
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 27 April 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.796027
 Heloísa Ferreira Pinto Santos1
Heloísa Ferreira Pinto Santos1 Lusiele Guaraldo1Renata Saraiva Pedro2Luana Santana Damasceno1
Lusiele Guaraldo1Renata Saraiva Pedro2Luana Santana Damasceno1 Cláudio Tadeu Daniel-Ribeiro3,4
Cláudio Tadeu Daniel-Ribeiro3,4 Patrícia Brasil1,4*
Patrícia Brasil1,4*Malaria is a curable disease for which early diagnosis and treatment, together with the elimination of vectors, are the principal control tools. Non-adherence to antimalarial treatment may contribute to therapeutic failure, development of antimalarial resistance, introduction or resurgence of malaria in non-endemic areas, and increased healthcare costs. The literature describes several methods to directly or indirectly assess adherence to treatment, but no gold standard exists. The main purpose of this review is to systematize the methods used to assess patient adherence to antimalarial treatment. A systematic review was performed, in accordance with the PRISMA statement, of the following databases: LILACS, EMBASE, PUBMED, COCHRANE, GOOGLE SCHOLAR, WEB OF SCIENCE, SCOPUS, and OPENGREY, through 14 December 2021. A snowball search was also performed by screening the references of the included studies as well as those cited in relevant reviews. Inclusion criteria were reporting assessment of the patient’s adherence to antimalarials in individuals with laboratory diagnosis of malaria, the description of antimalarials prescribed, and adherence estimates. Exclusion criteria were studies exclusively about directly observed therapy, studies of populations ≤12 yo and guidelines, commentaries, reviews, letters, or editorials. Study quality was assessed using MINORS and the Cochrane Risk of Bias Tool. Proportions were calculated to measure frequencies considering the number of articles as the denominator. Twenty-one studies were included in this review. Most of them (76.5%) assessed adherence to falciparum malaria treatment. Seventeen studies (80.9%) used a combination of methods. The methods described were pill counts, self-reports, biological assays, use of electronic pillboxes, and clinical cure. It was possible to identify different adherence classifications for all the methods used. Our review found that indirect methods like pill counts and self-reports are the most commonly used. Combining an method that gives solid proof of the ingestion of medication and a method that completes the research with information regarding factors, beliefs or barrier of adherence seems to be the best approach. Future studies of antimalarial treatment should standardize adherence classifications, and collect data on the types and causes of nonadherence, which can contribute to the development of tools to promote medication adherence.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020148054, identifier CRD42020148054
Malaria is a treatable disease endemic in several countries of Africa, Asia, and South America. The World Health Organization (WHO) estimates (World Health Organization, 2020) that 229 million cases and 409,000 deaths occurred worldwide in 2019. Prompt diagnosis and treatment are the principal tools for the control of malaria. WHO recommendations for antimalarial treatment vary according to the species responsible for the infection: artemisinin-based combination therapy (ACT) for uncomplicated falciparum malaria; chloroquine plus primaquine for Plasmodium vivax or P. ovale, and chloroquine for P. malarie (World Health Organization and Global Malaria Programme, 2015).
Non-adherence to antimalarial treatment is thought to be one of the main causes of failure and may contribute to the maintenance of malaria transmission in a given area, development of antimalarial resistance, inadequate control of the disease, and increased healthcare costs (Duarte and Gyorkos, 2003; World Health Organization and Global Malaria Programme, 2015).
Medication adherence, defined by WHO as “the extent to which a person’s behavior—taking medication, following a diet, and/or executing lifestyle changes—corresponds with agreed recommendations from a health care provider”, is a multidimensional phenomenon determined by the interaction of factors such as access to medication, patient behavior, socio-economic status, the pathology of the disease, and the treatment complexity (Sabate, 2003). Methods for measuring medication adherence are classified as direct or indirect (Cramer, 1991). Direct methods are biological assays that measure the concentrations of drugs, metabolites, or biomarkers in blood, hair, or urine. Indirect methods include self-reports (interviews and questionnaires), medication measurement (pill count), and electronic monitoring devices (Medication Event Monitoring System, MEMS), which record the opening of a medicine bottle.
Adherence to antimalarials has been reviewed previously, with focus on the effectiveness of interventions to improve adherence and effects on therapeutic response (Yeung and White, 2005), patterns of adherence and associated factors (Bruxvoort et al., 2014; Ahluwalia et al., 2020) on ACT exclusively (Banek et al., 2014; Yakasai et al., 2015). To date, no method for measuring medication adherence has been validated for malaria treatment. The present review aimed to systematize the information about the methods used to assess adherence to antimalarial therapy.
This review was developed according to the recommendations of the PRISMA statement (Page et al., 2021), and the protocol was registered in international prospective register of systematic reviews (PROSPERO, CRD42020148054) (Santos et al., 2020). A systematic search for the identification of studies about measurement of adherence to antimalarials was conducted through 14 December 2021 in the following databases: LILACS, EMBASE, MEDLINE (Medical Literature Analysis and Retrieval System Online, interface PUBMED), COCHRANE, GOOGLE SCHOLAR, WEB OF SCIENCE, SCOPUS, and OPENGREY. Additionally, a snowball search was performed by screening the references of the studies included in this review for eligibility, as well as references of other reviews (Yeung and White, 2005; Banek et al., 2014; Bruxvoort et al., 2014; Yakasai et al., 2015).
The search queries were developed using the PECO strategy. The PECO of this review is: P: participants with a laboratory diagnosis of malaria at least 13 years of age; E: malaria treatment; C: Not applicable; O: Methods to assess adherence to treatment. The search descriptors used were malaria, treatment, drug therapy, antimalarials, adherence (medication, patient), compliance (medication, patient) and humans. The search strategy was adapted to each database as necessary. The complete search strategy is available (Supplementary Table S1). There were no language or year restrictions on the searches of the databases.
References were imported to the reference manager Zotero (Zotero, 2020) and duplicates were removed. The selection was performed by pairs of independent reviewers (HFPS and RSP, HFPS and LSD) using the web application Rayyan (Ouzzani et al., 2016). Studies were included if reporting assessment of patients’ adherence to antimalarials in individuals with laboratory diagnosis of malaria, adherence estimates, and the antimalarials prescribed. We excluded studies exclusively about directly observed therapy (DOT) and studies of populations ≤12 years old. DOT studies were excluded as they do not assess but ensure adherence. Children depends on their parents or caregivers to administer their medications, making the evaluation of adherence more complex (Santer et al., 2014; El-Rachidi et al., 2017). Guidelines, commentaries, reviews, letters, and editorials were also excluded. Titles and abstracts were screened for relevance then full text reading was performed. Discrepancies were reviewed and resolved by consensus between two other reviewers (LG and PB).
Data were extracted independently by the same pairs reviewers who selected the studies (HFPS and RSP, HFPS and LSD). Discrepancies were reviewed and resolved by consensus. A standardized data extraction form was developed for the review using the software Epidata v. 3.1, including the following sections: identification of the study (authors, journal, year of publication, and language); study characteristics (design and duration); study population (total number of patients, age, sex, inclusion of pregnant women, and the plasmodial species responsible for the infection); treatment prescribed (drugs and duration of treatment); assessment of the patient’s adherence (method for measuring patient adherence to treatment, adherence classification, adherence criteria, estimate of adherence thereby obtained); and other miscellaneous information such as factors posited to explain nonadherence, and any caveats that the authors made about the estimates of adherence or limitations of the study.
Study quality was assessed using the Methodological Index for Non-randomized Studies (MINORS) for observational studies (Slim et al., 2003) and the Cochrane Risk of Bias Tool for Randomized Controlled Trials for clinical trials (Higgins and Green, 2011). Two reviewers (HFPS and LG) evaluated each article independently and discrepancies were resolved by consensus.
A description of the studies regarding the year of publication, study design, population (country, sample size, sex, and age), type of infection, antimalarial treatment described with treatment duration, adherence assessment methods (description, assessment day, and adherence categories) and the resulting estimates were performed. Proportions were calculated to measure frequencies of variables considering the number of articles as the denominator.
The search strategy returned 1721 studies (Figure 1). After the exclusion of duplicates and application of inclusion criteria, 19 studies were deemed suitable for inclusion in this review. Two additional studies were included after snowball search. Thus, a total of 21 studies were selected for this review.
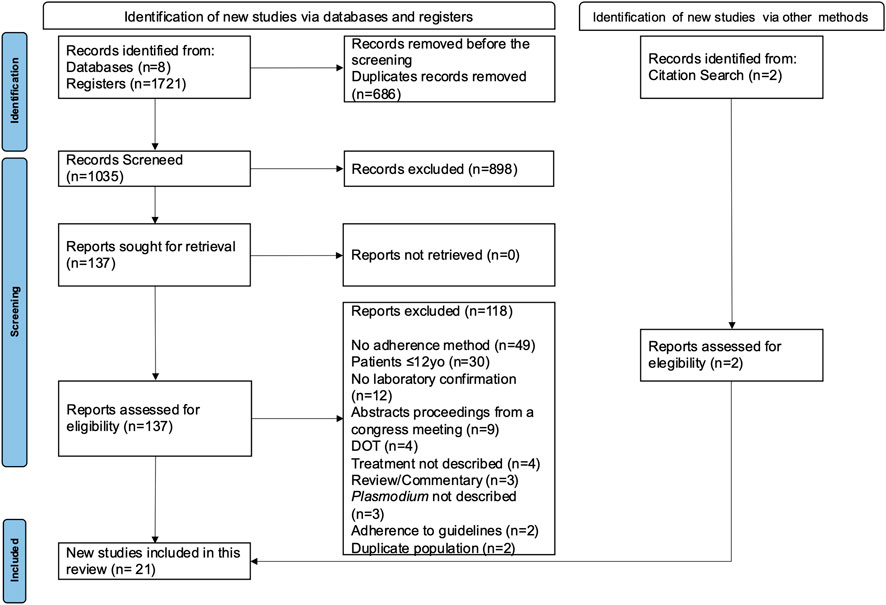
FIGURE 1. Flowchart of systematic search and selection for adherence methods to antimalarial studies.
Characteristics of the included studies (country, design, population, infection/treatment, adherence methods, estimates and quality) are outlined in Supplementary Table S2. The included studies were published between 1997 and 2020, and 66.7% (14/21) were published after 2011. They were carried out in countries that included malaria-endemic areas in Africa, Asia, and the Americas. In the Americas, all studies were conducted in Brazil. Regarding study design of the 21 studies included in this review, 14 (66.7%) were observational, six (28.5%) experimental, and one quasi-experimental (4.8%). The sample size described in the studies varied from 27 to 300 participants for the observational/quasi-experimental studies and from 50 to 324 participants for the experimental ones. The patient populations were children and adults, and nine (42.9%) studies excluded pregnant women (Fungladda et al., 1998; Lemma et al., 2011; Ferreira et al., 2014; Minzi et al., 2014; Osorio-de-Castro et al., 2015; Souza et al., 2016; Saravu et al., 2018; Oduro et al., 2019; Rosa et al., 2020). The eligible studies assessed adherence to antimalarials prescribed for the treatment of malaria caused by P. vivax (10/21, 47.6%) and P. falciparum (16/21, 76.2%). The drugs for vivax malaria were chloroquine or ACT and primaquine, and treatment duration ranged from 7–14 days. In the studies on falciparum malaria, the treatment regimen prescribed was ACT, with a single exception (Fungladda et al., 1998).
The quality assessment of the studies is summarized in Supplementary Table S2 and Figure 2 and Figure 3. Most of the observational/quasi-experimental studies (13/15, 86.6%) collected data prospectively and reported appropriate endpoints. About half (8/15, 53.3%) of them reported adequately loss to follow up less than 5% and the prospective calculation of study size (7/15, 46.6%). The same was observed for the quasi-experimental study, which is the only one that has comparative groups. Of the six clinical trials included in this review, five were deemed to be poor quality (Fungladda et al., 1998; Qingjun et al., 1998; Asante et al., 2009; Saravu et al., 2018; Bagchi et al., 2020), and one fair quality (Steury, 2016) according to the Cochrane Risk of Bias tool. None of the trials reported whether blinding was used either when assigning patients to treatment arms or when measuring endpoints.
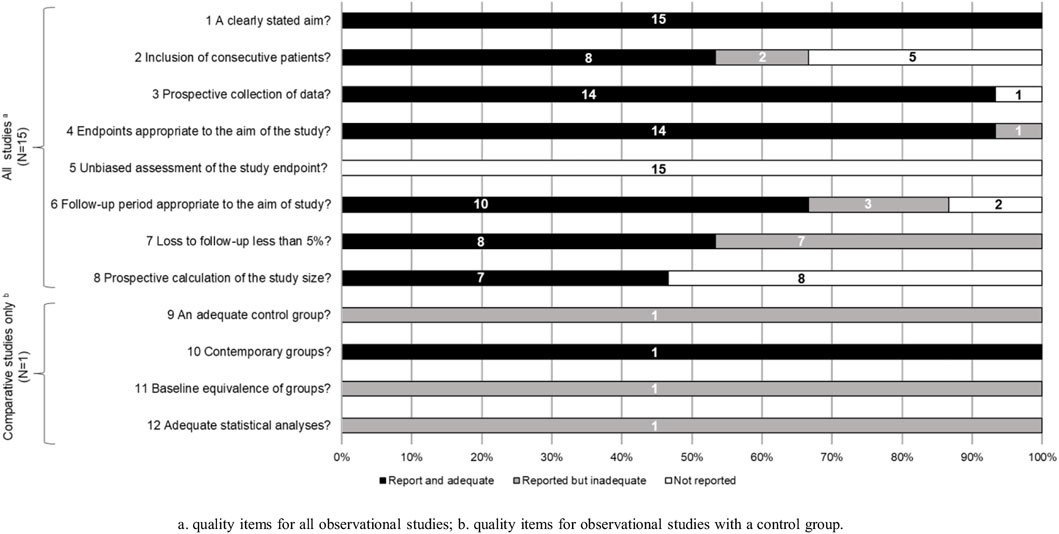
FIGURE 2. Quality assessment of the studies included in the systematic review according to the Methodological Index for Non-randomized Studies (Slim et al., 2003). (A). quality items for all observational studies; (B). quality items for observational studies with a control group.
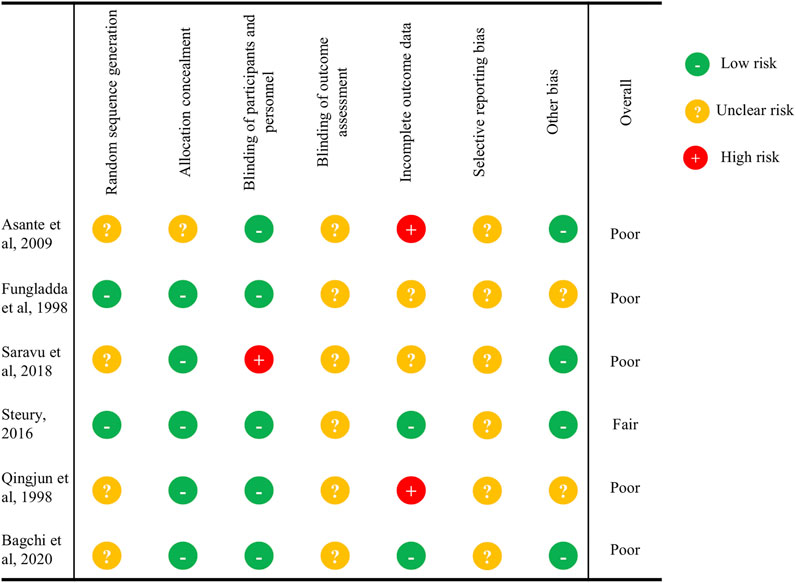
FIGURE 3. Quality assessment of the studies included in the systematic review according to the Cochrane Risk of Bias Tool for Randomized Controlled Trials for clinical trials (Higgins and Green, 2011).
Quantitative estimates of antimalarial adherence varied among treatments and methods used to assess adherence (Supplementary Table S2). Estimates of the rate of adherence to P. vivax treatment differed considerably depending upon the method used to measure adherence. When adherence was measured based on a biological assay, the estimated adherence rate was 95.3% (Cheoymang et al., 2015) versus 71.1–100% based on pill counts (Almeida et al., 2014; Cheoymang et al., 2015; Osorio-de-Castro et al., 2015), 50–100% (Rocha, 2008; Cheoymang et al., 2015; Osorio-de-Castro et al., 2015) based on interviews, and 63.8–83% based on questionnaires (Qingjun et al., 1998; Almeida et al., 2014). When adherence was measured using a combination of different methods, the estimated rate of adherence varied from 44.1 to 75% (Souza et al., 2016; Saravu et al., 2018; Rosa et al., 2020). Studies of P. falciparum treatment also reported a wide range of adherence rates: 45.4–92.6% by pill count (Asante et al., 2009; Amponsah et al., 2015; Osorio-de-Castro et al., 2015), 66.7–100% by interview (Rocha, 2008; Minzi et al., 2014; Osorio-de-Castro et al., 2015; Takahashi et al., 2018), 16.7% by electronic pillbox (Steury, 2016), and 86.8–100% by biological assays (Na-Bangchang et al., 1997; Minzi et al., 2014). The rate of adherence based on a combination of methods varied from 60 to 94.4% (Takahashi et al., 2018; Oduro et al., 2019; Bagchi et al., 2020).
The studies included in the review assessed adherence by indirect and direct methods. The indirect methods described were self-reports, pill counts, MEMS, and clinical cure. To measure adherence to antimalarial treatment, 76.2% (16/21) of the studies used a combination of methods, the most frequent of which were self-reported adherence and pill counts (Fungladda et al., 1998; Lemma et al., 2011; Tun et al., 2012; Almeida et al., 2014; Ferreira et al., 2014; Osorio-de-Castro et al., 2015; Souza et al., 2016; Saravu et al., 2018; Takahashi et al., 2018; Oduro et al., 2019; Bagchi et al., 2020) (Supplementary Table S2 and Table 1).
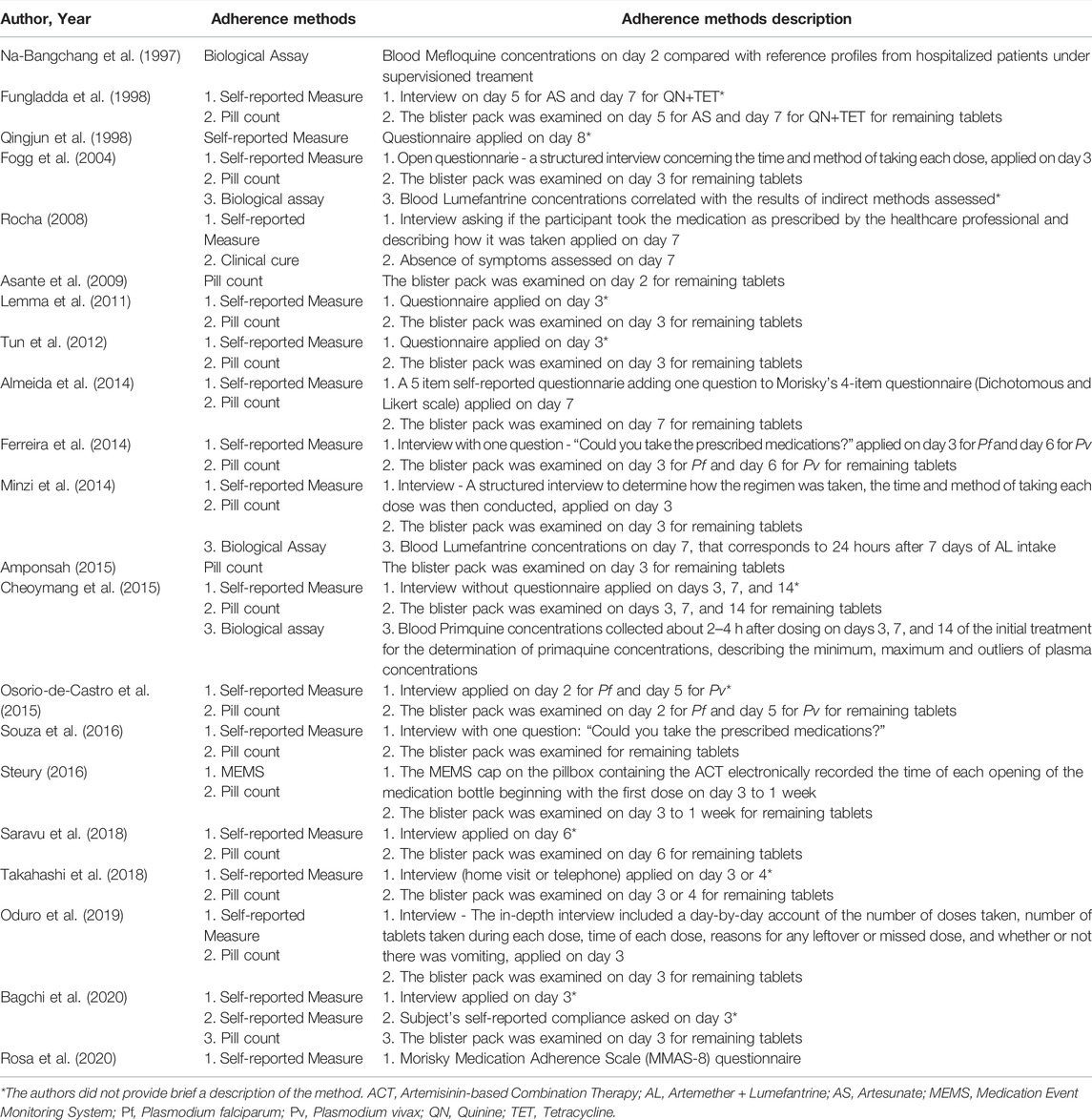
TABLE 1. Description of the methods to assess adherence used on the included studies.
Five studies included detailed descriptions of the questionnaires/interviews (Rocha, 2008; Almeida et al., 2014; Ferreira et al., 2014; Souza et al., 2016; Rosa et al., 2020). Two studies used a single question to assess adherence. The question was “Could you take the prescribed medications?” and patients who answered “yes” were considered adherent and those responding “no”, non-adherent (Ferreira et al., 2014; Souza et al., 2016). Another study (Almeida et al., 2014) developed a 5-item questionnaire by adding the following question to Morisky’s 4-item instrument (Morisky et al., 1986): “Do you replicate the dose when you are feeling sick?” The patients’ responses to this question were evaluated using both a dichotomous yes/no scale and a Likert scale (“all the time”, “nearly always”, “usually”, “sometimes”, “once a while”, and “never”). One study used the Morisky Medication Adherence Scale 8-item (MMAS-8) (Morisky et al., 2008) questionnaire with dichotomous responses (Rosa et al., 2020); however, study did not include a definition of adherence. Seven studies (Fogg et al., 2004; Lemma et al., 2011; Tun et al., 2012; Minzi et al., 2014; Souza et al., 2016; Oduro et al., 2019; Bagchi et al., 2020) reported that the questionnaire applied included the time and date of the medication used by the patient (Table 2).
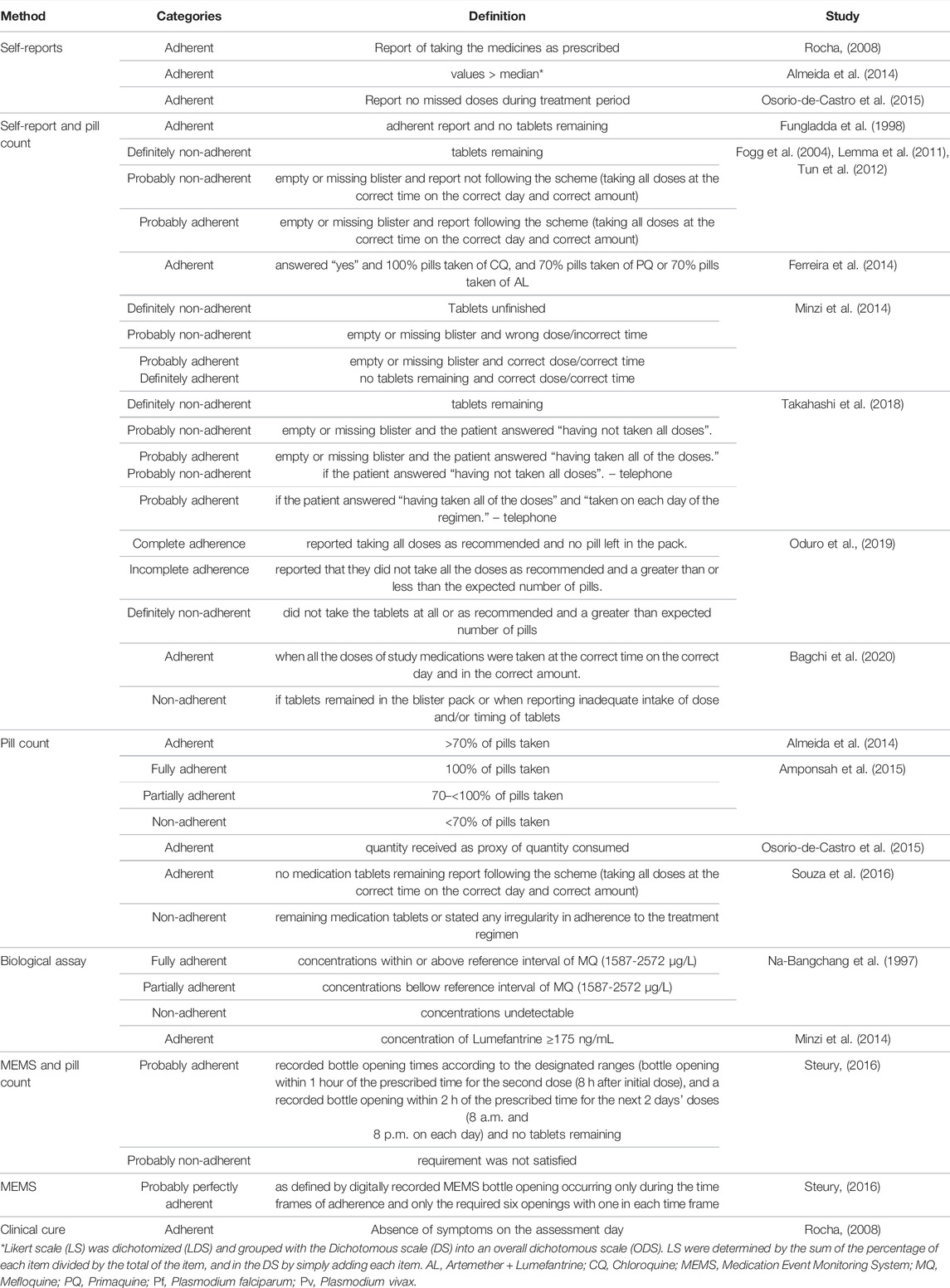
TABLE 2. Description of adherence categories.
More than half of the studies that utilized pill counts (12/18, 66.6%) classified the patient as adherent if there were no tablets remaining upon study completion (Fungladda et al., 1998; Fogg et al., 2004; Lemma et al., 2011; Tun et al., 2012; Minzi et al., 2014; Amponsah et al., 2015; Osorio-de-Castro et al., 2015; Souza et al., 2016; Steury, 2016; Takahashi et al., 2018; Oduro et al., 2019; Bagchi et al., 2020). Four studies compared self-reports to pill counts as a validatory step. In Fogg et al.’s (2004) and Osorio-de-Castro et al.’s (2015) studies, there was a substantial concordance between methods (Kappa coefficients 0.81 and 0.74). In Almeida et al.’s (Almeida et al., 2014) and Minzi et al.’s (2014) studies, the concordance was almost perfect (Kappa 0.94 and 0.96).
Adherence was measured directly by biological assays quantifying lumefantrine (Fogg et al., 2004; Minzi et al., 2014), mefloquine (Na-Bangchang et al., 1997), and primaquine (Cheoymang et al., 2015) in blood. The assessment required defining a threshold concentration above which the patient was considered adherent. The reference threshold varied among studies. In one study, the threshold was the median concentration of antimalarials in hospitalized patients (Na-Bangchang et al., 1997). Another utilized a pre-established concentration from a previous study (Minzi et al., 2014). The two remaining studies utilized a different method to determine the threshold (Fogg et al., 2004; Cheoymang et al., 2015). Fogg et al. (2004) correlates lumefantrine concentrations with the results of indirect methods assessed; Cheoymang et al. (2015) describes minimum, maximum and outliers primaquine plasma concentrations (Table 1).
The timing of the assessment of adherence differed somewhat among the studies. Most studies (17/21, 80.9%) measured adherence 1 day after treatment ended and two studies measured it on the final day of treatment (Na-Bangchang et al., 1997; Asante et al., 2009). In other two studies, adherence was assessed more than once (Minzi et al., 2014; Cheoymang et al., 2015). Finally, a single study (Osorio-de-Castro et al., 2015) evaluated adherence in the course of treatment. Furthermore, the articles utilized distinct models for following up with patient’s post-treatment. In the majority of studies (11/21, 52.4%), follow-up took the form of home visits (Fogg et al., 2004; Asante et al., 2009; Lemma et al., 2011; Tun et al., 2012; Almeida et al., 2014; Ferreira et al., 2014; Minzi et al., 2014; Osorio-de-Castro et al., 2015; Souza et al., 2016; Takahashi et al., 2018; Oduro et al., 2019). In six studies, the patient was required to return to the clinic (Na-Bangchang et al., 1997; Fungladda et al., 1998; Rocha, 2008; Cheoymang et al., 2015; Steury, 2016; Saravu et al., 2018), whereas three studies did not report where the follow up took place (Amponsah et al., 2015; Bagchi et al., 2020; Rosa et al., 2020). One study reported the use of telephone interview when home visits could not be conducted (Takahashi et al., 2018) and another used both telephone interviews and home visits (Qingjun et al., 1998) (Supplementary Table S2 and Table 1).
In total, sixteen studies classified adherence into categories. We identified five distinct systems for classifying adherence among these studies. In seven studies, participants were classified as “adherent” or “non-adherent” (Fungladda et al., 1998; Rocha, 2008; Almeida et al., 2014; Ferreira et al., 2014; Osorio-de-Castro et al., 2015; Souza et al., 2016; Bagchi et al., 2020); two studies used “fully adherent”, “partially adherent” and “non-adherent” (Na-Bangchang et al., 1997; Amponsah et al., 2015), five used “definitely non-adherent”, “probably non-adherent”, “probably adherent” (Fogg et al., 2004; Lemma et al., 2011; Tun et al., 2012; Minzi et al., 2014; Takahashi et al., 2018), one study used “probably perfectly adherent”, “probably adherent”, “probably non adherent”, and “probably not perfectly adherent” (Steury, 2016), and another study, which was the only study that utilized MEMS, classified participants as “complete adherent”, “incomplete adherent”, and “definitely non-adherent” (Oduro et al., 2019) (Supplementary Table S2). Twelve studies (Fungladda et al., 1998; Fogg et al., 2004; Lemma et al., 2011; Tun et al., 2012; Ferreira et al., 2014; Minzi et al., 2014; Souza et al., 2016; Steury, 2016; Saravu et al., 2018; Oduro et al., 2019; Bagchi et al., 2020; Rosa et al., 2020) used a combination of methods to classify the adherence (Table 2).
We reviewed a variety of methods for assessing adherence to antimalarials among patients whose infection was confirmed by parasitological examination. More than half of the studies (14/21, 66.7%) were published in the past decade, and one third (7/21, 33.3%) in the last 5 years, suggesting that concern about adherence has increased. Irrespective of the malaria species or drug regimen, the most frequently used methods to measure adherence were pill counts and self-reports. The widespread use of these methods can be attributed to their low cost (Gabarró, 1999), straightforward implementation, and suitability for any therapeutic regimen.
In eleven studies that used pill counts, home visits were realized to increase follow-up (Qingjun et al., 1998; Fogg et al., 2004; Asante et al., 2009; Lemma et al., 2011; Tun et al., 2012; Almeida et al., 2014; Minzi et al., 2014; Osorio-de-Castro et al., 2015; Souza et al., 2016; Takahashi et al., 2018; Oduro et al., 2019). Similar to studies of chronic diseases, most of these studies defined adherence as consumption of 70% of pills (Almeida et al., 2014; Ferreira et al., 2014; Amponsah et al., 2015). This cut-off may not be suitable for the treatment of an acute infectious disease like malaria, where the goal has to be completing a full therapeutic scheme. A limitation of pill counts is that the counts might not provide information on either the timing of consumption or reasons for non-adherence (Krousel-wood et al., 2004; Lam and Fresco, 2015). Furthermore, it is impossible to confirm whether missing pills were ingested rather than lost or discarded (social desirability bias). This bias can be reduced using unannounced visits, as performed by the studies of Fogg et al. (2004) and Minzi et al. (2014).
Self-reported methods differ in complexity. Interviews and questionnaires examine behavior, beliefs, attitudes toward symptoms, and the patient’s understanding of the drug regimen. Reasons for non-adherence reported in the literature include forgetfulness, adverse reactions, misunderstanding of medication instructions, and the patient’s belief of cure before the end of treatment (Fungladda et al., 1998; Fogg et al., 2004; Lemma et al., 2011; Ferreira et al., 2014; Amponsah et al., 2015; Cheoymang et al., 2015). However, self-reported reasons for non-adherence are subject to recall and social desirability bias if the patient deliberately or unintentionally withholds information (Garber et al., 2004; Cook et al., 2005). As methods of self-reporting varied among studies, it is difficult to assess the reliability between measures.
In the studies included in this review, MEMS and clinical cure were indirect methods that were always used together with other methods (Rocha, 2008; Steury, 2016). Electronic pillboxes are capable of recording the date and time when the bottle was opened, making it possible to recognize patterns of medication use such as only opening the pillbox before the follow-up visits (“White Coat Adherence”) (Schwed et al., 1999; Ailinger et al., 2008). However, pillbox opening does not guarantee ingestion of the pills and, just as failure to open the pillbox does not mean the pills are not being taken. Due to their high cost, the use of electronic pillboxes has been restricted primarily to clinical trials involving a single drug. This tends to limit the utility of MEMS to malaria monotherapy. When electronic pillboxes cannot be used, adherence can be measured via self-reports, pill counts, or biological assays, with blinding of the possible follow up visit to minimize “White Coat Adherence” (Fogg et al., 2004; Minzi et al., 2014).
Clinical cure was defined as the absence of malaria symptoms 6 days after diagnosis (Rocha, 2008). A study in Brazil reported that although symptoms of vivax malaria disappeared on the second day of treatment, 22.5% of patients still had a positive smear (Abdon et al., 2001). This finding casts doubt on the accuracy of clinical cure as an indicator of adherence. In light of this, clinical cure should be combined with laboratory confirmation of cure.
Less than a quarter of the studies (4/21, 23.5%) used direct methods that measured drug concentrations in blood (Na-Bangchang et al., 1997; Fogg et al., 2004; Minzi et al., 2014; Cheoymang et al., 2015), which provide the strongest evidence that the patient ingested the medication (Farmer, 1999; de Achaval and Suarez-Almazor, 2010; Bemt et al., 2012; Lam and Fresco, 2015). This is likely due to the fact that direct methods require specialized training and laboratory resources making them expensive and invasive. Furthermore, drug interactions and variations in drug pharmacokinetics may interfere with the evaluation of these methods. For instance, changes in the CYP 2D62C8 metabolic pathways can increase the risk of therapeutic failure of primaquine (Ingelman-Sundberg, 2005) and modify the kinetics of chloroquine (Kim et al., 2003), altering the perception of adherence. In addition, in the study of Fogg et al. (2004), the plasma concentration of lumefantrine was not used to classify adherence because the fraction absorbed is highly variable, and it was used only to assess the correlation with the indirect methods. These combination of factors impact on the feasibility of direct methods in clinical practice (Lam and Fresco, 2015). Furthermore, the definition of the reference value of drug concentrations is a challenge. None of the studies included utilized the same reference value. Half of them (2/4, 50%) (Fogg et al., 2004; Cheoymang et al., 2015) calculated the mean concentration of the adherent and non-adherent patients. As treatments for malaria are based on combined therapy avoid the evolution of resistance, the assessment of adherence via biological assays should consider all of the drugs that are included in the treatment regimen.
The timing of assessment of adherence was appropriate in all included studies. The proximity of self-report to the completion of treatment is beneficial as it tends to reduce recall problems. In studies of MEMS, there was no risk of memory bias since the date and time when the pill bottle was opened were recorded electronically.
We found that rates of medication adherence were classified into a wide variety of qualitative categories, which were not standardized across the studies. While seven of the 21 studies adopted binary classification as “adherent” or “non-adherent” (Fungladda et al., 1998; Rocha, 2008; Almeida et al., 2014; Ferreira et al., 2014; Osorio-de-Castro et al., 2015; Souza et al., 2016; Bagchi et al., 2020), four other categorizations were also used in the studies included in this review (Na-Bangchang et al., 1997; Fogg et al., 2004; Lemma et al., 2011; Tun et al., 2012; Minzi et al., 2014; Amponsah et al., 2015; Steury, 2016; Takahashi et al., 2018; Oduro et al., 2019). Recent studies have described adherence as a “spectrum” of behaviors ranging from refusal of treatment, to partial conformity, to precisely following the prescription (Julius et al., 2009). Until standardized categories are adopted in the literature, it will remain difficult to compare data from different studies and assess the efficacy of adherence-increasing interventions.
In our view it is beneficial to use multiple, complementary techniques, as any given method for measuring adherence will have limitations. A high level of concordance between pill count and self-report methods was shown in four studies included in this review (Fogg et al., 2004; Almeida et al., 2014; Minzi et al., 2014; Osorio-de-Castro et al., 2015). However, only two studies (Fogg et al., 2004; Minzi et al., 2014) used announced visits to minimize the social desirability bias, common in both methods. It should be noted that subjective and objective methods assess different dimensions of adherence. While subjective methods are useful in ascertaining the beliefs or barriers to adherence, objective methods provide more accurate data on the way patients intake in their medication regimens. As a gold standard method is not currently available, like other authors (Brown et al., 2016; Anghel et al., 2019), we recommend that two or three approaches be used in parallel. Since the resources available for antimalarial treatment may vary considerably among treatment sites, the best method to be applied in one setting may not necessarily be the best in another. Methods that require specialized equipment and personnel, such as biological assays and MEMS, tend to be more difficult to apply in clinical practice than in research settings, while other indirect methods can be applied in both.
The duration, timing, and frequency of doses were reported in eight studies included in this review (Fogg et al., 2004; Lemma et al., 2011; Tun et al., 2012; Minzi et al., 2014; Souza et al., 2016; Steury, 2016; Oduro et al., 2019; Bagchi et al., 2020). We recommend that these variables should be measured whenever possible. The study that used MEMS (Steury, 2016) detected lower adherence (16.7%) than the others. As electronic pillboxes automatically record the timing and frequency of doses, they are able to detect suboptimal adherence with high sensitivity (El Alili et al., 2016).
Among the strengths of this review are that we searched eight databases and the grey literature, with no restrictions on language, publication date, or drug regimen and only included studies with confirmed parasitological diagnosis. The limitations include the lack of information about the instruments used for self-reports, and uncertainty about medication intake based on pill counts and the cut-off value for biological assays. Another potential weakness of this review is that we did not request unpublished data from the authors of the eligible studies.
Future studies about adherence to antimalarial treatment should describe their methods in sufficient detail so that they can be replicated and utilize standardized categories of adherence to facilitate comparisons. Clinical outcomes such as clinical and radical cure can be used to define cut-off points that optimally stratifies the good versus poor adherence categories (Karve et al., 2009; O’Halloran Leach et al., 2021). A validation step should be considered for the methods, mainly for the indirect ones, but not for the direct adherence markers. For new instruments to be developed, self-reports should measure whether the patient was able to take the medications as prescribed, several times during the follow-up to test consistency in the response. Further, self-reports should assess if the patient ever missed a dose or experienced adverse events, as these data can be used to improve future therapies. Another suggestion is the development of studies that combine direct and indirect methods as a way to validate the different types of self-reports (Wilson et al., 2016). Studies designed to determine a range of cut-off values to assess drug metabolism should also be performed. The DOT can be used with direct methods for the definition of malaria drug concentration threshold, as well as assist in the development and validation of point -of- care tests to assess adherence (Gandhi et al., 2019). It is important to consider that using methods developed for chronic diseases might not be suitable for an acute disease like malaria, since the consequences of non-adherence are different. In antimalarial treatment, suboptimal medication adherence can cause relapses, severe malaria, death, development of antimalarial resistance, and spread of the disease (Duarte and Gyorkos, 2003; Bruxvoort et al., 2014; Siddiqui et al., 2015; World Health Organization and Global Malaria Programme, 2015).
Indirect methods for assessing adherence to antimalarial treatment have been used more frequently than direct ones and seem to be the most practical, irrespective of the malaria species or therapeutic scheme. In our view, the best approach for measuring treatment adherence is a combination of methods that evaluate adherence using different parameters and are feasible given local resources. Combining an objective method that gives solid proof of the ingestion of medication and a subjective method that complements the research with information regarding factors, beliefs or barrier of adherence seems to be the best approach. There is a need for methods that combine these approaches in a cost -effectiveness way.
Our review underscores the importance of developing an optimum adherence classification by methods and validating methods for assessing adherence to antimalarial treatment, including specific method for evaluating the causes of non-adherence, as it is a fundamental tool for improving the efficacy of therapy and control.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
LG, PB and HFPS conceived and designed the review. HFPS developed the search strategy. HFPS, LSD and RSP conducted the review and synthesizesd the findings. HFPS conducted the analysis and wrote the first draft of the manuscript. PB, LG, LSD, RSP and CTDR revised and edited the manuscript. All authors read and approved the final version of the manuscript.
This work is part of HFPS’ MSc research supported by the Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro - Brazil (FAPERJ)- Grant E-26/210.596/2019 and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior–Brazil (CAPES)—Finance Code 001. CTDR (312877/2013–7) and PB (307282/2017–1) are supported by CNPq, Brazil, through a Productivity Research Fellowship and CTDR (E-26/202.921/2018) and PB (E-26/202.862/2018) are “Cientistas do Nosso Estado” recognized by the Faperj. The Laboratório de Pesquisa em Malária, IOC, Fiocruz is a National Institute of Science and Technology (INCT) associated Laboratory and also an Associated Laboratory of the Neuroinflammation Network (Faperj). The work received partial support from the Secretaria de Vigilância em Saúde, Ministry of Health, Brazil, through a Global Fund project (TED/FNS-49/2018), and from the CNPq-Faperj/Pronex (E-26/010.001268/2016), Brazil.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
HFPS is grateful to the Postgraduate Program in Clinical Research in Infectious Diseases of the Instituto Nacional de Infectologia Evandro Chagas (INI) of Fundação Oswaldo Cruz (Fiocruz), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) for the MS fellowship and Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro - Brazil (FAPERJ). The authors are grateful to Trevon Fuller for the English review and suggestions for the improvement of the work.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.796027/full#supplementary-material
AS, Artesunate; AQ, Amodiaquine; AL, Artemether + Lumefantrine; AM, Arthemeter; MQ, Mefloquine; CQ, Chloroquine; DHA, Dihidroartemisinine; DOX, Doxycycline; G6PD, Glucose 6 Phosphate Dehydrogenase; DOT, Directly Observed Therapy, MEMS, Medication Event Monitoring System; MINORS, Methodological Index for Non-randomized Studies; PIP, Piperaquine; PQ, Primaquine; Pf, Plasmodium Falciparum; Pv, Plasmodium vivax; QN, Quinine; TET, Tetracycline; WHO, World Health Organization.
Abdon, N. P., Pinto, A. Y. d. N., das, N., Silva, R. d. S. U. d., Souza, J. M. d., Ahluwalia, J., et al. (2001). Avaliação da resposta aos esquemas de tratamento reduzidos para malária vivaxA Systematic Review of Factors Affecting Adherence to Malaria Chemoprophylaxis Amongst Travellers From Non-Endemic Countries. Rev. Soc. Bras. Med. Trop. Malar J. 3419, 34316–34348. doi:10.1590/S0037-86822001000400006
Ahluwalia, J., Brooks, S. K., Weinman, J., and James Rubin, G. (2020). A Systematic Review of Factors Affecting Adherence to Malaria Chemoprophylaxis Amongst Travellers From Non-Endemic Countries. Malar J. 19, 16. doi:10.1186/s12936-020-3104-4
Ailinger, R. L., Black, P. L., and Lima-Garcia, N. (2008). Use of Electronic Monitoring in Clinical Nursing Research. Clin. Nurs. Res. 17, 89–97. doi:10.1177/1054773808316941
Almeida, E. D., Rodrigues, L. C., and Vieira, J. L. (2014). Estimates of Adherence to Treatment of Vivax Malaria. Malar. J. 13, 321. doi:10.1186/1475-2875-13-321
Amponsah, A. O., Vosper, H., and Marfo, A. F. (2015). Patient Related Factors Affecting Adherence to Antimalarial Medication in an Urban Estate in Ghana. Malar. Res. Treat. 2015, 452539. doi:10.1155/2015/452539
Anghel, L. A., Farcas, A. M., and Oprean, R. N. (2019). An Overview of the Common Methods Used to Measure Treatment Adherence. Med. Pharm. Rep. 92, 117–122. doi:10.15386/mpr-1201
Asante, K. P., Owusu, R., Dosoo, D., Awini, E., Adjei, G., Amenga Etego, S., et al. (2009). Adherence to Artesunate-Amodiaquine Therapy for Uncomplicated Malaria in Rural Ghana: A Randomised Trial of Supervised versus Unsupervised Drug Administration. J. Trop. Med. 2009, 529583. doi:10.1155/2009/529583
Bagchi, C., Pramanik, N., Kundu, P. K., and Tripathi, S. K. (2020). Patient Adherence and Treatment Outcome in Uncomplicated Falciparum Malaria Treated with Supervised versus Non-Supervised Artesunate - Sulphadoxine - Pyrimethamine Regimen. jebmh 7, 1574–1580. doi:10.18410/jebmh/2020/331
Banek, K., Lalani, M., Staedke, S. G., and Chandramohan, D. (2014). Adherence to Artemisinin-Based Combination Therapy for the Treatment of Malaria: a Systematic Review of the Evidence. Malar. J. 13, 7. doi:10.1186/1475-2875-13-7
Brown, M. T., Bussell, J., Dutta, S., Davis, K., Strong, S., and Mathew, S. (2016). Medication Adherence: Truth and Consequences. Am. J. Med. Sci. 351, 387–399. doi:10.1016/j.amjms.2016.01.010
Bruxvoort, K., Goodman, C., Kachur, S. P., and Schellenberg, D. (2014). How Patients Take Malaria Treatment: A Systematic Review of the Literature on Adherence to Antimalarial Drugs. PLoS One 9, e84555. doi:10.1371/journal.pone.0084555
Cheoymang, A., Ruenweerayut, R., Muhamad, P., Rungsihirunrat, K., and Na-Bangchang, K. (2015). Patients' Adherence and Clinical Effectiveness of a 14-day Course of Primaquine when Given with a 3-day Chloroquine in Patients with Plasmodium Vivax at the Thai-Myanmar Border. Acta Trop. 152, 151–156. doi:10.1016/j.actatropica.2015.08.008
Cook, C. L., Wade, W. E., Martin, B. C., and Perri, M. (2005). Concordance Among Three Self-Reported Measures of Medication Adherence and Pharmacy Refill Records. J. Am. Pharm. Assoc. (2003) 45, 151–159. doi:10.1331/1544345053623573
Cramer, J. (1991). “Identifying and Improving Compliance Patterns,” in Patient Compliance in Medical Practice and Clinical Trials. Editors B. Spilker, and J. A. Cramer (New York: Raven Press), 387–392.
de Achaval, S., and Suarez-Almazor, M. E. (2010). Treatment Adherence to Disease-Modifying Antirheumatic Drugs in Patients with Rheumatoid Arthritis and Systemic Lupus Erythematosus. Int. J. Clin. Rheumtol 5, 313–326. doi:10.2217/ijr.10.15
Duarte, E. C., and Gyorkos, T. W. (2003). Self-Reported Compliance with Last Malaria Treatment and Occurrence of Malaria During Follow-Up in a Brazilian Amazon Population. Trop. Med. Int. Health 8, 518–524. doi:10.1046/j.1365-3156.2003.01042.x
El Alili, M., Vrijens, B., Demonceau, J., Evers, S. M., and Hiligsmann, M. (2016). A Scoping Review of Studies Comparing the Medication Event Monitoring System (MEMS) with Alternative Methods for Measuring Medication Adherence. Br. J. Clin. Pharmacol. 82, 268–279. doi:10.1111/bcp.12942
El-Rachidi, S., LaRochelle, J. M., and Morgan, J. A. (2017). Pharmacists and Pediatric Medication Adherence: Bridging the Gap. Hosp. Pharm. 52, 124–131. doi:10.1310/hpj5202-124
Farmer, K. C. (1999). Methods for Measuring and Monitoring Medication Regimen Adherence in Clinical Trials and Clinical Practice. Clin. Ther. 21, 1074–1073. doi:10.1016/S0149-2918(99)80026-5
Ferreira, R. G., Azevedo, R. C. d. S., Reiners, A. A. O., Souza, T. G. d., and Fontes, C. J. F. (2014). Adesão ao tratamento da malária e fatores Contribuintes. Rev. Eletr. Enf. 16, 35–43. doi:10.5216/ree.v16i1.19812
Fogg, C., Bajunirwe, F., Piola, P., Biraro, S., Checchi, F., Kiguli, J., et al. (2004). Adherence to a Six-Dose Regimen of Artemether-Lumefantrine for Treatment of Uncomplicated Plasmodium Falciparum Malaria in Uganda. Am. J. Trop. Med. Hyg. 71, 525–530. doi:10.4269/ajtmh.2004.71.525
Fungladda, W., Honrado, E. R., Thimasarn, K., Kitayaporn, D., Karbwang, J., Kamolratanakul, P., et al. (1998). Compliance with Artesunate and Quinine + Tetracycline Treatment of Uncomplicated Falciparum Malaria in Thailand. Bull. World Health Organ. 76, 59–66.
Gandhi, M., Bacchetti, P., Spinelli, M. A., Okochi, H., Baeten, J. M., Siriprakaisil, O., et al. (2019). Brief Report: Validation of a Urine Tenofovir Immunoassay for Adherence Monitoring to PrEP and ART and Establishing the Cutoff for a Point-of-Care Test. J. Acquir Immune Defic Syndr. 81, 72–77. doi:10.1097/QAI.0000000000001971
Garber, M. C., Nau, D. P., Erickson, S. R., Aikens, J. E., and Lawrence, J. B. (2004). The Concordance of Self-Report with Other Measures of Medication Adherence: A Summary of the Literature. Med. Care 42, 649–652. doi:10.1097/01.mlr.0000129496.05898.02
Higgins, J. P. T., and Green, S. (2011). Cochrane Handbook for Systematic Reviews of Interventions. [Updated March 2011]. The Cochrane Collaboration. Available at: http://handbook-5-1.cochrane.org/ (Accessed April 16, 2018).
Ingelman Sundberg, M. (2005). Genetic Polymorphisms of Cytochrome P450 2D6 (CYP2D6): Clinical Consequences, Evolutionary Aspects and Functional Diversity. Pharmacogenomics J. 5, 6–13. doi:10.1038/sj.tpj.6500285
Julius, R. J., Novitsky, M. A., and Dubin, W. R. (2009). Medication Adherence: A Review of the Literature and Implications for Clinical Practice. J. Psychiatr. Pract. 15, 34–44. doi:10.1097/01.pra.0000344917.43780.77
Karve, S., Cleves, M. A., Helm, M., Hudson, T. J., West, D. S., and Martin, B. C. (2009). Good and Poor Adherence: Optimal Cut-point for Adherence Measures Using Administrative Claims Data. Curr. Med. Res. Opin. 25, 2303–2310. doi:10.1185/03007990903126833
Kim, K. A., Park, J. Y., Lee, J. S., and Lim, S. (2003). Cytochrome P450 2C8 and CYP3A4/5 Are Involved in Chloroquine Metabolism in Human Liver Microsomes. Arch. Pharm. Res. 26, 631–637. doi:10.1007/BF02976712
Krousel-wood, M., Thomas, S., Muntner, P., and Morisky, D. (2004). Medication Adherence: a Key Factor in Achieving Blood Pressure Control and Good Clinical Outcomes in Hypertensive Patients. Curr. Opin. Cardiol. 19, 357–362. doi:10.1097/01.hco.0000126978.03828.9e
Lam, W. Y., and Fresco, P. (2015). Medication Adherence Measures: An Overview. Biomed. Res. Int. 2015, 217047217047–217112. doi:10.1155/2015/217047
Lemma, H., Löfgren, C., and San Sebastian, M. (2011). Adherence to a Six-Dose Regimen of Artemether-Lumefantrine Among Uncomplicated Plasmodium Falciparum Patients in the Tigray Region, Ethiopia. Malar. J. 10, 349. doi:10.1186/1475-2875-10-349
Minzi, O., Maige, S., Sasi, P., and Ngasala, B. (2014). Adherence to Artemether-Lumefantrine Drug Combination: A Rural Community Experience Six Years After Change of Malaria Treatment Policy in Tanzania. Malar. J. 13, 267. doi:10.1186/1475-2875-13-267
Morisky, D. E., Ang, A., Krousel Wood, M., and Ward, H. J. (2008). Predictive Validity of a Medication Adherence Measure in an Outpatient Setting. J. Clin. Hypertens. (Greenwich) 10, 348–354. doi:10.1111/j.1751-7176.2008.07572.x
Morisky, D. E., Green, L. W., and Levine, D. M. (1986). Concurrent and Predictive Validity of a Self-Reported Measure of Medication Adherence. Med. Care 24, 67–74. doi:10.1097/00005650-198601000-00007
Na Bangchang, K., Congpuong, K., Sirichaisinthop, J., Suprakorb, K., Karbwang, J., et al. (1997). Compliance with a 2 Day Course of Artemether-Mefloquine in an Area of Highly Multi-Drug Resistant Plasmodium Falciparum Malaria. Br. J. Clin. Pharmacol., 43, 639–642. doi:10.1046/j.1365-2125.1997.00604.x
Oduro, A. R., Chatio, S., Beeri, P., Anyorigiya, T., Baiden, R., Adongo, P., et al. (2019). Adherence to Dihydroartemisinin-Piperaquine Treatment Among Patients with Uncomplicated Malaria in Northern Ghana. J. Trop. Med. 2019. doi:10.1155/2019/5198010
O'Halloran Leach, E., Lu, H., Caballero, J., Thomas, J. E., Spencer, E. C., and Cook, R. L. (2021). Defining the Optimal Cut-point of Self-Reported ART Adherence to Achieve Viral Suppression in the Era of Contemporary HIV Therapy: a Cross-Sectional Study. AIDS Res. Ther. 18, 36. doi:10.1186/s12981-021-00358-8
Osorio-de-Castro, C. G., Suárez-Mutis, M. C., Miranda, E. S., and Luz, T. C. (2015). Dispensing and Determinants of Non-Adherence to Treatment for Non Complicated Malaria Caused by Plasmodium Vivax and Plasmodium Falciparum in High-Risk Municipalities in the Brazilian Amazon. Malar. J. 14, 471. doi:10.1186/s12936-015-0998-3
Ouzzani, M., Hammady, H., Fedorowicz, Z., and Elmagarmid, A. (2016). Rayyan-a Web and Mobile App for Systematic Reviews. Syst. Rev. 5, 210. doi:10.1186/s13643-016-0384-4
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 Statement: an Updated Guideline for Reporting Systematic Reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Qingjun, L., Jihui, D., Laiyi, T., Xiangjun, Z., Jun, L., Hay, A., et al. (1998). The Effect of Drug Packaging on Patients' Compliance with Treatment for Plasmodium Vivax Malaria in China. Bull. World Health Organ. 76, 21–27.
Rocha, M. N. A. (2008). Adesão Ao Tratamento da Malária: Um Estudo em Comunidades do Entorno da Usina Hidrelétrica de Tucuruí – Pará. Federal University of Pará. Belém (PA). [dissertation].
Rosa, E., Shafira, I. D., and Arifianto, A. (2020). Adherence to Plasmodium Vivax Malaria Treatment in Hanura Public Health Center, Pesawaran District of Indonesia. Research Square. doi:10.21203/rs.2.21806/v1
Sabate, E. (2003). Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization. http://www.who.int/chronic_conditions/en/adherence_report.pdf. (Accessed February 15, 2020).
Santer, M., Ring, N., Yardley, L., Geraghty, A. W., and Wyke, S. (2014). Treatment Non-Adherence in Pediatric Long-Term Medical Conditions: Systematic Review and Synthesis of Qualitative Studies of Caregivers' Views. BMC Pediatr. 14, 63. doi:10.1186/1471-2431-14-63
Santos, H., Damasceno, L., Pedro, R., Guaraldo, L., and Daniel-Ribeiro, C. T. Patricia Brasil (2020). Adherence to Malaria Treatment: A Systematic Review. PROSPERO 2020 CRD42020148054 Available at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020148054.
Saravu, K., Tellapragada, C., Kulavalli, S., Xavier, W., Umakanth, S., Brahmarouphu, G., et al. (2018). A Pilot Randomized Controlled Trial to Compare the Effectiveness of Two 14-day Primaquine Regimens for the Radical Cure of Vivax Malaria in South India. Malar. J. 17, 321. doi:10.1186/s12936-018-2472-5
Schwed, A., Fallab, C. L., Burnier, M., Waeber, B., Kappenberger, L., Burnand, B., et al. (1999). Electronic Monitoring of Compliance to Lipid-Lowering Therapy in Clinical Practice. J. Clin. Pharmacol. 39, 402–409. doi:10.1177/00912709922007976
Siddiqui, M. R., Willis, A., Bil, K., Singh, J., Mukomena Sompwe, E., and Ariti, C. (2015).Adherence to Artemisinin Combination Therapy for the Treatment of Uncomplicated Malaria in the Democratic Republic of the Congo, F1000Res, 4, 51. doi:10.12688/f1000research.6122.2
Slim, K., Nini, E., Forestier, D., Kwiatkowski, F., Panis, Y., and Chipponi, J. (2003). Methodological Index for Non-Randomized Studies (Minors): Development and Validation of a New Instrument. ANZ J. Surg. 73, 712–716. doi:10.1046/j.1445-2197.2003.02748.x
Souza, T. G., Reiners, A. A., Azevedo, R. C., Fontes, C. J., Ferreira, R. G., and Do Carmo, P. U. (2016). Malaria Knowledge and Treatment Adherence in a Brazilian Amazon Community. J. Infect. Dev. Ctries 10, 1258–1264. doi:10.3855/jidc.7129
Steury, E. E. (2016). Mobile Phone Short Message Service to Improve Malaria Pharmacoadherence in Zambia. J. Nurs. Scholarsh 48, 354–361. doi:10.1111/jnu.12216
Takahashi, E., Nonaka, D., Iwagami, M., Phoutnalong, V., Chanthakoumane, K., Kobayashi, J., et al. (2018). Patients’ Adherence to Artemisinin-Based Combination Therapy and Healthcare Workers’ Perception and Practice in Savannakhet Province, Lao PDR, Trop. Med. Healt. 46, 44. doi:10.1186/s41182-018-0125-6
Tun, Z. W., Lin, Z., Wai, K., Lin, K., Oung, M. T., and Kyaw, T. T. (2012). Adherence to the Recommended Regimen of Artemether-Lumefantrine for Treatment of Uncomplicated Falciparum Malaria in Myanmar. Myanmar Health Sci. Res. J. 24, 48–53.
van den Bemt, B. J., Zwikker, H. E., and van den Ende, C. H. (2012). Medication Adherence in Patients with Rheumatoid Arthritis: A Critical Appraisal of the Existing Literature. Expert Rev. Clin. Immunol. 8, 337–351. doi:10.1586/eci.12.23
Wilson, I. B., Lee, Y., Michaud, J., Fowler, F. J., and Rogers, W. H. (2016). Validation of a New Three-Item Self-Report Measure for Medication Adherence. AIDS Behav. 20, 2700–2708. doi:10.1007/s10461-016-1406-x
World Health Organization and Global Malaria Programme, (2015). Guidelines for the Treatment of Malaria. Geneva: World Health Organization.
World Health Organization, (2020). World Malaria Report 2020: 20 Years of Global Progress and Challenges. Geneva: World Health Organization.
Yakasai, A. M., Hamza, M., Dalhat, M. M., Bello, M., Gadanya, M. A., Yaqub, Z. M., et al. (20152015). Adherence to Artemisinin-Based Combination Therapy for the Treatment of Uncomplicated Malaria: A Systematic Review and Meta-Analysis. J. Trop. Med. 2015, 1–11. doi:10.1155/2015/189232
Yeung, S., and White, N. J. (2005). How Do Patients Use Antimalarial Drugs? A Review of the Evidence. Trop. Med. Int. Health 10, 121–138. doi:10.1111/j.1365-3156.2004.01364.x
Zotero (2020). Zotero [Computer Software]. Corporation for Digital Scholarship. Available at: https://Zotero.org.
Keywords: malaria, adherence, compliance, persistance, antimalarial treatment, method, systematic review
Citation: Santos HFP, Guaraldo L, Pedro RS, Damasceno LS, Daniel-Ribeiro CT and Brasil P (2022) Methods to Assess Adult and Adolescent Patients’ Adherence to Antimalarial Treatment: A Systematic Review. Front. Pharmacol. 13:796027. doi: 10.3389/fphar.2022.796027
Received: 18 October 2021; Accepted: 17 March 2022;
Published: 27 April 2022.
Edited by:
Robert L Lins, Independent Researcher, Antwerp, BelgiumReviewed by:
John Weinman, Institute of Psychiatry, Psychology and Neuroscience, United KingdomCopyright © 2022 Santos, Guaraldo, Pedro, Damasceno, Daniel-Ribeiro and Brasil. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Patrícia Brasil, cGF0cmljaWEuYnJhc2lsQGluaS5maW9jcnV6LmJy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.