
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 27 January 2021
Sec. Ethnopharmacology
Volume 11 - 2020 | https://doi.org/10.3389/fphar.2020.615657
This article is part of the Research Topic Herbal medicines in Managing Stroke and Neurodegenerative Diseases – Is there Evidence based on Basic and Clinical Studies? View all 10 articles
 Chien-Hung Lin1†
Chien-Hung Lin1† Hsienhsueh Elley Chiu1†
Hsienhsueh Elley Chiu1† Szu-Ying Wu1,2,3Shih-Ting Tseng1Tzu-Chan Wu1
Szu-Ying Wu1,2,3Shih-Ting Tseng1Tzu-Chan Wu1 Yu-Chiang Hung1,4
Yu-Chiang Hung1,4 Chung Y. Hsu5Hsuan-Ju Chen6,7Sheng-Feng Hsu8,9
Chung Y. Hsu5Hsuan-Ju Chen6,7Sheng-Feng Hsu8,9 Chun-En Kuo1,2*
Chun-En Kuo1,2* Wen-Long Hu1,10,11*
Wen-Long Hu1,10,11*Objective: Combinations of Chinese herbal products (CHPs) are widely used for Parkinson’s disease (PD) in Taiwan. Thereby, we investigated the use of CHPs in patients with PD.
Methods: This study was a population-based cohort study that analyzed the data of patients with PD from the National Health Insurance Research Database. A total of 9,117 patients were selected from a random sample of one million individuals included in this database. We used multiple logistic regression models to estimate the adjusted odds ratios of the demographic factors and analyzed the formula and single CHPs commonly used for PD.
Results: Traditional Chinese medicine users were more commonly female, younger, of white-collar status, and residents of Central Taiwan. Chaihu-Jia-Longgu-Muli-Tang was the most commonly used formula, followed by Ma-Zi-Ren-Wan and then Shao-Yao-Gan-Cao-Tang. The most commonly used single herb was Uncaria tomentosa (Willd. ex Schult.) DC., followed by Gastrodia elata Blume and then Radix et Rhizoma Rhei (Rheum palmatum L., Rheum tanguticum Maxim. ex Balf., and Rheum officinale Baill.). Chaihu-Jia-Longgu-Muli-Tang and U. tomentosa (Willd. ex Schult.) DC. have shown neuroprotective effects in previous studies, and they have been used for managing non-motor symptoms of PD.
Conclusion: Chaihu-Jia-Longgu-Muli-Tang and U. tomentosa (Willd. ex Schult.) DC. are the most commonly used CHPs for PD in Taiwan. Our results revealed the preferences in medication prescriptions for PD. Further studies are warranted to determine the effectiveness of these CHPs for ameliorating the various symptoms of PD, their adverse effects, and the mechanisms underlying their associated neuroprotective effects.
Parkinson’s disease (PD) results primarily from the loss of dopaminergic neurons in the substantia nigra. Treatment for PD includes drugs such as monoamine oxidase type B inhibitors, dopamine agonists, and levodopa. These agents can increase dopaminergic effects but can also result in side-effects, such as nausea, somnolence, dizziness, and headaches. More serious adverse reactions are common in the elderly, including confusion, hallucinations, delusions, agitation, psychosis, and orthostatic hypotension (Spindler and Tarsy, 2019). Levodopa is the most commonly used treatment for PD and is usually co-administered with an aromatic L-amino acid decarboxylase inhibitor to increase bioactivity, since levodopa is rapidly metabolized to dopamine by peripheral aromatic L-amino acid decarboxylase and catechol-O-methyltransferase (Rocha et al., 2017). However, it cannot penetrate the blood–brain barrier to act on the substantia nigra. Therefore, studies are currently seeking to elucidate methods to increase the levodopa levels in the brain, inhibit peripheral levodopa metabolism, and minimize the prevalence of side-effects (Ferreira et al., 2015).
Due to the limitations and side-effects of conventional therapy, patients often seek complementary and alternative medicine (CAM) (Han et al., 2017). In recent decades, the use of CAM for various diseases has increased among all adult age groups, including the elderly (Clarke et al., 2015). Previous studies have estimated the prevalence of CAM use for PD to be 25.7–76%, with survey response rates of 81–100%. Frequently utilized forms of CAM included acupuncture, massage, herbs, and vitamins/health supplements; these therapies were mainly used to improve the motor symptoms of PD (Wang et al., 2013b). Research has shown that Chinese herbal products (CHPs) have a high efficacy against PD, both in clinical trials and animal studies (Han et al., 2017). Despite the mostly positive attitude of the public toward traditional Chinese medicine (TCM), its clinical indications for specific diseases remain controversial (Hasan et al., 2010; Medagama and Bandara, 2014; Setty and Sigal, 2005). Research on the therapeutic effects of CAM may currently be restricted by small sample sizes or the lack of well-designed randomized controlled trials (Han et al., 2017).
The National Health Insurance (NHI) Research Database (NHIRD), which is widely used in Taiwan, provides a platform for understanding the utilization of CHPs by licensed TCM doctors. In this study, we analyzed the NHIRD to determine CHP utilization patterns for PD. The results may provide valuable information regarding the pattern of CHP prescription by TCM physicians, thereby improving PD treatment and forming the basis for subsequent pharmacological studies.
The NHI was established on March 1, 1995, and provides medical health care to 23 million residents in Taiwan. The coverage of NHI reached 99% by the end of 2014 and therefore represents most of the medication prescription patterns in Taiwan. Each individual has a unique personal identification number in this database.
For this study, data were extracted from the Longitudinal Health Insurance Database (LHID) 2000, a subset of the NHIRD that contains all medical reimbursement claims made under the NHI program for one million enrollees from 2000 to 2011. The NHI reported that there were no significant biases in sex or age distribution in the LHID 2000 recruitment. The data used were provided by the Taiwan National Health Research Institute and authorized by the Ministry of Health and Welfare, which manages the NHI claims. These are the most recent data available. The study was approved by the Institutional Review Board of China Medical University and Hospital (CMUH104-REC2-115).
From the random sample of one million individuals enrolled in the LHID 2000, we extracted the data of patients diagnosed with PD (ICD-9-CM332, based on the International Classification of Diseases, ninth revision, clinical modification (ICD-9-CM), between 2000 and 2011. All patients with PD utilized the outpatient services at least twice or inpatient hospitalization at least once, according to the database claims (n = 12,675). We excluded patients with missing data for sex and age (n = 4), patients with existing PD diagnoses before the end of 1999 (n = 3,483), and patients aged ≤20 years (n = 71). There were 9,117 new PD cases, including TCM (n = 4,060) and non-TCM users (n = 5,057). TCM users were those who visited a TCM clinic at least once during the study period. Non-TCM users were those who had never visited a TCM clinic after the initial PD diagnosis (Figure 1).
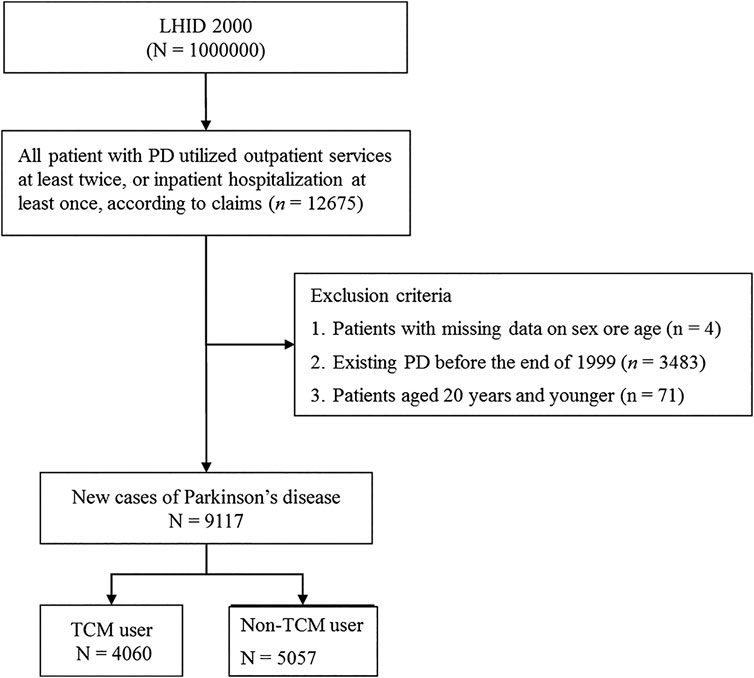
FIGURE 1. Flowchart of recruitment of subjects from LHID 2000 during 2000–2011 in Taiwan. Abbreviation: TCM, traditional Chinese medicine.
The NHI reimburses two types of Chinese herbal remedies: Chinese single herbs and Chinese herbal formulae. Each Chinese herbal formula is a combination of two or more Chinese single herbs in strict proportions, as per the TCM literature. We analyzed the prescription patterns for PD according to these two types of herbal remedies and their usage rates.
The following sociodemographic data were extracted from the NHIRD: sex, age, occupational status, and residential area. Occupational status was divided into three categories: office workers (white collar), manual workers (blue collar), and others. The residential areas of the population were based on the district branches of the National Health Insurance Administration, consisting of Northern Taiwan, Central Taiwan, Southern Taiwan, Eastern Taiwan, and offshore islands.
TCM user and non-TCM user data (including age, sex, occupational status, and residential areas) are described as means and standard deviations. Odds ratios (ORs) and 95% confidence intervals (CIs) were used to determine which group might have a greater tendency to use TCM, based on multiple logistic regression models. We used adjusted ORs to address potential sources of bias in the use of TCM. We set statistical significance at p < 0.05 (two-tailed). The TCM prescription patterns for PD were analyzed according to the frequency of Chinese single herbs and Chinese herbal formulae used. All statistical analyses were run in Statistic Analysis System (SAS) software, version 9.3 (SAS Institute, Cary, NC).
Among the 9,117 patients diagnosed with PD during the period 2000–2011, there were 4,060 TCM users and 5,057 non-TCM users; of the former, 434 (10.7%) used TCM, 3,578 (88.1%) used drugs for PD, and 375 (9.2%) used TCM in combination with drugs for the treatment of PD. Sex, age, occupational status, and residential areas are factors that may affect the use of TCM. Females were more likely to use TCM than males (51.1% vs. 48.9%; adjusted OR = 1.15). The mean age of TCM users (67.2 years) was lower than that of non-TCM users (72.8 years). Most of the TCM users were older than 60 years (77.1%). Younger patients were more likely to pursue TCM therapy than older patients. The adjusted ORs were 2.61 in the 20- to 29-year-old age group, 1.38 in the 30- to 39-year-old age group, 1.82 in the 40- to 49-year-old age group, and 1.63 in the 50- to 59-year-old age group. Overall, TCM users were more likely to be female, younger, of white-collar status, and living in Central Taiwan. The adjusted ORs and 95% CIs are shown in Table 1.
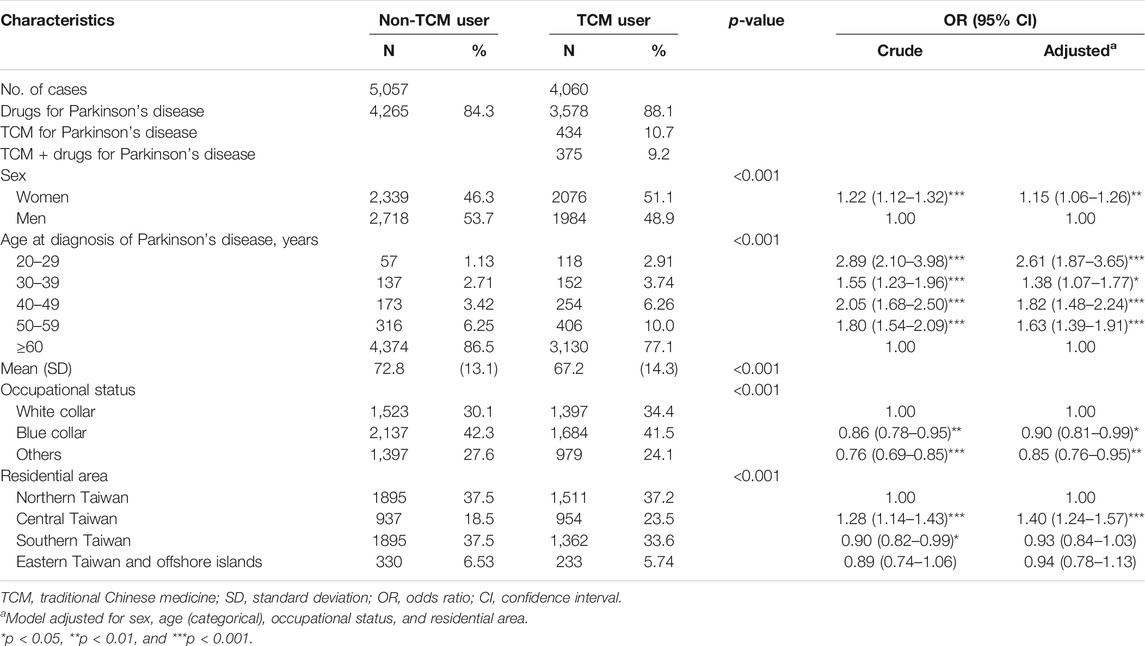
TABLE 1. Demographic characteristics and results of multiple logistic regression models showing the adjusted odds ratio and 95% confidence intervals for use of traditional Chinese medicine among patients with Parkinson’s disease during 2000–2011 in Taiwan.
An average of 5.65 CHPs were used in a single prescription for PD patients. Most prescriptions for PD involved 4 CHPs (22.4%) each, followed by prescriptions with 5 CHPs (16.2%) and prescriptions with 3 CHPs (12.1%). The most commonly used CHPs for PD by TCM doctors are shown in Table 2. Chaihu-Jia-Longgu-Muli-Tang (CJLMT, 2.7%) was the most commonly used formula, followed by Ma-Zi-Ren-Wan (MZRW, 2.12%), Shao-Yao-Gan-Cao-Tang (SYGCT, 1.58%), Tian-Wang-Bu-Xin-Dan (TWBXD, 1.57%), and Ping-Wei-San (PWS, 1.27%). The most commonly used single herbs were Uncaria tomentosa (Willd. ex Schult.) DC. (2.84%) followed by Gastrodia elata Blume (2.32%), Radix et Rhizoma Rhei (Rheum palmatum L., Rheum tanguticum Maxim. ex Balf., and Rheum officinale Baill.) (1.99%), Salvia miltiorrhiza Bunge (1.74%), and Polygala tenuifolia Willd. (1.55%) (Table 3).
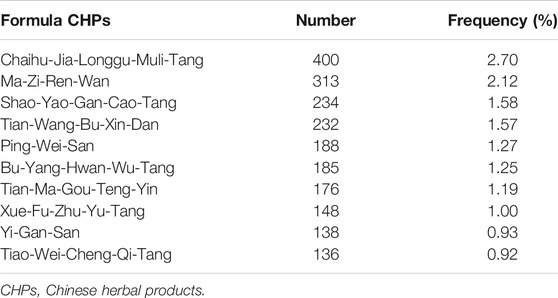
TABLE 2. The top-10 formula Chinese herbal products (CHPs) prescribed by traditional Chinese medicine physicians for treating patients with Parkinson’s disease during 2000–2011 in Taiwan (total number of CHPs, n = 14,794).
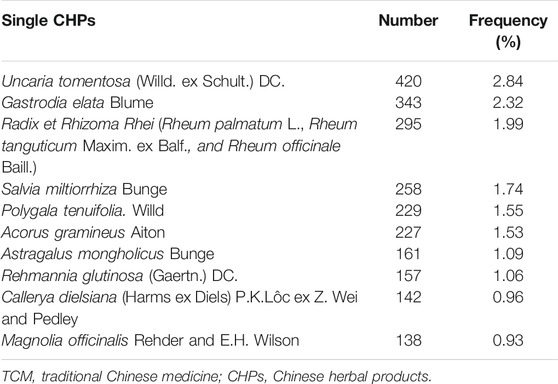
TABLE 3. The top-10 single Chinese herbal products (CHPs) prescribed by traditional Chinese medicine physicians for treating patients with Parkinson’s disease during 2000–2011 in Taiwan (total number of CHPs, n = 14,794).
The top-three most commonly used formula CHPs of two combinations for PD were CJLMT plus MZRW (0.77%), TWBXD plus CJLMT (0.69%), and PWS plus Tiao-Wei-Cheng-Qi-Tang (0.62%) (Table 4). The top-three most commonly used single CHPs of two combinations were U. tomentosa (Willd. ex Schult.) DC. plus G. elata Blume (0.83%), Acorus gramineus Aiton plus P. tenuifolia Willd. (0.56%), and Melia azedarach L. plus Fritillaria cirrhosa D. Don (0.49%) (Table 5).

TABLE 4. The top-5 most used formula Chinese herbal products (CHPs) of two combinations for Parkinson’s disease during 2000–2011 in Taiwan (total number of CHPs, n = 14,794).
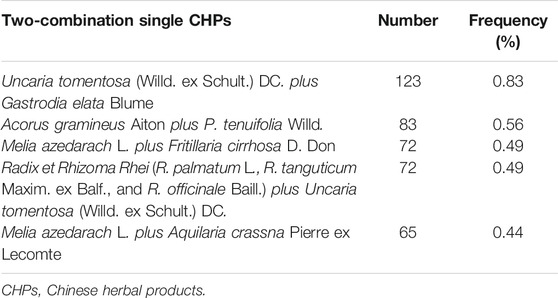
TABLE 5. The top-5 most used single Chinese herbal products (CHPs) of two combinations for Parkinson’s disease in Taiwan during 2000–2011 (total number of CHPs, n = 14,794).
We used the NHIRD to conduct a population-based cohort study to identify the prescription patterns of CHPs for patients with PD on a nationwide scale in Taiwan. This study reveals that CJLMT and U. tomentosa (Willd. ex Schult.) DC. are the most commonly used formula and single herb CHPs, respectively, for PD in Taiwan.
We further analyzed the factors that may affect TCM use by PD patients (Table 1). Females were more likely to use TCM treatment than males, consistent with the findings of Hung et al. in patients with ischemic stroke (Hung et al., 2015a). Furthermore, younger patients were more likely to use TCM than older individuals, concordant with the findings of Liao et al. in patients with chronic obstructive pulmonary disease (Liao et al., 2017). Thus, younger PD patients are more inclined to use TCM to treat their disease and maintain their daily activities, likely due to their aptitude in exploring their disease and its potential treatments. There has been no previous report regarding the relationship between TCM treatment and socioeconomic status; we found that blue-collar workers or those with other occupational statuses were less likely to seek TCM treatment than white-collar workers. Moreover, compared to the PD patients in Northern Taiwan, the PD patients in Central Taiwan tended to seek TCM treatments more often, concordant with the finding of Hung et al. that there are more TCM physicians and TCM clinics in this region than in other areas of Taiwan (Hung et al., 2015b). Therefore, people in Central Taiwan are more likely to seek combined treatment for various diseases, or to consider TCM first, than individuals residing in other areas in Taiwan.
In TCM theory, PD is characterized by tremors or muscle rigidity, which are caused by “Gan and Shan Yin deficiency,” and could result in malnourishment of the muscle, leading to “Gan Qi stagnation,” “Gan Yang excessive,” and “Endogenous Gan wind,” (Su et al., 2016). Based on the syndrome differentiation, the most common TCM syndrome patterns of PD are “Gan and Shan Yin deficiency,” “deficiency of Qi and blood,” “phlegm heat and wind stirring,” “blood stasis and wind stirring,” and “Qi stagnation and blood stasis” (Chen et al., 2017). CHPs are used depending on the syndrome differentiation. For example, Liu-Wei-Di-Huang-Wan is used for Gan and Shan Yin deficiency, and Tian-Ma-Gou-Teng-Yin is used for phlegm heat and wind stirring (Lu et al., 2016). A recent systematic review showed that several herbal extracts or their bioactive compounds had neuroprotective, neuroregenerative, and anti-oxidant properties that could reduce neuronal loss or neurodegeneration in PD models. These CHPs include Cistanches salsa Beck, Scutellaria baicalensis Georgi, Curcuma longa L., Carthamus tinctorius L., Panax ginseng C.A. Mey., and Silybum marianum (L.) Gaertn. (da Costa et al., 2017). However, as described above, the clinical indications of CHPs for specific diseases remain controversial. In our statistical analysis, we found that the most commonly used formula CHPs and herbs are CJLMT, MZRW, SYGCT, U. tomentosa (Willd. ex Schult.) DC., G. elata Blume, and Radix et Rhizoma Rhei (R. palmatum L., R. tanguticum Maxim. ex Balf., and R. officinale Baill.). The results of this study provide insights regarding personalized therapies and may form the basis for further clinical experiments and pharmacological research on the use of CHPs for the management of PD. The possible mechanisms underlying the effects of the CHPs, based on a review of the literature, are discussed below to provide insight into their pharmaceutical use.
CJLMT could harmonize Shaoyang, improve sleep quality, and alleviate depression. One of the mechanisms underlying depression includes decreased levels of monoamine neurotransmitters (norepinephrine, dopamine, and serotonin) and brain-derived neurotrophic factor in the hippocampus and prefrontal cortex. This effect can be reversed by the administration of antidepressants, such as monoamine oxidase inhibitors or selective serotonin reuptake inhibitors (Savegnago et al., 2007; Zhang et al., 2010). Saponins, which are extracted from CJLMT, were found to have antidepressant-like effects in rats; they increased the concentration of serotonin and promoted the expression of brain-derived neurotrophic factor in both the prefrontal cortex and hippocampus (Li et al., 2012). Moreover, an increase in the number of apoptotic cells in the hippocampus and cortex was found in a rat depression model, while antidepressants had an anti-apoptotic effect to protect the cells (Lucassen et al., 2004). Research has found that both saponins and antidepressants can inhibit Bax and caspase-3 (the protein associated with apoptosis) expression in the hippocampus in mice, which implies that CJLMT had an antidepressant effect via neuroprotection (Liu et al., 2010). Another rapid antidepressant is ketamine, which downregulates the N-methyl-D-aspartic acid receptor, and then upregulates the signal pathway of mammalian targets of rapamycin and α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptors in the prefrontal cortex and brain-derived neurotrophic factor expression in the hippocampus. Research has shown that CJLMT can downregulate the N-methyl-D-aspartic acid receptor expression, thus resulting in a rapid antidepressant effect similar to that of ketamine (Wang et al., 2019).
The second most commonly used formula was MZRW, which is described to treat constipation in Shang Han Lun, and was effective against functional constipation in previous clinical trials (Zhong et al., 2013). Patients with PD have decreased phasic rectal contractions, weak abdominal wall contraction, paradoxical anal sphincter contraction during defecation, and defects in enteric nervous system dopaminergic neurons (Feldman et al., 2016). MZRW contains bowel-stimulating components, including aloe emodin, rhein, emodin, hesperidin, and paeoniflorin (Hu et al., 2015). Rhein and aloe emodin, extracted from Radix et Rhizoma Rhei (R. palmatum L., R. tanguticum Maxim. ex Balf., and R. officinale Baill.), were applied in a constipation rat model. The Cmax and AUC of emodin in constipated rats were about ten times those of normal rats, while the t1/2 was remarkably decreased. However, a significant decrease in the AUC values for aloe emodin and rhein was observed in constipated rats compared to normal rats. Significant differences in the main pharmacokinetic parameters were found in normal and constipated rats. The study suggested that rhein and aloe emodin directly affect intestinal cell membranes, whereas emodin indirectly affects bowel movement through adjustment of the nervous system (Gong et al., 2015). Hesperidin and paeoniflorin, extracted from Citrus aurantium L. and Paeonia lactiflora Pall., respectively, have also been shown to stimulate gastrointestinal movement via the H1 histamine receptor (Fang et al., 2009).
SYGCT is typically used for Gan dysfunction, muscle cramping, spasticity, or tremors, according to Chinese medical theory. Paeonia lactiflora Pall. has antispastic and analgesic effects, whereas Glycyrrhiza glabra L. has analgesic and anti-inflammatory effects (Takao et al., 2015). SYGCT may normalize intracellular and extracellular potassium balance by inhibiting the ultra-rapid delayed rectifier potassium current and reducing potassium efflux, while the sodium-potassium pump promotes potassium influx into myofibers. Consequently, excess potassium may be reduced in the external space of myofibers. Thus, SYGCT may balance intracellular and extracellular potassium levels, and the resulting reduction in potassium levels in the external space of myofibers could alleviate muscle pain (Suganami et al., 2014). One of the components of Glycyrrhiza glabra L., licochalcone A, has neuroprotective as well as anti-inflammatory effects and prevents the reduction of dopaminergic neurons in PD models by inhibiting microglia-mediated neuroinflammation (Huang et al., 2017). Paeoniflorin, another bioactive component of Paeonia lactiflora Pall., reduces the acidosis-induced accumulation of α-synuclein and promotes autophagic degradation of α-synuclein by regulating both the expression and activity of acid-sensing ion channels, which are ligand-gated cation channels that respond to acidic stimuli (Sun et al., 2011). α-Synuclein aggregation is associated with PD pathophysiology and results in intracellular oxidative stress, inflammation, and apoptosis; thus, Paeonia lactiflora Pall. protects against α-synuclein cytotoxicity (Shah et al., 2014).
TWBXD is commonly used for insomnia in TCM practice. A systematic review showed the promising effect of TWBXD regarding alleviating insomnia (Yang et al., 2019). PWS is a commonly used medication for gastrointestinal disorders in TCM practice. The mechanisms of Western medicines for the treatment of functional dyspepsia include acid suppression, gastric mucosa protection, gastric motility promotion, and anti-Helicobacter pylori activity. Both clinical and laboratory research studies indicate that liver stagnation and spleen deficiency are the main syndromes of functional dyspepsia. Substance P is one of the most important brain–gut peptides in mammals and is composed of 11 amino acids. It is mainly distributed in the central nervous system, spinal cord dorsal root, and ENS. It promotes gastrointestinal peristalsis, protects the gastrointestinal epithelium to repair the impaired gastrointestinal mucosa, and causes gastric and intestinal mechanical hypersensitivity (Lin et al., 2012). PWS had therapeutic effects in rats with functional dyspepsia by influencing both brain–gut substance P and vasoactive intestinal peptide levels (Du et al., 2018).
U. tomentosa (Willd. ex Schult.) DC. was the most commonly used single herb for PD treatment; it relieves “Gan Yang excessive” and “endogenous Gan wind” according to Chinese medical theory. U. tomentosa (Willd. ex Schult.) DC. has protective effects on dopaminergic neurons by reducing reactive oxygen species (ROS) generation; it increased glutathione levels and inhibited caspase-3 activity in a PD cell model (Shim et al., 2009).
The second most commonly used single herb was G. elata Blume. G. elata Blume decreased L-3,4-dihydroxyphenylalanine (L-DOPA)-induced dyskinesia in a PD mouse model by inhibiting phosphorylated extracellular regulated protein kinases (pERK) and FBJ murine osteosarcoma viral oncogene homolog B (FosB) expression, which are abnormally activated by long-term use of L-DOPA (Doo et al., 2014). G. elata Blume ameliorated the rotation behavior in PD rats and enhanced the expression of tyrosine hydroxylase positive neurons in the midbrain ventral tegmental area, displaying a neuroprotective effect on tyrosine hydroxylase positive neurons (Wang et al., 2013a). Another study in a cell model of PD revealed that a compound isolated from G. elata Blume had neuroprotective effects by reducing apoptosis and oxidative stress via activation of the nuclear factor erythroid 2-related factor 2 (Nrf2)/anti-oxidant response element (ARE)/heme oxygenase-1 (HO-1) signaling pathway (Huang et al., 2016).
Radix et Rhizoma Rhei (R. palmatum L., R. tanguticum Maxim. ex Balf., and R. officinale Baill.), which is the third most commonly used single herb for PD, is used for constipation, jaundice, ulcers, and hemorrhages in TCM. It has been shown to exert anti-neuro-inflammatory effects by downregulating the mitogen-activated protein kinase and nuclear factor kappa B pathway, decreasing nitric oxide (NO) and ROS formation and inhibiting lipopolysaccharide-induced neuroinflammation in an animal study (Hwang et al., 2018). Rhein and aloe emodin are components with effects on bowel movements, as stated above.
Salvia miltiorrhiza Bunge is commonly used for dysmenorrhea, irregular menstrual cycles, ecchymosis, and insomnia in TCM practice. S. miltiorrhiza Bunge was found to inhibit α-synuclein aggregation both in vitro and in a PD model (Ji et al., 2016). Moreover, one of the effective components, tanshinone IIA, exerts neuroprotective effects by reducing the expression of lactaldehyde reductase (NADPH) oxidase and inducible nitric oxide synthase, which could further prevent nigrostriatal dopaminergic neuron loss (Ren et al., 2015).
P. tenuifolia Willd. is commonly used for insomnia and palpitation in TCM practice. P. tenuifolia Willd. exhibits anti-oxidant and anti-apoptotic activity by inhibiting ROS and NO production, which protected dopaminergic neurons in the substantia nigra and striatum against toxicity in a mouse study (Choi et al., 2011). The effects and mechanisms of the top-5 formula and single CHPs are listed in Table 6.
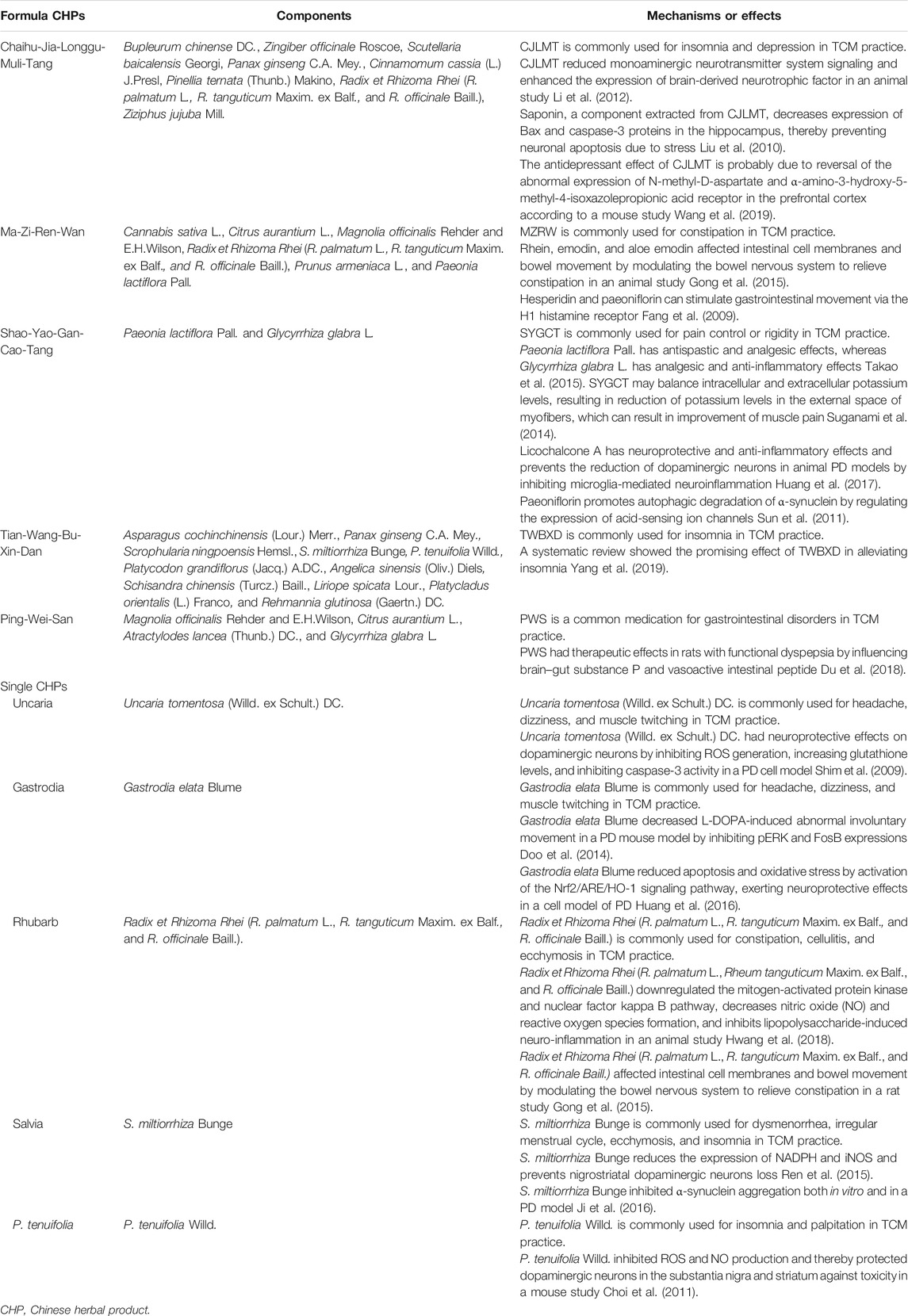
TABLE 6. Possible mechanisms underlying the effects of frequently used Chinese herbal products (CHPs) for Parkinson’s disease, ranked by prevalence of use.
In TCM theory, “Gan Qi stagnation” is one of the TCM syndromes of PD, and it can further result in depression, anxiety, or insomnia. The frequency of use of a CHP or CHP combination represents the priority of the frequency of symptoms (Ling, 2013). CJLMT can not only relieve “Gan Qi stagnation” but also improve psychiatric symptoms and constipation (Liang and Yang, 2018). PD involves both motor and non-motor symptoms (NMSs). NMSs include mood disorders, such as apathy, anhedonia, depression, cognitive dysfunction, and hallucinosis, as well as complex behavioral disorders (Lee and Andrew, 2016; Shi et al., 2017). CJLMT is used based on the syndrome differentiation of PD, and it also relieves the NMSs of PD. Hence, it is the most commonly used CHPs formula for PD. U. tomentosa (Willd. ex Schult.) DC. is used for "wind stirring" which results from “Gan Qi stagnation” and “Gan and Shan Yin deficiency.” U. tomentosa (Willd. ex Schult.) DC. is one of the major components of Tian-Ma-Gou-Teng-Yin and is used for “Gan and Shan Yin deficiency” with “wind stirring,” which improves tremors and insomnia in PD patients (Yang et al., 2017). Another study showed that the combined use of CJLMT and Zhichan decoction (the latter contains U. tomentosa (Willd. ex Schult.) DC.) can relieve “Gan Qi stagnation” and “Gan and Shan Yin deficiency.” This formula also improved insomnia, psychiatric symptoms, and tremors in PD patients (Jiang, 2019). Current research shows that U. tomentosa (Willd. ex Schult.) DC. has neuroprotective effects on dopaminergic neurons by inhibiting ROS generation, increasing glutathione levels; inhibiting caspase-3 activity (Shim et al., 2009); increasing cell viability and mitochondrial membrane potential; decreasing lipid peroxidation, intracellular ROS, and nitric oxide; and reducing the aggregation of α-synuclein (Shi et al., 2013). Hence, it is reasonable that U. tomentosa (Willd. ex Schult.) DC. is the most commonly used single CHP for PD. Our data showed that these are common PD prescriptions in Taiwan, and they may therefore be candidates for further investigations as treatments for NMSs in patients with PD.
Current research is focused on ways to increase the level of levodopa in the brain while inhibiting peripheral levodopa metabolism in order to minimize the side-effects of the medications for PD (Setty and Sigal, 2005). A meta-analysis has shown that combining TCM with dopamine-replacement therapy is generally safe and could improve the Unified Parkinson’s Disease Rating Scale score in PD patients (Zhang et al., 2015). Based on our findings of the top-5 formula and single CHPs for PD, Table 6 shows the possible mechanisms underlying the effects of frequently used CHPs for PD, ranked by prevalence of use. These CHPs may be taken into consideration as adjunctive treatment for NMSs in patients with PD and improving the side-effects of medications for PD, according to syndrome differentiation.
A few crude medicinal herbs, over-the-counter herbal treatments, health foods containing herbs, and herbs obtained without a physician’s prescription were not included in the classification surveyed in this study. Some Chinese herbal medications can be obtained from TCM pharmacies without a prescription; therefore, the frequency of CHPs usage might have been underreported in our study. However, because the NHI system has a wide coverage of TCM prescriptions, the likelihood that patients acquired substantial quantities of herbs outside of the NHI database is very small.
The NHIRD is a large, integrative database, which includes 22.60 million people out of the 22.96 million population in Taiwan. Therefore, it contained TCM prescription patterns and clinical records that were reflective of the general Taiwanese population. However, this study had several limitations. First, the effectiveness, adverse effects, and mechanisms of these CHPs for PD were not available from this study. The NHIRD could offer prescription data; however, the chart-level records, such as laboratory data and physician notes, were not available. Second, in Taiwan, approximately 5% of TCM clinics are not contracted with the NHI program; therefore, the usage rate of TCM may have been underestimated (Chang et al., 2015). Third, patients with PD present various TCM syndromes. The NHIRD did not include data that allowed differentiation between the types of TCM syndromes in PD patients and their corresponding prescriptions. Further basic research could be conducted based on the results of this study.
The most commonly used formula and single CHPs identified in this retrospective cohort study have been shown to have potential neuroprotective effects in PD by exerting anti-inflammatory, anti-oxidative, and anti-apoptotic effects. They also have effects on “Gan Qi stagnation” and “wind stirring” according to the TCM syndrome differentiation. Moreover, CJLMT has therapeutic effects on constipation, insomnia, and depression, which are common NMSs of PD. TCM adjuvant therapy may improve clinical symptoms of PD and relieve the side-effects of PD medications. Further studies are warranted to investigate the underlying mechanisms and the effectiveness of CJLMT and U. tomentosa (Willd. ex Schult.) DC. and to verify their use for the treatment of PD or as adjunctive medication that can be used in combination with dopaminergic agents.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding authors.
The study was approved by the Institutional Review Board of China Medical University and Hospital (CMUH104-REC2-115).
C-EK, Y-CH, and W-LH were responsible for the study concept and design. CH and H-JC contributed to the acquisition of data. C-HL, C-EK, Y-CH, and W-LH contributed to the data analysis and interpretation of data. C-HL, HC, C-EK, and W-LH drafted the manuscript. HC, S-FH, S-YW, S-TT, and T-CW critically reviewed the manuscript. All authors approved final version for publication.
This study was supported in part by the Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW108-TDU-B-212-133004), China Medical University Hospital, Academia Sinica Stroke Biosignature Project (BM10701010021), MOST Clinical Trial Consortium for Stroke (MOST 107-2321-B-039-04), Tseng-Lien Lin Foundation, Taichung, Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds, Japan. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
ARE, anti-oxidant response element; CAM, complementary and alternative medicine; CHP, Chinese herbal products; CI, confidence interval; CJLMT, Chaihu-Jia-Longgu-Muli-Tang; FosB, FBJ murine osteosarcoma viral oncogene homolog B; HO-1, heme oxygenase-1; iNOS, inducible nitric oxide synthase; LHID, longitudinal health insurance database; MZRW, Ma-Zi-Ren-Wan; NHI, National Health Insurance; NHIRD, National Health Insurance Research Database; NMS, non-motor symptoms; NO, nitric oxide; Nrf2, nuclear factor erythroid 2-related factor 2; OR, odds ratio; PD, Parkinson’s disease; pERK, phosphorylated extracellular regulated protein kinases; PWS, Ping-Wei-San; ROS, reactive oxygen species; SYGCT, Shao-Yao-Gan-Cao-Tang; TCM, traditional Chinese medicine; TWBXD, Tian-Wang-Bu-Xin-Dan.
Chang, C. M., Chu, H. T., Wei, Y. H., Chen, F. P., Wang, S., Wu, P. C., et al. (2015). The core pattern analysis on Chinese herbal medicine for Sjogren’s syndrome: a nationwide population-based study. Sci. Rep. 5, 9541. doi:10.1038/srep09541
Chen, H., Zhang, Z., He, J., Teng, L., and Yuan, C. (2017). Traditional Chinese medicine symptom pattern analysis for Parkinson’s disease. J. Tradit. Chin. Med. 37 (5), 688–694. doi:10.1016/S0254-6272(17)30324-2
Choi, J. G., Kim, H. G., Kim, M. C., Yang, W. M., Huh, Y., Kim, S. Y., et al. (2011). Polygalae radix inhibits toxin-induced neuronal death in the Parkinson’s disease models. J. Ethnopharmacol. 134 (2), 414–421. doi:10.1016/j.jep.2010.12.030
Clarke, T. C., Black, L. I., Stussman, B. J., Barnes, P. M., and Nahin, R. L. (2015). Trends in the use of complementary health approaches among adults: United States, 2002-2012. Natl. Health Stat. Report 10 (79), 1–16
da Costa, I. M., Cavalcanti, J., de Queiroz, D. B., de Azevedo, E. P., do Rêgo, A., Araújo Filho, I., et al. (2017). Supplementation with herbal extracts to promote behavioral and neuroprotective effects in experimental models of Parkinson’s disease: a systematic review. Phytother. Res. 31 (7), 959–970. doi:10.1002/ptr.5813
Doo, A. R., Kim, S. N., Hahm, D. H., Yoo, H. H., Park, J. Y., Lee, H., et al. (2014). Gastrodia elata Blume alleviates L-DOPA-induced dyskinesia by normalizing FosB and ERK activation in a 6-OHDA-lesioned Parkinson’s disease mouse model. BMC Compl. Alternative Med. 14, 107. doi:10.1186/1472-6882-14-107
Du, X., Liang, Q., Zhao, L., Liang, J., Mao, L., Lu, Y., et al. (2018). The changes of brain-gut SP and VIP levels in the rats with functional dyspepsia and the intervention of Pingwei capsule. J. Gastro. Hepat. Res. 7 (1), 2521–2529. doi:10.17554/j.issn.2224-3992.2018.07.749
Fang, Y. S., Shan, D. M., Liu, J. W., Xu, W., Li, C. L., Wu, H. Z., et al. (2009). Effect of constituents from Fructus Aurantii Immaturus and Radix Paeoniae Alba on gastrointestinal movement. Planta. Med. 75 (1), 24–31. doi:10.1055/s-0028-1088342
Feldman, M., Friedman, L. S., and Brandt, L. J. (2016). “Sleisenger and Fordtran’s gastrointestinal and liver disease: pathophysiology, diagnosis, management,” in Constipation. Editor AJ Lembo. 10th Edn (Philadelphia, WB: Saunders), 270–296.
Ferreira, J. J., Rocha, J. F., Falcão, A., Santos, A., Pinto, R., Nunes, T., et al. (2015). Effect of opicapone on levodopa pharmacokinetics, catechol-O-methyltransferase activity and motor fluctuations in patients with Parkinson’s disease. Eur. J. Neurol. 22 (5), 815–e56. doi:10.1111/ene.12666
Gong, X. H., Li, Y., Zhang, R. Q., Xie, X. F., Peng, C., and Li, Y. X. (2015). The synergism mechanism of Rhubarb anthraquinones on constipation elucidated by comparative pharmacokinetics of Rhubarb extract between normal and diseased rats. Eur. J. Drug Metab. Pharmacokinet. 40 (4), 379–388. doi:10.1007/s13318-014-0216-7
Han, L., Xie, Y. H., Wu, R., Chen, C., Zhang, Y., and Wang, X. P. (2017). Traditional Chinese medicine for modern treatment of Parkinson’s disease. Chin. J. Integr. Med. 23 (8), 635–640. doi:10.1007/s11655-016-2537-7
Hasan, S. S., See, C. K., Choong, C. L., Ahmed, S. I., Ahmadi, K., and Anwar, M. (2010). Reasons, perceived efficacy, and factors associated with complementary and alternative medicine use among Malaysian patients with HIV/AIDS. J. Alternative Compl. Med. 16 (11), 1171–1176. doi:10.1089/acm.2009.0657
Hu, D. D., Han, Q. B., Zhong, L. L., Li, Y. H., Lin, C. Y., Ho, H. M., et al. (2015). Simultaneous determination of ten compounds in rat plasma by UPLC-MS/MS: Application in the pharmacokinetic study of Ma-Zi-Ren-Wan. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 1000, 136–146. doi:10.1016/j.jchromb.2015.07.003
Huang, B., Liu, J., Ju, C., Yang, D., Chen, G., Xu, S., et al. (2017). Licochalcone A prevents the loss of dopaminergic neurons by inhibiting microglial activation in lipopolysaccharide (LPS)-Induced Parkinson’s disease models. Int. J. Mol. Sci. 18 (10), 2043. doi:10.3390/ijms18102043
Huang, J. Y., Yuan, Y. H., Yan, J. Q., Wang, Y. N., Chu, S. F., Zhu, C. G., et al. (2016). 20C, a bibenzyl compound isolated from Gastrodia elata, protects PC12 cells against rotenone-induced apoptosis via activation of the Nrf2/ARE/HO-1 signaling pathway. Acta Pharmacol. Sin. 37 (6), 731–740. doi:10.1038/aps.2015.154
Hung, I. L., Hung, Y. C., Wang, L. Y., Hsu, S. F., Chen, H. J., Tseng, Y. J., et al. (2015a). Chinese herbal products for ischemic stroke. Am. J. Chin. Med. 43 (7), 1365–1379. doi:10.1142/S0192415X15500779
Hung, Y. C., Tseng, Y. J., Hu, W. L., Chen, H. J., Li, T. C., Tsai, P. Y., et al. (2015b). Demographic and prescribing patterns of Chinese herbal products for individualized therapy for ischemic heart disease in Taiwan: population-based study. PLoS One 10 (8), e0137058. doi:10.1371/journal.pone.0137058
Hwang, D. S., Gu, P. S., Kim, N., Jang, Y. P., and Oh, M. S. (2018). Effects of Rhei Undulati Rhizoma on lipopolysaccharide-induced neuroinflammation in vitro and in vivo. Environ. Toxicol. 33 (1), 23–31. doi:10.1002/tox.22463
Ji, K., Zhao, Y., Yu, T., Wang, Z., Gong, H., Yang, X., et al. (2016). Inhibition effects of tanshinone on the aggregation of α-synuclein. Food Funct. 7 (1), 409–416. doi:10.1039/c5fo00664c
Jiang, L. H. (2019). Zhichan decoction and Chaihu Longgu Muli decoction in treating Parkinson’s disease complicated with depression for 42 cases. Chin. Med. Mod. Dis. Ed. of China 17 (13), 90–91. doi:10.3969/j.issn.1672-2779.2019.13.037
Lee, G., and Andrew, S. I. (2016). “Goldman-cecil medicine,” in Parkinsonism. Editor A. E Lang. 25th Edn (Philadelphia, WB: Saunders), 2454–2461.
Li, L. F., Lu, J., Li, X. M., Xu, C. L., Yang, J., Qu, R., et al. (2012). Antidepressant-like effects of the saponins extracted from Chaihu-jia-longgu-muli-tang in a rat unpredictable chronic mild stress model. Fitoterapia. 83 (1), 93–103. doi:10.1016/j.fitote.2011.09.017
Liang, M. Q., and Yang, N. (2018). Study on the formula-syndrome correspondence of Chaihu Longgu Muli decoction in treating nonmotor symptoms of Parkinson’s disease. J. Tradit. Chin. Med. 59 (24), 2148–2151. doi:10.13288/j.11-2166/r.2018.24.017
Liao, Y. N., Hu, W. L., Chen, H. J., and Hung, Y. C. (2017). The use of Chinese herbal medicine in the treatment of chronic obstructive pulmonary disease (COPD). Am. J. Chin. Med. 45 (2), 225–238. doi:10.1142/S0192415X17500148
Lin, C. C., Chen, W. N., Chen, C. J., Lin, Y. W., Zimmer, A., and Chen, C. C. (2012). An antinociceptive role for substance P in acid-induced chronic muscle pain. Proc. Natl. Acad. Sci. U.S.A. 109 (2), E76–E83. doi:10.1073/pnas.1108903108
Ling, Y. (2013). Traditional Chinese medicine in the treatment of symptoms in patients with advanced cancer. Ann. Palliat. Med. 2 (3), 141–152. doi:10.3978/j.issn.2224-5820.2013.04.05
Liu, Y., Ma, S., and Qu, R. (2010). SCLM, total saponins extracted from Chaihu-jia-longgu-muli-tang, reduces chronic mild stress-induced apoptosis in the hippocampus in mice. Pharm. Biol. 48 (8), 840–848. doi:10.3109/13880200903296154
Lu, Y. Y., Liu, Y. X., and Xiong, D. (2016). Parkinson’s disease treated with traditional Chinese medicine. J. of Chan. Univ.Chin. Med. 32 (2), 433–436. doi:10.13463/j.cnki.cczyy.2016.02.081
Lucassen, P. J., Fuchs, E., and Czeh, B. (2004). Antidepressant treatment with tianeptine reduces apoptosis in the hippocampal dentate gyrus and temporal cortex. Biol. Psychiatr. 55 (8), 789–796. doi:10.1016/j.biopsych.2003.12.014
Medagama, A. B., and Bandara, R. (2014). The use of complementary and alternative medicines (CAMs) in the treatment of diabetes mellitus: is continued use safe and effective? Nutr. J. 13, 102. doi:10.1186/1475-2891-13-102
Ren, B., Zhang, Y. X., Zhou, H. X., Sun, F. W., Zhang, Z. F., Wei, Z., et al. (2015). Tanshinone IIA prevents the loss of nigrostriatal dopaminergic neurons by inhibiting NADPH oxidase and iNOS in the MPTP model of Parkinson’s disease. J. Neurol. Sci. 348 (1), 142–152. doi:10.1016/j.jns.2014.11.026
Rocha, J. F., Sicard, É., Fauchoux, N., Falcão, A., Santos, A., Loureiro, A. I., et al. (2017). Effect of opicapone multiple-dose regimens on levodopa pharmacokinetics. Br. J. Clin. Pharmacol. 83 (3), 540–553. doi:10.1111/bcp.13156
Savegnago, L., Jesse, C. R., Pinto, L. G., Rocha, J. B., Nogueira, C. W., and Zeni, G. (2007). Monoaminergic agents modulate antidepressant-like effect caused by diphenyl diselenide in rats. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 31 (6), 1261–1269. doi:10.1016/j.pnpbp.2007.05.006
Setty, A. R., and Sigal, L. H. (2005). Herbal medications commonly used in the practice of rheumatology: mechanisms of action, efficacy, and side effects. Semin. Arthritis Rheum. 34 (6), 773–784. doi:10.1016/j.semarthrit.2005.01.011
Shah, M., Seibyl, J., Cartier, A., Bhatt, R., and Catafau, A. M. (2014). Molecular imaging insights into neurodegeneration: focus on α-synuclein radiotracers. J. Nucl. Med. 55 (9), 1397–1400. doi:10.2967/jnumed.113.136515
Shi, J., Tian, J., Li, T., Qin, B., Fan, D., Ni, J., et al. (2017). Efficacy and safety of SQJZ herbal mixtures on nonmotor symptoms in Parkinson disease patients: protocol for a randomized, double-blind, placebo-controlled trial. Medicine (Baltimore). 96 (50), e8824. doi:10.1097/MD.0000000000008824
Shi, Z., Lu, Z., Zhao, Y., Wang, Y., Zhao-Wilson, X., Guan, P., et al. (2013). Neuroprotective effects of aqueous extracts of Uncaria tomentosa: insights from 6-OHDA induced cell damage and transgenic Caenorhabditis elegans model. Neurochem. Int. 62 (7), 940–947. doi:10.1016/j.neuint.2013.03.001
Shim, J. S., Kim, H. G., Ju, M. S., Choi, J. G., Jeong, S. Y., and Oh, M. S. (2009). Effects of the hook of Uncaria rhynchophylla on neurotoxicity in the 6-hydroxydopamine model of Parkinson’s disease. J. Ethnopharmacol. 126 (2), 361–365. doi:10.1016/j.jep.2009.08.023
Spindler, M. A., and Tarsy, D. (2019). “Initial pharmacologic treatment of Parkinson disease,” in UpToDate. Editor H. I. Hurtig (Waltham, MA.(Accessed May 1, 2019)
Su, Q. Z., Liang, H. F., An, C., Li, Z., and Luo, X. D. (2016). [Pathogenesis of Parkinson’s disease viewing from modern Chinese medicine]. Zhongguo Zhong Xi Yi Jie He Za Zhi. 36 (12), 1515–1517. doi:10.7661/CJIM.2016.12.1515
Suganami, A., Sakamoto, K., Ono, T., Watanabe, H., Hijioka, N., Murakawa, M., et al. (2014). The inhibitory effect of shakuyakukanzoto on K+ current in H9c2 cells. Fukushima J. Med. Sci. 60 (1), 22–30. doi:10.5387/fms.2013-16
Sun, X., Cao, Y. B., Hu, L. F., Yang, Y. P., Li, J., Wang, F., et al. (2011). ASICs mediate the modulatory effect by paeoniflorin on α-synuclein autophagic degradation. Brain Res. 1396 (17), 77–87. doi:10.1016/j.brainres.2011.04.011
Takao, Y., Takaoka, Y., Sugano, A., Sato, H., Motoyama, Y., Ohta, M., et al. (2015). Shakuyaku-kanzo-to (Shao-Yao-Gan-Cao-Tang) as treatment of painful muscle cramps in patients with lumbar spinal stenosis and its minimum effective dose. Kobe J. Med. Sci. 61 (5), E132–E137. doi:10.24546/81009388
Wang, X., Zou, Z., Shen, Q., Huang, Z., Chen, J., Tang, J., et al. (2019). Involvement of NMDA-AKT-mTOR signaling in rapid antidepressant-like activity of chaihu-jia-longgu-muli-tang on olfactory bulbectomized mice. Front. Pharmacol. 9, 1537. doi:10.3389/fphar.2018.01537
Wang, Y., Wu, Z., Liu, X., and Fu, Q. (2013a). Gastrodin ameliorates Parkinson’s disease by downregulating connexin 43. Mol. Med. Rep. 8 (2), 585–590. doi:10.3892/mmr.2013.1535
Wang, Y., Xie, C. L., Wang, W. W., Lu, L., Fu, D. L., Wang, X. T., et al. (2013b). Epidemiology of complementary and alternative medicine use in patients with Parkinson’s disease. J. Clin. Neurosci. 20 (8), 1062–1067. doi:10.1016/j.jocn.2012.10.022
Yang, K., Zou, J. L., and Ji, Y. X. (2017). Clinical effect observation of Tianma Gouteng decoction in the treatment of Parkinson’s disease. Clin. Res. Prac. 2 (9), 97–98. doi:10.19347/j.cnki.2096-1413.201709050
Yang, X. Q., Liu, L., Ming, S. P., Fang, J., and Wu, D. N. (2019). Tian Wang bu Xin dan for insomnia: a systematic review of efficacy and safety. Evid Based Complement Alternat. Med. 2019, 4260801. doi:10.1155/2019/4260801
Zhang, G., Xiong, N., Zhang, Z., Liu, L., Huang, J., Yang, J., et al. (2015). Effectiveness of traditional Chinese medicine as an adjunct therapy for Parkinson’s disease: a systematic review and meta-analysis. PLoS One 10 (3), e0118498. doi:10.1371/journal.pone.0118498
Zhang, Y., Gu, F. H., Chen, J., and Dong, W. Y. (2010). Chronic antidepressant administration alleviates frontal and hippocampal BDNF deficits in CUMS rat. Brain Res. 1366, 141–148. doi:10.1016/j.brainres.2010.09.095
Keywords: Chaihu-Jia-Longgu-Muli-Tang, Chinese herbal products, Chinese medicine, Parkinson’s disease, Uncaria tomentosa (Willd. ex Schult.) DC.
Citation: Lin C-H, Chiu HE, Wu S-Y, Tseng S-T, Wu T-C, Hung Y-C, Hsu CY, Chen H-J, Hsu S-F, Kuo C-E and Hu W-L (2021) Chinese Herbal Products for Non-Motor Symptoms of Parkinson’s Disease in Taiwan: A Population-Based Study. Front. Pharmacol. 11:615657. doi: 10.3389/fphar.2020.615657
Received: 09 October 2020; Accepted: 23 December 2020;
Published: 27 January 2021.
Edited by:
Huazheng Liang, Shanghai Fourth People’s Hospital, ChinaReviewed by:
Paul Chazot, Durham University, United KingdomCopyright © 2021 Lin, Chiu, Wu, Tseng, Wu, Hung, Hsu, Chen, Hsu, Kuo and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wen-Long Hu, b29sb25naHVAZ21haWwuY29t; Chun-En Kuo, bGVjaGVycmllc0BnbWFpbC5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.