 Po Huang
Po Huang Xiangchun Zheng
Xiangchun Zheng
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 01 June 2021
Sec. Drugs Outcomes Research and Policies
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.682232
Purpose: The meta-analysis aims to identify whether septic shock patients can benefit from esmolol.
Materials and Methods: The relevant studies from MEDLINE, Cochrane Library, Embase were searched by two independent investigators using a variety of keywords. Stata software (version 12.0, Stata Corp LP, College Station, TX, United States)was used for statistical analysis.
Results: A total of 14 studies were identified and incorporated into the meta-analysis. For overall analysis, the treatment of esmolol was associated with decreased 28-day mortality (RR = 0.66, 95% CI = 0.56–0.77, p < 0.001). Meanwhile, our analysis found that, esmolol could decrease HR (SMD: −1.70; 95% CI: [−2.24−(−1.17)], cTnI (SMD: −1.61; 95% CI: [−2.06−(−1.16)] compared with standard treatment. No significant differences between the two groups were found in MAP, Lac, CI, and SVI.
Conclusion: The findings of this meta-analysis intend to demonstrate that septic shock patients with high heart beats rate might be benefit from esmolol treatment despite enough fluid resuscitation. While, dependent on the study published, with the further development of septic shock, the positive impact of esmolol varies. The appropriate heart rate change interval cannot be confirmed, further high-quality and large-scale RCTs should be performed to verify it and screening more suitable heart rate levels.
Systematic Review Registration: CRD42021239513
Septic shock is typically defined in a clinical setting by low systolic pressure (≤90 mmHg) or mean arterial blood pressure (≤65 mmHg) accompanied by signs of hypoperfusion (Berger Rebecca, 2017). For septic shock, vasoactive drugs are important means to maintain the stability of hemodynamics and ensure the perfusion of major organs (Seymour Christopher and Rosengart Matthew, 2015). Norepinephrine (NE) is the first-line drug for septic shock (Jean-Louis and Post Emiel, 2016). While, long term application of norepinephrine can lead to adverse reactions, such as arrhythmia, the most common of which is tachycardia (Schwinger Robert, 2021). Ventricular tachycardia is a direct response to catecholamine exposure and an independent prognostic factor in patients with septic shock (Hasegawa, et al., 2021).
As a common drug of cardiovascular disease, β-receptor blocker has the function of controlling heart rate, anti-arrhythmia, improving myocardial remodeling, metabolism and immune regulation (Szentmiklosi, et al., 2015). Esmolol is a highly selective β1 receptor blocker with short half-life, which can be pumped drip. It has the advantages of rapid onset, good tolerance and easy regulation, which is the most commonly used preparation in critical care medicine (Alberto, et al., 2021). Considering the negative inotropic effect of β-receptor, it can reduce myocardial contractility and cardiac output, which has the potential risk of further aggravating shock. Thus, β-receptor has not been recommended in the guideline (Shankar-Hari, et al., 2016).
Recently, there have been a number of randomized controlled trials comparing esmolol with standard treatment for septic shock. However, there is still much controversy in the influence of esmolol on mortality, MAP, CI and HR. In view of this, it is necessary to conduct a systematic review to evaluate the efficacy and safety of esmolol in the treatment of septic shock, so as to provide evidence-based evidence for the treatment of septic shock.
This meta-analysis was conducted according to the recommendations and checklist from the preferred reporting items for systematic review and meta-analysis (PRISMA) statement (Panic et al., 2013).
We searched the relevant studies from Pubmed, Cochrane Library, Embase from their inception to March 2021, conference proceedings, and reference lists of relevant articles were also searched.
Inclusion criteria: 1) Participants: we included septic shock patients with tachycardia, regardless of the gender and ethnicity; 2) Interventions: Esmolol; 3) Control: Standard therapy; 4) Outcomes: Primary outcomes: 28-day mortality; secondary outcomes:heart rate (HR), mean arterial pressure (MAP), lactate level, cardiac index (CI), stroke volume index (SVI), cardiac troponin I (cTnI), adverse events; 5) The study design was randomized controlled trial (RCT).
Exclusion criteria: a study with duplicate publication and/or abstract only.
Two reviewers independently identified studies through inclusion criteria by screening the title and abstract of each record and retrieved their full-text if necessary. Any disagreement between the two reviewers was solved with a discussion with a third reviewer. Otherwise, the agreement was accomplished by a consensus.
We designed a pre-defined data extraction form and two reviewers independently extracted the following information from the selected trials: the first author, published year, sample size, intervention, control and outcomes. Any disagreement between two reviewers was discussed with the third reviewer until a consensus was reached.
Quality assessment was performed by two reviewers. RCTs were scored as per the Jadad Scale. According to its principle, one to three indicating a low-quality study and four to five indicating a high-quality study, the maximum of Jadad score is five.
Stata software (version 12.0, Stata Corp LP, College Station, TX, United States) was used for statistical analysis. According to the Cochrane Handbook of Systematic Reviews, we chose risk ratios (RRs) and 95% confidence intervals (CIs) as the appropriate parameters to evaluate the dichotomous outcomes. In terms of continuous outcomes, the mean difference and its 95% CI were used. Between-study heterogeneity was evaluated using an I2 test (25% or lower is defined as low heterogeneity, 50% as moderate heterogeneity, 75% as high heterogeneity). The fixed-effect model was applied if there was no or low heterogeneity, and pooled RRs were estimated using the Mantel-Haenszel method. Publication bias was assessed if there are more than ten studies in one outcome. All hypotheses were tested at the alpha = 0.05 level.
We identified 246 records based on this search strategy, and 86 potentially eligible records were obtained after removing duplicate publications. After screening the titles and abstracts, a total of 67 studies were excluded. Fourteen studies with 927 participants were included (Figure 1). The characteristics of the included studies are presented in Table 1. Risk of bias for the included studies were assessed by the Jadad scale, and the result are presented in Supplementary Table S1.
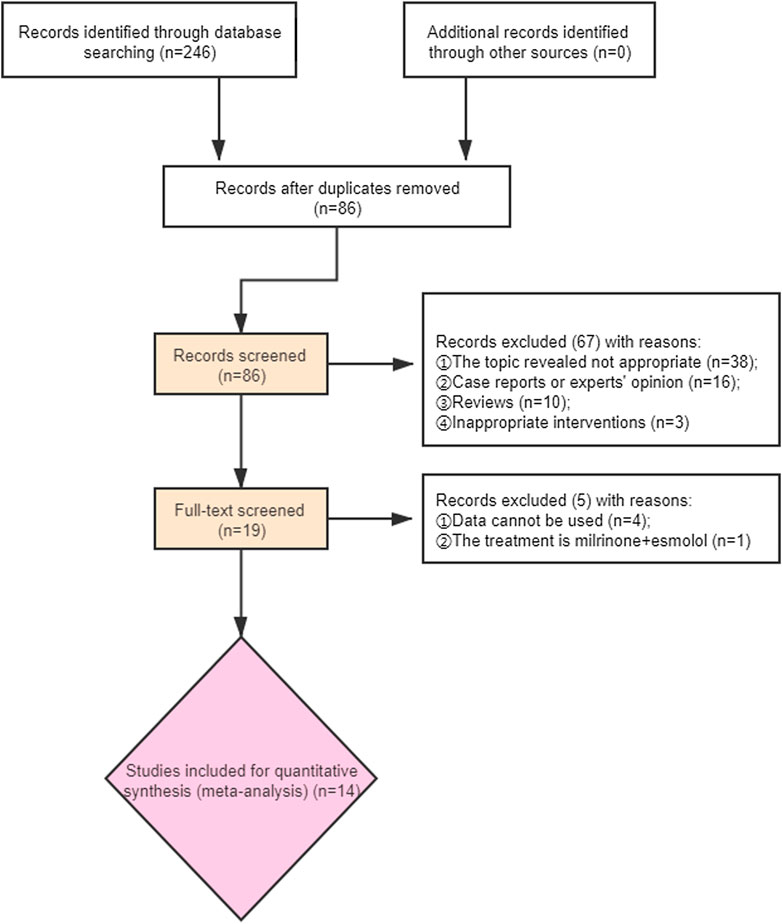
FIGURE 1. Flow chart of included studies selection.
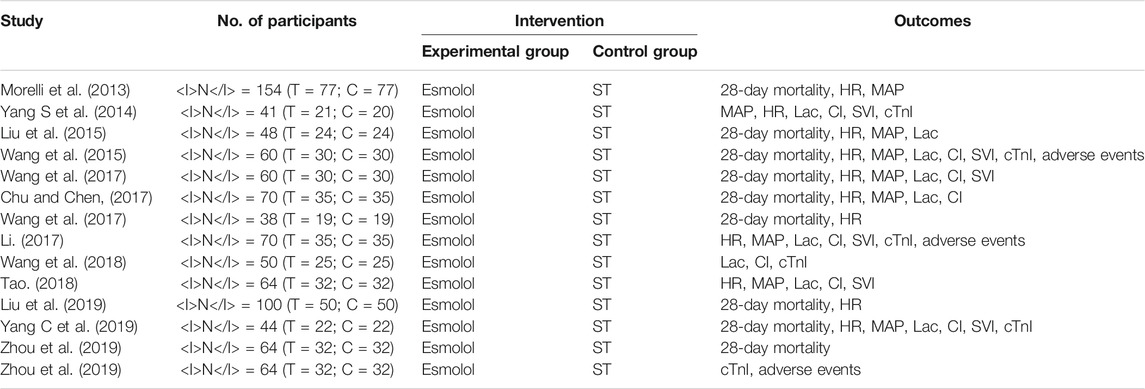
TABLE 1. the characteristics of the included studies.
The primary outcome is 28-day mortality. Nine studies (Morelli et al., 2013; Liu et al., 2015; Wang et al., 2015; Wang et al., 2017; Chu and Chen, 2017; Wang et al., 2017; Liu et al., 2019; Yang C et al., 2019; Zhou et al., 2019) with 708 participants reported 28-day mortality. The result showed that 28-day mortality is lower in esmolol group than control group (RR = 0.66, 95% CI = (0.56,0.77), p < 0.01) (Figure 2).
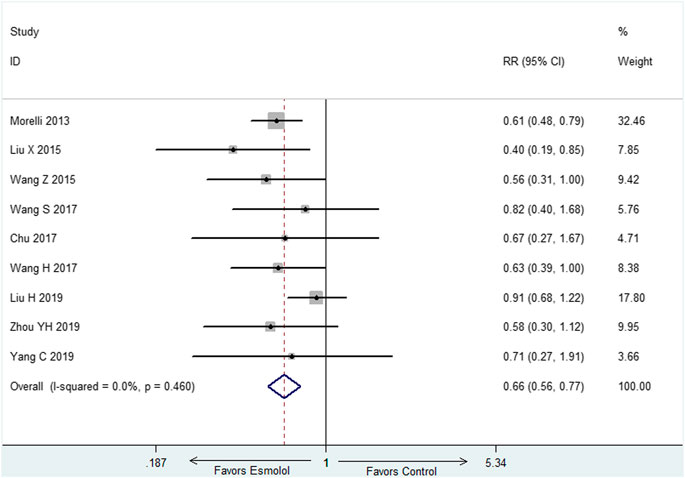
FIGURE 2. Forest plot of 28-day mortality.
Eleven studies (Morelli et al., 2013; Yang et al., 2014; Liu et al., 2015; Wang et al., 2015; Wang et al., 2017; Chu and Chen, 2017; Wang et al., 2017; Li, 2017; Tao, 2018; Liu H et al., 2019; Yang C et al., 2019) employed HR at 72-h as outcome measure. There was obvious heterogeneity among these included studies, thus, random effect model was utilized for statistical analysis. The results indicated that esmolol plus standard treatment could decrease HR when compared with standard therapy (SMD: −1.70; 95% CI: [−2.24−(−1.17)] (Figure 3).
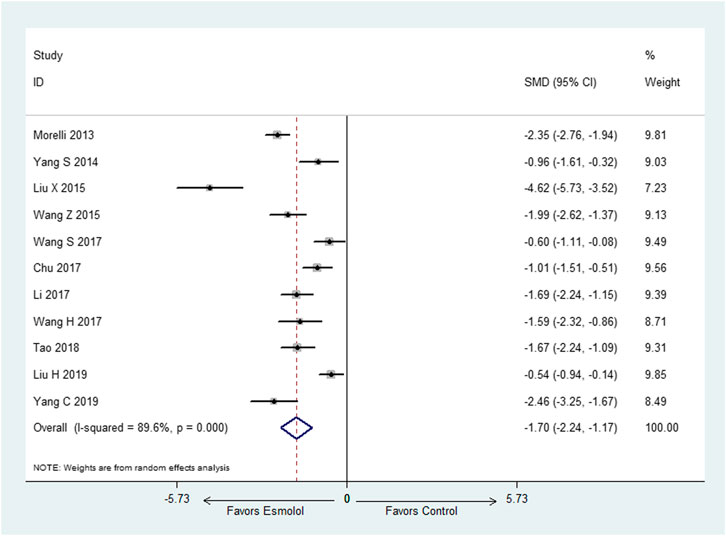
FIGURE 3. Forest plot of HR.
There were nine studies (Morelli et al., 2013; Yang et al., 2014; Liu et al., 2015; Wang et al., 2015; Wang et al., 2017; Chu and Chen, 2017; Li, 2017; Tao, 2018; Yang C et al., 2019) reported MAP at 72-h, we selected fixed effect model since there was no heterogeneity in both of the two subgroups (I2 = 0). The meta-analysis showed that compared with standard therapy, adding esmolol has no influence on MAP at 72-h (SMD: 0.13; 95% CI: −0.03–0.29) (Figure 4).
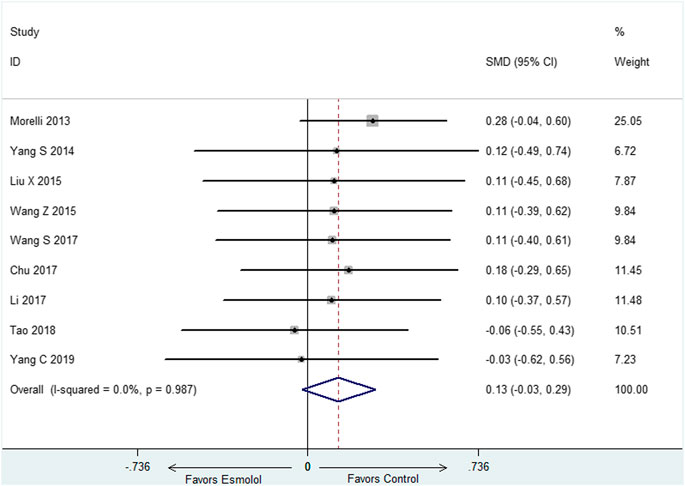
FIGURE 4. Forest plot of MAP.
Six studies (Yang et al., 2014; Wang et al., 2015; Li, 2017; Wang et al., 2018; Yang C et al., 2019; Zhou et al., 2019) with 329 participants reported cTnI at 72-h, random effect model was utilized (I2 = 68.6%). The result demonstrated that cTnI at 72-h was decreased in the group of esmolol compared with standard treatment (SMD: −1.61; 95% CI: [−2.06−(−1.16)] (Figure 5).
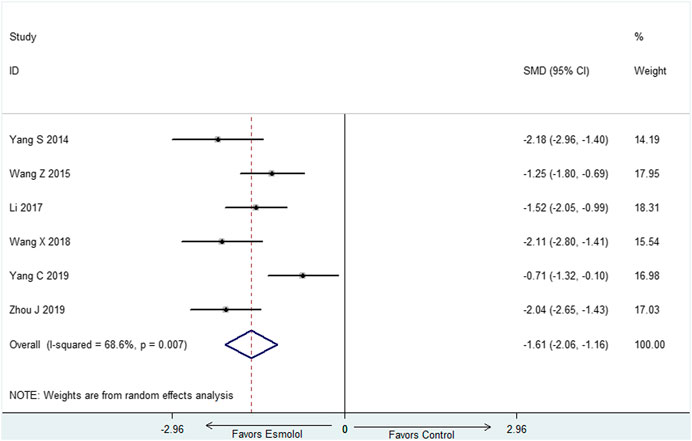
FIGURE 5. Forest plot of cTnI.
Random effect models were utilized (I2> 75%) in the above three outcomes. The results showed that there was no influence on Lac, CI and SVI at 72-h in the group of esmolol compared with standard treatment (Supplementary Figures S1–S3).
Three studies reported adverse events and there was no significant difference in the adverse effects among the two groups.
The analysis aims to identify the efficacy and safety of esmolol for septic shock. The results showed a survival benefit with esmolol compared with standard treatment. Meanwhile, our analysis found that the use of esmolol could decrease HR and cTnI with no influence on MAP, CI, SVI, and Lac (Table 2). Thus, based on the results of our analysis, esmolol is recommended for septic shock patients with tachycardia.
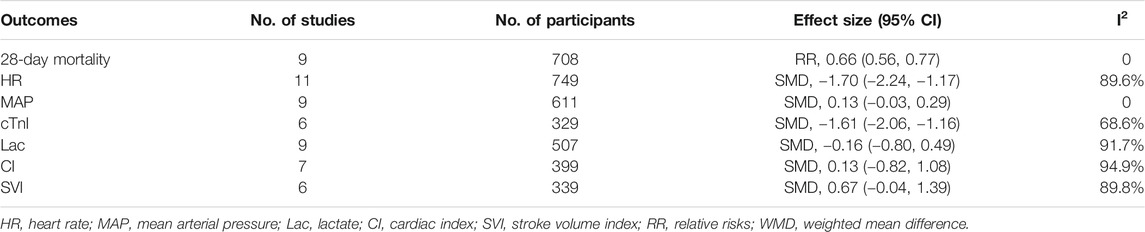
TABLE 2. Summary of meta-analysis.
As we all known, Morelli et al. (Morelli et al., 2013) conducted the first randomized controlled study to evaluate the efficacy and safety of esmolol in septic shock. Surprisingly, this study reported a substantial reduction in mortality with a 28 days mortality of 49.4% in the esmolol group and 80.5% in the control group. Meanwhile, it is interesting that norepinephrine and resuscitative fluid volume requirements were reduced in the esmolol group whilst maintaining MAP ≥65 mmHg. This study has raised questions and stimulated interest into why, when and in whom esmolol are beneficial.
First, septic shock related cardiac dysfunction is mainly associated with prolonged catecholamine exposure and β receptor overactivation (Suzuki et al., 2017). Long-term excessive stimulation can lead to imbalance of myocardial energy supply. Rapid ventricular rate is a direct response to catecholamine exposure, and it is also an independent prognostic factor. The recent study demonstrated that the application of esmolol can up-regulate the β-receptor on the surface of myocardial cells, restore heart rate variability and sensitivity to catecholamine (Orbegozo et al., 2014). In addition, the negative frequency effect of β-blocker prolonged left ventricular diastolic period, increased left ventricular ejection fraction and left ventricular blood volume (Harada et al., 2020). What’s more, the related studies reported that esmolol can reduce the expression of chemokines and inflammatory factors in cardiac dysfunction (Karlsen et al., 2019).
Second, the appropriate timing of esmolol administration has not yet been determined. Tachycardia is the main compensatory mechanism to prevent the decrease of cardiac output (Mohammed et al., 2021). At this time, if the heart rate is reduced blindly, it may lead to organ perfusion insufficiency and damage organ function. Sufficient fluid resuscitation is important for septic shock, whereas, esmolol maybe useful if the heart rate rise above 100 despite initial resuscitation. Usually, if tachycardia still exists after sufficient fluid resuscitation and exclusion of common causes such as hypovolemia, it is considered that it may be caused by sympathetic excitation, and esmolol is more appropriate at this time. However, the standard of sufficient fluid resuscitation is still lack, which could be evaluated by bedside echocardiography and Pulse Contour Cardiac Output (PiCCO).
Last but not least, relevant studies have shown that the increase of heart rate is positively correlated with the mortality of patients with septic shock, so septic shock with tachycardia is the indication of esmolol (Lee Young et al., 2019; DellaVolpe Jeffrey et al., 2015; Emmanuel et al., 2018). Most of the included studies selected septic shock patients with HR ≥ 100 beats/min. However, the range of heart rate is too large, and the upper limit of heart rate is not limited. Liu et al. reported that the 28-day mortality was higher in esmolol group compared with control group in septic shock patients with HR ≥ 120, though there was no statistical difference between two group (Liu et al., 2019). This finding suggests that patients with septic shock whose heart rate is more than 120 beats/min may not benefit from esmolol. After further review of the included studies, we found that only one study (Liu et al., 2019) performed the subgroup analyze for heart rate in the outcome of mortality. The data demonstrated that there was a positive correlation between heart rate and mortality in both groups. By logistic regression analysis, it was found that 28-day mortality risk of septic shock patients increased by 1.568 times for every 10 beats/min increase in initial heart rate, and increased by 2.207 times for every 10 beats/min increase in overall heart rate after treatment (Liu et al., 2019). Compared with control group, septic shock patients could benefit from esmolol when heart rate rang from 110 to120. Whereas, the benefit cannot be obtained when heart rate rang from 100 to 110 or 120 to 130. Dependent on the study published, with the further development of septic shock, the positive impact of esmolol varies. Based on the existing evidence, the upper limit of heart rate cannot be confirmed, and more studies are needed to confirm the precise heart rate range. Besides, the severity of the disease (such as SOFA and APACHE Ⅱ score), complications, basic heart conditions will affect the efficacy of esmolol. Thus, how to distinguish the benefit patients of esmolol in patients with septic shock needs further study.
Though there exit three similar reviews (Yu et al., 2016; Liu et al., 2018; Li et al., 2020), there are some differences between our review and the three reviews. First, we found that some of the included studies in the previous reviews were repetitive studies. Second, most of the studies were not included, which limits the credibility of the results. Third, our review included the largest number of studies and the most comprehensive evaluation index to evaluated the efficacy and safety of esmolol for septic shock. Through our review, we found that through esmolol could decrease 28-day mortality in septic shock, the appropriate heart rate range is unclear, which limited the application in clinic. Through further reading of the included studies, we found that most of the studies set the heart rate interval above 100 beats/min, and they did not set the upper limit. One of the studies found that esmolol had no significant protective effect on death when the heart rate exceeded 120 beats per min (Liu H et al., 2019). Thus, we speculate that esmolol may be more suitable for septic shock patients with heart rate of 100–120 beats/min. Of course, this conjecture needs to be confirmed by more high-quality randomized controlled trials in the future.
Several limitations exit in this review. First, most of the included studies were performed in China, which cannot represent patients with septic shock in other regions. Second, most of the included studies were published in Chinese, only three studies (Morelli et al., 2013; Liu et al., 2015; Wang et al., 2015) were published in English. Third, Since the treatment of septic shock is comprehensive, the effects of other united medication can't exclude.
The findings of this meta-analysis intend to demonstrate that septic shock patients with high heart beats rate might be benefit from esmolol treatment despite enough fluid resuscitation. While, dependent on the study published, with the further development of septic shock, the positive impact of esmolol varies. The appropriate heart rate change interval cannot be confirmed, further high-quality and large-scale RCTs should be performed to verify it and screening more suitable heart rate levels.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
PH and XF created the research idea and designed the study. PH, XZ, and ZL acquired the data. PH, ZL, and XF analyzed and interpreted the data. PH and ZL performed the statistical analysis. Each author contributed important intellectual content during manuscript drafting and accepts accountability for the overall work.
This study was supported by the national natural science foundation of China (No.81673934); Basic scientific research business project of Beijing University of traditional Chinese medicine in 2021 (2021-JYB-XJSJJ-065); Key emergency department of Beijing Administration of Traditional Chinese Medicine (040203001017).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.682232/full#supplementary-material
Alberto, Zangrillo., Elena, Bignami., Noè, Beatrice., Nardelli Pasquale., , Margherita, Licheri., Gerli, Chiara., et al. (2021). Esmolol in Cardiac Surgery: A Randomized Controlled Trial. J. Cardiothorac. Vasc. Anesth. 35 (4), 1106–1114. doi:10.1053/j.jvca.2020.12.029
Berger Rebecca, E. (2017). Rivers Emanuel., Levy Mitchell M.Management of Septic Shock. N. Engl. J. Med. 376 (23), 2282–2285. doi:10.1056/NEJMclde1705277
Chu, Xiaoqiong., and Chen, Weibiao. (2017). Effect of Esmolol on Cardiac Insufficiency Caused by Septic Shock. Chin. J. Rural Med. Pharm. 24 (14), 7–8. doi:10.3969/j.issn.1006-5180.2017.14.003
Chun, Yang., Wang, Cheng., Ting, Chen., Wang, Jinpeng., Weng, Yinyan., Lai, Zhizhen., et al. (2019). Clinical Study on the Cardioprotection of Esmolol in Patients with Septic Shock. Chin. J. Crit. Care Med. (Electronic Edition) 12 (1), 15–19. doi:10.3877/cma.j.issn.1674-6880.2019.01.003
DellaVolpe Jeffrey, D., Moore Jason, E., and Pinsky Michael, R. (2015). Arterial Blood Pressure and Heart Rate Regulation in Shock State. Curr. Opin. Crit. Care 21 (5), 376–380. doi:10.1097/MCC.0000000000000239
Emmanuel, Boselli., Matthias, Jacquet-Lagrèze., Ayoub, Jean-Yves., Lionel, Bouvet., Olivier, Dauwalder., Mansour, Christelle., et al. (2018). Effects of Esmolol on Systemic Hemodynamics and Heart Rate Variability Measured Using the Analgesia/Nociception Index in Resuscitated Piglets with Pseudomonas aeruginosa Septic Shock. J. Vet. Emerg. Crit. Care (San Antonio) 28 (5), 447–456. doi:10.1111/vec.12756
Harada, Daisuke., Hidetsugu, Asanoi., Noto, Takahisa., and Takagawa, Junya. (2020). The Impact of Right Ventricular Dysfunction on the Effectiveness of Beta-Blockers in Heart Failure with Preserved Ejection Fraction. J. Cardiol. 76 (4), 325–334. doi:10.1016/j.jjcc.2020.05.001
Hasegawa, D., Sato, R., Narut., P., Nishida, K., Takahashi, K., Yatabe, T., et al. (2021). Effect of Ultrashort-Acting β-Blockers on Mortality in Patients with Persistent Tachycardia Despite Initial Resuscitation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Chest. doi:10.1016/j.chest.2021.01.009
Jean-Louis, Vincent., and Post Emiel, H. (2016). Sepsis: Vasopressin: a First-Line Agent for Septic Shock? Nat. Rev. Nephrol. 12 (12), 718–719. doi:10.1038/nrneph.2016.144
Karlsen, H., Bergan, H. A., Halvorsen, P. S., Sunde, K., Qvigstad, E., Andersen, G. Ø., et al. (2019). Esmolol for Cardioprotection during Resuscitation with Adrenaline in an Ischaemic Porcine Cardiac Arrest Model. Intensive Care Med. Exp. 7 (1), 65. doi:10.1186/s40635-019-0279-5
Lee Young, R., Michael Sadanand, Seth., Soney, Dylan., and Dai, Hanyu. (2019). Benefits of Beta-Blockade in Sepsis and Septic Shock: A Systematic Review. Clin. Drug Investig. 39 (5), 429–440. doi:10.1007/s40261-019-00762-z
Li, Ji'an., Sun, Wanli., Guo, Yuqi., Ren, Yunxia., Li, Yangjun., and Yang, Zhenhua. (2020). Prognosis of β-adrenergic Blockade Therapy on Septic Shock and Sepsis: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. Cytokine 126 (undefined), 154916. doi:10.1016/j.cyto.2019.154916
Li, Songlin. (2017). Clinical Study on Esmolol in Improvement of Septic Shock Cardiac Function. Drugs & Clinic 32 (7), 1229–1233. doi:10.7501/j.issn.1674-5515.2017.07.015
Liu, H., Ding, X. F., Zhang, S. G., Wang, H. X., Luo, Y. G., Duan, X. G., et al. (2019). Effect of Esmolol in Septic Shock Patients with Tachycardia: a Randomized Clinical Trial. Zhonghua Yi Xue Za Zhi. 99 (17), 1317–1322. doi:10.3760/cma.j.issn.0376-2491.2019.17.009
Liu, Ping., Wu, Qi., Tang, Yu., Zhou, Zhiguo., and Feng, Malong. (2018). The Influence of Esmolol on Septic Shock and Sepsis: A Meta-Analysis of Randomized Controlled Studies. Am. J. Emerg. Med. 36 (3), 470–474. doi:10.1016/j.ajem.2017.11.013
Liu, Xinqiang., Huang, Weiping., Wen, Miaoyun., Zeng, Wenxin., Jiang, Wenqiang., Chen, Shenglong., et al. (2015). Esmolol Improves Clinical Outcome and Tissue Oxygen Metabolism in Patients with Septic Shock through Controlling Heart Rate. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 27 (9), 759–763.
Mohammed, Sameer., Baruah, Sudip. Dutta., Menon, Sabarinath., Baiju Sasi, Dharan., Ramanan Sowmya, V., Raja Javid, S., et al. (2021). Overdrive Suppression of Postoperative Sustained Ventricular Tachycardia by Atrial Pacing and its Hemodynamic Effect. Ann. Pediatr. Cardiol. 14 (1), 88–90. doi:10.4103/apc.APC_174_19
Morelli, Andrea., Christian, Ertmer., Martin, Westphal., Rehberg, Sebastian., Kampmeier, Tim., Ligges, Sandra., et al. (2013). Effect of Heart Rate Control with Esmolol on Hemodynamic and Clinical Outcomes in Patients with Septic Shock: a Randomized Clinical Trial. JAMA 310 (16), 1683–1691. doi:10.1001/jama.2013.278477
Orbegozo Cortes, D., Njimi, H., Dell'Anna, A. M., and Taccone, F. S. (2014). Esmolol for Septic Shock: More Than Just Heart Rate Control? Minerva Anestesiol 80 (2), 254–258.
Panic, Nikola., Emanuele, Leoncini., de Belvis Giulio., , Walter, Ricciardi., and Boccia, Stefania. (2013). Evaluation of the Endorsement of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement on the Quality of Published Systematic Review and Meta-Analyses. PLoS One 8 (12), e83138. doi:10.1371/journal.pone.0083138
Schwinger Robert, H. G. (2021). Pathophysiology of Heart Failure. Cardiovasc. Diagn. Ther. 11 (1), 263–276. doi:10.21037/cdt-20-302
Seymour Christopher, W., and Rosengart Matthew, R. (2015). Septic Shock: Advances in Diagnosis and Treatment. JAMA 314 (7), 708–717. doi:10.1001/jama.2015.7885
Shankar-Hari, Manu., Phillips Gary, S., Levy Mitchell, L., Seymour Christopher, W., Liu Vincent, X., Deutschman Clifford, S., et al. (2016). Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 315 (8), 775–787. doi:10.1001/jama.2016.0289
Suzuki, Takeshi., Suzuki, Yuta., Okuda, Jun., Kurazumi, Takuya., Suhara, Tomohiro., Ueda, Tomomi., et al. (2017). Sepsis-induced Cardiac Dysfunction and β-adrenergic Blockade Therapy for Sepsis. J. Intensive Care 5 (undefined), 22. doi:10.1186/s40560-017-0215-2
Szentmiklosi, A. József., Norbert, Szentandrássy., Bence, Hegyi., Horvath, Balázs., and Magyar, János. (2015). Magyar János., Bányász Tamás., etChemistry, Physiology, and Pharmacology of β-adrenergic Mechanisms in the Heart. Why Are β-blocker Antiarrhythmics superior?. Curr. Pharm. Des. 21 (8), 1030–1041. doi:10.2174/1381612820666141029111240
Tao, Yuanzhuo. (2018). Effects of Esmolol on Hemodynamics and Inflammatory Response in Patients with Septic Shock. Mod. Med. Health Res. 000 (003), 69.
Wang, Haiyan., Liu, Xianghua., Wang, Jianli., Qu, Xiuhui., and Song, Huifang. (2017). J. Clin. Med. 4 (5), 797–798. doi:10.3877/j.issn.2095-8242.2017.05.004
Wang, Shupeng., Li, Min., Duan, Jun., Yi, Li., Huang, Xu., Chen, Desheng., et al. (2017). Effect of Esmolol on Hemodynamics and Clinical Outcomes in Patients with Septic Shock. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 29 (5), 390–395. doi:10.3760/cma.j.issn.2095-4352.2017.05.002
Wang, Xuliang., Sun, Guolei., and Zhao, Jiangang. (2018). Protective Effect of Esmolol on Cardiac Function in Patients with Septic Shock. J. China Prescription Drug 16 (8), 81–82. doi:10.3969/j.issn.1671-945X.2018.08.052
Wang, Zenggeng., Wu, Qinghua., Nie, Xiangbi., Guo, Jinghua., and Yang, Chunli. (2015). Combination Therapy with Milrinone and Esmolol for Heart protection in Patients with Severe Sepsis: a Prospective, Randomized Trial. Clin. Drug Investig. 35 (11), 707–716. doi:10.1007/s40261-015-0325-3
Yang, Shengqiang., Liu, Zhen., Yang, Wenbao., Zhang, Guizhen., Hou, Baojun., Liu, Jihua., et al. (2014). Effects of the β-blockers on Cardiac protection and Hemodynamics in Patients with Septic Shock: a Prospective Study. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 26 (10), 714–717. doi:10.3760/cma.j.issn.2095-4352.2014.10.007
Yu, Yanwu., Sun, Tongwen., Wan, Youdong., Liu, Ziqi., and Kan, Quancheng. (2016). Effects of β-blockers in Patients with Septic Shock: a Meta Analysis. Natl. Med. J. China 96 (7), 570–574. doi:10.3760/cma.j.issn.0376-2491.2016.07.017
Zhou, Jie., Yang, Aixiang., and Tao, Weiyi. (2019). Effects of Esmolol on Cardiac Function, Inflammatory Markers and Prognosis in Elderly Patients with Septic Shock. Clin. Medication J. 17 (12), 57–60. doi:10.3969/j.issn.1672-3384.2019.12.014
Keywords: septic shock, tachycardia, esmolol, meta-analysis, systematic review
Citation: Huang P, Zheng X, Liu Z and Fang X (2021) The Efficacy and Safety of Esmolol for Septic Shock: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Front. Pharmacol. 12:682232. doi: 10.3389/fphar.2021.682232
Received: 18 March 2021; Accepted: 13 May 2021;
Published: 01 June 2021.
Edited by:
Saraschandra Vallabhajosyula, Emory University, United StatesReviewed by:
Rolf Bass, Retired, Berlin, GermanyCopyright © 2021 Huang, Zheng, Liu and Fang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaolei Fang, ZmFuZ3hpYW9sZWlfNTg2QDEyNi5jb20=; Zhi Liu, bGl1emhpXzcyNUAxMjYuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.