 Xiuehui Chen1
Xiuehui Chen1 Lingyue Zhao
Lingyue Zhao Wenqin Guo
Wenqin Guo- 1Longhua District Central Hospital, Shenzhen, China
- 2Fuwai Hospital Chinese Academy of Medical Sciences, Shenzhen, China
- 3Huazhong University of Science and Technology Union Shenzhen Hospital, Shenzhen, China
Background: The most favorable gastrointestinal (GI) bleeding safety profile among different types of direct oral anticoagulants (DOACs) remains controversial. This meta-analysis includes the latest studies and aims to compare GI bleeding risk associated with the use of various DOACs.
Methods: PubMed, Cochrane library, and clinicaltrial.gov were searched. Randomized control trials (RCTs) evaluating the safety of DOACs were identified. The primary endpoint assessed was major GI bleeding.
Results: A total of 37 RCTs were included in the analyses. Based on the traditional meta-analysis, the major GI bleeding risk was different among various DOACs (interactive p-value <.10). Network meta-analysis findings showed that no DOACs increased the risk of major GI bleeding compared with conventional therapy. Furthermore, a 10 mg daily administration of apixaban reduced the major GI bleeding risk more than daily doses of 60 mg edoxaban, ≥15 mg rivaroxaban, and 300 mg dabigatran etexilate. No difference was observed between daily doses of 300 mg dabigatran etexilate, 60 mg edoxaban, and ≥15 mg rivaroxaban. The major GI bleeding risk associated with 30 mg daily dose of edoxaban was lower than with 10 mg daily rivaroxaban, and no differences between daily 5 mg apixaban, 30 mg edoxaban, and 220 mg dabigatran etexilate were observed.
Conclusion: Differences in the major GI bleeding risk were observed when various DOACs were compared. Among standard-dose DOACs, apixaban was associated with the lowest degree of major GI risk. Among low-dose DOACs, edoxaban was associated with a lower major GI bleeding risk than rivaroxaban.
Introduction
Indications for the use of direct oral anticoagulants (DOACs) are widening to include stroke prevention in those with high-risk atrial fibrillation (AF) and venous thromboembolism prevention and treatment (Kearon, et al., 2016; Steffel, et al., 2021). Although DOACs reduce thromboembolism risk, the risk of concomitant bleeding—especially major gastrointestinal (GI) bleeding—is of clinical concern. The occurrence of major GI bleeding reduces medication compliance and increases thromboembolism and even mortality risk (Deitelzweig, et al., 2021).
Previous studies have evaluated the relationship between DOAC use and major GI bleeding. A prior meta-analysis showed that major GI bleeding risk was not elevated in those receiving DOACs compared with a control group (Miller, et al., 2017). Furthermore, another meta-analysis revealed that, unlike other types of DOACs, rivaroxaban significantly increased major GI bleeding risk (Gu, et al., 2020). Rivaroxaban use was associated with increased rates of GI bleeding compared with apixaban and dabigatran etexilate use, regardless of the indication (Ingason, et al., 2021). A network meta-analysis assessed major GI bleeding risk differences associated with different dosages and types of NOAC therapy; its results showed that major GI bleeding risk associated with 5 mg BID apixaban was lower than that with 20 mg QD rivaroxaban and 150 mg BID dabigatran etexilate (Radadiya, et al., 2021). We conducted a network meta-analysis that showed that both apixaban and edoxaban were associated with a significantly reduced risk of major GI bleeding compared with dabigatran etexilate and rivaroxaban, suggesting that apixaban and edoxaban have optimal major GI bleeding safety profiles, while the use of rivaroxaban and dabigatran etexilate is less safe (Guo, et al., 2019).
Controversy regarding major GI bleeding risk differences among different dosages and types of DOACs remains. Studies published until 2019 were considered in previous meta-analyses (Guo, et al., 2019; Radadiya, et al., 2021). In the past three years, additional work has evaluated the efficacy and safety of DOACs in the treatment of disease. Therefore, we aimed to perform an updated network meta-analysis that includes the latest studies to comprehensively evaluate GI bleeding risk differences among patients receiving various DOACs.
Materials and methods
We report this meta-analysis in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Moher, et al., 2009).
Research strategy
We searched PubMed, Cochran Library, clinicaltrial.gov and reference lists of relevant papers. The following keywords were used for searches: “apixaban,” “edoxaban,” “rivaroxaban,” and “dabigatran etexilate.” Studies published up to 1 April 2022, were considered.
Inclusion and exclusion criteria
The inclusion criteria were: 1) the intervention was a DOAC (apixaban, rivaroxaban, dabigatran etexilate, and edoxaban); 2) control treatment of a DOAC, placebo, conventional treatment regimens including vitamin K antagonists (VKA), low molecular weight heparin, or aspirin; 3) major GI bleeding reported as an outcome; 4) randomized controlled trials. If there were multiple reports from the same study, the most recently published that reported major GI bleeding events was included. The exclusion criteria were: 1) studies that included cancer patients, because patients with GI tumors were at increased risk of GI bleeding; 2) studies that included very elderly patients with mean ages greater than 85 years; 3) the background therapy included an antiplatelet regimen; 4) the intervention was not a DOAC or the intervention was a DOAC combined with antiplatelet therapy; 5) studies not reporting major GI bleeding events; 6) observational studies or research letters.
Data extraction and assessment of primary outcome and study quality
Two researchers designed a table that was used for data extraction. The table was then filled with relevant information using data from the included studies. In the case of a dispute between the two researchers regarding the process of information extraction, a third researcher was consulted. The primary endpoint of the study was major GI bleeding, which was defined according to the individual studies. The Cochrane risk-of-bias tool for randomized trials was used to evaluate the quality of all included studies (Higgins, et al., 2011).
Statistical analysis
Meta-analysis
When performing a traditional meta-analysis, odds ratio (OR) and 95% confidence intervals (CIs) were used to measure the effect size for dichotomous data. The significance threshold was set at p-value <.05. Considering the potential for heterogeneity among the studies, we used the DerSimonian-Laird random-effects model to assess data when performing a traditional meta-analysis (DerSimonian and Laird, 1986). Heterogeneity between studies was analyzed using I2-statistic and Cochran Q tests [10]. I2 values <25%, ≥25% and <50%, ≥50% and <75%, and ≥75% indicated no, low, moderate, and high heterogeneity among studies, respectively (Higgins, et al., 2003). The subgroup analysis was performed based on the dose and type of the DOACs prescribed. An interaction test was performed to evaluate differences among DOACs. Values of p < .1 suggested that differences among subgroups were statistically significant. An R software meta package (version 4.0.3) was used.
Network meta-analysis
In the network meta-analysis, ORs and 95% credible intervals (CrIs) were used to assess the effect size. A CrI that did not include one indicated statistically significant differences. A Bayesian random-effects model was used for the analysis and a Markov Chain–Monte Carlo method was used for Bayesian inference (Dias, et al., 2013a). We used informative variance prior to generating the posterior distributions of the model parameters and fitted three chains, yielding 300,000 iterations (100,000 per chain) (Turner, et al., 2012; Wolfe, et al., 2018). Convergence was assessed by the Brooks–Gelman–Rubin diagnostic (Brooks and Gelman, 1998). Model fit was assessed with a deviance information criterion (Dias, et al., 2013b). Node-splitting was used to evaluate inconsistency between direct and indirect evidence and for p-value calculation (Dias, et al., 2010). Values of p < .05 indicated inconsistencies between direct and indirect evidence. To evaluate the association between population and study characteristics and the clinical outcome, we performed a network meta-regression analysis using mean age, proportion of males, body mass index (BMI), body weight, proportion of Asians, indication, and follow-up time as variables (Dias, et al., 2013a). Publication bias was assessed by drawing a comparison-adjusted funnel plot (Salanti, et al., 2011). The network meta-analysis was performed using gemtc and rjags R software (version 4.0.3) and STATA13.1 packages.
Results
A flow chart depicting the literature search strategy is shown in Figure 1. In total, 2,346 studies were identified through database searching and 86 were identified through other sources. After reading the title and abstract, 1,230 studies were eliminated, and the remaining 65 were downloaded; the full text of each article was read. After reading the full text of these, 28 studies were excluded. The reasons for excluding the studies are shown in the Supplementary Appendix.
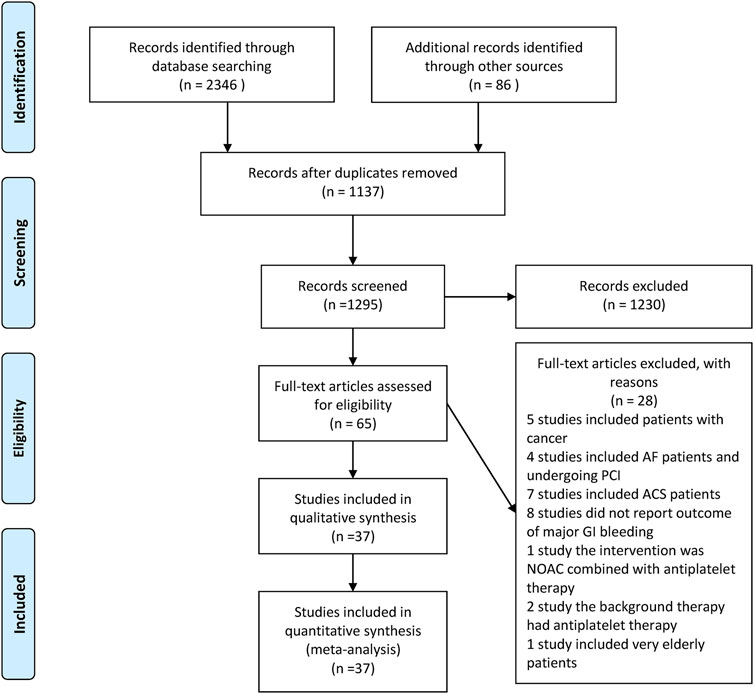
FIGURE 1. Flowchart of study screening.
In the end, 37 studies were included in the meta-analysis (references to the included studies are shown in Supplementary Appendix). Among these, six were three-arm trials (Eriksson, et al., 2006; Connolly, et al., 2009; Chung, et al., 2011; Ogawa, et al., 2011; Agnelli, et al., 2013; Giugliano, et al., 2013). From the three-arm COMPASS study, the 5 mg BID rivaroxaban and aspirin-alone groups were included in the analysis, based on the inclusion and exclusion criteria (Eikelboom, et al., 2017). A network plot is shown in Figure 2. The characteristics of the included studies and each study population are shown in Table 1. The international normalized ratio (INR) values of 2–3 were maintained among patients taking VKA in most studies; however, in Japanese studies, INR values ranging from 1.5 to 2.5 were observed. The mean age, proportion of males and Asians, BMI, weight, and follow-up time varied widely among the studies. Definitions of “major bleeding” used in each individual study are shown inSupplementary Table S1. A Cochrane risk-of-bias assessment is shown in Supplementary Figure S1. The results showed that most studies were of high quality.
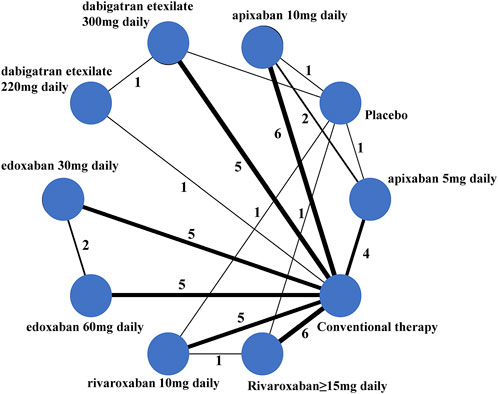
FIGURE 2. Network plot for the Bayesian network meta-analysis. Each node represents a regimen, the lines between the nodes represent the head-to-head comparisons, the thickness of the lines represents the number of studies, and the number of studies is marked beside.
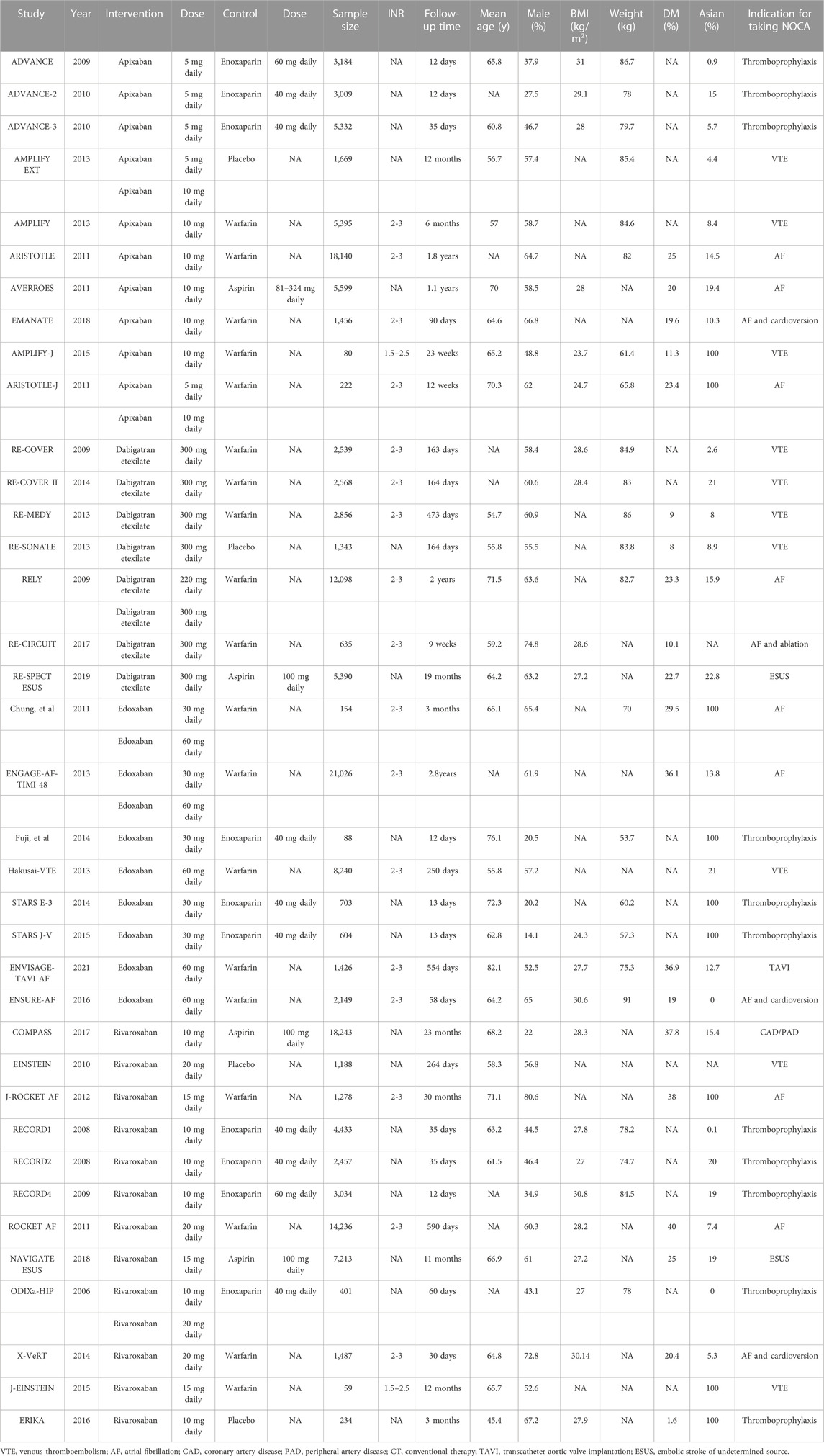
TABLE 1. Characteristics of the included studies and populations.
Meta-analysis
Compared with the control groups, DOACs did not increase the risk of major GI bleeding (OR: 1.08, 95% CI: .89–1.31, p = .4206, I2 = 51%) (shown in Figure 3; Supplemental Figure S2). However, subgroup analysis based on dosages and types of DOACs revealed that, compared with controls, 30 mg daily edoxaban significantly reduced (OR: .67, 95% CI: 0.54–.84, I2 = 0%), whereas 10 mg daily rivaroxaban significantly increased, major GI bleeding risk (OR: 1.41, 95% CI: 1.04–1.93, I2 = 0%). No differences in GI bleeding risk were observed when other DOACs and controls were compared. Significant differences in major GI bleeding risk were observed among patients receiving different DOACs (interactive p-value = .0009).
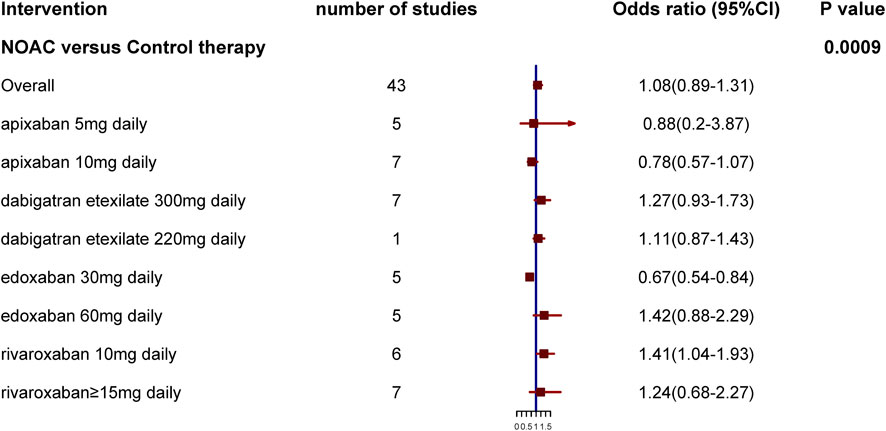
FIGURE 3. Results of subgroup analysis based on dosages and type of direct oral anticoagulants.
Network meta-analysis
The results of this network meta-analysis are shown in Table 2. No DOACs were associated with an increased risk of major GI bleeding compared with conventional therapy. The doses of 300 mg daily dabigatran etexilate, 60 mg daily edoxaban, 10 mg daily rivaroxaban, and ≥15 mg daily rivaroxaban were associated with a higher major GI bleeding risk than the placebo. Among standard-dose DOACs, the risk of major GI bleeding associated with 10 mg daily apixaban was significantly reduced compared with 300 mg daily dabigatran etexilate, 60 mg daily edoxaban, and ≥15 mg daily rivaroxaban (OR: .58, 95% CrI: .34–.97 for dabigatran etexilate, OR: .53, 95% CrI: .28–.86 for edoxaban, and OR: .55, 95% CrI: .31–.93 for rivaroxaban, respectively). The degree of risk associated with 300 mg daily dabigatran etexilate, 60 mg daily edoxaban, and ≥15 mg daily rivaroxaban did not differ.
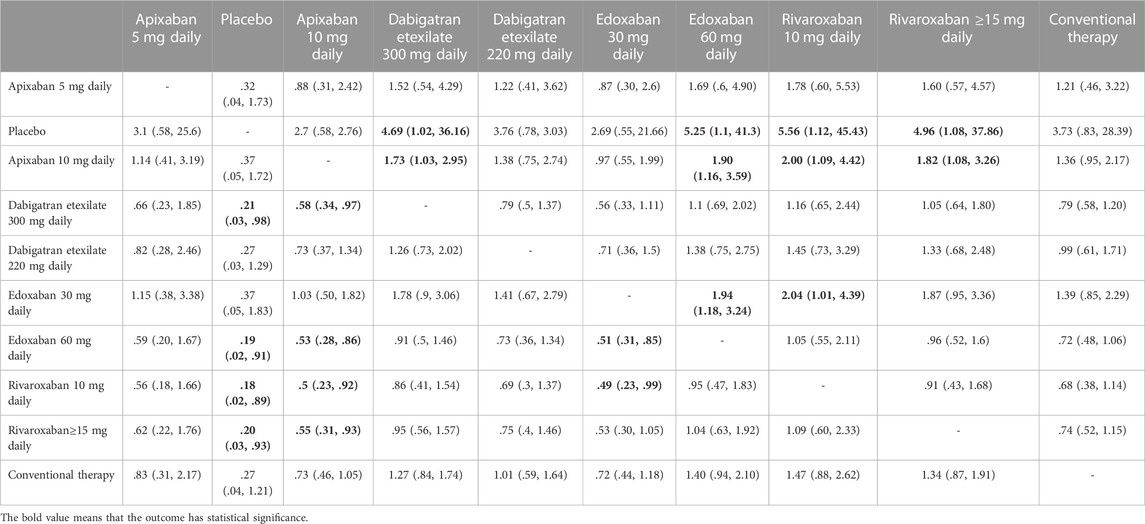
TABLE 2. Estimated relative treatment effects as odds ratio (OR) and corresponding 95% credible intervals.
Among low-dose DOACs, the risk of major GI bleeding associated with 30 mg daily edoxaban was lower than that with 10 mg daily rivaroxaban (OR: .49, 95% CrI: .23–.99). There were no differences between individuals administered with 5 mg daily apixaban, 10 mg daily rivaroxaban, and 220 mg daily dabigatran etexilate, nor between those who received 30 mg daily edoxaban, 5 mg daily apixaban, and 220 mg daily dabigatran etexilate.
Additionally, the dose of 10 mg daily apixaban had a lower major GI bleeding risk than 10 mg daily rivaroxaban. The major GI bleeding risk of 30 mg daily edoxaban was lower than that of 60 mg daily edoxaban.
No inconsistency was observed between direct and indirect evidence (Supplementary Table S2). The results of our network meta-regression analysis showed that clinical outcomes were independent of mean age, BMI, body weight, proportion of males, proportion of Asians, indication, and follow-up time (Supplementary Table S3). A comparison-adjusted funnel plot suggested no publication bias (Supplementary Figure S3).
Discussion
The main findings of the traditional meta-analysis showed that rates of major GI bleeding differ among groups administered with different doses and types of DOACs (p < .1). The network meta-analysis showed that 10 mg daily apixaban was associated with a lower degree of major GI bleeding risk than 300 mg daily dabigatran etexilate, ≥15 mg daily rivaroxaban, and 60 mg daily edoxaban. No between-group differences in bleeding risk associated with 300 mg daily dabigatran etexilate, ≥15 mg daily rivaroxaban, and 60 mg daily edoxaban were observed. The risk of major GI bleeding was reduced in those administered with 30 mg daily edoxaban compared with those administered with 10 mg daily rivaroxaban; no major GI bleeding risk differences between patients administered with 5 mg daily apixaban, 30 mg daily edoxaban, and 220 mg daily dabigatran etexilate were observed.
Differences in the major GI bleeding risk among different DOACs have been observed in previous studies. The COMPASS study evaluated the efficacy and safety of low-dose NOAC use for preventing stable atherosclerotic cardiovascular disease. The risk of major GI bleeding with 10 mg QD rivaroxaban alone was significantly greater than that with aspirin alone (Eikelboom, et al., 2017). The RE-Ly study, which evaluated the use of dabigatran etexilate for the prevention of stroke in AF patients showed that 150 mg and 110 mg BID dabigatran etexilate increased the risk of major GI bleeding compared with warfarin. Furthermore, major GI bleeding risk was significantly higher with dabigatran etexilate 150 mg BID than with 110 mg BID (Connolly, et al., 2009). The ENGAGE AF-TIMI study evaluated the efficacy and safety of edoxaban use for preventing stroke in AF patients (Giugliano, et al., 2013). Its results showed that 60 mg QD edoxaban was associated with a greater degree of major GI bleeding risk than warfarin, while 30 mg QD edoxaban showed lower major GI bleeding risk compared with warfarin. Our study integrated all current research on DOAC use and indirectly compared differences in the major GI bleeding risk associated with different dosages and types of DOACs. The results showed that, among patients administered standard-dose DOACs, those who received apixaban had the lowest risk of major GI bleeding. Furthermore, among those administered with low-dose DOACs, major GI bleeding risk associated with edoxaban was lower than with rivaroxaban. Indeed, the DOACs were commonly used to reduce ischemic events. Nevertheless, it also increased bleeding risk, which causes confusion for clinicians. Our study suggested that major GI bleeding risk differed across DOACs. These findings are important because the drug with the most favorable GI bleeding safety profile should be preferred, especially for treating those at high risks of GI bleeding.
The different bleeding risks among DOACs may be related to the pharmacokinetics of the drugs. For example, rivaroxaban and edoxaban are administered once daily, while dabigatran etexilate and apixaban are administered twice daily, with higher peak plasma concentrations for the former than for the latter. Two previous studies have shown that the peak plasma concentration of rivaroxaban is almost twice that of apixaban, and that the anti-Xa activity is highly correlated with plasma concentrations, such as rivaroxaban with higher maximum anti-Xa activity and higher 24-h area under the curve for anti-Xa activity (Frost, et al., 2014; Kreutz, et al., 2017). However, the above mechanisms still do not fully explain the different bleeding risks between apixaban and dabigatran etexilate as both were administered twice daily. Further studies are needed to elucidate the mechanisms underlying the differences in major GI bleeding risks among DOACs.
Comparison with other studies
In agreement with evidence from previously reported studies, major GI bleeding risk differences were observed among DOACs. In patients with AF, apixaban better reduced the risk of major GI bleeding than rivaroxaban and dabigatran etexilate, and rivaroxaban was associated with a higher risk of major GI bleeding compared with dabigatran etexilate (Abraham, et al., 2017). Rivaroxaban increases the risk of GI bleeding compared with dabigatran etexilate and apixaban, a finding that was independent of the indication for use (Ingason, et al., 2021). However, the above studies were retrospective with the potential for selection bias. Furthermore, their data were limited to those contained within databases, which were limited regarding edoxaban bleeding risk assessment. To date, no studies have directly compared GI bleeding risks amongst individual DOACs due to the very large sample sizes required to perform such studies. Network meta-analyses may be used to indirectly compare the safety of different regimens; thus, performing a network meta-analysis that compares the bleeding risks of different types of DOACs is of great importance. We previously performed a network meta-analysis to evaluate the GI bleeding risk differences among different DOACs. Our findings revealed that apixaban and edoxaban have favorable GI bleeding safety profiles, unlike rivaroxaban and dabigatran etexilate (Guo, et al., 2019). Another study showed that standard-dose apixaban reduced the risk of major GI bleeding compared with standard-dose rivaroxaban and dabigatran etexilate; however, no favorable GI bleeding safety profile was observed with regard to edoxaban use (Radadiya, et al., 2021). Notably, only studies published before 2019 were considered in the above studies. Since then, more studies evaluating the efficacy and safety of DOACs in the treatment of disease have been reported. After including such studies, we found that standard-dose apixaban was associated with a lower risk of major GI bleeding than standard-dose rivaroxaban and dabigatran etexilate; this was similar to the results of the previous meta-analysis. However, our study also found that standard-dose apixaban was associated with a lower major GI risk than standard-dose edoxaban. Additionally, we also compared the major GI bleeding risks between low-dose DOACs, which showed that low-dose edoxaban is associated with a lower degree of GI bleeding risk compared with low-dose rivaroxaban. These findings are additional to the results of the previous meta-analysis.
Study limitations
Our study has some limitations. First, we included studies with different indications for treatment, which may have resulted in bleeding risk differences among the populations considered, thereby increasing study heterogeneity. However, our study excluded studies that recruited patients with cancer, the very elderly, and those receiving antiplatelet background therapy, to minimize the heterogeneity between studies. Furthermore, a random effect model was used to combine evidence. Second, a wide ranging mean age, a prevalence of males and Asians, and follow-up time data also increased heterogeneity between studies. However, we used network meta-regression analysis to evaluate the association between study/population characteristics and clinical outcomes. The analysis revealed that the clinical outcome was independent of study/population characteristics. Third, recent studies have suggested that patients with prior GI bleeding could benefit from DOACs rather than warfarin (Lip, et al., 2021). Our study was based on the study level, and limited data were available regarding patients with prior GI bleeding; therefore, we could not compare GI bleeding risks associated with different DOACs in patients with prior GI bleeding.
Conclusion
This study revealed that DOAC dosage and type affect major GI bleeding risk. Among standard-dose DOACs, apixaban use was associated with the lowest degree of major GI bleeding risk. Among low-dose DOACs, edoxaban was associated with lower major GI bleeding risk than rivaroxaban.
Author contributions
XC and WG designed the research and revised the paper. WG and XC had full access to all the data in the study, took responsibility for the integrity of the data and the accuracy of the data analysis, and wrote the paper. XC, LZ, HL, and LW directed the revision of the paper. WH and LZ performed data searches and conducted data selection. WG and LZ helped with data analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.1049283/full#supplementary-material
Abbreviations
AF, atrial fibrillation; BMI, body mass index; CIs, confidence intervals; CrI, credible interval; DOACs, direct oral anticoagulants; GI, gastrointestinal; INR, international normalized ratio; OR, odds ratio; VKA, vitamin K antagonists.
References
Abraham, N. S., Noseworthy, P. A., Yao, X., Sangaralingham, L. R., and Shah, N. D. (2017). Gastrointestinal safety of direct oral anticoagulants: A large population-based study. Gastroenterology 152 (5), 1014–1022. doi:10.1053/j.gastro.2016.12.018
Agnelli, G., Buller, H. R., Cohen, A., Curto, M., Gallus, A. S., Johnson, M., et al. (2013). Apixaban for extended treatment of venous thromboembolism. N. Engl. J. Med. 368 (8), 699–708. doi:10.1056/NEJMoa1207541
Brooks, S. P., and Gelman, A. (1998). General methods for monitoring convergence of iterative simulations. J. Comput. Graph. Statistics 7 (4), 434–455. doi:10.1080/10618600.1998.10474787
Chung, N., Jeon, H. K., Lien, L. M., Lai, W. T., Tse, H. F., Chung, W. S., et al. (2011). Safety of edoxaban, an oral factor Xa inhibitor, in Asian patients with non-valvular atrial fibrillation. Thromb. Haemost. 105 (3), 535–544. doi:10.1160/TH10-07-0451
Connolly, S. J., Ezekowitz, M. D., Yusuf, S., Eikelboom, J., Oldgren, J., Parekh, A., et al. (2009). Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 361 (12), 1139–1151. doi:10.1056/NEJMoa0905561
Deitelzweig, S., Keshishian, A., Kang, A., Dhamane, A. D., Luo, X., Balachander, N., et al. (2021). Burden of major gastrointestinal bleeding among oral anticoagulant-treated non-valvular atrial fibrillation patients. Ther. Adv. Gastroenterol. 14, 1756284821997352. doi:10.1177/1756284821997352
DerSimonian, R., and Laird, N. (1986). Meta-analysis in clinical trials. Control Clin. Trials 7 (3), 177–188. doi:10.1016/0197-2456(86)90046-2
Dias, S., Sutton, A. J., Ades, A. E., and Welton, N. J. (2013a). Evidence synthesis for decision making 2: A generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Mak. 33 (5), 607–617. doi:10.1177/0272989X12458724
Dias, S., Sutton, A. J., Welton, N. J., and Ades, A. E. (2013b). Evidence synthesis for decision making 3: heterogeneity--subgroups, meta-regression, bias, and bias-adjustment. Med. Decis. Mak. 33 (5), 618–640. doi:10.1177/0272989X13485157
Dias, S., Welton, N. J., Caldwell, D. M., and Ades, A. E. (2010). Checking consistency in mixed treatment comparison meta-analysis. Stat. Med. 29 (7-8), 932–944. doi:10.1002/sim.3767
Eikelboom, J. W., Connolly, S. J., Bosch, J., Dagenais, G. R., Hart, R. G., Shestakovska, O., et al. (2017). Rivaroxaban with or without aspirin in stable cardiovascular disease. N. Engl. J. Med. 377 (14), 1319–1330. doi:10.1056/NEJMoa1709118
Eriksson, B. I., Borris, L., Dahl, O. E., HaaS, S., Huisman, M. V., Kakkar, A. K., et al. (2006). Oral, direct Factor Xa inhibition with BAY 59-7939 for the prevention of venous thromboembolism after total hip replacement. J. Thromb. Haemost. 4 (1), 121–128. doi:10.1111/j.1538-7836.2005.01657.x
Frost, C., Song, Y., Barrett, Y. C., Wang, J., Pursley, J., Boyd, R. A., et al. (2014). A randomized direct comparison of the pharmacokinetics and pharmacodynamics of apixaban and rivaroxaban. Clin. Pharmacol. 6, 179–187. doi:10.2147/CPAA.S61131
Giugliano, R. P., Ruff, C. T., Braunwald, E., Murphy, S. A., Wiviott, S. D., Halperin, J. L., et al. (2013). Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 369 (22), 2093–2104. doi:10.1056/NEJMoa1310907
Gu, Z. C., Wei, A. H., Zhang, C., Wang, X. H., Zhang, L., Shen, L., et al. (2020). Risk of major gastrointestinal bleeding with new vs conventional oral anticoagulants: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 18 (4), 792–799. e761. doi:10.1016/j.cgh.2019.05.056
Guo, W. Q., Chen, X. H., Tian, X. Y., and Li, L. (2019). Differences in gastrointestinal safety profiles among novel oral anticoagulants: Evidence from A network meta-analysis. Clin. Epidemiol. 11, 911–921. doi:10.2147/CLEP.S219335
Higgins, J. P., Altman, D. G., Gotzsche, P. C., Juni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928. doi:10.1136/bmj.d5928
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327 (7414), 557–560. doi:10.1136/bmj.327.7414.557
Ingason, A. B., Hreinsson, J. P., Agustsson, A. S., Lund, S. H., Rumba, E., Palsson, D. A., et al. (2021). Rivaroxaban is associated with higher rates of gastrointestinal bleeding than other direct oral anticoagulants : A nationwide propensity score-weighted study. Ann. Intern. Med. 174 (11), 1493–1502. doi:10.7326/M21-1474
Kearon, C., Akl, E. A., Ornelas, J., Blaivas, A., Jimenez, D., Bounameaux, H., et al. (2016). Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 149 (2), 315–352. doi:10.1016/j.chest.2015.11.026
Kreutz, R., Persson, P. B., Kubitza, D., Thelen, K., Heitmeier, S., SchwerS, S., et al. (2017). Dissociation between the pharmacokinetics and pharmacodynamics of once-daily rivaroxaban and twice-daily apixaban: A randomized crossover study. J. Thromb. Haemost. 15 (10), 2017–2028. doi:10.1111/jth.13801
Lip, G. Y. H., Keshishian, A. V., Zhang, Y., Kang, A., Dhamane, A. D., Luo, X., et al. (2021). Oral anticoagulants for nonvalvular atrial fibrillation in patients with high risk of gastrointestinal bleeding. JAMA Netw. Open 4 (8), e2120064. doi:10.1001/jamanetworkopen.2021.20064
Miller, C. S., Dorreen, A., Martel, M., Huynh, T., and Barkun, A. N. (2017). Risk of gastrointestinal bleeding in patients taking non-vitamin K antagonist oral anticoagulants: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 15 (11), 1674–1683. e1673. doi:10.1016/j.cgh.2017.04.031
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6 (7), e1000097. doi:10.1371/journal.pmed.1000097
Ogawa, S., Shinohara, Y., and Kanmuri, K. (2011). Safety and efficacy of the oral direct factor xa inhibitor apixaban in Japanese patients with non-valvular atrial fibrillation. -The ARISTOTLE-J study. Circ. J. 75 (8), 1852–1859. doi:10.1253/circj.cj-10-1183
Radadiya, D., Devani, K., Brahmbhatt, B., and Reddy, C. (2021). Major gastrointestinal bleeding risk with direct oral anticoagulants: Does type and dose matter? - a systematic review and network meta-analysis. Eur. J. Gastroenterol. Hepatol. 33, e50–e58. doi:10.1097/MEG.0000000000002035
Salanti, G., Ades, A. E., and Ioannidis, J. P. (2011). Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 64 (2), 163–171. doi:10.1016/j.jclinepi.2010.03.016
Steffel, J., Collins, R., Antz, M., Cornu, P., Desteghe, L., Haeusler, K. G., et al. (2021). European heart rhythm association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Europace 23 (10), 1612–1676. doi:10.1093/europace/euab065
Turner, R. M., Davey, J., Clarke, M. J., Thompson, S. G., and Higgins, J. P. (2012). Predicting the extent of heterogeneity in meta-analysis, using empirical data from the Cochrane Database of Systematic Reviews. Int. J. Epidemiol. 41 (3), 818–827. doi:10.1093/ije/dys041
Keywords: randomized controlled trial, major gastrointestinal bleeding, novel oral anticoagulants, meta-analysis, network meta-analysis
Citation: Chen X, Wang L, Li H, Huang W, Zhao L and Guo W (2023) Comparative differences in the risk of major gastrointestinal bleeding among different direct oral anticoagulants: An updated traditional and Bayesian network meta-analysis. Front. Pharmacol. 13:1049283. doi: 10.3389/fphar.2022.1049283
Received: 20 September 2022; Accepted: 01 December 2022;
Published: 04 January 2023.
Edited by:
Christos Kontogiorgis, Democritus University of Thrace, GreeceReviewed by:
Guo Chengxian, Third Xiangya Hospital, Central South University, ChinaWalter Jeske, Loyola University Chicago, United States
Copyright © 2023 Chen, Wang, Li, Huang, Zhao and Guo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenqin Guo, Z3Vvd2VucWluMjAxMUBvdXRsb29rLmNvbQ==