 Elena Ramírez1*
Elena Ramírez1* Mikel Urroz1
Mikel Urroz1 Amelia Rodríguez1
Amelia Rodríguez1 Miguel González-Muñoz2Alberto Martín-Vega3Yuri Villán4Enrique Seco1Jaime Monserrat1
Miguel González-Muñoz2Alberto Martín-Vega3Yuri Villán4Enrique Seco1Jaime Monserrat1 Jesús Frías1Antonio J. Carcas1
Jesús Frías1Antonio J. Carcas1 Alberto M. Borobia1*
Alberto M. Borobia1*- 1Department of Clinical Pharmacology, La Paz University Hospital-IdiPAZ, School of Medicine, Autonomous University of Madrid, Madrid, Spain
- 2Department of Immunology, La Paz University Hospital-IdiPAZ, Madrid, Spain
- 3CSUR Coordination, La Paz University Hospital-IdiPAZ, Madrid, Spain
- 4Safety and Quality Unit, La Paz University Hospital-IdiPAZ, Madrid, Spain
BACKGROUND: From March to April 2020, Spain was the center of the SARS-CoV-2 pandemic, particularly Madrid with approximately 30% of the cases in Spain. The aim of this study is to report the suspected serious adverse drug reactions (SADRs) in COVID-19 patients vs. non-COVID-19 patients detected by the prospective pharmacovigilance program based on automatic laboratory signals (ALSs) in the hospital (PPLSH) during that period. We also compared the results with the suspected SADRs detected during the same period for 2019.
METHODS: All ALSs that reflected potential SADRs including neutropenia, pancytopenia, thrombocytopenia, anemia, eosinophilia, leukocytes in cerebrospinal fluid, hepatitis, pancreatitis, acute kidney injury, rhabdomyolysis, and hyponatremia were prospectively monitored in hospitalized patients during the study periods. We analyzed the incidence and the distribution of causative drugs for the COVID-19 patients.
RESULTS: The incidence rate of SADRs detected in the COVID-19 patients was 760.63 (95% CI 707.89–816.01) per 10,000 patients, 4.75-fold higher than the SADR rate for non-COVID-19 patients (160.15 per 10,000 patients, 95% CI 137.09–186.80), and 5.84-fold higher than the SADR rate detected for the same period in 2019 (130.19 per 10,000 patients, 95% CI 109.53–154.36). The most frequently related drugs were tocilizumab (59.84%), dexketoprofen (13.93%), azithromycin (8.43%), lopinavir-ritonavir (7.35%), dexamethasone (7.62%), and chloroquine/hydroxychloroquine (6.91%).
CONCLUSIONS: The incidence rate of SADRs detected by the PPSLH in patients with COVID-19 was 4.75-fold higher than that of the non-COVID-19 patients. Caution is recommended when using medications for COVID-19 patients, especially drugs that are hepatotoxic, myotoxic, and those that induce thromboembolic events.
Introduction
From March to April 2020, Spain was the center of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, (Center for Coordination of Health Alerts and Emergencies) with Madrid accounting for approximately 30% of the cases in Spain. (Current situation in the Community of Madrid) In response, the Spanish Ministry of Health published protocols for the care and management of COVID-19 patients. Azithromycin, chloroquine, hydroxychloroquine and lopinavir/ritonavir have been recommended for treatment during the infectious phase. Subsequently, anti-inflammatory drugs (such as corticosteroids and other compounds) were recommended for COVID-19 patients who progressed to the inflammatory phase of the disease. The drugs employed during that period were off-label or under development as potential treatment options for COVID-19.
In this situation, more attention should be paid to the safety of these drugs, whose toxicity profile is relatively well understood based on trials and the post-marketing experience in the indications for which they are approved. (Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products) Although the most frequent reactions to these drugs are usually mild, serious adverse effects have also been reported with their use. It is also unclear whether the use of these drugs by COVID-19 patients poses greater risks, because COVID-19 itself could be a predisposing factor to certain serious adverse drug reactions (SADRs).
In recent decades, large, computerized clinical databases linked to electronic medical records (EMRs) have helped implement prospective programs for detecting SADRs and aiding clinicians in reacting quickly and appropriately to these reactions. (Hannan, 1999) Since 2007, our hospital has employed a prospective pharmacovigilance program based on the systematic detection of predefined abnormal laboratory signals (ALSs) through our laboratory information system (Pharmacovigilance Program from Laboratory Signals in Hospital [PPLSH]) for the early detection of SADRs. The screening for specific anomalous laboratory data enables us to monitor a large number of patients with limited resources, thereby accessing high-quality information in a timely manner. (Ramirez et al., 2010) We conducted a thorough evaluation of ALSs during the current pandemic to help detect those events associated with the treatments and the disease and provide a basis for decision making in drug risk management during a possible second wave of the pandemic.
The aim of the study was to report the suspected SADRs in COVID-19 patients vs. non-COVID-19 patients detected by the PPLSH from March to April 2020. We also compared the results with the suspected SADRs detected during the same period for the previous year.
Materials and Methods
Setting
La Paz University Hospital in Madrid, Spain, is a tertiary-care teaching facility, where all admissions to wards are monitored by the PPLSH. The program was conducted according to the Spanish Personal Data Protection Law, (Organic law 3/2018, december 5, 2018, protection of personal data and guarantee of digital rights (BOE núm. 294, 119788-11985) and approval for publishing the program was obtained from the Institutional Review Board at La Paz University Hospital (protocol PI-3226). The technical document of the Spanish Ministry of Health for the clinical management of COVID-19 in emergencies and in hospital was adapted and implemented in the hospital. (Spanish Ministry of Health; World Health Organization).
Information System and Coverage
A specific database application was developed within the integrated laboratory system (Labtrack Integrated Laboratory System), available in the hospital since 2003, which we employed to collect the predefined ALSs. We reviewed all ALSs retrieved systematically from these patients’ medical records.
At the time of the study, all of the patients’ medical information was collected in the hospital’s EMRs and included all laboratory data, imaging and other exploratory results, previous medical reports, medication prescription record, comments on the patients’ progression, and discharge summaries. Discharge summaries were coded according to International Statistical Classification of Diseases and Related Health Problems tenth revision (ICD-10).
Hospital laboratories that conduct blood tests for inpatients and emergency patients are certified and accredited under the appropriate International Standards Organization (ISO 9001:2000 and ISO 15189).
Definition of Signals
Table 1 lists the criteria for selecting the drug-induced ALS.
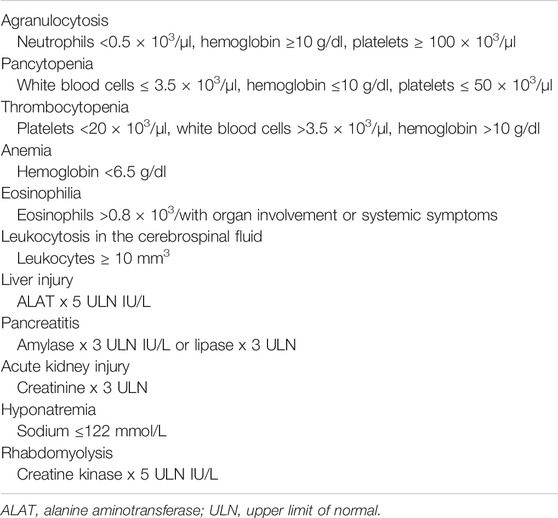
TABLE 1. Definition of automatic laboratory signals used to detect serious adverse drug reactions.
Definitions of Adverse Drug Reaction
We employed the E2D definition of SADR of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. (ICH Guideline on E2D Postapproval Safety Data Management: Definitions and Standards for Expedited Reporting) For the program’s purposes, we excluded ADRs caused by accidental or intentional overdose, as well as medical errors, which we considered to be any error in the written prescription, dispensation or administration. Errors in decision making (use in contraindicated clinical conditions or drug interactions) were considered SADRs and were therefore included. Adverse reactions caused by chemotherapy drugs were excluded from hematological ALSs, given that agranulocytosis, anemia, pancytopenia and thrombocytopenia are expected and explained by the pharmacodynamic properties of these drugs.
Detecting and Evaluating Adverse Drug Reactions
The procedure for detecting and evaluating ADRs has been described elsewhere. (Yelehe-Okouma et al., 2018) Briefly, in phase I, on-file laboratory data at admission or during hospitalization were screened 7 days a week, 24 h a day, for ALS from March to April 2019 and for the same period in 2020. In phase II, the patients were identified to avoid duplicates, and EMRs were reviewed. In phase III, a case-by-case evaluation was performed for the remaining cases (Figure 1). The causality assessment was performed using the algorithm of the Spanish Pharmacovigilance System. (Aguirre and García, 2016) We considered the categories of possible, probable or definite for drug-related reactions. Regarding the evaluation of the drug cause vs. the alternative cause (nondrug-induced), we only considered a drug cause when there was no alternative cause to explain the signal and, for the COVID-19 patients, when there was a dissociation between the clinical and lab parameters for improvement but a worsening of the ALS in the evaluation.
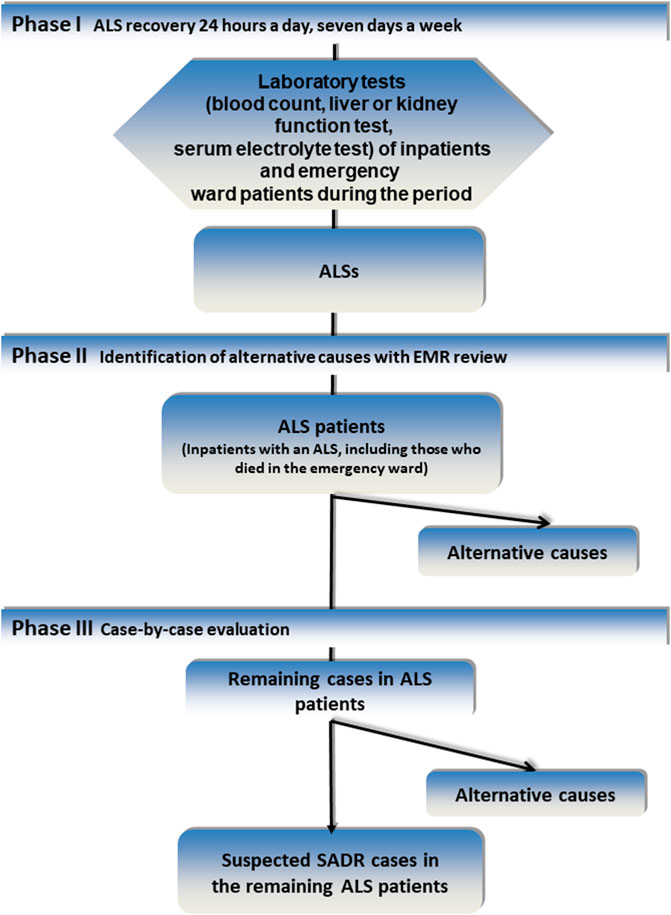
FIGURE 1. Methodology of the Pharmacovigilance Program From Laboratory Signals in Hospital. Abbreviations: ALS, automatic laboratory signal; EMR, electronic medical record; SADR, serious adverse reaction.
Monitoring COVID-19 Patients
During hospitalization, patients with COVID-19 infection were monitored by their physicians to assess hepatic and renal function (alanine aminotransferase), aspartate aminotransferase, alkaline phosphatase, creatinine, gamma-glutamyl transferase, glomerular filtration rate, bilirubin, prothrombin activity and thromboembolic risk (hemoglobin, Chronic Kidney Disease Epidemiology Collaboration equation, D-dimer, fibrinogen, platelets). The lab controls varied depending on the patients’ clinical situation, usually daily during the first three weeks. We evaluated the laboratory test results for each drug for treating COVID-19 using the following structure: The baseline value was the value before drug administration; value 1 was the first value after administration; values 2–19 were the values on days 1–20 after the first dose administration; and values 20–39 were the results between days 21 and 60 after dose administration during the hospitalization.
Collection of Patient Data and Reporting
For all patients initially categorized as having a suspected SADR, a complete report was submitted to the pharmacovigilance center in Madrid (https://www.notificaram.es).
Data Analysis
The results are presented using central tendency measures (mean for quantitative variables and median for ordinal ones) and measures of dispersion (standard deviation and interquartile range, respectively) and percentages (95% confidence interval) for discrete variables. The in-hospital incidence rate for each SADR and other etiologies of ALS were calculated by dividing the number of cases of drug-induced reactions in hospitalized or deceased patients in the emergency department by the number of patients hospitalized during the selected months. We assessed the uncertainty of association by calculating the 95% two-sided Poisson confidence interval. The chi-squared test was performed to compare sex distribution and morbidity variables, and Student’s t-test or the Mann Whitney test, as appropriate, was used to compare the ages of patients in the SADR cohorts. We employed IBM SPSS Statistics for Windows, Version 20.0 (IBM Corporation, Armonk, NY, US) for the statistical analysis.
Results
A total of 7,365 patients were hospitalized from March 1 to April 30, 2020, 2,682 (36.4%) of whom had COVID-19 infection. Figure 2 shows the sequence of drugs administered in the various phases of COVID-19 disease. The number of cases with ALS during the period was 1,341, with 575 COVID-19 patients and 766 non-COVID-19 patients. The COVID-19 patients had fewer hematological, pancreatitis and hyponatremia ALSs but more hepatitis, acute kidney injury, and rhabdomyolysis ALSs (Table 2). There were 1,153 cases with ALSs in the same period for 2019. The patients with COVID-19 in 2020 had an overall 3-fold higher rate of suspected SADRs than the non-COVID-19 patients in 2020 and 2019 (35.5% vs. 9.8% and 9.2%, respectively), with the following rates of SADRs: pancytopenia (57.1% vs. 1.4% and 4.5%), agranulocytosis (50% vs. 2.8% and 14.7%), thrombocytopenia (100% vs. 6.3% and 5.9%), anemia (43.8% vs. 3.2% and 27.6%), eosinophilia (14.1% vs. 5.7% and 4.1%), leukocytes in the cerebrospinal fluid (50% vs. 20.8% and 5.4%), hepatitis (45.1% vs. 23.7% and 12.4%), pancreatitis (58.3% vs. 15.6% and 7%), acute kidney injury (21.4% vs. 1.0% and 8.8%), rhabdomyolysis (15.3% vs. 4.4% and 9.5%) and hyponatremia (94.4% vs. 25.0% and 27.8%) (Table 2). The incidence rate of suspected SADRs detected by PPLSH in the COVID-19 patients was 760.63 (95% CI 707.89–816.01) per 10,000 patients, 4.75-fold higher than the SADR rate in the non-COVID-19 patients for the same period (160.15 per 10,000 patients, 95% CI 137.09–186.80) and 5.84-fold higher than the SADR rate for the same period in 2019 (130.19, 95% CI 109.53–154.36) (Table 3). The description of the demographic characteristics and morbidities of the patients who had SADRs during the study periods are shown in Table 4. Non-COVID-19 patients with SADRs were significantly older and there were significantly more females that COVID-19 patients, but the morbidities did not show significant differences between cohorts. Table 5 lists the drugs that most frequently produced SADRs in the COVID-19 patients, which includes: tocilizumab (59.84%), dexketoprofen (13.93%), azithromycin (8.43%), lopinavir-ritonavir (7.35%), dexamethasone (7.62%), and chloroquine/hydroxychloroquine (6.91%). The overall mortality rate for the COVID-19 vs. the non-COVID-19 patients (in 2020 and 2019) was 21.6% vs. 3.6% and 3.0%, respectively. The mortality rate for the COVID-19 patients with SADRs vs. the non-COVID-19 patients with SADRs (in 2020 and 2019) was 30.5% vs. 3.9% and 3.3%, respectively. Table 5 lists the mortality rate per drug for COVID-19 patients with SADRs.
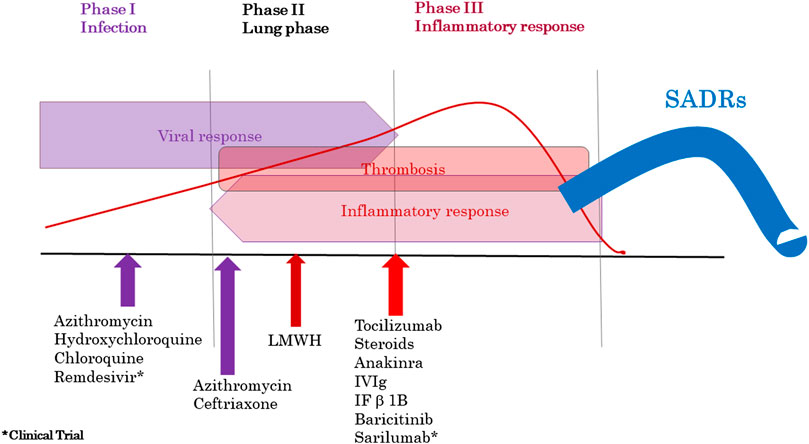
FIGURE 2. COVID-19 infection stages and treatments employed. Abbreviations: LMWH, low-molecular-weight heparin; Ig, immunoglobulin; IV Ig, intravenous immunoglobulin; IF β-1b, interferon beta-1b; SADRs, serious adverse drug reactions.
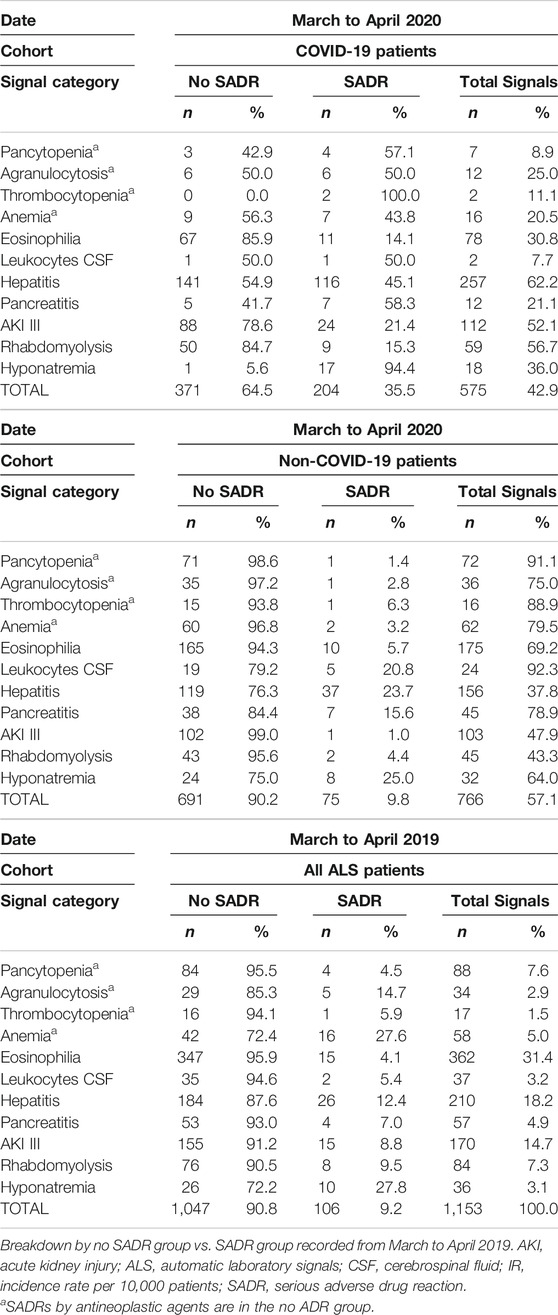
TABLE 2. Breakdown by no SADR group vs. SADR group recorded from March to April 2020 in COVID-19 patients vs. non-COVID-19 patients.
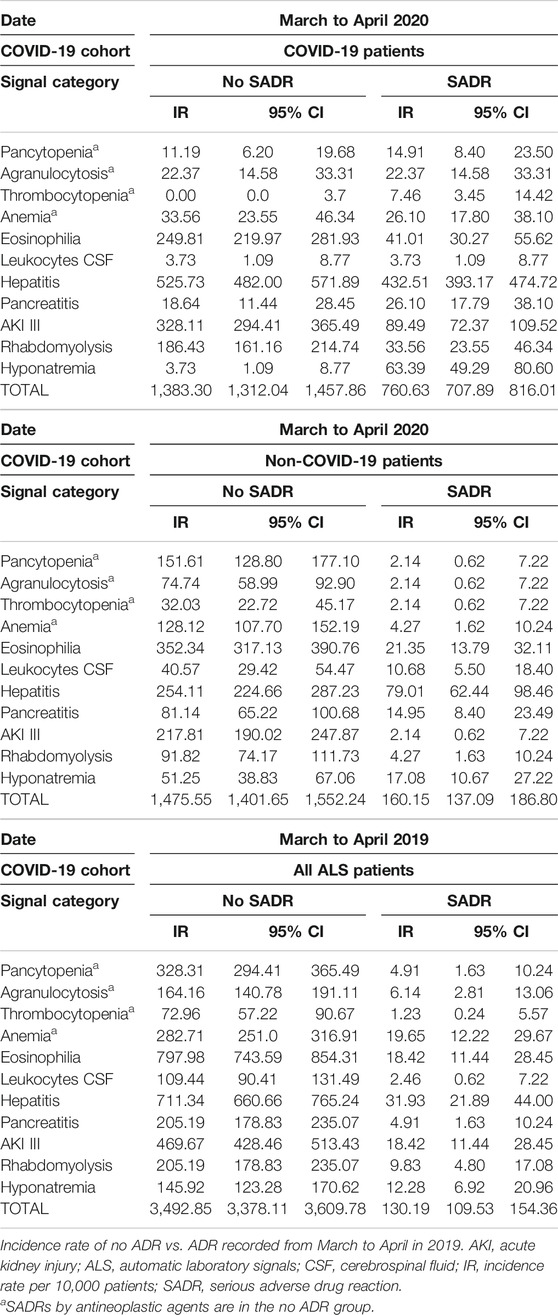
TABLE 3. Incidence rate (Poisson 95% CI) per 10,000 patients of no SADR vs. SADR recorded from March to April 2020 in COVID-19 patients vs. non-COVID-19 patients.
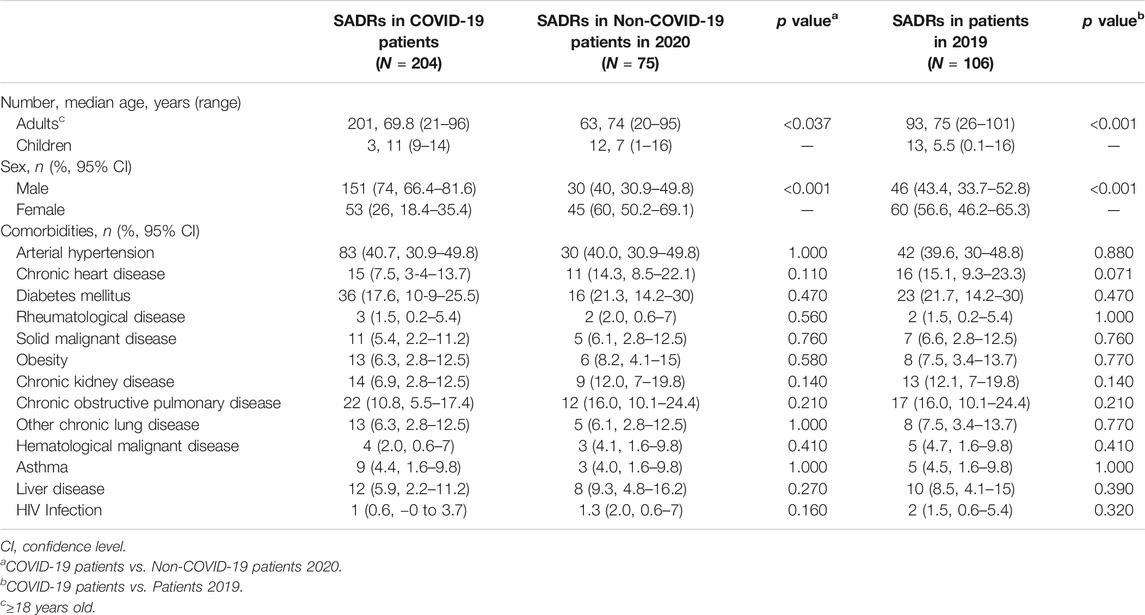
TABLE 4. Characteristics of the patients who had SADRs during the study periods.
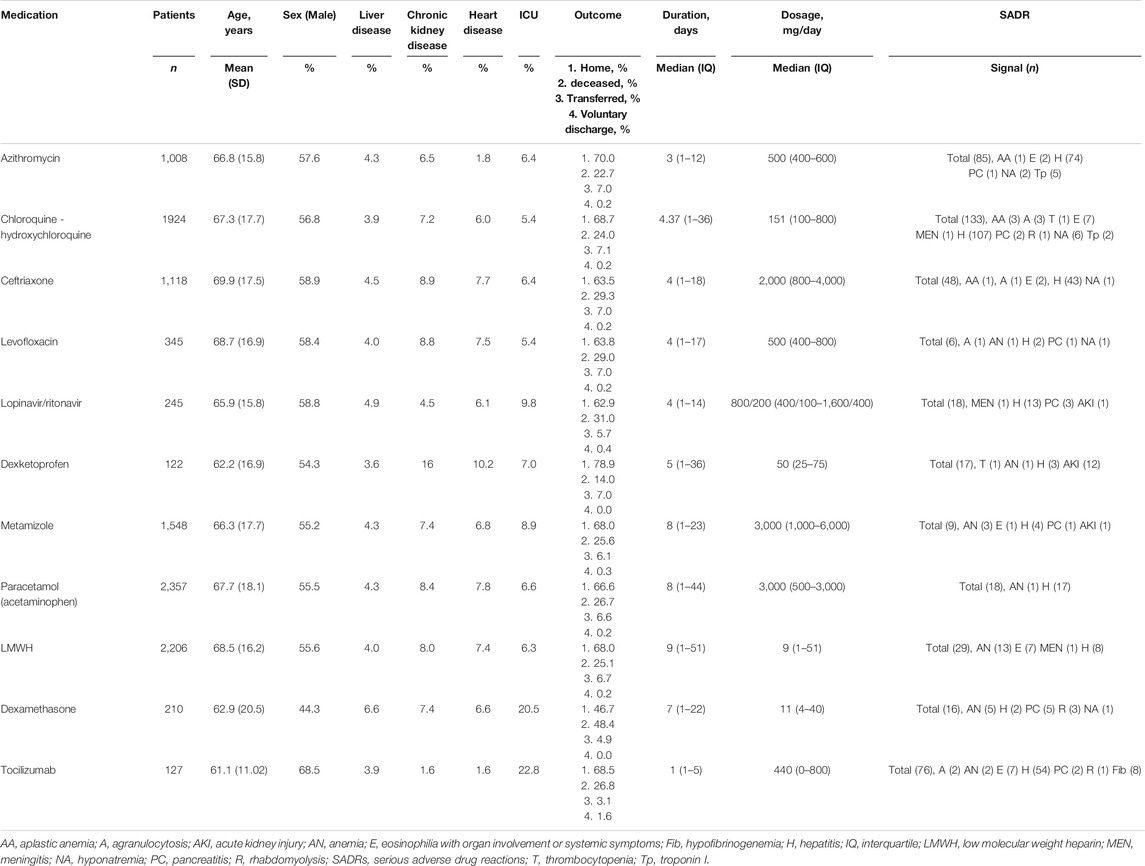
TABLE 5. Medications, prescriptions, comorbidities, outcome, serious adverse drug reactions.
At the time of hospitalization, the COVID-19 patients had slightly abnormal liver function, based on alanine aminotransferase and gamma-glutamyl transferase levels that were slightly above the upper limit of normality (ULN), which were normal in most patients. Figure 3 shows the statistically significant worsening of liver function in the COVID-19 patients associated with the drugs used in phase I of the infection. Liver function parameters in the patients who took ceftriaxone typically increased by the end of the first week, in patients who took azithromycin increased in the second week, and in the patients who took lopinavir-ritonavir or hydroxychloroquine increased in the third week. However, liver function trended towards normalization during hospitalization for the patients who took dexamethasone. Metamizole and paracetamol showed no statistically significant effect. At the time of hospitalization, the COVID-19 patients had an increased thromboembolic risk measured by the number of fold increases in D-dimer levels above the ULN. Figure 4 shows the worsening of D-dimer, fibrinogen, and hemoglobin levels in the patients treated with the various drugs during phase II of the infection. Tocilizumab and dexamethasone produced a statistically significant reduction in fibrinogen and hemoglobin levels, along with a significant increase in D-dimer levels. Oral anticoagulants, dexamethasone and low-molecular-weight heparins were associated with a decrease in hemoglobin levels after the start of the drug in this hospitalization phase.
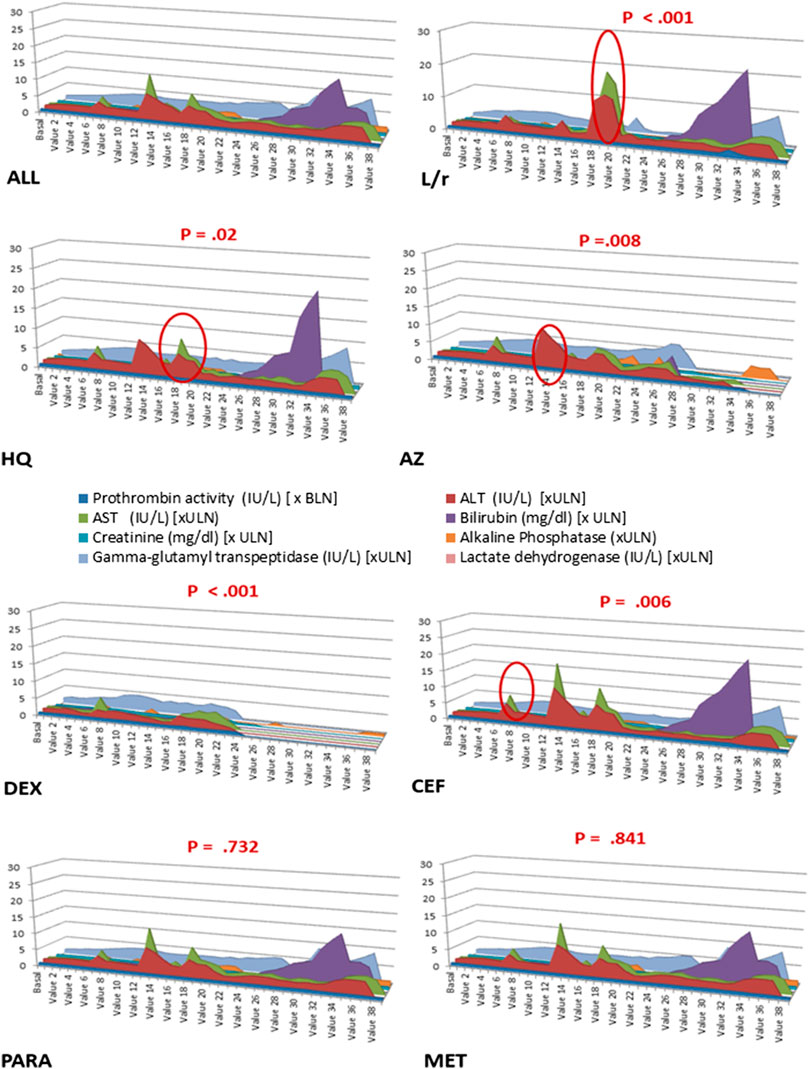
FIGURE 3. Sequence chart: Progression of parameters related to liver function in COVID-19 patients during hospitalization according to the treatment undergone. The X-axis indicates the value number (baseline, the last value before drug administration; value 1, first value after administration; values 2–19, values on days 1–20 after the first dose administration; values 20–39, results between days 21 and 60 of hospitalization). The Y-axis indicates the number of times above or below the limit of normality, as appropriate. The red circle indicates the points with statistical significance. ALL, all patients; AZ, azithromycin; BLN, below limit of normal; CEF, ceftriaxone; HQ, hydroxychloroquine; DEX, dexamethasone, L/r, lopinavir/ritonavir; MET, metamizole; PARA, paracetamol; ULN, upper limit of normality.
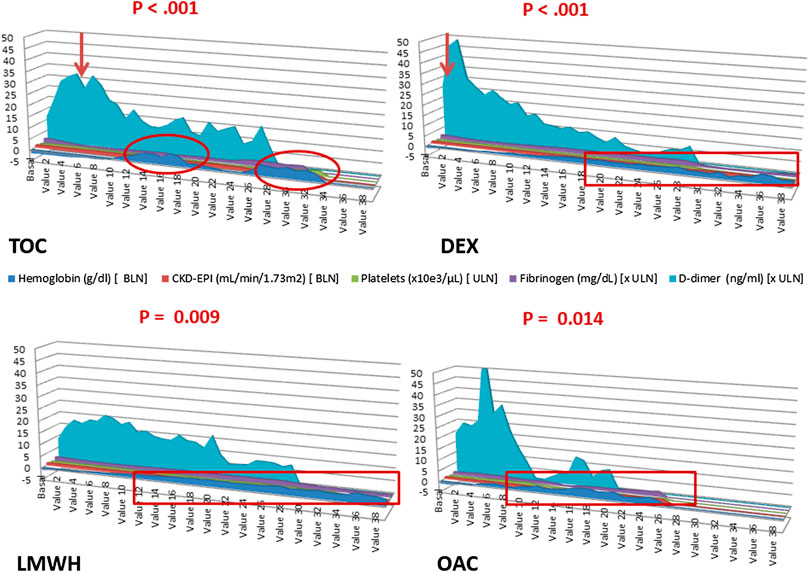
FIGURE 4. Sequence chart: Progression of parameters related to coagulation status in COVID-19 patients during hospitalization according to the treatment undergone. The X-axis indicates the value number (baseline, the last value before drug administration; value 1, first value after administration; values 2–19, values on days 1–20 after the first dose administration; values 20–39, results between days 21–60 of hospitalization). The Y-axis indicates the number of times above or below the limit of normality, as appropriate. The arrows indicate the change in the trend of normality. The red circles indicate the points with statistical significance. BLN, below limit of normal; DEX, dexamethasone; LMWH, low-molecular-weight heparins; OAC, oral anticoagulants; TOC, tocilizumab; ULN, upper limit of normal.
Discussion
Since 2007, physicians of the Clinical Pharmacology Department of our hospital maintain uninterruptedly a pharmacovigilance program based on laboratory signals using its available information systems. ALSs were chosen on the basis that they were detectable in the routine tests of almost all laboratories and were therefore easily detectable in inpatients and because the ALSs could warn of relevant SADRs with significant impact on patient health and wellbeing. Agranulocytosis, aplastic anemia, eosinophilia, liver injury, and rhabdomyolysis are frequently evaluated ALSs in the literature. (Risks of agranulocytosis and aplastic anemia. A first report of their relation to drug use with special reference to analgesics. The International Agranulocytosis and Aplastic Anemia Study, 1986; Ramírez et al., 2017; Andrade et al., 2005; Wen et al., 2019) Thrombocytopenia, anemia, leukocytes in cerebrospinal fluid, pancreatitis, acute kidney injury, and hyponatremia are increasingly frequent drug-induced reactions. (Aster and Bougie, 2007; Carnovale et al., 2015; Yelehe-Okouma et al., 2018; Wu and Huang, 2018; Ramírez et al., 2019; Zheng et al., 2019) This study enabled us to detect a relevant number of ALSs that are potentially related to SADRs and to determine their in-hospital incidence. During March-April 2020, there was a significant 72% reduction in the number of spontaneous SADRs (not from the PPLSH) compared with the same period in 2019, although 4 drug reactions with eosinophilia and systemic symptoms, 2 cases of Stevens Johnson syndrome, and 1 case of acute generalized exanthematous pustulosis were included. In addition, we considered a spontaneous SADR as a sentinel event that motivated a root cause analysis from the hospital, which included, as an improvement action, a drug safety note for the Spanish Agency for Medicine and Health Products.
Overall, we detected a 5.8-fold higher rate of SADRs in the COVID-19 patients than during the same period of the previous year. The use of off-label medicines has been associated with more ADRs than the use of labeled medicines. (Bellis et al., 2014; Viola et al., 2016; Auffret et al., 2017), This off-label use would be acceptable if the evidence of potential benefits outweighs the ADR risk. More than 150 clinical trials are currently underway to study drugs that prevent or treat COVID-19 infection, some of which have shown no benefit, such as lopinavir-ritonavir, azithromycin, chloroquine and hydroxychloroquine. (Cao et al., 2020; Rosenberg et al., 2020; Tang et al., 2020a) During the COVID-19 pandemic period, we detected more SADRs in the non-COVID-19 patients than during the same period in 2019, an effect that can be explained by the overloading of the health system, which resulted in a patient safety problem: changes in prescription due to supply problems, insufficient deprescribing, more empiric treatments, and drug interactions in non-COVID-19 patients.
The PPLSH detected that 35.5% of the ALSs in the COVID-19 patients were SADRs, which agrees with the results from the China Hospital Pharmacovigilance System that detected ADRs in 37.8% of COVID-19 patients, which were predominately drug-induced gastrointestinal disorders and liver disorders (23.0% vs. 13.8% respectively). (Sun et al., 2020) Drug-induced liver injury was the most frequent SADR detected (116/204, 56.86%) in the study. Liver damage in mild cases of COVID-19 is often transient, and liver function can return to normal without special treatment. (Alqahtani and Schattenberg, 2020) Moderate and severe liver damage could be drug-induced, which might explain the large variation in liver impairment observed across the various cohorts. (Aggarwal et al., 2020; Borobia et al., 2020; Chen et al., 2020; Guan et al., 2020; Zhou et al., 2020) Immune-mediated inflammation, such as cytokine storms and pneumonia-associated hypoxia, might also have contributed to liver injury and even to the development of liver failure in critically ill patients with COVID-19. Figure 2 shows the increase in bilirubin and transaminase levels in the patients hospitalized for more than 4 weeks, corresponding to the critically ill patients.
Increased D-dimer levels have been reported as one of the most common laboratory findings in COVID-19 patients requiring hospitalization. (Tang et al., 2020b) D-dimer levels on admission 4-fold higher than the ULN have been associated with in-hospital mortality for patients with COVID-19. (Zhang et al., 2020) Despite the difficulties in standardizing D-dimer levels, test kit manufacturers, normal values and units, D-dimer is a marker of thromboembolic disease and disseminated intravascular coagulation. (Favaloro and Thachil, 2020) Drugs for treating phase II of infection-associated hyperinflammatory syndrome that can cause life-threatening acute respiratory distress syndrome in patients with COVID-19 pneumonia can also cause thromboembolic disease. These drugs include dexamethasone, baricitinib, sarilumab, interferon beta 1B, and intravenous immunoglobulins. (Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products) Thrombocytopenia has been associated with anakinra, and hypofibrinogenemia has been related to tocilizumab. (Spanish Agency for Medicines and Health Products; Spanish Agency for Medicines and Health Products) Our study therefore reports a statistically significant effect of hypofibrinogenemia with an increase in D-dimer levels associated with tocilizumab and to a lesser extent with dexamethasone. Anemization was also observed in the patients treated with low-molecular-weight heparins or oral anticoagulants during this phase of COVID-19.
This study’s main limitation is that the evaluation of causality of a possible SADR does not completely exclude the influence of COVID-19. Considering the current evidence, some overlap with COVID-19 cannot be ruled out. However, a drug-related cause was only considered when there was a dissociation between clinical improvement and worsening of the ALS. Longer follow-up periods are needed to assess the recovery or sequelae of these SADRs and to study the immunological and pharmacogenetic mechanisms and the re-exposure effects of these SADRs.
In conclusion, PPLSH has been useful in detecting and evaluating specific SADRs during the avalanche of hospitalizations of patients with COVID-19. The incidence rate of SADRs detected by PPSLH in the patients with COVID-19 was 4.75-fold higher than that of the non-COVID-19 patients. Caution is recommended in using drugs to treat patients with COVID-19, because the drugs cause additional damage, especially those that are hepatotoxic, myotoxic, or induce thromboembolic events.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Institutional Review Board at La Paz University Hospital (protocol PI-3226). Written informed consent for participation was not provided by the participants’ legal guardians/next of kin because: The requirement for informed consent was waived because the data collection was retrospective. All suspected ADRs were notified to the Spanish Pharmacovigilance System.
Author Contributions
Participated in research design: ER and AMB. Data curation: MU, AR, YV, and ES. Participated in data analysis: JM, AM-V, and MG-M. Participated in the writing of the paper: ER, MU, and AMB. Writing – review and editing: MG-M, JF, and AC.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors are grateful to all hospital staff for their dedication to patient safety, even when the system was overwhelmed by the COVID-19 pandemic.
References
Aggarwal, S., Garcia-Telles, N., Aggarwal, G., Lavie, C., Lippi, G., and Henry, B. M. (2020). Clinical features, laboratory characteristics, and outcomes of patients hospitalized with coronavirus disease 2019 (COVID-19): early report from the United States. Diagnosis (Berl) 7 (2), 91–96. doi:10.1515/dx-2020-0046.
Aguirre, C., and García, M. (2016). Evaluación de la causalidad en las comunicaciones de reacciones adversas a medicamentos. Algoritmo del Sistema Español de Farmacovigilancia. Med. Clínica 147 (10), 461–464. doi:10.1016/j.medcli.2016.06.012.
Alqahtani, S. A., and Schattenberg, J. M. (2020). Liver injury in COVID-19: the current evidence. United European Gastroenterol. J. 8 (5), 509–519. doi:10.1177/2050640620924157.
Andrade, R. J., Lucena, M. I., Fernández, M. C., Pelaez, G., Pachkoria, K., García-Ruiz, E., et al. (2005). Drug-induced liver injury: an analysis of 461 incidences submitted to the Spanish registry over a 10-year period. Gastroenterology 129 (2), 512–521. doi:10.1053/j.gastro.2005.05.006.
Aster, R. H., and Bougie, D. W. Drug-induced Immune thrombocytopenia. N. Engl. J. Med. 357 (6), 580–587. doi:10.1056/nejmra066469.
Auffret, M., Labreuche, J., Duhamel, A., Deheul, S., Cottencin, O., Bordet, R., et al. (2017). Proactive regional pharmacovigilance system versus national spontaneous reporting for collecting safety data on concerning off-label prescribing practices: an example with baclofen and alcohol dependence in France. Drug Saf. 40 (3), 257–262. doi:10.1007/s40264-016-0489-7.
Bellis, J. R., Kirkham, J. J., Nunn, A. J., and Pirmohamed, M. (2014). Adverse drug reactions and off-label and unlicensed medicines in children: a prospective cohort study of unplanned admissions to a paediatric hospital. Br. J. Clin. Pharmacol. 77 (3), 545–553. doi:10.1111/bcp.12222.
Borobia, A., Carcas, A., Arnalich, F., Álvarez-Sala, R., Monserrat-Villatoro, J., Quintana, M., et al. (2020). A cohort of patients with COVID-19 in a major teaching hospital in Europe. J. Clin. Med. 9 (6), 1733. doi:10.3390/jcm9061733.
Cao, B., Wang, Y., Wen, D., Liu, W., Wang, J., Fan, G., et al. (2020). A trial of lopinavir-ritonavir in adults hospitalized with severe covid-19. N. Engl. J. Med. 382 (19), 1787–1799. doi:10.1056/NEJMoa2001282.
Carnovale, C., Brusadelli, T., Casini, M. L., Renda, F., Ruggieri, S., Pimpinella, G., et al. (2015). Drug-induced anaemia: a decade review of reporting to the Italian Pharmacovigilance data-base. Int. J. Clin. Pharm. 37 (1), 23–26. doi:10.1007/s11096-014-0054-3.
Center for Coordination of Health Alerts and Emergencies, . “Coronavirus disease (COVID-19). Spain: ministery of health.” Available at:https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/situacionActual.html (Accessed July 1, 2020).
Chen, N., Zhou, M., Dong, X., Qu, J., Gong, F., Han, Y., et al. (2020). Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 395 (10223), 507–513. doi:10.1016/S0140-6736(20)30211-7.
COVID-19: Current situation in the Community of Madrid. Situation Report. Available at: https://www.comunidad.madrid/servicios/salud/2019-nuevo-coronavirus#situacion-epidemiologica-actual (Accessed July 1, 2020).
Favaloro, E. J., and Thachil, J. (2020). Reporting of D-dimer data in COVID-19: some confusion and potential for misinformation. Clin. Chem. Lab. Med. 58 (8), 1191–1199. doi:10.1515/cclm-2020-0573.
Guan, W.-j., Ni, Z.-y., Hu, Y., Liang, W.-h., Ou, C.-q., He, J.-x., et al. (2020). Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 382 (18), 1708–1720. doi:10.1056/NEJMoa2002032.
Hannan, T. (1999). Detecting adverse drug reactions to improve patient outcomes. Int. J. Med. Inf. 55 (1), 61. doi:10.1016/s1386-5056(99)00020-9.
ICH guideline on E2D postapproval safety data management: definitions and standards for expedited reporting. London, UK: 2004. Available at: https://www.ema.europa.eu/en/documents/scientific-guideline/international-conference-harmonisation-technical-requirements-registration-pharmaceuticals-human-use_en-12.pdf (Accessed July 1, 2020).
Organic law 3/2018, december 5, 2018, protection of personal data and guarantee of digital rights (BOE núm. 294, 2017, 119788–11985). Available at: https://apdcat.gencat.cat/web/.content/01-autoritat/normativa/documentos/Llei-organica-pd-2018.pdf (Accessed July 1, 2020).
Ramirez, E., Carcas, A. J., Borobia, A. M., Lei, S. H., Piñana, E., Fudio, S., et al. (2010). A pharmacovigilance program from laboratory signals for the detection and reporting of serious adverse drug reactions in hospitalized patients. Clin. Pharmacol. Ther. 87 (1), 74. doi:10.1038/clpt.2009.185.
Ramírez, E., Medrano-Casique, N., Tong, H. Y., Bellón, T., Cabañas, R., Fiandor, A., et al. (2017). Eosinophilic drug reactions detected by a prospective pharmacovigilance programme in a tertiary hospital. Br. J. Clin. Pharmacol. 83 (2), 400–415. doi:10.1111/bcp.13096.
Ramírez, E., Rodríguez, A., Queiruga, J., García, I., Díaz, L., Martínez, L., et al. (2019). Severe hyponatremia is often drug induced: 10‐year results of a prospective pharmacovigilance program. Clin. Pharmacol. Ther. 106 (6), 1362–1379. doi:10.1002/cpt.1562.
(1986). Risks of agranulocytosis and aplastic anemia. A first report of their relation to drug use with special reference to analgesics. The International Agranulocytosis and Aplastic Anemia Study. J. Am. Med. Assoc. 256 (1), 1749–1757.
Rosenberg, E. S., Dufort, E. M., Udo, T., Wilberschied, L. A., Kumar, J., Tesoriero, J., et al. (2020). Association of treatment with hydroxychloroquine or azithromycin with in-hospital mortality in patients with COVID-19 in New York state. J. Am. Med. Assoc. 323 (24), 2493–2502. doi:10.1001/jama.2020.8630.
Spanish Agency for Medicines and Health Products. Available at:https://cima.aemps.es/cima/dochtml/ft/65600/FT_65600.html (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Resochin®. Available at:https://cima.aemps.es/cima/dochtml/ft/15797/FT_15797.html (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Dolquine®. Available at:https://cima.aemps.es/cima/dochtml/ft/74904/FT_74904.html (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Ceftriaxone Normon®. Available at: https://cima.aemps.es/cima/dochtml/ft/62641/FT_62641.html (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Kaletra®. Available at: https://cima.aemps.es/cima/dochtml/ft/01172006/FT_01172006.html (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Dexametasona Kern Pharma®. Available at: https://cima.aemps.es/cima/dochtml/ft/67455/FT_67455.html (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Dexametason Kern Pharma®. Available at: https://cima.aemps.es/cima/dochtml/ft/67455/FT_67455.html (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Olumiant®. Available at: https://cima.aemps.es/cima/pdfs/ft/1161170002/FT_1161170002.pdf (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Betaferon®. Available at: https://cima.aemps.es/cima/pdfs/ft/95003005/FT_95003005.pdf (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Privigen®. Available at: https://cima.aemps.es/cima/pdfs/ft/08446001/FT_08446001.pdf (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Kineret®. Available at: https://cima.aemps.es/cima/dochtml/ft/102203006/FT_102203006.html (Accessed July 1, 2020).
Spanish Agency for Medicines and Health Products. Technical data sheet Roactemra®. Available at: https://cima.aemps.es/cima/dochtml/ft/108492007/FT_108492007.html (Accessed July 1, 2020).
Sun, J., Deng, X., Chen, X., Huang, J., Huang, S., Li, Y., et al. (2020). Incidence of adverse drug reactions in COVID‐19 patients in China: an active monitoring study by hospital pharmacovigilance system. Clin. Pharmacol. Ther. 108, 791. doi:10.1002/cpt.1866.
Tang, N., Li, D., Wang, X., and Sun, Z. (2020a). Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemostasis. 18, 844–847. doi:10.1111/jth.14768.
Tang, W., Cao, Z., Han, M., Wang, Z., Chen, J., Sun, W., et al. (2020b). Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: open label, randomised controlled trial. BMJ. 369, m1849. doi:10.1136/bmj.m1849.
Spanish Ministry of Health. Technical Document. Clinical management of COVID-19: hospital care. Available at: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/Protocolo_manejo_clinico_ah_COVID-19.pdf (Accessed July 1, 2020).
World Health Organization. Technical Document. Emergency management of COVID-19. Available at: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov-China/documentos/Manejo_urgencias_pacientes_con_COVID-19.pdf (Accessed July 1, 2020).
Viola, E., Trifirò, G., Ingrasciotta, Y., Sottosanti, L., Tari, M., Giorgianni, F., et al. (2016). Adverse drug reactions associated with off-label use of ketorolac, with particular focus on elderly patients. An analysis of the Italian pharmacovigilance database and a population based study. Expet Opin. Drug Saf. 15 (Suppl. 2), 61–67. doi:10.1080/14740338.2016.1221401.
Wen, Z., Liang, Y., Hao, Y., Delavan, B., Huang, R., Mikailov, M., et al. (2019). Drug-Induced Rhabdomyolysis Atlas (DIRA) for idiosyncratic adverse drug reaction management. Drug Discov. Today. 24 (1), 9–15. doi:10.1016/j.drudis.2018.06.006.
Wu, H., and Huang, J. (2018). Drug-induced nephrotoxicity: pathogenic mechanisms, biomarkers and prevention strategies. Cdm. 19 (7), 559–567. doi:10.2174/1389200218666171108154419.
Yelehe-Okouma, M., Czmil-Garon, J., Pape, E., Petitpain, N., and Gillet, P. (2018). Drug-induced aseptic meningitis: a mini-review. Fundam. Clin. Pharmacol. 32 (3), 252–260. doi:10.1111/fcp.12349.
Zhang, L., Yan, X., Fan, Q., Liu, H., Liu, X., Liu, Z., et al. (2020). D‐dimer levels on admission to predict in‐hospital mortality in patients with Covid‐19. J. Thromb. Haemostasis. 18 (6), 1324–1329. doi:10.1111/jth.14859.
Zheng, J., Yang, Q.-J., Dang, F.-T., and Yang, J. (2019). Drug-induced pancreatitis: an update. Arab J. Gastroenterol. 20 (4), 183–188. doi:10.1016/j.ajg.2019.11.005.
Keywords: adverse drug reaction, corona virus disease-19 (COVID-19), serious adverse drug reaction, pharmacovigilance process, adverse (side) effects
Citation: Ramírez E, Urroz M, Rodríguez A, González-Muñoz M, Martín-Vega A, Villán Y, Seco E, Monserrat J, Frías J, Carcas AJ and Borobia AM (2020) Incidence of Suspected Serious Adverse Drug Reactions in Corona Virus Disease-19 Patients Detected by a Pharmacovigilance Program by Laboratory Signals in a Tertiary Hospital in Spain: Cautionary Data. Front. Pharmacol. 11:602841. doi: 10.3389/fphar.2020.602841
Received: 04 September 2020; Accepted: 09 November 2020;
Published: 03 December 2020.
Edited by:
Maria Dimitrova, Medical University-Sofia, BulgariaReviewed by:
Anthony Kar Hsing Chan, Pfizer, IrelandElena Bresciani, University of Milano-Bicocca, Italy
Copyright © 2020 Ramírez, Urroz, Rodríguez, González‐Muñoz, MartínVega, Villán, Seco, Monserrat, Frías, Carcas and Borobia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elena Ramírez, ZWxlbmEucmFtaXJlemdAdWFtLmVz; Alberto M. Borobia, YWxiZXJ0by5ib3JvYmlhQHNhbHVkLm1hZHJpZC5vcmc=