 Yuanyuan Zhang1Panpan He1Guobao Wang1Min Liang1Di Xie1Jing Nie1Chengzhang Liu2
Yuanyuan Zhang1Panpan He1Guobao Wang1Min Liang1Di Xie1Jing Nie1Chengzhang Liu2 Yun Song3
Yun Song3 Lishun Liu3Binyan Wang2
Lishun Liu3Binyan Wang2 Jianping Li4
Jianping Li4 Yan Zhang4
Yan Zhang4 Xiaobin Wang5
Xiaobin Wang5 Yong Huo4
Yong Huo4 Fan Fan Hou1
Fan Fan Hou1 Xiping Xu1
Xiping Xu1 Xianhui Qin1*
Xianhui Qin1*- 1State Key Laboratory of Organ Failure Research, Guangzhou Regenerative Medicine and Health Guangdong Laboratory, Division of Nephrology, Nanfang Hospital, National Clinical Research Center for Kidney Disease, Guangdong Provincial Institute of Nephrology, Guangdong Provincial Clinical Research Center for Kidney Disease, Guangdong Provincial Key Laboratory of Renal Failure Research, Southern Medical University, Guangzhou, China
- 2Institute of Biomedicine, Anhui Medical University, Hefei, China
- 3Beijing Advanced Innovation Center for Food Nutrition and Human Health, College of Food Science and Nutritional Engineering, China Agricultural University, Beijing, China
- 4Department of Cardiology, Peking University First Hospital, Beijing, China
- 5Department of Population, Family and Reproductive Health, Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD, United States
The relation of alkaline phosphatase (ALP) with chronic kidney disease (CKD) is still uncertain. We aimed to examine the prospective association between serum ALP and CKD progression, and the modifying effect of serum ALP on folic acid in preventing CKD progression in treated hypertensive patients. This is a post-hoc analysis of 12,734 hypertensive adults with relevant measurements and without liver disease at baseline from the renal sub-study of the China Stroke Primary Prevention Trial, where participants were randomly assigned to daily treatments of 10 mg enalapril and 0.8 mg folic acid, or 10 mg enalapril alone. The primary outcome was CKD progression, defined as a decrease in estimated glomerular filtration rate (eGFR) of ≥30% and to a level of <60 ml/min/1.73 m2 if baseline eGFR was ≥60 ml/min/1.73 m2; or a decrease in eGFR of ≥50% if baseline eGFR was <60 ml/min/1.73 m2; or end-stage renal disease. Over a median of 4.4 years, in the enalapril only group, participants with baseline serum ALP≥110IU/L (quartile 4) had a significantly higher risk of CKD progression (3.4% vs 2.3%; adjusted OR,1.61; 95%CI:1.11, 2.32), compared with those with ALP<110IU/L. For those with enalapril and folic acid treatment, compared with the enalapril only treatment, the risk of CKD progression was reduced from 3.4 to 2.1% (adjusted OR, 0.53; 95%CI:0.34, 0.83) among participants with baseline ALP≥110IU/L, whereas there was no significant effect among those with ALP<110IU/L. In hypertensive patients, higher serum ALP was associated with increased risk of CKD progression, and this risk was reduced by 47% with folic acid treatment.
Introduction
Chronic kidney disease (CKD) is a global public health problem, affecting more than 500 million people worldwide (Chen et al., 2019). CKD is independently associated with end-stage renal disease (ESRD), cardiovascular disease (CVD), and all-cause mortality (Go et al., 2004; Coresh et al., 2014; Tanaka et al., 2017), and leads to high health care costs (Jha et al., 2013). It is therefore important to identify more risk factors of CKD that would reduce the public health burden and serious clinical consequences by leading to early detection and prevention.
Previous studies have found an obvious association between liver and renal disease, and suggested that liver damage and CKD may share some common mechanisms, such as oxidative stress and inflammation (Contreras et al., 2007; Er et al., 2020; Sansoè et al., 2020). Alkaline phosphatase (ALP) is a generally accepted clinical useful marker for liver and bone disease (Harmey et al., 2004). It has been reported that ALP is an important risk factor for cardiovascular diseases (CVD) and mortality (Park et al., 2013; Kunutsor et al., 2014; Kabootari et al., 2018), owing to its role in endothelial dysfunction, inflammation, and oxidative stress (Haarhaus et al., 2017). Moreover, the serum ALP levels are commonly elevated in CKD and dialysis patients (Damera et al., 2011). Due to the similar involved mechanisms and the increased ALP levels in CKD patients, we speculate that ALP may also play an important role in the development of CKD. However, few prospective studies have examined the possible relation of ALP and the development of CKD in the general population.
Furthermore, in a previous study, we reported that folic acid treatment can delay the progression of CKD by 55% among hypertensive patients with CKD (Xu et al., 2016). Given that folic acid, in addition to having antioxidant and anti-inflammatory properties, can directly improve endothelial function (Title et al., 2000; Joshi et al., 2001; Solini et al., 2006; Spence et al., 2017), it is biologically plausible that folic acid treatment may counteract the possible detrimental effects of elevated ALP on CKD. However, this hypothesis has not been tested in previous studies.
Our current report was motivated by the limited data regarding the ALP and incident CKD, and an exceptional opportunity to address this question in a large, randomized controlled folic acid intervention trial with regular antihypertensive treatments, BP measurements and CKD status reports. Specifically, using data from the renal sub-study of the China Stroke Primary Prevention Trial (CSPPT) (Xu et al., 2016), we sought to investigate the effect of serum ALP on the risk of CKD progression and on the efficacy of folic acid treatment in prevention of CKD progression in general hypertensive adults.
Materials and Methods
Study Design and Participants
Details regarding the study design, methods, and major results of the CSPPT (ClinicalTrials.gov identifier NCT00794885) (Qin et al., 2013; Huo et al., 2015; Qin et al., 2017a; Qin et al., 2017b) and the renal sub-study of the CSPPT (Xu et al., 2016) have been reported previously. Briefly, the CSPPT was a multi-community, randomized, double-blind, controlled trial conducted from May 2008 to August 2013 in 32 communities in Anhui and Jiangsu provinces in China. Eligible participants were men and women aged 45–75 years who had hypertension, defined as seated, resting systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg at both the screening and recruitment visit, or who were on anti-hypertensive medication. The major exclusion criteria included history of physician-diagnosed stroke, myocardial infarction, heart failure, post-coronary revascularization, and/or congenital heart disease, and/or current supplementation by folic acid, vitamin B12 or vitamin B6.
In the CSPPT, a total of 20,702 eligible participants were enrolled. The renal sub-study of the CSPPT included 15,104 participants from 20 communities in Jiangsu province with an estimated glomerular filtration rate (eGFR) ≥30 ml/min/1.73 m2. Our current study is a post-hoc analysis of the renal sub-study of the CSPPT, where a total of 12,734 participants with complete relevant measurements and without liver disease (self-reported chronic hepatitis, hepatic adipose infiltration, or cirrhosis) at baseline were included (Supplemental Figure S1).
The parent study (the CSPPT) and the current study were approved by the Ethics Committee of the Institute of Biomedicine, Anhui Medical University, Hefei, China (FWA assurance number: FWA00001263). All participants provided written informed consent.
Intervention and Follow-Up
Eligible participants were randomized to receive a daily oral dose of one tablet containing 10-mg enalapril and 0.8-mg folic acid (single pill combination, the enalapril-folic acid group) or one tablet containing 10-mg enalapril only (the enalapril-only group).
Participants were scheduled for follow-up every 3 months. At each follow-up visit, BP was measured; study drug compliance, concomitant medication use, adverse events and possible endpoint events were documented by trained research staff and physicians.
Laboratory Assessment
Serum and spot urine samples were obtained from each study participant at baseline and at the exit visit. Serum fasting creatinine, ALP, gamma glutamyl transpeptidase (GGT), alanine aminotransferase (ALT), aspartate aminotransferase (AST), total homocysteine (tHcy), uric acid, phosphate, calcium, albumin, lipids and fasting glucose were measured with the use of automatic clinical analyzers (Beckman Coulter) at the core laboratory of the National Clinical Research Center for Kidney Disease, Nanfang Hospital, Guangzhou, China. Estimated GFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (Levey et al., 2009).
Study Outcomes
The primary outcome was CKD progression, defined as a decrease in eGFR ≥30% and to a level <60 ml/min/1.73 m2 at the exit visit if baseline eGFR was ≥60 ml/min/1.73 m2; or a decrease in eGFR ≥50% at the exit visit if baseline eGFR was <60 ml/min/1.73 m2; or end-stage renal disease (eGFR <15 ml/min/1.73 m2 or need for dialysis).
Secondary outcomes included the following: 1) CKD incidence, defined as eGFR ≥60 ml/min/1.73 m2 at baseline, and eGFR <60 ml/min/1.73 m2 at the exit visit; 2) rapid decline in renal function, defined as a decline in eGFR of 40% or more; 3) annual rate of relative decline in eGFR, estimated as (
Statistical Analysis
Baseline characteristics are presented as means ± standard deviations (SDs) and proportions for continuous and categorical variables, respectively. Statistical significance of differences in baseline characteristics was assessed by baseline serum ALP quartiles using ANOVA tests or chi-square tests, accordingly.
Logistic (primary outcome and secondary outcome 1–2) or linear regression (secondary outcome 3) models were performed to estimate the relation of baseline serum ALP levels with the primary and secondary renal outcomes in the enalapril-only group without and with adjustment for major covariates. In addition, the effect modification of baseline serum ALP levels on folic acid efficacy in the primary outcome in the total population (participants from the enalapril-only group and the enalapril-folic acid group) were evaluated both before and after adjustment for major covariates. In addition, the association of folic acid treatment with primary and secondary outcomes across each serum ALP subgroup [≥110 (quartile 4) or <110 IU/L] were estimated and their interactions were assessed.
A two-tailed p < 0.05 was considered statistically significant in all analyses. R software, version 3.6.3 (http://www.R-project.org/) was used to perform all statistical analyses.
Results
Study Participants and Baseline Characteristics
In this study, a total of 12,734 participants (6,389 in the enalapril-only group and 6,345 in the enalapril-folic acid group) with baseline ALP measurements and complete renal outcomes, and without liver disease at baseline, were included in the final analyses (Supplemental Figure S1).
Baseline characteristics of participants in the enalapril-only group by baseline ALP quartiles are presented in Supplemental Table S1. The mean and median serum ALP levels in the enalapril-only group were 95.4 (SD, 28.2) and 92 IU/L, respectively. Participants with higher ALP levels were more likely to be female. Among females, those with higher ALP levels were more likely to be older, had higher SBP, triglycerides (TG), fasting glucose (FG), albumin-corrected calcium and phosphate levels, and a higher prevalence of diabetes and proteinuria; had a lower frequency in use of antihypertensive drugs at baseline, as well as higher time-averaged SBP during the treatment period (Supplemental Table S2). Similar trends were found in males (Supplemental Table S3).
However, almost all population characteristics at baseline, as well as time-averaged BP and concomitant medication usage during the trial were comparable between the 2 treatment groups within each baseline ALP stratum [≥110 (quartile 4) or <110 IU/L] (Table 1).
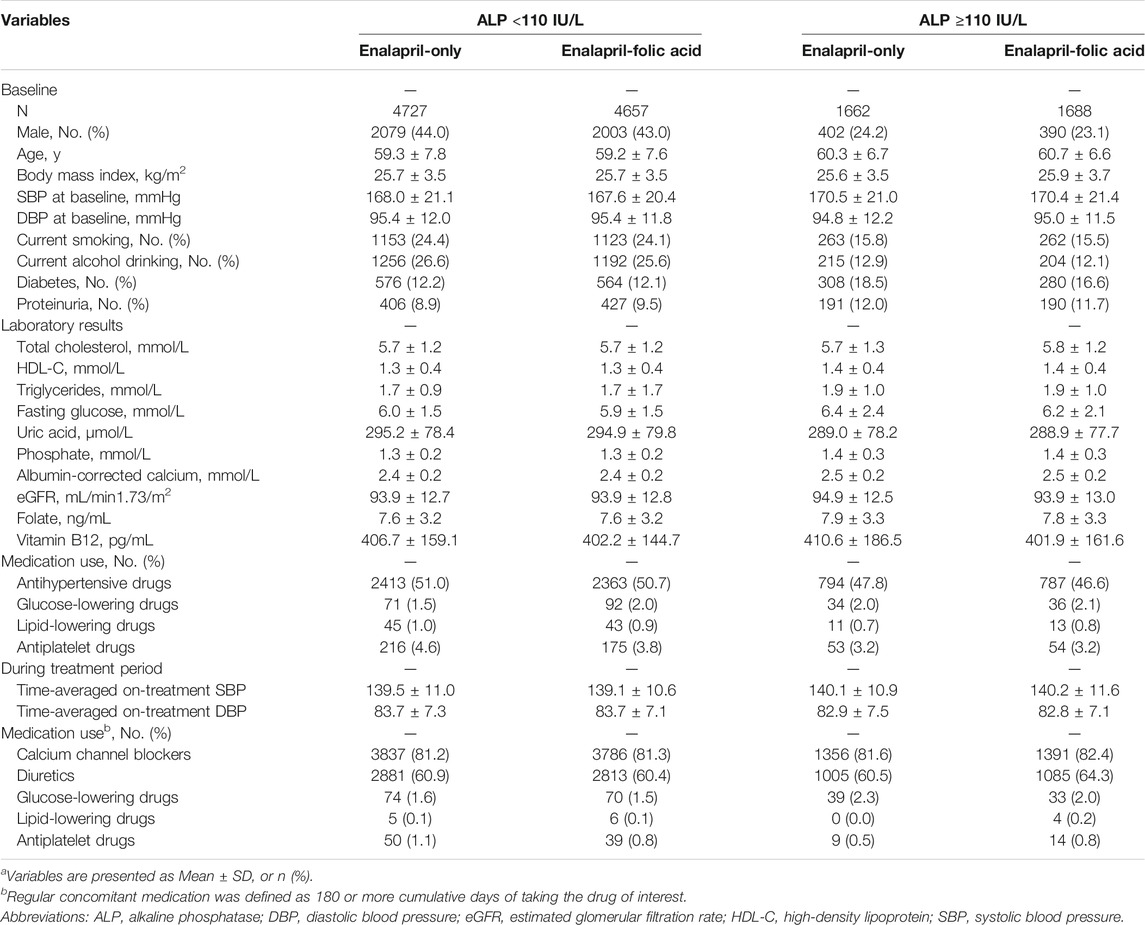
TABLE 1. Characteristics of the study participants by baseline serum ALP strata (<110 and ≥110 IU/L) and treatment groupa.
Baseline Serum Alkaline Phosphatase and the Risk of Renal Outcomes in the Enalapril-Only Group
The median follow-up duration was 4.4 years (interquartile range, 4.0–4.8 years). The relationship of serum ALP with the risk of CKD progression (Figure 1), CKD incidence (Supplemental Figure S2A), rapid decline in renal function (Supplemental Figure S2B) and annual rate of relative decline in eGFR (Supplemental Figure S2C) in the enalapril-only group are presented in Figure 1 and Supplemental Figure S2. When serum ALP was assessed as quartiles, among the enalapril-only group, a significantly higher risk of CKD progression was found in participants in quartile 4 (ALP ≥110 IU/L; 3.4% vs 2.3%; adjusted OR, 1.61; 95% CI: 1.11, 2.32), compared with those in quartile 1–3 (ALP <110 IU/L) (Table 2). Similar trends were found for CKD incidence (ALP ≥110 vs <110 IU/L; adjusted OR, 1.54; 95% CI: 1.11, 2.13), rapid decline in renal function (ALP ≥110 vs <110 IU/L; adjusted OR, 1.39; 95% CI: 0.88, 2.22) and annual rate of relative decline in eGFR (ALP ≥110 vs <110 IU/L; adjusted β, 0.24; 95% CI: 0.04, 0.44) (Table 2).
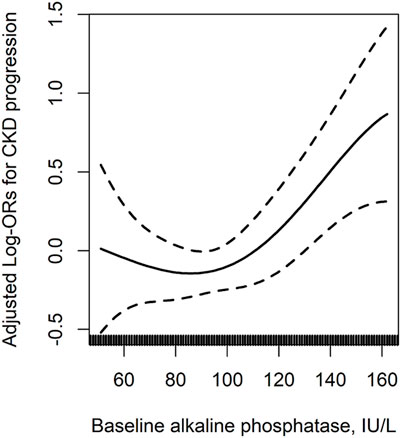
FIGURE 1. The relation of baseline serum alkaline phosphatase with CKD progression in the enalapril-only population*. *Adjusted for age, sex, body mass index, smoking, alcohol drinking, albumin-corrected calcium, phosphate, uric acid, total cholesterol, fasting glucose, eGFR, systolic blood pressure (SBP), proteinuria and antihypertensive drug usage at baseline, as well as time-averaged SBP, the use of calcium channel blockers (CCB) and diuretics during the treatment period. †Only participants with baseline eGFR ≥60 ml/min/1.73 m2 were included in this analysis. AbbreviationsCKD, chronic kidney disease; eGFR, estimated glomerular filtration rate.

TABLE 2. The association between baseline serum alkaline phosphatase and renal outcomes in the enalapril-only treatment group.
In addition, similar results were also found in participants with a normal range of baseline serum ALP (20–140 IU/L) levels (Sharma et al., 2014) in the enalapril-only group (Supplemental Table S4). More importantly, further adjustment for other liver enzymes, including GGT, ALT, AST did not substantially change the results (ALP ≥110 vs <110 IU/L; adjusted OR, 1.67; 95% CI: 1.16, 2.42) (Supplemental Table S5).
Effect of Baseline Serum ALP Levels on the Efficacy of Folic Acid Treatment in Preventing Renal Outcomes Among the Total Population
Among the total participants, compared with the enalapril-only group, for those with folic acid treatment, the risk of CKD progression was reduced from 3.4 to 2.1% (adjusted OR, 0.53; 95%CI: 0.34, 0.83) among participants with baseline serum ALP ≥110 IU/L. In contrast, folic acid treatment had no significant effect on CKD progression in those with baseline serum ALP <110 IU/L (2.0% in the enalapril-folic acid group vs 2.3% in the enalapril-only group; adjusted OR, 0.91; 95% CI: 0.68, 1.22). The interaction between ALP levels and folic acid treatment on CKD progression was significant (p = 0.047) (Table 3).
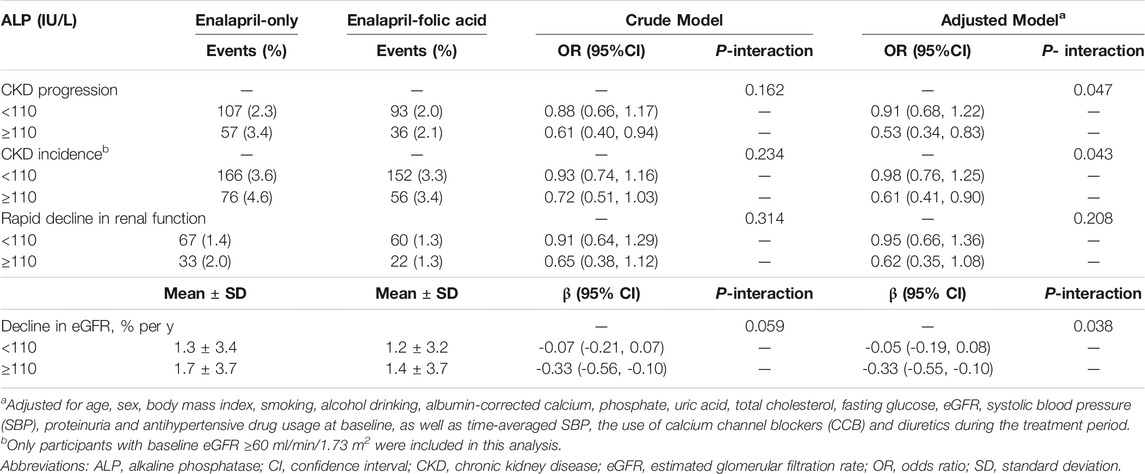
TABLE 3. Effect modification of baseline serum alkaline phosphatase levels (<110 and ≥110 IU/L) on efficacy of enalapril-folic acid treatment in renal outcomes, compared to enalapril-only treatment group.
Similar results were found for CKD incidence, rapid decline in renal function, and annual rate of relative decline in eGFR (Table 3), and in participants with a normal range of serum ALP levels (Supplemental Table S6). Further adjustment for other liver enzymes, (Supplemental Table S7) did not substantially change the results.
Stratified Analyses
In all the subgroups, including sex (male vs female), age (<65 vs ≥65 years), BMI (<24 vs ≥24 kg/m2), SBP (<160 vs ≥160 mmHg), TC (<5.2 vs ≥5.2 mmol/L), tHcy [<12.5 (median) vs ≥12.5 μmol/L], folate [<7.3 (median) vs ≥7.3 ng/ml], vitamin B12 [<370.8 (median) vs ≥370.8 pg/ml], phosphate [<1.3 (median) vs ≥1.3 mmol/L], albumin-corrected calcium [<2.4 (median) vs ≥2.4 mmol/L], FG (<5.6 vs 5.6-<7.0 mmol/L vs diabetes), and CKD (no vs yes) at baseline, as well as time-averaged SBP (<140 vs ≥140 mmHg), diuretics usage (no vs yes) and calcium channel blockers usage (no vs yes) over the trial period, there was a greater beneficial effect of folic acid treatment for participants with higher baseline serum ALP (≥110 IU/L) than for those with lower baseline serum ALP (<110 IU/L) (Supplemental Table S8).
Of note, among those with both CKD and higher serum ALP (≥110 IU/L) at baseline, compared with enalapril alone, enalapril and folic acid treatment was associated with 73% reduction in CKD progression (3.3% in the enalapril-folic acid group vs 10.6% in the enalapril-only group; adjusted OR, 0.27; 95% CI: 0.11, 0.65) (Supplemental Table S8).
Discussion
To our knowledge, this is the first study to examine the prospective association between serum ALP and CKD progression, and the modifying effect of serum ALP on folic acid in preventing CKD progression in treated hypertensive patients. We found that among hypertensive adults, those participants with higher serum ALP had significantly increased risk of CKD progression. More importantly, in participants with higher serum ALP, folic acid treatment significantly reduced the risk of CKD progression by 47 and 73%, respectively, in the total population and in those with CKD at baseline. Our findings are clinically meaningful in term of the magnitude of the CKD progression risk reduction.
Multiple previous studies have reported that ALP is associated with increased risk of mortality in CKD patients, despite whether they were dialysis-dependent (Fan et al., 2017; Zhan et al., 2019) or non-dialysis dependent patient (Taliercio et al., 2013; Sumida et al., 2018). To date, however, only two small studies (Yamazoe et al., 2016; Majoni et al., 2020) have investigated the association between serum ALP and renal outcomes. One study conducted in Japan (Yamazoe et al., 2016), reported that the risk of worsening renal function during hospitalization increased by 69 and 95%, respectively, in patients in ALP tertile 2 (203–278 IU/L) and tertile 3 (>278 IU/L), compared with those in tertile 1 (<203 IU/L), among 972 patients with acute decompensated heart failure, and who were not on hemodialysis or peritoneal dialysis. Of note, this study was performed in patients with acute decompensated heart failure, whose pathophysiology differed from that of the general population. In addition, serum ALP levels in this study were considerably higher (median, 238 IU/L) than that of the current study (median, 92 IU/L). Another recent study (Majoni et al., 2020) including only 547 adults suggested that there was a positive association between serum ALP and increased risk of poor renal outcomes. It is worth noting that the study sample was relative small, and some imported variables such as BP levels or information of medications were not included in the regression models, and therefore could not draw an accurate conclusion.
In contrast to the prior studies, our study provides some new insights in the field. It is by far the first and largest study of its kind demonstrating a positive association between serum ALP and the risk of CKD progression during a treatment period of 4.4 years in general treated hypertensive adults. Moreover, we further found that the increased risk of CKD progression associated with higher serum ALP levels could be significantly reduced by folic acid treatment this risk was reduced by 47% with folic acid treatment.
The exact mechanisms by which higher serum ALP increases the risk of CKD progression, or by which folic acid treatment has higher efficacy on reducing the risk in this subgroup remains to be delineated. However, our findings are biologically plausible based on the available literature. It is well-known that oxidative stress (Coppolino et al., 2018), endothelial dysfunctions (Jourde-Chiche et al., 2019), and chronic inflammation (Mihai et al., 2018) play important roles in the pathophysiology of CKD development. Previous studies have suggested that elevated ALP is significantly associated with systemic inflammation (Cheung et al., 2008; Damera et al., 2011). ALP levels may, therefore, partially reflect inflammation of hepatic origin. Additionally, a study conducted in hypertensive individuals revealed that higher serum ALP increased the risk of endothelial dysfunction (Perticone et al., 2015). The possible mechanisms for this may be that ALP can reduce nitric oxide (NO) bioavailability by inhibiting tyrosine kinase activity into endothelial cells, leading to the consequent impairment of endothelial NO synthase function and the reduction of NO production (Schultz-Hector et al., 1993; Boo and Jo, 2003). Moreover, increased ALP levels may promote the production of reactive oxygen species and apoptosis (Perticone et al., 2015). Taken together, we hypothesized that oxidative stress, endothelial dysfunction, and chronic inflammation that may mediate the associations of ALP with increased risk of CKD.
On the other hand, possible antioxidant activities and anti-inflammatory properties of folic acid have been reported in previous studies (Joshi et al., 2001; Solini et al., 2006). Prior studies have demonstrated that folic acid can scavenge thiyl radicals, repair these thiols at physiological pH (Joshi et al., 2001), and reduce levels of interleukins (Solini et al., 2006). Moreover, folic acid also plays a crucial role in endothelium-protection (Stanhewicz and Kenney, 2017). Folic acid, in counteracting these detrimental effects, could therefore, significantly reduce the risk of CKD in a population with increased ALP levels. However, the detailed underlying mechanisms still need to be further investigated in future studies.
In our study, the increased risk of CKD progression associated with ALP levels and the beneficial effect of folic acid were mainly observed among those in quartile 4 of ALP levels. However, only in China, there were about 244.5 million of the adult population ≥18 years of age had hypertension (Wang et al., 2018). That is to say that about 61 million Chinese adults had increased CKD progression risk associated with higher ALP (quartile 4), and may benefit from folic acid supplementation. During about 4.5 years of folic acid supplementation (a safe and inexpensive treatment), about 67.1 thousand Chinese hypertensive patients may be exempt from the CKD progression risk. Therefore, our findings may be clinically meaningful.
Several potential limitations are worth mentioning. First, this is a post-hoc analysis. Although our current study adjusted for a broad array of covariates in the regression models, the possibility of residual confounding cannot be excluded. Second, creatinine was accessed only at baseline and the exit visit; more frequent measurements of creatinine would have allowed for a more accurate assessment of CKD progression. Third, in the current study, we collected total serum ALP rather than ALP isozymes. Fourth, our study was performed in Chinese hypertensive patients. The generalization of our results to other populations or patients with other kidney diseases needs to be further determined. Overall, further confirmation of our findings in more studies is essential.
In conclusions, our study suggests that higher serum ALP levels were associated with increased risk of CKD progression in general hypertensive adults, and this risk was reduced by 47% with folic acid treatment. Obtaining ALP levels is relatively easy, rapid, and universally available in general clinical laboratories. Our findings, if confirmed, have important clinical and public health implications. Our data suggest that identifying hypertensive patients with higher serum ALP levels, could help detect those individuals who are at high risk of CKD progression and who would particularly benefit from folic acid supplementation, a treatment that is simple, safe, and inexpensive.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Institute of Biomedicine, Anhui Medical University, Hefei, China (FWA assurance number: FWA00001263). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
YZ, XX and XQ designed research; YZ, JL, YZ, BW, YH, FFH, XX and XQ conducted research; YZ, PH, GW, ML, DX, JN, CL, YS, LL, BW, JL, YZ, XW, YH, FH, XX, and XQ contributed to acquisition, analysis, or interpretation of data; YZ, CL and XQ performed statistical analysis; YZ and XQ wrote paper; All authors revised the manuscript and approved the final version of the manuscript.
Funding
The study was supported by funding from the following: the National Key Research and Development Program (2020YFC2005000; JN; 2016YFE0205400, 2018ZX09739010, 2018ZX09301034003; XPX), the Science and Technology Planning Project of Guangzhou, China (201707020010; XPX); the Science, Technology and Innovation Committee of Shenzhen (JSGG20170412155639040, GJHS20170314114526143, JSGG20180703155802047; XPX); the Economic, Trade and Information Commission of Shenzhen Municipality (20170505161556110, 20170505160926390; XPX); the National Natural Science Foundation of China (81730019, 81973133; XHQ) and Outstanding Youths Development Scheme of Nanfang Hospital, Southern Medical University (2017J009, XHQ). The funders had no role in the design and/or conduct of the study; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.753803/full#supplementary-material
References
Boo, Y. C., and Jo, H. (2003). Flow-dependent Regulation of Endothelial Nitric Oxide Synthase: Role of Protein Kinases. Am. J. Physiol. Cell Physiol 285 (3), C499–C508. doi:10.1152/ajpcell.00122.2003
Chen, T. K., Knicely, D. H., and Grams, M. E. (2019). Chronic Kidney Disease Diagnosis and Management: A Review. JAMA 322 (13), 1294–1304. doi:10.1001/jama.2019.14745
Cheung, B. M., Ong, K. L., Cheung, R. V., Wong, L. Y., Wat, N. M., Tam, S., et al. (2008). Association between Plasma Alkaline Phosphatase and C-Reactive Protein in Hong Kong Chinese. Clin. Chem. Lab. Med. 46 (4), 523–527. doi:10.1515/CCLM.2008.111
Contreras, A. M., Ruiz, I., Polanco-Cruz, G., Monteón, F. J., Celis, A., Vázquez, G., et al. (2007). End-stage Renal Disease and Hepatitis C Infection: Comparison of Alanine Aminotransferase Levels and Liver Histology in Patients with and without Renal Damage. Ann. Hepatol. 6 (1), 48–54. doi:10.1016/s1665-2681(19)31953-2
Coppolino, G., Leonardi, G., Andreucci, M., and Bolignano, D. (2018). Oxidative Stress and Kidney Function: A Brief Update. Curr. Pharm. Des. 24 (40), 4794–4799. doi:10.2174/1381612825666190112165206
Coresh, J., Turin, T. C., Matsushita, K., Sang, Y., Ballew, S. H., Appel, L. J., et al. (2014). Decline in Estimated Glomerular Filtration Rate and Subsequent Risk of End-Stage Renal Disease and Mortality. JAMA 311 (24), 2518–2531. doi:10.1001/jama.2014.6634
Damera, S., Raphael, K. L., Baird, B. C., Cheung, A. K., Greene, T., and Beddhu, S. (2011). Serum Alkaline Phosphatase Levels Associate with Elevated Serum C-Reactive Protein in Chronic Kidney Disease. Kidney Int. 79 (2), 228–233. doi:10.1038/ki.2010.356
Er, R., Aydın, B., Şekeroğlu, V., and Atlı Şekeroğlu, Z. (2020). Protective Effect of Argan Oil on Mitochondrial Function and Oxidative Stress against Acrylamide-Induced Liver and Kidney Injury in Rats. Biomarkers 25 (6), 458–467. doi:10.1080/1354750X.2020.1797877
Fan, Y., Jin, X., Jiang, M., and Fang, N. (2017). Elevated Serum Alkaline Phosphatase and Cardiovascular or All-Cause Mortality Risk in Dialysis Patients: A Meta-Analysis. Sci. Rep. 7 (1), 13224. doi:10.1038/s41598-017-13387-z
Go, A. S., Chertow, G. M., Fan, D., McCulloch, C. E., and Hsu, C. Y. (2004). Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N. Engl. J. Med. 351 (13), 1296–1305. doi:10.1056/NEJMoa041031
Haarhaus, M., Brandenburg, V., Kalantar-Zadeh, K., Stenvinkel, P., and Magnusson, P. (2017). Alkaline Phosphatase: a Novel Treatment Target for Cardiovascular Disease in CKD. Nat. Rev. Nephrol. 13 (7), 429–442. doi:10.1038/nrneph.2017.60
Harmey, D., Hessle, L., Narisawa, S., Johnson, K. A., Terkeltaub, R., and Millán, J. L. (2004). Concerted Regulation of Inorganic Pyrophosphate and Osteopontin by Akp2, Enpp1, and Ank: an Integrated Model of the Pathogenesis of Mineralization Disorders. Am. J. Pathol. 164 (4), 1199–1209. doi:10.1016/S0002-9440(10)63208-7
Huo, Y., Li, J., Qin, X., Huang, Y., Wang, X., Gottesman, R. F., et al. (2015). Efficacy of Folic Acid Therapy in Primary Prevention of Stroke Among Adults with Hypertension in China: the CSPPT Randomized Clinical Trial. JAMA 313 (13), 1325–1335. doi:10.1001/jama.2015.2274
Jha, V., Garcia-Garcia, G., Iseki, K., Li, Z., Naicker, S., Plattner, B., et al. (2013). Chronic Kidney Disease: Global Dimension and Perspectives. Lancet 382 (9888), 260–272. doi:10.1016/S0140-6736(13)60687-X
Joshi, R., Adhikari, S., Patro, B. S., Chattopadhyay, S., and Mukherjee, T. (2001). Free Radical Scavenging Behavior of Folic Acid: Evidence for Possible Antioxidant Activity. Free Radic. Biol. Med. 30 (12), 1390–1399. doi:10.1016/s0891-5849(01)00543-3
Jourde-Chiche, N., Fakhouri, F., Dou, L., Bellien, J., Burtey, S., Frimat, M., et al. (2019). Endothelium Structure and Function in Kidney Health and Disease. Nat. Rev. Nephrol. 15 (2), 87–108. doi:10.1038/s41581-018-0098-z
Kabootari, M., Raee, M. R., Akbarpour, S., Asgari, S., Azizi, F., and Hadaegh, F. (2018). Serum Alkaline Phosphatase and the Risk of Coronary Heart Disease, Stroke and All-Cause Mortality: Tehran Lipid and Glucose Study. BMJ Open 8 (11), e023735. doi:10.1136/bmjopen-2018-023735
Kunutsor, S. K., Apekey, T. A., and Khan, H. (2014). Liver Enzymes and Risk of Cardiovascular Disease in the General Population: a Meta-Analysis of Prospective Cohort Studies. Atherosclerosis 236 (1), 7–17. doi:10.1016/j.atherosclerosis.2014.06.006
Levey, A. S., Stevens, L. A., Schmid, C. H., Zhang, Y. L., Castro, A. F., Feldman, H. I., et al. (2009). A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 150 (9), 604–612. doi:10.7326/0003-4819-150-9-200905050-00006
Majoni, S. W., Barzi, F., Hoy, W., MacIsaac, R. J., Cass, A., Maple-Brown, L., et al. (2020). Baseline Liver Function Tests and Full Blood Count Indices and Their Association with Progression of Chronic Kidney Disease and Renal Outcomes in Aboriginal and Torres Strait Islander People: the eGFR Follow- up Study. BMC Nephrol. 21 (1), 523. doi:10.1186/s12882-020-02185-x
Mihai, S., Codrici, E., Popescu, I. D., Enciu, A. M., Albulescu, L., Necula, L. G., et al. (2018). Inflammation-Related Mechanisms in Chronic Kidney Disease Prediction, Progression, and Outcome. J. Immunol. Res. 2018, 2180373. doi:10.1155/2018/2180373
Park, J. B., Kang, D. Y., Yang, H. M., Cho, H. J., Park, K. W., Lee, H. Y., et al. (2013). Serum Alkaline Phosphatase Is a Predictor of Mortality, Myocardial Infarction, or Stent Thrombosis after Implantation of Coronary Drug-Eluting Stent. Eur. Heart J. 34 (12), 920–931. doi:10.1093/eurheartj/ehs419
Perticone, F., Perticone, M., Maio, R., Sciacqua, A., Andreucci, M., Tripepi, G., et al. (2015). Serum Alkaline Phosphatase Negatively Affects Endothelium-dependent Vasodilation in Naïve Hypertensive Patients. Hypertension 66 (4), 874–880. doi:10.1161/HYPERTENSIONAHA.115.06117
Qin, X., Li, Y., He, M., Tang, G., Yin, D., Liang, M., et al. (2017). Folic Acid Therapy Reduces Serum Uric Acid in Hypertensive Patients: a Substudy of the China Stroke Primary Prevention Trial (CSPPT). Am. J. Clin. Nutr. 105 (4), 882–889. doi:10.3945/ajcn.116.143131
Qin, X., Shen, L., Zhang, R., Li, Y., Wang, X., Wang, B., et al. (2017). Effect of Folic Acid Supplementation on Cancer Risk Among Adults with Hypertension in China: A Randomized Clinical Trial. Int. J. Cancer 141 (4), 837–847. doi:10.1002/ijc.30094
Qin, X., Zhang, Y., Cai, Y., He, M., Sun, L., Fu, J., et al. (2013). Prevalence of Obesity, Abdominal Obesity and Associated Factors in Hypertensive Adults Aged 45-75 Years. Clin. Nutr. 32 (3), 361–367. doi:10.1016/j.clnu.2012.08.005
Sansoè, G., Aragno, M., and Wong, F. (2020). Pathways of Hepatic and Renal Damage through Non-classical Activation of the Renin-Angiotensin System in Chronic Liver Disease. Liver Int. 40 (1), 18–31. doi:10.1111/liv.14272
Schultz-Hector, S., Balz, K., Böhm, M., Ikehara, Y., and Rieke, L. (1993). Cellular Localization of Endothelial Alkaline Phosphatase Reaction Product and Enzyme Protein in the Myocardium. J. Histochem. Cytochem. 41 (12), 1813–1821. doi:10.1177/41.12.8245430
Sharma, U., Pal, D., and Prasad, R. (2014). Alkaline Phosphatase: An Overview. Indian J. Clin. Biochem. 29 (3), 269–278. doi:10.1007/s12291-013-0408-y
Solini, A., Santini, E., and Ferrannini, E. (2006). Effect of Short-Term Folic Acid Supplementation on Insulin Sensitivity and Inflammatory Markers in Overweight Subjects. Int. J. Obes. (Lond) 30 (8), 1197–1202. doi:10.1038/sj.ijo.0803265
Spence, J. D., Yi, Q., and Hankey, G. J. (2017). B Vitamins in Stroke Prevention: Time to Reconsider. Lancet Neurol. 16 (9), 750–760. doi:10.1016/S1474-4422(17)30180-1
Stanhewicz, A. E., and Kenney, W. L. (2017). Role of Folic Acid in Nitric Oxide Bioavailability and Vascular Endothelial Function. Nutr. Rev. 75 (1), 61–70. doi:10.1093/nutrit/nuw053
Sumida, K., Molnar, M. Z., Potukuchi, P. K., Thomas, F., Lu, J. L., Obi, Y., et al. (2018). Prognostic Significance of Pre-end-stage Renal Disease Serum Alkaline Phosphatase for post-end-stage Renal Disease Mortality in Late-Stage Chronic Kidney Disease Patients Transitioning to Dialysis. Nephrol. Dial. Transpl. 33 (2), 264–273. doi:10.1093/ndt/gfw412
Taliercio, J. J., Schold, J. D., Simon, J. F., Arrigain, S., Tang, A., Saab, G., et al. (2013). Prognostic Importance of Serum Alkaline Phosphatase in CKD Stages 3-4 in a Clinical Population. Am. J. Kidney Dis. 62 (4), 703–710. doi:10.1053/j.ajkd.2013.04.012
Tanaka, K., Watanabe, T., Takeuchi, A., Ohashi, Y., Nitta, K., Akizawa, T., et al. (2017). Cardiovascular Events and Death in Japanese Patients with Chronic Kidney Disease. Kidney Int. 91 (1), 227–234. doi:10.1016/j.kint.2016.09.015
Title, L. M., Cummings, P. M., Giddens, K., Genest, J. J., and Nassar, B. A. (2000). Effect of Folic Acid and Antioxidant Vitamins on Endothelial Dysfunction in Patients with Coronary Artery Disease. J. Am. Coll. Cardiol. 36 (3), 758–765. doi:10.1016/s0735-1097(00)00809-3
Wang, Z., Chen, Z., Zhang, L., Wang, X., Hao, G., Zhang, Z., et al. (2018). Status of Hypertension in China: Results from the China Hypertension Survey, 2012-2015. Circulation 137 (22), 2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
Xu, X., Qin, X., Li, Y., Sun, D., Wang, J., Liang, M., et al. (2016). Efficacy of Folic Acid Therapy on the Progression of Chronic Kidney Disease: The Renal Substudy of the China Stroke Primary Prevention Trial. JAMA Intern. Med. 176 (10), 1443–1450. doi:10.1001/jamainternmed.2016.4687
Yamazoe, M., Mizuno, A., Nishi, Y., Niwa, K., and Isobe, M. (2016). Serum Alkaline Phosphatase as a Predictor of Worsening Renal Function in Patients with Acute Decompensated Heart Failure. J. Cardiol. 67 (5), 412–417. doi:10.1016/j.jjcc.2015.08.004
Keywords: serum alkaline phosphatase, folic acid, CKD progression, hypertension, cohort study
Citation: Zhang Y, He P, Wang G, Liang M, Xie D, Nie J, Liu C, Song Y, Liu L, Wang B, Li J, Zhang Y, Wang X, Huo Y, Hou FF, Xu X and Qin X (2022) Interaction of Serum Alkaline Phosphatase and Folic Acid Treatment on Chronic Kidney Disease Progression in Treated Hypertensive Adults. Front. Pharmacol. 12:753803. doi: 10.3389/fphar.2021.753803
Received: 05 August 2021; Accepted: 22 December 2021;
Published: 13 January 2022.
Edited by:
Norberto Perico, Mario Negri Pharmacological Research Institute (IRCCS), ItalyReviewed by:
Anxin Wang, Beijing Tiantan Hospital, Capital Medical University, ChinaGaetano La Manna, University of Bologna, Italy
Copyright © 2022 Zhang, He, Wang, Liang, Xie, Nie, Liu, Song, Liu, Wang, Li, Zhang, Wang, Huo, Hou, Xu and Qin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xianhui Qin, cGhhcm1hcWluQDEyNi5jb20=