 Irina I. Belyaeva1,2
Irina I. Belyaeva1,2 Anna G. Subbotina1,2Ivan I. Eremenko1,2Vadim V. Tarasov2,3
Anna G. Subbotina1,2Ivan I. Eremenko1,2Vadim V. Tarasov2,3 Vladimir N. Chubarev2Helgi B. Schiöth1,3
Vladimir N. Chubarev2Helgi B. Schiöth1,3 Jessica Mwinyi1*
Jessica Mwinyi1*- 1Department of Surgical Sciences, Functional Pharmacology and Neuroscience, University of Uppsala, Uppsala, Sweden
- 2Department of Pharmacology, Institute of Pharmacy, I. M. Sechenov First Moscow State Medical University, Moscow, Russia
- 3Institute of Translational Medicine and Biotechnology, I. M. Sechenov First Moscow State Medical University, Moscow, Russia
Primary headache disorders, such as migraine, tension-type headache (TTH), and cluster headache, belong to the most common neurological disorders affecting a high percentage of people worldwide. Headache induces a high burden for the affected individuals on the personal level, with a strong impact on life quality, daily life management, and causes immense costs for the healthcare systems. Although a relatively broad spectrum of different pharmacological classes for the treatment of headache disorders are available, treatment effectiveness is often limited by high variances in therapy responses. Genetic variants can influence the individual treatment success by influencing pharmacokinetics or pharmacodynamics of the therapeutic as investigated in the research field of pharmacogenetics. This review summarizes the current knowledge on important primary headache disorders, including migraine, TTH, and cluster headache. We also summarize current acute and preventive treatment options for the three headache disorders based on drug classes and compounds taking important therapy guidelines into consideration. Importantly, the work summarizes and discusses the role of genetic polymorphisms regarding their impact on metabolism safety and the effect of therapeutics that are used to treat migraine, cluster headache, and TTH exploring drug classes such as nonsteroidal anti-inflammatory drugs, triptans, antidepressants, anticonvulsants, calcium channel blockers, drugs with effect on the renin–angiotensin system, and novel headache therapeutics such as ditans, anti-calcitonin-gene-related peptide antibodies, and gepants. Genetic variants in important phase I-, II-, and III-associated genes such as cytochrome P450 genes, UGT genes, and different transporter genes are scrutinized as well as variants in genes important for pharmacodynamics and several functions outside the pharmacokinetic and pharmacodynamic spectrum. Finally, the article evaluates the potential and limitations of pharmacogenetic approaches for individual therapy adjustments in headache disorders.
Introduction
Approximately one-half of the adult population worldwide is affected by a headache disorder (Hainer and Matheson, 2013). Headache is the most frequently occurring neurological symptom and the most prevalent type of pain in children and adolescents (Faedda et al., 2016). Headache has a disabling potential and leads to reduced life quality and limitations in the social sphere (Nieswand et al., 2020). Headache disorders are ranked as the second most common cause of years of life spent with disability worldwide (Schwaiger et al., 2009; Saylor and Steiner, 2018). For tension-type headache (TTH), the global age-standardized prevalence was 26.1% overall: 30.8% for women and 21.4% for men, and for migraine, the global age-standardized prevalence was 14.4% overall: 18.9% for women and 9.8% for men, according to the Global Burden of Diseases, Injuries, and Risk Factors studies (GBD 2016 Headache Collaborators, 2018). In the European Union, the total annual cost of headache among adults aged 18–65 years was estimated at 173 billion euros, apportioned in 64% to migraine, 12% to TTH, 21% to medication-overuse headache, and 2% to other types of headaches (Linde et al., 2012).
Today, a high number of treatment possibilities are available for headache disorders. However, headache patients react differently to given drugs leading to a wide variety of treatment responses. It is estimated that only 50% of migraine patients adequately respond to acute and preventive therapy (Pomes et al., 2019; Zobdeh et al., 2021). Likewise, many patients with cluster headache fail to respond adequately to pharmacological treatment approaches. Additionally, a significant number of these patients experience misdiagnoses or diagnostic delays, which constraints the possibility of the timely application of adequate abortive and preventive therapy (Ljubisavljevic and Zidverc Trajkovic, 2019). The therapeutic efficacy of analgesics in TTH tends to decrease with increasing headache frequency (Bendtsen et al., 2010). Especially, patients with TTH have a higher risk of developing medication overuse headache due to the regular and frequent use of analgesics, with a subsequent drug-induced increase in headache frequency and chronification (Diener et al., 2019).
Pharmacogenetics investigates the association between genetic markers and the pharmacokinetics and pharmacodynamics of the drug and aims at predicting the individual therapy response based on these associations (Valdes and Yin, 2016). In recent times, advances have been made in neuropsychiatry regarding the understanding of the role of genetic polymorphisms in therapy response to treatment approaches as in major depressive disorder (Shalimova et al., 2021), schizophrenia (Jovanović et al., 2010), or epilepsy (Al-Eitan et al., 2020). The role of pharmacogenetics for therapy success with compounds used for the treatment of headache disorders is not as largely investigated, and pharmacogenetic information is hitherto practically not used to predict efficacy or adverse effects in clinical practice in this field (Christensen et al., 2016).
A rather broad number of therapeutics are nowadays available for the treatment of headache disorders. These include, e.g., nonsteroidal anti-inflammatory drugs (NSAIDs), triptans, ergot derivatives, gepants, and ditans for the acute treatment for migraines and calcitonin-gene-related peptide (CGRP) monoclonal antibodies, onabotulinumtoxinA, calcium channel blockers (CCBs), beta-blockers, and anticonvulsants for prophylactic treatment for migraines. Cluster headache is as well treated by triptans and ergot derivatives besides the use of oxygen in the acute phase and by anti-CGRP monoclonal antibodies, CCBs, anticonvulsants prophylactically. NSAIDs are used as an acute treatment for TTH. Tricyclic antidepressants (TCAs) and neurotransmitter release antagonists are used as prophylactic treatment for TTH. Therapeutics of several important classes of drugs that are used for the treatment of headache disorders have been shown to be substrates of polymorphically expressed metabolizing enzymes, transport systems, or receptors. However, the translation of this knowledge into applicable recommendations for individual dose adjustments is currently missing in the area of headache disorders.
The review summarizes the current knowledge about drug classes and compounds used for the treatment of commonly occurring and important types of primary headache disorders, characterizes important pharmacogenetic variants that affect the pharmacokinetics and pharmacodynamics of these drugs, and sheds light on the question to what extent the pharmacogenetic achievements may have been translated into treatment recommendations.
Methods
The review aimed to include broad and comprehensive information regarding treatment guidelines and pathophysiology of the headache disorders TTH, cluster headache, and migraine and information regarding pharmacogenetics and its role in the safety and efficacy of drugs used for the treatment of the mentioned diseases. This was achieved by a thorough search in the scientific literature using the search database PubMed and using search terms in different combinations and different long combination chains including “epidemiology, prevalence of migraine/TTH/cluster headache; pathophysiology, triggers, symptoms, diagnosis, acute/chronic treatment, treatment recommendations, pharmacotherapy of migraine/TTH/cluster headache; mechanism of action, metabolism/metabolic pathways, pharmacokinetics, pharmacodynamics, pharmacogenetics, candidate genes, genetic polymorphism/SNP/genetic variants, cytochrome P450/CYP, safety, efficacy/effect, adverse effects/adverse reactions in combinations which each of the headache disorders and different recommended drug/drug classes.” The focus was mainly laid on drug and drug classes recommended by the official treatment guidelines in Europe and the USA, which were considered separately in the search runs together with the three different headache types in focus. Articles considered were mainly clinical trials and studies that included human subjects.
Important Types of Headaches—Disease Burden, Clinical Forms, and Pathophysiology
Migraine
Migraine is one of the most common types of headaches. Twelve percent are affected at least once by an acute migraine attack, and approximately 2.5% of the global population show chronic migraine. Migraine ranks second place among the causes of temporary disability worldwide (GBD 2016 Headache Collaborators, 2018; Burch et al., 2019). Migraine is characterized by a strong unilateral headache occurring with nausea, vomiting, photophobia, and phonophobia that lasts from several hours to several days. Two main subtypes of migraine are distinguished, i.e., migraine with aura and migraine without aura (Cephalalgia, 2018). In contrast to migraine without aura, migraine with aura manifests with a headache accompanied by various local neurological and visual symptoms, of which photopsia, photophobia, and temporary visual disturbances are very common. Symptoms, such as, e.g., sensitivity disorders, vestibular symptoms, or temporary paresis, may also be observed. Rare and atypical migraine syndromes include familial hemiplegic migraine, basilar migraine, ophthalmoplegic migraine, and exceptional retinal migraine (Fraser et al., 2019). In contrast to episodic migraine, chronic migraine occurs on 15 or more days per month for at least 3 months (Cephalalgia, 2018).
The etiopathogenetic mechanisms of migraine development are not fully understood. Migraine affects women three times more often than men (Broner et al., 2017) and shows the highest incidences in young patients between 30 and 40 years (GBD 2016 Headache Collaborators, 2018). There is evidence for a hereditary component that influences the likelihood of developing migraine (de Boer et al., 2019). Genetic susceptibility factors differ between migraine with and without aura (Pisanu et al., 2017a). Other risk factors comprise concomitant psychological and psychiatric disorders (Pisanu et al., 2020), hormonal status, myofascial syndromes, and the influence of various adverse environmental factors, including nutritional factors or stressful situations (Chai et al., 2014; Pisanu et al., 2017b; Marmura, 2018; Zobdeh et al., 2021). Numerous studies have identified a variety of factors that can trigger migraine attacks. Examples are psychological and physical stress, menstrual cycle changes, weather changes, sleep disturbances, alcohol and other dietary compounds, barometric changes, or starvation (Marmura, 2018). The widely accepted theory of migraine pathophysiology suggests the abundance of a neurovascular conflict involving the trigeminal nerve and underlying neuroinflammation, which causes changes in vascular tone, represented by initial vasospasm and subsequent vasodilation (Charles, 2018; Ferrari et al., 2015; Kojić and Stojanović, 2013). It is assumed that the trigeminovascular conflict is preceded by complex interactions between the cortex, hypothalamus, and subcortical nuclei responsible for pain perception and activation of the antinociceptive system (Dodick, 2018). The interaction between the hypothalamus and the trigeminal nucleus caudalis probably triggers the activation of the trigeminovascular system and subsequently occurring migraine attacks. Cortical spreading depression is assumed to play a key role in the trigeminal activation in migraine with aura (Haanes and Edvinsson, 2019).
An imbalance in the system of serotonin and norepinephrine and other monoamines is assumed to also play a role in the pathogenesis of migraine (Tardiolo et al., 2019). In recent years, CGRP has been recognized as one of the key mediators of migraine development. CGRP plays a relevant role in the trigeminovascular system as an intermediary agent between vascular reactions and the perception of changes in vascular tone as a pain stimulus (Iyengar et al., 2019). It has been shown that CGRP levels are significantly increased in migraine patients compared with the healthy population (Schou et al., 2017). CGRP release from the primary afferent fibers in the trigeminal ganglion is closely associated with the nitric oxide system and other agents that cause peripheral and central neuronal sensitization, which underlies the transition of acute to chronic forms of migraine (Goadsby et al., 2017; Puledda et al., 2017). The elucidation of CGRP led to a new era in migraine therapy based on CGRP antibodies and receptor antagonists that are currently the most efficient compounds available in chronic migraine (Deen et al., 2017; Negro and Martelletti, 2019).
Tension-Type Headache
TTH affects many individuals worldwide (Ashina et al., 2021). The lifetime prevalence of TTH ranges between 30 and 78% (Wrobel Goldberg et al., 2014). According to the European Headache Federation (EHF), most people occasionally experience TTH, whereas 10% show frequent repeats of TTH. Chronic TTH occurs in approximately 3% of adults and in some children in Europe (Steiner et al., 2019). Mainly because of its high prevalence, the socioeconomic consequences of TTH are significant (Wrobel Goldberg et al., 2014). Studies show that frequent episodic and chronic TTH occur significantly more frequently in women than men (Russell, 2005). TTH is most commonly observed among women aged 15–49 years (GBD 2016 Headache Collaborators, 2018).
TTH is subdivided into episodic and chronic types. Although infrequent episodic TTH usually has a rather little impact on the individual and is often self-limiting, frequent episodic TTH can be associated with considerable disability and may warrant pharmacological treatment (Cephalalgia, 2018). Chronic TTH occurs on 15 days a month or more for at least 3 months, may be daily and unremitting, and may be associated with mild nausea (Steiner et al., 2019). Chronic TTH is a serious disease, causing greatly decreased quality of life and a high rate of disability (Cephalalgia, 2018).
The pathophysiology of TTH is still not fully understood (Monteith and Oshinsky, 2009). Sensitization of second-order neurons at the level of the spinal dorsal horn or trigeminal nucleus, sensitization of supraspinal neurons, and decreased descending inhibition from supraspinal structures play a major role in the pathophysiology of chronic TTH. Furthermore, an increased pericranial myofascial pain sensitivity may also play a role (Bendtsen, 2000). The pain is usually bilateral, mild to moderate, is of a pressing or tightening quality, and is usually not accompanied by other symptoms (Wrobel Goldberg et al., 2014). Sometimes, it is difficult to distinguish between migraine, TTH, or other headache types (Burch, 2019a). Several triggers are known for TTH. Certain myofascial trigger points in the muscles of the head and neck may cause a local twitching reaction and spontaneous pain (Gildir et al., 2019). Sleep disorders have been identified as a risk factor for TTH and a transition from episodic to chronic TTH (Rains et al., 2015). TTH can also be triggered by negative affect and sunlight (Wang et al., 2013). Frequent episodic and chronic TTH is assumed to be caused by a combination of genetic and environmental factors, whereas infrequent episodic TTH is assumed to be primarily triggered by environmental factors (Russell, 2007).
TTH therapy comprises both non-pharmacological treatments, including patient education, disease information, and lifestyle change advice, and pharmacological therapy approaches, such as the use of NSAIDs and TCAs (Lenaerts, 2009) (Tables 1 and 2). The choice of a particular approach depends on the severity of the disease. Mild forms should be initially non-pharmacologically treated (Steiner et al., 2019). Amitriptyline may be used as a preventive therapy for chronic TTH (Wrobel Goldberg et al., 2014). Nonprescription analgesics are indicated for the management of episodic TTH (Scripter, 2018). Chronic TTH often does not respond to drug treatment and makes it necessary to apply psychological approaches (Steiner et al., 2019).
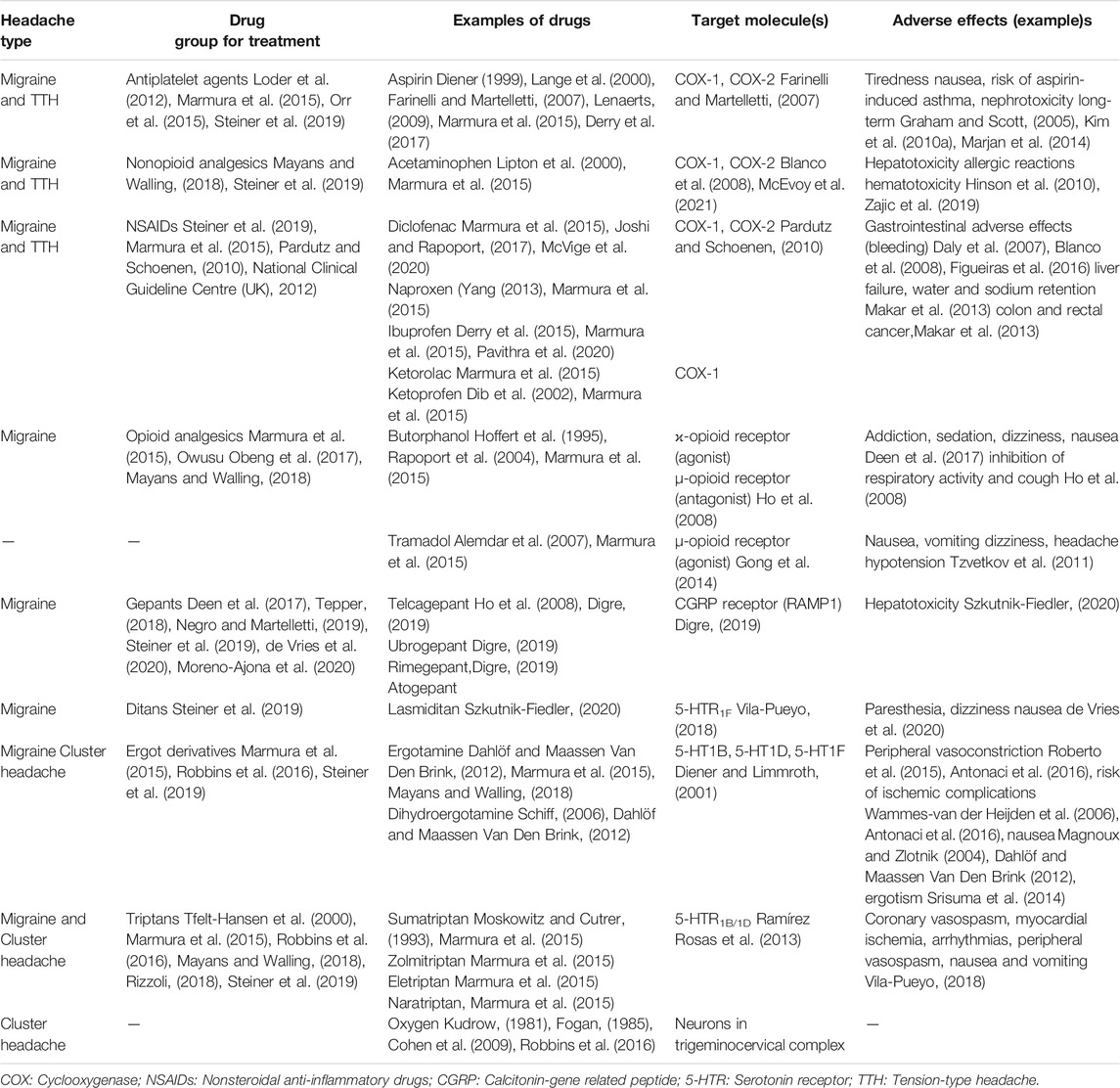
TABLE 1. Treatment principles of primary headache disorders—acute treatment options.
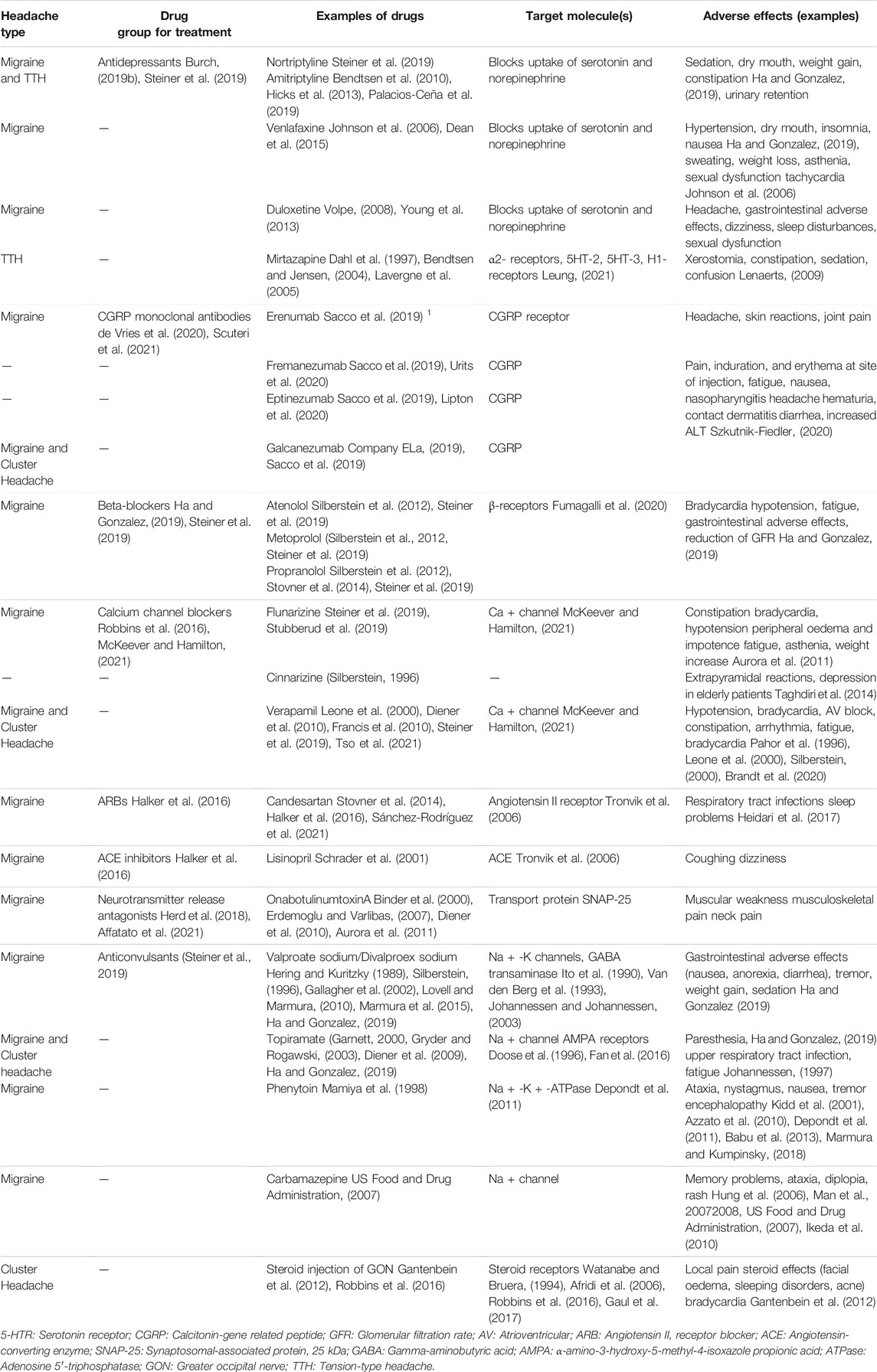
TABLE 2. Treatment principles of primary headache disorders—treatment options for prevention.
Cluster Headache
Cluster headache has a prevalence of 0.2–0.3% in Europe, and it has a rather low frequency compared with other headaches considered in this review (Stovner and Andree, 2010). The headache type is more prevalent in men with a male-to-female ratio of 6–7:1 (Rozen et al., 2001) and typically begins between 20 and 40 years of age (Weaver-Agostoni, 2013). The severity of the disorder has major effects on the patient's quality of life and is, in some very severe cases, associated with suicidal ideation (Hoffmann and May, 2018). Patients describe a cluster headache attack as an intense and severe strictly unilateral pain, typically in the supraorbital, retro-orbital, or temporal regions and arising from deep within (Wei et al., 2019). Attacks last 15–180 min and may be accompanied by tears, conjunctival injection (redness of the sclera), rhinorrhea, nasal congestion, hyperhidrosis (excessive sweating), and eyelid edema (May et al., 2018). Cluster headache attacks can occur once every other day at the start of the disease and increase up to eight times a day (Lai et al., 2009). Cluster headache is subdivided into episodic and chronic types. Patients are deemed to have episodic cluster headache if the break between the bouts lasts longer than 3 months while not taking a preventive treatment. Patients who have bouts of attacks with breaks of less than 3 months between are classified as having chronic cluster headaches (Cephalalgia, 2018).
The exact pathophysiology of cluster headache remains unknown (Brandt et al., 2020). Current theories implicate mechanisms, such as vascular dilation, trigeminal nerve stimulation, and circadian effects, histamine release, genetic factors, and autonomic nervous system activation (Weaver-Agostoni, 2013). Triggers for cluster headaches include vasodilators (e.g., alcohol, nitroglycerin) and histamine. Tobacco use or secondary childhood exposure is a risk factor for cluster headaches (Weaver-Agostoni, 2013). There is, to some degree, a genetic component, as first-degree family members are 18 times more likely to be diagnosed with cluster headaches (Kandel and Mandiga, 2021).
Cluster headache requires drug therapy (Weatherall, 2015). The usual first-line preventive treatment for cluster headache is verapamil (Weatherall, 2015; Leone et al., 2000) (Table 2). If verapamil is not tolerated or effective, then typical second-line therapies include topiramate and lithium carbonate (Weatherall, 2015). For acute treatment of cluster headache, triptans, high-flow oxygen, octreotide, or local anesthetics are used (Cohen et al., 2009; Law et al., 2013; Weatherall, 2015). Effective treatment of cluster headache should be established by a doctor as soon as possible. In addition to drug therapy, neuromodulation can be used. Every patient with active cluster headache requires frequent follow-up both to ensure that optimum acute and preventative treatments are maintained and to monitor for treatment toxicity (Steiner et al., 2019).
Important Drug Groups Used for the Treatment of Headache Disorders
Migraine
Migraine treatment can be divided into two main areas, i.e., the treatment of an acute migraine attack to achieve symptomatic pain relief and pharmacological prevention of attacks in chronic migraine (Digre, 2019). For relief of an acute migraine attack, EHF, the American Academy of Neurology (AAN), and the Canadian Headache Society recommend using drugs belonging to the drug classes of triptans (sumatriptan, zolmitriptan, eletriptan, and naratriptan), NSAIDs (ibuprofen, ketoprofen, naproxen, diclofenac, and ketorolac), aspirin, paracetamol, and gepants (telcagepant, ubrogepant, rimegepant, and atogepant), and ditans (lasmiditan) (Loder et al., 2012; Marmura et al., 2015; Orr et al., 2015; Rawson et al., 2017; Steiner et al., 2019). In very difficult cases with uncontrolled symptoms, opioids, such as tramadol or butorphanol, can be used according to AAN and American Headache Society (AHS) (Loder et al., 2012; Marmura et al., 2015). Treatment choice should be based on the patient's age, the presence of concomitant diseases, and the effectiveness in the particular patient (Rizzoli, 2018). Most of these therapeutics are only effective in relieving the pain symptoms of migraine but are not effective against aura symptoms. Triptans have been shown to improve also symptoms such as photopsia and visual disturbances (Tang et al., 2020). Ergot alkaloids remain as second-line options due to their adverse event profile with increased risk, e.g., cardiovascular adverse effects (Tfelt-Hansen et al., 2000; Dahlöf and Maassen Van Den Brink, 2012; Srisuma et al., 2014; Antonaci et al., 2016; Mayans and Walling, 2018).
Drugs used for the treatment of acute migraine have relevant adverse effects. NSAIDs are associated with gastrointestinal bleeding, hepatotoxicity, and cardiovascular adverse effects, whereas the most important adverse effects for acetaminophen are hepatotoxicity, allergic reactions, and hematotoxicity (Zajic et al., 2019). Gepants (ubrogepant and rimegepant) are known to be associated with hypersensitivity reactions, nausea, insomnia, dry mouth, and probably hepatotoxicity (Moreno-Ajona et al., 2020; Szkutnik-Fiedler, 2020). Triptans can induce peripheral vasospasm, coronary vasospasm, myocardial ischemia, arrhythmias, nausea, and vomiting, whereas ditans can cause sedation, vertigo, paraesthesia, and anxiety (Vila-Pueyo, 2018) (Table 1).
Preventive treatment of migraines can be divided into three main areas, i.e., preemptive, short-term, and maintenance treatment (Sacco et al., 2019). Preemptive treatment is relevant in the case a trigger is known (e.g., physical activity). In this case, a drug such as, e.g., an NSAID or triptan, is taken a few hours before the trigger starts. Short-term treatment can be effective in the case a trigger lasts longer (for example, staying at a high altitude or menstruation) and is implemented through preventive administration of NSAIDs or triptans (frovatriptan) before the start and during the triggering event. Maintenance treatment is carried out constantly and is indicated for frequent migraine attacks that limit the ability to work and reduce the quality of life and for special types of migraines (hemiplegic migraine, migraine with a stem aura) (Ha and Gonzalez, 2019; Marmura et al., 2015). According to the recommendations of EHF, AAN, and the Canadian Headache Society, the key drugs for preventive maintenance treatment include anticonvulsants (sodium valproate, topiramate, and divalproex sodium), drugs from the group of beta-blockers (metoprolol, timolol, propranolol, etc.), TCAs (e.g., amitriptyline), selective serotonin reuptake inhibitors or serotonin–norepinephrine reuptake inhibitors (SNRIs, e.g., venlafaxine), angiotensin-converting enzyme inhibitors (ACE inhibitors, lisinopril), angiotensin receptor blockers (ARBs, candesartan), and CCBs (e.g., flunarizine and verapamil) (Steiner et al., 2019; Silberstein et al., 2012; Loder et al., 2012) (Table 2). Cinnarizine and verapamil may be used as alternative drugs to prevent migraines, e.g., in refractory migraine cases or when flunarizine is not available (Knezevic et al., 2018). Food and Drug Administration (FDA) (2019) and European Medicines Agency (2018) have recently approved using CGRP monoclonal antibodies (erenumab, galcanezumab, fremanezumab, and eptinezumab) for the prevention treatment of chronic migraine (Steiner et al., 2019; Moreno-Ajona et al., 2020; Sacco et al., 2019; Suwała et al., 2019; Shams et al., 2006). Therapy with botulinum toxin type A (onabotulinumtoxinA) is recommended by EHF and AAN as an equally significant and effective alternative for migraine prevention (Digre, 2019; Affatato et al., 2021; Herd et al., 2018) (Table 2). The drugs described earlier have a wide range of adverse effects. Anticonvulsants are known to be associated with central (vertigo, hallucinations, depression, nystagmus, tinnitus, dysarthria, dyskinesia, etc.) and peripheral (arrhythmias, hematologic toxicity, liver failure, interstitial nephritis, and allergic reactions) adverse effects and have a teratogenic potential (Silberstein, 1996; Diener et al., 2009; Fricke-Galindo et al., 2018b; Marmura and Kumpinsky, 2018). Beta-blockers, calcium antagonists, and ACE inhibitors have been shown to affect the heart rate (bradycardia) and myocardial contractility, blood pressure (hypotension), and renal function (reduction of GFR), respectively (Ha and Gonzalez, 2019; Steiner et al., 2019). Anti-CGRP monoclonal antibodies can cause hypersensitivity reactions (including skin rash, pruritus, angioedema, and anaphylaxis) and constipation (Szkutnik-Fiedler, 2020).
Tension-Type Headache
The EHF states that the objective of management in both episodic and chronic subtypes of TTH is total attack suppression. Drugs exist to control TTH attacks, but prevention is the overall aim of treatment (Steiner et al., 2019). The EHF recommends starting the treatment of TTH with lifestyle changes and over-the-counter analgesics. If this treatment approach is insufficient amitriptyline or nortriptyline (first line drugs), mirtazapine (second-line drug) or venlafaxine (third-line drug) can be used (Steiner et al., 2019).
A systematic review recently summarized the effectiveness of onabotulinumtoxinA in chronic TTH. The review showed mixed results, which were likely due to variable study designs used in the 22 studies identified, and concluded that there was only low quality of evidence for the effect of onabotulinumtoxinA in TTH (Erdemoglu and Varlibas, 2007). OnabotulinumtoxinA is not recommended for TTH by the EHF and the AAN (Simpson et al., 2016; Steiner et al., 2019). The TCA amitriptyline is widely used for the prophylactic treatment of chronic TTH based on studies that demonstrated the efficacy of amitriptyline in chronic TTH (Ghadiri-Sani and Silver, 2016). Venlafaxine and mirtazapine are also effective for the treatment of TTH (Ashina et al., 2021). The effectiveness of venlafaxine has been proven in a clinical study on 60 patients (Zissis et al., 2007). Mirtazapine's effectiveness in chronic TTH was proven in a clinical trial with 24 patients (Bendtsen and Jensen, 2004). Ibuprofen can be used to treat acute headache attacks in patients with episodic TTH, reaching a relief of paint around 2 h later (Derry et al., 2015) (Tables 1 and 2).
Cluster Headache
The treatment of cluster headache can be divided into three therapy approaches, i.e., a fast-acting abortive treatment, preventive drug treatment, and transitional treatment approaches to bridge the period between patients starting preventive drug treatment and the drugs asserting an effect. The main goal in cluster headache treatment should always be to prevent all attacks (Brandt et al., 2020).
The EHF recommends triptans and oxygen as an acute treatment of cluster headaches. Preventive treatment should be started using prednisolone as a transition therapy (Obermann et al., 2021) option to obtain a quicker response according to the EHF (Tables 1 and 2). Verapamil, lithium carbonate, and topiramate can be used for maintenance prophylaxis (Steiner et al., 2019). The AHS recommends the use of CCBs (e.g., verapamil) and civamide (capsaicin) and the injection of steroids, lithium, and melatonin as preventive treatment options. The AHS and the EHF recommend triptans and oxygen for acute therapy (Robbins et al., 2016). The EHF and the AHS do not recommend sodium valproate for cluster headaches. Some studies have shown that valproate sodium may be effective for treating cluster headache as reviewed in Magnoux and Zlotnik (2004) and shown for refractory forms of this headache type (Magnoux and Zlotnik, 2004). The effectiveness of ergotamine in cluster headaches varies depending on the expression of certain genes (Borro et al., 2019). According to the AHS, there is insufficient evidence to advise the use of ergotamine for the acute treatment of cluster headaches (Robbins et al., 2016). The EHF does not mention ergotamine as a treatment option for cluster headaches (Steiner et al., 2019). Galcanezumab (Emgality) was recently approved by the FDA for the treatment of episodic cluster headache. The recommended dosage of Emgality is 300 mg (administered as three consecutive subcutaneous injections of 100 mg each) at the onset of the cluster period and then monthly until the end of the cluster period (Company ELa, 2019).
Pharmacogenetics of Important Drugs Used in Migraine, Tension-Type Headache, and Cluster Headache
Antiplatelet Agents
Acetylsalicylic acid (ASA, Aspirin) is an irreversible inhibitor of cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2). The complex effect of aspirin on pain and headache disorders is explained by its anti-inflammatory, antiplatelet, and analgesic properties (Farinelli and Martelletti, 2007). Adverse effects of aspirin are similar to those of NSAIDs. Aspirin is characterized by an increased risk of bleeding (due to antiplatelet properties), a higher risk of aspirin-induced asthma, and rebound headaches with long time use (Marjan et al., 2014; Graham and Scott, 2005). ASA is deacetylated to salicylic acid (SA). SA is only to a minor extent hydroxylated by cytochrome P450 enzymes. The main way of metabolism of SA is the conversion to different types of glucuronides as performed by several UDP-glucuronosyltransferases (UGTs, e.g., UGT1A6) (Kuehl et al., 2006). Pharmacogenetic investigations in relation to ASA are rare. A genome-wide association study detected the polymorphism rs7572857G > A in the gene CEP68, encoding for a centrosomal protein of 68 kDa in length, to be a risk factor for aspirin intolerant asthma (Kim et al., 2010a) (Table 3). Using in silico tools for docking experiments, a research group predicted that the single-nucleotide polymorphism (SNP) rs117122585 in the gene PTGS1 encoding COX-1 might have the potential to decrease the inhibitory potential of ASA on COX-1 with putative consequences for adverse effect and efficacy potential of ASA in these patients (Marjan et al., 2014).
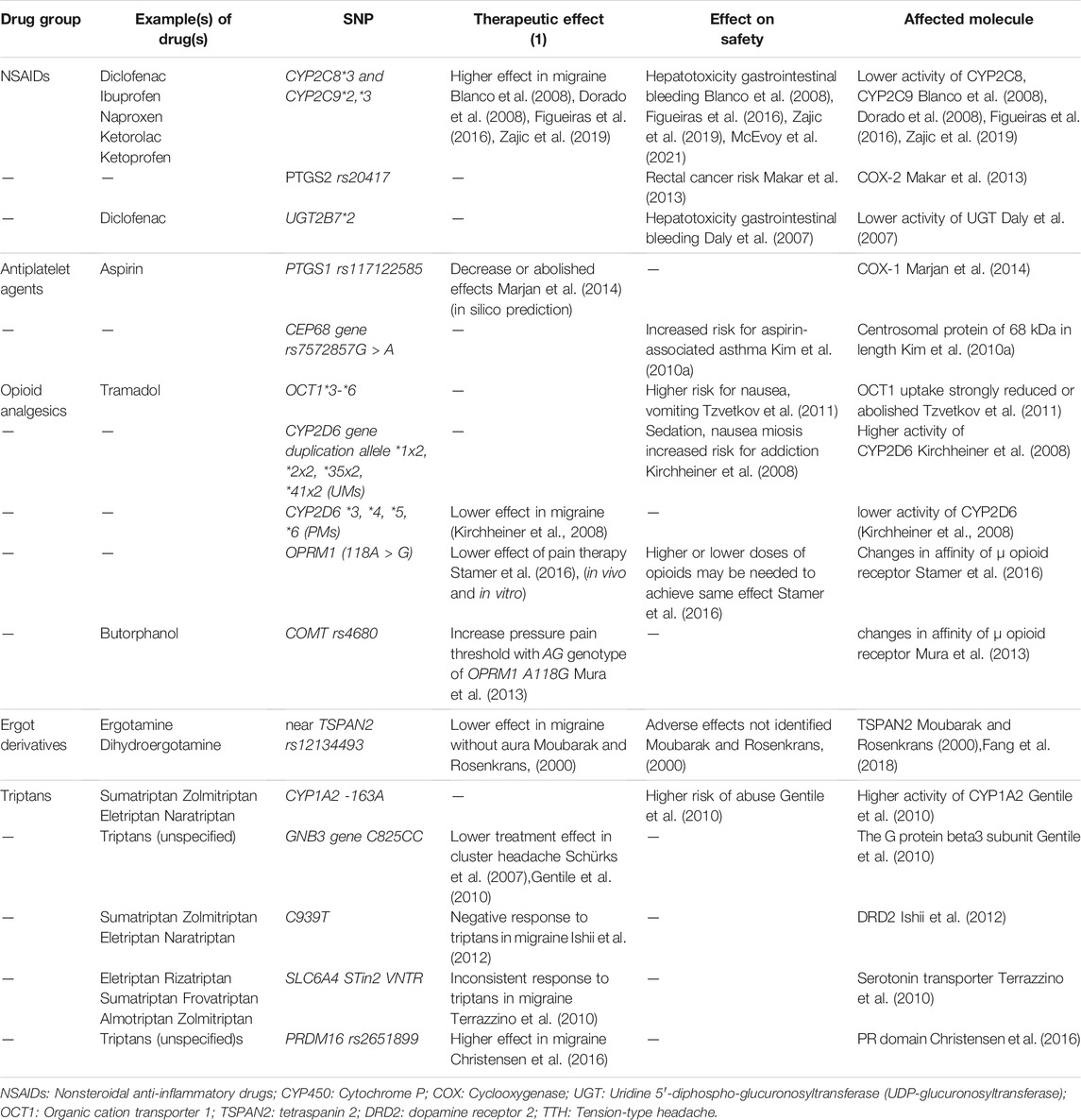
TABLE 3. Important pharmacogenetic markers in treatment of acute primary headaches.
Nonsteroidal Anti-Inflammatory Drugs
The analgesic and anti-inflammatory properties of NSAIDs lead to a wide use for the relief of acute migraine attacks and TTHs (Pavithra et al., 2020; Pardutz and Schoenen, 2010; National Clinical Guideline Centre (UK), 2012). The main mechanism of their action is the inhibition of the enzymes COX-1 and/or COX-2, which are responsible for the synthesis of prostaglandins that are involved in the inflammatory cascade and in hyperalgesia (Blanco et al., 2008; McEvoy et al., 2021). Adverse effects induced by nonselective NSAIDs are caused by the inhibition of constitutionally expressed COX-1 found in different tissues. The suppression of prostaglandin synthesis increases the risk for the development of upper gastrointestinal tract injuries and bleeding, renal fluid and natrium retention, and increased blood pressure (Pomes et al., 2019). NSAIDs are able to induce asthma due to a relative increase of leukotriene synthesis (Marjan et al., 2014). All NSAIDs are strongly metabolized in the liver and, thus, have a strong hepatotoxic potential (Table 1).
The metabolism of NSAIDs is realized in two stages. During phase one metabolism, NSAIDs are strongly metabolized by CYP2C8, CYP2C9, and CYP2C19 (Marjan et al., 2014). Phase two metabolism of NSAIDs is executed by different UDP-glucuronosyltransferases, such as the polymorphically expressed UGT2B7.
Genetic polymorphisms of the mentioned phase one genes, i.e., CYP2C8*3 and CYP2C9 2* and *3, are responsible for the reduced activity of the enzymes, which potentially lead to higher plasma levels of NSAIDs and, thus, stronger adverse effects of these drugs (Dorado et al., 2008; Figueiras et al., 2016; Zajic et al., 2019; Blanco et al., 2008). The mentioned genetic variants have been associated with an increased risk of adverse effects, including hepatotoxicity and gastrointestinal bleeding (Figueiras et al., 2016; Zajic et al., 2019; Blanco et al., 2008; McEvoy et al., 2021) (Table 3). Genetic polymorphisms in the genes coding for UDP-glucuronosyltransferases that are responsible for the conjugation of NSAID metabolites may also be associated with impaired clearance of NSAIDs. The polymorphism UGT2B7*2 is associated with reduced activity of the UDP-glucuronosyltransferase enzyme, which increases the risk of hepatotoxicity and damage to the upper gastrointestinal tract when using diclofenac (Daly et al., 2007). The polymorphism rs20417 of the PTGS2 gene encoding COX-2 has been associated with an increased risk of rectal cancer in case of chronic NSAID use in a population-based study of more than 3,000 colorectal cancer patients and healthy individuals in the USA (Makar et al., 2013).
Opioid Analgesics
Opioids are rarely used for acute migraine due to their significant and undesirable adverse effects and the availability of safer and more effective drugs (Orr et al., 2015; Gong et al., 2014). However, butorphanol, meperidine, morphine, hydromorphone, and tramadol have been mentioned as beneficial agents for acute migraine treatment. Tramadol and butorphanol are the most commonly used compounds in this drug group in association with the mentioned indication. Butorphanol is an agonist–antagonist of opioid receptors (an agonist of κ-receptors and an antagonist of μ-receptors). Tramadol is an agonist of opioid receptors and also suppresses the reuptake of norepinephrine and 5-hydroxytryptamine (5-HT) in the central nervous system, thus, promoting hyperpolarization of nerve cell membranes with inhibition of nerve impulse conduction and enhancement of the activity of the antinociceptive system (Owusu Obeng et al., 2017; Stamer et al., 2016) (Table 1). The complex mechanism of action of tramadol allows affecting several key pathogenic features of migraine at once. The increase of monoamines affects the trigeminovascular system, and the activation of opioid receptors suppresses pain and negative emotional perception of pain. Tramadol induces opioid typical adverse effects, such as addiction, fatigue, weakness, lethargy, paradoxical stimulation, and sleep disorders (Kirchheiner et al., 2008; Tzvetkov, 2017). In addition to the central effects, tramadol can affect the gastrointestinal tract, inducing nausea, dry mouth, and constipation, the genitourinary system (difficulty urinating), and the cardiovascular system (arrhythmias and orthostatic hypotension) (Gong et al., 2014).
Tramadol is metabolized in two phases in the liver. Initially, CYP2D6 and CYP3A4 catalyze its N - and O-demethylation, followed by UGT1A8- and UGT2B7-dependent glucuronidation in the second phase (Tzvetkov, 2017). Polymorphisms in drug-metabolizing enzymes have a significant impact on tramadol pharmacokinetics and pharmacodynamics. Carriers of CYP2D6 gene duplications (*1x2, *2x2, *35x2, and *41x2) belong to the group ultrarapid metabolizers (UMs) (Kirchheiner et al., 2008). The excessive concentration of the active metabolite O-desmethyltramadol in the plasma of UMs increases the risk of adverse effects with tramadol, such as sedation, nausea, miosis, and the development of addiction (Kirchheiner et al., 2008). On the contrary, carriers of combinations of the CYP2D6 alleles*3, *4, *5, and *6, causing a poor metabolizer (PM) phenotype, are characterized by an increased concentration of tramadol in plasma decreased efficacy (Kirchheiner et al., 2008) (Table 3).
The organic cation transporter 1 accomplishes the uptake of tramadol and o-desmethyltramadol into the hepatocytes (Tzvetkov et al., 2011). As shown in postoperative patients, polymorphisms in the encoding gene SLC22A1 [rs12208357 (*3, Arg61Cy), rs34130495 (*4, Gly401Ser)] greatly reduce the uptake and increase the risk of adverse effects (Tzvetkov et al., 2011). The polymorphisms rs34059508 (*5, Gly465Arg) and rs55918055 (*6, Cys88Arg) are associated with the complete absence of tramadol uptake by hepatocytes that further increase the risk of adverse events (Tzvetkov et al., 2011).
In the future, it may be of value to study the polymorphisms of OPRM1 encoding the μ opioid receptor. Studies in animals and humans have shown that the OPRM1 polymorphism 118A > G leads to interindividual differences in the sensitivity to pain and analgesic response to opioids and that carriers of the 118G allele may require higher opioid doses compared with carriers of the 118A allele (Stamer et al., 2016). As it was recently shown in a randomized placebo-controlled trial including 108 healthy individuals, the AA genotype of rs4680 or A_T_C_A/A_T_C_A (rs6269_rs4633_ rs4818_rs4680) diplotype of COMT gene, combined with the AG genotype of OPRM1 A118G, showed significantly increased pressure pain threshold from butorphanol (Mura et al., 2013; Ho et al., 2020). However, studies investigating these SNPs specifically in migraine patients are missing.
Ergot Derivatives
Ergot alkaloids are selective 5-HT1B, 5-HT1D, and possibly 5-HT1F receptor agonists (Diener and Limmroth, 2001). Ergotamine and dihydroergotamine have been on the market for a long time and are used to treat acute migraine and cluster headaches (Schiff, 2006) (Table 1). Ergotamine derivatives are substrates of CYP3A4 and should not be coadministered with strong CYP3A4 inhibitors (e.g., protease inhibitors, some macrolide antibiotics, and azole antifungals) due to the risk of acute ergot toxicity as shown in animal studies and humans (Moubarak and Rosenkrans, 2000; Srisuma et al., 2014). Pharmacogenetics has been poorly studied in association with these drugs. The presence of the tetraspanin 2 (TSPAN2) gene SNP rs12134493 tended to be associated with a lower effect of ergotamine in migraine without aura, as studied in 244 Danish individuals (Christensen et al., 2016). This SNP has also been detected as a risk SNP for migraine in the Chinese Han population (Fang et al., 2018) (Table 3).
Triptans
Triptans (e.g., sumatriptan, zolmitriptan, eletriptan, naratriptan, and rizatriptan) are used in acute migraine and cluster headaches. The main molecular targets of triptans are 5-HT1 receptors (Christensen et al., 2016; Ong and De Felice, 2018). Triptans induce cranial vasoconstriction (stimulation of 5-HT1B receptors), inhibition of the trigeminovascular system and neurovascular conflict, and the reduction of CGRP accumulation and release (stimulation of 5-HT1D receptors) (Ahn and Basbaum, 2005; Aggarwal et al., 2012) (Table 1). Additionally, triptans activate the antinociceptive system and stabilize trigeminal nucleus caudalis activity (Ahn and Basbaum, 2005). Triptans are contraindicated in patients with cardio- and cerebrovascular diseases, uncontrolled hypertension, and severe hepatic impairment and in patients with rare migraine variants such as hemiplegic migraine (Ahn and Basbaum, 2005).
Triptans are metabolized primarily by the monoamine oxidase A (MAO-A) system and by CYP1A2 and CYP3A4 (Aggarwal et al., 2012). In a study on 124 women, different MAO-A polymorphisms (leading to MAO-A-high or MAO-A-low activity) did not influence the efficacy or the risk of abuse of triptans to a significant extent (Gentile et al., 2010). At the same time, patients with the -163A allele polymorphism in CYP1A2 have been shown to have higher enzyme activity and a higher risk of abuse compared with patients carrying the -163C allele (Gentile et al., 2010). In a study including 231 Caucasian patients, Schürks et al. (2007) demonstrated that a polymorphism in the gene encoding the G protein beta3 subunit (GNB3 C825T) is significantly associated with triptan treatment outcome in cluster headache (Gentile et al., 2010) (Table 3). The authors described a better response to treatment in the GNB3 C825T heterozygous group compared with carriers of the C825C genotype (Schürks et al., 2007; Gentile et al., 2010). Interestingly, carriers of the C/C genotype at the polymorphic position C939T in the dopamine receptor 2 gene (DRD2) were more likely to have a negative response to triptan treatment in migraine as investigated in a clinical trial including 46 consistent and 14 inconsistent responders to triptans in Japan (Ishii et al., 2012). The STin2 VNTR polymorphism in the gene SLC6A4 encoding the serotonin transporter (SERT) was found to correlate with inconsistent response to triptans in migraine patients (Terrazzino et al., 2010). The rs2651899 polymorphism in the PRDM16 gene encoding the PR domain containing 16 proteins, a zinc finger transcription factor, appears to be associated with a better therapy efficacy of triptans in migraine, as shown in a Danish study including 1,806 patients, of which 1,386 reported an effect of triptans and 376 reported no effect (Christensen et al., 2016).
Antidepressants
According to the recommendations of the EHF, antidepressants can be used for the preventive treatment of migraine and TTH. Amitriptyline and nortriptyline are used to prevent TTH, mirtazapine is a second-line drug, and venlafaxine is a third-line drug (Steiner et al., 2019). Amitriptyline has the best evidence for use in migraine prevention (Sarchielli et al., 2012; Burch, 2019b). Nortriptyline is an alternative in patients who may not tolerate amitriptyline (Burch, 2019b). Amitriptyline is mainly metabolized by CYP2C19 to active metabolites, including nortriptyline, and by CYP2D6, leading to a less active 10-hydroxy-metabolite (Dean et al., 2012a; Hicks et al., 2013). Amitriptyline blocks the uptake of serotonin and norepinephrine and has furthermore strong affinities for histamine (H1), alpha-1 adrenergic, and muscarinic (M1) receptors, which account for its adverse effects, such as sedation, weight gain, blurred vision, dry mouth, and constipation (UpToDate (2016). Tricycli, 2016). The main routes of nortriptyline metabolism are 10-hydroxylation (major route) and N-demethylation (a minor route) (Alexanderson and Borga, 1973; Mellström et al., 1981). 10-Hydroxylation is mediated mainly by cytochrome P450 2D6 (CYP2D6), although in vitro studies have shown that CYP3A4 is also involved (Venkatakrishnan et al., 19991999). Nortriptyline appears to be less toxic than other TCAs. It is, furthermore, the least problematic of the TCAs in drug interactions, being only a weak CYP2D6 and CYP2C19 inhibitor (Shin et al., 2002).
CYP2C19*17 creates a new binding site for the transcription factor that leads to higher expression and, thus, the activity of CYP2C19 (Sim et al., 2006). A trial including 50 patients with depressive disorders has observed that CYP2C19 UMs have a higher risk for adverse effects, such as, e.g., neuromuscular, anticholinergic/gastrointestinal, and symptoms, due to the accumulation of nortriptyline (Steimer et al., 2005). The Clinical Pharmacogenetics Implementation Consortium (CPIC) suggests monitoring CYP2C19 UMs with amitriptyline treatment tighter or choosing antidepressants with no major CYP2C19 metabolic pathway as an option (Hicks et al., 2013). However, it should be kept in mind that the frequency of alleles varies between different ethnic groups (Strom et al., 2012). Polymorphic variants associated with slow metabolism of CYP2C19, i.e., CYP2C19*2, *3, and *4, lead to a decrease in the metabolism of TCAs (Goldstein et al., 1997; Aynacioglu et al., 1999). These polymorphisms have been associated with a higher likelihood of adverse effects with TCAs, including anticholinergic adverse effects, cardiotoxicity, and dizziness (Dean et al., 2012a).
CYP2D6 UMs have an increased metabolism of TCAs, with reduced TCA plasma concentrations. CYP2D6*4/*41, *5/*9, and *4/*10, which encode for intermediate metabolizers (IMs), have a slightly reduced TCA metabolism with increased plasma concentrations and an increased risk for adverse effects, such as anticholinergic adverse effects, cardiotoxicity, and dizziness (Hicks et al., 2013). CYP2D6 PMs carrying variant combinations of CYP2D6*3, *4, *5, and *6 (Dean et al., 2012a) have the highest risk for adverse effects (Steimer et al., 2005). It is worth remembering that the frequency distributions of alleles vary between different populations (Sistonen et al., 2007).
A study of 23 women with chronic persistent midfacial TTH showed that carriers of the “LL” genotype of the serotonin transporter gene-linked polymorphic region (HTTLPR) responded better to the therapy with amitriptyline than patients with “SS” or “LS” genotypes (Agius and Muscat, 2019). A small trial in 80 patients detected a link between the NOS3 gene Glu298Asp polymorphism, the production of NO, and the response of patients to TCAs when treated for migraine attacks. Migraine patients carrying the TT genotype produce less NO, which may lead to a better response to TCAs in comparison with carriers of GT and GG genotypes, which is reflected in a lower frequency of migraine attacks (Molana et al., 2014) (Table 4).
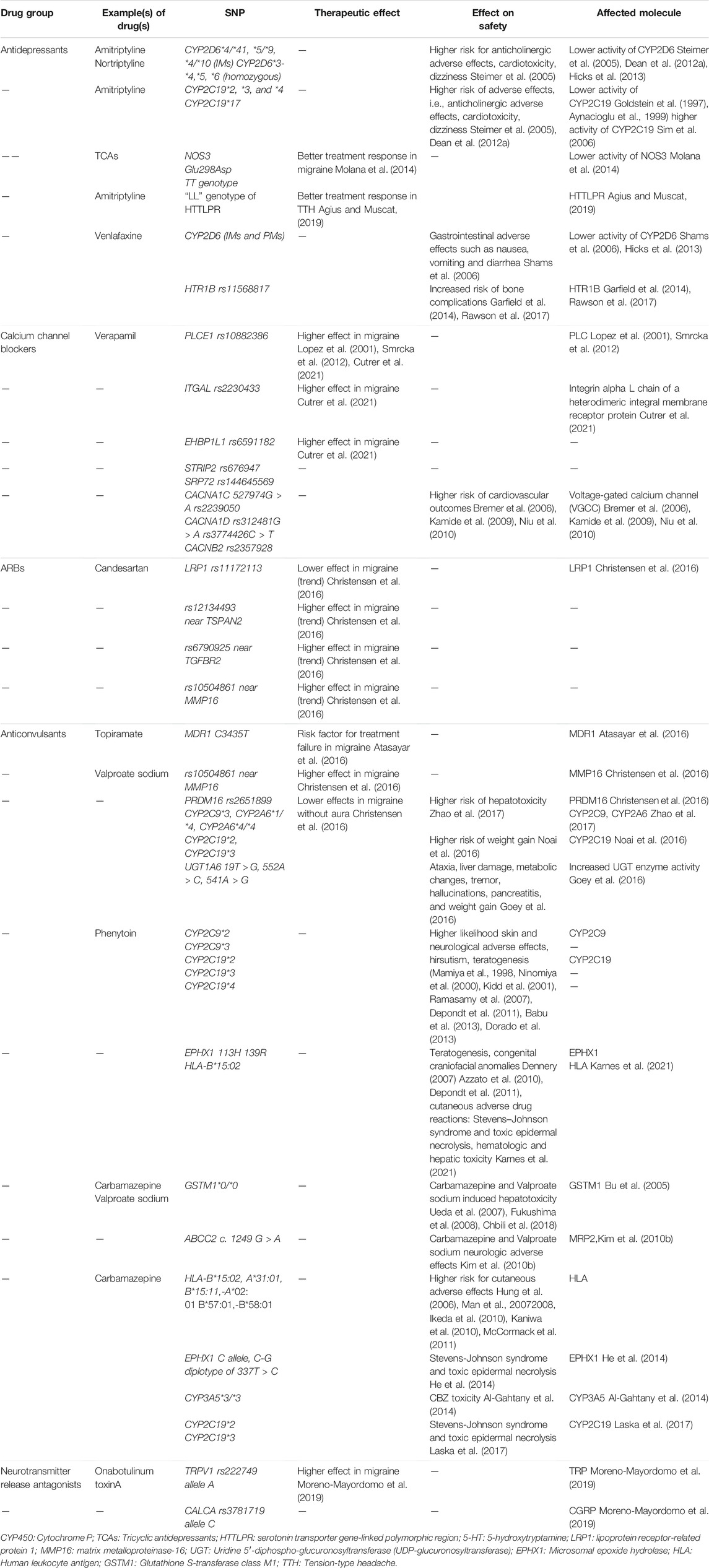
TABLE 4. Important pharmacokinetic markers in preventive treatment of primary headaches.
Mirtazapine, an atypical or tetracyclic antidepressant, is a noradrenergic and specific serotonergic antidepressant that increases central noradrenaline and serotonin by central presynaptic alpha‐2 antagonism; it also acts antagonistically on 5HT-2, 5HT‐3, and H1 receptors (Leung, 2021). Mirtazapine is metabolized in the liver by demethylation and then hydroxylation via cytochrome P450 enzymes (CYP1A2, CYP2D6, and CYP3A4) (Dahl et al., 1997). No studies were identified that have investigated genetic variants in relation to mirtazapine treatment outcome in headache disorders.
Venlafaxine belongs to the drug class of SNRIs. Venlafaxine is metabolized into the active metabolite, O-desmethylvenlafaxine, primarily by the CYP2D6 enzyme (Dean et al., 2015). Adverse effects occur more frequently in CYP2D6 PMs, such as vomiting and diarrhea, hypertension, tachycardia, and prolonged QTc interval (Johnson et al., 2006). Venlafaxine has been to a lesser extent investigated in pharmacogenetic studies than, for example, selective serotonin reuptake inhibitors, and the results of already performed investigations are, in some parts, contradictory or originate from single studies. However, it seems that several genetic polymorphisms are involved in its effectiveness and safety (Suwała et al., 2019). People with CYP2D6 *6/*4, *5/*4, or *6/*6 (PMs) are more likely to experience gastrointestinal adverse effects such as nausea, vomiting, and diarrhea (Shams et al., 2006). The HTR1B variant rs11568817 seems to be a promising marker of an increased risk of bone complications during VEN treatment (Garfield et al., 2014; Rawson et al., 2017) (Table 4).
Duloxetine belongs to the drug class of SNRIs. CYP1A2 and CYP2D6 contribute predominantly to the metabolism of duloxetine (Kapur et al., 2014). In a clinical study of 45 people, duloxetine was shown to be effective in preventing episodic migraine (Young et al., 2013) and effective in a study investigating comorbid migraine and depression, including 30 individuals (Volpe, 2008). The administration of duloxetine to CYP2D6 PMs, along with inhibition of CYP1A2, led to clinically significant higher duloxetine exposure, emphasizing that coadministration with a potent CYP1A2 inhibitor should be avoided (Knezevic et al., 2018). No studies were identified regarding genetic variants and their impact on duloxetine efficacy in headache disorders.
Calcium Channel Blockers
CCBs inhibit the inward movement of calcium by binding to the L-type “long-acting” voltage-gated calcium channels in the heart, vascular smooth muscle, and pancreas. Dihydropyridines belong to this group and act especially as peripheral vasodilators and are used for the treatment of hypertension, post-intracranial hemorrhage-associated vasospasm, and migraines (McKeever and Hamilton, 2021). The effect of CCBs in cluster headaches may be at least in part dependent on the reduction of calcium-dependent neurotransmission between climbing fibers and Purkinje cells in the cerebellum (Tso et al., 2021). CCBs are absorbed well orally, with a low bioavailability due to a high first-pass metabolism in the liver (Tso et al., 2021). Cinnarizine and flunarizine are metabolized mainly via CYP2D6 and CYP2B6 (Kariya et al., 1996). CYP450 3A4 and CYP1A2 are responsible for verapamil N-dealkylation, and the P450 2C subfamily (especially CYP2C8, CYP2C9) is responsible for verapamil O-dealkylation (Kroemer et al., 1993; Busse et al., 1995; Tracy et al., 1999).
Polymorphisms in several genes other than CYP genes have been recently associated with a decrease in the average duration of migraine when using verapamil, i.e., rs144645569 (SRP72), rs676947 (STRIP2), rs6591185 (EHBP1L1), and rs10882386 (PLCE1). In this study investigating the effect of migraine prophylaxis in 185 individuals using verapamil, the strongest decrease in the number of days with a headache after treatment was seen in carriers of the variant rs2230433 in the ITGAL gene, which encodes the integrin alpha L chain of a heterodimeric integral membrane receptor protein that is involved in costimulatory signaling and intercellular adhesion (Cutrer et al., 2021). Also, significantly associated with headache reduction was rs10882386 in PLCE1. PLCE1 encodes a phospholipase C enzyme that catalyzes the hydrolysis of 1‐phosphatidyl‐1D‐myo‐inositol 4,5‐bisphosphate (Lopez et al., 2001; Smrcka et al., 2012). Several studies have shown that polymorphisms in genes encoding different ion channels, for example, voltage-gated calcium channel CACNA1C (527974G > A and rs2239050), CACNA1D (rs312481G > A and rs3774426C > T), and CACNB2 (rs2357928) influence the risk of adverse cardiovascular outcomes especially with verapamil (Bremer et al., 2006; Kamide et al., 2009; Niu et al., 2010) (Table 4).
Angiotensin II Receptor Blockers and Angiotensin-Converting Enzyme Inhibitors
Angiotensin II receptor antagonists (or blockers, ARBs, candesartan) (Stovner et al., 2014; Sánchez-Rodríguez et al., 2021) and ACE inhibitors (lisinopril) can be used for the preventive treatment of migraine (Loder et al., 2012; Stovner et al., 2014; Steiner et al., 2019; Sánchez-Rodríguez et al., 2021). The main mechanism of action of ARBs is the blockade of angiotensin II type 1 (ATII) receptors, whereas the main mechanism of ACE inhibitors is the blockade of angiotensin I conversion to angiotensin II. ARBs and ACE inhibitors decrease angiotensin II-mediated vasoconstriction and aldosterone production, regulation of fluid and electrolyte balance, and regulation of morphological structure of vessels. The main area of their therapeutic use is the treatment of arterial hypertension and chronic heart failure (Tronvik et al., 2006; Do et al., 2014; Halker et al., 2016; Heidari et al., 2017). The mechanisms by which ARBs and ACE inhibitors act beneficially in migraine are not fully understood, but it is possible that their effectiveness is due to the blockade of type ATII receptors and decrease of the influence of angiotensin II in cerebral vessels, which reduces the tone of smooth muscles and increases their resistance to vasospastic stimuli; in addition, the decrease in aldosterone production under the action of ARBs may play a role (Tronvik et al., 2006). Serious adverse effects of ARBs occur infrequently; sometimes, there is slight dizziness, less often headache, as well as an increase in the frequency of respiratory infections and also includes dry cough for ACE inhibitors (Lopez et al., 2001; Cutrer et al., 2021). ARBs are metabolized in the liver, but the main part is excreted unchanged by the kidneys, whereas lisinopril is fully excreted unchanged by the kidneys.
In migraineurs, only nominal significant associations between a polymorphism in LRP1 (rs 11172113) encoding the low-density lipoprotein receptor-related protein 1 (lower efficacy), rs12134493 near the tetraspanin 2 gene TSPAN2, and rs6790925 near the transforming growth factor, beta receptor II gene TGFBR2 and rs10504861 near the matrix metalloproteinase-16 gene MMP16 (better efficacy) have been found for migraine patients treated with sartans (Christensen et al., 2016). There is no evidence that polymorphisms in the RAS system are important for the efficacy and safety of lisinopril or ARBs in migraineurs (Tronvik et al., 2008).
Anticonvulsants
Valproate sodium, topiramate, phenytoin, and carbamazepine (CBZ) are used to treat migraine (Christensen et al., 2016; Atasayar et al., 2016; Fricke-Galindo et al., 2018a). Topiramate is also efficacious in cluster headache and may have some effect in migraine with medication overuse (Diener et al., 2007; Silberstein et al., 2007; Diener et al., 2009; Steiner et al., 2019) (Table 2).
Valproic acid increases the level of gamma-aminobutyric acid (GABA) by inhibiting the GABA-transaminase, which is involved in the metabolism of the transmitter (Ghodke-Puranik et al., 2013). It also blocks voltage-gated sodium, potassium, and calcium channels (including those coded for by CACNA1C, CACNA1D, CACNA1N, and CACNA1F) and the gene family encoding voltage-gated sodium channels (SCN) (Johannessen and Johannessen, 2003; Van den Berg et al., 1993). Valproic acid is 50% glucuronidated and 40% β-oxidized in the mitochondria. It is to a minor extent metabolized by cytochrome P450 (CYP)-mediated oxidation (10%) (Ito et al., 1990; Argikar and Remmel, 2009; Tan et al., 2010). Carriers of the variants CYP2C9*3 and CYP2A6*4 showed increased levels of hepatotoxic metabolites compared with the wild type, as shown in 279 individuals from China (Zhao et al., 2017). Mutations in a DNA polymerase subunit gamma (POLG) gene are also related to increased incidence of serious liver adverse effects in patients under valproate therapy, as shown in a study including 17 individuals from the USA (Stewart et al., 2010). Japanese females carrying the variants CYP2C19*2, or CYP2C19*3, were more susceptible to valproate-induced weight gain (Noai et al., 2016). Carriers of UGT1A6 19T > G, 552A > C, and 541A > G alleles displayed increased UGT enzyme activity compared with wild-type carriers, whereas UGT1A6 552A > C carriers showed a longer elimination half-life and a lower clearance rate associated with VPA-related adverse drug reactions, such as ataxia, liver damage, metabolic changes, tremor, hallucinations, pancreatitis, and weight gain (Goey et al., 2016) (Table 4). There were no significant correlations between the treatment responses to valproic acid and MDR1, CYP2D6, and CYP2C19 gene polymorphisms, as shown in the study, including 251 migraine patients (230 female and 21 male subjects) with or without aura (Atasayar et al., 2016). Based on data from the Danish Headache Centre, the effectiveness of anticonvulsant treatment in all types of migraine in humans is increased in the case of polymorphism rs10504861 near MMP16, whereas in the case of PRDM16 variant rs2651899, the effectiveness of anticonvulsant treatment of migraine without aura is reduced as investigated in 365 migraine cases (Christensen et al., 2016).
The mechanism of action of CBZ is not well understood, but it has been suggested that it binds mainly to sodium channels and also interacts with calcium and potassium channels. CBZ is a positive allosteric modulator of GABA-A receptor (Iannaccone et al., 2021). CBZ is almost entirely metabolized in the liver by epoxidation and hydroxylation (Fricke-Galindo et al., 2018b). CBZ-10,11-epoxide is formed by CYP3A4, CYP3A5, and CYP2C8. This reactive metabolite is pharmacologically active and potentially toxic (Korinthenberg et al., 1994) due to its capability to form covalent protein adducts (Bu et al., 2005). CBZ-10,11-epoxide is further metabolized to the inactive molecule by the microsomal epoxide hydrolase (EPHX1) (Pearce et al., 2002). Both glutathione S-transferase class M1 (GSTM1) and class T1 (GSTT1) are involved in conjugation reactions of the main metabolite and also in the detoxification of toxic metabolites of CBZ (Bu et al., 2005). Findings in 129 Tunisian epileptic patients treated with CBZ suggest that the GSTM1 (-) allele may be considered as a risk factor for CBZ-induced hepatotoxicity (Chbili et al., 2018). Japanese researchers observed a link between the lack of GSTM1 and increased levels of hepatic enzymes in 192 patients treated with CBZ and in 149 patients treated with valproate sodium (Ueda et al., 2007; Fukushima et al., 2008). The polymorphism c. 1249 G > A in ABCC2 encoding for the transporter MRP2 has been linked with neurological adverse reactions in patients using CBZ and valproic acid (Kim et al., 2010b) (Table 4).
The EPHX1 gene polymorphism 337T > C has been associated with an increased risk for adverse effects such as Stevens–Johnson syndrome and toxic epidermal necrolysis in patients with epilepsy, putatively through an increase in the concentration of a CBZ 10,11-epoxide (He et al., 2014). CBZ toxicity has been furthermore more often observed in patients carrying CYP3A5*3/*3 (Al-Gahtany et al., 2014), CYP2C19*2, and CYP2C19*3 (Laska et al., 2017) (Table 4).
Genes encoding the human leukocyte antigens (HLAs) are organized as a complex on chromosome 6. They encode cell-surface proteins that regulate the actions of the immune system (Barquera et al., 2008). Certain HLA alleles (B*15:02, A*31:01, B*15:11, A*02:01, B*57:01, and B*58:01) have been associated with a higher risk for cutaneous adverse effects in people of different nationalities when using CBZ (Hung et al., 2006; Man et al., 20072008; Ikeda et al., 2010; Kaniwa et al., 2010; McCormack et al., 2011). The Clinical Pharmacogenetics Implementation Consortium recommends genotyping for HLA-B*15:02 and HLA-A*31:01 alleles (Phillips et al., 2018). This information is furthermore included in the CBZ label of FDA and the European Medicines Agency, i.e., recommending genetic testing for HLA gene polymorphisms (US Food and Drug Administration, 2007) (Table 4).
Phenytoin inhibits voltage-gated sodium channels (Yang et al., 2012). The drug has a hepatotoxic potential (FDA, 2020; Karnes et al., 2021). Phenytoin metabolism is almost completely hepatic. CYP2C9 is responsible for 90% of metabolism, and CYP2C19 is responsible for the remaining 10%. Studies in patients have shown that carriers of the variants CYP2C9*2, CYP2C9*3 and CYP2C19*2, CYP2C19*3, CYP2C19*4, show a higher likelihood for adverse effects with phenytoin, such as gum hyperplasia, hirsutism, skin and neurological symptoms, such as confusion, dysarthria, memory loss or deterioration, astasia, and dizziness (Mamiya et al., 1998; Ninomiya et al., 2000; Kidd et al., 2001; Ramasamy et al., 2007; Depondt et al., 2011; Babu et al., 2013; Dorado et al., 2013). EPHX1 produces reactive oxide intermediates, which causes the teratogenic phenytoin effect (Dennery, 2007; Depondt et al., 2011). The genetic variants 113H and 139R of EPHX1 have been associated with congenital craniofacial anomalies in newborns in connection to phenytoin treatment (Azzato et al., 2010). The HLA-B*15:02 allele has been associated with phenytoin-induced cutaneous adverse drug reactions, including Stevens–Johnson syndrome and toxic epidermal necrolysis (Table 4).
Topiramate modulates voltage-activated sodium channels and cation influx through α-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid and kainic acid receptor channels, potentiates GABAA receptor-mediated currents, and inhibits carbonic anhydrase isoenzymes (Zona et al., 1997; Poulsen et al., 2004; Gryder and Rogawski, 2003). Topiramate is rapidly and completely absorbed after oral administration (Fan et al., 2016). Protein binding is at a 3–4% low (Doose et al., 1996). Eighty-five percent of the dose is excreted unchanged in the urine (Garnett, 2000), and the remaining 15% is metabolized through hydrolysis, hydroxylation, and glucuronidation (Johannessen, 1997). Topiramate is exported out of the brain tissue by MDR1 (Wang-Tilz et al., 2006). According to a study performed in 251 patients at a headache outpatient clinic in Turkey, topiramate is more efficient against migraine in carriers of the MDR1 genotype 3435TT compared with carriers of the genotypes CC and CT. The ABCB1 polymorphism C3435T was also found to be a risk factor for topiramate treatment failure in migraine as studied by Atasayar et al. (2016) in a clinical trial including 251 individuals (Table 4). There was no significant relationship between treatment response to topiramate in migraine patients and either CYP2D6 or CYP2C19 polymorphisms (Atasayar et al., 2016).
Ditans, Gepants, and Anti-Calcitonin-Gene-Related Peptide Monoclonal Antibodies
In recent years, new classes of drugs have been approved for the treatment of migraine, whose mechanisms of action are associated with specific effects on the pathophysiology of migraine (Szkutnik-Fiedler, 2020). These include ditans, gepants, and anti-CGRP monoclonal antibodies (Negro and Martelletti, 2019; Szkutnik-Fiedler, 2020). Ditans (e.g., lasmiditan) selectively activate 5-HT1F receptors, which determines their effectiveness similar to triptans and leads to a decrease of CGRP release, with fewer adverse effects due to vasoconstriction, as ditans do not bind to 5-HT1B and 5-HT1D receptors (Stewart et al., 2010). Gepants (telcagepant, ubrogepant, rimegepant, and atogepant) act directly by blocking CGRP receptors and reduce vascular nociceptive transmission and trigeminal nociceptive activation (Garnett, 2000). Anti-CGRP monoclonal antibodies have a similar effect. Galcanezumab, fremanezumab, and eptinezumab bind CGRP directly with high affinity, whereas erenumab binds to the CGRP receptor and blocks its CGRP binding (Garnett, 2000). There are currently no studies on the pharmacogenetics of these drugs and no data available on gene polymorphisms that could affect their efficacy and safety (Johannessen, 1997). It can be hypothesized that various polymorphisms in the 5-HT1F receptor system and the relating signaling pathways may be associated with the efficacy of ditans. It is possible that polymorphisms in the CGRP system and its receptor are most closely associated with the efficacy and safety of gepants and anti-CGRP monoclonal antibodies (Johannessen, 1997). Further studies on the pharmacogenetics of ditans, gepants, and anti-CGRP monoclonal antibodies are needed to elucidate polymorphisms that are important for their efficacy and safety.
Corticosteroids
Blumenthal (1952) and Frohner (1953) were the first to demonstrate a clinical effect of corticosteroids in migraine. Corticosteroids reduce pain by inhibiting prostaglandin synthesis, which leads to inflammation, and by reducing vascular permeability that results in tissue edema (Watanabe and Bruera, 1994; Mensah-Nyagan et al., 2009). Exogenous administration of corticosteroids suppresses excessive stress and inflammatory response from the hypothalamic–pituitary axis (Chrousos and Gold, 1992). Steroid receptors are found in the central and peripheral nervous systems and are responsible for the growth, differentiation, development, and plasticity of neurons (Watanabe and Bruera, 1994). In particular, corticosteroids reduce spontaneous discharge in an injured nerve, which reduces neuropathic pain (Mensah-Nyagan et al., 2009). Corticosteroids suppress neurogenic inflammation (Mensah-Nyagan et al., 2009) and modulate neuroplasticity, thereby reducing pain (Mensah-Nyagan et al., 2009). In the literature, single-dose intravenous dexamethasone has been discussed as a treatment option for managing resistant, severe, or prolonged migraine attacks (Woldeamanuel et al., 2015). Corticosteroids are not recommended by EHF and AAN for migraine treatment (Loder et al., 2012). A suboccipital steroid injection can be used as a preventive treatment for episodic and chronic cluster headaches. Greater occipital nerve blockade is highly effective in reducing headache attacks and even aborting cluster bouts in cluster headache patients without requiring additional prophylactic treatment, which has been proven in experiments involving 51 and 60 patients (Gantenbein et al., 2012; Gönen et al., 2019). At present, no studies have been found investigating the pharmacogenetics of these drugs in an association of drug effectiveness in cluster headaches.
Benzodiazepines
The actions of benzodiazepines are due to the potentiation of the neural inhibition that is mediated by GABA. Practically all effects of the benzodiazepines result from their actions on the ionotropic GABA (A) receptors in the central nervous system. Benzodiazepines do not activate GABA (A) receptors directly, but they require GABA. The main effects of benzodiazepines are sedation, hypnosis, decreased anxiety, anterograde amnesia, centrally mediated muscle relaxation, and anticonvulsant activity (Möhler et al., 2002).
EHF, AHS, and AAN do not list the use of benzodiazepines in their guidelines for preventive or acute therapy of migraine, TTH, or cluster headache (Loder et al., 2012; Silberstein et al., 2012; Marmura et al., 2015; Robbins et al., 2016; Steiner et al., 2019). Benzodiazepines are sometimes used in clinical practice for the treatment of different headache types such as migraines, TTH, or medication overuse headache and are therefore mentioned here.
Diazepam is metabolized in the liver with only traces of the unchanged drug being excreted in the urine. The two major pathways of diazepam metabolism, the formation of N-desmethyldiazepam and temazepam, are catalyzed by different CYP isoforms (Inaba et al., 1988). The third potential metabolite, 4-hydroxydiazepam, seems to be less important. Studies with a series of CYP isoform-selective inhibitors and an inhibitory anti-CYP2C antibody indicate that temazepam formation is carried out mainly by CYP3A isoforms, whereas the formation of N-desmethyldiazepam is mediated by both CYP3A isoenzymes and CYP2C19 (Andersson et al., 1994; Kato and Yamazoe, 1994).
Benzodiazepines have adverse effects, including dependence, rebound anxiety, memory impairment, discontinuation syndrome, and others and should therefore be used with caution and only over a short time (Uzun et al., 2010). A clinical trial including 144 Japanese individuals tested a combined treatment of TTH with etizolam, a benzodiazepine derivative, and NSAIDs and showed that this treatment is effective in young patients (Hirata et al., 2007).
In a study including 30 Russian individuals, it was observed that CYP2C19*1/*2 and CYP2C19*2/*2 genotypes increase the risk of adverse effects when using diazepam, whereas CYP2C19*1/*17 and CYP2C19*17/*17 genotypes, on the contrary, reduce the risk of adverse effects, which was later confirmed in a second trial including 50 Russian subjects (Skryabin et al., 2020; Skryabin et al., 2021). Similar observations were made in other populations (Bertilsson et al., 1989; Wan et al., 1996; Qin et al., 1999; Dean et al., 2012b). In 3,705 elderly patients, CYP2C9*2 and CYP2C9*3 were shown to be associated with an increased fall risk (Ham et al., 2017). The effect of the polymorphism of CYP3A5 on the pharmacokinetics of benzodiazepines remains inconclusive, as some studies show a negligible effect on the pharmacokinetics of drugs (Kuehl et al., 2001; Shih and Huang, 2002; Park et al., 2006).
OnabotulinumtoxinA
OnabotulinumtoxinA has demonstrated high efficacy and is approved for the treatment of chronic migraine (Silberstein et al., 2012; Steiner et al., 2019). This drug is a toxin of Clostridium botulinum, which disrupts the release of neurotransmitters from the presynaptic membrane into the synaptic cleft (Affatato et al., 2021). Currently, its mechanisms of action in migraine are not fully understood. There is evidence that onabotulinumtoxinA disrupts the release of glutamate, substance P, and CGRP in the trigeminally innervated craniofacial–cervical region, which blocks key mechanisms of migraine attack pathophysiology (Szok et al., 2015; Burstein et al., 2020; Affatato et al., 2021). In the context of beneficial effects, specifically in chronic migraine, the ability to reduce central sensitization under the action of onabotulinumtoxinA has to be mentioned, which underlies the reduction in the frequency and intensity of migraine attacks (Szok et al., 2015; Burstein et al., 2020; Affatato et al., 2021).
There are currently no reliable data on the pharmacokinetics and metabolism of onabotulinumtoxinA due to its high neurotoxicity, but it is most likely that most of the toxin is cleaved by proteases, and products of proteolysis are used in normal metabolic pathways (Frampton and Silberstein, 2018). OnabotulinumtoxinA is determined in negligible concentrations in plasma and has low immunogenicity, but it has been shown that toxin-neutralizing antibodies can be synthesized after 12 weeks of its use (Frampton and Silberstein, 2018).
Two SNPs have been associated with onabotulinumtoxinA efficacy in chronic migraine. Rrs222749 located on the gene transient receptor potential cation channel subfamily v member 1 (TRPV1) occurred with a frequency of 12.5% in nonresponders and 4.17% in the group of responders and SNP rs3781719 of the gene calcitonin related polypeptide alpha (CALCA) where allele C represents 26.9% in responders and 40.9% in nonresponders (Moreno-Mayordomo et al., 2019) (Table 4). Further studies of genetic polymorphisms associated with the efficacy and safety of OnabotulinumtoxinA in the treatment of chronic migraine are needed.
Discussion
The review provides a comprehensive overview regarding the pathophysiology, therapy safety, and efficacy of three important primary headache disorders, i.e., TTH, migraine, and cluster headache. In this context, the review summarizes the current options regarding pharmacological treatment of acute and chronic forms of the mentioned headache types and, most importantly, sheds light on the current state of the art regarding the impact of pharmacogenetic variants on the safety and efficacy of compounds used in the acute and preventive treatment of migraine, TTH, or cluster headache.
Genetic polymorphisms of relevance identified in the area of headache disorders are foremost associated with a change in the risk for adverse effects of the therapeutics used. This includes several variants in genes that are responsible for phase I and phase II metabolism or transport of the therapeutics discussed. Important examples comprise CYP genes such as CYP2C8, CYP2C9 (CYP2C8*3, CYP2C9*2, and *3), variants in CYP2D6 (PM variants such as, e.g., *3 -*6 or gene duplications/multiplications), and in CYP2C19 (PM variants *2, *3, UM variant *17). Variants in these genes have been shown to modify the safety of compounds belonging to often used drugs classes NSAIDs (CYP2C8, CYP2C9), antiepileptics (CYP2C9, CY2C19, phenytoin), or antidepressants (CYP2D6, CYP2C19, TCAs) and to more seldomly used drug classes such as opioids (CYP2D6). Moreover, polymorphisms in genes encoding for enzymes involved in phase II metabolism, such as in UDP-glucanosyltransferases [e.g., UGT2B7*2 (NSAIDs)] and GSTM1 (GSTM1 *0/*0, CBZ, valproate sodium), as well as SNPs in drug transporters such as MDR1 (ABCB1, opioids, topiramate) organic cation transporter 1 (SLC22A1, opioids) or MRP2 (ABCC2, CBZ), have been associated with modulations of drug safety in headache disorders. SNPs in pharmacodynamic targets have been to a lesser extent linked with side drug adverse effects in headaches, but examples of such variants can be found in the COX 1 gene (PTGS1; aspirin) or in OPRM1 (opioids) or in voltage-gated calcium channels (verapamil). Only a few examples could be found, where genes with functions other than pharmacokinetics or -dynamics have been linked to drug safety in headache disorders. An important example displays variants in the HLA system that have been associated with partly severe adverse effects of phenytoin and CBZ. Another example comprises the polymorphically expressed gene CEP68 that has been associated with aspirin-induced asthma.
The number of studies investigating genetic variants in relation to the therapy success of headache therapeutics is much smaller. Those studies include only small sample sizes, which lead to overall much less well characterized genetic variants associated with therapeutic efficacy in headache disorders as compared with SNPs linked to drug safety in this therapeutic area. It also becomes obvious that studies investigating pharmacogenetics in relation to therapy efficacy have so far mainly concentrated on migraine, whereas efficacy-related pharmacogenetics studies investigating cluster headache or TTH patients have only very rarely been performed. Interestingly, variants associated with drug efficacy show a much more heterogeneous gene spectrum compared with polymorphically expressed genes that have been linked to drug safety. Genetic variants in genes such as SLC6A4 (SERT), DRD2 (dopamine receptor), PRDM16 or CYP1A2, and GNB3 have been associated with a modified therapy outcome with triptans in migraine and cluster headache, respectively. Of note, a polymorphic expression of PRDM16 has been, together with MMP16, also linked to modulated therapy success with anticonvulsants in migraine. Furthermore, genetic variants related to MMP16, TGFBR2, TSPAN2, and LMP1 have been linked to therapy outcome changes with sartans in migraine. In this context, it is noted that polymorphisms in genes including TGFBR2, TSPAN2, and PRDM16 are also associated with migraine risk (Gormley et al., 2016), underlining a potentially important role of these genes in migraine pathogenesis and therapy success in migraine. Likewise, MMP16 should be further investigated with regard to efficacy shifts due to the repeatedly observed influence on therapy effect with different compounds. Further pharmacogenetics studies with larger sample sizes are needed to confirm the described findings and observations. The knowledge regarding polymorphisms and their impact on therapy outcomes in headache disorders is very limited for opioids and TCAs. Likewise, pharmacogenetic markers for therapy efficacy in headache disorders when using ergot derivatives, beta-blockers, and novel therapy options such as ditans, anti-CGRP monoclonal antibodies, and gepants have not been studied enough to be able to draw conclusions on the usability of genetic variants for therapy response prediction in headache disorders.
Although a limitation of this review may be that the search was not performed following a systematic protocol such as PRISMA, the review is, to our knowledge, unique in the sense that it very comprehensively sheds light on both the safety and efficacy of acute and preventively used drugs of three important headache disorders taking established and novel knowledge on pharmacogenetic markers into consideration.
The main goal of precision medicine is to prescribe the most appropriate, effective, and safe treatment for the disease based on the individual characteristics of the patient (including genetic polymorphisms of enzymes significant for the pharmacodynamics and pharmacokinetics of drugs). A wide class of medications is used in the treatment of headaches, for both the relief of attacks and the prevention of chronic headaches, which have a wide range of adverse effects (Pomes et al., 2018), as presented in this review. Additionally, there is an increased risk of life-threatening drug-to-drug interactions when they are used in combination, especially in comorbid patients who are being treated for multiple diseases simultaneously, as summarized in Pomes et al. (2018). It can be concluded that there is currently not enough data available to be able to create a unified system and concept for the selection of headache drugs for a particular patient with headaches only based on his genetic profile (Cader, 2020). Although advances have been made regarding an understanding of genetic risk factors important for adverse effects of compounds used for migraine, TTH, or cluster headache, it becomes obvious that more pharmacogenetics studies are needed exploring the influence of genetic variants on therapy outcome in primary headache disorders. This is especially relevant for novel therapeutic options such as ditans, CGRP monoclonal antibodies, and gepants, for which studies regarding genetic variants and their impact on efficacy are currently missing. In this context, pharmacogenetic effect studies in migraine may also further explore polymorphically expressed genes that have been identified to influence both disease risk and therapy response to further understand the importance of these genes for individual disease risk and therapy adaptation.
Author Contributions
IB, AS, and IE wrote the review. VT, VC, and HS critically reviewed and adjusted the manuscript. JM conceptualized the review, took part in review writing, and adjusted the manuscript.
Funding
The paper is supported by a grant from the VR (2019–01066) to HS.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1https://www.clinicaltrialsarena.com/projects/aimovig-erenumab-treatment-episodic-migraine/
References
Affatato, O., Moulin, T. C., Pisanu, C., Babasieva, V. S., Russo, M., Aydinlar, E. I., et al. (2021). High Efficacy of onabotulinumtoxinA Treatment in Patients with Comorbid Migraine and Depression: a Meta-Analysis. J. Transl Med. 19 (1), 133. doi:10.1186/s12967-021-02801-w
Afridi, S. K., Shields, K. G., Bhola, R., and Goadsby, P. J. (2006). Greater Occipital Nerve Injection in Primary Headache Syndromes-Pprolonged Effects from a Single Injection. Pain 122 (1-2), 126–129. doi:10.1016/j.pain.2006.01.016
Aggarwal, M., Puri, V., and Puri, S. (2012). Serotonin and CGRP in Migraine. Ann. Neurosci. 19 (2), 88–94. doi:10.5214/ans.0972.7531.12190210
Agius, A. M., and Muscat, R. (2019). Chronic Tension-type Facial Pain-A Pilot Study on HTTLPR Genetic Polymorphisms. Rhinology Online 2 (2), 125–133. doi:10.4193/rhinol/19.036
Ahn, A. H., and Basbaum, A. I. (2005). Where Do Triptans Act in the Treatment of Migraine. Pain 115 (1-2), 1–4. doi:10.1016/j.pain.2005.03.008
Al-Eitan, L. N., Al-Dalala, I. M., Elshammari, A. K., Khreisat, W. H., Nimiri, A. F., Alnaamneh, A. H., et al. (2020). Genetic Association of Epilepsy and Anti-epileptic Drugs Treatment in Jordanian Patients. Pharmgenomics Pers Med. 13, 503–510. doi:10.2147/PGPM.S273125
Al-Gahtany, M., Karunakaran, G., and Munisamy, M. (2014). Pharmacogenetics of CYP3A5 on Carbamazepine Pharmacokinetics in Epileptic Patients Developing Toxicity. BMC Genomics 15. P2. doi:10.1186/1471-2164-15-S2-P2
Alemdar, M., Pekdemir, M., and Selekler, H. M. (2007). Single-dose Intravenous Tramadol for Acute Migraine Pain in Adults: a Single-Blind, Prospective, Randomized, Placebo-Controlled Clinical Trial. Clin. Ther. 29 (7), 1441–1447. doi:10.1016/j.clinthera.2007.07.017
Alexanderson, B., and Borga, O. (1973). Urinary Excretion of Nortriptyline and Five of its Metabolites in Man after Single and Multiple Oral Doses. Eur. J. Clin. Pharmacol. 5, 174–180. doi:10.1007/BF00564899
Andersson, T., Miners, J. O., Veronese, M. E., and Birkett, D. J. (1994). Diazepam Metabolism by Human Liver Microsomes Is Mediated by Both S-Mephenytoin Hydroxylase and CYP3A Isoforms. Br. J. Clin. Pharmacol. 38 (2), 131–137. doi:10.1111/j.1365-2125.1994.tb04336.x
Antonaci, F., Ghiotto, N., Wu, S., Pucci, E., and Costa, A. (2016). Recent Advances in Migraine Therapy. Springerplus 5, 637. doi:10.1186/s40064-016-2211-8
Argikar, U. A., and Remmel, R. P. (2009). Effect of Aging on Glucuronidation of Valproic Acid in Human Liver Microsomes and the Role of UDP-Glucuronosyltransferase UGT1A4, UGT1A8, and UGT1A10. Drug Metab. Dispos 37 (1), 229–236. doi:10.1124/dmd.108.022426
Ashina, S., Mitsikostas, D. D., Lee, M. J., Yamani, N., Wang, S. J., Messina, R., et al. (2021). Tension-type Headache. Nat. Rev. Dis. Primers 7 (1), 24. doi:10.1038/s41572-021-00257-2
Atasayar, G., Eryilmaz, I. E., Karli, N., Egeli, U., Zarifoglu, M., Cecener, G., et al. (2016). Association of MDR1, CYP2D6, and CYP2C19 Gene Polymorphisms with Prophylactic Migraine Treatment Response. J. Neurol. Sci. 366, 149–154. doi:10.1016/j.jns.2016.05.019
Aurora, S. K., Winner, P., Freeman, M. C., Spierings, E. L., Heiring, J. O., DeGryse, R. E., et al. (2011). OnabotulinumtoxinA for Treatment of Chronic Migraine: Pooled Analyses of the 56-week PREEMPT Clinical Program. Headache 51 (9), 1358–1373. doi:10.1111/j.1526-4610.2011.01990.x
Aynacioglu, A. S., Sachse, C., Bozkurt, A., Kortunay, S., Nacak, M., Schröder, T., et al. (1999). Low Frequency of Defective Alleles of Cytochrome P450 Enzymes 2C19 and 2D6 in the Turkish Population. Clin. Pharmacol. Ther. 66, 185–192. doi:10.1053/cp.1999.v66.100072001
Azzato, E. M., Chen, R. A., Wacholder, S., Chanock, S. J., Klebanoff, M. A., and Caporaso, N. E. (2010). Maternal EPHX1 Polymorphisms and Risk of Phenytoin-Induced Congenital Malformations. Pharmacogenet Genomics 20 (1), 58–63. doi:10.1097/FPC.0b013e328334b6a3
Babu, S. P., Ramesh, V., Samidorai, A., and Charles, N. S. (2013). Cytochrome P450 2C9 Gene Polymorphism in Phenytoin Induced Gingival Enlargement: A Case Report. J. Pharm. Bioallied Sci. 5, 237–239. doi:10.4103/0975-7406.116828
Barquera, R., Zúñiga, J., Hernández-Díaz, R., Acuña-Alonzo, V., Montoya-Gama, K., Moscoso, J., et al. (2008). HLA Class I and Class II Haplotypes in Admixed Families from Several Regions of Mexico. Mol. Immunol. 45 (4), 1171–1178. doi:10.1016/j.molimm.2007.07.042
Bendtsen, L. (2000). Central Sensitization in Tension-type Headache-Ppossible Pathophysiological Mechanisms. Cephalalgia 20 (5), 486–508. doi:10.1046/j.1468-2982.2000.00070.x
Bendtsen, L., Evers, S., Linde, M., Mitsikostas, D. D., Sandrini, G., and Schoenen, J. (2010). EFNS Guideline on the Treatment of Tension-type Headache - Report of an EFNS Task Force. Eur. J. Neurol. 17 (11), 1318–1325. doi:10.1111/j.1468-1331.2010.03070.x
Bendtsen, L., and Jensen, R. (2004). Mirtazapine Is Effective in the Prophylactic Treatment of Chronic Tension-type Headache. Neurology 62 (10), 1706–1711. doi:10.1212/01.wnl.0000127282.90920.8c
Bertilsson, L., Henthorn, T. K., Sanz, E., Tybring, G., Säwe, J., and Villén, T. (1989). Importance of Genetic Factors in the Regulation of Diazepam Metabolism: Relationship to S-Mephenytoin, but Not Debrisoquin, Hydroxylation Phenotype. Clin. Pharmacol. Ther. 45 (4), 348–355. doi:10.1038/clpt.1989.40
Binder, W. J., Brin, M. F., Blitzer, A., Schoenrock, L. D., and Pogoda, J. M. (2000). Botulinum Toxin Type A (BOTOX) for Treatment of Migraine Headaches: an Open-Label Study. Otolaryngol. Head Neck Surg. 123 (6), 669–676. doi:10.1067/mhn.2000.110960
Blanco, G., Martínez, C., Ladero, J. M., Garcia-Martin, E., Taxonera, C., Gamito, F. G., et al. (2008). Interaction of CYP2C8 and CYP2C9 Genotypes Modifies the Risk for Nonsteroidal Anti-inflammatory Drugs-Related Acute Gastrointestinal Bleeding. Pharmacogenet Genomics 18 (1), 37–43. doi:10.1097/FPC.0b013e3282f305a9
Borro, M., Guglielmetti, M., Simmaco, M., Martelletti, P., and Gentile, G. (2019). The Future of Pharmacogenetics in the Treatment of Migraine. Pharmacogenomics 20 (16), 1159–1173. doi:10.2217/pgs-2019-0069
Brandt, R. B., Doesborg, P. G. G., Haan, J., Ferrari, M. D., and Fronczek, R. (2020). Pharmacotherapy for Cluster Headache. CNS Drugs 34 (2), 171–184. doi:10.1007/s40263-019-00696-2
Bremer, T., Man, A., Kask, K., and Diamond, C. (2006). CACNA1C Polymorphisms Are Associated with the Efficacy of Calcium Channel Blockers in the Treatment of Hypertension. Pharmacogenomics 7 (3), 271–279. doi:10.2217/14622416.7.3.271
Broner, S. W., Bobker, S., and Klebanoff, L. (2017). Migraine in Women. Semin. Neurol. 37 (6), 601–610. doi:10.1055/s-0037-1607393
Bu, H. Z., Kang, P., Deese, A. J., Zhao, P., and Pool, W. F. (2005). Human In Vitro Glutathionyl and Protein Adducts of Carbamazepine-10,11-Epoxide, a Stable and Pharmacologically Active Metabolite of Carbamazepine. Drug Metab. Dispos 33 (12), 1920–1924. doi:10.1124/dmd.105.006866
Burch, R. (2019). Antidepressants for Preventive Treatment of Migraine. Curr. Treat. Options. Neurol. 21 (4), 18. doi:10.1007/s11940-019-0557-2
Burch, R. (2019). Migraine and Tension-type Headache: Diagnosis and Treatment. Med. Clin. North. Am. 103 (2), 215–233. doi:10.1016/j.mcna.2018.10.003
Burch, R. C., Buse, D. C., and Lipton, R. B. (2019). Migraine: Epidemiology, Burden, and Comorbidity. Neurol. Clin. 37 (4), 631–649. doi:10.1016/j.ncl.2019.06.001
Burstein, R., Blumenfeld, A. M., Silberstein, S. D., Manack Adams, A., and Brin, M. F. (2020). Mechanism of Action of OnabotulinumtoxinA in Chronic Migraine: A Narrative Review. Headache 60 (7), 1259–1272. doi:10.1111/head.13849
Burton, M. E., Shaw, L. M., Schentag, J. J., and Evans, W. E. (2006). Applied Pharmacokinetics & Pharmacodynamics Principles of Therapeutic Drug Monitoring. Baltimore: American Association of Colleges of Pharmacy.
Busse, D., Cosme, J., Beaune, P., Kroemer, H. K., and Eichelbaum, M. (1995). Cytochromes of the P450 2C Subfamily Are the Major Enzymes Involved in the O-Demethylation of Verapamil in Humans. Naunyn Schmiedebergs Arch. Pharmacol. 353 (1), 116–121. doi:10.1007/BF00168924
Cader, M. Z. (2020). The Genetics of Migraine and the Path to Precision Medicine. Prog. Brain Res. 255, 403–418. doi:10.1016/bs.pbr.2020.06.008
Capi, M., Gentile, G., Lionetto, L., Salerno, G., Cipolla, F., Curto, M., et al. (2018). Pharmacogenetic Considerations for Migraine Therapies. Expert Opin. Drug Metab. Toxicol. 14 (11), 1161–1167. doi:10.1080/17425255.2018.1541452
Chai, N. C., Peterlin, B. L., and Calhoun, A. H. (2014). Migraine and Estrogen. Curr. Opin. Neurol. 27 (3), 315–324. doi:10.1097/WCO.0000000000000091
Charles, A. (2018). The Pathophysiology of Migraine: Implications for Clinical Management. Lancet Neurol. 17 (2), 174–182. doi:10.1016/S1474-4422(17)30435-0
Chbili, C., Hassine, A., Fathallah, N., Nouira, M., Naija, S., Ben Ammou, S., et al. (2018). Glutathione S-Transferase M1 and T1 Polymorphisms and the Risk of Mild Hepatotoxicity Induced by Carbamazepine in a Tunisian Population Study. BMC Neurol. 18 (1), 24. doi:10.1186/s12883-018-1013-8
Christensen, A. F., Esserlind, A. L., Werge, T., Stefánsson, H., Stefánsson, K., and Olesen, J. (2016). The Influence of Genetic Constitution on Migraine Drug Responses. Cephalalgia 36 (7), 624–639. doi:10.1177/0333102415610874
Chrousos, G. P., and Gold, P. W. (1992). The Concepts of Stress and Stress System Disorders. Overview of Physical and Behavioral Homeostasis. JAMA 267, 1244–1252. doi:10.1001/jama.1992.03480090092034
Cohen, A. S., Burns, B., and Goadsby, P. J. (2009). High-flow Oxygen for Treatment of Cluster Headache: a Randomized Trial. JAMA 302 (22), 2451–2457. doi:10.1001/jama.2009.1855
Company ELa (2019). FDA Approves Emgality® (Galcanezumab-gnlm) as the First and Only Medication for the Treatment of Episodic Cluster Headache that Reduces the Frequency of Attacks. Available at: https://www.prnewswire.com/news-releases/fda-approves-emgality-galcanezumab-gnlm-as-the-first-and-only-medication-for-the-treatment-of-episodic-cluster-headache-that-reduces-the-frequency-of-attacks-300862172.html (Accessed 06 04, 2019).
Cutrer, F. M., Moyer, A. M., Atkinson, E. J., Wang, L., Tian, S., Wu, Y., et al. (2021). Genetic Variants Related to Successful Migraine Prophylaxis with Verapamil. Mol. Genet. Genomic Med. 9 (6), e1680. doi:10.1002/mgg3.1680
Dahl, M.-L., Voortman, G., Alm, C., Elwin, C.-E., Delbressine, L., Vos, R., et al. (1997). In Vitro and In Vivo Studies on the Disposition of Mirtazapine in Humans. Clin. Drug Invest. 13, 37–46. doi:10.2165/00044011-199713010-00005
Dahlöf, C., and Maassen Van Den Brink, A. (2012). Dihydroergotamine, Ergotamine, Methysergide and Sumatriptan - Basic Science in Relation to Migraine Treatment. Headache 52 (4), 707–714. doi:10.1111/j.1526-4610.2012.02124.x
Daly, A. K., Aithal, G. P., Leathart, J. B., Swainsbury, R. A., Dang, T. S., and Day, C. P. (2007). Genetic Susceptibility to Diclofenac-Induced Hepatotoxicity: Contribution of UGT2B7, CYP2C8, and ABCC2 Genotypes. Gastroenterology 132 (1), 272–281. doi:10.1053/j.gastro.2006.11.023
de Boer, I., van den Maagdenberg, A. M. J. M., and Terwindt, G. M. (2019). Advance in Genetics of Migraine. Curr. Opin. Neurolpmcid 32 (3), 413PMC6522206–421. doi:10.1097/WCO.0000000000000687
de Vries, T., Villalón, C. M., and MaassenVanDenBrink, A. (2020). Pharmacological Treatment of Migraine: CGRP and 5-HT beyond the Triptans. Pharmacol. Ther. 211, 107528. doi:10.1016/j.pharmthera.2020.107528
Dean, L. (2012a). “Amitriptyline Therapy and CYP2D6 and CYP2C19 Genotype,” in Medical Genetics Summaries [Internet]. Editors V. M. Pratt, S. A. Scott, M. Pirmohamed, B. Esquivel, M. S. Kane, B. L. Kattman, and A. J. Malheiro (Bethesda (MD): National Center for Biotechnology Information US). 2017 Mar 23.
Dean, L. (2012b). “Clobazam Therapy and CYP2C19 Genotype,” in Medical Genetics Summaries [Internet]. Editors V. M. Pratt, S. A. Scott, M. Pirmohamed, B. Esquivel, M. S. Kane, B. L. Kattman, and A. J. Malheiro (Bethesda (MD): National Center for Biotechnology Information US). 2019 Sep 23.
Dean, L. (2015). “Venlafaxine Therapy and CYP2D6 Genotype,” in Medical Genetics Summaries [Internet]. Editors VM Pratt, SA Scott, M Pirmohamed, B Esquivel, M. S. Kane, B. L. Kattman, and A. J. Malheiro (Bethesda (MD): National Center for Biotechnology Information US). [updated 2020 Jun 29]2012–. PMID: 28520361.
Deen, M., Correnti, E., Kamm, K., Kelderman, T., Papetti, L., Rubio-Beltrán, E., et al. (2017). Blocking CGRP in Migraine Patients - a Review of Pros and Cons. J. Headache Pain 18 (1), 96. doi:10.1186/s10194-017-0807-1
Dennery, P. A. (2007). Effects of Oxidative Stress on Embryonic Development. Birth Defects Res. C Embryo Today 81, 155–162. doi:10.1002/bdrc.20098
Depondt, C., Godard, P., Espel, R. S., Da Cruz, A. L., Lienard, P., and Pandolfo, M. (2011). A Candidate Gene Study of Antiepileptic Drug Tolerability and Efficacy Identifies an Association of CYP2C9 Variants with Phenytoin Toxicity. Eur. J. Neurol. 18 (9), 1159–1164. doi:10.1111/j.1468-1331.2011.03361.x
Derry, S., Wiffen, P. J., and Moore, R. A. (2017). Aspirin for Acute Treatment of Episodic Tension-type Headache in Adults. Cochrane Database Syst. Rev. 1 (1), CD011888. doi:10.1002/14651858.CD011888.pub2
Derry, S., Wiffen, P. J., Moore, R. A., and Bendtsen, L. (2015). Ibuprofen for Acute Treatment of Episodic Tension-type Headache in Adults. Cochrane Database Syst. Rev. 2015 (7), CD011474. doi:10.1002/14651858.CD011474.pub2
Dib, M., Massiou, H., Weber, M., Henry, P., Garcia-Acosta, S., Bousser, M. G., et al. (2002). Efficacy of Oral Ketoprofen in Acute Migraine: a Double-Blind Randomized Clinical Trial. Neurology 58 (11), 1660–1665. doi:10.1212/wnl.58.11.1660
Diener, H. C., Bussone, G., Van Oene, J. C., Lahaye, M., Schwalen, S., and Goadsby, P. J. (2007). Topiramate Reduces Headache Days in Chronic Migraine: a Randomized, Double-Blind, Placebo-Controlled Study. Cephalalgia 27, 814–823. doi:10.1111/j.1468-2982.2007.01326.x
Diener, H. C., Dodick, D., Evers, S., Holle, D., Jensen, R. H., Lipton, R. B., et al. (2019). Pathophysiology, Prevention, and Treatment of Medication Overuse Headache. Lancet Neurol. 18 (9), 891–902. doi:10.1016/S1474-4422(19)30146-2
Diener, H. C., Dodick, D. W., Aurora, S. K., Turkel, C. C., DeGryse, R. E., Lipton, R. B., et al. (2010). OnabotulinumtoxinA for Treatment of Chronic Migraine: Results from the Double-Blind, Randomized, Placebo-Controlled Phase of the PREEMPT 2 Trial. Cephalalgia 30 (7), 804–814. doi:10.1177/0333102410364677
Diener, H. C., Dodick, D. W., Goadsby, P. J., Bigal, M. E., Bussone, G., Silberstein, S. D., et al. (2009). Utility of Topiramate for the Treatment of Patients with Chronic Migraine in the Presence or Absence of Acute Medication Overuse. Cephalalgia 29 (10), 1021–1027. doi:10.1111/j.1468-2982.2009.01859.x
Diener, H. C. (1999). Efficacy and Safety of Intravenous Acetylsalicylic Acid Lysinate Compared to Subcutaneous Sumatriptan and Parenteral Placebo in the Acute Treatment of Migraine. A Double-Blind, Double-Dummy, Randomized, Multicenter, Parallel Group Study. The ASASUMAMIG Study Group. Cephalalgia 19 (6), 581–542. doi:10.1046/j.1468-2982.1999.019006581.x
Diener, H. C., and Limmroth, V. (2001). Advances in Pharmacological Treatment of Migraine. Expert Opin. Investig. Drugs 10 (10), 1831–1845. doi:10.1517/13543784.10.10.1831
Digre, K. B. (2019). What's New in the Treatment of Migraine J. Neuroophthalmol 39 (3), 352–359. doi:10.1097/WNO.0000000000000837
Do, A. N., Irvin, M. R., Lynch, A. I., Claas, S. A., Boerwinkle, E., Davis, B. R., et al. (2014). The Effects of Angiotensinogen Gene Polymorphisms on Cardiovascular Disease Outcomes during Antihypertensive Treatment in the GenHAT Study. Front. Pharmacol. 5, 210. doi:10.3389/fphar.2014.00210
Dodick, D. W. (2018). A Phase-by-phase Review of Migraine Pathophysiology. Headache 58 (Suppl. 1), 4–16. doi:10.1111/head.13300
Doose, D. R., Walker, S. A., Gisclon, L. G., and Nayak, R. K. (1996). Single-dose Pharmacokinetics and Effect of Food on the Bioavailability of Topiramate, a Novel Antiepileptic Drug. J. Clin. Pharmacol. 36 (10), 884–891. doi:10.1002/j.1552-4604.1996.tb04754.x
Dorado, P., Cavaco, I., Cáceres, M. C., Piedade, R., Ribeiro, V., and Llerena, A. (2008). Relationship between CYP2C8 Genotypes and Diclofenac 5-hydroxylation in Healthy Spanish Volunteers. Eur. J. Clin. Pharmacol. 64 (10), 967–970. doi:10.1007/s00228-008-0508-4
Dorado, P., López-Torres, E., Peñas-Lledó, E. M., Martínez-Antón, J., and Llerena, A. (2013). Neurological Toxicity after Phenytoin Infusion in a Pediatric Patient with Epilepsy: Influence of CYP2C9, CYP2C19 and ABCB1 Genetic Polymorphisms. Pharmacogenomics J. 13 (4), 359–361. doi:10.1038/tpj.2012.19
Erdemoglu, A. K., and Varlibas, A. (2007). The Long-Term Efficacy and Safety of Botulinum Toxin in Refractory Chronic Tension-type Headache. J. Headache Pain 8 (5), 294–300. doi:10.1007/s10194-007-0414-7
Faedda, N., Cerutti, R., Verdecchia, P., Migliorini, D., Arruda, M., and Guidetti, V. (2016). Behavioral Management of Headache in Children and Adolescents. J. Headache Pain 17 (1), 80. doi:10.1186/s10194-016-0671-4
Fan, H. C., Lee, H. S., Chang, K. P., Lee, Y. Y., Lai, H. C., Hung, P. L., et al. (2016). The Impact of Anti-epileptic Drugs on Growth and Bone Metabolism. Int. J. Mol. Sci. 17 (8), 1242. doi:10.3390/ijms17081242
Fang, J., Yuan, X., An, X., Qu, H., Wang, C., Hong, G., et al. (2018). Involvement of the Tetraspanin 2 (TSPAN2) Gene in Migraine: A Case-Control Study in Han Chinese. Front. Neurol. 9, 714. doi:10.3389/fneur.2018.00714
Farinelli, I., and Martelletti, P. (2007). Aspirin and Tension-type Headache. J. Headache Pain 8 (1), 49–55. doi:10.1007/s10194-006-0357-4
Ferrari, M. D., Klever, R. R., Terwindt, G. M., Ayata, C., and van den Maagdenberg, A. M. (2015). Migraine Pathophysiology: Lessons from Mouse Models and Human Genetics. Lancet Neurol. 14 (1), 65–80. doi:10.1016/S1474-4422(14)70220-0
Figueiras, A., Estany-Gestal, A., Aguirre, C., Ruiz, B., Vidal, X., Carvajal, A., et al. (2016). CYP2C9 Variants as a Risk Modifier of NSAID-Related Gastrointestinal Bleeding: a Case-Control Study. Pharmacogenet Genomics 26 (2), 66–73. doi:10.1097/FPC.0000000000000186
Fogan, L. (1985). Treatment of Cluster Headache. A Double-Blind Comparison of Oxygen V Air Inhalation. Arch. Neurol. 42 (4), 362–363. doi:10.1001/archneur.1985.04060040072015
Frampton, J. E., and Silberstein, S. (2018). OnabotulinumtoxinA: A Review in the Prevention of Chronic Migraine. Drugs 78 (5), 589–600. doi:10.1007/s40265-018-0894-6
Francis, G. J., Becker, W. J., and Pringsheim, T. M. (2010). Acute and Preventive Pharmacologic Treatment of Cluster Headache. Neurology 75 (5), 463–473. doi:10.1212/WNL.0b013e3181eb58c8
Fraser, C. L., Hepschke, J. L., Jenkins, B., and Prasad, S. (2019). Migraine Aura: Pathophysiology, Mimics, and Treatment Options. Semin. Neurol. 39 (6), 739–748. doi:10.1055/s-0039-1700525
Fricke-Galindo, I., Jung-Cook, H., LLerena, A., and López-López, M. (2018a). Pharmacogenetics of Adverse Reactions to Antiepileptic Drugs. Neurologia 33 (3), 165–176. English, Spanish. doi:10.1016/j.nrl.2015.03.005
Fricke-Galindo, I., LLerena, A., Jung-Cook, H., and López-López, M. (2018b). Carbamazepine Adverse Drug Reactions. Expert Rev. Clin. Pharmacol. 11 (7), 705–718. doi:10.1080/17512433.2018.1486707
Frohner, R. N. (1953). Cortisone in Migraine and Histamine Headaches. Rocky Mt Med. J. 50 (11), 882.
Fukushima, Y., Seo, T., Hashimoto, N., Higa, Y., Ishitsu, T., and Nakagawa, K. (2008). Glutathione-S-transferase (GST) M1 Null Genotype and Combined GSTM1 and GSTT1 Null Genotypes Are Risk Factors for Increased Serum Gamma-Glutamyltransferase in Valproic Acid-Treated Patients. Clin. Chim. Acta 389 (1-2), 98–102. doi:10.1016/j.cca.2007.11.035
Fumagalli, C., Maurizi, N., Marchionni, N., and Fornasari, D. (2020). β-Blockers: Their New Life from Hypertension to Cancer and Migraine. Pharmacol. Res. 151, 104587. doi:10.1016/j.phrs.2019.104587
Gallagher, R. M., Mueller, L. L., and Freitag, F. G. (2002). Divalproex Sodium in the Treatment of Migraine and Cluster Headaches. J. Am. Osteopath Assoc. 102 (2), 92–94. PMID: 11866398.
Gantenbein, A. R., Lutz, N. J., Riederer, F., and Sándor, P. S. (2012). Efficacy and Safety of 121 Injections of the Greater Occipital Nerve in Episodic and Chronic Cluster Headache. Cephalalgia 32 (8), 630–634. doi:10.1177/0333102412443335
Garfield, L. D., Müller, D. J., Kennedy, J. L., Mulsant, B. H., Reynolds, C. F., Teitelbaum, S. L., et al. (2014). Genetic Variation in the Serotonin Transporter and HTR1B Receptor Predicts Reduced Bone Formation during Serotonin Reuptake Inhibitor Treatment in Older Adults. World J. Biol. Psychiatry 15 (5), 404–410. doi:10.3109/15622975.2013.832380
Garnett, W. R. (2000). Clinical Pharmacology of Topiramate: a Review. Epilepsia 41 (S1), 61–65. doi:10.1111/j.1528-1157.2000.tb02174.x
Gaul, C., Roguski, J., Dresler, T., Abbas, H., Totzeck, A., Görlinger, K., et al. (2017). Efficacy and Safety of a Single Occipital Nerve Blockade in Episodic and Chronic Cluster Headache: a Prospective Observational Study. Cephalalgia 37 (9), 873–880. doi:10.1177/0333102416654886
Gentile, G., Borro, M., Lala, N., Missori, S., Simmaco, M., and Martelletti, P. (2010). Genetic Polymorphisms Related to Efficacy and Overuse of Triptans in Chronic Migraine. J. Headache Pain 11 (5), 431–435. doi:10.1007/s10194-010-0241-0
Ghadiri-Sani, M., and Silver, N. (2016). Headache (Chronic Tension-type). BMJ Clin. Evid. 2016, 1205.
Ghodke-Puranik, Y., Thorn, C. F., Lamba, J. K., Leeder, J. S., Song, W., Birnbaum, A. K., et al. (2013). Valproic Acid Pathway: Pharmacokinetics and Pharmacodynamics. Pharmacogenet Genomics 23 (4), 236–241. doi:10.1097/FPC.0b013e32835ea0b2
Gildir, S., Tüzün, E. H., Eroğlu, G., and Eker, L. (2019). A Randomized Trial of Trigger point Dry Needling versus Sham Needling for Chronic Tension-type Headache. Medicine (Baltimore) 98 (8), e14520. doi:10.1097/MD.0000000000014520
Giuliano, C., Smalligan, R. D., Mitchon, G., and Chua, M. (2012). Role of Dexamethasone in the Prevention of Migraine Recurrence in the Acute Care Setting: A Review. Postgrad. Med. 124, 110–115. doi:10.3810/pgm.2012.05.2554
GBD 2016 Headache Collaborators (2018). Global, Regional, and National burden of Migraine and Tension-type Headache, 1990-2016: a Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 17(11), 954–976. doi:10.1016/S1474-4422(18)30322-3
Goadsby, P. J., Holland, P. R., Martins-Oliveira, M., Hoffmann, J., Schankin, C., and Akerman, S. (2017). Pathophysiology of Migraine: A Disorder of Sensory Processing. Physiol. Rev. 97 (2), 553–622. doi:10.1152/physrev.00034.2015
Goey, A. K., Sissung, T. M., Peer, C. J., and Figg, W. D. (2016). Pharmacogenomics and Histone Deacetylase Inhibitors. Pharmacogenomics 17 (16), 1807–1815. doi:10.2217/pgs-2016-0113
Goldstein, J. A., Ishizaki, T., Chiba, K., de Morais, S. M., Bell, D., Krahn, P. M., et al. (1997). Frequencies of the Defective CYP2C19 Alleles Responsible for the Mephenytoin Poor Metabolizer Phenotype in Various Oriental, Caucasian, Saudi Arabian and American Black Populations. Pharmacogenetics 7, 59–64. doi:10.1097/00008571-199702000-00008
Gönen, M., Balgetir, F., Aytaç, E., Taşcı, İ., Demir, C. F., and Müngen, B. (2019). Suboccipital Steroid Injection Alone as a Preventive Treatment for Cluster Headache. J. Clin. Neurosci. 68, 140–145. doi:10.1016/j.jocn.2019.07.009
Gong, L., Stamer, U. M., Tzvetkov, M. V., Altman, R. B., and Klein, T. E. (2014). PharmGKB Summary: Tramadol Pathway. Pharmacogenet Genomics 24 (7), 374–380. doi:10.1097/FPC.0000000000000057
Gormley, P., Anttila, V., Winsvold, B. S., Palta, P., Esko, T., Pers, T. H., et al. (2016). Meta-analysis of 375,000 Individuals Identifies 38 Susceptibility Loci for Migraine. Nat. Genet. 48 (8), 856–866. doi:10.1038/ng.3598
Graham, G. G., and Scott, K. F. (2005). Mechanism of Action of Paracetamol. Am. J. Ther. 12 (1), 46–55. doi:10.1097/00045391-200501000-00008
Gryder, D. S., and Rogawski, M. A. (2003). Selective Antagonism of GluR5 Kainate-Receptor-Mediated Synaptic Currents by Topiramate in Rat Basolateral Amygdala Neurons. J. Neurosci. 23 (18), 7069–7074. doi:10.1523/jneurosci.23-18-07069.2003
Haanes, K. A., and Edvinsson, L. (2019). Pathophysiological Mechanisms in Migraine and the Identification of New Therapeutic Targets. CNS Drugs 33 (6), 525–537. doi:10.1007/s40263-019-00630-6
Hainer, B. L., and Matheson, E. M. (2013). Approach to Acute Headache in Adults. Am. Fam. Physician 87 (10), 682–687.
Halker, R. B., Starling, A. J., Vargas, B. B., and Schwedt, T. J. (2016). ACE and ARB Agents in the Prophylactic Therapy of Migraine-How Effective Are They. Curr. Treat. Options. Neurol. 18 (4), 15. doi:10.1007/s11940-016-0397-2
Ham, A. C., Ziere, G., Broer, L., Swart, K. M., Enneman, A. W., van Dijk, S. C., et al. (2017). CYP2C9 Genotypes Modify Benzodiazepine-Related Fall Risk: Original Results from Three Studies with Meta-Analysis. J. Am. Med. Dir. Assoc. 18 (1), 88–e15. doi:10.1016/j.jamda.2016.09.02110.1016/j.jamda.2016.09.021
He, X. J., Jian, L. Y., He, X. L., Tang, M., Wu, Y., Xu, Y. Y., et al. (2014). Association of ABCB1, CYP3A4, EPHX1, FAS, SCN1A, MICA, and BAG6 Polymorphisms with the Risk of Carbamazepine-Induced Stevens-Johnson Syndrome/toxic Epidermal Necrolysis in Chinese Han Patients with Epilepsy. Epilepsia 55 (8), 1301–1306. doi:10.1111/epi.12655
Heidari, F., Vasudevan, R., Mohd Ali, S. Z., Ismail, P., and Arkani, M. (2017). RAS Genetic Variants in Interaction with ACE Inhibitors Drugs Influences Essential Hypertension Control. Arch. Med. Res. 48 (1), 88–95. doi:10.1016/j.arcmed.2017.03.003
Herd, C. P., Tomlinson, C. L., Rick, C., Scotton, W. J., Edwards, J., Ives, N., et al. (2018). Botulinum Toxins for the Prevention of Migraine in Adults. Cochrane Database Syst. Rev. 6 (6), CD011616. doi:10.1002/14651858.CD011616.pub2
Hering, R., and Kuritzky, A. (1989). Sodium Valproate in the Treatment of Cluster Headache: an Open Clinical Trial. Cephalalgia 9 (3), 195–198. doi:10.1046/j.1468-2982.1989.0903195.x
Hicks, J. K., Swen, J. J., Thorn, C. F., Sangkuhl, K., Kharasch, E. D., Ellingrod, V. L., et al. (2013). Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Tricyclic Antidepressants. Clin. Pharmacol. Ther. 93 (5), 402–408. doi:10.1038/clpt.2013.2
Hinson, J. A., Roberts, D. W., and James, L. P. (2010). Mechanisms of Acetaminophen-Induced Liver Necrosis. Handb Exp. Pharmacol. 196, 369–405. doi:10.1007/978-3-642-00663-0_12
Hirata, K., Tatsumoto, M., Araki, N., Takeshima, T., Igarashi, H., Shibata, K., et al. (2007). Multi-center Randomized Control Trial of Etizolam Plus NSAID Combination for Tension-type Headache. Intern. Med. 46 (8), 467–472. doi:10.2169/internalmedicine.46.6226
Ho, K. W. D., Wallace, M. R., Staud, R., and Fillingim, R. B. (2020). OPRM1, OPRK1, and COMT Genetic Polymorphisms Associated with Opioid Effects on Experimental Pain: a Randomized, Double-Blind, Placebo-Controlled Study. Pharmacogenomics J. 20 (3), 471–481. doi:10.1038/s41397-019-0131-z
Ho, T. W., Ferrari, M. D., Dodick, D. W., Galet, V., Kost, J., Fan, X., et al. (2008). Efficacy and Tolerability of MK-0974 (Telcagepant), a New Oral Antagonist of Calcitonin Gene-Related Peptide Receptor, Compared with Zolmitriptan for Acute Migraine: a Randomised, Placebo-Controlled, Parallel-Treatment Trial. Lancet 372 (9656), 2115–2123. doi:10.1016/S0140-6736(08)61626-8
Hoffert, M. J., Couch, J. R., Diamond, S., Elkind, A. H., Goldstein, J., Kohlerman, N. J., et al. (1995). Transnasal Butorphanol in the Treatment of Acute Migraine. Headache 35 (2), 65–69. doi:10.1111/j.1526-4610.1995.hed3502065.x
Hoffmann, J., and May, A. (2018). Diagnosis, Pathophysiology, and Management of Cluster Headache. Lancet Neurol. 17 (1), 75–83. doi:10.1016/S1474-4422(17)30405-2
Hung, S. I., Chung, W. H., Jee, S. H., Chen, W. C., Chang, Y. T., Lee, W. R., et al. (2006). Genetic Susceptibility to Carbamazepine-Induced Cutaneous Adverse Drug Reactions. Pharmacogenet Genomics 16 (4), 297–306. doi:10.1097/01.fpc.0000199500.46842.4a
Iannaccone, T., Sellitto, C., Manzo, V., Colucci, F., Giudice, V., Stefanelli, B., et al. (2021). Pharmacogenetics of Carbamazepine and Valproate: Focus on Polymorphisms of Drug Metabolizing Enzymes and Transporters. Pharmaceuticals (Basel) 14 (3), 204. doi:10.3390/ph14030204
Ikeda, H., Takahashi, Y., Yamazaki, E., Fujiwara, T., Kaniwa, N., Saito, Y., et al. (2010). HLA Class I Markers in Japanese Patients with Carbamazepine-Induced Cutaneous Adverse Reactions. Epilepsia 51 (2), 297–300. doi:10.1111/j.1528-1167.2009.02269.x
Inaba, T., Tait, A., Nakano, M., Mahon, W. A., and Kalow, W. (1988). Metabolism of Diazepam In Vitro by Human Liver. Independent Variability of N-Demethylation and C3-Hydroxylation. Drug Metab. Dispos 16 (4), 605–608.
Ishii, M., Sakairi, Y., Hara, H., Imagawa, A., Shimizu, S., Takahashi, J., et al. (2012). Negative Predictors of Clinical Response to Triptans in Patients with Migraine. Neurol. Sci. 33 (2), 453–461. doi:10.1007/s10072-011-0716-z
Ito, M., Ikeda, Y., Arnez, J. G., Finocchiaro, G., and Tanaka, K. (1990). The Enzymatic Basis for the Metabolism and Inhibitory Effects of Valproic Acid: Dehydrogenation of Valproyl-CoA by 2-Methyl-Branched-Chain Acyl-CoA Dehydrogenase. Biochim. Biophys. Acta 1034 (2), 213–218. doi:10.1016/0304-4165(90)90079-c
Iyengar, S., Johnson, K. W., Ossipov, M. H., and Aurora, S. K. (2019). CGRP and the Trigeminal System in Migraine. Headache 59 (5), 659–681. doi:10.1111/head.13529
Johannessen, C. U., and Johannessen, S. I. (2003). Valproate: Past, Present, and Future. CNS Drug Rev. 9 (2), 199–216. doi:10.1111/j.1527-3458.2003.tb00249.x
Johannessen, S. I. (1997). Pharmacokinetics and Interaction Profile of Topiramate: Review and Comparison with Other Newer Antiepileptic Drugs. Epilepsia 38 (Suppl. 1), S18–S23. doi:10.1111/j.1528-1157.1997.tb04512.x
Johnson, E. M., Whyte, E., Mulsant, B. H., Pollock, B. G., Weber, E., Begley, A. E., et al. (2006). Cardiovascular Changes Associated with Venlafaxine in the Treatment of Late-Life Depression. Am. J. Geriatr. Psychiatry 14 (9), 796–802. doi:10.1097/01.JGP.0000204328.50105.b3
Joshi, S., and Rapoport, A. M. (2017). Diclofenac Potassium for Oral Solution (CAMBIA®) in the Acute Management of a Migraine Attack: Clinical Evidence and Practical Experience. Ther. Adv. Neurol. Disord. 10 (4), 217–226. doi:10.1177/1756285616684494
Jovanović, N., Božina, N., Lovrić, M., Medved, V., Jakovljević, M., and Peleš, A. M. (2010). The Role of CYP2D6 and ABCB1 Pharmacogenetics in Drug-Naïve Patients with First-Episode Schizophrenia Treated with Risperidone. Eur. J. Clin. Pharmacol. 66 (11), 1109–1117. doi:10.1007/s00228-010-0850-1
Kamide, K., Yang, J., Matayoshi, T., Takiuchi, S., Horio, T., Yoshii, M., et al. (2009). Genetic Polymorphisms of L-type Calcium Channel alpha1C and alpha1D Subunit Genes Are Associated with Sensitivity to the Antihypertensive Effects of L-type Dihydropyridine Calcium-Channel Blockers. Circ. J. 73 (4), 732–740. doi:10.1253/circj.cj-08-0761
Kandel, S. A., and Mandiga, P. (2021). “Cluster Headache,” in StatPearls [Internet] (Treasure Island (FL: StatPearls Publishing).
Kaniwa, N., Saito, Y., Aihara, M., Matsunaga, K., Tohkin, M., Kurose, K., et al. (2010). HLA-B*1511 Is a Risk Factor for Carbamazepine-Induced Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in Japanese Patients. Epilepsia 51 (12), 2461–2465. doi:10.1111/j.1528-1167.2010.02766.x
Kapur, B. M., Lala, P. K., and Shaw, J. L. (2014). Pharmacogenetics of Chronic Pain Management. Clin. Biochem. 47 (13-14), 1169–1187. doi:10.1016/j.clinbiochem.2014.05.065
Kariya, S., Isozaki, S., Uchino, K., Suzuki, T., and Narimatsu, S. (1996). Oxidative Metabolism of Flunarizine and Cinnarizine by Microsomes from B-Lymphoblastoid Cell Lines Expressing Human Cytochrome P450 Enzymes. Biol. Pharm. Bull. 19 (11), 1511–1514. doi:10.1248/bpb.19.1511
Karnes, J. H., Rettie, A. E., Somogyi, A. A., Huddart, R., Fohner, A. E., Formea, C. M., et al. (2021). Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C9 and HLA-B Genotypes and Phenytoin Dosing: 2020 Update. Clin. Pharmacol. Ther. 109 (2), 302–309. doi:10.1002/cpt.2008
Kato, R., and Yamazoe, Y. (1994). The Importance of Substrate Concentration in Determining Cytochromes P450 Therapeutically Relevant In Vivo. Pharmacogenetics 4 (6), 359–362. doi:10.1097/00008571-199412000-00010
Kidd, R. S., Curry, T. B., Gallagher, S., Edeki, T., Blaisdell, J., and Goldstein, J. A. (2001). Identification of a Null Allele of CYP2C9 in an African-American Exhibiting Toxicity to Phenytoin. Pharmacogenetics 11, 803–808. doi:10.1097/00008571-200112000-00008
Kim, J. H., Park, B. L., Cheong, H. S., Bae, J. S., Park, J. S., Jang, A. S., et al. (2010). Genome-wide and Follow-Up Studies Identify CEP68 Gene Variants Associated with Risk of Aspirin-Intolerant Asthma. PLoS One 5 (11), e13818. doi:10.1371/journal.pone.0013818
Kim, W. J., Lee, J. H., Yi, J., Cho, Y. J., Heo, K., Lee, S. H., et al. (2010). A Nonsynonymous Variation in MRP2/ABCC2 Is Associated with Neurological Adverse Drug Reactions of Carbamazepine in Patients with Epilepsy. Pharmacogenet Genomics 20 (4), 249–256. doi:10.1097/FPC.0b013e328338073a
Kirchheiner, J., Keulen, J. T., Bauer, S., Roots, I., and Brockmöller, J. (2008). Effects of the CYP2D6 Gene Duplication on the Pharmacokinetics and Pharmacodynamics of Tramadol. J. Clin. Psychopharmacol. 28 (1), 78–83. doi:10.1097/JCP.0b013e318160f827
Knezevic, N., Tverdohleb, T., Knezevic, I., and Candido, K. (2018). The Role of Genetic Polymorphisms in Chronic Pain Patients. Ijms 19 (6), 1707. doi:10.3390/ijms19061707
Kojić, Z., and Stojanović, D. (2013). Pathophysiology of Migraine-Ffrom Molecular to Personalized Medicine. Med. Pregl 66 (1-2), 53–57. doi:10.2298/mpns1302053k
Korinthenberg, R., Haug, C., and Hannak, D. (1994). The Metabolization of Carbamazepine to CBZ-10,11-Epoxide in Children from the Newborn Age to Adolescence. Neuropediatrics 25 (04), 214–216. doi:10.1055/s-2008-1073024
Kroemer, H. K., Gautier, J. C., Beaune, P., Henderson, C., Wolf, C. R., and Eichelbaum, M. (1993). Identification of P450 Enzymes Involved in Metabolism of Verapamil in Humans. Naunyn Schmiedebergs Arch. Pharmacol. 348 (3), 332–337. doi:10.1007/BF00169164
Kudrow, L. (1981). Response of Cluster Headache Attacks to Oxygen Inhalation. Headache 21 (1), 1–4. doi:10.1111/j.1526-4610.1981.hed2101001.x
Kuehl, G. E., Bigler, J., Potter, J. D., and Lampe, J. W. (2006). Glucuronidation of the Aspirin Metabolite Salicylic Acid by Expressed UDP-Glucuronosyltransferases and Human Liver Microsomes. Drug Metab. Dispos 34 (2), 199–202. doi:10.1124/dmd.105.005652
Kuehl, P., Zhang, J., Lin, Y., Lamba, J., Assem, M., Schuetz, J., et al. (2001). Sequence Diversity in CYP3A Promoters and Characterization of the Genetic Basis of Polymorphic CYP3A5 Expression. Nat. Genet. 27 (4), 383–391. doi:10.1038/86882
Lai, T. H., Fuh, J. L., and Wang, S. J. (2009). Cranial Autonomic Symptoms in Migraine: Characteristics and Comparison with Cluster Headache. J. Neurol. Neurosurg. Psychiatry 80 (10), 1116–1119. doi:10.1136/jnnp.2008.157743
Lange, R., Schwarz, J. A., and Hohn, M. (2000). Acetylsalicylic Acid Effervescent 1000 Mg (Aspirin) in Acute Migraine Attacks; a Multicentre, Randomized, Double-Blind, Single-Dose, Placebo-Controlled Parallel Group Study. Cephalalgia 20 (7), 663–667. doi:10.1111/j.1468-2982.2000.00101.x
Laska, A. J., Han, M. J., Lospinoso, J. A., Brown, P. J., and Beachkofsky, T. M. (2017). CYP2C19*2 Status in Patients with Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Pharmgenomics Pers Med. 10, 183–186. doi:10.2147/PGPM.S129908
Lavergne, F., Berlin, I., Gamma, A., Stassen, H., and Angst, J. (2005). Onset of Improvement and Response to Mirtazapine in Depression: a Multicenter Naturalistic Study of 4771 Patients. Neuropsychiatr. Dis. Treat. 1 (1), 59–68. doi:10.2147/nedt.1.1.59.52296
Law, S., Derry, S., and Moore, R. A. (2013). Triptans for Acute Cluster Headache. Cochrane Database Syst. Revpmcid 2013 (7), CD008042PMC6494511. doi:10.1002/14651858.CD008042.pub3
Lenaerts, M. E. (2009). Pharmacotherapy of Tension-type Headache (TTH). Expert Opin. Pharmacother. 10 (8), 1261–1271. doi:10.1517/14656560902942046
Leone, M., D'Amico, D., Frediani, F., Moschiano, F., Grazzi, L., Attanasio, A., et al. (2000). Verapamil in the Prophylaxis of Episodic Cluster Headache: a Double-Blind Study versus Placebo. Neurology 54 (6), 1382–1385. doi:10.1212/wnl.54.6.1382
Leung, S. M. (2021). Drug Use Evaluation: A Two-Year Retrospective Review of the Effectiveness and Tolerability of Agomelatine versus Mirtazapine in Patients with Depressive Disorder. Brain Behav. 11 (8), e2311. doi:10.1002/brb3.2311
Linde, M., Gustavsson, A., Stovner, L. J., Steiner, T. J., Barré, J., Katsarava, Z., et al. (2012). The Cost of Headache Disorders in Europe: the Eurolight Project. Eur. J. Neurol. 19 (5), 703–711. doi:10.1111/j.1468-1331.2011.03612.x
Lipton, R. B., Baggish, J. S., Stewart, W. F., Codispoti, J. R., and Fu, M. (2000). Efficacy and Safety of Acetaminophen in the Treatment of Migraine: Results of a Randomized, Double-Blind, Placebo-Controlled, Population-Based Study. Arch. Intern. Med. 160 (22), 3486–3492. doi:10.1001/archinte.160.22.3486
Lipton, R. B., Goadsby, P. J., Smith, J., Schaeffler, B. A., Biondi, D. M., Hirman, J., et al. (2020). Efficacy and Safety of Eptinezumab in Patients with Chronic Migraine: PROMISE-2. Neurology 94 (13), e1365–e1377. doi:10.1212/WNL.0000000000009169
Ljubisavljevic, S., and Zidverc Trajkovic, J. (2019). Cluster Headache: Pathophysiology, Diagnosis and Treatment. J. Neurol. 266 (5), 1059–1066. doi:10.1007/s00415-018-9007-4
Loder, E., Burch, R., and Rizzoli, P. (2012). The 2012 AHS/AAN Guidelines for Prevention of Episodic Migraine: a Summary and Comparison with Other Recent Clinical Practice Guidelines. Headache 52 (6), 930–945. doi:10.1111/j.1526-4610.2012.02185.x
Lopez, I., Mak, E. C., Ding, J., Hamm, H. E., and Lomasney, J. W. (2001). A Novel Bifunctional Phospholipase C that Is Regulated by Galpha 12 and Stimulates the Ras/mitogen-Activated Protein Kinase Pathway. J. Biol. Chem. 276 (4), 2758–2765. doi:10.1074/jbc.M008119200
Lovell, B. V., and Marmura, M. J. (2010). Valproate Semisodium ER for Migraine and Cluster Headache Prophylaxis. Expert Opin. Drug Metab. Toxicol. 6 (4), 495–504. doi:10.1517/17425251003693547
Magnoux, E., and Zlotnik, G. (2004). Outpatient Intravenous Dihydroergotamine for Refractory Cluster Headache. Headache 44 (3), 249–255. doi:10.1111/j.1526-4610.2004.04055.x
Makar, K. W., Poole, E. M., Resler, A. J., Seufert, B., Curtin, K., Kleinstein, S. E., et al. (2013). COX-1 (PTGS1) and COX-2 (PTGS2) Polymorphisms, NSAID Interactions, and Risk of colon and Rectal Cancers in Two Independent Populations. Cancer Causes Control 24 (12), 2059–2075. doi:10.1007/s10552-013-0282-1
Mamiya, K., Ieiri, I., Shimamoto, J., Yukawa, E., Imai, J., Ninomiya, H., et al. (1998). The Effects of Genetic Polymorphisms of CYP2C9 and CYP2C19 on Phenytoin Metabolism in Japanese Adult Patients with Epilepsy: Studies in Stereoselective Hydroxylation and Population Pharmacokinetics. Epilepsia 39 (12), 1317–1323. doi:10.1111/j.1528-1157.1998.tb01330.x
Man, C. B., Kwan, P., Baum, L., Yu, E., Lau, K. M., Cheng, A. S., et al. (2007). Association between HLA-B*1502 Allele and Antiepileptic Drug-Induced Cutaneous Reactions in Han ChineseErratum in. EpilepsiaEpilepsia 4849 (55), 1015941–1015948. doi:10.1111/j.1528-1167.2007.01022.x
Marjan, M. N., Hamzeh, M. T., Rahman, E., and Sadeq, V. (2014). A Computational prospect to Aspirin Side Effects: Aspirin and COX-1 Interaction Analysis Based on Non-synonymous SNPs. Comput. Biol. Chem. 51, 57–62. doi:10.1016/j.compbiolchem.2014.05.002
Marmura, M. J., and Kumpinsky, A. S. (2018). Refining the Benefit/Risk Profile of Anti-epileptic Drugs in Headache Disorders. CNS Drugs 32 (8), 735–746. doi:10.1007/s40263-018-0555-z
Marmura, M. J., Silberstein, S. D., and Schwedt, T. J. (2015). The Acute Treatment of Migraine in Adults: the American Headache Society Evidence Assessment of Migraine Pharmacotherapies. Headache 55 (1), 3–20. doi:10.1111/head.12499
Marmura, M. J. (2018). Triggers, Protectors, and Predictors in Episodic Migraine. Curr. Pain Headache Rep. 22 (12), 81. doi:10.1007/s11916-018-0734-0
May, A., Schwedt, T. J., Magis, D., Pozo-Rosich, P., Evers, S., and Wang, S. J. (2018). Cluster Headache. Nat. Rev. Dis. Primers 4, 18006. doi:10.1038/nrdp.2018.6
Mayans, L., and Walling, A. (2018). Acute Migraine Headache: Treatment Strategies. Am. Fam. Physician 97 (4), 243–251. PMID: 29671521.
McCormack, M., Alfirevic, A., Bourgeois, S., Farrell, J. J., Kasperavičiūtė, D., Carrington, M., et al. (2011). HLA-A*3101 and Carbamazepine-Induced Hypersensitivity Reactions in Europeans. N. Engl. J. Med. 364 (12), 1134–1143. doi:10.1056/NEJMoa1013297
McEvoy, L., Carr, D. F., and Pirmohamed, M. (2021). Pharmacogenomics of NSAID-Induced Upper Gastrointestinal Toxicity. Front. Pharmacol. 12, 684162. doi:10.3389/fphar.2021.684162
McKeever, R. G., and Hamilton, R. J. (2021). “Calcium Channel Blockers”in StatPearls [Internet] (Treasure Island (FL): StatPearls Publishing). PMID: 29494080.
McVige, J. W., Hogan, R. M., Shanahan, C. M., Amend, D. L., and Ferger, S. M. (2020). An Open-Label Study Evaluating the Pharmacokinetics and Safety of Diclofenac Potassium for Oral Solution for the Acute Treatment of MWA or MWoA in Pediatric Participants. Headache 60 (9), 1939–1946. doi:10.1111/head.13922
Mellström, B., Bertilsson, L., Säwe, J., Schulz, H. U., and Sjöqvist, F. (1981). E- and Z-10-Hydroxylation of Nortriptyline: Relationship to Polymorphic Debrisoquine Hydroxylation. Clin. Pharmacol. Ther. 30 (2), 189–193. doi:10.1038/clpt.1981.147
Mensah-Nyagan, A. G., Meyer, L., Schaeffer, V., Kibaly, C., and Patte-Mensah, C. (2009). Evidence for a Key Role of Steroids in the Modulation of Pain. Psychoneuroendocrinology 34 (Suppl. 1), S169–S177. doi:10.1016/j.psyneuen.2009.06.004
Möhler, H., Fritschy, J. M., and Rudolph, U. (2002). A New Benzodiazepine Pharmacology. J. Pharmacol. Exp. Ther. 300 (1), 2–8. doi:10.1124/jpet.300.1.2
Molana, A., Mehrpour, M., Vousooghi, N., Hajighasem, M. R., and Joghataei, M. T. (2014). Effect of NOS3 Gene Polymorphism on Response to Tricyclic Antidepressants in Migraine Attacks. Iranian J. Neurol. 13 (3), 154–159.
Monteith, T. S., and Oshinsky, M. L. (2009). Tension-type Headache with Medication Overuse: Pathophysiology and Clinical Implications. Curr. Pain Headache Rep. 13 (6), 463–469. doi:10.1007/s11916-009-0075-0
Moreno-Ajona, D., Pérez-Rodríguez, A., and Goadsby, P. J. (2020). Gepants, Calcitonin-Gene-Related Peptide Receptor Antagonists: what Could Be Their Role in Migraine Treatment. Curr. Opin. Neurol. 33 (3), 309–315. doi:10.1097/WCO.0000000000000806
Moreno-Mayordomo, R., Ruiz, M., Pascual, J., Gallego de la Sacristana, M., Vidriales, I., Sobrado, M., et al. (2019). CALCA and TRPV1 Genes Polymorphisms Are Related to a Good Outcome in Female Chronic Migraine Patients Treated with OnabotulinumtoxinA. J. Headache Pain 20 (1), 39. doi:10.1186/s10194-019-0989-9
Moskowitz, M. A., and Cutrer, F. M. (1993). SUMATRIPTAN: a Receptor-Targeted Treatment for Migraine. Annu. Rev. Med. 44, 145–154. doi:10.1146/annurev.me.44.020193.001045
Moubarak, A. S., and Rosenkrans, C. F. (2000). Hepatic Metabolism of Ergot Alkaloids in Beef Cattle by Cytochrome P450. Biochem. Biophys. Res. Commun. 274 (3), 746–749. doi:10.1006/bbrc.2000.3210
Mura, E., Govoni, S., Racchi, M., Carossa, V., Ranzani, G. N., Allegri, M., et al. (2013). Consequences of the 118A>G Polymorphism in the OPRM1 Gene: Translation from Bench to Bedside. J. Pain Res. 6, 331–353. doi:10.2147/JPR.S42040
National Clinical Guideline Centre (UK) (2012). Headaches: Diagnosis and Management of Headaches in Young People and Adults. [Internet]. London: Royal College of Physicians UK. PMID: 26065049.
Negro, A., and Martelletti, P. (2019). Gepants for the Treatment of Migraine. Expert Opin. Investig. Drugs 28 (6), 555–567. doi:10.1080/13543784.2019.1618830
Nieswand, V., Richter, M., and Gossrau, G. (2020). Epidemiology of Headache in Children and Adolescents-Another Type of Pandemia. Curr. Pain Headache Rep. 24 (10), 62. doi:10.1007/s11916-020-00892-6
Ninomiya, H., Mamiya, K., Matsuo, S., Ieiri, I., Higuchi, S., and Tashiro, N. (2000). Genetic Polymorphism of the CYP2C Subfamily and Excessive Serum Phenytoin Concentration with central Nervous System Intoxication. Ther. Drug Monit. 22, 230–232. doi:10.1097/00007691-200004000-00016
Niu, Y., Gong, Y., Langaee, T. Y., Davis, H. M., Elewa, H., Beitelshees, A. L., et al. (2010). Genetic Variation in the Beta2 Subunit of the Voltage-Gated Calcium Channel and Pharmacogenetic Association with Adverse Cardiovascular Outcomes in the INternational VErapamil SR-Trandolapril STudy GENEtic Substudy (INVEST-GENES). Circ. Cardiovasc. Genet. 3 (6), 548–555. doi:10.1161/CIRCGENETICS.110.957654
Cephalalgia (2018). Headache Classification Committee of the International Headache Society (IHS) the International Classification of Headache Disorders, 3rd Edition. Cephalalgia 38 (1), 1–211. doi:10.1177/0333102417738202
Noai, M., Soraoka, H., Kajiwara, A., Tanamachi, Y., Oniki, K., Nakagawa, K., et al. (2016). Cytochrome P450 2C19 Polymorphisms and Valproic Acid-Induced Weight Gain. Acta Neurol. Scand. 133 (3), 216–223. doi:10.1111/ane.12473
Obermann, M., Nägel, S., Ose, C., Sonuc, N., Scherag, A., Storch, P., et al. (2021). Safety and Efficacy of Prednisone versus Placebo in Short-Term Prevention of Episodic Cluster Headache: a Multicentre, Double-Blind, Randomised Controlled Trial. Lancet Neurol. 20 (1), 29–37. doi:10.1016/S1474-4422(20)30363-X
Ong, J. J. Y., and De Felice, M. (2018). Migraine Treatment: Current Acute Medications and Their Potential Mechanisms of Action. Neurotherapeutics 15 (2), 274–290. doi:10.1007/s13311-017-0592-1
Orr, S. L., Aubé, M., Becker, W. J., Davenport, W. J., Dilli, E., Dodick, D., et al. (2015). Canadian Headache Society Systematic Review and Recommendations on the Treatment of Migraine Pain in Emergency Settings. Cephalalgia 35 (3), 271–284. doi:10.1177/0333102414535997
Owusu Obeng, A., Hamadeh, I., and Smith, M. (2017). Review of Opioid Pharmacogenetics and Considerations for Pain Management. Pharmacotherapy 37 (9), 1105–1121. doi:10.1002/phar.1986
Pahor, M., Manto, A., Pedone, C., Carosella, L., Guralnik, J. M., and Carbonin, P. (1996). Age and severe adverse drug reactions caused by nifedipine and verapamil. Gruppo Italiano di Farmacovigilanza nell' Anziano (GIFA). J. Clin. Epidemiol. 49 (8), 921–928. doi:10.1016/0895-4356(96)00056-x
Palacios-Ceña, M., Wang, K., Castaldo, M., Ordás-Bandera, C., Torelli, P., Arendt-Nielsen, L., et al. (2019). Variables Associated with the Use of Prophylactic Amitriptyline Treatment in Patients with Tension-type Headache. Clin. J. Pain 35 (4), 315–320. doi:10.1097/AJP.0000000000000685
Pardutz, A., and Schoenen, J. (2010). NSAIDs in the Acute Treatment of Migraine: A Review of Clinical and Experimental Data. Pharmaceuticals (Basel) 3 (6), 1966–1987. doi:10.3390/ph3061966
Park, J. Y., Kim, K. A., Park, P. W., Lee, O. J., Kang, D. K., Shon, J. H., et al. (2006). Effect of CYP3A5*3 Genotype on the Pharmacokinetics and Pharmacodynamics of Alprazolam in Healthy Subjects. Clin. Pharmacol. Ther. 79 (6), 590–599. doi:10.1016/j.clpt.2006.02.008
Pavithra, V., Mishra, D., Behera, S., and Juneja, M. (2020). Paracetamol versus Ibuprofen for the Acute Treatment of Migraine Headache in Children: A Blinded Randomized Controlled Trial. Indian J. Pediatr. 87 (10), 781–786. doi:10.1007/s12098-020-03315-x
Pearce, R. E., Vakkalagadda, G. R., and Leeder, J. S. (2002). Pathways of Carbamazepine Bioactivation In Vitro I. Characterization of Human Cytochromes P450 Responsible for the Formation of 2- and 3-hydroxylated Metabolites. Drug Metab. Dispos. 30 (11), 1170–1179. doi:10.1124/dmd.30.11.1170
Phillips, E. J., Sukasem, C., Whirl-Carrillo, M., Müller, D. J., Dunnenberger, H. M., Chantratita, W., et al. (2018). Clinical Pharmacogenetics Implementation Consortium Guideline for HLA Genotype and Use of Carbamazepine and Oxcarbazepine: 2017 Update. Clin. Pharmacol. Ther. 103 (4), 574–581. doi:10.1002/cpt.1004
Pisanu, C., Lundin, E., Preisig, M., Gholam-Rezaee, M., Castelao, E., Pistis, G., et al. (2020). Major Depression Subtypes Are Differentially Associated with Migraine Subtype, Prevalence and Severity. Cephalalgia 40 (4), 347–356. doi:10.1177/0333102419884935
Pisanu, C., Preisig, M., Castelao, E., Glaus, J., Pistis, G., Squassina, A., et al. (2017a). A Genetic Risk Score Is Differentially Associated with Migraine with and without Aura. Hum. Genet. 136 (8), 999–1008. doi:10.1007/s00439-017-1816-5
Pisanu, C., Preisig, M., Castelao, E., Glaus, J., Cunningham, J. L., Del Zompo, M., et al. (2017b). High Leptin Levels Are Associated with Migraine with Aura. Cephalalgia 37 (5), 435–441. doi:10.1177/0333102416648650
Pomes, L. M., Gentile, G., Simmaco, M., Borro, M., and Martelletti, P. (2018). Tailoring Treatment in Polymorbid Migraine Patients through Personalized Medicine. CNS Drugs 32 (6), 559–565. doi:10.1007/s40263-018-0532-6
Pomes, L. M., Guglielmetti, M., Bertamino, E., Simmaco, M., Borro, M., and Martelletti, P. (2019). Optimising Migraine Treatment: from Drug-Drug Interactions to Personalized Medicine. J. Headache Pain 20 (1), 56. doi:10.1186/s10194-019-1010-3
Poulsen, C. F., Simeone, T. A., Maar, T. E., Smith-Swintosky, V., White, H. S., and Schousboe, A. (2004). Modulation by Topiramate of AMPA and Kainate Mediated Calcium Influx in Cultured Cerebral Cortical, Hippocampal and Cerebellar Neurons. Neurochem. Res. 29 (1), 275–282. doi:10.1023/b:nere.0000010456.92887.3b
Puledda, F., Messina, R., and Goadsby, P. J. (2017). An Update on Migraine: Current Understanding and Future Directions. J. Neurol. 264 (9), 2031–2039. doi:10.1007/s00415-017-8434-y
Qin, X. P., Xie, H. G., Wang, W., He, N., Huang, S. L., Xu, Z. H., et al. (1999). Effect of the Gene Dosage of CgammaP2C19 on Diazepam Metabolism in Chinese Subjects. Clin. Pharmacol. Ther. 66 (6), 642–646. doi:10.1016/S0009-9236(99)90075-9
Rains, J. C., Davis, R. E., and Smitherman, T. A. (2015). Tension-type Headache and Sleep. Curr. Neurol. Neurosci. Rep. 15 (2), 520. doi:10.1007/s11910-014-0520-2
Ramasamy, K., Narayan, S. K., Chanolean, S., and Chandrasekaran, A. (2007). Severe Phenytoin Toxicity in a CYP2C9*3*3 Homozygous Mutant from India. Neurol. India 55, 408–409. doi:10.4103/0028-3886.33300
Ramírez Rosas, M. B., Labruijere, S., Villalón, C. M., and Maassen Vandenbrink, A. (2013). Activation of 5-hydroxytryptamine1B/1D/1F Receptors as a Mechanism of Action of Antimigraine Drugs. Expert Opin. Pharmacother. 14 (12), 1599–1610. doi:10.1517/14656566.2013.806487
Rapoport, A. M., Bigal, M. E., Tepper, S. J., and Sheftell, F. D. (2004). Intranasal Medications for the Treatment of Migraine and Cluster Headache. CNS Drugs 18 (10), 671–685. doi:10.2165/00023210-200418100-00004
Rawson, K. S., Dixon, D., Civitelli, R., Peterson, T. R., Mulsant, B. H., Reynolds, C. F., et al. (2017). Bone Turnover with Venlafaxine Treatment in Older Adults with Depression. J. Am. Geriatr. Soc. 65 (9), 2057–2063. doi:10.1111/jgs.14936
Rizzoli, P. B. (2018). What the Pharmacological Management of Migraine Can Tell Us about the Future of Migraine Patient Care. Neurol. Sci. 39 (Suppl. 1), 39–45. doi:10.1007/s10072-018-3338-x
Robbins, M. S., Starling, A. J., Pringsheim, T. M., Becker, W. J., and Schwedt, T. J. (2016). Treatment of Cluster Headache: The American Headache Society Evidence-Based Guidelines. Headache 56 (7), 1093–1106. doi:10.1111/head.12866
Roberto, G., Raschi, E., Piccinni, C., Conti, V., Vignatelli, L., D'Alessandro, R., et al. (2015). Adverse Cardiovascular Events Associated with Triptans and Ergotamines for Treatment of Migraine: Systematic Review of Observational Studies. Cephalalgia 35 (2), 118–131. doi:10.1177/0333102414550416
Rozen, T. D., Niknam, R. M., Shechter, A. L., Young, W. B., and Silberstein, S. D. (2001). Cluster Headache in Women: Clinical Characteristics and Comparison with Cluster Headache in Men. J. Neurol. Neurosurg. Psychiatrypmcid 70 (5), 613PMC1737364–7. doi:10.1136/jnnp.70.5.613
Russell, M. B. (2007). Genetics of Tension-type Headache. J. Headache Pain 8 (2), 71–76. doi:10.1007/s10194-007-0366-y
Russell, M. B. (2005). Tension-type Headache in 40-Year-Olds: a Danish Population-Based Sample of 4000. J. Headache Pain 6 (6), 441–447. doi:10.1007/s10194-005-0253-3
Sacco, S., Bendtsen, L., Ashina, M., Reuter, U., Terwindt, G., Mitsikostas, D. D., et al. (2019). European Headache Federation Guideline on the Use of Monoclonal Antibodies Acting on the Calcitonin Gene Related Peptide or its Receptor for Migraine Prevention. J. Headache Pain 20 (1), 6. doi:10.1186/s10194-018-0955-y
Sánchez-Rodríguez, C., Sierra, Á., Planchuelo-Gómez, Á., Martínez-Pías, E., Guerrero, Á. L., and García-Azorín, D. (2021). Real World Effectiveness and Tolerability of Candesartan in the Treatment of Migraine: a Retrospective Cohort Study. Sci. Rep. 11 (1), 3846. doi:10.1038/s41598-021-83508-2
Sarchielli, P., Granella, F., Prudenzano, M. P., Pini, L. A., Guidetti, V., Bono, G., et al. (2012). Italian Guidelines for Primary Headaches: 2012 Revised Version. J. Headache Pain 13 (Suppl. 2), S31–S70. doi:10.1007/s10194-012-0437-6
Saylor, D., and Steiner, T. J. (2018). The Global Burden of Headache. Semin. Neurol. 38 (2), 182–190. doi:10.1055/s-0038-1646946
Schou, W. S., Ashina, S., Amin, F. M., Goadsby, P. J., and Ashina, M. (2017). Calcitonin Gene-Related Peptide and Pain: a Systematic Review. J. Headache Pain 18 (1), 34. doi:10.1186/s10194-017-0741-2
Schrader, H., Stovner, L. J., Helde, G., Sand, T., and Bovim, G. (2001). Prophylactic Treatment of Migraine with Angiotensin Converting Enzyme Inhibitor (Lisinopril): Randomised, Placebo Controlled, Crossover Study. BMJ 322 (7277), 19–22. doi:10.1136/bmj.322.7277.19
Schürks, M., Kurth, T., Stude, P., Rimmbach, C., de Jesus, J., Jonjic, M., et al. (2007). G Protein Beta3 Polymorphism and Triptan Response in Cluster Headache. Clin. Pharmacol. Ther. 82 (4), 396–401. doi:10.1038/sj.clpt.6100159
Schwaiger, J., Kiechl, S., Seppi, K., Sawires, M., Stockner, H., Erlacher, T., et al. (2009). Prevalence of Primary Headaches and Cranial Neuralgias in Men and Women Aged 55-94 Years (Bruneck Study). Cephalalgia 29 (2), 179–187. doi:10.1111/j.1468-2982.2008.01705.x
Scuteri, D., Corasaniti, M. T., Tonin, P., Nicotera, P., and Bagetta, G. (2021). Role of CGRP Pathway Polymorphisms in Migraine: a Systematic Review and Impact on CGRP mAbs Migraine Therapy. J. Headache Pain 22 (1), 87. doi:10.1186/s10194-021-01295-7
Shalimova, A., Babasieva, V., Chubarev, V. N., Tarasov, V. V., Schiöth, H. B., and Mwinyi, J. (2021). Therapy Response Prediction in Major Depressive Disorder: Current and Novel Genomic Markers Influencing Pharmacokinetics and Pharmacodynamics. Pharmacogenomics 22 (8), 485–503. doi:10.2217/pgs-2020-0157
Shams, M. E., Arneth, B., Hiemke, C., Dragicevic, A., Müller, M. J., Kaiser, R., et al. (2006). CYP2D6 Polymorphism and Clinical Effect of the Antidepressant Venlafaxine. J. Clin. Pharm. Ther. 31 (5), 493–502. doi:10.1111/j.1365-2710.2006.00763.x
Shih, P. S., and Huang, J. D. (2002). Pharmacokinetics of Midazolam and 1'-hydroxymidazolam in Chinese with Different CYP3A5 Genotypes. Drug Metab. Dispos 30 (12), 1491–1496. doi:10.1124/dmd.30.12.1491
Shin, J. G., Park, J. Y., Kim, M. J., Shon, J. H., Yoon, Y. R., Cha, I. J., et al. (2002). Inhibitory Effects of Tricyclic Antidepressants (TCAs) on Human Cytochrome P450 Enzymes In Vitro: Mechanism of Drug Interaction between TCAs and Phenytoin. Drug Metab. Dispos 30 (10), 1102–1107. doi:10.1124/dmd.30.10.1102
Silberstein, S. D. (1996). Divalproex Sodium in Headache: Literature Review and Clinical Guidelines. Headache 36 (9), 547–555. doi:10.1046/j.1526-4610.1996.3609547.x
Silberstein, S. D., Holland, S., Freitag, F., Dodick, D. W., Argoff, C., and Ashman, E. (2012). Evidence-based Guideline Update: Pharmacologic Treatment for Episodic Migraine Prevention in Adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology 78 (17), 1337–1345. doi:10.1212/WNL.0b013e3182535d20
Silberstein, S. D., Lipton, R. B., Dodick, D. W., Freitag, F. G., Ramadan, N., Mathew, N., et al. (2007). Efficacy and Safety of Topiramate for the Treatment of Chronic Migraine: a Randomized, Double-Blind, Placebo-Controlled Trial. Headache 47, 170–180. doi:10.1111/j.1526-4610.2006.00684.x
Silberstein, S. D. (2000). Practice Parameter: Evidence-Based Guidelines for Migraine Headache (An Evidence-Based Review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 55 (6), 754–762. doi:10.1212/wnl.55.6.754
Sim, S. C., Risinger, C., Dahl, M. L., Aklillu, E., Christensen, M., Bertilsson, L., et al. (2006). A Common Novel CYP2C19 Gene Variant Causes Ultrarapid Drug Metabolism Relevant for the Drug Response to Proton Pump Inhibitors and Antidepressants. Clin. Pharmacol. Ther. 79 (1), 103–113. doi:10.1016/j.clpt.2005.10.002
Simpson, D. M., Hallett, M., Ashman, E. J., Comella, C. L., Green, M. W., Gronseth, G. S., et al. (2016). Practice Guideline Update Summary: Botulinum Neurotoxin for the Treatment of Blepharospasm, Cervical Dystonia, Adult Spasticity, and Headache: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 86 (19), 1818–1826. doi:10.1212/WNL.0000000000002560
Sistonen, J., Sajantila, A., Lao, O., Corander, J., Barbujani, G., and Fuselli, S. (2007). CYP2D6 Worldwide Genetic Variation Shows High Frequency of Altered Activity Variants and No continental Structure. Pharmacogenet Genomics 17 (2), 93–101. doi:10.1097/01.fpc.0000239974.69464.f2
Skryabin, V. Y., Zastrozhin, M., Torrado, M., Grishina, E., Ryzhikova, K., Shipitsyn, V., et al. (2021). Effects of CYP2C19*17 Genetic Polymorphisms on the Steady-State Concentration of Diazepam in Patients with Alcohol Withdrawal Syndrome. Hosp. Pharm. 56 (5), 592–596. doi:10.1177/0018578720931756
Skryabin, V. Y., Zastrozhin, M. S., Torrado, M. V., Grishina, E. A., Ryzhikova, K. A., Shipitsyn, V. V., et al. (2020). How Do CYP2C19*2 and CYP2C19*17 Genetic Polymorphisms Affect the Efficacy and Safety of Diazepam in Patients with Alcohol Withdrawal Syndrome. Drug Metab. Pers Ther. 35, j/dmdi.2020.35.issue-1/dmpt-2019-0026/dmpt-2019-0026.xml. doi:10.1515/dmpt-2019-0026
Smrcka, A. V., Brown, J. H., and Holz, G. G. (2012). Role of Phospholipase Cε in Physiological Phosphoinositide Signaling Networks. Cell Signal 24 (6), 1333–1343. doi:10.1016/j.cellsig.2012.01.009
Srisuma, S., Lavonas, E. J., and Wananukul, W. (2014). Ergotism and Factitious Hypotension Associated with Interaction of Ergotamine with CYP3A4 Inhibitors. Clin. Toxicol. (Phila) 52 (7), 674–677. doi:10.3109/15563650.2014.933230
Stamer, U. M., Musshoff, F., Stüber, F., Brockmöller, J., Steffens, M., and Tzvetkov, M. V. (2016). Loss-of-function Polymorphisms in the Organic Cation Transporter OCT1 Are Associated with Reduced Postoperative Tramadol Consumption. Pain 157 (11), 2467–2475. doi:10.1097/j.pain.0000000000000662
Steimer, W., Zöpf, K., von Amelunxen, S., Pfeiffer, H., Bachofer, J., Popp, J., et al. (2005). Amitriptyline or Not, that Is the Question: Pharmacogenetic Testing of CYP2D6 and CYP2C19 Identifies Patients with Low or High Risk for Side Effects in Amitriptyline Therapy. Clin. Chem. 51 (2), 376–385. doi:10.1373/clinchem.2004.041327
Steiner, T. J., Jensen, R., Katsarava, Z., Linde, M., MacGregor, E. A., Osipova, V., et al. (2019). Aids to Management of Headache Disorders in Primary Care (2nd Edition) : on Behalf of the European Headache Federation and Lifting the Burden: the Global Campaign against Headache. J. Headache Pain 20 (1), 57. doi:10.1186/s10194-018-0899-2
Stewart, J. D., Horvath, R., Baruffini, E., Ferrero, I., Bulst, S., Watkins, P. B., et al. (2010). Polymerase γ Gene POLG Determines the Risk of Sodium Valproate-Induced Liver Toxicity. Hepatology 52 (5), 1791–1796. doi:10.1002/hep.23891
Stovner, L. J., and Andree, C. (2010). Prevalence of Headache in Europe: a Review for the Eurolight Project. J. Headache Pain 11 (4), 289–299. doi:10.1007/s10194-010-0217-0
Stovner, L. J., Linde, M., Gravdahl, G. B., Tronvik, E., Aamodt, A. H., Sand, T., et al. (2014). A Comparative Study of Candesartan versus Propranolol for Migraine Prophylaxis: A Randomised, Triple-Blind, Placebo-Controlled, Double Cross-Over Study. Cephalalgia 34 (7), 523–532. doi:10.1177/0333102413515348
Strom, C. M., Goos, D., Crossley, B., Zhang, K., Buller-Burkle, A., Jarvis, M., et al. (2012). Testing for Variants in CYP2C19: Population Frequencies and Testing Experience in a Clinical Laboratory. Genet. Med. 14 (1), 95–100. doi:10.1038/gim.0b013e3182329870
Stubberud, A., Flaaen, N. M., McCrory, D. C., Pedersen, S. A., and Linde, M. (2019). Flunarizine as Prophylaxis for Episodic Migraine: a Systematic Review with Meta-Analysis. Pain 160 (4), 762–772. doi:10.1097/j.pain.0000000000001456
Suwała, J., Machowska, M., and Wiela-Hojeńska, A. (2019). Venlafaxine Pharmacogenetics: a Comprehensive Review. Pharmacogenomics 20 (11), 829–845. doi:10.2217/pgs-2019-0031
Szkutnik-Fiedler, D. D. (2020). Pharmacokinetics, Pharmacodynamics and Drug-Drug Interactions of New Anti-migraine Drugs-Lasmiditan, Gepants, and Calcitonin-Gene-Related Peptide (CGRP) Receptor Monoclonal Antibodies. Pharmaceutics 12 (12), 1180. doi:10.3390/pharmaceutics12121180
Szok, D., Csáti, A., Vécsei, L., and Tajti, J. (2015). Treatment of Chronic Migraine with OnabotulinumtoxinA: Mode of Action, Efficacy and Safety. Toxins (Basel) 7 (7), 2659–2673. doi:10.3390/toxins7072659
Taghdiri, F., Togha, M., Razeghi Jahromi, S., and Refaeian, F. (2014). Cinnarizine for the Prophylaxis of Migraine Associated Vertigo: a Retrospective Study. Springerplus 3, 231. doi:10.1186/2193-1801-3-231
Tan, L., Yu, J. T., Sun, Y. P., Ou, J. R., Song, J. H., and Yu, Y. (2010). The Influence of Cytochrome Oxidase CYP2A6, CYP2B6, and CYP2C9 Polymorphisms on the Plasma Concentrations of Valproic Acid in Epileptic Patients. Clin. Neurol. Neurosurg. 112 (4), 320–323. doi:10.1016/j.clineuro.2010.01.002
Tang, C., Unekawa, M., Kitagawa, S., Takizawa, T., Kayama, Y., Nakahara, J., et al. (2020). Cortical Spreading Depolarisation-Induced Facial Hyperalgesia, Photophobia and Hypomotility Are Ameliorated by Sumatriptan and Olcegepant. Sci. Rep. 10 (1), 11408. doi:10.1038/s41598-020-67948-w
Tardiolo, G., Bramanti, P., and Mazzon, E. (2019). Migraine: Experimental Models and Novel Therapeutic Approaches. Int. J. Mol. Sci. 20 (12), 2932. doi:10.3390/ijms20122932
Tepper, S. J. (2018). History and Review of Anti-calcitonin Gene-Related Peptide (CGRP) Therapies: From Translational Research to Treatment. Headache 58 Suppl 3 (Suppl. 3), 238–275. doi:10.1111/head.13379
Terrazzino, S., Viana, M., Floriddia, E., Monaco, F., Mittino, D., Sances, G., et al. (2010). The Serotonin Transporter Gene Polymorphism STin2 VNTR Confers an Increased Risk of Inconsistent Response to Triptans in Migraine Patients. Eur. J. Pharmacol. 641 (2-3), 82–87. doi:10.1016/j.ejphar.2010.04.049
Tfelt-Hansen, P., Saxena, P. R., Dahlöf, C., Pascual, J., Láinez, M., Henry, P., et al. (2000). Ergotamine in the Acute Treatment of Migraine: a Review and European Consensus. Brain 123 (Pt 1), 9–18. doi:10.1093/brain/123.1.9
Tracy, T. S., Korzekwa, K. R., Gonzalez, F. J., and Wainer, I. W. (1999). Cytochrome P450 Isoforms Involved in Metabolism of the Enantiomers of Verapamil and Norverapamil. Br. J. Clin. Pharmacol. 47 (5), 545–552. doi:10.1046/j.1365-2125.1999.00923.x
Tronvik, E., Stovner, L. J., Bovim, G., White, L. R., Gladwin, A. J., Owen, K., et al. (2008). Angiotensin-converting Enzyme Gene Insertion/deletion Polymorphism in Migraine Patients. BMC Neurol. 8, 4. doi:10.1186/1471-2377-8-4
Tronvik, E., Stovner, L. J., Schrader, H., and Bovim, G. (2006). Involvement of the Renin-Angiotensin System in Migraine. J. Hypertens. Suppl. 24 (1), S139–S143. doi:10.1097/01.hjh.0000220419.86149.11
Tso, A. R., Brudfors, M., Danno, D., Grangeon, L., Cheema, S., Matharu, M., et al. (2021). Machine Phenotyping of Cluster Headache and its Response to Verapamil. Brain 144 (2), 655–664. doi:10.1093/brain/awaa388
Turner, S. T., Bailey, K. R., Schwartz, G. L., Chapman, A. B., Chai, H. S., and Boerwinkle, E. (2012). Genomic Association Analysis Identifies Multiple Loci Influencing Antihypertensive Response to an Angiotensin II Receptor Blocker. Hypertension 59 (6), 1204–1211. doi:10.1161/HYP.0b013e31825b30f8
Tzvetkov, M. V. (2017). OCT1 Pharmacogenetics in Pain Management: Is a Clinical Application within Reach. Pharmacogenomics 18 (16), 1515–1523. doi:10.2217/pgs-2017-0095
Tzvetkov, M. V., Saadatmand, A. R., Lötsch, J., Tegeder, I., Stingl, J. C., and Brockmöller, J. (2011). Genetically Polymorphic OCT1: Another Piece in the Puzzle of the Variable Pharmacokinetics and Pharmacodynamics of the Opioidergic Drug Tramadol. Clin. Pharmacol. Ther. 90 (1), 143–150. doi:10.1038/clpt.2011.56
Ueda, K., Ishitsu, T., Seo, T., Ueda, N., Murata, T., Hori, M., et al. (2007). Glutathione S-Transferase M1 Null Genotype as a Risk Factor for Carbamazepine-Induced Mild Hepatotoxicity. Pharmacogenomics 8, 435–442. doi:10.2217/14622416.8.5.435
UpToDate (2016). Tricyclic and Tetracyclic Drugs: Pharmacology, Administration, and Side Effects. Available from: https://www.uptodate.com/contents/tricyclic-and-tetracyclic-drugs-pharmacology-administration-and-side effects?source=machineLearning&search=tricyclic+antidepressants&selectedTitle=1∼150§ionRank=2&anchor=H31 - references (Cited August 2, 2016).
Urits, I., Clark, G., An, D., Wesp, B., Zhou, R., Amgalan, A., et al. (2020). An Evidence-Based Review of Fremanezumab for the Treatment of Migraine. Pain Ther. 9 (1), 195–215. doi:10.1007/s40122-020-00159-3
US Food and Drug Administration (2007). Carbamazepine (Marketed as Carbatrol, Equetro, Tegreto and Generics) FDA. Baltimore: US Food and Drug Administration. [consultado 7 Jun 2014].
US Food and Drug Administration (FDA) (2020). Phenytoin Drug Label. Available at: https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&varApplNo=010151 (Accessed January 10, 2020).
Uzun, S., Kozumplik, O., Jakovljević, M., and Sedić, B. (2010). Side Effects of Treatment with Benzodiazepines. Psychiatr. Danub 22 (1), 90–93.
Valdes, R., and Yin, D. T. (2016). Fundamentals of Pharmacogenetics in Personalized, Precision Medicine. Clin. Lab. Med. 36 (3), 447–459. doi:10.1016/j.cll.2016.05.006
Van den Berg, R. J., Kok, P., and Voskuyl, R. A. (1993). Valproate and Sodium Currents in Cultured Hippocampal Neurons. Exp. Brain Res. 93 (2), 279–287. doi:10.1007/BF00228395
Venkatakrishnan, K., von Moltke, L. L., and Greenblatt, D. J. (19991999). Nortriptyline E-10-Hydroxylation In Vitro Is Mediated by Human CYP2D6 (High Affinity) and CYP3A4 (Low Affinity): Implications for Interactions with Enzyme-Inducing drugsErratum in. J. Clin. Pharmacolj Clin. Pharmacol. 3939 (68), 567866–567877. PMID: 10354960. doi:10.1177/00912709922008173
Vila-Pueyo, M. (2018). Targeted 5-HT1F Therapies for Migraine. Neurotherapeutics 15 (2), 291–303. doi:10.1007/s13311-018-0615-6
Volpe, F. M. (2008). An 8-week, Open-Label Trial of Duloxetine for Comorbid Major Depressive Disorder and Chronic Headache. J. Clin. Psychiatry 69 (9), 1449–1454. doi:10.4088/jcp.v69n0912
Wammes-van der Heijden, E. A., Rahimtoola, H., Leufkens, H. G., Tijssen, C. C., and Egberts, A. C. (2006). Risk of Ischemic Complications Related to the Intensity of Triptan and Ergotamine Use. Neurology 67 (7), 1128–1134. doi:10.1212/01.wnl.0000240128.76399.fa
Wan, J., Xia, H., He, N., Lu, Y. Q., and Zhou, H. H. (1996). The Elimination of Diazepam in Chinese Subjects Is Dependent on the Mephenytoin Oxidation Phenotype. Br. J. Clin. Pharmacol. 42 (4), 471–474. doi:10.1046/j.1365-2125.1996.42712.x
Wang, J., Huang, Q., Li, N., Tan, G., Chen, L., and Zhou, J. (2013). Triggers of Migraine and Tension-type Headache in China: a Clinic-Based Survey. Eur. J. Neurol. 20 (4), 689–696. doi:10.1111/ene.12039
Wang-Tilz, Y., Tilz, C., Wang, B., Tilz, G. P., and Stefan, H. (2006). Influence of Lamotrigine and Topiramate on MDR1 Expression in Difficult-To-Treat Temporal Lobe Epilepsy. Epilepsia 47 (2), 233–239. doi:10.1111/j.1528-1167.2006.00414.x
Watanabe, S., and Bruera, E. (1994). Corticosteroids as Adjuvant Analgesics. J. Pain Symptom Manage. 9, 442–445. doi:10.1016/0885-3924(94)90200-3
Weatherall, M. W. (2015). Drug Therapy in Headache. Clin. Med. (Lond) 15 (3), 273–279. doi:10.7861/clinmedicine.15-3-273
Wei, D. Y., Khalil, M., and Goadsby, P. J. (2019). Managing Cluster Headache. Pract. Neurol. 19 (6), 521–528. doi:10.1136/practneurol-2018-002124
Woldeamanuel, Y., Rapoport, A., and Cowan, R. (2015). The Place of Corticosteroids in Migraine Attack Management: a 65-year Systematic Review with Pooled Analysis and Critical Appraisal. Cephalalgia. 35, 996–1024. doi:10.1177/0333102414566200
Wrobel Goldberg, S., Silberstein, S., and Grosberg, B. M. (2014). Considerations in the Treatment of Tension-type Headache in the Elderly. Drugs Aging 31 (11), 797–804. doi:10.1007/s40266-014-0220-2
Yang, L. P. (2013). Sumatriptan/naproxen Sodium: a Review of its Use in Adult Patients with Migraine. Drugs 73 (12), 1339–1355. doi:10.1007/s40265-013-0099-y
Yang, M., Kozminski, D. J., Wold, L. A., Modak, R., Calhoun, J. D., Isom, L. L., et al. (2012). Therapeutic Potential for Phenytoin: Targeting Na(v)1.5 Sodium Channels to Reduce Migration and Invasion in Metastatic Breast Cancer. Breast Cancer Res. Treat. 134 (2), 603–615. doi:10.1007/s10549-012-2102-9
Young, W. B., Bradley, K. C., Anjum, M. W., and Gebeline-Myers, C. (2013). Duloxetine Prophylaxis for Episodic Migraine in Persons without Depression: a Prospective Study. Headache 53 (9), 1430–1437. doi:10.1111/head.12205
Zajic, S. C., Jarvis, J. P., Zhang, P., Rajula, K. D., Brangan, A., Brenner, R., et al. (2019). Individuals with CYP2C8 and CYP2C9 Reduced Metabolism Haplotypes Self-Adjusted Ibuprofen Dose in the Coriell Personalized Medicine Collaborative. Pharmacogenet Genomics 29 (3), 49–57. doi:10.1097/FPC.0000000000000364
Zhao, M., Zhang, T., Li, G., Qiu, F., Sun, Y., and Zhao, L. (2017). Associations of CYP2C9 and CYP2A6 Polymorphisms with the Concentrations of Valproate and its Hepatotoxin Metabolites and Valproate-Induced Hepatotoxicity. Basic Clin. Pharmacol. Toxicol. 121 (2), 138–143. doi:10.1111/bcpt.12776
Zissis, N. P., Harmoussi, S., Vlaikidis, N., Mitsikostas, D., Thomaidis, T., Georgiadis, G., et al. (2007). A Randomized, Double-Blind, Placebo-Controlled Study of Venlafaxine XR in Out-Patients with Tension-type Headache. Cephalalgia 27 (4), 315–324. doi:10.1111/j.1468-2982.2007.01300.x
Zobdeh, F., Kraiem, A., Attwood, M. M., Chubarev, V. N., Tarasov, V. V., Schiöth, H. B., et al. (2021). Pharmacological Treatment of Migraine: Drug Classes, Mechanisms of Action, Clinical Trials and New Treatments. Br. J. Pharmacol. 178, 4588–4607. doi:10.1111/bph.15657
Zona, C., Ciotti, M. T., and Avoli, M. (1997). Topiramate Attenuates Voltage-Gated Sodium Currents in Rat Cerebellar Granule Cells. Neurosci. Lett. 231, 123–126. doi:10.1016/s0304-3940(97)00543-0
Glossary
5-HT 5-hydroxytryptamine
5-HTR 5-HT receptors
AAN American Academy of Neurology
ACE inhibitors Angiotensin converting enzyme inhibitors
ARBs Angiotensin II type 1 receptor blockers
CBZ Carbamazepine
CCB Calcium channel blockers
CGRP Calcitonin-gene related peptide
COX Cyclooxygenase
CYP450 Cytochrome P450
DPWG Dutch Pharmacogenetics Working Group
EHF European Headache Federation
EPHX1: Microsomal epoxide hydrolase
FDA Food and Drug Administration
GABA γ-aminobutyric acid
GFR Glomerular filtration rate
GSTM1 Glutathione S-transferase class M1 GSTT1: Glutathione S-transferase class T1
H1 receptors Histamine receptors type 1
HLA Human Leukocyte Antigen
IM Intermediate metabolizer
MAO Monoamine oxidase
MAT Monoamine transporter
NSAIDs Nonsteroidal anti-inflammatory drugs
OPRM1 Opioid receptor μ
RAMP1 Receptor activity-modifying protein 1
SERT (5-HTT) Serotonin (5-HT) transporter
SNRIs Serotonin–norepinephrine reuptake inhibitors
TCAs Tricyclic antidepressants
UGT Uridine 5′-diphospho-glucuronosyltransferase (UDP-glucuronosyltransferase)
Keywords: pharmacogenetics, migraine, cluster headache (CH), tension-type headache, drug treatment, pharmacokinetics, pharmacodynamics
Citation: Belyaeva II, Subbotina AG, Eremenko II, Tarasov VV, Chubarev VN, Schiöth HB and Mwinyi J (2022) Pharmacogenetics in Primary Headache Disorders. Front. Pharmacol. 12:820214. doi: 10.3389/fphar.2021.820214
Received: 22 November 2021; Accepted: 23 December 2021;
Published: 10 February 2022.
Edited by:
Alessio Squassina, University of Cagliari, ItalyReviewed by:
Paolo Martelletti, Sapienza University of Rome, ItalyFélix Javier Jiménez-Jiménez, Hospital Universitario del Sureste, Spain
Copyright © 2022 Belyaeva, Subbotina, Eremenko, Tarasov, Chubarev, Schiöth and Mwinyi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica Mwinyi, SmVzc2ljYS5Nd2lueWlAbmV1cm8udXUuc2U=