implementation of FCPEMs in Taizhou and to explore the policy’s effects on income-related inequality in its first years’ implementation.
Taizhou is a prefecture-level city with a total area of 10,050 km2 in Zhejiang Province, located in the central area of the Yangtze River Delta in China. The city administers three urban districts (Jiaojiang, Huangyan, and Luqiao), three county-level cities (Linhai, Wenling, and Yuhuan), and three counties (Tianhai, Xianju, and Sanmen). In 2016, Taizhou had a population of 5.2 million, with 9.1% of them older than 65 years and 19.3% aged 45–64 years. The annual disposable income per capita was 5321.5 dollars. The average number of health professionals, hospital beds, physicians, and nurses for every thousand residents was 6.8, 4.5, 2.8, and 2.7, respectively (Taizhou Bureau of Statistics, 2017).
In 2017, we collected electronic health records of patients with hypertension or diabetes from 2011 to 2016, which included patients’ demographics and regular follow-up data (e.g., medicines prescribed, level of medication adherence, and health behaviors such as smoking and drinking) (Li et al., 2017). We used a retrospective longitudinal study design to analyze the impact of FCPEMs. As the policy was implemented in the nine districts/counties with different schedules, patient records collected 12 months prior to policy implementation were regarded as baseline data. Records of 1–12 months, 13–24 months, and 25–36 months after policy implementation were regarded jointly as follow-up data. Thus, we generated a set of 4-year retrospective longitudinal data. Due to system upgrades, only data of Huangyan district, Linhai city, and Wenling city were unabridged and eligible over the study period. Therefore, the analysis of this study was limited to patients residing in these three areas. The policy implementation schedule and the medicine catalog for each area are shown in Supplementary Appendix Table S1.
According to the Chronic Disease Management Services of China (Lai et al., 2021), family physicians should administer follow-up surveys regularly (every 3 months) to monitor disease status. In Taizhou, medication adherence would be assessed in follow-up surveys and be translated into three categories: “regular medication use,” “irregular medication use,” and “taking no medication.” Patients taking medicines strictly following the prescribed schedule were assigned “regular medication use,” and patients reporting no medicine use was were assigned “taking no medication.” The remaining would be categorized into “irregular medication use.” In our analysis, “regular medication use” was treated as high adherence (computed as 1), and “irregular medication use” and “taking no medication” were regarded as poor adherence (computed as 0).
If the patient had used the medicines covered under FCEMPs in the given year, they would be categorized as FCPEM covered (computed as 1), otherwise as not covered (computed as 0).
Based on a previous research (Marsicano et al., 2015; Cathbert, 2019; Sipos et al., 2021), our analysis also included the following regular follow-up variables which might impact medication adherence (Table 1): gender, age, income group (the low-/middle-/high-income group with one-third of population by rank of the annual household income), hukou status, residential area, marital status, employment status, education level, medical insurance, smoking, drinking, and disease type.
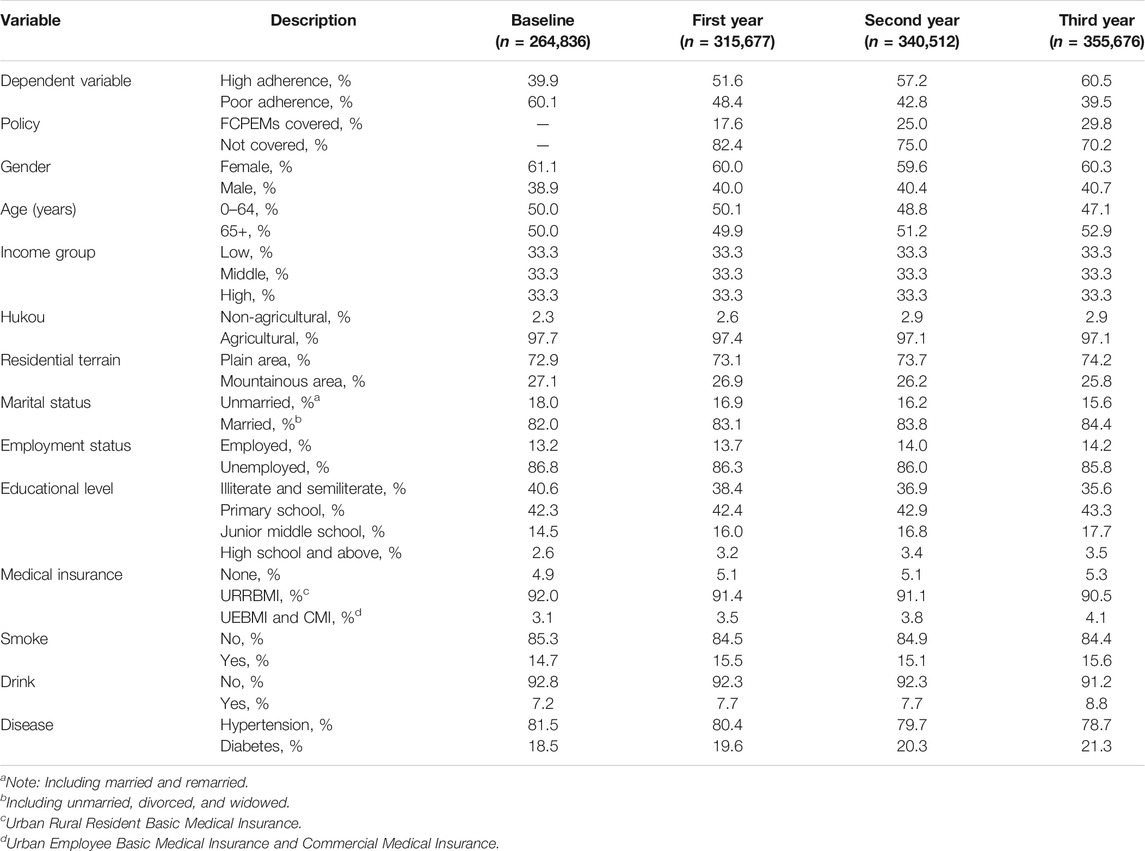
TABLE 1. Characteristics of the study population in the 4 years.
The concentration index (CI) and its decomposition recommended by Wagstaff and Van Doorslaer were applied to analyze the inequality of medication adherence and the contribution of the determinant factors (Fu et al., 2020; Lai et al., 2021). The calculation formula of CI is as follows:
where
where
In order to understand the effect of FCPEMs on medication adherence, the Oaxaca-type decomposition (Pulok et al., 2020) is applied, and the equation is as follows:
where
Table 1 shows the characteristics of the study population from baseline to 3 years after the implementation of FCPEMs. The sample size rose from 264,836 at baseline to 315,677, 340,512, and 355,676 patients by each follow-up year, of which 81.5, 80.4, 79.7, and 78.7% were patients with hypertension, respectively. Over the study period, the proportion of patients with high adherence increased from 39.9% to 51.6, 57.2, and 60.5%. The proportion of patients taking free medicines also increased with time, from 17.6 to 25.0% and 29.8% after the FCPEMs.
Table 2 demonstrates changes in medication adherence, stratified by income, and CI of medication adherence over the 4 years. Patients from all income groups experienced varying degrees of improvement in medication adherence. Patients from the low-income group experienced largest improvement (from 33.2% to 53.0, 61.2, and 65.4%), followed by patients from the middle-income group (from 42.6% to 51.6, 56.6, and 59.3%). Patients from the high-income group experienced the smallest increase in the adherence rate, from 44.6% to 50.2, 53.6, and 56.5%. CI of medication adherence decreased from 0.073 to −0.011, −0.029, and −0.035, showing an increasing favorability of FCPEMs’ effects toward the lower income.

TABLE 2. Medication adherence and CI of the 4 years.
Table 3 presents the elasticity and the rate of contribution of determinants on CI of medication adherence over the 4 years. During the follow-up period, the elasticity of the policy increased from 0.103 to 0.131, 0.141, respectively, implying that the positive association between CI of the policy and medication adherence strengthened overtime. The rate of the contribution of the policy to medication adherence changed from 54.792 to 1.223% and −19.092% by the end of each follow-up year, respectively. Its ranking dropped from 2nd/13 at the end of the first follow-up year to 7th/13 by the second year and climbed back to 2nd/13 by the end of the follow-up period. Meanwhile, the CI of medication adherence were −0.011, −0.029, and −0.035, respectively. FCPEMs was a pro-poor contributing factor at the initial 2 years of implementation and a pro-rich contribution factor in the third year.
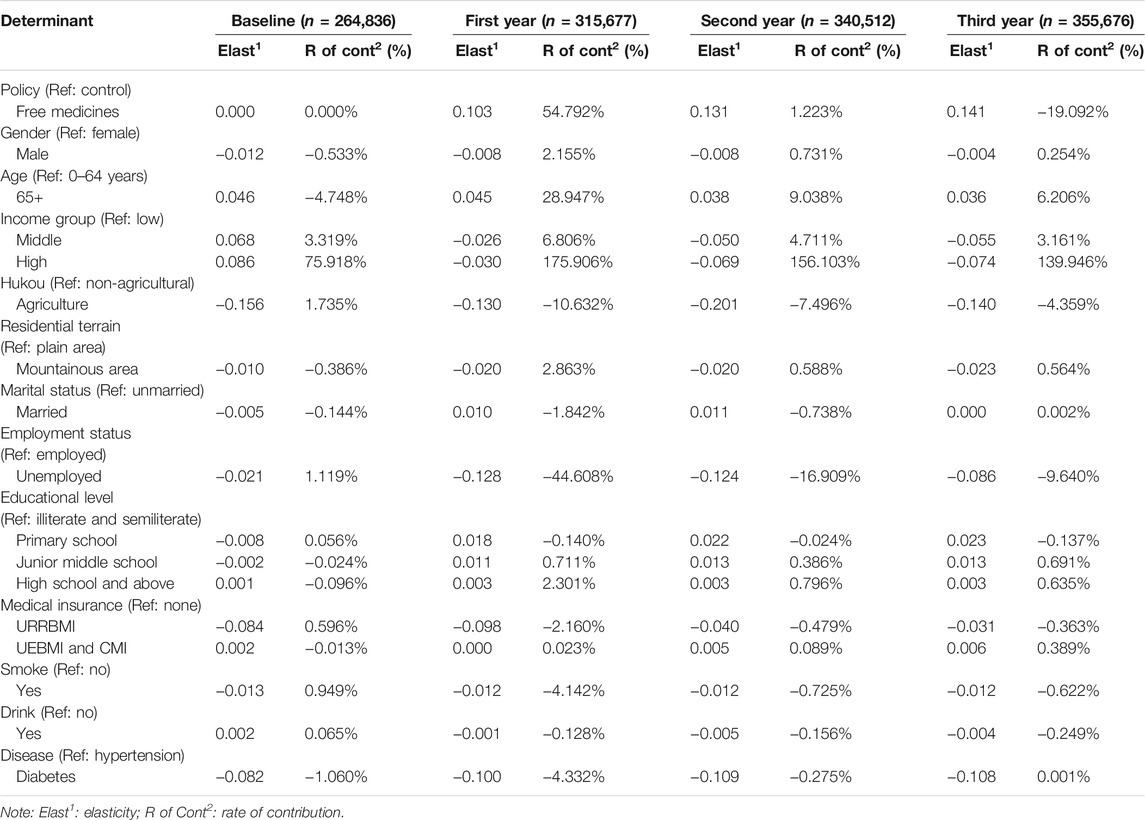
TABLE 3. Decomposition of CI in medication adherence over the 4 years.
Table 4 presents the contribution of all determinants in changes medication adherence every 2 years, with an Oaxaca-type decomposition. The change in CI in medication adherence was −0.084, −0.018, and −0.006 for every 2 years from baseline to 3 years after FCPEMs, of which the contribution of the FCPEMs was −0.0061, 0.0057, and 0.0070 and it ranked at the 2nd/13, 2nd/13, and 1st/13 place, respectively. From the results of the Oaxaca-type decomposition, the contribution of the policy was mainly attributable to the changes in CI of FCPEMs (−0.0061, 0.0074, and 0.0070) and experienced a minor impact by the changes of sensitivity (0.0000, −0.0017, and 0.0000).
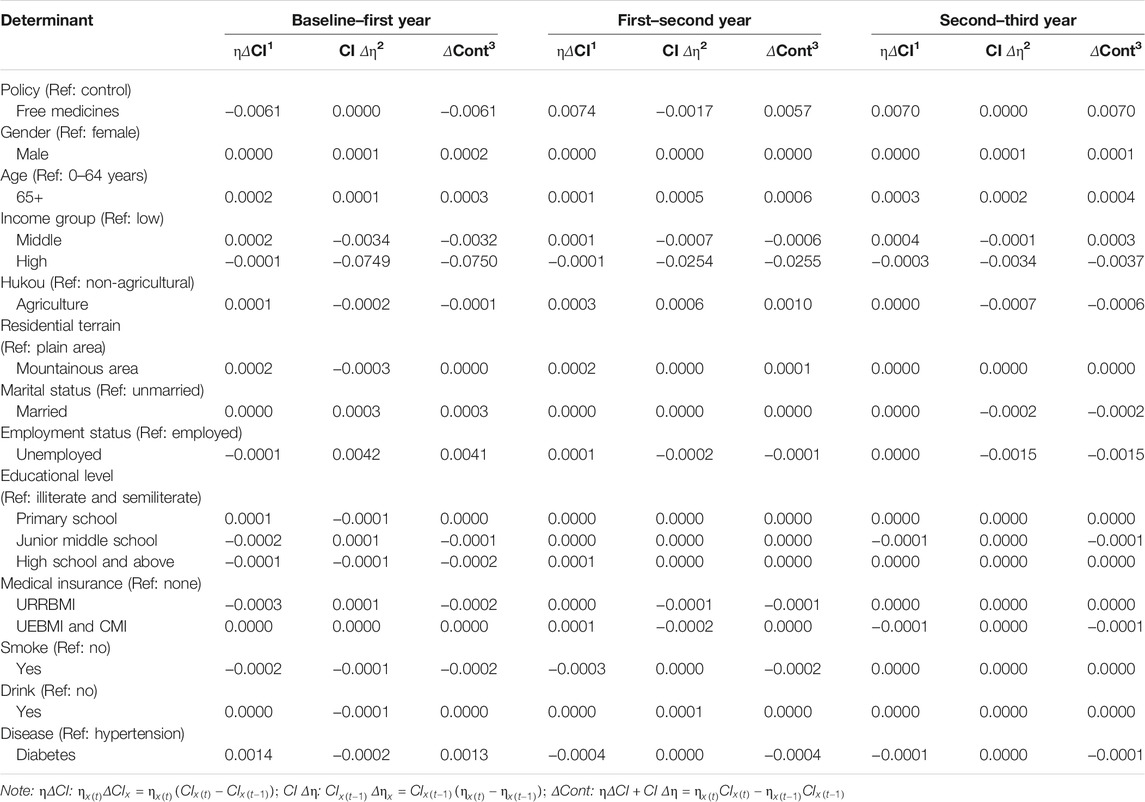
TABLE 4. Oaxaca decomposition of CI in medication adherence over the 4 years.
This study examined income-related inequalities in medicine adherence using a retrospective longitudinal study design and a sample of patients with hypertension or diabetes in Taizhou, China. We identified that FCPEMs promoted overall medication adherence and favorably benefited patients from the low-income group over patients from other income groups.
Our study results are consistent with similar studies in a sense that medication adherence among patients improved after the implementation of FCPEMs and that largest improvement was observed in low-income population. With an increasing proportion of patients taking covered medicines by each year, medication adherence of the general population improved. In other studies of FCPMs, low-income patients who converted from poor to high medication adherence contributed to an increase of 7.8% in medication adherence to statins (Gonzalez et al., 2017) and increased twice more than the high-income patients with diabetes (Ross-Degnan et al., 2020).
Although the income-related inequality in medication adherence did not show consistent improvement over the follow-up period, FCPEMs was effective in improving the inequality in medication adherence. Over the study period, the inequality of medication adherence improved in the first 2 years, but the outcome was conversed in the latter 2 years. In this process, FCPEMs helped in mitigating the changes of inequality. As two studies showed, FCPMs for cardiovascular disease and cancer reduced racial and ethnic disparities in medicines between white and non-white patients after an episode of myocardial infarction (Choudhry et al., 2014; Cole et al., 2020). For the exacerbated inequality, income group (high) was still the greatest barrier to realize equality, and FCPEMs became a positive element against it. As many studies suggest, medication non-adherence is significantly associated with low income (Sunny et al., 2020; Riley et al., 2021). Our study shows that FCPEMs could be a protecting factor against this income-related inequality in medication adherence experienced by low-income patients with hypertension and diabetes. This echoes a Targeted Poverty Alleviation program in China demonstrating that FCPMs could protect low-income patients against heavy burden of medicine costs (Chen and Pan, 2019).
However, due to the comprehensive impact of various factors, FCPEMs not always favorably benefited low-income patients. In our study, we knew change in CI of FCPEMs was the main contributor. The proportion of patients taking free medicines of different groups was thus the key to achieving sustainable equality in access and adherence to covered medicines. However, factors contributing to uptake of free medicines varied. One study showed that lower medication adherence among patients from high-income groups could result from a mismatch of free medicines with their health needs (Marsicano et al., 2015). Another study showed that age was a promoting factor for the uptake of free medicines; 40% of the older adults used free medicines to ameliorate their burden of medicine costs (Tavares et al., 2016). In this study, we found that the uptake of free medicines might be positively associated with an increase in free medicines covered by the catalog (Supplementary Appendix Table S1). We can reasonably conclude that the more health needs the medicines covered under FCPMs could meet, the more likely FCPMs could improve inequality in accessing and adherence to medicines. The geographical accessibility of designated health facilities (Emmerick et al., 2017), qualification of health professionals and pharmacists at these facilities (Zombre et al., 2017; Varas-Doval et al., 2020), and support from families and social networks (Tavares et al., 2016; Zhou et al., 2021) were also critical factors to consider.
It is also worth noting that long-term longitudinal data are necessary for evaluating the inequality in medication adherence and revising the FCPMs programs accordingly. If we only used 1-year data in this study after FCPEMs, the results and conclusions would be different or opposite. Meanwhile, medication adherence is influenced by many factors, thus it would need a comprehensive reform to improve inequality (Fosse-Edorh et al., 2015; Kolasa and Kowalczyk, 2016). During the reform, long-term longitudinal data were important for exhibiting the dynamic results (Zombre et al., 2017) and adjust the intervention precisely, such as the FCPEMs and FCPMs. All these highlighted the value of 4-year longitudinal data used by this study.
Nevertheless, our study has several limitations. First, the prevalence of hypertension and diabetes among residents registered in the local EMR database was 11.2 and 3.2%, respectively, in 2016, which were lower than the disease prevalence shown by epidemiological data (Li, 2021; Li et al., 2021; Xia et al., 2021). This implies a participant bias and that our sample might not be fully representative of the general population residing in Taizhou. Second, our measurement of the medication adherence was also subject to recall bias and administration bias as health records and follow-up surveys were collected by medical staffs, who might have varying degrees of training in administering surveys. Third, our results might have been affected by missing data and influence factors in the database, such as comorbidities. We made controls for this by aggregating all medical records of a patient within one calendar year into an annual data input. Patients with missing data after data aggregation were excluded from our study. Last, our baseline covered only 1 year as the database for chronic disease management was only established since 2011, and data prior to the year were inaccessible. This study schedule might influence the interpretation of our longitudinal data. However, we identified no other significant policy during local investigations, and our result that FCPEMs was a major driver for improvements in medication adherence still holds.
In conclusion, overall medication adherence of the study population improved after the implementation of FCPEMs in Taizhou, and the low-income population experienced the largest increase in adherence to medicines. Interventions in the future should look into designing an optimal medicine catalog by first investigating the health needs of local residents to promote intervention uptake.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
Data of this study were from the electronic health records of Taizhou city, China, and were retrospective without direct contact with human subjects. Data usage was permitted by the Local Department of Health. Before we received the data, all information was anonymized and de-identified through a privacy protection process. Ethical approval for this study was obtained from the Peking University Institutional Review Board (IRB00001052-18024-Exemption). All authors confirm that methods of the study were carried out in accordance with relevant guidelines and regulations.
ZG, XG, and LS proposed the study and participated in the design, data collection and analysis, and drafting of the manuscript. LZ, MF, HL, and LB participated in data collection and analysis and provided comments on the manuscript. All authors read and approved the final manuscript.
This study was supported by the National Natural Science Foundation of China (71774005 and 72104011) and Beijing Natural Science Foundation (9204031). The foundations had no role in the study design, data collection, data analysis and interpretation, writing of the manuscript, and the decision to publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors sincerely thank all participants from the local health department and acknowledge the Center for Disease Control and Prevention of Taizhou city, Zhejiang Province, China. We appreciate the editor and anonymous reviewers for all the suggestions and valuable comments.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.802219/full#supplementary-material
Bose, M., and Dutta, A. (2018). Health Financing Strategies to Reduce Out-Of-Pocket burden in India: a Comparative Study of Three States. BMC Health Serv. Res. 18 (1), 830. doi:10.1186/s12913-018-3633-5
Cathbert, T. (2019). Affordability Effect of Diabetic Medicine on Patient's Treatment Adherence Case Study: Itojo Hospital in Ntungamo District. Diabetes Metab. Syndr. 13 (3), 2025–2031. doi:10.1016/j.dsx.2019.04.029
Chen, C., and Pan, J. (2019). The Effect of the Health Poverty Alleviation Project on Financial Risk protection for Rural Residents: Evidence from Chishui City, China. Int. J. Equity Health 18 (1), 79. doi:10.1186/s12939-019-0982-6
Choudhry, N. K., Avorn, J., Glynn, R. J., Antman, E. M., Schneeweiss, S., Toscano, M., et al. (2011). Full Coverage for Preventive Medications after Myocardial Infarction. N. Engl. J. Med. 365 (22), 2088–2097. doi:10.1056/NEJMsa1107913
Choudhry, N. K., Bykov, K., Shrank, W. H., Toscano, M., Rawlins, W. S., Reisman, L., et al. (2014). Eliminating Medication Copayments Reduces Disparities in Cardiovascular Care. Health Aff. (Millwood) 33 (5), 863–870. doi:10.1377/hlthaff.2013.0654
Cole, M. B., Ellison, J. E., and Trivedi, A. N. (2020). Association between High-Deductible Health Plans and Disparities in Access to Care Among Cancer Survivors. JAMA Netw. Open 3 (6), e208965. doi:10.1001/jamanetworkopen.2020.8965
Emmerick, I. C. M., Campos, M. R., da Silva, R. M., Chaves, L. A., Bertoldi, A. D., Ross-Degnan, D., et al. (2020). Hypertension and Diabetes Treatment Affordability and Government Expenditures Following Changes in Patient Cost Sharing in the "Farmácia Popular" Program in Brazil: an Interrupted Time Series Study. BMC Public Health 20 (1), 24. doi:10.1186/s12889-019-8095-0
Emmerick, I. C. M., Campos, M. R., Luiza, V. L., Chaves, L. A., Bertoldi, A. D., and Ross-Degnan, D. (2017). Retrospective Interrupted Time Series Examining Hypertension and Diabetes Medicines Usage Following Changes in Patient Cost Sharing in the 'Farmácia Popular' Programme in Brazil. BMJ Open 7 (11), e017308. doi:10.1136/bmjopen-2017-017308
Fosse-Edorh, S., Fagot-Campagna, A., Detournay, B., Bihan, H., Eschwege, E., Gautier, A., et al. (2015). Impact of Socio-Economic Position on Health and Quality of Care in Adults with Type 2 Diabetes in France: the Entred 2007 Study. Diabet Med. 32 (11), 1438–1444. doi:10.1111/dme.12783
Fu, X. Z., Wang, L. K., Sun, C. Q., Wang, D. D., He, J. J., Tang, Q. X., et al. (2020). Inequity in Inpatient Services Utilization: a Longitudinal Comparative Analysis of Middle-Aged and Elderly Patients with the Chronic Non-communicable Diseases in China. Int. J. Equity Health 19 (1), 6. doi:10.1186/s12939-019-1117-9
Garchitorena, A., Miller, A. C., Cordier, L. F., Ramananjato, R., Rabeza, V. R., Murray, M., et al. (2017). In Madagascar, Use of Health Care Services Increased when Fees Were Removed: Lessons for Universal Health Coverage. Health Aff. (Millwood) 36 (8), 1443–1451. doi:10.1377/hlthaff.2016.1419
Gong, W., Zhang, C., Xu, D. R., Xiao, S., Yu, Y., and Caine, E. D. (2020). The Association between a Free Medicine Program and Functioning in People with Schizophrenia: a Cross-Sectional Study in Liuyang, China. PeerJ 8, e8929. doi:10.7717/peerj.8929
González López-Valcárcel, B., Librero, J., García-Sempere, A., Peña, L. M., Bauer, S., Puig-Junoy, J., et al. (2017). Effect of Cost Sharing on Adherence to Evidence-Based Medications in Patients with Acute Coronary Syndrome. Heart 103 (14), 1082–1088. doi:10.1136/heartjnl-2016-310610
Ito, K., Avorn, J., Shrank, W. H., Toscano, M., Spettel, C., Brennan, T., et al. (2015). Long-term Cost-Effectiveness of Providing Full Coverage for Preventive Medications after Myocardial Infarction. Circ. Cardiovasc. Qual. Outcomes 8 (3), 252–259. doi:10.1161/CIRCOUTCOMES.114.001330
Kolasa, K., and Kowalczyk, M. (2016). Does Cost Sharing Do More Harm or More Good? - a Systematic Literature Review. BMC Public Health 16, 992. doi:10.1186/s12889-016-3624-6
Laba, T. L., Cheng, L., Worthington, H. C., Mcgrail, K. M., Chan, F. K. I., Mamdani, M., et al. (2020). What Happens to Drug Use and Expenditure when Cost Sharing Is Completely Removed? Evidence from a Canadian Provincial Public Drug Plan. Health Policy 124 (9), 977–983. doi:10.1016/j.healthpol.2020.05.001
Lai, S., Lu, L., Zhou, Z., Shen, C., Yang, X., Zhao, Y., et al. (2021). The Effects of Family Physician-Contracted Service on Health-Related Quality of Life and Equity in Health in China. Int. J. Equity Health 20 (1), 15. doi:10.1186/s12939-020-01348-4
Li, C., Chen, K., Cornelius, V., Tomeny, E., Wang, Y., Yang, X., et al. (2021). Applicability and Cost-Effectiveness of the Systolic Blood Pressure Intervention Trial (SPRINT) in the Chinese Population: A Cost-Effectiveness Modeling Study. Plos Med. 18 (3), e1003515. doi:10.1371/journal.pmed.1003515
Li, X., Li, Z., Liu, C., Zhang, J., Sun, Z., Feng, Y., et al. (2017). Evaluation of the Three-In-One Team-Based Care Model on Hierarchical Diagnosis and Treatment Patterns Among Patients with Diabetes: a Retrospective Cohort Study Using Xiamen's Regional Electronic Health Records. BMC Health Serv. Res. 17 (1), 779. doi:10.1186/s12913-017-2705-2
Li, X. (2021). Association of Age and Blood Pressure Among 3.3 Million Adults: Insights from China PEACE Million Persons Project. J. Hypertens. 39 (6), 1143–1154. doi:10.1097/HJH.0000000000002793
Marsicano, E. O., Fernandes, N. S., Colugnati, F. A., Fernandes, N. M., De Geest, S., and Sanders-Pinheiro, H. (2015). Multilevel Correlates of Non-adherence in Kidney Transplant Patients Benefitting from Full Cost Coverage for Immunosuppressives: A Cross-Sectional Study. PLoS One 10 (11), e0138869. doi:10.1371/journal.pone.0138869
Pinto, I. V. L., Lima, M. G., Pantuzza, L. L. N., Ceccato, M. D. G. B., Silveira, M. R., and Reis, A. M. M. (2020). Free Access to Medicines Among Older Adults in Primary Care: a Cross-Sectional Study. Sao Paulo Med. J. 138 (3), 235–243. doi:10.1590/1516-3180.2019.0541.R1.19022020
Puig-Junoy, J., García-Gómez, P., and Casado-Marín, D. (2016). Free Medicines Thanks to Retirement: Impact of Coinsurance Exemption on Pharmaceutical Expenditures and Hospitalization Offsets in a National Health Service. Health Econ. 25 (6), 750–767. doi:10.1002/hec.3182
Pulok, M. H., Chirwa, G. C., Novignon, J., Aizawa, T., and Makate, M. (2020). Levels of and Changes in Socioeconomic Inequality in Delivery Care Service: A Decomposition Analysis Using Bangladesh Demographic Health Surveys. PLoS One 15 (11), e0242325. doi:10.1371/journal.pone.0242325
Riley, I. L., Jackson, B., Crabtree, D., Riebl, S., Que, L. G., Pleasants, R., et al. (2021). A Scoping Review of International Barriers to Asthma Medication Adherence Mapped to the Theoretical Domains Framework. J. Allergy Clin. Immunol. Pract. 9 (1), 410–e4. e4. doi:10.1016/j.jaip.2020.08.021
Ross-Degnan, D., Wallace, J., Zhang, F., Soumerai, S. B., Garabedian, L., and Wharam, J. F. (2020). Reduced Cost-Sharing for Preventive Drugs Preferentially Benefits Low-Income Patients with Diabetes in High Deductible Health Plans with Health Savings Accounts. Med. Care 58 (Suppl. 6 1), S4–S13. doi:10.1097/MLR.0000000000001295
Sipos, M., Farcas, A., Prodan, N., and Mogosan, C. (2021). Relationship between Beliefs about Medicines and Adherence in Elderly Patients with Cardiovascular and Respiratory Diseases: A Cross-Sectional Study in Romania. Patient Educ. Couns. 104 (4), 911–918. doi:10.1016/j.pec.2020.09.001
Sunny, A. A., Iyer, R. S., Kumaran, S. G., Bunshaw, N. G., Shanmugham, K., and Govindaraj, U. (2020). Affordability, Availability and Tolerability of Anti-seizure Medications Are Better Predictors of Adherence Than Beliefs: Changing Paradigms from a Low Resource Setting. Seizure 83, 208–215. doi:10.1016/j.seizure.2020.11.003
Taizhou Bureau of Statistics, Taizhou Investigation Team of National Bureau of Statistics (2017). Taizhou Statistical Year Book. Beijing, China: China Statistics Press. http://tjj.zjtz.gov.cn/art/2017/11/24/art_1229020475_42753763.html.
Tavares, N. U., Luiza, V. L., Oliveira, M. A., Costa, K. S., Mengue, S. S., Arrais, P. S., et al. (2016). Free Access to Medicines for the Treatment of Chronic Diseases in Brazil. Rev. Saude Publica 50 (Suppl. 2), 7s. doi:10.1590/S1518-8787.2016050006118
Varas-Doval, R., Gastelurrutia, M. A., Benrimoj, S. I., García-Cárdenas, V., Sáez-Benito, L., and Martinez-Martínez, F. (2020). Clinical Impact of a Pharmacist-Led Medication Review with Follow up for Aged Polypharmacy Patients: A Cluster Randomized Controlled Trial. Pharm. Pract. (Granada) 18 (4), 2133. doi:10.18549/PharmPract.2020.4.2133
Wang, Y., Zhu, Y., Shi, H., Sun, X., Chen, N., and Li, X. (2019). The Effect of the Full Coverage of Essential Medicines Policy on Utilization and Accessibility of Primary Healthcare Service for Rural Seniors: A Time Series Study in Qidong, China. Int. J. Environ. Res. Public Health 16 (22), 4316. doi:10.3390/ijerph16224316
Xia, M., Liu, K., Feng, J., Zheng, Z., and Xie, X. (2021). Prevalence and Risk Factors of Type 2 Diabetes and Prediabetes Among 53,288 Middle-Aged and Elderly Adults in China: A Cross-Sectional Study. Diabetes Metab. Syndr. Obes. 14, 1975–1985. doi:10.2147/DMSO.S305919
Yaogo, M. (2017). Free versus Subsidised Healthcare: Options for Fee Exemptions, Access to Care for Vulnerable Groups and Effects on the Health System in Burkina Faso. Health Res. Pol. Syst 15 (Suppl. 1), 58. doi:10.1186/s12961-017-0210-z
Yu, B., Zhang, X., and Wang, G. (2013). Full Coverage for Hypertension Drugs in Rural Communities in China. Am. J. Manag. Care 19 (1), e22–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4538950/.
Zhao, Y., Zhou, Z., Fan, X., Nawaz, R., Zhao, D., Xu, T., et al. (2021). Comparison of Inequity in Health-Related Quality of Life Among Unemployed and Employed Individuals in China. BMC Public Health 21 (1), 52. doi:10.1186/s12889-020-10038-3
Zheng, N. T., Haber, S., Hoover, S., and Feng, Z. (2017). Access to Care for Medicare-Medicaid Dually Eligible Beneficiaries: The Role of State Medicaid Payment Policies. Health Serv. Res. 52 (6), 2219–2236. doi:10.1111/1475-6773.12591
Zhou, Z. H., Wu, Y. F., Yan, Y., Liu, A. Q., Yu, Q. Y., Peng, Z. X., et al. (2021). Persistence with Medical Treatment for Wilson Disease in China Based on a Single center's Survey Research. Brain Behav. 11 (6), e02168. doi:10.1002/brb3.2168
Keywords: full coverage policy, free, essential medicines, inequality in medication adherence, concentration index, China
Citation: Guo Z, Zheng L, Fu M, Li H, Bai L, Guan X and Shi L (2022) Effects of the Full Coverage Policy of Essential Medicines on Inequality in Medication Adherence: A Longitudinal Study in Taizhou, China. Front. Pharmacol. 13:802219. doi: 10.3389/fphar.2022.802219
Received: 26 October 2021; Accepted: 13 January 2022;
Published: 03 February 2022.
Edited by:
Lon J. Van Winkle, Rocky Vista University, United StatesReviewed by:
Elisangela Da Costa Lima, Federal University of Rio de Janeiro, BrazilCopyright © 2022 Guo, Zheng, Fu, Li, Bai, Guan and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaodong Guan, Z3VhbnhpYW9kb25nQHBrdS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.