 Li-Min Sun
Li-Min Sun Cheng-Li Lin
Cheng-Li Lin Sean Sun4
Sean Sun4 Chia-Hung Kao
Chia-Hung Kao- 1Department of Radiation Oncology, Zuoying Branch of Kaohsiung Armed Forces General Hospital, Kaohsiung, Taiwan
- 2Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan
- 3College of Medicine, China Medical University, Taichung, Taiwan
- 4Department of Cardiovascular Science, Midwestern University, Glendale, AZ, United States
- 5Graduate Institute of Biomedical Sciences and School of Medicine, College of Medicine, China Medical University, Taichung, Taiwan
- 6Department of Computer Science and Information Engineering, Asia University, Taichung, Taiwan
- 7Department of Nuclear Medicine, China Medical University Hospital, Taichung, Taiwan
- 8Department of Bioinformatics and Medical Engineering, Asia University, Taichung, Taiwan
Background: Earlier studies have indicated a relatively higher risk of occurring meningioma among female breast cancer survivors and have suggested that tamoxifen might decrease this risk. The present study evaluated whether tamoxifen use in breast cancer patients can reduce the risk of meningioma.
Methods: We designed a population-based cohort study by using data from the National Health Insurance system of Taiwan to assess this issue. Between January 1, 2000, and December 31, 2008, women with breast cancer and of age ≥20 years were included. They were divided into two groups: those who had not received tamoxifen therapy and those who had. The Cox’s proportion hazard regression analysis was conducted to estimate the effects of tamoxifen treatment and the subsequent meningioma risk.
Results: We identified a total of 50,442 tamoxifen users and 30,929 non-tamoxifen users. Tamoxifen users had a borderline significantly lower overall risk of meningioma than non-tamoxifen users [adjusted hazard ratio (aHR) = 0.64, 95% confidence interval (95% CI) = 0.40–1.02]. A statistically significant difference was found in those patients with tamoxifen treatment duration longer than 1,500 days (aHR = 0.42, 95% CI = 0.19–0.91) or with cumulative dosage exceeding 26,320 mg (aHR = 0.44, 95% CI = 0.22–0.88). Furthermore, no statistically significant joint effect of aromatase inhibitors and tamoxifen on the occurrence of meningioma among breast cancer patients was seen.
Conclusion: Tamoxifen users had a non-significantly (36%) lower risk of developing meningioma than did tamoxifen non-users; however, our data indicated that tamoxifen therapy is associated with a reduced meningioma risk for Taiwanese breast cancer patients receiving long duration or high cumulative dosage treatment with tamoxifen.
Introduction
Among women in low-, middle-, and high-income countries, breast cancer is the most frequently occurring cancer, with an estimated 2.09 million new cases diagnosed worldwide in 2018 International Agency for Research on Cancer (IARC) and World Health Organization (WHO). Similarly, in Taiwan, breast cancer has been the most prevalent cancer among women for two decades, during which the age-adjusted incidence rate has risen gradually from 55.88 per 100,000 people in 2002 to 89.21 per 100,000 people in 2012 (Chiang et al., 2016). In the near future, increasing numbers of long-term survivors of breast cancer can be expected because of factors such as effective cancer screening, improved diagnostic tools that enable early detection, improved adjuvant treatments, relatively favorable prognoses with slower progression than most other cancers, and the aging population. As a result, surveillance and follow-up care of such survivors have become pertinent topics, both for the control of the cancer and its treatment-related health conditions (Howard-Anderson et al., 2012).
Meningioma originates in the meningothelial cells of the arachnoid membrane and is the most prevalent primary intracranial neoplasm in adults. Between 2008 and 2012, in the United States, meningioma accounted for 36.4% of all primary tumors occurring in the brain and other organs of the central nervous system (Ostrom et al., 2015). The rate of meningioma incidence in women is nearly two times that in men, especially during the reproductive period of life (Claus et al., 2008; Wiemels et al., 2010; Ostrom et al., 2015). Breast cancer in women has been associated with meningioma (Helseth et al., 1989; Lieu et al., 2003; Rao et al., 2009; Milano and Grossman, 2017). Approximately 66% of all breast cancers (and even higher in older women) are hormone receptor–positive (Rakha et al., 2007; Morrison et al., 2012). Thus, for most patients, hormone therapy should be considered as an adjuvant to surgery. Evidence suggests that tamoxifen—among the most extensively administered selective estrogen receptor modulators in hormone receptor–positive breast cancer patients—increases disease-free and overall survival rates (Lin and Winer, 2008). Even though tamoxifen is generally well tolerated, with a fair adherence rate (Wigertz et al., 2012), the safety of tamoxifen treatment is of clinical concern (Perez, 2007). The occurrence of meningioma and tamoxifen use might plausibly be connected; hormonal factors have been proven to be involved in the development of meningioma (Hsu et al., 1997; Wahab and Al-Azzawi, 2003; Lee et al., 2006; Korhonen et al., 2010; Cea-Soriano et al., 2012), and approximately 70% of meningiomas show progesterone receptor expression whereas approximately 30% show estrogen receptor expression (Wahab and Al-Azzawi, 2003). An early study suggested that tamoxifen treatment may prevent the development of meningioma in breast cancer patients (Ji et al., 2016).
In the present retrospective cohort study, we used a population-based database derived from Taiwan’s National Health Insurance (NHI) system to investigate whether tamoxifen treatment can effectively protect breast cancer survivors against meningioma development and whether the duration or cumulative dosage of tamoxifen treatment affects this possible relationship.
Methods
Data Source
Taiwan provides medical insurance coverage to 99% of its 23.74 million residents; data regarding medical insurance recipients are stored in the NHI Research Database (NHIRD) (Database NHIR). The Registry for Catastrophic Illness Patient Database (RCIPD), a subset of the NHIRD, was used for this retrospective cohort study. In Taiwan, when patients apply for qualified catastrophic illness certificates, their illnesses must be confirmed by clinical physicians. The RCIPD has been discussed in detail in the literature (Peng et al., 2015; Huang et al., 2016). The diagnoses in the NHIRD are coded on the basis of the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
Study Population
In the data for the period from January 1, 2000, to December 31, 2008, we identified women with breast cancer and of age ≥20 years (ICD-9-CM 174). The identified patients were divided into two groups: those who had not received tamoxifen therapy (i.e., the non-tamoxifen cohort or controls) and those who had (i.e., the tamoxifen cohort). The index date in the tamoxifen cohort was set as the day of first tamoxifen treatment. For each patient in the non-tamoxifen cohort, the index date was a randomly selected date with the same index year as that in the tamoxifen cohort. Patients younger than 20 years and those with a history of meningioma (ICD-9-CM 225.2) or other cancers (namely, ICD-9-CM 140-173 and 175-208) prior to the index date were excluded.
Outcome and Comorbidities and Medication
From the index date onward, both cohorts were followed until withdrawal from the NHI program, meningioma occurrence, or December 31, 2011. Patients whose claims records revealed a diagnosis of alcohol-related illness (ICD-9-CM 291, 303, 305, 571.0, 571.1, 571.2, 571.3, 790.3, A215, and V11.3), chronic obstructive pulmonary disease (COPD) (ICD-9-CM: 491, 492, and 496), coronary artery disease (CAD) (ICD-9-CM 410–414), diabetes (ICD-9-CM 250), hypertension (ICD-9-CM 401–405), or stroke (ICD-9-CM 430–438) at the baseline were defined as having comorbidities. The medications included steroids, statins, and thiazide diuretics. In addition, treatment information for breast cancer patients who received surgical operations, aromatase inhibitors, chemotherapy, and radiotherapy was considered in our study.
Statistical Analysis
The distributions of age, comorbidities, drug, and breast cancer treatment were calculated as frequency (relative frequency, %) or mean ± standard deviation. The differences in the data of the two cohorts were analyzed through Student t testing for continuous variables and chi-square testing for categorical variables. We used the Kaplan–Meier method to assess the cumulative incidence of meningioma in the tamoxifen and non-tamoxifen cohorts and estimated the differences between the cohorts through log-rank testing. In addition, the incidence density of meningioma per 10,000 person-years was computed for each cohort. Univariable and multivariable Cox proportional hazards models were employed to calculate the hazard ratios (HRs) and 95% confidence intervals (CIs) of meningioma in the tamoxifen cohort relative to the non-tamoxifen cohort. Given that during the study period, the patients may have taken tamoxifen irregularly, the calculations here may have underestimated the drug effect. To diminish this bias in estimating the meningioma risk, we employed Cox proportional hazard model with time-dependent exposure covariates. We evaluated the effects of tamoxifen use duration (≤365, 366–1,500, and >1,500 days) and cumulative dosage (≤4,280, 4,281–12,980, 12,981–26,320, and >26,320 mg) on the risk of meningioma in patients with breast cancer. Furthermore, we assessed the joint effects of aromatase inhibitor use and tamoxifen use. All data were analyzed using the SAS statistical package (v9.4; SAS Institute Inc., Cary, NC, USA). Any difference with two-tailed P < 0.05 was considered statistically significant.
Results
Table 1 presents a comparison of the baseline characteristics of the two cohorts. On average, patients in the tamoxifen cohort were younger than those in the non-tamoxifen cohort. The non-tamoxifen cohort had higher proportions of patients with CAD, stroke, hypertension, diabetes, statin use, and thiazide diuretics use. The tamoxifen cohort exhibited higher proportions of breast surgery, radiotherapy, aromatase inhibitor alone, and combined aromatase inhibitor and chemotherapy treatment; however, the non-tamoxifen cohort had a higher proportion of chemotherapy alone.
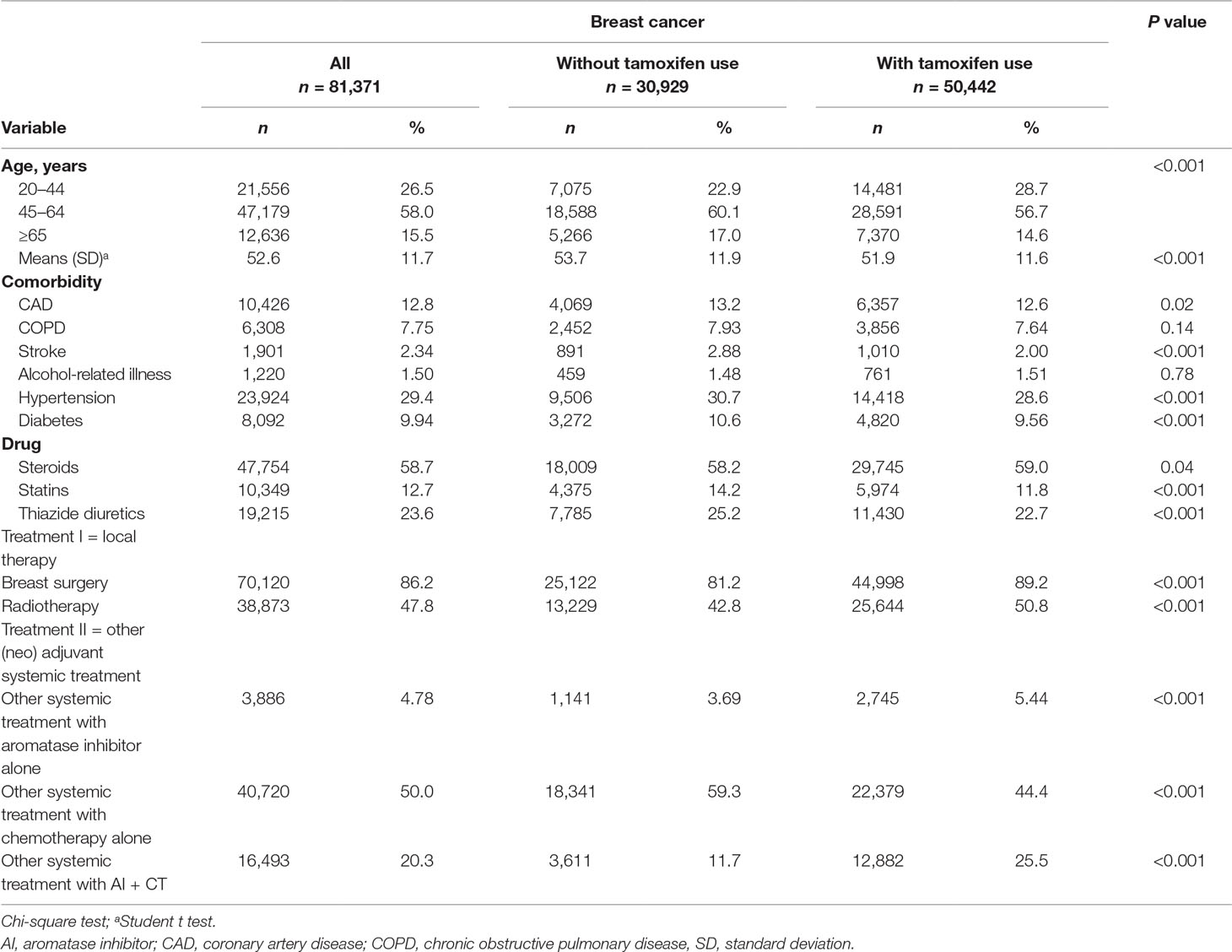
Table 1 Demographic and comorbidity data of breast cancer patients classified by tamoxifen use status.
The mean follow-up periods were 4.71 (SD = 3.30) and 3.77 (SD = 3.17) years in the tamoxifen cohort and non-tamoxifen cohort, respectively (data not shown). At the end of the 12-year follow-up period, per the Kaplan–Meier analysis, the cumulative incidence of meningioma was significantly lower in the tamoxifen cohort than in the non-tamoxifen cohort (log-rank test: P = 0.02) (Figure 1).
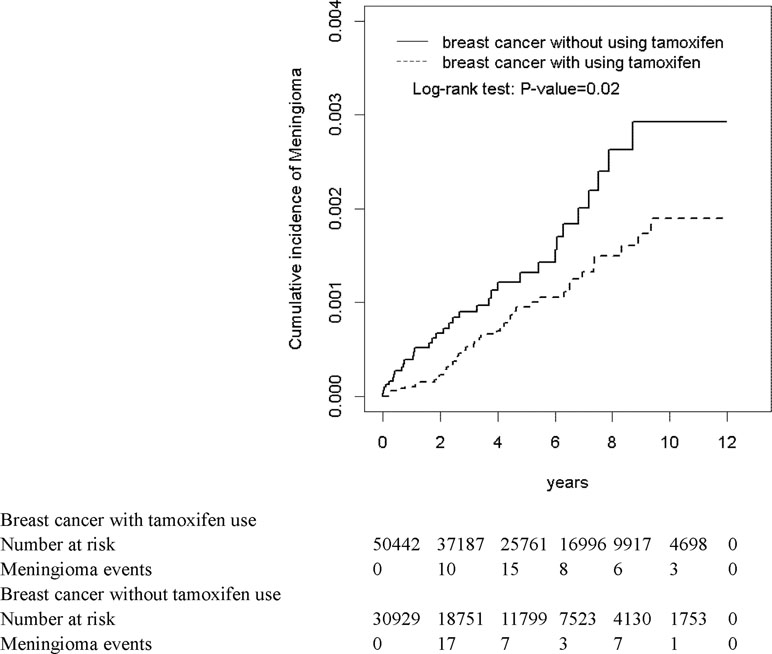
Figure 1 Cumulative incidence curves of meningioma for breast cancer with and without tamoxifen use.
The overall incidence density of meningioma was lower in the tamoxifen cohort than that in the non-tamoxifen cohort (1.77 versus 3.00 per 10,000 person-years) (Table 2). After adjusting for age, comorbidity, steroid use, statin use, thiazide diuretics use, treatment I, and treatment II, the adjusted hazard ratio (aHR) and 95% confidence interval (CI) for meningioma was 0.64-fold (95% CI = 0.40–1.02) for the tamoxifen users as compared with non-tamoxifen users.
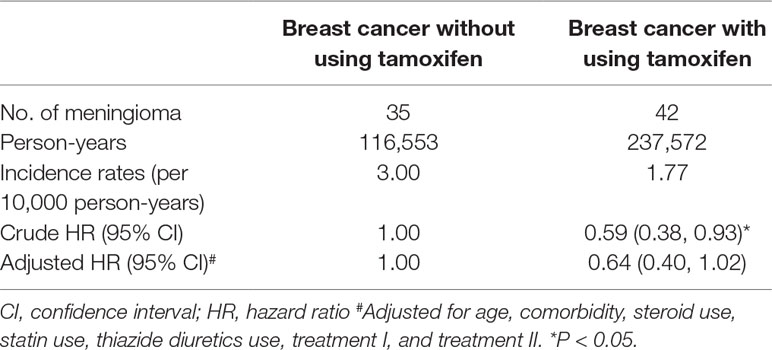
Table 2 Hazard ratios for meningioma among patients with breast cancer with and without using tamoxifen as revealed by the time-dependent regression model.
Breast cancer patients receiving >1,500 days of tamoxifen treatment exhibited significantly decreased meningioma risk compared with breast cancer patients who had not received tamoxifen treatment (aHR = 0.42, 95% CI = 0.19–0.91) (Table 3). Similar results were observed among breast cancer patients with different cumulative dosages of tamoxifen use; compared with breast cancer patients who did not use tamoxifen, the patients who used >26,320 mg of tamoxifen had a significantly (aHR = 0.44; 95% CI = 0.22–0.88) lower risk of developing meningioma (Table 4).
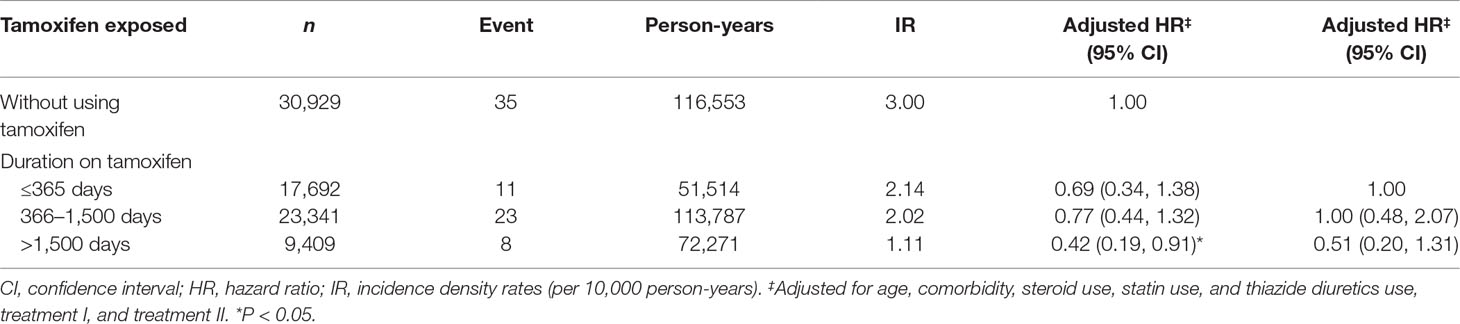
Table 3 Adjusted hazard ratio and incidence of meningioma by duration of tamoxifen therapy in patients with breast cancer with and without tamoxifen use.
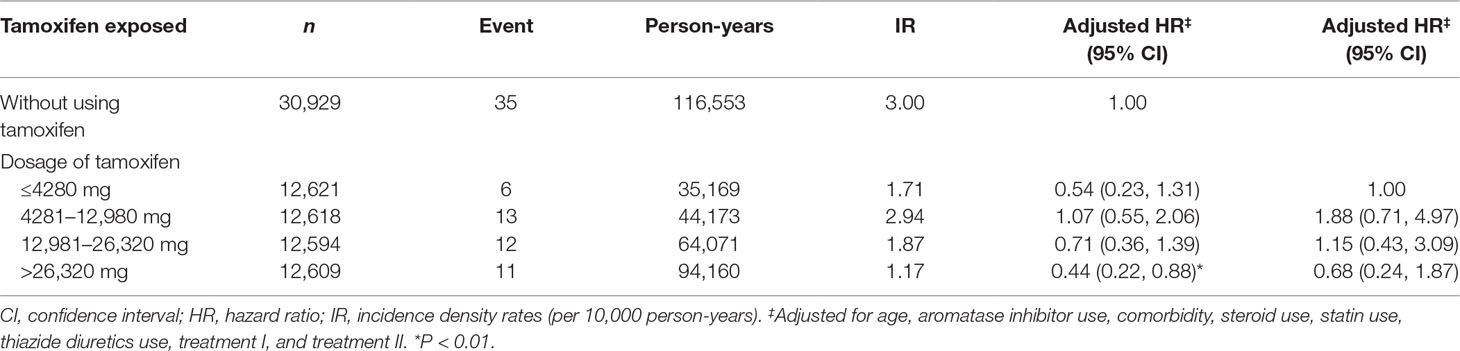
Table 4 Adjusted hazard ratio and incidence of meningioma by cumulative dosage of tamoxifen use in patients with breast cancer with and without tamoxifen use.
Table 5 illustrates the joint effect of aromatase inhibitor treatment and tamoxifen therapy on meningioma risk. Patients that received aromatase inhibitor treatment in addition to tamoxifen therapy did not have a significantly decreased risk of meningioma compared with patients without either treatment (aHR = 0.59, 95% CI = 0.31–1.15).

Table 5 Joint effects of aromatase inhibitor use and tamoxifen use on the risk of meningioma in patients with breast cancer as revealed by the time-dependent regression model.
Discussion
This large study used a comprehensive national database to assess the meningioma risk in patients with previous diagnoses of breast cancer with or without tamoxifen use. In our study, tamoxifen users had a non-significantly (36%) lower risk of developing meningioma than did tamoxifen non-users. However, the decreased risk became significant when patients took tamoxifen treatment for longer than 1,500 days or took a cumulative dosage larger than 26,320 mg.
The breast cancer–meningioma relationship has been investigated for decades, but the results have been discordant. Several studies have detected a positive association between these two conditions (Schoenberg et al., 1975; Helseth et al., 1989; Lieu et al., 2003; Rakha et al., 2007; Rao et al., 2009; Milano and Grossman, 2017). For example, Rao et al. found a strong association between breast cancer and meningioma, but only in women (Rao et al., 2009). Conversely, some studies have reported lower degrees of risk (Jacobs et al., 1992; Custer et al., 2002; Criscitiello et al., 2014). Rather than a causal link, this association is likely related to shared common etiological factors, for example, shared genetic predisposition (e.g., variations in DNA repair polymorphisms) and endogenous and exogenous hormones (Bethke et al., 2008; Wiemels et al., 2010).
Studies have suggested that hormonal factors may be involved in regulating the growth of meningioma (Hsu et al., 1997; Wahab and Al-Azzawi, 2003; Lee et al., 2006; Korhonen et al., 2010; Cea-Soriano et al., 2012; Ji et al., 2016). Researchers have indicated that hormone replacement therapy (especially estrogen-only) increases the risk of meningioma (Anderson et al., 2013; Benson et al., 2015). Previous studies have found that meningiomas tend to express progesterone receptors more frequently (32.1%–86.3%) than estrogen receptors (7.1%–50%) (Lieu et al., 2003; Wahab and Al-Azzawi, 2003; Korhonen et al., 2010), suggesting that progesterone and estrogen may influence tumor growth. Progesterone and estrogen antagonists may therefore inhibit tumor growth. An early study has found that selected meningiomas are subject to hormonal influence in vitro, and the inhibition of meningioma growth in vitro was observed by the antiprogesterone (Olson et al., 1986). Antiprogesteronal therapy and antiestrogenic therapy have been proposed for managing meningiomas (Markwalder et al., 1985; Goodwin et al., 1993; Grunberg, 1994; Ji et al., 2015); however, no definite role has been confirmed. Generally, tamoxifen binds to estrogen receptors and acts as partial antagonist or agonist depending on the type of target tissue (Yeh et al., 2014). Two studies have focused on the treatment effect of tamoxifen in refractory, recurrent, or unresectable meningiomas, but neither indicated a favorable response of meningiomas to antiestrogenic therapy (Goodwin et al., 1993; Grunberg, 1994). Regardless of the null therapeutic effect, investigators have been interested in the prophylactic role of tamoxifen in meningioma among breast cancer patients. For example, Ji et al. evaluated the association of tamoxifen with meningioma in the Swedish population and reported that women with breast cancer who did not use tamoxifen had increased meningioma incidence, whereas in breast cancer patients treated with tamoxifen, the incidence was nearly the same as that of the general population, which suggests that tamoxifen likely plays in preventing meningioma development (Ji et al., 2016). Although the current study could not conclusively establish that for breast patients, tamoxifen treatment significantly decreases the risk of subsequent meningioma compared with non-tamoxifen treatment, the results were borderline significant, with a direction (protective role) consistent with their findings. The potential mechanisms account for this discrepancy of treatment and inverse association of tamoxifen in meningioma is still undetermined. We have to acknowledge that the information regarding mechanism of action and pharmacokinetic profiles of tamoxifen in meningothelial cells is scarce. Furthermore, the possible molecular mechanism(s) in the link between tamoxifen and meningioma is undetermined yet.
The NHI patient records provide a unique resource for a nationwide investigation of meningioma incidence among breast cancer patients. Other available and useful information was also retrieved for this study. The etiology of meningioma remains unclear, and ionizing radiation exposure and chemotherapy agents may be risk factors for meningioma development (Braun et al., 2004; Umansky et al., 2008; Wiemels et al., 2010). The basic treatment information is available in the NHIRD, and we have adjusted these two factors in our analyses.
Tamoxifen in Taiwan is normally prescribed in breast cancer patients with a daily dose of 20 mg for a 5-year continuous treatment. Stratified analysis by treatment duration and cumulative dosage revealed that the inverse association of tamoxifen in meningioma among breast cancer patients was limited to those patients with long-term use (>1,500 days) and dosage larger than 26,320 mg. The compliance of patients to tamoxifen may be related to the long-term use and total dosage, and it may imply that good compliance of patients to tamoxifen can reduce the risk of meningioma. Earlier studies from NHIRD evaluating the compliance of other drugs also supported this inference (Li and Huang, 2015; Tung et al., 2017). We speculate that meningiomas are dependent on estrogen receptor (ER) as one of the reasons for the positive correlation between long-term tamoxifen use and reduced meningioma incidence. Presently, prescriptions that last longer than 5 years are uncommon as an adjuvant therapy for breast cancer. However, extending the duration of adjuvant treatment to 10 years has been previously reported to have a reduced risk of late breast cancer recurrence, thus improving survival (Davies et al., 2013). Table 4 also displays a possible biphasic dose–response curve; however, the possible reasons accounting for this phenomenon are unclear. A previous paper has assessed hormone replacement therapy and the risk of meningioma and found that the risk of meningioma increases with duration of use of combined estrogen–progestagen within 1 year and ≥10 years, which also revealed a biphasic duration–response relationship (Anderson et al., 2013). We acknowledge that the underlying mechanisms may be worth exploring in other studies. No significant joint effect was observed for treatment with tamoxifen and aromatase inhibitors. Similarly, no evidence was noted regarding whether the use of aromatase inhibitors affects the association between tamoxifen and meningioma. In addition, aromatase inhibitors without a similar association may be related to different mechanisms of anti-estrogen effect. Tamoxifen is known to antagonize activation function (AF)-2 in estrogen receptor (ER) but selectively activate estrogen receptor (ER)-AF1 and the AF1-mediated specific target genes, which are associated either with meningioma development or prevention. On the other hand, aromatase inhibitors work by inhibiting the action of the enzyme aromatase, which converts androgens into estrogens by aromatization. A previous study has found that there is a significantly increased risk of meningioma among men users of androgen analogues (Cea-Soriano et al., 2012), and we speculate that this may partially account for the null protective effect of aromatase inhibitors in the development of meningioma.
To the best of our knowledge, this research is the first study with nationwide coverage in an Asian country to focus on consequent meningioma incidence among women with breast cancer taking tamoxifen. A major strength of the present study is that it used a nationwide population-based database for comprehensive analyses, which increases the statistical power of the study and generalizability. However, the database has several intrinsic limitations. First, the NHIRD does not contain detailed histology and phenotype information regarding breast cancer and meningioma; thus, we cannot control for breast cancer subtype when comparing the differences between the use of tamoxifen. We cannot evaluate the exact estrogen receptor and progesterone receptor statuses to further correlate the hormone effects on the possible relationship between tamoxifen and meningioma, either. Furthermore, grade of meningiomas cannot be differentiated from NHIRD, and it hinders us to assess if tamoxifen use or not has different effects on different grades of meningioma. Milano et al. found that women with both breast cancer and meningioma tended to have more advanced breast cancers and smaller-sized meningiomas compared with women having only one of these diagnoses (Milano and Grossman, 2017); unfortunately, the current study cannot justify it. Second, precise brain MRI and CT information is unavailable in the NHIRD, and the resulting potential surveillance bias precludes a fair comparison of the risk of meningioma in breast cancer patients with that in the normal population. This might not be a big issue to be concerned since the central neural system (CNS) is not routinely screened in breast cancer patients, unless for patients with symptoms. On the other hand, meningioma is not systematically screened by brain MRI or CT, and the tumor may be found incidentally on an MRI or CT scan performed for other reasons. Third, information relevant to the lifestyle and behavior of the patients is scarce in the NHIRD, which made it difficult to adjust for the health behavior–related factors, such as smoking and unhealthy diets, which are well documented to increase the risk of certain cancers (Schwarz et al., 2007); moreover, the association of cigarette smoking and meningioma case status varies significantly by gender (Claus et al., 2012). Fourth, we realized that the comparator groups are not balanced in some factors as shown in Table 1; thus, we did the adjustment for these factors. However, residual confounding may still exist even after adjustment. Fifth, body mass index information is not recorded in the NHIRD, so we cannot adjust this factor in the analyses, either. Finally, tamoxifen user and non-user groups do not share cancer phenotypes. In general, patients who were prescribed tamoxifen were hormone receptor-positive, while those who were not prescribed tamoxifen were hormone receptor-negative. The former patients were known to have significantly better survival than the latter (Cianfrocca and Goldstein, 2004; Ren et al., 2014). The statistical data provided in this study could be misinterpreted since the comparison analysis in this specific setting can be compromised by other phenotypic variables. In addition, meningioma is typically a slow-growing tumor, and many cases never produce any symptoms. The risk of meningioma is higher in tamoxifen non-users partially because they were more likely to receive brain MRI or CT, for which they were easier to metastasize to brain compared with tamoxifen users. However, the current database cannot adjust for such confounding factor. Although some intrinsic limitations were imposed by the database, the data used in this study regarding the diagnoses of breast cancer and meningioma, the use of tamoxifen, as well as other treatments of breast cancer are highly trustworthy.
In summary, although primary hypothesis testing that tamoxifen use can decrease the risk of meningioma was not statistically significant, a trend of decreased risk of meningioma development among Taiwanese breast cancer survivors treated with tamoxifen was observed, especially for those with a long duration or a high dosage of tamoxifen therapy. The plausible mechanisms for the potential protective involvement of tamoxifen treatment in the meningioma development remain to be defined clearly. Although this could be explained partially by the hormone factor, additional comprehensive studies are warranted, and confirmatory evidence would be required before appropriate recommendations can be made.
Ethics Statement
The NHIRD encrypts patient personal information to protect privacy and provides researchers with anonymous identification numbers associated with relevant claims information, including sex, date of birth, medical services received, and prescriptions. Therefore, patient consent is not required to access the NHIRD. This study was approved to fulfill the condition for exemption by the Institutional Review Board (IRB) of China Medical University (CMUH104-REC2-115-CR3). The IRB also specifically waived the consent requirement.
Author Contributions
Conception and design: LS and CK; administrative support: CK; collection and assembly of data: all authors; data analysis and interpretation: all authors; manuscript writing: all authors; final approval of manuscript: all authors.
Funding
This study is supported in part by Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW108-TDU-B-212-133004), China Medical University Hospital (CMU106-ASIA-12, DMR-108-207), Academia Sinica Stroke Biosignature Project (BM10701010021), MOST Clinical Trial Consortium for Stroke (MOST 108-2321-B-039-003-), Tseng-Lien Lin Foundation, Taichung, Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds, Japan.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
HR, hazard ratio; CI, confidence interval; NHIRD, National Health Insurance Research Database; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease
References
Anderson, L., Friis, S., Hallas, J., Ravn, P., Schrøder, H. D., Gaist, D. (2013). Hormone replacement therapy increases the risk of cranial meningioma. Eur. J. Cancer 49, 3303–3310. doi: 10.1016/j.ejca.2013.05.026
Benson, V. S., Kirichek, O., Beral, V., Green, J. (2015). Menopausal hormone therapy and central nervous system tumor risk: large UK prospective study and meta-analysis. Int. J. Cancer 136, 2369–2377. doi: 10.1002/ijc.29274
Bethke, L., Murray, A., Webb, E., Sc hoemaker, M., Muir, K., McKinney, P., et al. (2008). Comprehensive analysis of DNA repair gene variants and risk of meningioma. J. Natl. Cancer Inst. 100, 270–276. doi: 10.1093/jnci/djn004
Braun, B., Lange, M., Oeckler, R., Mueller, M. M. (2004). Expression of G-CSF and GM-CSF in human meningiomas correlates with increased tumor proliferation and vascularization. J. Neurooncol. 68, 131–140. doi: 10.1023/B:NEON.0000027751.87894.f0
Cea-Soriano, L., Blenk, T., Wallander, M. A., Rodríguez, L. A. (2012). Hormonal therapies and meningioma: is there a link? Cancer Epidemiol. 36, 198–205. doi: 10.1016/j.canep.2011.08.003
Chiang, C. J., Lo, W. C., Yang, Y. W., You, S. L., Chen, C. J., Lai, M. S. (2016). Incidence and survival of adult cancer patients in Taiwan, 2002–2012. J. Formos. Med. Assoc. 115, 1076–1088. doi: 10.1016/j.jfma.2015.10.011
Cianfrocca, M., Goldstein, L. J. (2004). Prognostic and predictive factors in early-stage breast cancer. Oncologist 9, 606–616. doi: 10.1634/theoncologist.9-6-606
Claus, E. B., Park, P. J., Carroll, R., Chan, J., Black, P. M. (2008). Specific genes expressed in association with progesterone receptors in meningioma. Cancer Res. 68, 314–322. doi: 10.1158/0008-5472.CAN-07-1796
Claus, E. B., Walsh, K. M., Calvocoressi, L., Bondy, M. L., Schildkraut, J. M., Wrensch, M., et al. (2012). Cigarette smoking and risk of meningioma: the effect of gender. Cancer Epidemiol. Biomarkers Prev. 21, 943–950. doi: 10.1158/1055-9965.EPI-11-1059
Criscitiello, C., Disalvatore, D., Santangelo, M., Rotmensz, N., Bazolli, B., Maisonneuve, P., et al. (2014). No link between breast cancer and meningioma: results from a large monoinstitutional retrospective analysis. Cancer Epidemiol. Biomarkers Prev. 23, 215–217. doi: 10.1158/1055-9965.EPI-13-1041
Custer, B. S., Koepsell, T. D., Mueller, B. A. (2002). The association between breast carcinoma and meningioma in women. Cancer 94, 1626–1635. doi: 10.1002/cncr.10410
Davies, C., Pan, H., Godwin, J., Gray, R., Arriagada, R., Raina, V., et al. (2013). Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial. Lancet 381, 805–816. doi: 10.1016/S0140-6736(12)61963-1
Goodwin, J. W., Crowley, J., Eyre, H. J., Stafford, B., Jaeckle, K. A., Townsend, J. J. (1993). A phase II evaluation of tamoxifen in unresectable or refractory meningiomas: a Southwest Oncology Group study. J. Neurooncol. 15, 75–77. doi: 10.1007/BF01050266
Grunberg, S. M. (1994). Role of antiprogestational therapy for meningiomas. Hum. Reprod. 9(Suppl 1), 202–207. doi: 10.1093/humrep/9.suppl_1.202
Helseth, A., Mørk, S. J., Johansen, A., Tretli, S. (1989). Neoplasms of the central nervous system in Norway. APMIS. 97, 646–654. doi: 10.1111/j.1699-0463.1989.tb00456.x
Howard-Anderson, J., Ganz, P. A., Bower, J. E., Stanton, A. L. (2012). Quality of life, fertility concerns, and behavioral health outcomes in younger breast cancer survivors: a systematic review. J. Natl. Cancer. Inst. 104, 386–405. doi: 10.1093/jnci/djr541
Hsu, D. W., Efird, J. T., Hedley-Whyte, E. T. (1997). Progesterone and estrogen receptors in meningiomas: prognostic considerations. J. Neurosurg. 86, 113–120. doi: 10.3171/jns.1997.86.1.0113
Huang, K. W., Kuan, Y. C., Luo, J. C., Lin, C. L., Liang, J. A., Kao, C. H. (2016). Impact of long-term gastric acid suppression on spontaneous bacterial peritonitis in patients with advanced decompensated liver cirrhosis. Eur. J. Intern. Med. 32, 91–95. doi: 10.1016/j.ejim.2016.04.016
International Agency for Research on Cancer (IARC) and World Health Organization (WHO). GLOBOCAN 2012: Estimated cancer incidence, mortality and prevalence worldwide in 2012. http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx (last accessed April 9, 2019).
Jacobs, D. H., Holmes, F. F., McFarlane, M. J. (1992). Meningiomas are not significantly associated with breast cancer. Arch. Neurol. 49, 753–756. doi: 10.1001/archneur.1992.00530310101020
Ji, Y., Rankin, C., Grunberg, S., Sherrod, A. E., Ahmadi, J., Townsend, J. J., et al. (2015). Double-blind phase III randomized trial of the antiprogestin agent mifepristone in the treatment of unresectable meningioma: SWOG S9005. J. Clin. Oncol. 33, 4093–4098. doi: 10.1200/JCO.2015.61.6490
Ji, J., Sundquist, J., Sundquist, K. (2016). Association of tamoxifen with meningioma: a population-based study in Sweden. Eur. J. Cancer Prev. 25, 29–33. doi: 10.1097/CEJ.0000000000000133
Korhonen, K., Raitanen, J., Isola, J., Haapasalo, H., Salminen, T., Auvinen, A. (2010). Exogenous sex hormone use and risk of meningioma: a population-based case–control study in Finland. Cancer Causes Control 21, 2149–2156. doi: 10.1007/s10552-010-9634-2
Lee, E., Grutsch, J., Persky, V., Glick, R., Mendes, J., Davis, F. (2006). Association of meningioma with reproductive factors. Int. J. Cancer 119, 1152–1157. doi: 10.1002/ijc.21950
Li, Y. C., Huang, W. L. (2015). Effects of adherence to statin therapy on health care outcomes and utilizations in Taiwan: a population-based study. Biomed. Res. Int. 2015, 149573. doi: 10.1155/2015/149573
Lieu, A. S., Hwang, S. L., Howng, S. L. (2003). Intracranial meningioma and breast cancer. J. Clin. Neurosci. 10, 553–556. doi: 10.1016/S0967-5868(02)00305-3
Lin, N. U., Winer, E. P. (2008). Advances in adjuvant endocrine therapy for postmenopausal women. J. Clin. Oncol. 26, 798–805. doi: 10.1200/JCO.2007.15.0946
Markwalder, T. M., Seiler, R. W., Zava, D. T. (1985). Antiestrogenic therapy of meningioma—a pilot study. Surg. Neurol. 24, 245–249. doi: 10.1016/0090-3019(85)90030-8
Milano, M. T., Grossman, C. E. (2017). Meningioma in breast cancer patients: population-based analysis of clinicopathologic characteristics. Am. J. Clin. Oncol. 40, 11–16. doi: 10.1097/COC.0000000000000052
Morrison, D. H., Rahardja, D., King, E., Peng, Y., Sarode, V. R. (2012). Tumour biomarker expression relative to age and molecular subtypes of invasive breast cancer. Br. J. Cancer 107, 382–387. doi: 10.1038/bjc.2012.219
Olson, J. J., Beck, D. W., Schlechte, J., Loh, P. M. (1986). Hormonal manipulation of meningiomas in vitro. J. Neurosurg. 65, 99–107. doi: 10.3171/jns.1986.65.1.0099
Ostrom, Q. T., Gittleman, H., Fulop, J., Liu, M., Blanda, R., Kromer, C., et al. (2015). CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2008–2012. Neuro. Oncol. 17 (Suppl 4), iv1–iv62. doi: 10.1093/neuonc/nov189
Peng, Y. C., Lin, C. L., Hsu, W. Y., Chang, C. S., Yeh, H. Z., Tung, C. F., et al. (2015). Statins are associated with a reduced risk of cholangiocarcinoma: a population-based case–control study. Br. J. Clin. Pharmacol. 80, 755–761. doi: 10.1111/bcp.12641
Perez, E. A. (2007). Safety profiles of tamoxifen and the aromatase inhibitors in adjuvant therapy of hormone-response early breast cancer. Ann. Oncol. 18 (Suppl 8), viii26–35. doi: 10.1093/annonc/mdm263
Rakha, E. A., El-Sayed, M. E., Green, A. R., Paish, E. C., Powe, D. G., Gee, J., et al. (2007). Biologic and clinical characteristics of breast cancer with single hormone receptor positive phenotype. J. Clin. Oncol. 25, 4772–4778. doi: 10.1200/JCO.2007.12.2747
Rao, G., Giordano, S. H., Liu, J., McCutcheon, I. E. (2009). The association of breast cancer and meningioma in men and women. Neurosurgery 65, 483–489. doi: 10.1227/01.NEU.0000350876.91495.E0
Ren, Z., Li, Y., Hameed, O., Siegal, G. P., Wei, S. (2014). Prognostic factors in patients with metastatic breast cancer at the time of diagnosis. Pathol. Res. Pract. 210, 301–306. doi: 10.1016/j.prp.2014.01.008
Schoenberg, B. S., Christine, B. W., Whisnant, J. P. (1975). Nervous system neoplasms and primary malignancies of other sites. Neurology 25, 705–712. doi: 10.1212/WNL.25.8.705
Schwarz, S., Messerschmidt, H., Dören, M. (2007). Psychosocial risk factors for cancer development. Med. Klin. (Munich). 102, 967–979. doi: 10.1007/s00063-007-1128-y
Tung, Y. C., Huang, Y. C., Wu, L. S., Chang, C. J., Chu, P. H. (2017). Medications compliance and clinical outcome of fixed-dose combinations vs free combinations of an angiotensin II receptor blocker and a calcium channel blocker in hypertension treatment. J. Clin. Hypertens. (Greenwich) 19, 983–989. doi: 10.1111/jch.13035
Umansky, F., Shoshan, Y., Rosenthal, G., Fraifeld, S., Spektor, S. (2008). Radiation-induced meningioma. Neurosurg. Focus 24, E7. doi: 10.3171/FOC/2008/24/5/E7
Wahab, M., Al-Azzawi, F. (2003). Meningioma and hormonal influence. Climacteric 6, 285–293. doi: 10.1080/cmt.6.4.285.292
Wiemels, J., Wrensch, M., Claus, E. B. (2010). Epidemiology and etiology of meningioma. J. Neurooncol. 99, 307–314. doi: 10.1007/s11060-010-0386-3
Wigertz, A., Ahlgren, J., Holmqvist, M., Fornander, T., Adolfsson, J., Lindman, H., et al. (2012). Adherence and discontinuation of adjuvant hormonal therapy in breast cancer patients: a population-based study. Breast Cancer Res. Treat. 133, 367–373. doi: 10.1007/s10549-012-1961-4
Keywords: breast cancer, meningioma, tamoxifen, population-based study, cohort study
Citation: Sun L-M, Lin C-L, Sun S, Hsu CY, Shae Z and Kao C-H (2019) Long-Term Use of Tamoxifen Is Associated With a Decreased Subsequent Meningioma Risk in Patients With Breast Cancer: A Nationwide Population-Based Cohort Study. Front. Pharmacol. 10:674. doi: 10.3389/fphar.2019.00674
Received: 01 December 2018; Accepted: 23 May 2019;
Published: 12 June 2019.
Edited by:
Marc Poirot, Institut National de la Santé et de la Recherche Médicale (INSERM), FranceReviewed by:
Florence Dalenc, Institut Claudius Regaud, FrancePhilippe G. Frank, Université de Tours, France
Copyright © 2019 Sun, Lin, Sun, Hsu, Shae and Kao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chia-Hung Kao, ZDEwMDQwQG1haWwuY211aC5vcmcudHc=