
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 21 September 2021
Sec. Pharmacogenetics and Pharmacogenomics
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.648262
This article is part of the Research Topic NSAIDs Pharmacogenomics View all 9 articles
 Yolanda Macías1,2
Yolanda Macías1,2 Jesús M. García-Menaya3,4
Jesús M. García-Menaya3,4 Manuel Martí1,2
Manuel Martí1,2 Concepción Cordobés3,4
Concepción Cordobés3,4 Raquel Jurado-Escobar5,6José A. Cornejo-García5,6
Raquel Jurado-Escobar5,6José A. Cornejo-García5,6 María J. Torres6,7
María J. Torres6,7 Natalia Blanca-López8,9Gabriela Canto8,9
Natalia Blanca-López8,9Gabriela Canto8,9 Miguel Blanca8,9
Miguel Blanca8,9 José J. Laguna9,10
José J. Laguna9,10 Joan Bartra11,12
Joan Bartra11,12 Ana Rosado13Javier Fernández14,15
Ana Rosado13Javier Fernández14,15 Elena García-Martín1,2
Elena García-Martín1,2 José A. G. Agúndez1,2*
José A. G. Agúndez1,2*Cross-hypersensitivity to non-steroidal anti-inflammatory drugs (NSAIDs) is a relatively common, non-allergic, adverse drug event triggered by two or more chemically unrelated NSAIDs. Current evidence point to COX-1 inhibition as one of the main factors in its etiopathogenesis. Evidence also suggests that the risk is dose-dependent. Therefore it could be speculated that individuals with impaired NSAID biodisposition might be at increased risk of developing cross-hypersensitivity to NSAIDs. We analyzed common functional gene variants for CYP2C8, CYP2C9, and CYP2C19 in a large cohort composed of 499 patients with cross-hypersensitivity to NSAIDs and 624 healthy individuals who tolerated NSAIDs. Patients were analyzed as a whole group and subdivided in three groups according to the main enzymes involved in the metabolism of the culprit drugs as follows: CYP2C9, aceclofenac, indomethacin, naproxen, piroxicam, meloxicam, lornoxicam, and celecoxib; CYP2C8 plus CYP2C9, ibuprofen and diclofenac; CYP2C19 plus CYP2C9, metamizole. Genotype calls ranged from 94 to 99%. No statistically significant differences between patients and controls were identified in this study, either for allele frequencies, diplotypes, or inferred phenotypes. After patient stratification according to the enzymes involved in the metabolism of the culprit drugs, or according to the clinical presentation of the hypersensitivity reaction, we identified weak significant associations of a lower frequency (as compared to that of control subjects) of CYP2C8*3/*3 genotypes in patients receiving NSAIDs that are predominantly CYP2C9 substrates, and in patients with NSAIDs-exacerbated cutaneous disease. However, these associations lost significance after False Discovery Rate correction for multiple comparisons. Taking together these findings and the statistical power of this cohort, we conclude that there is no evidence of a major implication of the major functional CYP2C polymorphisms analyzed in this study and the risk of developing cross-hypersensitivity to NSAIDs. This argues against the hypothesis of a dose-dependent COX-1 inhibition as the main underlying mechanism for this adverse drug event and suggests that pre-emptive genotyping aiming at drug selection should have a low practical utility for cross-hypersensitivity to NSAIDs.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are the most common drugs used to relieve pain and to decrease inflammation and fever. NSAIDs are among the most used drugs in the world, and they comprise a wide range of chemically unrelated compounds. It is estimated that over 30 million people worldwide use these medications daily, not only as prescription drugs but also over-the-counter (OTC) (Singh, 2000). As a general rule, prescription NSAIDs are effective to relieve chronic musculoskeletal pain and inflammation, and OTC NSAIDs, normally at lower doses, are effective to relieve acute or minor aches and pains. These drugs are quite safe, but despite being available OTC in many countries, they could bring about adverse drug reactions (ADRs).
ADRs have been reported in approximately 1.5% of the patients with at least one NSAIDs prescribed and around 23.3% of the adverse drug reactions to NSAIDs are due to hypersensitivity reactions (Blumenthal et al., 2016, 2017). One specific type of ADRs, hypersensitivity drug reactions (HDRs) can be divided into two main groups: on one side those which are initiated by specific immunological mechanisms (also described as drug allergy), the response is induced by a single drug, and patients are classified as selective drug responders. These reactions can be IgE-mediated, designated as immediate drug allergy, or T cell-mediated, designated as delayed drug allergy. On the other side, HDRs whose mechanisms are nonimmunological (also described as nonallergic hypersensitivity), the reaction is induced by two or more chemically unrelated drugs, and patients are classified as cross-intolerant or cross-hypersensitivity subjects (Johansson et al., 2004; Szczeklik et al., 2009; Doña et al., 2011).
According to their clinical presentation, cross-hypersensitivity reactions could be classified as NSAIDs-exacerbated respiratory disease (NERD), NSAIDs-exacerbated cutaneous disease (NECD), and NSAID-induced urticaria/angioedema (NIUA) (Kowalski et al., 2013). These non-immunological reactions are believed to be originated via inhibition of cyclooxygenase 1 (COX-1) enzyme and the release of histamine and sulphidopeptide leukotrienes (Kowalski et al., 2007; Doña et al., 2018; Bakhriansyah et al., 2019; Li and Laidlaw, 2019; Mastalerz et al., 2019). In this context, it is important to bear in mind that NSAIDs antagonize inflammation by interfering with the function of cyclooxygenases, and therefore their association with nonallergic hypersensitivity might be related to disequilibrium in the arachidonic acid degradation pathways, that is, interference with the formation of prostaglandins and thromboxanes, thus resulting in the shunting of arachidonic acid metabolism towards the 5-lipoxygenase pathway, and the consequent increase in the release of cysteinyl leukotrienes (Sánchez-Borges, 2010; Caimmi et al., 2012).
Interindividual variability in drug metabolism is likely to be involved in HDRs (Agúndez et al., 2015a, Agúndez et al., 2018; García-Martín et al., 2015; Ariza et al., 2016; Sánchez-Gómez et al., 2016; Plaza-Serón et al., 2018). A substantial part of such interindividual variability is associated with polymorphisms in genes coding drug-metabolizing enzymes. NSAIDs are extensively metabolized by Cytochrome P450 2C enzymes (CYP2C) and CYP2C gene variants are strongly related to the pharmacokinetics, pharmacological effects, and adverse drug reactions for many NSAIDs (Agúndez JA. et al., 2009; Agúndez et al., 2009 J.; Agúndez et al., 2011; Szczeklik et al., 2009; Martínez et al., 2014; Macías et al., 2020; Theken et al., 2020). Impaired CYP2C metabolism brings about decreased clearance, increased drug exposure, and therefore, increased COX-inhibition. Since cross-hypersensitivity induced by NSAIDs is believed to be related to COX-inhibition, it is conceivable that individuals with genetic alterations leading to impairment in NSAID metabolism would be more prone to developing cross-hypersensitivity induced by these drugs. However, no studies have been conducted to test such a hypothesis. We analyzed such putative association in a large study group with enough sample size to support or discard a major association between common CYP2C functional gene variants and the risk of developing cross-hypersensitivity with NSAIDs metabolized by these enzymes.
A total cohort of 1.123 participants was analyzed in this study, all were Spanish individuals with South European Ancestry. Ancestry was self-reported. Four hundred and ninety-nine patients who developed hypersensitivity to acetylsalicylic acid (ASA) and one or more chemically different NSAIDs mainly metabolized by CYP2C enzymes were included in the study. Their mean age was 42 (SD = 17.46) years. Also, six hundred and twenty-four healthy individuals with an average age of 21 (SD = 2.32) years participated as control subjects. All control individuals tolerated NSAIDs that are CYP2C substrates. Patients and controls were recruited between 2007 and 2020 from the Allergy Services of the following hospitals in Spain: Badajoz University Hospital, Málaga University Hospital, Madrid Cruz Roja Hospital, Barcelona Clinic Hospital, Madrid Infanta Leonor Hospital, Alcorcón University Hospital, and Elche University Hospital. Control individuals were selected among the staff and students assessed through anamnesis, clinical history and/or self-reported tolerance to COX-1 inhibitors. Inclusion criteria for the patients were as follows: Diagnosis of cross-hypersensitivity (Pérez-Alzate et al., 2017; Blanca-López et al., 2018, Blanca-López et al., 2019) by clinical history and a positive drug provocation test, for one or more of the following NSAIDs: ibuprofen, diclofenac, aceclofenac, indomethacin, naproxen, piroxicam, meloxicam, lornoxicam, celecoxib, and metamizole. ASA-positivity was included as a requisite in the diagnosis because in cross-reactive (non-allergic) hypersensitivity patients react to all strong COX-1 inhibitors, including ASA, whereas allergic hypersensitivity patients tolerate ASA (Kowalski et al., 2013; Pérez-Alzate et al., 2017; Angeletti et al., 2020); besides, CYP2C9 plays a role in ASA metabolism (Thiessen, 1983; Hutt et al., 1986; Bigler et al., 2001; Palikhe et al., 2011; Gómez-Tabales et al., 2020). Patients who presented with hypersensitivity triggered by other NSAIDs whose metabolism is not mainly catalyzed by CYP2C enzymes (including clonixinate, dexketoprofen, ketorolac, etofenamate, ketoprofen, piketoprofen, propifenazone, phenylbutazone, aminophenazone, acetaminophen, etoricoxib and oxyphenbutazone) were excluded from the study. The study was conducted according to the principles of the Declaration of Helsinki and approved by the Ethics Committees of each participating hospital. Written informed consent was obtained from all the participants involved in the study.
The main NSAIDs (Figure 1) that triggered the hypersensitivity reaction are shown in Table 1. The clinical presentations stratified according to the culprit drugs involved are summarized in Table 2.
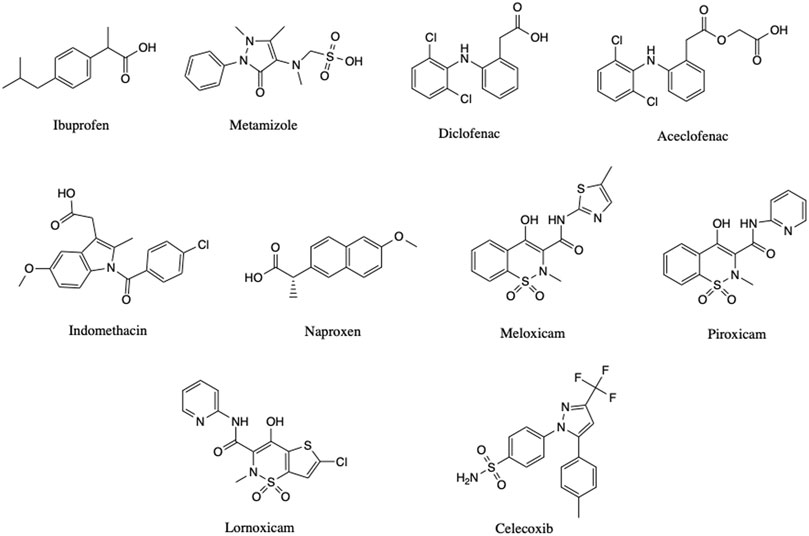
FIGURE 1. Drug structures.
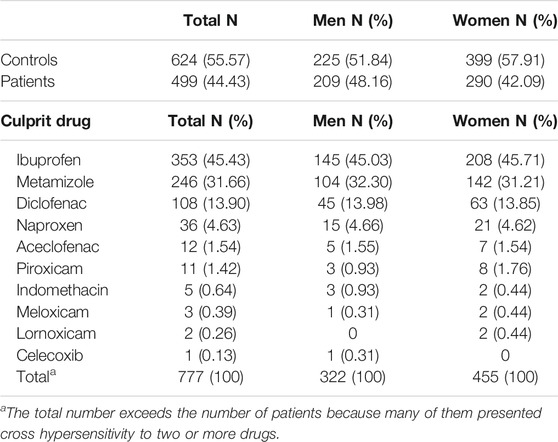
TABLE 1. Characteristics of the individuals and drug involved in NSAID-induced cross-hypersensitivity in this study.
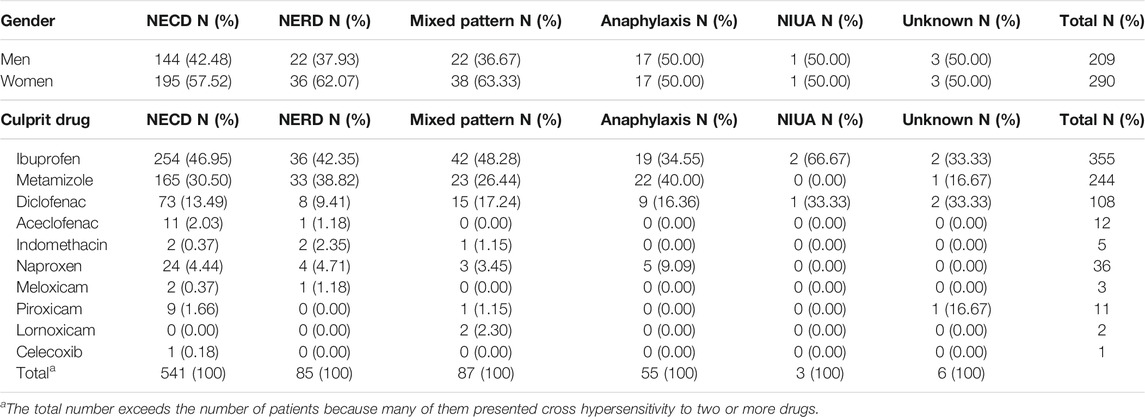
TABLE 2. Gender and clinical presentation of NSAID-induced cross-hypersensitivity in this study.
Genomic DNA was obtained and purified by following standard procedures and then genotypic analyses were performed using a real-time quantitative polymerase chain reaction (qPCR). The target SNVs were selected according to their functional effect or clinical implications, as well as the signature allele frequencies in the population studied. The analyses focused on the signature SNVs for Tier 1 variant alleles according to the PharmVar database (https://www.pharmvar.org/). For CYP2C9, Tier 1 alleles are CYP2C9*2, *3, *5, *6, *8, and *11 (Pratt et al., 2019). Among these, the alleles CYP2C9*5, *6, *8, and *11 were not included in the analyses because their signature SNVs had extremely low frequencies (ranging from 0.00002 to 0.003) in European individuals according to public databases (https://gnomad.broadinstitute.org). Therefore, we analyzed CYP2C9*2 (rs1799853) and CYP2C9*3 (rs1057910). Regarding CYP2C19, Tier 1 alleles are the CYP2C19 alleles *2 (rs12769205), *3 (rs4986893) and *17 (rs12248560) (Botton et al., 2020; Pratt et al., 2018). CYP2C19*3 allele was excluded from the study because its signature SNV has a very low allele frequency (equal to 0.0003) in European individuals (Botton et al., 2020). Although no Tier 1 variants have been defined for CYP2C8, we used the same criteria as reported elsewhere (Pratt et al., 2018, Pratt et al., 2019), based on their reported clinical relevance, CYP2C8-associated medications, and their frequency. We selected the variant alleles CYP2C8*3 (rs11572080) and *4 (rs1058930). CYP2C8*2 (rs11572103) was not included because its signature SNV has a very low frequency among Europeans (0.003). All SNVs were tested by using TaqMan Assays (Life Sciences, Alcobendas, Madrid, Spain) pre-designed to detect the above-mentioned SNVs. Details of the TaqMan probes and minor allele frequencies in the study population are shown in Table 3. Assignment of predicted phenotype based on genotype was carried out as described elsewhere for CYP2C9 (Theken et al., 2020), and CYP2C19 (Lima et al., 2020). For CYP2C8, predicted phenotype was carried out assuming that both, CYP2C8*3 and CYP2C8*4 alleles, lead to decreased metabolic activity (Bahadur et al., 2002).
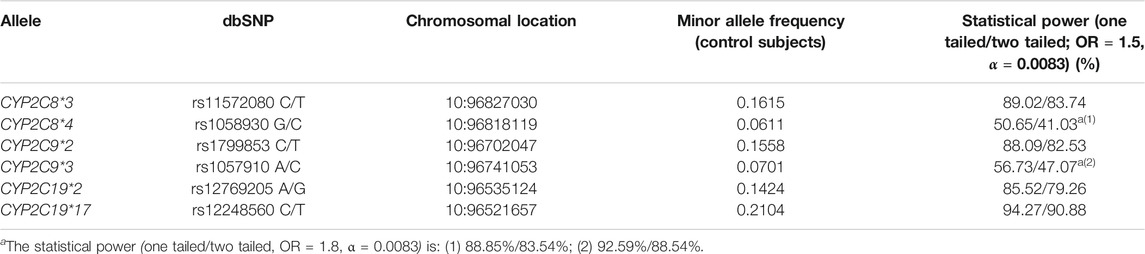
TABLE 3. SNVs analyzed in this study.
The R package SNPassoc (González et al., 2014) was used to calculate allele and genotypic frequencies, to determine the Hardy-Weinberg’s equilibrium (HWE) using the exact test as described elsewhere (Wigginton et al., 2005) and to analyze differences between groups (González et al., 2007).
The comparison of the frequencies of each SNV between traits was performed by using binary logistic regression, assuming different genetic models. To evaluate the genotype risks we applied a traditional logistic regression establishing the most frequent level (*1/*1) as the baseline. The model also includes sex as a predictor and offers two different adjusted p-values from the likelihood ratio test (LRT). The specific p-value measures the significance of the risk of a particular level with respect to the *1/*1 diplotype while the global p-value measures whether the inclusion of all diplotypes different to *1/*1 as a predictor brings about significant additional information about the trait.
When assessing allele risks, the additive model (each copy of the minor allele modifies the risk in an additive form) was used. The analysis was carried out generating a numeric feature with value 0 for the baseline (wild type), 1 for heterozygous for defect alleles, and 2 for homozygous. The additive model was also applied to measure the risk of inferred phenotypes. For CYP2C8 and CYP2C9 the baseline level is RM, while for CYP2C19 we have established NM as baseline level, IM as intermediate high risk level, PM as higher risk level, RM as intermediate low risk level and UR as lower risk level.
The p-values (Tables 4, 5) were adjusted by gender and were obtained by likelihood ratio test (LRT), comparing the likelihood of the nested model that only includes gender as predictor, with the least restrictive model that includes gender and alleles or inferred genotype as predictor.

TABLE 4. Alleles, genotypes and inferred phenotypes observed in overall patients and healthy controls.
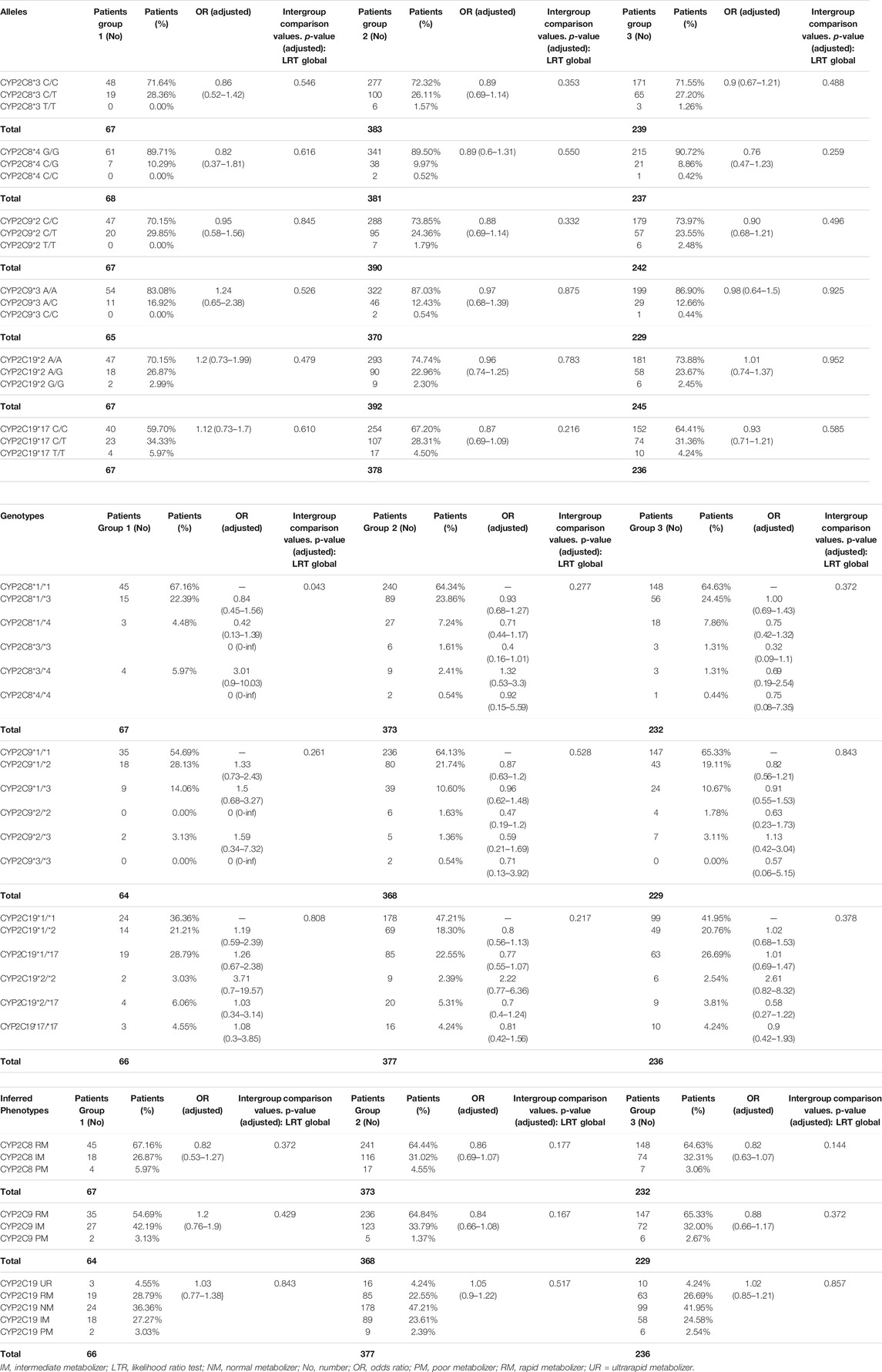
TABLE 5. Alleles, genotypes and inferred phenotypes observed in the three subgroups of patients.
The results were considered statistically significant when p-values were equal or under 0.05. Also, the odds ratio (OR) of Wald Test associated was estimated with a 95% confidence interval (CI). False Discovery Rate (FDR) correction was used for multiple comparison adjustments (Benjamini et al., 2001).
The statistical power for the sample size of this study was calculated to analyze the minor allele frequency (MAF) with a genetic model with an odds ratio value = 1.5 determined from the allele frequencies observed in healthy subjects in previous studies carried out in Spaniards (García-Martín et al., 2001, García-Martín et al., 2004, García-Martín et al., 2015; Alonso-Navarro et al., 2006; Blanco et al., 2008; Ladero et al., 2012; Martínez et al., 2014). The Bonferroni correction was used to make an adjustment for multiple comparisons: the significance level of 0.05 was reduced (α = 0.0083) according to the number of comparisons made (6 in this study). The statistical power for all cases and each SNV analyzed is detailed in Table 3. For most SNVs the statistical power was high enough to detect an OR = 1.5 with a bilateral power higher than 80%. For two SNVs (rs1058930 and rs1057910), because of the low MAF observed in this study, the statistical power was not sufficient to detect an OR = 1.5, but it was sufficient to detect an OR = 1.8 (Table 3).
The most common drugs involved for cross-reactive hypersensitivity induced by NSAIDs were ibuprofen, metamizole and diclofenac (Table 1), and the most frequent clinical presentation was NECD (Table 2). Since many patients experienced cross-reactive hypersensitivity with more than one drug, the sum of the patients in each subgroup in these Tables exceeds the total number of patients. The clinical presentation was strongly related to the drug involved. NECD was particularly related to ibuprofen, whereas anaphylaxis was mainly related to metamizole (Table 2).
To determine the influence of genetic polymorphisms in the risk of developing cross-reactive hypersensitivity, genotypes, diplotypes, and inferred phenotypes were compared in overall patients and healthy controls (Table 4). Genotype calls were very high for all SNVs as follows: CYP2C8*3: 97.6% patients and 97.8% controls; CYP2C8*4: 96.6% patients and 94.4% controls; CYP2C9*2: 99.0% patients and 98.2% controls; CYP2C9*3: 94.2% patients and 94.9% controls; CYP2C19*2: 99.6% patients and 99.0% controls; and CYP2C19*17: 96.2% patients and 96.0% controls. All SNVs were at Hardy-Weinberg’s equilibrium in patients and control individuals and the allele frequencies correspond with those previously described in Spaniards (Martínez et al., 2001; García-Martín et al., 2006; Blanco et al., 2008; Martínez et al., 2014; García-Martín et al., 2015), as well as those reported in public databases (https://gnomad.broadinstitute.org). For individuals who were successfully genotyped for all relevant SNVs in each gene, inferred phenotypes were calculated from diplotypes as described under Methods. The percentage of individuals with inferred phenotypes were as follows: CYP2C8: 95.0% patients and 92.9% controls; CYP2C9: 93.2% patients and 94.4% controls; and CYP2C19: 95.8% patients and 95.5% controls. No statistically significant differences either in allele frequencies, genotypes, or inferred phenotypes were observed when comparing patients with control individuals (Table 4), thus suggesting that CYP2C-related impaired NSAID metabolism is not strongly related to the risk of developing cross-hypersensitivity to NSAIDs.
Since the role of CYP2C enzymes in the metabolism of NSAIDs vary depending on the substrate, patients were divided into three subgroups according to the main enzymes involved in the metabolism of the culprit drugs: group 1: drugs mainly metabolized by CYP2C9 (aceclofenac, indomethacin, naproxen, piroxicam, meloxicam, lornoxicam, and celecoxib); group 2: drugs mainly metabolized by CYP2C8 and CYP2C9 (ibuprofen and diclofenac); and group 3: drugs mainly metabolized by CYP2C19 and CYP2C9 (metamizole) (Leemann et al., 1993; Bonnabry et al., 1996; Miners et al., 1996; Türck et al., 1996; Hamman et al., 1997; Chesné et al., 1998; FDA (Food and Drug Administration), 1998; Skjodt and Davies, 1998; Bort et al., 1999; Davies and Skjodt, 1999; Davies et al., 2000; Henrotin et al., 2001; Tang et al., 2001; Martínez et al., 2005; Perini et al., 2005; Tornio et al., 2007; Chang et al., 2008; Agúndez JA. et al., 2009; Byrav et al., 2009; Neunzig et al., 2012; Abdalla et al., 2014; Martínez et al., 2014; Lucas, 2016; ). Table 5 shows the genotyping and inferred phenotype results. Again, no statistically significant differences were observed between any of the patient’s subgroups and control individuals.
The only statistically significant difference observed was in the subgroup of patients with cross-hypersensitivity to drugs that are predominantly CYP2C9 substrates although the significance was weak and it was related to the CYP2C8 genotypes (Table 5). This difference (p = 0.043) is attributable to a lower frequency of carriers of CYP2C8*3/*3 among patients as compared to control individuals. However, such a difference was not statistically significant after FDR correction (p = 0.129). When patients were stratified according to the clinical presentation (Supplementary Tables S1–S4), the only statistically significant difference was related to a low frequency of NECD patients homozygous for the CYP2C8*3 allele, as compared to healthy individuals (p = 0.029). However, the statistical significance disappeared after FDR correction (p = 0.174).
The role of COX-1 inhibition in the etiopathogenesis of cross-hypersensitivity to NSAIDs has been the object of controversy for years (Kowalski et al., 2007; Doña et al., 2018; Mastalerz et al., 2019). Supporting this hypothesis, it has been shown that COX-2 inhibitors are well tolerated among patients with cross-hypersensitivity to NSAIDs (Morales et al., 2014; Bakhriansyah et al., 2019) and that patients with PTGS1 gene variants related to a decreased activity (Agúndez et al., 2014; Agúndez et al., 2015b; Lucena et al., 2019) are at increased risk of developing cross-hypersensitivity to NSAIDs (García-Martín et al., 2021). Interestingly, preliminary evidence suggests that cross-hypersensitivity to NSAIDs is dose-dependent (Palmer, 2005; Kong et al., 2007; Kowalski et al., 2013; Blumenthal et al., 2017) and, therefore, it could be speculated that individuals with impaired NSAID clearance (and therefore increased drug exposure) might have increased risk of developing cross-hypersensitivity. This hypothesis, however, was not investigated in detail. Preliminary studies have shown the lack of association of Aspirin Induced Asthma and CYP2C19 genotypes (Kooti et al., 2020), which is not surprising since CYP2C19 is not relevant in aspirin metabolism. This aside, no studies have been conducted to assess the putative role of impaired NSAID metabolism in the risk of developing cross-hypersensitivity to NSAIDs.
Strengths in this study include a large sample of patients with cross-reactive hypersensitivity induced to NSAID (n = 499). This sample size allows a good statistical power. A limitation of this study is that plasma levels of the NSAIDs and metabolites could not be obtained because the serum of patients during the acute phase was not available. Therefore, the putative association between genotypes and plasma levels could not be ascertained. Nevertheless, it is widely accepted that the genetic variants analyzed in this study are strongly related to pharmacokinetic changes, and several clinical practice guidelines on CYP2C enzymes (all based on the potential of gene variants to induce pharmacokinetic changes in drugs known to be CYP2C substrates) have been published (Johnson et al., 2011, Johnson et al., 2017; Caudle et al., 2014; Hicks et al., 2017; Moriyama et al., 2017; Karnes et al., 2020; Lima et al., 2020; Theken et al., 2020; Westergaard et al., 2020). Another limitation is that treatment regimen was not specifically recorded, although usually the hypersensitivity reaction occurs after a single standard dose of the corresponding NSAID.
The results of this study do not support a major association between common CYP2C gene variants leading to altered NSAID metabolism and the risk of developing cross-hypersensitivity to NSAIDs. These findings are unexpected if the hypothesis of a putative dose-dependent COX-1 inhibition as a major factor in the development of cross-hypersensitivity is correct. However, the high sample size and the statistical power obtained in this study rule out a major association. It cannot be ruled out putative associations with very rare detrimental allelic variants that have not been analyzed here because of the extremely low frequencies, however, the lack of association with common detrimental alleles observed in this study makes it very unlikely that such putative associations with rare alleles might exist.
It is to be noted that all cases involved ASA, and that therefore, our conclusions are valid only for patients with cross-hypersensitivity involving ASA. CYP2C enzymes play a minor role in ASA metabolism (Agúndez et al., 2009). However, CYP2C9 plays a major role in the metabolism of salicylic acid to gentisic acid (Gómez-Tabales et al., 2020). Also, CYP2C9 is involved in the production of NADPH-dependent hydrogen peroxide in the presence of salicylic acid. Therefore, although the role of CYP2C9 in ASA biodisposition might be quantitatively small, a role in adverse reactions due to ASA cannot be ruled out.
The findings obtained in this study argue against the hypothesis of a dose-dependent (in this case a drug exposure-dependent) COX-1 inhibition as a relevant mechanism in cross-hypersensitivity to NSAIDs and, therefore, will add to the controversy of the mechanisms underlying the development of cross-hypersensitivity to NSAIDs. The main clinical implication of our findings is that we found no evidence supporting the utility of pre-emptive CYP2C genotyping aiming at drug selection for patients with a previous history of cross-hypersensitivity to NSAIDs. However, the findings obtained in this study do not rule out the potential of pharmacogenetics testing combined with phenotyping factors and testing for other genes involved in NSAID pharmacodynamics and/or genes involved in the development and the clinical presentation of the hypersensitivity reactions, such as genes related to the arachidonic acid pathway, as well as those related to inflammation mediators, and oxidative stress.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
The studies involving human participants were reviewed and approved by the Badajoz University Hospital, Málaga University Hospital, Madrid Cruz Roja Hospital, Barcelona Clinic Hospital, Madrid Infanta Leonor Hospital, Alcorcón University Hospital, and Elche University Hospital. The patients/participants provided their written informed consent to participate in this study.
Author contribution statement: All authors have made substantial contributions as follows: Study design: EG-M and JA. Manuscript Drafting: YM, EG-M and JA. Genotyping analyses: YM, EG-M, and JA. Statistical analyses MM, YM, and JA. Patient recruitment and clinical evaluation: JG-M, CC, RJ-E, JC-G, MT, NB-L, GC, MB, JL, JB, AR, and JF. All authors gave final approval of the version to be published. All authors agreed to be accountable for all aspects of the work.
This work was partly supported by Grants PI15/00303, PI18/00540, and RETICS ARADyAL RD16/0006/0004 from Fondo de Investigación Sanitaria, Instituto de Salud Carlos III, Madrid, Spain, and IB16170, IB20134 and GR18145 from Junta de Extremadura, Spain. Financed in part with FEDER funds from the European Union.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We are grateful to Prof. James McCue for his assistance in language editing.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.648262/full#supplementary-material
Abdalla, S. O., Elouzi, A. A., Saad, S. E., Alem, M. D. E. O., and Nagaah, T. A. (2014). Study on the Relationship between Genetic Polymorphisms of Cytochrome CYP2C19 and Metabolic Bioactivation of Dipyrone. J. Chem. Pharm. Res. 6 (6), 992–999.
Agúndez, J. A., García-Martín, E., and Martínez, C. (2009a). Genetically Based Impairment in CYP2C8- and CYP2C9-dependent NSAID Metabolism as a Risk Factor for Gastrointestinal Bleeding: Is a Combination of Pharmacogenomics and Metabolomics Required to Improve Personalized Medicine?. Expert Opin. Drug Metab. Toxicol. 5 (6), 607–620. doi:10.1517/17425250902970998
Agúndez, J., Martínez, C., Pérez-Sala, D., Carballo, M., Torres, M., and García-Martín, E. (2009b). Pharmacogenomics in Aspirin Intolerance. Curr. Drug Metab. 10 (9), 998–1008. doi:10.2174/138920009790711814
Agúndez, J. A., Lucena, M. I., Martínez, C., Andrade, R. J., Blanca, M., Ayuso, P., et al. (2011). Assessment of Nonsteroidal Anti-inflammatory Drug-Induced Hepatotoxicity. Expert Opin. Drug Metab. Toxicol. 7 (7), 817–828. doi:10.1517/17425255.2011.574613
Agúndez, J. A., Gonzalez-Alvarez, D. L., Vega-Rodriguez, M. A., Botello, E., and Garcia-Martin, E. (2014). Gene Variants and Haplotypes Modifying Transcription Factor Binding Sites in the Human Cyclooxygenase 1 and 2 (PTGS1 and PTGS2) Genes. Curr. Drug Metab. 15 (2), 182–195. doi:10.2174/138920021502140327180336
Agúndez, J. A., Mayorga, C., and García-Martin, E. (2015a). Drug Metabolism and Hypersensitivity Reactions to Drugs. Curr. Opin. Allergy Clin. Immunol. 15 (4), 277–284. doi:10.1097/ACI.0000000000000174
Agúndez, J. A., Blanca, M., Cornejo-García, J. A., and García-Martín, E. (2015b). Pharmacogenomics of Cyclooxygenases. Pharmacogenomics 16 (5), 501–522. doi:10.2217/pgs.15.6
Agúndez, J. A. G., Gómez-Tabales, J., Ruano, F., and García-Martin, E. (2018). The Potential Role of Pharmacogenomics and Biotransformation in Hypersensitivity Reactions to Paracetamol. Curr. Opin. Allergy Clin. Immunol. 18 (4), 302–309. doi:10.1097/ACI.0000000000000452
Alonso-Navarro, H., Martínez, C., García-Martín, E., Benito-León, J., García-Ferrer, I., Vázquez-Torres, P., et al. (2006). CYP2C19 Polymorphism and Risk for Essential Tremor. Eur. Neurol. 56 (2), 119–123. doi:10.1159/000095702
Angeletti, F., Meier, F., Zöller, N., Meissner, M., Kaufmann, R., and Valesky, E. M. (2020). Hypersensitivity Reactions to Non-steroidal Anti-inflammatory Drugs (NSAIDs) - A Retrospective Study. J. Dtsch Dermatol. Ges. 18 (12), 1405–1414. doi:10.1111/ddg.14292
Ariza, A., García-Martín, E., Salas, M., Montañez, M. I., Mayorga, C., Blanca-Lopez, N., et al. (2016). Pyrazolones Metabolites Are Relevant for Identifying Selective Anaphylaxis to Metamizole. Sci. Rep. 6 (1), 23845. doi:10.1038/srep23845
Bahadur, N., Leathart, J. B., Mutch, E., Steimel-Crespi, D., Dunn, S. A., Gilissen, R., et al. (2002). CYP2C8 Polymorphisms in Caucasians and Their Relationship with Paclitaxel 6alpha-Hydroxylase Activity in Human Liver Microsomes. Biochem. Pharmacol. 64 (11), 1579–1589. doi:10.1016/s0006-2952(02)01354-0
Bakhriansyah, M., Meyboom, R. H. B., Souverein, P. C., de Boer, A., and Klungel, O. H. (2019). Cyclo-oxygenase Selectivity and Chemical Groups of Nonsteroidal Anti-inflammatory Drugs and the Frequency of Reporting Hypersensitivity Reactions: a Case/noncase Study in VigiBase. Fundam. Clin. Pharmacol. 33 (5), 589–600. doi:10.1111/fcp.12463
Benjamini, Y., Drai, D., Elmer, G., Kafkafi, N., and Golani, I. (2001). Controlling the False Discovery Rate in Behavior Genetics Research. Behav. Brain Res. 125 (1–2), 279–284. doi:10.1016/s0166-4328(01)00297-2
Bigler, J., Whitton, J., Lampe, J. W., Fosdick, L., Bostick, R. M., and Potter, J. D. (2001). CYP2C9 and UGT1A6 Genotypes Modulate the Protective Effect of Aspirin on colon Adenoma Risk. Cancer Res. 61 (9), 3566–3569.
Blanca-López, N., Haroun-Diaz, E., Ruano, F. J., Pérez-Alzate, D., Somoza, M. L., Vázquez de la Torre Gaspar, M., et al. (2018). Acetyl Salicylic Acid challenge in Children with Hypersensitivity Reactions to Nonsteroidal Anti-inflammatory Drugs Differentiates between Cross-Intolerant and Selective Responders. J. Allergy Clin. Immunol. Pract. 6 (4), 1226–1235. doi:10.1016/j.jaip.2017.08.029
Blanca-López, N., Soriano, V., Garcia-Martin, E., Canto, G., and Blanca, M. (2019). NSAID-induced Reactions: Classification, Prevalence, Impact, and Management Strategies. J. Asthma Allergy 12, 217–233. doi:10.2147/JAA.S164806
Blanco, G., Martínez, C., Ladero, J. M., Garcia-Martin, E., Taxonera, C., Gamito, F. G., et al. (2008). Interaction of CYP2C8 and CYP2C9 Genotypes Modifies the Risk for Nonsteroidal Anti-inflammatory Drugs-Related Acute Gastrointestinal Bleeding. Pharmacogenet Genom. 18 (1), 37–43. doi:10.1097/FPC.0b013e3282f305a9
Blumenthal, K. G., Lai, K. H., Wickner, P. G., Goss, F. R., Seger, D. L., Slight, S. P., et al. (2016). Reported Incidence of Hypersensitivity Reactions to Non-Steroidal Anti-inflammatory Drugs in the Electronic Health Record. J. Allergy Clin. Immunol. 137 (2), AB196. doi:10.1016/j.jaci.2015.12.772
Blumenthal, K. G., Lai, K. H., Huang, M., Wallace, Z. S., Wickner, P. G., and Zhou, L. (2017). Adverse and Hypersensitivity Reactions to Prescription Nonsteroidal Anti-inflammatory Agents in a Large Health Care System. J. Allergy Clin. Immunol. Pract. 5 (3), 737–e3. doi:10.1016/j.jaip.2016.12.006
Bonnabry, P., Leemann, T., and Dayer, P. (1996). Role of Human Liver Microsomal CYP2C9 in the Biotransformation of Lornoxicam. Eur. J. Clin. Pharmacol. 49 (4), 305–308. doi:10.1007/BF00226332
Bort, R., Macé, K., Boobis, A., Gómez-Lechón, M. J., Pfeifer, A., and Castell, J. (1999). Hepatic Metabolism of Diclofenac: Role of Human CYP in the Minor Oxidative Pathways. Biochem. Pharmacol. 58 (5), 787–796. doi:10.1016/s0006-2952(99)00167-7
Botton, M. R., Whirl‐Carrillo, M., Del Tredici, A. L., Sangkuhl, K., Cavallari, L. H., Agúndez, J. A. G., et al. (2020). PharmVar GeneFocus: CYP2C19. Clin. Pharmacol. Ther. 109, 352–366. doi:10.1002/cpt.1973
Byrav, P. D. S., Medhi, B., Prakash, A., Patyar, S., and Wadhwa, S. (2009). Lornoxicam: a Newer NSAID. Indian J. Phys. Med. Rehabil. 20 (1), 27–31.
Caimmi, S., Caimmi, D., Bousquet, P. J., and Demoly, P. (2012). How Can We Better Classify NSAID Hypersensitivity Reactions?-Vvalidation from a Large Database. Int. Arch. Allergy Immunol. 159 (3), 306–312. doi:10.1159/000337660
Caudle, K. E., Rettie, A. E., Whirl-Carrillo, M., Smith, L. H., Mintzer, S., Lee, M. T., et al. (2014). Clinical Pharmacogenetics Implementation Consortium Guidelines for CYP2C9 and HLA-B Genotypes and Phenytoin Dosing. Clin. Pharmacol. Ther. 96 (5), 542–548. doi:10.1038/clpt.2014.159
Chang, S. Y., Li, W., Traeger, S. C., Wang, B., Cui, D., Zhang, H., et al. (2008). Confirmation that Cytochrome P450 2C8 (CYP2C8) Plays a Minor Role in (S)-(+)- and (R)-(-)-ibuprofen Hydroxylation In Vitro. Drug Metab. Dispos. 36 (12), 2513–2522. doi:10.1124/dmd.108.022970
Chesné, C., Guyomard, C., Guillouzo, A., Schmid, J., Ludwig, E., and Sauter, T. (1998). Metabolism of Meloxicam in Human Liver Involves Cytochromes P4502C9 and 3A4. Xenobiotica 28 (1), 1–13. doi:10.1080/004982598239704
Davies, N. M., and Skjodt, N. M. (1999). Clinical Pharmacokinetics of Meloxicam. A Cyclo-Oxygenase-2 Preferential Nonsteroidal Anti-inflammatory Drug. Clin. Pharmacokinet. 36 (2), 115–126. doi:10.2165/00003088-199936020-00003
Davies, N. M., McLachlan, A. J., Day, R. O., and Williams, K. M. (2000). Clinical Pharmacokinetics and Pharmacodynamics of Celecoxib: a Selective Cyclo-Oxygenase-2 Inhibitor. Clin. Pharmacokinet. 38 (3), 225–242. doi:10.2165/00003088-200038030-00003
Doña, I., Barrionuevo, E., Salas, M., Laguna, J. J., Agúndez, J., García-Martín, E., et al. (2018). NSAIDs-hypersensitivity Often Induces a Blended Reaction Pattern Involving Multiple Organs. Sci. Rep. 8 (1), 16710. doi:10.1038/s41598-018-34668-1
Doña, I., Blanca-López, N., Cornejo-García, J. A., Torres, M. J., Laguna, J. J., Fernández, J., et al. (2011). Characteristics of Subjects Experiencing Hypersensitivity to Non-steroidal Anti-inflammatory Drugs: Patterns of Response. Clin. Exp. Allergy 41 (1), 86–95. doi:10.1111/j.1365-2222.2010.03651.x
FDA (Food and Drug Administration) (1998). Celebrex (Celecoxib). Clinical Pharmacology and Biopharmaceutics Review. New Drug Application number: 20-998. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/nda/98/20998.cfm (Accessed August 15, 2021).
García-Martín, E., García-Menaya, J. M., Esguevillas, G., Cornejo-García, J. A., and Doña, I. (2021). Deep sequencing of prostaglandin-endoperoxide synthase (PTGE) genes reveals genetic susceptibility for cross-reactive hypersensitivity to NSAID. Br. J. Pharmacol. 178 (5), 1218–1233. doi:10.1111/bph.15366
García-Martín, E., Martínez, C., Ladero, J. M., Gamito, F. J., and Agúndez, J. A. (2001). High Frequency of Mutations Related to Impaired CYP2C9 Metabolism in a Caucasian Population. Eur. J. Clin. Pharmacol. 57 (1), 47–49. doi:10.1007/s002280100264
García-Martín, E., Martínez, C., Tabarés, B., Frías, J., and Agúndez, J. A. (2004). Interindividual Variability in Ibuprofen Pharmacokinetics Is Related to Interaction of Cytochrome P450 2C8 and 2C9 Amino Acid Polymorphisms. Clin. Pharmacol. Ther. 76 (2), 119–127. doi:10.1016/j.clpt.2004.04.006
García-Martín, E., Martínez, C., Ladero, J. M., and Agúndez, J. A. (2006). Interethnic and Intraethnic Variability of CYP2C8 and CYP2C9 Polymorphisms in Healthy Individuals. Mol. Diagn. Ther. 10 (1), 29–40. doi:10.1007/BF03256440
García-Martín, E., Esguevillas, G., Blanca-López, N., García-Menaya, J., Blanca, M., Amo, G., et al. (2015). Genetic Determinants of Metamizole Metabolism Modify the Risk of Developing Anaphylaxis. Pharmacogenet Genom. 25 (9), 462–464. doi:10.1097/FPC.0000000000000157
García-Martín, E., García-Menaya, J. M., Esguevillas, G., Cornejo-García, J. A., Doña, I., Jurado-Escobar, R., Torres, MJ., Blanca-López, N., Canto, G., Blanca, M., Laguna, JJ., Bartra, J., Rosado, A., Fernández, J., Cordobćs, C., and Agúndez, JAG. Deep sequencing of prostaglandin-endoperoxide synthase (PTGE) genes reveals genetic susceptibility for cross-reactive hypersensitivity to NSAID. Br J Pharmacol. Br. J. Pharmacol. 2021 178 (5), 1218–1233. doi:10.1111/bph.15366
Gómez-Tabales, J., García-Martín, E., Agúndez, J. A. G., and Gutierrez-Merino, C. (2020). Modulation of CYP2C9 Activity and Hydrogen Peroxide Production by Cytochrome B5. Sci. Rep. 10 (1), 15571. doi:10.1038/s41598-020-72284-0
González, J. R., Armengol, L., Solé, X., Guinó, E., Mercader, J. M., Estivill, X., et al. (2007). SNPassoc: an R Package to Perform Whole Genome Association Studies. Bioinformatics 23 (5), 644–645. doi:10.1093/bioinformatics/btm025
González, J. R., Armengol, L., Guinó, E., Solé, X., and Moreno, V. (2014). SNPassoc: SNPs-Based Whole Genome Association Studies. Available at: https://cran.r-project.org/package=SNPassoc (Accessed August 15, 2021).
Hamman, M. A., Thompson, G. A., and Hall, S. D. (1997). Regioselective and Stereoselective Metabolism of Ibuprofen by Human Cytochrome P450 2C. Biochem. Pharmacol. 54 (1), 33–41. doi:10.1016/s0006-2952(97)00143-3
Henrotin, Y., de Leval, X., Mathy-Hartet, M., Mouithys-Mickalad, A., Deby-Dupont, G., Dogné, J. M., et al. (2001). In Vitro effects of Aceclofenac and its Metabolites on the Production by Chondrocytes of Inflammatory Mediators. Inflamm. Res. 50 (8), 391–399. doi:10.1007/PL00000261
Hicks, J. K., Sangkuhl, K., Swen, J. J., Ellingrod, V. L., Müller, D. J., Shimoda, K., et al. (2017). Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2D6 and CYP2C19 Genotypes and Dosing of Tricyclic Antidepressants: 2016 Update. Clin. Pharmacol. Ther. 102 (1), 37–44. doi:10.1002/cpt.597
Hutt, A. J., Caldwell, J., and Smith, R. L. (1986). The Metabolism of Aspirin in Man: a Population Study. Xenobiotica 16 (3), 239–249. doi:10.3109/00498258609043527
Johansson, S. G., Bieber, T., Dahl, R., Friedmann, P. S., Lanier, B. Q., Lockey, R. F., et al. (2004). Revised Nomenclature for Allergy for Global Use: Report of the Nomenclature Review Committee of the World Allergy Organization. J. Allergy Clin. Immunol. 113 (5), 832–836. doi:10.1016/j.jaci.2003.12.591
Johnson, J. A., Gong, L., Whirl-Carrillo, M., Gage, B. F., Scott, S. A., Stein, C. M., et al. (2011). Clinical Pharmacogenetics Implementation Consortium Guidelines for CYP2C9 and VKORC1 Genotypes and Warfarin Dosing. Clin. Pharmacol. Ther. 90 (4), 625–629. doi:10.1038/clpt.2011.185
Johnson, J. A., Caudle, K. E., Gong, L., Whirl-Carrillo, M., Stein, C. M., Scott, S. A., et al. (2017). Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Pharmacogenetics-Guided Warfarin Dosing: 2017 Update. Clin. Pharmacol. Ther. 102 (3), 397–404. doi:10.1002/cpt.668
Karnes, J. H., Rettie, A. E., Somogyi, A. A., Huddart, R., Fohner, A. E., Formea, C. M., et al. (2020). Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C9 and HLA‐B Genotypes and Phenytoin Dosing: 2020 Update. Clin. Pharmacol. Ther. 109, 302–309. doi:10.1002/cpt.2008
Kong, J. S., Teuber, S. S., and Gershwin, M. E. (2007). Aspirin and Nonsteroidal Anti-inflammatory Drug Hypersensitivity. Clin. Rev. Allergy Immunol. 32 (1), 97–110. doi:10.1007/BF02686086
Kooti, W., Abdi, M., Malik, Y. S., Nouri, B., Jalili, A., Rezaee, M. A., et al. (2020). Association of CYP2C19 and HSP70 Genes Polymorphism with Aspirin- Exacerbated Respiratory Disease in a Kurd Population. Endocr. Metab. Immune Disord. Drug Targets 20 (2), 256–262. doi:10.2174/1872214812666190527104329
Kowalski, M. L., Borowiec, M., Kurowski, M., and Pawliczak, R. (2007). Alternative Splicing of Cyclooxygenase-1 Gene: Altered Expression in Leucocytes from Patients with Bronchial Asthma and Association with Aspirin-Induced 15-HETE Release. Allergy 62 (6), 628–634. doi:10.1111/j.1398-9995.2007.01366.x
Kowalski, M. L., Asero, R., Bavbek, S., Blanca, M., Blanca-Lopez, N., Bochenek, G., et al. (2013). Classification and Practical Approach to the Diagnosis and Management of Hypersensitivity to Nonsteroidal Anti-inflammatory Drugs. Allergy 68 (10), 1219–1232. doi:10.1111/all.12260
Ladero, J. M., Agúndez, J. A., Martínez, C., Amo, G., Ayuso, P., and García-Martín, E. (2012). Analysis of the Functional Polymorphism in the Cytochrome P450 CYP2C8 Gene Rs11572080 with Regard to Colorectal Cancer Risk. Front. Genet. 3, 278. doi:10.3389/fgene.2012.00278
Leemann, T., Transon, C., and Dayer, P. (1993). Cytochrome P450TB (CYP2C): a Major Monooxygenase Catalyzing Diclofenac 4'-hydroxylation in Human Liver. Life Sci. 52 (1), 29–34. doi:10.1016/0024-3205(93)90285-b
Li, L., and Laidlaw, T. (2019). Cross-reactivity and Tolerability of Celecoxib in Adult Patients with NSAID hypersensitivityThe Journal of Allergy and Clinical Immunology. J. Allergy Clin. Immunol. Pract. 7 (8), 2891In practice. doi:10.1016/j.jaip.2019.04.042
Lima, J. J., Thomas, C. D., Barbarino, J., Desta, Z., Van Driest, S. L., El Rouby, N., et al. (2020). Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clin. Pharmacol. Ther. 109, 1417–1423. doi:10.1002/cpt.2015
Lucas, S. (2016). The Pharmacology of Indomethacin. Headache 56 (2), 436–446. doi:10.1111/head.12769
Lucena, M. I., García-Martín, E., Daly, A. K., Blanca, M., Andrade, R. J., and Agúndez, J. A. G. (2019). Next-Generation Sequencing of PTGS Genes Reveals an Increased Frequency of Non-synonymous Variants Among Patients with NSAID-Induced Liver Injury. Front. Genet. 10, 134. doi:10.3389/fgene.2019.00134
Macías, Y., Gómez Tabales, J., García-Martín, E., and Agúndez, J. A. G. (2020). An Update on the Pharmacogenomics of NSAID Metabolism and the Risk of Gastrointestinal Bleeding. Expert Opin. Drug Metab. Toxicol. 16 (4), 319–332. doi:10.1080/17425255.2020.1744563
Martínez, C., García-Martín, E., Ladero, J. M., Sastre, J., Garcia-Gamito, F., Diaz-Rubio, M., et al. (2001). Association of CYP2C9 Genotypes Leading to High Enzyme Activity and Colorectal Cancer Risk. Carcinogenesis 22 (8), 1323–1326. doi:10.1093/carcin/22.8.1323
Martínez, C., García-Martín, E., Blanco, G., Gamito, F. J., Ladero, J. M., and Agúndez, J. A. (2005). The Effect of the Cytochrome P450 CYP2C8 Polymorphism on the Disposition of (R)-ibuprofen Enantiomer in Healthy Subjects. Br. J. Clin. Pharmacol. 59 (1), 62–69. doi:10.1111/j.1365-2125.2004.02183.x
Martínez, C., Andreu, I., Amo, G., Miranda, M. A., Esguevillas, G., Torres, M. J., et al. (2014). Gender and Functional CYP2C and NAT2 Polymorphisms Determine the Metabolic Profile of Metamizole. Biochem. Pharmacol. 92(3), 457–466. doi:10.1016/j.bcp.2014.09.005
Mastalerz, L., Tyrak, K. E., Ignacak, M., Konduracka, E., Mejza, F., Ćmiel, A., et al. (2019). Prostaglandin E2 Decrease in Induced Sputum of Hypersensitive Asthmatics during Oral challenge with Aspirin. Allergy 74 (5), 922–932. doi:10.1111/all.13671
Miners, J. O., Coulter, S., Tukey, R. H., Veronese, M. E., and Birkett, D. J. (1996). Cytochromes P450, 1A2, and 2C9 Are Responsible for the Human Hepatic O-Demethylation of R- and S-Naproxen. Biochem. Pharmacol. 51 (8), 1003–1008. doi:10.1016/0006-2952(96)85085-4
Morales, D. R., Lipworth, B. J., Guthrie, B., Jackson, C., Donnan, P. T., and Santiago, V. H. (2014). Safety Risks for Patients with Aspirin-Exacerbated Respiratory Disease after Acute Exposure to Selective Nonsteroidal Anti-inflammatory Drugs and COX-2 Inhibitors: Meta-Analysis of Controlled Clinical Trials. J. Allergy Clin. Immunol. 134 (1), 40–45. doi:10.1016/j.jaci.2013.10.057
Moriyama, B., Obeng, A. O., Barbarino, J., Penzak, S. R., Henning, S. A., Scott, S. A., et al. (2017). Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for CYP2C19 and Voriconazole Therapy. Clin. Pharmacol. Ther. 102 (1), 45–51. doi:10.1002/cpt.583
Neunzig, I., Göhring, A., Drăgan, C. A., Zapp, J., Peters, F. T., Maurer, H. H., et al. (2012). Production and NMR Analysis of the Human Ibuprofen Metabolite 3-hydroxyibuprofen. J. Biotechnol. 157 (3), 417–420. doi:10.1016/j.jbiotec.2011.12.016
Palikhe, N. S., Kim, S. H., Nam, Y. H., Ye, Y. M., and Park, H. S. (2011). Polymorphisms of Aspirin-Metabolizing Enzymes CYP2C9, NAT2 and UGT1A6 in Aspirin-Intolerant Urticaria. Allergy Asthma Immunol. Res. 3 (4), 273–276. doi:10.4168/aair.2011.3.4.273
Palmer, G. M. (2005). A Teenager with Severe Asthma Exacerbation Following Ibuprofen. Anaesth. Intensive Care 33 (2), 261–265. doi:10.1177/0310057X0503300218
Pérez-Alzate, D., Cornejo-García, J., Pérez-Sánchez, N., Andreu, I., García-Moral, A., Agúndez, J., et al. (2017). Immediate Reactions to More Than 1 NSAID Must Not Be Considered Cross-Hypersensitivity unless Tolerance to ASA Is Verified. J. Investig. Allergol. Clin. Immunol. 27 (1), 32–39. doi:10.18176/jiaci.0080
Perini, J. A., Vianna-Jorge, R., Brogliato, A. R., and Suarez-Kurtz, G. (2005). Influence of CYP2C9 Genotypes on the Pharmacokinetics and Pharmacodynamics of Piroxicam. Clin. Pharmacol. Ther. 78 (4), 362–369. doi:10.1016/j.clpt.2005.06.014
Plaza-Serón, M. D. C., García-Martín, E., Agúndez, J. A., and Ayuso, P. (2018). Hypersensitivity Reactions to Nonsteroidal Anti-inflammatory Drugs: an Update on Pharmacogenetics Studies. Pharmacogenomics 19 (13), 1069–1086. doi:10.2217/pgs-2018-0079
Pratt, V. M., Del Tredici, A. L., Hachad, H., Ji, Y., Kalman, L. V., Scott, S. A., et al. (2018). Recommendations for Clinical CYP2C19 Genotyping Allele Selection: a Report of the Association for Molecular Pathology. J. Mol. Diagn. 20 (3), 269–276. doi:10.1016/j.jmoldx.2018.01.011
Pratt, V. M., Cavallari, L. H., Del Tredici, A. L., Hachad, H., Ji, Y., Moyer, A. M., et al. (2019). Recommendations for Clinical CYP2C9 Genotyping Allele Selection: a Joint Recommendation of the Association for Molecular Pathology and College of American Pathologists. J. Mol. Diagn. 21 (5), 746–755. doi:10.1016/j.jmoldx.2019.04.003
Sánchez-Borges, M. (2010). NSAID Hypersensitivity (Respiratory, Cutaneous, and Generalized Anaphylactic Symptoms). Med. Clin. North. Am. 94 (4), 853. doi:10.1016/j.mcna.2010.03.005
Sánchez-Gómez, F. J., Díez-Dacal, B., García-Martín, E., Agúndez, J. A., Pajares, M. A., and Pérez-Sala, D. (2016). Detoxifying Enzymes at the Cross-Roads of Inflammation, Oxidative Stress, and Drug Hypersensitivity: Role of Glutathione Transferase P1-1 and Aldose Reductase. Front. Pharmacol. 7, 237. doi:10.3389/fphar.2016.00237
Singh, G. (2000). Gastrointestinal Complications of Prescription and Over-the-counter Nonsteroidal Anti-inflammatory Drugs: a View from the ARAMIS Database. Arthritis, Rheumatism, and Aging Medical Information System. Am. J. Ther. 7 (2), 115–121. doi:10.1097/00045391-200007020-00008
Skjodt, N. M., and Davies, N. M. (1998). Clinical Pharmacokinetics of Lornoxicam. A Short Half-Life Oxicam. Clin. Pharmacokinet. 34 (6), 421–428. doi:10.2165/00003088-199834060-00001
Szczeklik, A., Niżankowska-Mogilnicka, E., and Sanak, M. (2009). “Hypersensitivity to Aspirin and Non-Steroidal Antiinflammatory Drugs,” in Middelton’s Allergy, Principles and Practice. Editors N. F. Adkinson, B. S. Bochner, W. W. Busse, S. T. Holgate, R. F. Lemanske, and F. E. R. Simons. 7th ed (Philadelphia: Mosby Elsevier), 1227–1243. doi:10.1016/b978-0-323-05659-5.00069-3
Tang, C., Shou, M., Rushmore, T. H., Mei, Q., Sandhu, P., Woolf, E. J., et al. (2001). In-vitro Metabolism of Celecoxib, a Cyclooxygenase-2 Inhibitor, by Allelic Variant Forms of Human Liver Microsomal Cytochrome P450 2C9: Correlation with CYP2C9 Genotype and In-Vivo Pharmacokinetics. Pharmacogenetics 11 (3), 223–235. doi:10.1097/00008571-200104000-00006
Theken, K. N., Lee, C. R., Gong, L., Caudle, K. E., Formea, C. M., Gaedigk, A., et al. (2020). Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-inflammatory Drugs. Clin. Pharmacol. Ther. 108 (2), 191–200. doi:10.1002/cpt.1830
Thiessen, J. J. (1983). Aspirin: Plasma Concentration and Effects. Thromb. Res. Suppl. 4, 105–111. doi:10.1016/0049-3848(83)90365-1
Tornio, A., Niemi, M., Neuvonen, P. J., and Backman, J. T. (2007). Stereoselective Interaction between the CYP2C8 Inhibitor Gemfibrozil and Racemic Ibuprofen. Eur. J. Clin. Pharmacol. 63 (5), 463–469. doi:10.1007/s00228-007-0273-9
Türck, D., Roth, W., and Busch, U. (1996). A Review of the Clinical Pharmacokinetics of Meloxicam. Br. J. Rheumatol. 35 (Suppl. 1), 13–16. doi:10.1093/rheumatology/35.suppl_1.13
Westergaard, N., Søgaard Nielsen, R., Jørgensen, S., and Vermehren, C. (2020). Drug Use in Denmark for Drugs Having Pharmacogenomics (PGx) Based Dosing Guidelines from CPIC or DPWG for CYP2D6 and CYP2C19 Drug-Gene Pairs: Perspectives for Introducing PGx Test to Polypharmacy Patients. J. Pers Med. 10 (1), 3. doi:10.3390/jpm10010003
Keywords: CYP2C8, CYP2C9, CYP2C19, NSAID, polymorphisms, hypersensitivity
Citation: Macías Y, García-Menaya JM, Martí M, Cordobés C, Jurado-Escobar R, Cornejo-García JA, Torres MJ, Blanca-López N, Canto G, Blanca M, Laguna JJ, Bartra J, Rosado A, Fernández J, García-Martín E and Agúndez JAG (2021) Lack of Major Involvement of Common CYP2C Gene Polymorphisms in the Risk of Developing Cross-Hypersensitivity to NSAIDs. Front. Pharmacol. 12:648262. doi: 10.3389/fphar.2021.648262
Received: 31 December 2020; Accepted: 06 September 2021;
Published: 21 September 2021.
Edited by:
Paola Patrignani, University of Studies G. d’Annunzio Chieti and Pescara, ItalyReviewed by:
Ursula Amstutz, University of Bern, SwitzerlandCopyright © 2021 Macías, García-Menaya, Martí, Cordobés, Jurado-Escobar, Cornejo-García, Torres, Blanca-López, Canto, Blanca, Laguna, Bartra, Rosado, Fernández, García-Martín and Agúndez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José A. G. Agúndez, amFndW5kZXpAdW5leC5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.