 Yuanxuan Cai
Yuanxuan Cai Linhui Yang
Linhui Yang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 20 October 2021
Sec. Drugs Outcomes Research and Policies
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.736618
This article is part of the Research Topic Leveraging Pharmacovigilance Data Mining with “The Patient” in Mind View all 12 articles
Introduction: Cephalosporins are widely used in clinical treatment of children, but it is difficult to carry out clinical trials and there is no strong evidence of their safety. Therefore, adverse drug reactions (ADR) of cephalosporins can be a public health problem that deserves attention.
Methods: ADR reports collected by the Hubei Adverse Drug Reaction Monitoring Center from 2014 to 2019 were analysed. The safety of Cephalosporins was described by descriptive analysis and three signal mining methods, including the reporting odd ratio (ROR), proportional reporting ratio (PRR), and comprehensive standard method (MHRA).
Results: The findings indicated that the age groups of 0–1 and 2–3 years had the highest rates of reporting ADRs. Children aged 0–4 years reported more ADRs, while the proportion of severe ADRs was lower than the average (6.63%). Among the 37 cephalosporins, the severe ADRs of ceftezole, ceftazidime, cefoperazone/sulbactam, cefotaxime, ceftriaxone were reported more and the proportion of severe ADRs was higher. The proportion of severe ADRs of most cephalosporin compound preparations was higher than that of corresponding single components. A total of 99.18% of the cases improved after treatment. There were four deaths whose ADRs were mainly anaphylactic shock, dyspnoea, and anaphylactoid reaction. In signal mining, the three methods produced 206 signals that were the same, and 73 of them were off-label ADRs.
Conclusion: ADRs were common but not serious in children aged 0–4 years. And the reported rate of serious ADRs in children aged over 4 years increased with age. ADR reports of ceftezole, ceftazidime, cefoperazone/sulbactam, cefotaxime, ceftriaxone were numerous and serious, and the safety of cephalosporin compound preparations in children was doubtful. Ceftezole may cause off-label ADRs including tremor, face oedema, cyanosis, pallor, rigors, and palpitation. The labeling of ADRs in children in cephalosporin instructions and the record of allergic history need to be improved.
Cephalosporins belong to β-lactam class of antibiotics and have been developed to the fifth generation at present. Cephalosporins are widely used in the world for their broad antibacterial spectrum, low toxicity, penicillinase resistance and rich varieties. The subsequent adverse drug reactions (ADRs) have also become the focus of public concern. In China, an ADR is defined as the harmful reaction of qualified drugs under normal usage and dosage, which has nothing to do with the purpose of drug use (2011). The annual reports of national ADR monitoring in China from 2017 to 2019 all showed that ADR reports of cephalosporins were the most in the reports of anti-infective drugs, which also had the most reports of serious ADRs (Administration, N.M.P, 2018; Administration, N.M.P, 2019; Administration, N.M.P, 2020).
With the implementation of the two-child policy in 2015 and the three-child policy in 2021, the number of children (0–14) in China has increased rapidly, and the safety of children’s medication has become a key point to improve the health of children. G. M. Park found that antibiotics were the most common ADR causing drugs in children, among which the third cephalosporin was the most common (Park et al., 2012). Jung also believed that antibiotics were the most common drugs that might cause ADRs in children (n = 5,159), among which cephalosporins were the most common drugs (n = 5,101). Gastrointestinal tract and skin clinical features were the most frequently reported ADR (Jung et al., 2017). In 2015, the National Medical Products Administration warned that cefathiamidine could cause severe ADRs like anaphylactic shock, and a high proportion of ADRs of cefathiamidine have been reported in the ADR reports of children (Administration, S.F.a.D, 2015). Children, as a special medication population, are prone to ADR due to their underdevelopment of liver, kidney and central nervous system and poor ability of metabolism, excretion and tolerance of drugs.
Cephalosporin ADRs in children is a public health problem that deserves attention. It is difficult to carry out clinical trials in children, and there is no strong evidence of safety. And the use of cephalosporins is mostly based on long-term clinical practice. Therefore, it is necessary to re-evaluate the safety of cephalosporins in children after marketing. The purpose of this study was to analyze the provincial spontaneous reporting system (SRS) database to investigate the safety of cephalosporins in children from all aspects of ADRs.
The data of the ADR reports collected by Adverse Drug Reaction Monitoring Center of Hubei Province from January 2014 to December 2019 were classified and analysed.
The data were cleaned and preprocessed to ensure that they were clean and complete. The ADR database includes all reported ADR reports. Reports of cephalosporin in children aged 0–14 were selected for inclusion. The analysis only included reports with certain, probable, and possible relationships of drugs and ADR evaluated by the reporting unit, and excluded reports that were unlikely or impossible to evaluate. Since there was no unified standard for the entry of drug names and ADRs in the report, the names of active pharmaceutical ingredients (APIs) registered in the National Center For Drug Evaluation were used as the standard to unify the generic names and the ADRs and clinical manifestations were organized according to the World Health Organization Adverse Reaction Terms (WHO-ART).
For the death cases, relevant information was detailed and carefully analysed to find other key points that had contributed.
From January 2014 to December 2019, the ADR Monitoring Center collected a total of 420,114 reports, containing 60,433 reports from children aged 0–14. There were 15,857 reports meeting the inclusion criteria. Since there might be two or more ADRs in a report or case, and the occurrence of an ADR in the use of a certain drug was considered an event, 20,681 events were included in the statistics.
A descriptive analysis of sex, age, allergic history, drug, severity, types, and results of ADRs in the reports was carried out.
The amount of each ADR of each cephalosporin was sorted for ADR signal mining, which quantifies the qualitative nature of the relationship between drugs and ADRs (Hauben et al., 2005). In ADR signal mining, the reporting odds ratio (ROR), proportional reporting ratio (PRR), and comprehensive standard method (MHRA) as measures of disproportionality were adopted, which is generally used in this area to detect the imbalance of target events compared with other events in the database (Hauben et al., 2005; Moore et al., 2005). When the frequency of the target drug event combination (DEC) is significantly higher and reaches the threshold compared to the background frequency, a signal is considered to be generated (van Puijenbroek et al., 2002). The strength of the association between drugs and ADRs was expressed as the ROR and PRR with 95% confidence intervals (CIs). The fourfold table used in the measures of disproportionality is shown in Table 1. The calculation formulas and the threshold for generating a signal with these three methods are presented in Table 2. In this study, signal mining of a single drug and a single ADR was conducted without considering the combination of drug use and drug interaction.
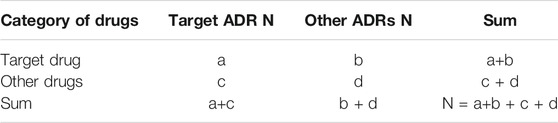
TABLE 1. The fourfold table used in measures of disproportionality.
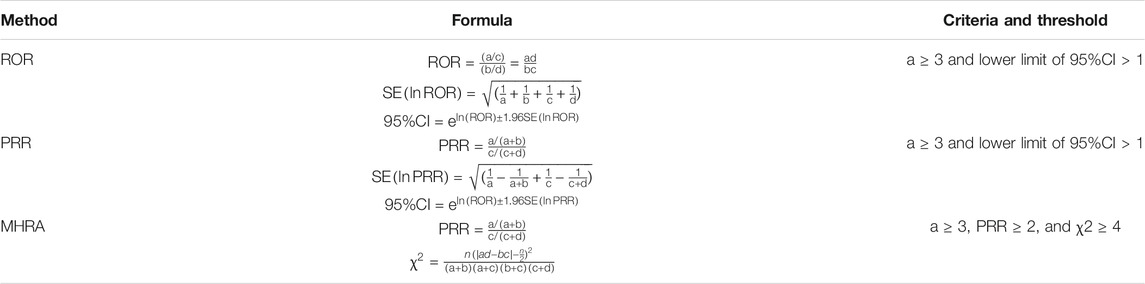
TABLE 2. Formulas and criteria for generating signals of ROR, PRR, and MHRA.
Among the 15,857 reports related to cephalosporins in children, except for 14 cases in which the sex was unknown, the number of men (9,740) who had ADRs was significantly greater than that of women (6,103), and the male-female ratio was 1.60:1 with a big discrepancy. Excluding six reports of unknown age, the age groups with higher reporting rates were concentrated in 0-1-year-olds (3,145) and 2-3-year-olds (2,361) (see Figure 1). That is, newborns, infants, and young children were the most common.
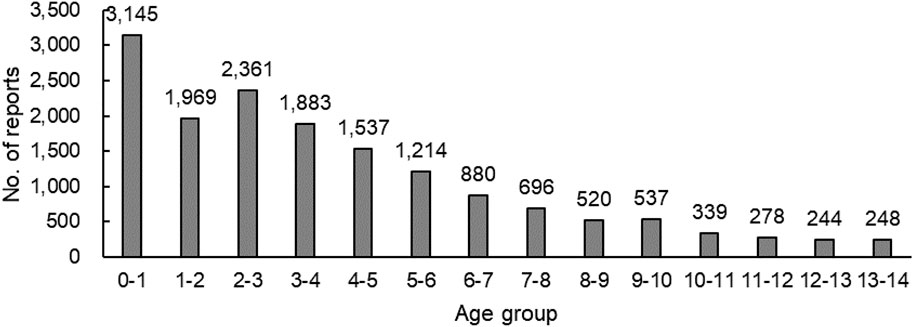
FIGURE 1. Number of reports in each age group (n=15,851).
According to the data that had been recorded, 38 reports were allergic to cephalosporin; 45 reports were allergic to penicillin; 10 reports were allergic to both of them; and 10 reports had a history of alcohol consumption.
A total of 15,857 cases of cephalosporins in children were reported, which involved 37 kinds of cephalosporins except three cases of unknown cephalosporins. The third cephalosporin was the most reported. Ceftezole, ceftazidime, cefamandole nafate, and cefoperazone/sulbactam were reported in large numbers (see Table 3).
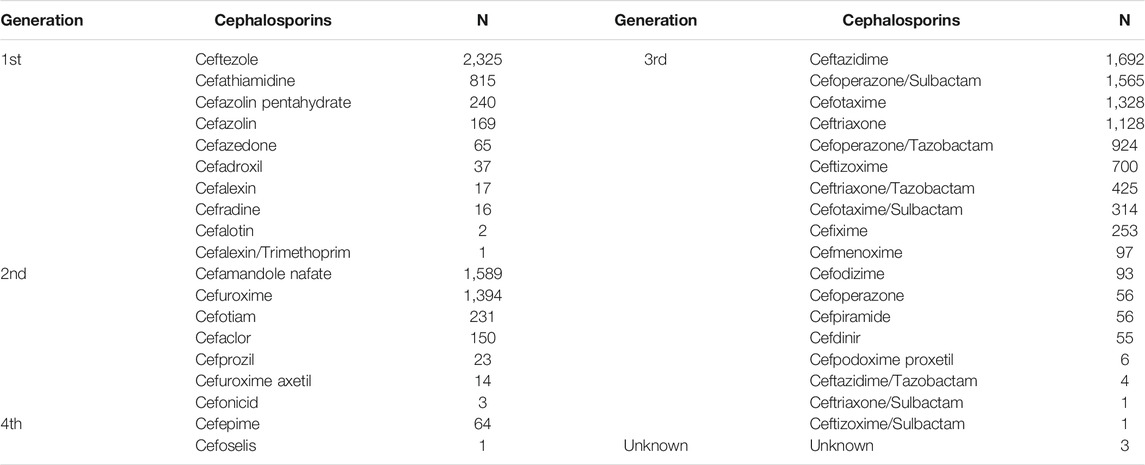
TABLE 3. Number of reports of cephalosporins (n = 15,857).
The main route of administration was injection (15,271, 96.30%), followed by oral administration (581, 3.66%).
The Administrative Measures on Reporting and Monitoring of ADRs states that according to the severity of ADRs, ADRs were divided into serious and non-serious ADRs. Serious ADRs result in death, life-threatening effects, cancer, a congenital anomaly, birth defects, significant or permanent human disability, damage to organ function, hospitalization or prolonged hospitalization or events that require intervention and treatment to avoid the above results. New and known ADRs are also subdivided according to whether the ADRs are recorded in the drug insert. In addition, ADRs whose types are known but whose severity is greater than that described in the drug insert are also regarded as new ADRs (Administration, 2011) Serious and new ADRs have always been the focus of ADR research, as they pose a greater threat to the life and health of patients.
Among the 15,857 reports related to cephalosporins in children, there were 1,052 reports of serious ADRs, accounting for 6.63% of the total reports, of which 154 were new and serious reports. There were 14,805 non-serious reports containing 1,573 new and non-serious reports, accounting for 93.37% of the total. The severity of ADRs in males and females was presented in Figure 2. The severity of ADRs was not significantly different by sex (χ2 = 0.219, p = 0.640 > 0.05). Figure 3 described serious and non-serious reports in different age groups and the proportion of serious reports, excluding six cases with age unknown. It could be found that the proportion of severe ADRs in children aged 0–4 years was lower than the average (6.63%) although there were more reported ADRs, while the proportion of severe ADRs in children older than 4 years was higher than the average (χ2 = 31.691, p = 0.000 < 0.05).
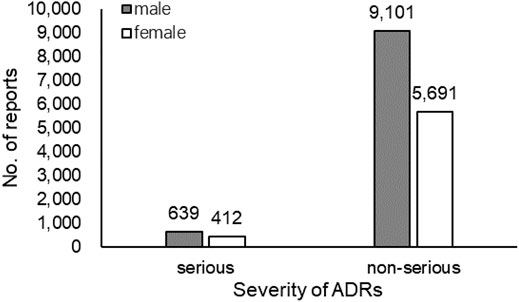
FIGURE 2. Number of serious and non-serious reports by sex (n=15,843).
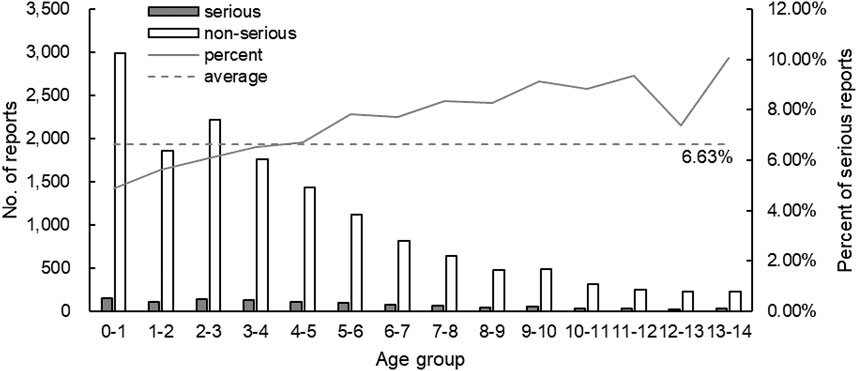
FIGURE 3. Number of reports and the proportion of serious reports in each age group (n=15,851).
Table 4 shows the number and proportion of serious reports of cephalosporin in children (ordered by the number of reports). Ceftezole, ceftazidime, cefoperazone/sulbactam, cefotaxime, and ceftriaxone had the most severe reports with a higher proportion of severe ADRs. It is worth mentioning that the proportion of severe ADRs of compound preparations was higher than that of corresponding single components except for compound preparations with a small number of reports, such as cefoperazone/sulbactam (9.14% > 7.14%), ceftriaxone/tazobactam (7.76% > 7.27%), and cefotaxime/sulbactam (8.60% > 7.83%).

TABLE 4. Number and proportion of serious reports by cephalosporin in children (n = 15,857).
A total of 20,681 events involved a total of 21 system-organ damage, mainly including skin and appendage disorders, body as a whole-general disorders and gastro-intestinal system disorders. The detailed number and proportion of events were shown in Table 5.
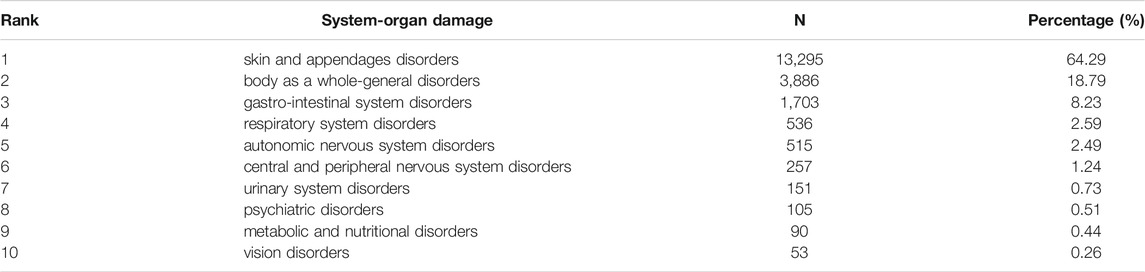
TABLE 5. Number and percentage of ADR events related to system-organ damage (top 10, n = 20,681).
According to the statistics, a total of 153 ADRs were identified, which were concentrated in rash, pruritus, urticaria, maculo-papular rash, allergic reaction, nausea, and vomiting. Table 6 shows the distribution of the number of ADRs in the top 95%. Allergic reaction were the most concerned ADRs, accounting for 15.92%.
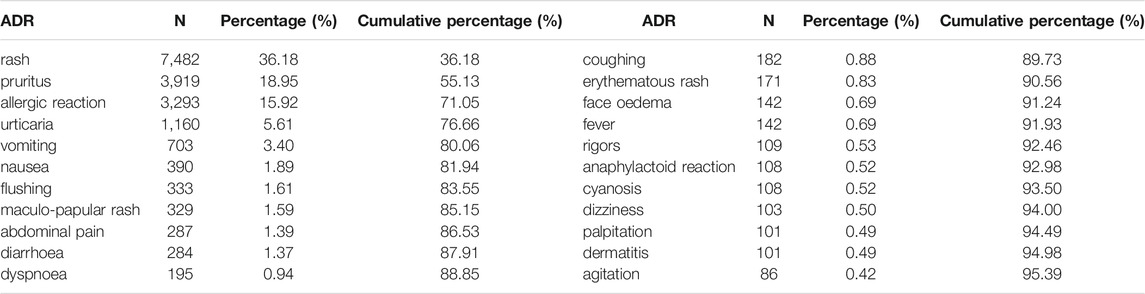
TABLE 6. Number and proportion of ADRs (n = 23,377).
The vast majority of children (99.18%) improved or recovered after treatment and intervention after the occurrence of ADRs. Among the four deaths, two were males and two were females. The children mainly suffered from respiratory and urologic diseases. The main ADRs were anaphylactic shock (2), dyspnoea (1) and anaphylactoid reaction (1) (see Table 7).

TABLE 7. Detailed information of the 4 deaths.
According to the calculation formulas and thresholds, DEC signals that do not meet the criteria were excluded. The ROR generated 211 signals, the PRR generated 207 signals, and the MHRA generated 376 signals. The three signal mining methods produced a total of 206 signals of the same DECs, and some of the signals are shown in Table 8. The larger the ROR and PRR values, the stronger is the correlation between the drug and ADR. All positive signals were sorted into Table 9, and off-label ADRs were marked.
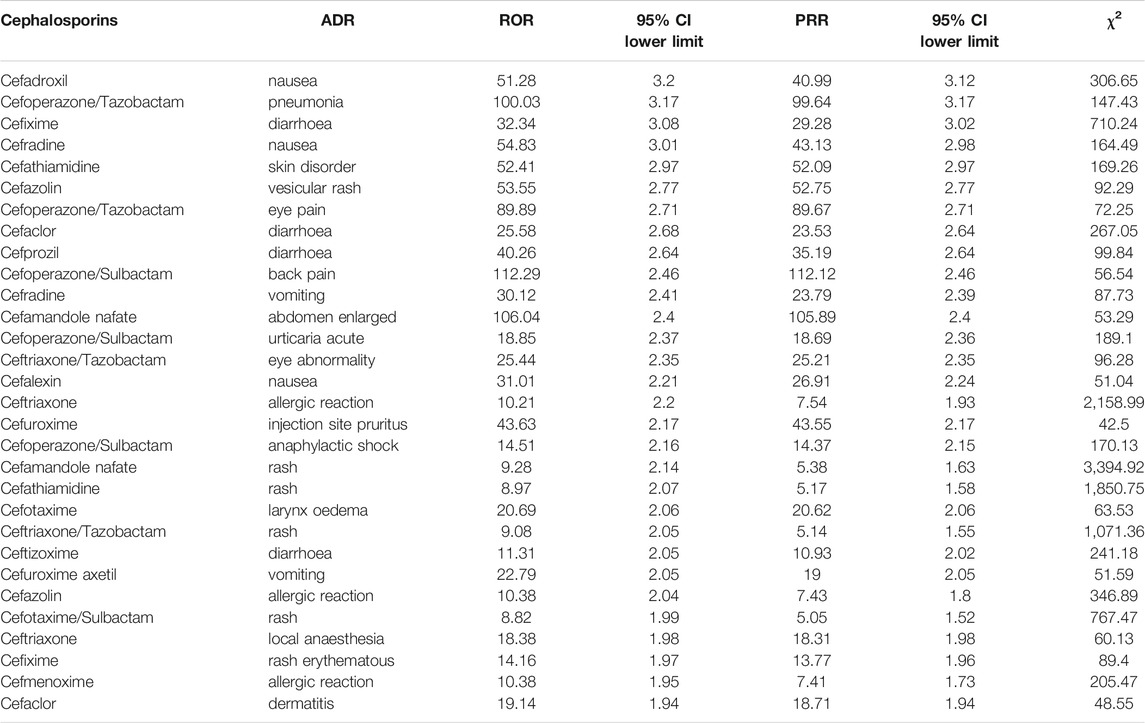
TABLE 8. Some of the signals of ADRs (3 methods).
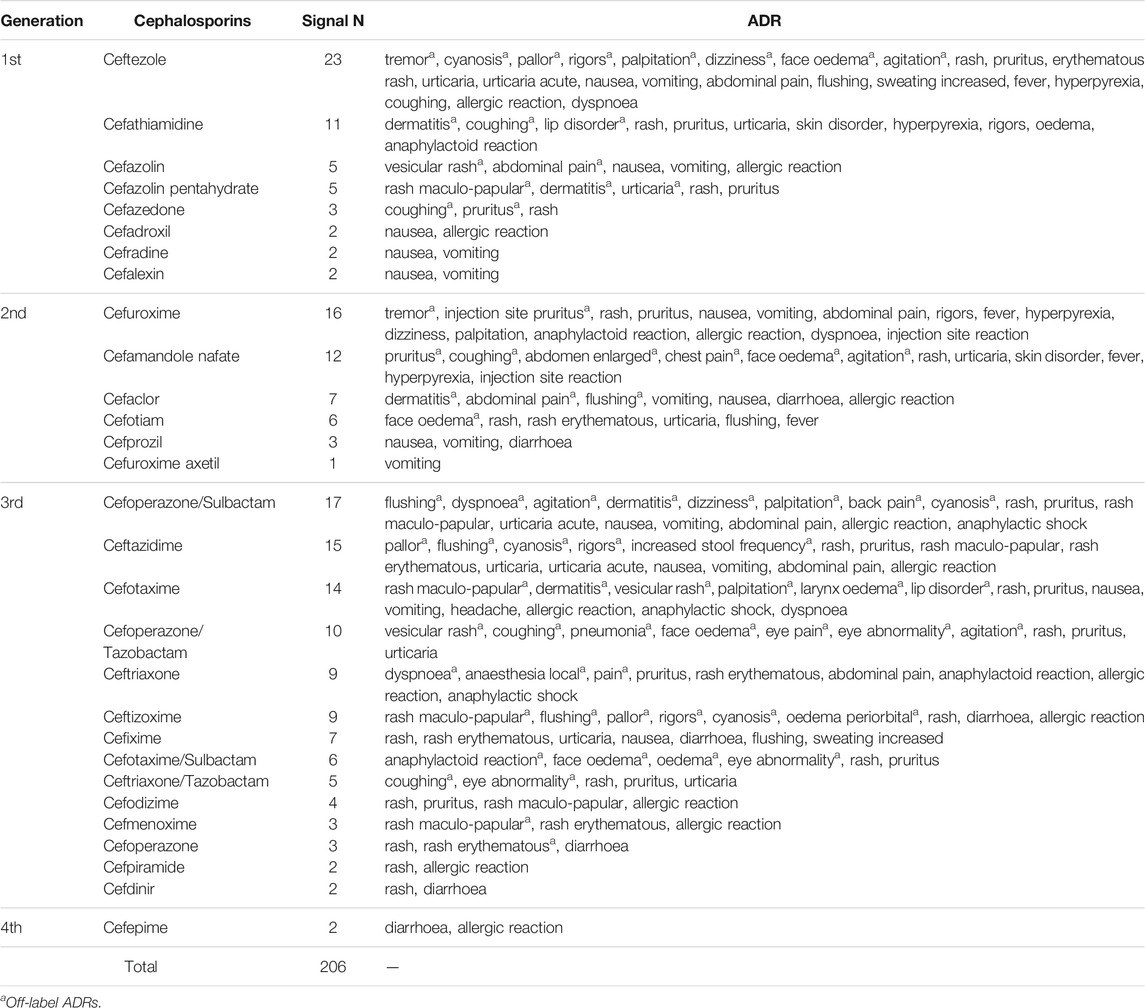
TABLE 9. All positive ADR signals.
According to statistics, in recent 6 years, the ADR reports of cephalosporins in children aged 0–14 reported by SRS were mainly concentrated in children aged 0–3. Jiang found that among the people who had ADRs after taking cephalosporins, young children were the most prominent (Jiang et al., 2021). Zheng’s investigation on a hospital found that the number of children with ADRs to cephalosporins was mainly 0–3 years old (Zheng et al., 2018). The above results were consistent with the results of this study, which suggested that the physiological function of children, especially newborns and infants, was not fully mature; drug metabolism was slow; and drug accumulation was easy to occur, resulting in a high incidence of ADR. Due to the limitations of data collection, it was not possible to know the frequency of cephalosporin use by age group.
The patient’s allergy history may be incomplete, making it difficult to make a meaningful analysis. However, a study involving 13,153 cases of cefazolin skin testing in South Korea found that 15% of patients with a history of β-lactam allergy were positive for the skin test; 1.35% of the patients without a history of β-lactam antibiotic allergy were positive, indicating that the history of β-lactam allergy may be associated with the occurrence of cephalosporin allergic reactions (Kwon et al., 2019). In addition, there may also be cross-reactivity in cephalosporin allergy (Li et al., 2019). Perfecting the records of allergic history will be helpful to the prediction of allergic reactions.
Combined with the severity of ADRs, the results showed that there was no significant difference in the distribution of the severity of ADRs between different sexes. Notably, although there were many ADR reports in children aged 0–4 years, the proportion of severe ADRs is the lowest. The likely reason was that doctors were more cautious in using cephalosporins when treating newborns and infants, prioritizing safety over efficacy (Lu et al., 2018). The reported rate of severe ADRs generally increased with age. Children at this age were in a period of rapid growth and development, and their physical conditions fluctuated greatly, so it was difficult to determine the appropriate dose. This may have something to do with the difficulty in accurately estimating the appropriate dose from experience and the increasing confidence of doctors in medication as children age. It was suggested that doctors strictly followed the drug instructions and antibiotic medication guidelines, comprehensively analyzed the state of the children, strictly controlled the dosage and prevented the inducing of drug resistance.
This study found that the use of cephalosporin compound preparations in children was more prominent in severe ADRs, and the proportion of severe ADRs in most cephalosporin compound preparations was higher than the average. At present, there were few studies on ADRs of cephalosporin compound preparations, among which the research of cefoperazone/sulbactam was the most abundant. In China, a number of retrospective studies on efficacy and ADRs reported that the efficacy of cefoperazone/sulbactam was significantly higher than that of ceftazidime in the control group, and the incidence of ADRs was considered lower than that of the control group (Zhu, 2019; Wang et al., 2020). The subjects in these studies were all older than 20 years. The noninferiority trial conducted by Liu on pneumonia patients over 18 years old showed no significant difference in the mortality rate and proportion of severe ADRs in the cefoperazone/sulbactam group compared with the cefepime group, suggesting that the two groups had the same efficacy and safety (Liu et al., 2019). In adults, ADRs and severe ADRs caused by cephalosporin compound preparations appeared to be no different or better than those caused by other conventional cephalosporins. Few studies have been conducted on ADRs of cephalosporin compound preparations in children. But the only studies that have been done on children seem to come to a different conclusion than adults, Pareek et al. compared the efficacy and safety of cefotaxime/sulbactam with amoxicillin clavulanate (conventional treatment) and found that one patient in the cefotaxime/sulbactam group reported a severe ADR to convulsion, except that both drugs were safe and well tolerated in the study population (Pareek et al., 2008). A clinical study involving 986 patients treated with cefotaxime/sulbactam found a higher incidence of ADRs in children than adults (12.73 vs. 6.46%, p < 0.05) (Chen et al., 2017). The ADRs of cephalosporin compound preparations in children may have different characteristics from that of adults. In addition, the pharmacokinetic trials of cephalosporin compound preparations in human volunteers were conducted in healthy adults, and the results showed no pharmacokinetic interaction between the two components, but it was not clear whether the it was consistent in children (Ma et al., 2003; Mingjie et al., 2008; Yang et al., 2011). ADRs, severe ADRs, factors and other aspects related to the safety of cephalosporin compound preparations in children may need more and in-depth studies.
In this study, it was found that the proportion of severe ADRs of most cephalosporin compound preparations was higher than that of the corresponding single formulations. Cephalosporins in compound preparation can effectively prevent bacteria from synthesizing cell wall and inhibit bacterial division, but is easily hydrolyzed by β-lactamase. Sulbactam and tazobactam are β-lactamase inhibitors, which can inhibit the activity of hydrolase but have weak antibacterial effect. Combined use of the two can increase the stability of cephalosporins and enhance the antibacterial effect. Many in vitro and in vivo experiments at earlier times have confirmed that cephalosporin compound preparations have better antibacterial effect than the corresponding single preparations (Crosby and Gump, 1982; Knapp et al., 1990; Fu et al., 2002; You et al., 2003; Prakash et al., 2005; Yong et al., 2006; Li et al., 2010). However, no comparative studies on safety between compound preparations and single preparations have been found, and only comparative studies on toxicity reactions were identified. Li investigated the difference of toxicity reaction between cefoperazone/tazobactam and single component. Acute toxicity test showed no abnormal reaction and no death in the tested animals; The long-term toxicity test showed no significant differences in hematology, blood biochemistry, coefficient of vital organs and pathology between the cefoperazone/tazobactam group and the single component group (Li et al., 2003). This study suggested that the use of cephalosporin compound preparations in children may increase the efficacy as well as ADR compared with the single preparations, probably because the impurity profile of compound preparations is not the simple summation of impurity profile of single formulations, but there are more new impurities and change quickly, indicating more allergic reactions.
ADRs of Cephalosporins in children mainly involved skin and accessory damage, systemic damage and gastrointestinal system damage, including rash, pruritus, urticaria, allergic reaction, vomiting, and nausea. There were only a few ADRs such as liver function damage, hematuria, and leucopenia. Misreporting was a common problem in SRS. Reactions of skin, gastrointestinal tract and the whole body were easy to detect, while ADRs related to liver, kidney, and blood may need to be reflected by biochemical indicators. And it was possible that medical institutions and doctors may choose not to report serious ADRs out of self-interest.
After treatment and intervention, ADRs of most patients have been improved or cured, but a few patients still left sequelae or died. Anaphylactoid reaction and anaphylactic shock accounted for the majority of the death reports, among which three cases of death reports used ceftriaxone from the same manufacturer. So it cannot be ruled out that ADRs may be caused by product quality problems. Besides, the safety of ceftriaxone has been a prominent problem. In the pharmacovigilance database of Iran from 1998 to 2009, ceftriaxone had the highest number of deaths (49 cases) (Shalviri et al., 2012); Ceftriaxone was the main drug in 112 cases of anaphylactic shock reported by SRS of Republic of Crimea from 2010 to 2018. Some literature analysis on severe ADRs of ceftriaxone showed that there were more cases of severe allergic reaction and anaphylactic shock, and anaphylactic shock was the main cause of death (Zhang et al., 2010; Lu et al., 2011). The safety of ceftriaxone still needs extra attention. Doctors should strictly follow the medication indications, strengthen the monitoring and treatment of allergic reactions, and actively carry out anti-allergy treatment.
In this study, ADR signals obtained from signal mining in the background of medication use in children may have child specificity. Combined with the drug instructions, 73 off-label ADRs were found. The off-label ADR signals of ceftezole with the largest number of reported cases were analyzed one by one.
De-Sarro reported that ceftezole was characterized by the presence of a tetrazole nucleus similar to pententytetrazole at position seven, and thus has convulsion activity. Tremor, convulsion and limb spasm occurred in both rats and dogs after intravenous administration (De Sarro et al., 1995). No cases of tremor after using ceftezole have been found in children, but a documented case of tremor and convulsion after intravenous ceftezole in an adult woman with uremia has been reported (Jin, 2009). Due to uremia, drug excretion was slowed down; plasma half-life was prolonged; the blood-brain barrier was damaged; and drugs accumulated in the central nervous system. Patients with uremia were more likely to develop antibiotic encephalopathy, or in severe cases of grand mal epilepsy. Given the six cases reported in this study and the fact that renal function and blood-brain barrier were not fully developed in children, tremor may be associated with the drug.
The occurrence of dizziness appeared to be a rare ADR of ceftezole, and few cases have been identified in related studies. When Geng evaluated the efficacy of a drug in children with ceftezole as the control group, dizziness occurred in three out of 40 cases (Geng, 2017). In the drug efficacy studies without age limits, Wang found dizziness in four cases (n = 40) and Yang found dizziness in three cases (n = 136) (Yang et al., 2010; Wang and Zeng, 2021). However, the specific mechanism of ceftezole induced dizziness remained unclear and more research was needed.
No facial edema has been reported with ceftezole. In this study, facial edema was mainly presented as facial and eyelid edema. Given the positive signals and description of the reported data, more studies were needed.
Anxiety with ceftezole was not common. Ma used the SF-36 score to evaluate the mental state of patients (without age limit) after the use of ceftezole. The higher the score, the better the state. The study obtained a low mental state score of 61.29 (Ma, 2018). It was difficult to judge whether the anxiety and restlessness was caused by the drug, because it seemed understandable that the child was anxious in an unfamiliar environment and in a state of physical discomfort.
Reports of ADRs such as cyanosis, pallor, chill, and palpitation with ceftezole have occasionally been seen. Wei analyzed 113 cases of ADRs of ceftezole in a hospital, and found two cases of chill (Jiao et al., 2010). Guo reported a case of elderly patients with sudden palpitations, pallor, and cold extremities after the injection of ceftezole (Guo and Sun, 2005). Since there were few studies related to children, there were no reported cases of these ADRs in children, and the relevant mechanism studies were even less.
In cephalosporin instructions, ADRs are well documented, most of which include the data of clinical trial and passive monitoring. In the process of examining the instructions, it was found that the ADR items of each cephalosporin were approximately consistent with the statistics for the number of ADRs in the study. However, there are few ADR annotations and clinical trial reports of ADRs related to medication in children in cephalosporin instructions. Due to economic and ethical issues, clinical trials of medicines for children are limited, resulting in a lack of efficacy and safety data for children. Some European countries have introduced relevant policies and regulations that allow manufacturers to enrich clinical trials of drugs with children as research subjects when conditions permit (Marinovic et al., 2016; Ciato et al., 2017). In addition, ADR signals of cephalosporins with children’s particularity could be obtained by data mining, which could be used as data support of ADRs in the instructions to enrich the label of ADRs related to medication in children.
The statistical results and ADR signals obtained in this study are helpful in guiding the safe use of cephalosporins for children in the clinic, and might be clues for ADR mechanism research, even providing advice for modifying drug labels based on results that may be special to children and the detection of off-label ADRs. In addition, this study has potential limitations. The effect estimated in the study is based on the data of a single province. Although the data are considerable, the external validity of the conclusion still needs to be improved. Due to the limitation of the selected signal mining method, the combination of drugs is not considered, and the conclusions may be biased.
ADRs were common but not serious in children aged 0–4 years. And the reported rate of serious ADRs in children aged over 4 years increased with age, possibly because the body fluctuated greatly at this stage and it was difficult to determine the appropriate dose with empirical medication. ADR reports of ceftezole, ceftazidime, cefoperazone/sulbactam, cefotaxime, ceftriaxone were numerous, and serious, which deserved attention. Studies on the safety of cephalosporin compound preparations in children were few, and the safety of cephalosporin compound preparations in children was doubtful. ADR signal mining was helpful to identify off-label ADRs. Ceftezole may cause off-label ADRs including tremor, face oedema, cyanosis, pallor, rigors, and palpitation. It was also found that the labeling of ADRs in children in cephalosporin instructions and the record of allergic history need to be improved.
The data analyzed in this study is subject to the following licenses/restrictions: The data is provided by Adverse Drug Reaction Monitoring Center of Hubei Province and the data is not publicly available due to institutional confidentiality requirements. Requests to access these datasets should be directed to RH, aHlzMTk4MTA2MTJAMTYzLmNvbQ==.
Conceptualization: RH. Methodology: YC. Formal analysis: LY. Investigation: XS. Resources: RH. Data curation: YC and LY. Writing original draft preparation: YC. Review and editing: YC and XS. Visualization: YZ. Supervision: RH. Project administration: RH. funding acquisition: RH. All authors listed have sufficiently made contributions to the entire content of the article and have given their consent for publication.
This work was supported by National Natural Science Foundation of China (Grant number: 7187040708) and Scientific research project of Hubei Provincial Medical Products Administration (Grant number: 20200106).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank Adverse Drug Reaction Monitoring Center of Hubei Province for providing ADR reports.
Administration (2011). The Reporting and Monitoring Administration Measure on ADR [Online]. Available at: http://www.gov.cn/flfg/2011-05/24/content_1870110.htm (Accessed 6, , 2021).
Administration, N.M.P. (2018). Announcement On the Release of the National Annual Report On Adverse Drug Reactions Monitoring (2017) [Online]. Available at: https://www.nmpa.gov.cn/yaopin/ypggtg/ypqtgg/20180413171401472.html (Accessed 6 1, 2021).
Administration, N.M.P. (2019). Announcement On the Release of the National Annual Report On Adverse Drug Reactions Monitoring (2018) [Online]. Available at: https://www.nmpa.gov.cn/xxgk/ggtg/qtggtg/20191018151301540.html (Accessed 6 1, 2021).
Administration, N.M.P. (2020). Announcement On the Release of the National Annual Report On Adverse Drug Reactions Monitoring (2019) [Online]. Available at: https://www.nmpa.gov.cn/xxgk/yjjsh/ypblfytb/20200413094901811.html (Accessed 6 2021).
Administration, S.F.a.D. (2015). Attention Should Be Paid to Anaphylactic Shock and the Risk of Medication Causing by Cefathiamidine for Injection in Children [Online]. Available at: https://www.nmpa.gov.cn/yaopin/ypjgdt/20151211141601757.html (Accessed 6 2021).
Chen, H., Mo, C., and Huang, B. (2017). Analysis of Clinical Rational Application of Cefotaxime Sodium and Sulbactam Sodium. J. North Pharm. 14 (06), 80–81. doi:10.3969/j.issn.1672-8351.2017.06.074
Ciato, D., Mumbach, A. G., Paez-Pereda, M., and Stalla, G. K. (2017). Currently Used and Investigational Drugs for Cushing´s Disease. Expert Opin. Investig. Drugs 26 (1), 75–84. doi:10.1080/13543784.2017.1266338
Crosby, M. A., and Gump, D. W. (1982). Activity of Cefoperazone and Two Beta-Lactamase Inhibitors, Sulbactam and Clavulanic Acid, against Bacteroides Spp. Correlated with Beta-Lactamase Production. Antimicrob. Agents Chemother. 22 (3), 398–405. doi:10.1128/aac.22.3.398
De Sarro, A., Ammendola, D., Zappala, M., Grasso, S., and De Sarro, G. B. (1995). Relationship between Structure and Convulsant Properties of Some Beta-Lactam Antibiotics Following Intracerebroventricular Microinjection in Rats. Antimicrob. Agents Chemother. 39 (1), 232–237. doi:10.1128/aac.39.1.232
Fu, J., Kuang, S., and Wang, X. (2002). Study on Antibacterial Activity of Cefoperazone Sodium and Tazobactam Sodium In Vivo. Chin. Pharmacol. Bull. 18 (3), 318–320. doi:10.3321/j.issn:1001-1978.2002.03.023
Geng, P. (2017). Clinical Evaluation of Amoxicillin/potassium Clavulanate in the Treatment of Children with Acute Suppurative Tonsillitis. Contemp. Med. 23 (33), 80–82. doi:10.3969/j.issn.1009-4393.2017.33.031
Guo, Y., and Sun, H. (2005). One Case of Anaphylactic Shock Caused by Ceftezole Sodium. Pract. Pharm. Clin. Remedies (02), 30. doi:10.3969/j.issn.1673-0070.2005.02.055
Hauben, M., Madigan, D., Gerrits, C. M., Walsh, L., and Van Puijenbroek, E. P. (2005). The Role of Data Mining in Pharmacovigilance. Expert Opin. Drug Saf. 4 (5), 929–948. doi:10.1517/14740338.4.5.929
Jiang, M., Wang, J., and Yi, J. (2021). Causes and Safety Evaluationof Adverse Drug Reactions Caused by Cephalosporins. Anti-Infection Pharm. 18 (02), 274–277. doi:10.13493/j.issn.1672-7878.2021.02-037
Jiao, Y., Wei, H., and Li, X. (2010). An Analysis of 113 ADR Induced by Ceftezole Sodium in Our Hospital. J. Pediatr. Pharm. 16 (04), 49–50. doi:10.13407/j.cnki.jpp.1672-108x.2010.04.025
Jin, N. (2009). Clinical Analysis on Convulsive Seizures Caused by Using Cephalosporins 12 Uremic Patients. China Pharmaceuticals 18 (11), 74–75. doi:10.3969/j.issn.1006-4931.2009.11.051
Jung, J.-A., Nam, Y.-H., Lee, S.-K., and Kim, J. H. (2017). Analysis of Pediatric Adverse Drug Reactions Reported to Regional Pharmacovigilance Center in Single University Hospital. J. Allergy Clin. Immunol. 139 (2), AB41. doi:10.1016/j.jaci.2016.12.192
Knapp, C. C., Sierra-Madero, J., and Washington, J. A. (1990). Comparative In Vitro Activity of Cefoperazone and Various Combinations of Cefoperazone/sulbactam. Diagn. Microbiol. Infect. Dis. 13 (1), 45–49. doi:10.1016/0732-8893(90)90053-x
Kwon, J. W., Kim, Y. J., Yang, M. S., Song, W. J., Kim, S. H., Cho, S. H., et al. (2019). Results of Intradermal Skin Testing with Cefazolin According to a History of Hypersensitivity to Antibiotics. J. Korean Med. Sci. 34 (50), e319. doi:10.3346/jkms.2019.34.e319
Li, C., Chen, W., and Wang, T. (2010). 4648 Proportion [n] of an Overall Area. Chin. J. New Drugs 19 (9), 759. doi:10.1007/978-3-540-76435-9_10659
Li, J., Green, S. L., Krupowicz, B. A., Capon, M. J., Lindberg, A., Hoyle, P., et al. (2019). Cross-reactivity to Penicillins in Cephalosporin Anaphylaxis. Br. J. Anaesth. 123 (6), E532–E534. doi:10.1016/j.bja.2019.09.011
Li, P., Zeng, X., Fu, J., Zhang, L., and Xie, S. (2003). Toxicologic Experimental Study of Ceftazidime/Tazobactam Sodium (2:1) for Injection. Hainan Med. J. (05), 63–65.
Liu, J. W., Chen, Y. H., Lee, W. S., Lin, J. C., Huang, C. T., Lin, H. H., et al. (2019). Randomized Noninferiority Trial of Cefoperazone-Sulbactam versus Cefepime in the Treatment of Hospital-Acquired and Healthcare-Associated Pneumonia. Antimicrob. Agents Chemother. 63 (8), e00023–19. doi:10.1128/aac.00023-19
Lu, J., Li, P., and Shen, A. (2011). Early-warning Effect of Domestic Professional Academic Journals on Severe Allergic Reaction Resulted from Ceftriaxone Sodium. China Pharm. 22 (6), 481–483. doi:10.1007/s11606-010-1517-4
Lu, Q., Li, Z., Liu, X., and Fu, C. (2018). A Survey on the Rational Use of Antibiotics Among Pediatricians in China in 2016. Chin. J. Pediatr. 56 (12), 897–906. doi:10.3760/cma.j.issn.0578-1310.2018.12.004
Ma, R., Zhang, H., Wei, M., Zhao, C., Hou, J., and Zhao, D. (2003). Pharmacokinetics Study on Cefoperazone and Tazobactam Compound Injection in Health Volunteers. Chin. J. Antibiot. 28 (11), 682–688. doi:10.3969/j.issn.1001-8689.2003.11.012
Ma, Z. (2018). Infective Endocarditis. Henan Med. Res. 27 (01), 90–91. doi:10.1002/9781119547808.ch22
Marinović, I., Marušić, S., Mucalo, I., Mesarić, J., and Bačić Vrca, V. (2016). Clinical Pharmacist-Led Program on Medication Reconciliation Implementation at Hospital Admission: Experience of a Single university Hospital in Croatia. Croat. Med. J. 57 (6), 572–581. doi:10.3325/cmj.2016.57.572
Mingjie, S. U. N., Lu, H., Guixing, D., and Ting, W. (2008). Cefotaxime Sodium/sulbactam Sodium for Injection(2:1). Chin. J. New Drugs 17 (7), 613–617. doi:10.1016/S1872-2075(08)60042-4
Moore, N., Thiessard, F., and Begaud, B. (2005). The History of Disproportionality Measures (Reporting Odds Ratio, Proportional Reporting Rates) in Spontaneous Reporting of Adverse Drug Reactions. Pharmacoepidemiol. Drug Saf. 14 (4), 285–286. doi:10.1002/pds.1058
Pareek, A., Kulkarni, M., Daga, S., Deshpande, A., and Chandurkar, N. (2008). Comparative Evaluation of Efficacy and Safety of Cefotaxime-Sulbactam with Amoxicillin-Clavulanic Acid in Children with Lower Respiratory Tract Infections. Expert Opin. Pharmacother. 9 (16), 2751–2757. doi:10.1517/14656566.9.16.2751
Park, G. M., Seo, J. H., Kim, H. Y., Hwang, Y. W., Na, Y. S., Song, Y. C., et al. (2012). Analysis of Adverse Drug Reactions in Children. J. Allergy Clin. Immunol. 129 (2), AB99. doi:10.1016/j.jaci.2011.12.496
Prakash, S. K., Arora, V., Prashad, R., and Sharma, V. K. (2005). In Vitro activity of Ceftriaxone Plus Tazobactam against Members of Enterobacteriaceae. J. Assoc. Physicians India 53, 595–598.
Shalviri, G., Yousefian, S., and Gholami, K. (2012). Adverse Events Induced by Ceftriaxone: a 10-year Review of Reported Cases to Iranian Pharmacovigilance Centre. J. Clin. Pharm. Ther. 37 (4), 448–451. doi:10.1111/j.1365-2710.2011.01321.x
van Puijenbroek, E. P., Bate, A., Leufkens, H. G., Lindquist, M., Orre, R., and Egberts, A. C. (2002). A Comparison of Measures of Disproportionality for Signal Detection in Spontaneous Reporting Systems for Adverse Drug Reactions. Pharmacoepidemiol. Drug Saf. 11 (1), 3–10. doi:10.1002/pds.668
Wang, F., and Zeng, H. (2021). Clinical Efficacy of Cefotizole Sodium Combined with Levocarnitine in the Treatment of Infective Endocarditis. Chiness J. Clin. Rational Drug Use 14 (06), 76–78. doi:10.15887/j.cnki.13-1389/r.2021.06.028
Wang, K., Lu, J., and Cui, s. (2020). Analysis of Clinical Effect of Cefoperazone Sodium and Sulbactam Sodium. Cardiovasc. Dis. Electron. J. integrated traditional Chin. West. Med. 8 (15), 62. doi:10.16282/j.cnki.cn11-9336/r.2020.15.051
Yang, G. U. O., Dezhu, S. U. N., Min, S., Taijun, H., Lin, Y., and Aidong, W. E. N. (2011). Pharmacokinetics of Ceftriaxone Sodium-Tazobactam Sodium for Injection in Healthy Chinese Volunteers. J. China Pharm. Univ. 42 (4), 354–358. doi:10.1631/jzus.B1000135
Yang, S., Zhang, L., Wang, B., and Li, D. (2010). Therapeutic Effects of Domestic Ceftezole Sodium in the Treatment of Acute Respiratory Tract and Urinary Tract Infection. World Clin. Drugs 31 (09), 543–547.
Yong, L. I. U., Zhijie, Z., Na, L. I., Jimei, S. U. N., Xiuzhen, Z., Xi, Z., et al. (2006). In Vitro antibacterial Activities of Different Formula Cefotaxime/sulbactam. Chin. J. Clin. Pharmacol. 22 (1), 59–64. doi:10.13699/j.cnki.1001-6821.2006.01.016
You, X., Lou, R., Zhang, W., Wang, Y., Yang, X., and Chen, H. (2003). In Vitro and In Vivo Antibacterial Activities of Cefoperazone/tazobactam. Chin. J. New Drugs 12 (5), 338–342. doi:10.3321/j.issn:1003-3734.2003.05.006
Zhang, Z., Lin, Z., Tang, L., and Chen, C. (2010). Analysis of Severe Adverse Drug Reactions Caused by Ceftriaxone Sodium Injection. China J. Mod. Med. 20 (14), 2224–2227.
Zheng, Q., Liu, D., Zhou, R., and Cai, B. (2018). Analysis of 80 Cases of Adverse Drug Reactions Induced by Cephalosporin in Children. J. Harbin Med. Univ. 52 (06), 569–572.
Keywords: cephalosporin, children, spontaneous reporting system, signal detection, measures of disproportionality
Citation: Cai Y, Yang L, Shangguan X, Zhao Y and Huang R (2021) Status and Safety Signals of Cephalosporins in Children: A Spontaneous Reporting Database Study. Front. Pharmacol. 12:736618. doi: 10.3389/fphar.2021.736618
Received: 05 July 2021; Accepted: 05 October 2021;
Published: 20 October 2021.
Edited by:
Maribel Salas, Daiichi Sankyo, United StatesReviewed by:
Hasan Ejaz, Al Jouf University, Saudi ArabiaCopyright © 2021 Cai, Yang, Shangguan, Zhao and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rui Huang, aHlzMTk4MTA2MTJAMTYzLmNvbQ==
†These authors have contributed equally to this work.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.