 Prakasini Satapathy
Prakasini Satapathy Radha Kanta Ratho1*
Radha Kanta Ratho1* Sunil Sethi
Sunil Sethi
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Pharmacol., 16 November 2022
Sec. Pharmacology of Infectious Diseases
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.1065124
This article is part of the Research TopicRe-emergence of neglected tropical diseases amid the COVID-19 pandemic: Epidemiology, transmission, mitigation strategies, and recent advances in chemotherapy and vaccinesView all 13 articles
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a member of the genus Betacoronavirus, was initially reported in Wuhan city, Hubei Province, China in late December 2019 (Gralinski and Menachery, 2020; Zhu et al., 2020). As SARS-CoV-2 spreads rapidly across the world, the World Health Organization (WHO) declared it a pandemic and public health emergency of international concern on 11 March 2020. The COVID-19 pandemic has severely impacted global public health activities, the economy, and curative services. It worsened the elimination program and adherence to treatment of TB, HIV (human immunodeficiency virus), malaria, measles, dengue fever, and neglected tropical diseases (NTDs) like lymphatic filariasis, soil-transmitted helminths, schistosomiasis, onchocerciasis, and trachoma (Mohan et al., 2021; Roberts, 2021; Toor et al., 2021; Aborode et al., 2022) As per 2021, WHO global survey report, 44% countries had disruption of NTD activities (World Health Organization (WHO), 2021a). Many ongoing NTD activities like mass administration campaigns of drugs and vaccines, case detection and vector control were postponed during the pandemic to avoid the additional transmission of SARS-COV-2 which ultimately leads to increased burden of NTDs in high transmission area (Toor et al., 2021).
TB is an infectious disease caused by Mycobacterium tuberculosis, is transmitted by aerosol affecting the lungs. It is a key public health concern due to mortality in low and middle-income countries. The majority of people exposed to MTB during childhood are asymptomatic and remain in latent form, whereas 5–10% of those exposed turn up with active disease (Dheda et al., 2017). National lockdown adversely affected TB care access, thereby leading to disease progression in many cases (Shariq et al., 2022). According to WHO, in 2020 death from tuberculosis increased from 1.4 million to 1.5 million with a 18% decline of new cases globally. Philippines (37%), Indonesia (31%), South Africa (26%) and India (25%) account for major declined of case detection globally (World Health Organization (WHO), 2021b). This requires further intervention to elucidate the risk factors in both SARS COV-2 and TB coinfection in terms of improvisation in case detection and management of TB in endemic countries.
Lungs are the common platform for both SARS-COV-2 and MTB, where both the pathogen replicate in alveolar macrophages and ciliated mucus-secreting epithelial type-2 pneumocytes. MTB utilises various pattern recognition receptors i.e., FCγ receptors, toll-like receptors, mannose receptors, complement receptors, nod- like receptors, dendritic cell-specific intercellular adhesion molecule grabbing nonintegrin, CD14 receptors, and scavenger receptors either singly or in combination (Russell, 2001). MTB induces the expression of ACE2 receptors for cell entry, which interestingly serves for the entry of SARS-COV-2 (Rosas Mejia et al., 2022), also thereby, sharing the common cell entry pathways. Patients with severe COVID-19 reported to have elevated levels of IL-2, IL-4, IL-6, IL-10, IFN-γ, TNF-α and G-CSF cytokines and chemokines in comparison to mild cases (Huang et al., 2020; Lee et al., 2021). Following alveolar entry, MTB infects type II pneumocytes, alveolar macrophages, and alveolar epithelial cells to release TNF-α, IL-1α. IL-1β, IFN-γ chemokines mediating inflammatory pathway (Etna et al., 2014). MTB favours intracellular survival through downgrading nitric oxide production, phagosomal maturation, and blocking IFN-γ signalling pathway in macrophages (Abdalla et al., 2016). Similarly Influenzae viruses also aggravate TB through elevated IL-10 in co-infected patients (Ring et al., 2019). There is every possibility that severe COVID-19 might reactivate the latent tuberculosis (LTBI) with in the patients.
T-cell-mediated immunity plays pivotal role in controlling disease progression. The frequencies of CD4 + T cells, CD8 + T cells, and NK cells reported to be low in COVID-19 patients associated with lymphopenia (Chen et al., 2020a; Tan et al., 2020), which possibly triggers the reactivation of LTBI (Amelio et al., 2019; Leonso et al., 2022). The mouse coronavirus model also reflects the reactivation of dormant TB by virus that triggering type-1 interferon signalling and activation of mesenchymal stem cell-based defence (Singh et al., 2020). Further studies have reported the reactivation of LTBI during corticosteroid (CST) therapy in COVID-19 patients, due to generalised immunosuppression (Gopalaswamy and Subbian, 2021; Friedman and DeGeorge, 2022).
Table 1 shows a list of studies that reported coinfection of COVID-19 and TB and its severity. COVID-19 in TB patients is more commonly observed in high TB burden countries like India, China, and Vietnam (Dong et al., 2020). MTB infection in patients with COVID-19 was more commonly found than other comorbidities like diabetes, hypertension, and coronary heart disease (Guan et al., 2020). When comparing patients with TB and COVID-19 with pneumonia, 22% of the patients had mild clinical disease, while 78% of COVID-19 had increased severity (Chen et al., 2020b; Guan et al., 2020). Co-infection with SARS CoV-2 and MTB is of concern as the diagnosis of tuberculosis is more likely to be missed due to nonspecific presentation and a lack of typical radiological findings. Pre-existing TB and underlying lung comorbidities aggravate the disease in COVID-19 (Tadolini et al., 2020) possibly through alteration in metabolic pathways. A metabolomic analysis reveals low levels of metabolic biomarkers (Branch chain amino acids, Betaine and its derivatives) as a consequence of post TB infections, are associated with COVID-19 severity (Diboun et al., 2022).
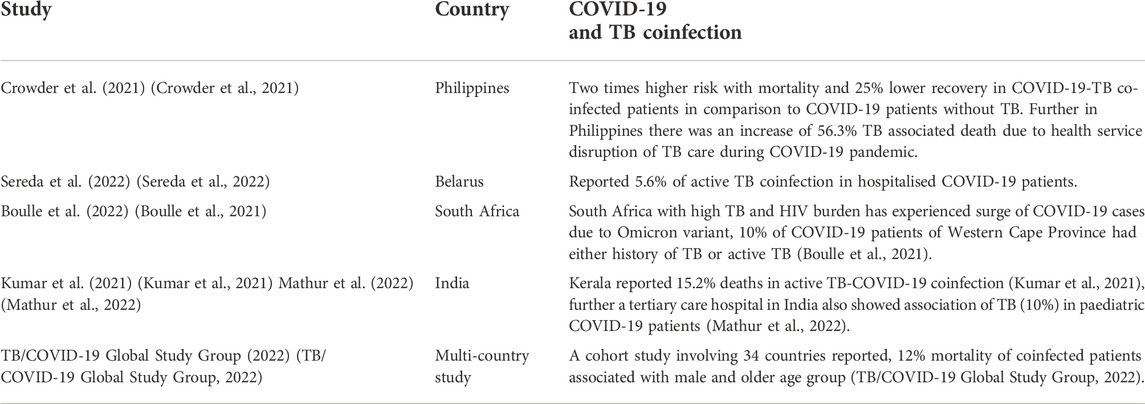
TABLE 1. Studies reported COVID-19 and TB Coinfection.
Chen Y, et al., reported MTB and SARS-COV-2 coinfection induces disease progression and severity in hospitalized COVID-19 patients in China (Chen et al., 2020b). A modelling study by Hogan AB, et al., assumed that COVID-19 pandemic response could increase TB mortality up to 20% with in 2020 and 2025 (Hogan et al., 2020). The disruption epidemiological surveillance and reduction in tuberculosis tests due to COVID-19 pandemic might lead to increase in tuberculosis mortality. In addition to mortality treatment adherence and follow up of TB patients have been negatively affected.
Even though MTB is an apparent risk factor for COVID-19 aggravation, features like alcohol consumption, smoking, HIV and other viral, bacterial and fungal co-infections might have associated risk. Thus, clinical details and social determinants of coinfected patients needs to be assessed for the risk of morbidity and mortality. Early diagnosis of the disease or co-infections makes it mandatory for at risk and compromised patient groups for better management.
Despite mass vaccination breakthrough COVID-19 infections have been reported in TB endemic countries, because of emergence of new variants of the SARS-CoV-2 that can escape the host’s immune response (Hacisuleyman et al., 2021; Prévost and Finzi, 2021; Cascella et al., 2022). A study demonstrated that in countries vaccinated with BCG, the frequency of the S 614G variant was associated with the highest mortality rate related to COVID-19 (Toyoshima et al., 2020).
According to the World Health Organization, exacerbation of TB appeared as the consequences of the COVID-19 epidemic. The possible key factors are: The emergence of COVID-19 pandemic has exerted high pressure on existing health system, weakened many national programmes including national TB elimination programme as well as the intricate association between the two pathogen within the host (Visca et al., 2021). This problem still needs a better evaluation of the coinfection of patients with TB and COVID-19.
Simultaneous testing for TB and COVID-19 may help in detecting new TB cases that missed public services in the context of COVID-19 (MacLean et al., 2022). Some of the strategies adopted to control COVID-19 pandemic may be implemented towards strengthening TB control programme like, teleconsultation, virtually support for self-administration of therapy to avoid delay in treatment, contact tracing and community awareness about any changes in health services etc. Hotspot mapping for active cases could help to identify the undiagnosed TB cases during the pandemic. Further social distancing to be implemented with MDR TB patients living overcrowded location with poor sanitation.
The rapid spread of the new variants of SARS-CoV-2 and drug resistance MTB has warned the public health system and requires active molecular and genomic surveillance of disease transmission and pathogenicity. It is important to recuperate in massive screening, case finding, including targeting high risk groups and allocation of more resources to find the missed TB cases during the COVID-19 pandemic to achieve the end goal of TB. Other chronic diseases, especially those spread through close contacts, should not be ignored in pandemic times and utmost care must be taken to avoid mortality from coinfection and inaccessibility of timely treatment.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ACE, Angiotensin-converting enzyme; CD, Clusters of differentiation; FC receptor, Fragment crystallizable receptor; G-CSF, Filgrastim and granulocyte colony-stimulating factor; IL, Interleukin; INF, Interferons; NK cells, Natural Killer cells; SARS-CoV-2, Severe acute respiratory syndrome coronavirus 2; T cells, T lymphocytes; TNF, Tumor necrosis factor.
Abdalla, A. E., Lambert, N., Duan, X., and Xie, J. (2016). Interleukin-10 family and tuberculosis: An old story renewed. Int. J. Biol. Sci. 12 (6), 710–717. doi:10.7150/ijbs.13881
Aborode, A. T., Corriero, A. C., Fajemisin, E. A., Hasan, M. M., Kazmi, S. K., and Olajiga, O. (2022). Dengue and Coronavirus disease (COVID-19) syndemic: Double threat to an overburdened healthcare system in Africa. Int. J. Health Plann. Manage. 37 (3), 1851–1854. doi:10.1002/hpm.3334
Amelio, P., Portevin, D., Hella, J., Reither, K., Kamwela, L., Lweno, O., et al. (2019). “HIV infection functionally impairs Mycobacterium tuberculosis-specific CD4 and CD8 T-cell responses,”J. Virol. Editor G. Silvestri, 93. doi:10.1128/JVI.01728-185
Boulle, A., Davies, M-A., Hussey, H., Ismail, M., Morden, E., Vundle, Z., et al. (2021). Risk factors for coronavirus disease 2019 (COVID-19) death in a population cohort study from the western cape Province, South Africa. Clin. Infect. Dis. 73 (7), e2005–e2015. doi:10.1093/cid/ciaa1198
Cascella, M., Rajnik, M., Aleem, A., Dulebohn, S. C., and Di Napoli, R. (2022). Features, evaluation, and treatment of coronavirus (COVID-19). Available at: http://www.ncbi.nlm.nih.gov/pubmed/32150360.
Chen, G., Wu, D., Guo, W., Cao, Y., Huang, D., Wang, H., et al. (2020). Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Invest. 130 (5), 2620–2629. doi:10.1172/JCI137244
Chen, Y., Wang, Y., Fleming, J., Yu, Y., Gu, Y., Liu, C., et al. (2020). Active or latent tuberculosis increases susceptibility to COVID-19 and disease severity. Prepr medRxiv. Published online. doi:10.1101/2020.03.10.20033795
Crowder, R., Geocaniga-Gaviola, D. M., Fabella, R. A., Lim, A., Lopez, E., Kadota, J. L., et al. (2021). Impact of shelter-in-place orders on TB case notifications and mortality in the Philippines during the COVID-19 pandemic. J. Clin. Tuberc. Other Mycobact. Dis. 25, 100282. doi:10.1016/j.jctube.2021.100282
Dheda, K., Gumbo, T., Maartens, G., Dooley, K. E., McNerney, R., Murray, M., et al. (2017). The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis. Lancet Respir. Med. 5 (4), 291–360. doi:10.1016/S2213-2600(17)30079-6
Diboun, I., Cyprian, F. S., Anwardeen, N. R., Yassine, H. M., Elrayess, M. A., Rahmoon, S. M., et al. (2022). Identification of prognostic metabolomic biomarkers at the interface of mortality and morbidity in pre-existing TB cases infected with SARS-CoV-2. Front. Cell. Infect. Microbiol. 12, 929689. doi:10.3389/fcimb.2022.929689
Dong, E., Du, H., and Gardner, L. (2020). An interactive web-based dashboard to track COVID-19 in real time. Lancet. Infect. Dis. 20 (5), 533–534. doi:10.1016/S1473-3099(20)30120-1
Etna, M. P., Giacomini, E., Severa, M., and Coccia, E. M. (2014). Pro- and anti-inflammatory cytokines in tuberculosis: A two-edged sword in TB pathogenesis. Semin. Immunol. 26 (6), 543–551. doi:10.1016/j.smim.2014.09.011
Friedman, A., and DeGeorge, K. C. (2022). Reactivation of latent tuberculosis in a COVID-19 patient on corticosteroid treatment. BMJ Case Rep. 15 (5), e247562. doi:10.1136/bcr-2021-247562
Gopalaswamy, R., and Subbian, S. (2021). Corticosteroids for COVID-19 therapy: Potential implications on tuberculosis. Int. J. Mol. Sci. 22 (7), 3773. doi:10.3390/ijms22073773
Gralinski, L. E., and Menachery, V. D. (2020). Return of the coronavirus: 2019-nCoV. Viruses 12 (2), 135. doi:10.3390/v12020135
Guan, W., Ni, Z., Hu, Y., Liang, W. H., Ou, C. Q., He, J. X., et al. (2020). Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 382 (18), 1708–1720. doi:10.1056/NEJMoa2002032
Hacisuleyman, E., Hale, C., Saito, Y., Blachere, N. E., Bergh, M., Conlon, E. G., et al. (2021). Vaccine breakthrough infections with SARS-CoV-2 variants. N. Engl. J. Med. 384 (23), 2212–2218. doi:10.1056/NEJMoa2105000
Hogan, A. B., Jewell, B. L., Sherrard-Smith, E., Vesga, J. F., Watson, O. J., Whittaker, C., et al. (2020). Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet. Glob. Health 8 (9), e1132–e1141. doi:10.1016/S2214-109X(20)30288-6
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., et al. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395 (10223), 497–506. doi:10.1016/S0140-6736(20)30183-5
Kumar, M. S., Surendran, D., Manu, M. S., Rakesh, P. S., and Balakrishnan, S. (2021). Mortality due to TB-COVID-19 coinfection in India. Int. J. Tuberc. Lung Dis. 25 (3), 250–251. doi:10.5588/ijtld.20.0947
Lee, J., Park, S-S., Kim, T. Y., Lee, D-G., and Kim, D-W. (2021). Lymphopenia as a biological predictor of outcomes in COVID-19 patients: A nationwide cohort study. Cancers (Basel) 13 (3), 471. doi:10.3390/cancers13030471
Leonso, A-A., Brown, K., Prol, R., Rawat, S., Khunger, A., and Bromberg, R. (2022). A rare case of latent tuberculosis reactivation secondary to a COVID-19 infection. Infect. Dis. Rep. 14 (3), 446–452. doi:10.3390/idr14030048
MacLean, E. L., Villa-Castillo, L., Ruhwald, M., Ugarte-Gil, C., and Pai, M. (2022). Integrated testing for TB and COVID-19. Med. (New York, NY) 3 (3), 162–166. doi:10.1016/j.medj.2022.02.002
Mathur, S. B., Saxena, R., Pallavi, P., Jain, R., Mishra, D., and Jhamb, U. (2022). Effect of concomitant tuberculosis infection on COVID-19 disease in children: A matched, retrospective cohort study. J. Trop. Pediatr. 68 (4), fmac056. doi:10.1093/tropej/fmac056
Mohan, A., Temitope, R. A., Çavdaroğlu, S., Hasan, M. M., Costa, A. C. D. S., Ahmad, S., et al. (2021). Measles returns to the democratic republic of Congo: A new predicament amid the COVID-19 crisis. J. Med. Virol. 93 (10), 5691–5693. doi:10.1002/jmv.27137
Prévost, J., and Finzi, A. (2021). The great escape? SARS-CoV-2 variants evading neutralizing responses. Cell Host Microbe 29 (3), 322–324. doi:10.1016/j.chom.2021.02.010
Ring, S., Eggers, L., Behrends, J., Wutkowski, A., Schwudke, D., Kroger, A., et al. (2019). Blocking IL-10 receptor signaling ameliorates Mycobacterium tuberculosis infection during influenza-induced exacerbation. JCI Insight 4 (10), 126533. doi:10.1172/jci.insight.126533
Roberts, L. (2021). How COVID is derailing the fight against HIV, TB and malaria. Nature 597 (7876), 314. doi:10.1038/d41586-021-02469-8
Rosas Mejia, O., Gloag, E. S., Li, J., Ruane-Foster, M., Claeys, T. A., Farkas, D., et al. (2022). “Mice infected with Mycobacterium tuberculosis are resistant to acute disease caused by secondary infection with SARS-CoV-2,”.PLOS Pathog,18. 3, e1010093 Editor P. Salgame, doi:10.1371/journal.ppat.1010093
Russell, D. G. (2001). Mycobacterium tuberculosis: Here today, and here tomorrow. Nat. Rev. Mol. Cell Biol. 2 (8), 569–577. doi:10.1038/35085034
Sereda, Y., Korotych, O., Klimuk, D., Zhurkin, D., Solodovnikova, V., Grzemska, M., et al. (2022). Tuberculosis Co-infection is common in patients requiring hospitalization for COVID-19 in Belarus: Mixed-methods study. Int. J. Environ. Res. Public Health 19 (7), 4370. doi:10.3390/ijerph19074370
Shariq, M., Sheikh, J. A., Quadir, N., Sharma, N., Hasnain, S. E., and Ehtesham, N. Z. (2022). COVID-19 and tuberculosis: The double whammy of respiratory pathogens. Eur. Respir. Rev. 31 (164), 210264. doi:10.1183/16000617.0264-2021
Singh, A., Prasad, R., Gupta, A., Das, K., and Gupta, N. (2020). Severe acute respiratory syndrome coronavirus-2 and pulmonary tuberculosis: Convergence can be fatal. Monaldi Arch. Chest Dis. 90 (3). doi:10.4081/monaldi.2020.1368
Tadolini, M., Codecasa, L. R., García-García, J. M., Blanc, F. X., Borisov, S., Alffenaar, J. W., et al. (2020). Active tuberculosis, sequelae and COVID-19 co-infection: First cohort of 49 cases. Eur. Respir. J. 56 (1), 2001398. doi:10.1183/13993003.01398-2020
Tan, M., Liu, Y., Zhou, R., Deng, X., Li, F., Liang, K., et al. (2020). Immunopathological characteristics of coronavirus disease 2019 cases in Guangzhou, China. Immunology 160 (3), 261–268. doi:10.1111/imm.13223
TB/COVID-19 Global Study Group (2022). Tuberculosis and COVID-19 co-infection: Description of the global cohort. Eur. Respir. J. 59 (3), 2102538. doi:10.1183/13993003.02538-2021
Toor, J., Adams, E. R., Aliee, M., Amoah, B., Anderson, R. M., Ayabina, D., et al. (2021). Predicted impact of COVID-19 on neglected tropical disease programs and the opportunity for innovation. Clin. Infect. Dis. 72 (8), 1463–1466. doi:10.1093/cid/ciaa933
Toyoshima, Y., Nemoto, K., Matsumoto, S., Nakamura, Y., and Kiyotani, K. (2020). SARS-CoV-2 genomic variations associated with mortality rate of COVID-19. J. Hum. Genet. 65 (12), 1075–1082. doi:10.1038/s10038-020-0808-9
Visca, D., Ong, C. W. M., Tiberi, S., Centis, R., D'Ambrosio, L., Chen, B., et al. (2021). Tuberculosis and COVID-19 interaction: A review of biological, clinical and public health effects. Pulmonology 27 (2), 151–165. doi:10.1016/j.pulmoe.2020.12.012
World Health Organization (Who) (2021). Control of neglected tropical diseases. Available at: https://www.who.int/teams/control-of-neglected-tropical-diseases/overview/ntds-and-covid-19.
World Health Organization (Who) (2021). WHO Global tuberculosis report. Available at: https://www.who.int/publications/digital/global-tuberculosis-report-2021.
Keywords: Mycobacterium tuberculosis (M Tuberculosis), COVID, coinfections, biomarkers (MESH D015415), treatment regimens
Citation: Satapathy P, Ratho RK and Sethi S (2022) Immunopathogenesis in SARS-CoV-2 and Mycobacterium tuberculosis: The danger of overlapping crises. Front. Pharmacol. 13:1065124. doi: 10.3389/fphar.2022.1065124
Received: 09 October 2022; Accepted: 03 November 2022;
Published: 16 November 2022.
Edited by:
Ranjan K. Mohapatra, Government College of Engineering, Keonjhar, IndiaReviewed by:
Izhar Hyder Qazi, Shaheed Benazir Bhutto University of Veterinary and Animal Sciences, PakistanCopyright © 2022 Satapathy, Ratho and Sethi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Prakasini Satapathy, cHJha2FzaW5pLnNhdGFwYXRoeUBnbWFpbC5jb20=; Radha Kanta Ratho, cmF0aG9wZ2lAeWFob28uY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.