 Wan-Tong Zhang1†
Wan-Tong Zhang1† Xu-Jie Wang1†
Xu-Jie Wang1† Chun-Miao Xue2†Xin-Yu Ji3Lin Pan2Wei-Liang Weng1,4
Chun-Miao Xue2†Xin-Yu Ji3Lin Pan2Wei-Liang Weng1,4 Qiu-Yan Li1,4*Guo-Dong Hua2*
Qiu-Yan Li1,4*Guo-Dong Hua2* Bao-Chen Zhu2*
Bao-Chen Zhu2*- 1Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, China
- 2Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, China
- 3Institute of Basic Research in Clinical Medicine, China Academy of Chinese Medical Sciences, Beijing, China
- 4National Clinical Research Center for Chinese Medicine Cardiology, Beijing, China
Background: Multiple studies have revealed that idiopathic pulmonary fibrosis (IPF) patients are more at risk for cardiovascular diseases and that many IPF patients receive cardiovascular medications like statins, angiotensin-converting enzyme inhibitor (ACEI), angiotensin receptor blocker (ARB), and anticoagulants. Existing studies have reported divergent findings on the link between cardiovascular medications and fibrotic disease processes. The aim of this study is to synthesize the evidence on the efficacy of cardiovascular medications in IPF.
Methods: We searched studies reporting the effect of cardiovascular medications on IPF in the PubMed, Embase, Web of Science, Cochrane Library, and two Chinese databases (China National Knowledge Infrastructure database and China Wanfang database). We calculated survival data, forced vital capacity (FVC) decline, and IPF-related mortality to assess the efficacy of cardiovascular medications in IPF. We also estimated statistical heterogeneity by using I2 and Cochran Q tests, and publication bias was evaluated by risk of bias tools ROBINS-I.
Results: A total of 12 studies were included in the analysis. The included studies had moderate-to-serious risk of bias. Statin use was associated with a reduction in mortality (hazard ratio (HR), 0.89; 95% CI 0.83–0.97). Meta-analysis did not demonstrate any significant relationship between statin use and the FVC decline (HR, 0.86; 95% CI 0.73–1.02), ACEI/ARB use, and survival data (HR, 0.92; 95% CI 0.73–1.15) as well as anticoagulant use and survival data (HR, 1.16; 95% CI 0.62–2.19).
Conclusion: Our study suggested that there is a consistent relationship between statin therapy and survival data in IPF population. However, there is currently insufficient evidence to conclude the effect of ACEI, ARB, and anticoagulant therapy on IPF population especially to the disease-related outcomes in IPF.
Introduction
Idiopathic pulmonary fibrosis (IPF) is a specific form of interstitial lung disease (ILD) (Raghu et al., 2011), characterized by progressive decline in lung function, worsening dyspnea, and impaired health-related quality of life. It generally progresses relentlessly and carries the poorest prognosis of the chronic idiopathic interstitial pneumonias, with a median survival of 3–5 years (Bjoraker et al., 1998). The pathogenesis of IPF is poorly understood. It is hypothesized that alveolar epithelial cell injury triggers release of cytokines such as transforming growth factor beta 1 (TGF-β1), platelet-derived growth factor (PDGF), and tumor necrosis factor (TNF) α. Cardiovascular diseases (Hyldgaard et al., 2014) are common comorbidities in patients with IPF, and many patients with IPF are receiving medications to reduce cardiovascular risk such as statins, anti-hypotentive agents, and anticoagulants. Statins are well known for its lipid-lowering properties through inhibition of 3-hydroxy-3-methylglutaryl coenzyme-A (HMG-CoA) reductase (LaRosa et al., 1999). In vitro study on lung fibroblasts showed that simvastatin can inhibit the induction of collagen production by TGF-β (Oka et al., 2013). In vivo study showed that simvastatin treatment severely reduced fibrosis, bronchiole adventitial collagen, and bronchiole epithelium (Kruzliak et al., 2015). Angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) are widely used in the management of cardiovascular diseases and systemic hypertension (Chobanian et al., 2003). ACEI inhibits angiotensin I from converting to angiotensin II by inhibiting the activity of angiotensin converting enzyme, thus promoting vasodilation through the kallikrein–kinin system (KKS) to achieve the purpose of lowering blood pressure (Turner and Kodali, 2020). ARB directly inhibits the binding of angiotensin II type 1 receptor (AT1) with angiotensin II receptor (Piepho, 2000). In an in vitro study, ACEI has potential anti-pulmonary fibrosis effect by inhibiting apoptosis of human lung epithelial cells (Uhal et al., 1998). An in vivo study has proven that ACEI can alleviate focal alveolar lesions, alleviate lung inflammation and pulmonary fibrosis, and improve the survival rate of pulmonary fibrosis rats (Gao et al., 2013; Molteni et al., 2007). Anticoagulants are commonly used to combat thrombotic disorders such as atrial fibrillation and strokes. Recent studies have shown a systemic prothrombotic state in people with IPF (Navaratnam et al., 2014). Several researches with large datasets from different populations reveal an increased risk of vascular events in IPF patients (Hubbard et al., 2008; Sode et al., 2010; Sprunger et al., 2012; Schulman and Crowther, 2012). Also, coagulant and plasminergic proteases are likely to have fibrotic actions, which involve cell-mediated responses via receptors (e.g., PARs and uPAR) and coreceptors (e.g., integrins) (Schuliga, et al., 2018). Based on the above studies, it is thought that there may be a potential benefit to the use of anticoagulants in patients with IPF. There is increasing awareness that the broader pharmacologic properties of statins, ACEI, ARB, and anticoagulants encompass the abilities to modulate local fibroproliferative pathways in a variety of organ systems or prolong the survival of IPF patients.
Existing studies have reported divergent findings on the link between medications used for cardiovascular diseases and fibrotic disease processes. The potential effect of these medications in interstitial fibrosis remains unclear. IPF remains a progressive disease, and new antifibrotic therapies do not reverse existing fibrosis. To address this knowledge gap, we conducted a systematic review and meta-analysis of all medications used in cardiovascular diseases to evaluate their relative efficacy and safety for IPF. Therefore, evaluating the effect of the potential adjuvant therapy may offer new approaches in the management of IPF.
Methods
Our systematic review and meta-analysis was conducted under the Cochrane Handbook (Higgins et al., 2020). Reporting was consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Guise et al., 2017).
Search Strategy
We systematically searched PubMed, Embase, Web of Science, Cochrane Library (Cochrane Central Register of Controlled Trials), and two Chinese databases (China National Knowledge Infrastructure database and China Wanfang database) to identify non-randomized studies of cardiovascular medications for IPF published from January 2000 to July 2021, with no language restriction. The full search strategy was employed using combinations of MeSH terms and text words around “statin,” “hydroxymethylglutaryl-CoA reductase inhibitors,” “ACEI,” “angiotensin-converting enzyme inhibitors,” “angiotensin converting enzyme inhibitors,” “ARB,” “angiotensin receptor antagonists,” “angiotensin receptor blockers,” “anticoagulants,” “anticoagulant drugs,” “idiopathic pulmonary fibrosis,” “IPF,” “pulmonary fibroses,” “non-randomised studies,” “retrospective studies,” “prospective studies,” “cohort studies,” “case-control studies,” and “clinical trial.” Additional studies were derived from screening the reference lists of included non-randomized studies and previous systematic reviews.
Eligibility Criteria
We included the studies with the following criteria: 1) they included participants with diagnosis of IPF; 2) intervention involving any form of statins, ACEI, ARB, and anticoagulants; 3) controls including placebo or other IPF therapy; and 4) reporting disease-related outcomes including mortality and pulmonary function.
Data Extraction
Two independent authors (W-TZ and B-CZ) assessed all studies for eligibility, extracted the data, and assessed study quality. Disagreements were resolved by consensus-based discussion. The full-text articles were downloaded, and the same inclusion criteria were used to decide whether to include or exclude articles. Each reviewer carried out the quality assessment of each selected article, assessed the completeness of the data extraction, and confirmed the quality rating to reduce bias independently.
Quality Assessment
Three authors (W-TZ, B-CZ, and X-JW) evaluated all the included studies. Any disagreement was solved through discussion and rechecking of the article. For the included studies, the Cochrane risk of bias tool ROBINS-I was used to assess the risk of bias (Sterne et al., 2016), including 1) confounding, 2) selection of participants into the study, 3) classification of interventions, 4) intended intervention, 5) missing data, 6) measurement of outcomes, and 7) selection of the reported results and other possible sources of bias. In this way, all articles selected for inclusion in the review were graded under the categories of low, moderate, serious, critical, or no information risk of bias.
Data Synthesis
Primary outcome measurements of survival data were performed. Since survival data include survival outcomes such as survival rate, mortality, censoring, and survival time, we merged the survival data in the meta-analysis. Secondary outcomes were forced vital capacity (FVC) decline and IPF-related mortality. Where more than one study reported the same outcome measured in similar way, a meta-analysis was undertaken. Alternatively, a narrative synthesis of the findings was conducted. For meta-analysis, we calculated a hazard ratio (HR) and 95% CIs using a fixed-effects model. Heterogeneity of included studies was quantified using the chi-squared test (Q test) and I2 statistic. We used RevMan software for statistical analysis.
Results
Study Selection and Characteristics of the Included Studies
We initially identified 2,270 potentially relevant publications through database searches and other sources. After deleting 313 duplicate articles, we screened the titles and abstracts of 43 related articles. Thirty-five articles were selected for full-text review. Ultimately, 12 studies met our inclusion criteria and were included for the final analysis (Figure 1). The characteristics of studies included in the systematic review and meta-analysis are shown in Table 1.
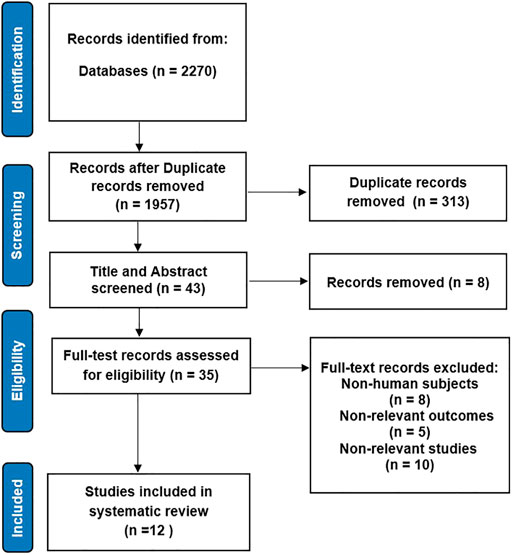
FIGURE 1. Flowchart.
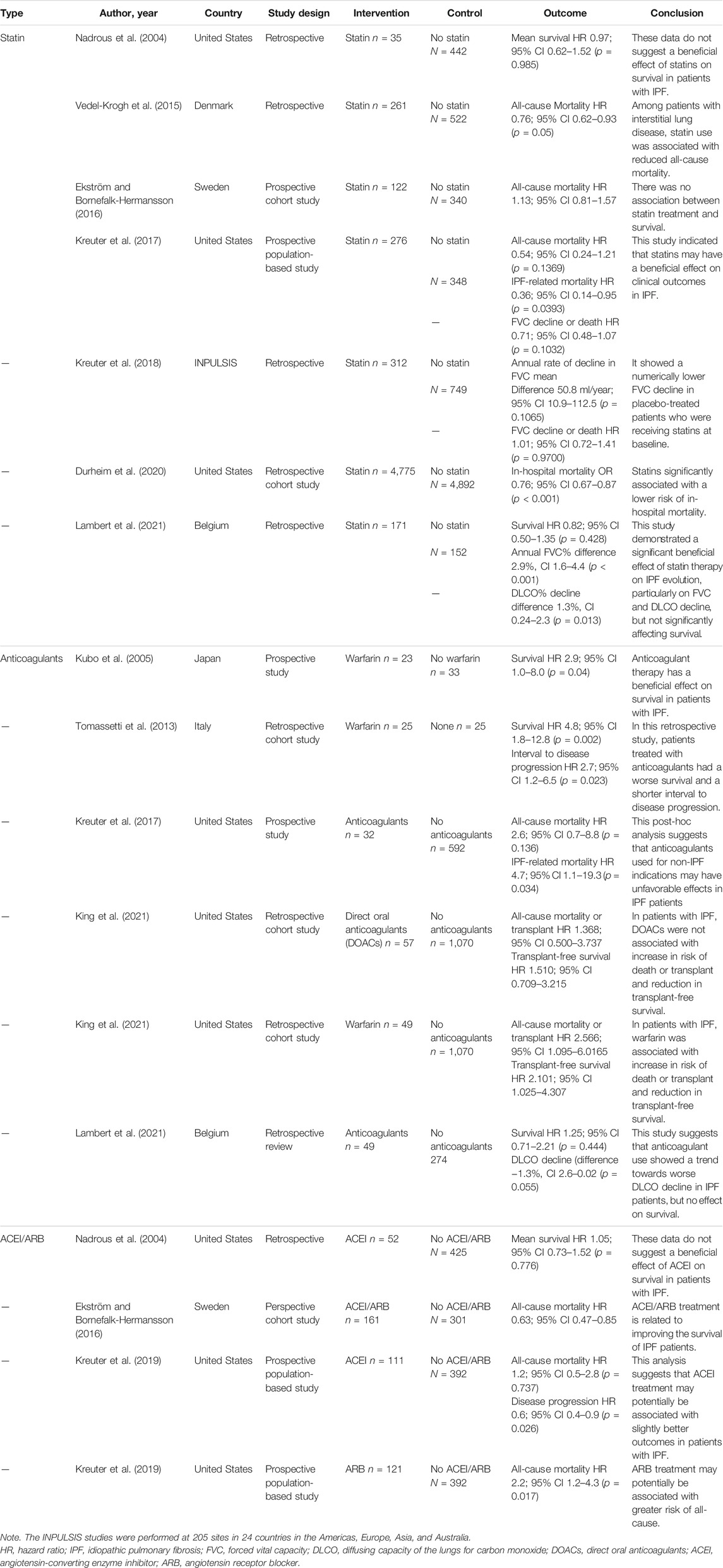
TABLE 1. Characteristics of the included studies.
Risk of Bias
A total of 12 non-randomized studies were included in this study, of which seven were retrospective studies and five were prospective studies. The above studies were reasonable for non-randomized studies, but none of them could achieve the quality of well-implemented randomized trials. Therefore, the overall bias was assessed as moderate-to-serious risk (Figure 2). The lack of diagnostic criteria for IPF in a prospective cohort study (Ekström and Bornefalk-Hermansson, 2016) based on the National Swedevox Register, where approximately 80% of the patients had IPF, assessed the bias in selection of participants as high risk. One retrospective cohort study (Durheim Michael T, 2020) had data from 740 hospitals in the United States, but the data registration information was not stated in the article, so the bias due to missing data was assessed as moderate risk. Although five studies (Nadrous Hassan F, 2004; Durheim Michael T, 2020; M Lambert Eline, 2021; Kubo et al., 2005; Tomassetti S, 2013) had no indications for selective reporting, they lacked evidence support such as prior registration information or data analysis plan, so their bias in selection of the reported result was assessed as a moderate risk of bias.
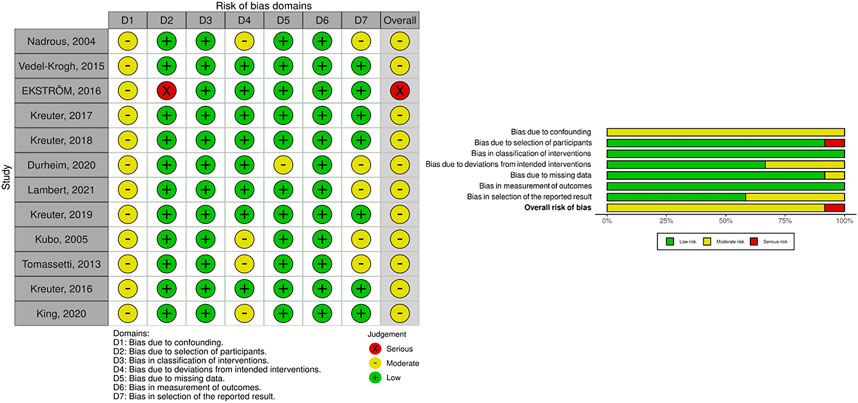
FIGURE 2. Risk of bias graph.
Meta-Analysis Result of Statin
Of seven included statin studies, six studies reported the survival data. In the fixed-effects meta-analysis, statin use was associated with a reduction in mortality (HR, 0.89; 95% CI 0.83–0.97) (Figure 3A).
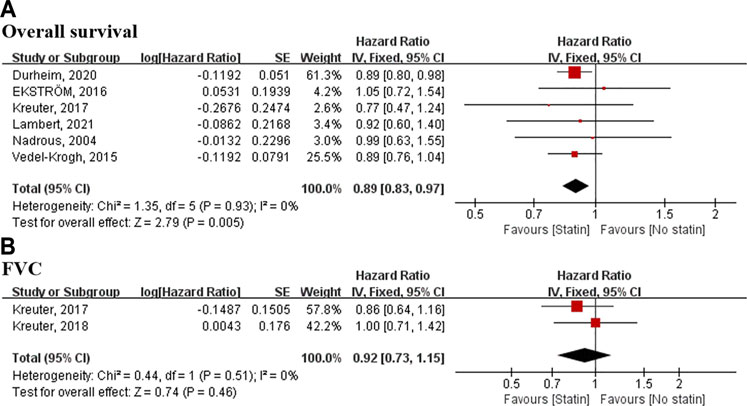
FIGURE 3. Meta-analyses of the included studies examining overall survival and FVC for statin vs. no statin. The marker size indicates the relative weight of the study, as it contributes to the results of the overall comparison. IV indicates inverse-variance random-effects analysis; HR, hazard ratio; FVC, forced vital capacity.
Two studies involving 1,685 patients reported on a composite measure of FVC decline of >10% or death. The meta-analysis did not demonstrate any significant relationship between statin use and the composite outcome (HR, 0.86; 95% CI 0.73–1.02) (Figure 3B).
Meta-Analysis Result of Angiotensin-Converting Enzyme Inhibitor/Angiotensin Receptor Blocker
Four studies involving 1,955 patients reported a relationship between ACEI/ARB use and survival data. The meta-analysis did not demonstrate any significant relationship between ACEI/ARB use and survival data (HR, 0.92; 95% CI 0.73–1.15) (Figure 4).
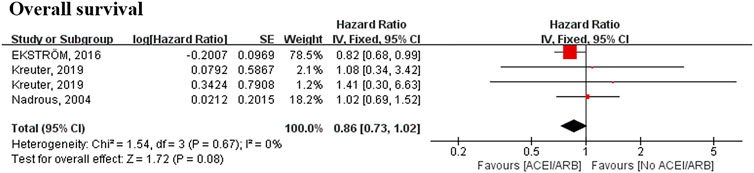
FIGURE 4. Meta-analyses of the included studies examining overall survival for ACEI/ARB vs. no ACEI/ARB. The marker size indicates the relative weight of the study, as it contributes to the results of the overall comparison. IV indicates inverse-variance random-effects analysis; HR, hazard ratio; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker.
Meta-Analysis Result of Anticoagulants
Six studies involving 2,172 patients reported a relationship between anticoagulant use and survival data. Although the meta-analysis did not demonstrate any significant relationship between anticoagulant use and survival data (HR, 1.16; 95% CI 0.62–2.19) (Figure 5), five of six studies included in the meta-analysis showed that patients given anticoagulant medication remained at increased risk of mortality.
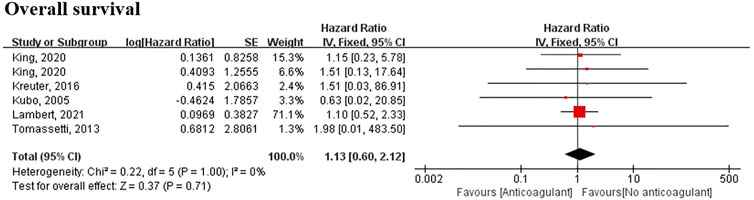
FIGURE 5. Meta-analyses of the included studies examining overall survival for anticoagulant vs. no anticoagulant. The marker size indicates the relative weight of the study, as it contributes to the results of the overall comparison. IV indicates inverse-variance random-effects analysis; HR, hazard ratio.
Discussion
IPF is defined as a chronic, progressive, fibrosing ILD of unknown etiology. Multiple studies have revealed associated pulmonary as well as extra-pulmonary comorbidities (Buendía-Rold´an et al., 2017). Likewise, patients are more at risk for cardiovascular disorders such as ischemic heart disease, atrial fibrillation, and thrombotic vascular events. To reduce their cardiovascular risk, many IPF patients receive cardiovascular medications like statins, ACEI, ARB, and anticoagulants (Hubbard, et al., 2008). Existing studies have reported divergent findings on the link between medications used for cardiovascular diseases and fibrotic disease processes. Given the increasing awareness that pharmacologic properties of statins, ACEI, ARB, and anticoagulants encompass the abilities to modulate fibroproliferative pathways, therefore, identifying the treatment with the best safety and efficacy is important. This systematic review and meta-analysis including 12 non-randomized studies, covering four types of cardiovascular medications, aimed to evaluate the relationship between cardiovascular medications and IPF. To the best of our knowledge, this is currently the first systematic review and meta-analysis investigating different types of cardiovascular medications for IPF. Our study suggested a consistent relationship between statin therapy and all-cause mortality in IPF population. There was no statistically significant association between ACEI/ARB use and decline in FVC. Meanwhile, although the meta-analysis did not demonstrate any significant relationship between anticoagulant use and survival data, we found that all the six studies related to survival data showed the result that patients given anticoagulant medication remained at increased risk of mortality.
Regarding the statin use in IPF patients, of seven included studies, five studies reported survival analysis, through which three studies suggested a beneficial effect of statins on survival. One study reported IPF-related mortality, which suggested that statin use at baseline significantly reduced chance of IPF-related death. Two studies reported on a composite measure of FVC decline of >10% or death with no statistically difference. Regarding the ACEI/ARB use in IPF patients, of four included studies, only one study suggested that ACEI/ARB treatment is related to improving the survival of IPF patients, same with the result of meta-analysis. Regarding the anticoagulant use in IPF patients, of six included studies, only one study suggested that warfarin has a beneficial effect on survival in patients with IPF. Interestingly, others all indicated that patients treated with anticoagulants had a worse survival. Above all, we found that among the cardiovascular medications, only statin was beneficial to survival data of IPF patients. However, since only one study reported IPF-related death, we could not specify the true pharmacological action on IPF clearly. More studies focused on the outcome of IPF-related death should be conducted in the future.
This study has some limitations. Firstly, we concentrated our research on published literatures and did not screen gray literature. This is because the use of the risk of bias tools ROBINS-I requires very explicit and comprehensive reporting of the primary research study. Secondly, most studies used all-cause mortality and survival rate but not IPF-related death as their primary outcomes. So the causes of death were missing in the majority of studies. Thirdly, all studies included are non-randomized, and half of the studies are retrospective. Therefore, there exists some bias due to missing data and confounding that cannot be avoided. Given these challenges, larger-scale samples and higher-quality studies are needed in the future to draw conclusions about the exact causal relationship between survival data of IPF and cardiovascular medications.
Nevertheless, a crucial strength of the present study lies in the large number of included patients and full analysis of the relationship between different types of cardiovascular medications and survival data. Lastly, we would like to propose two suggestions for future clinical trials especially randomized controlled trials (RCTs) of cardiovascular medications for IPF. The combination, especially with antifibrotic drugs, could maximize the treatment effects of cardiovascular medications, but the majority of included trials were not clarified. If the included patients are grouped according to different antifibrotic treatments or non-antifibrotic treatments, then we can then classify and synthesize the outcome data as different types of syndromes in the systematic review, and the analyzed results can provide more pointed guidance for clinical practice. On the other hand, the quality of life of patients was not reported in most of the included studies. As IPF is defined as a chronic, progressive ILD, the multidimensional quality of life is an indispensable indicator and evaluation tool to show the trend of treatment effectiveness. We suggested that future prospective trials should be improved in related fields.
Conclusion
Our study suggested a consistent relationship between statin therapy and survival data in IPF population. However, there is currently insufficient evidence to conclude the effect of ACEI, ARB, and anticoagulant therapy on IPF population especially to the disease-related outcomes in IPF. Considering the limitations of available literature, we would recommend a prospective RCT or cohort study that captures IPF-related outcomes of cardiovascular medications and use of concurrent antifibrotic treatment.
Author Contributions
All authors were involved in the review, interpretation of the results, and manuscript preparation. W-TZ, Q-YL, and C-MX conceived and designed the study. W-TZ and X-JW drafted the report. X-JW and B-CZ did the data analysis. W-TZ, X-JW, C-MX, X-YJ, LP, W-LW, Q-YL, G-DH, and B-CZ revised the report and approved the final version before submission.
Funding
This study was supported by National Natural Science Foundation of China (No. 82004352), National Natural Science Foundation of China (No. 82004125), and Academic Inheritance studio of Professor W-LW.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bjoraker, J. A., Ryu, J. H., Edwin, M. K., Myers, J. L., Tazelaar, H. D., Schroeder, D. R., et al. (1998). Prognostic Significance of Histopathologic Subsets in Idiopathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 157 (1), 199–203. doi:10.1164/ajrccm.157.1.9704130
Buendía-Roldán, I., Mejía, M., Navarro, C., and Selman, M. (2017). Idiopathic Pulmonary Fibrosis: Clinical Behavior and Aging Associated Comorbidities. Respir. Med. 129, 46–52. doi:10.1016/j.rmed.2017.06.001
Chobanian, A. V., Bakris, G. L., Black, H. R., Cushman, W. C., Green, L. A., Izzo, J. L., et al. (2003). The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 Report. JAMA 289 (19), 2560–2572. doi:10.1001/jama.289.19.2560
Durheim, M. T., Judy, J., Bender, S., Neely, M. L., Baumer, D., Robinson, S. B., et al. (2020). A Retrospective Study of In-Hospital Mortality in Patients with Idiopathic Pulmonary Fibrosis between 2015 and 2018. Medicine (Baltimore) 99 (47), e23143. doi:10.1097/MD.0000000000023143
Ekström, M., and Bornefalk-Hermansson, A. (2016). Cardiovascular and Antacid Treatment and Mortality in Oxygen-dependent Pulmonary Fibrosis: A Population-Based Longitudinal Study. Respirology 21 (4), 705–711. doi:10.1111/resp.12781
Gao, F., Fish, B. L., Moulder, J. E., Jacobs, E. R., and Medhora, M. (2013). Enalapril Mitigates Radiation-Induced Pneumonitis and Pulmonary Fibrosis if Started 35 Days after Whole-Thorax Irradiation. Radiat. Res. 180 (5), 546–552. doi:10.1667/RR13350.1
Guise, J. M., Butler, M. E., Chang, C., Viswanathan, M., Pigott, T., Tugwell, P., et al. (2017). AHRQ Series on Complex Intervention Systematic Reviews-Paper 6: PRISMA-CI Extension Statement and Checklist. J. Clin. Epidemiol. 90 (undefined), 43–50. doi:10.1016/j.jclinepi.2017.06.016
Hubbard, R. B., Smith, C., Le Jeune, I., Gribbin, J., and Fogarty, A. W. (2008). The Association between Idiopathic Pulmonary Fibrosis and Vascular Disease: a Population-Based Study. Am. J. Respir. Crit. Care Med. 178 (12), 1257–1261. doi:10.1164/rccm.200805-725OC
Hyldgaard, C., Hilberg, O., and Bendstrup, E. (2014). How Does Comorbidity Influence Survival in Idiopathic Pulmonary Fibrosis? Respir. Med. 108 (4), 647–653. doi:10.1016/j.rmed.2014.01.008
version 6.1 (updated September 2020) J. P. T. Higgins, J. Thomas, J. Chandler, M. Cumpston, T. Li, M. J. Pageet al. (Editors) (2020). Cochrane Handbook for Systematic Reviews of Interventions (Cochrane. Available from www.training.cochrane.org/handbook.
King, C. S., Freiheit, E., Brown, A. W., Shlobin, O. A., Aryal, S., Ahmad, K., et al. (2021). Association between Anticoagulation and Survival in Interstitial Lung Disease: An Analysis of the Pulmonary Fibrosis Foundation Patient Registry. Chest 159 (4), 1507–1516. doi:10.1016/j.chest.2020.10.019
Kreuter, M., Bonella, F., Maher, T. M., Costabel, U., Spagnolo, P., Weycker, D., et al. (2017). Effect of Statins on Disease-Related Outcomes in Patients with Idiopathic Pulmonary Fibrosis. Thorax 72 (2), 148–153. doi:10.1136/thoraxjnl-2016-208819
Kreuter, M., Costabel, U., Richeldi, L., Cottin, V., Wijsenbeek, M., Bonella, F., et al. (2018). Statin Therapy and Outcomes in Trials of Nintedanib in Idiopathic Pulmonary Fibrosis. Respiration 95 (5), 317–326. doi:10.1159/000486286
Kreuter, M., Lederer, D. J., Molina-Molina, M., Noth, I., Valenzuela, C., Frankenstein, L., et al. (2019). Association of Angiotensin Modulators with the Course of Idiopathic Pulmonary Fibrosis. Chest 156 (4), 706–714. doi:10.1016/j.chest.2019.04.015
Kruzliak, P., Hare, D. L., Zvonicek, V., Klimas, J., and Zulli, A. (2015). Simvastatin Impairs the Induction of Pulmonary Fibrosis Caused by a Western Style Diet: a Preliminary Study. J. Cel Mol Med 19 (11), 2647–2654. doi:10.1111/jcmm.12637
Kubo, H., Nakayama, K., Yanai, M., Suzuki, T., Yamaya, M., Watanabe, M., et al. (2005). Anticoagulant Therapy for Idiopathic Pulmonary Fibrosis. Chest 128 (3), 1475–1482. doi:10.1378/chest.128.3.1475
Lambert, M. E., Wuyts, W. A., Yserbyt, J., and De Sadeleer, L. J. (2021). Statins: Cause of Fibrosis or the Opposite? Effect of Cardiovascular Drugs in Idiopathic Pulmonary Fibrosis. Respir. Med. 176 (undefined), 106259. doi:10.1016/j.rmed.2020.106259
LaRosa, J. C., He, J., and Vupputuri, S. (1999). Effect of Statins on Risk of Coronary Disease: a Meta-Analysis of Randomized Controlled Trials. JAMA 282 (24), 2340–2346. doi:10.1001/jama.282.24.2340
Molteni, A., Wolfe, L. F., Ward, W. F., Ts'ao, C. H., Molteni, L. B., Veno, P., et al. (2007). Effect of an Angiotensin II Receptor Blocker and Two Angiotensin Converting Enzyme Inhibitors on Transforming Growth Factor-Beta (TGF-Beta) and Alpha-Actomyosin (Alpha SMA), Important Mediators of Radiation-Induced Pneumopathy and Lung Fibrosis. Curr. Pharm. Des. 13 (13), 1307–1316. doi:10.2174/138161207780618777
Nadrous, H. .F., Ryu, J. H., Douglas, W. W., Decker, P. A., and Olson, E. J. (2004). Impact of Angiotensin-Converting Enzyme Inhibitors and Statins on Survival in Idiopathic Pulmonary Fibrosis. Chest 126 (2), 438–446. doi:10.1378/chest.126.2.438
Navaratnam, V., Fogarty, A. W., McKeever, T., Thompson, N., Jenkins, G., Johnson, S. R., et al. (2014). Presence of a Prothrombotic State in People with Idiopathic Pulmonary Fibrosis: a Population-Based Case-Control Study. Thorax 69 (3), 207–215. doi:10.1136/thoraxjnl-2013-203740
Oka, H., Ishii, H., Iwata, A., Kushima, H., Toba, S., Hashinaga, K., et al. (2013). Inhibitory Effects of Pitavastatin on Fibrogenic Mediator Production by Human Lung Fibroblasts. Life Sci. 93 (null), 968–974. doi:10.1016/j.lfs.2013.10.026
Piepho, R. W. (2000). Overview of the Angiotensin-Converting-Enzyme Inhibitors. Am. J. Health Syst. Pharm. 57 Suppl 1 (57 Suppl. 1), S3–S7. doi:10.1093/ajhp/57.suppl_1.S3
Raghu, G., Collard, H. R., Egan, J. J., Martinez, F. J., Behr, J., Brown, K. K., et al. (2011). An Official ATS/ERS/JRS/ALAT Statement: Idiopathic Pulmonary Fibrosis: Evidence-Based Guidelines for Diagnosis and Management. Am. J. Respir. Crit. Care Med. 183 (6), 788–824. doi:10.1164/rccm.2009-040GL
Schuliga, M., Grainge, C., Westall, G., and Knight, D. (2018). Westall Glen., and Knight DarrylThe Fibrogenic Actions of the Coagulant and Plasminogen Activation Systems in Pulmonary Fibrosis. Int. J. Biochem. Cel Biol. 97 (undefined), 108–117. doi:10.1016/j.biocel.2018.02.016
Schulman, S., and Crowther, M. A. (2012). How I Treat with Anticoagulants in 2012: New and Old Anticoagulants, and when and How to Switch. Blood 119 (13), 3016–3023. doi:10.1182/blood-2011-10-378950
Sode, B. F., Dahl, M., Nielsen, S. F., and Nordestgaard, B. G. (2010). Venous Thromboembolism and Risk of Idiopathic Interstitial Pneumonia: a Nationwide Study. Am. J. Respir. Crit. Care Med. 181 (10), 1085–1092. doi:10.1164/rccm.200912-1951OC
Sprunger, D. B., Olson, A. L., Huie, T. J., Fernandez-Perez, E. R., Fischer, A., Solomon, J. J., et al. (2012). Pulmonary Fibrosis Is Associated with an Elevated Risk of Thromboembolic Disease. Eur. Respir. J. 39 (1), 125–132. doi:10.1183/09031936.00041411
Sterne, J. A., Hernán, M. A., Reeves, B. C., Savović, J., Berkman, N. D., Viswanathan, M., et al. (2016). ROBINS-I: a Tool for Assessing Risk of Bias in Non-randomised Studies of Interventions. BMJ 355 (undefined), i4919. doi:10.1136/bmj.i4919
Tomassetti, S., Ruy, J. H., Gurioli, C., Ravaglia, C., Buccioli, M., Tantalocco, P., et al. (2013). The Effect of Anticoagulant Therapy for Idiopathic Pulmonary Fibrosis in Real Life Practice. Sarcoidosis Vasc. Diffuse Lung Dis. 30 (2), 121–127.
Turner, J. M., and Kodali, R. (2020). Should Angiotensin-Converting Enzyme Inhibitors Ever Be Used for the Management of Hypertension? Curr. Cardiol. Rep. 22 (9), 95. doi:10.1007/s11886-020-01352-8
Uhal, B. D., Gidea, C., Bargout, R., Bifero, A., Ibarra-Sunga, O., Papp, M., et al. (1998). Captopril Inhibits Apoptosis in Human Lung Epithelial Cells: a Potential Antifibrotic Mechanism. Am. J. Physiol. 275 (5), L1013–L1017. doi:10.1152/ajplung.1998.275.5.L1013
Keywords: idiopathic pulmonary fibrosis, ACEI/ARB, statin, anticoagulants, meta-analysis
Citation: Zhang W-T, Wang X-J, Xue C-M, Ji X-Y, Pan L, Weng W-L, Li Q-Y, Hua G-D and Zhu B-C (2021) The Effect of Cardiovascular Medications on Disease-Related Outcomes in Idiopathic Pulmonary Fibrosis: A Systematic Review and Meta-Analysis. Front. Pharmacol. 12:771804. doi: 10.3389/fphar.2021.771804
Received: 07 September 2021; Accepted: 11 October 2021;
Published: 11 November 2021.
Edited by:
Jian Gao, Shanghai Children’s Medical Center, ChinaReviewed by:
Lin Zhu, Second Affiliated Hospital of Tianjin University of Traditional Chinese Medicine, ChinaJun Yang, Changzhou Traditional Chinese Medicine Hospital, China
Copyright © 2021 Zhang, Wang, Xue, Ji, Pan, Weng, Li, Hua and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qiu-Yan Li, bGlxaXV5YW4xOTY4QHNvaHUuY29t; Guo-Dong Hua, emhhb2podWFnZEAxMjYuY29t; Bao-Chen Zhu, emJjYm9jazEyM0BzaW5hLmNvbQ==
†These authors have contributed equally to this work