 Huma Rasheed
Huma Rasheed Ludwig Höllein1
Ludwig Höllein1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pharmacol. , 31 August 2018
Sec. Drugs Outcomes Research and Policies
Volume 9 - 2018 | https://doi.org/10.3389/fphar.2018.00995
This article is part of the Research Topic Pharmacy Technology and Practice View all 9 articles
Substandard and falsified (SF) medicines have emerged as a global public health issue within the last two decades especially in low- and middle-income countries (LMICs). Serious consequences of this problem include a loss of trust and increased financial costs due to less disease control and more frequent complications during therapy. Of note, antimicrobial resistance is an additional long-term implication of poor-quality antimicrobials. This review covers information technology tools including medicines authentication tools (MAT) as mobile apps and messaging service, 2D barcoding approaches with drug safety alert systems, web based drug safety alerts, radiofrequency identification tags, databases to support visual inspection, digital aids to enhance the performance of quality evaluation kits, reference libraries for identification of falsified and substandard medicines, and quality evaluation kits based on machine learning for field testing. While being easy to access and simple to use, these initiatives are gaining acceptance in LMICs. Implementing 2D barcoding based on end-to-end verification and “Track and Trace” systems has emerged as a step toward global security in the supply chain. A breakthrough in web-based drug safety alert systems and data bases was the establishment of the Global Surveillance and Monitoring System by the World Health Organization in 2013. Future applications include concepts including “lab on a chip” and “paper analytical devices” and are claimed to be convenient and simple to use as well as affordable. The principles discussed herein are making profound impact in the fight against substandard and falsified medicines, offering cheap and accessible solutions.
Low- and middle-income countries (LMICs) are frequently affected by the pandemic of substandard and falsified (SF) medicines. Three quarters of the samples included in the latest World Health Organization (WHO) review were collected in LMICs and show a percentage failure rate of 9.9–10.9% amounting to a crude worth estimate of 30.5 billion USD per annum (World Health Organization, 2017a). In May 2017, the WHO revised the definition of SF medical products, whereby the term “counterfeit” has been withdrawn from this context (World Health Organization, 2017b). In brief, SF medicines are differentiated, the latter referring to unclear identity, composition, or source of the respective product.
Among the various solutions and strategies devised for combating poor-quality medicines (Kovacs et al., 2014; Höllein et al., 2016), a substantial portion is based upon information technology tools for fighting falsified medicines (Mackey and Nayyar, 2017). Information technology is defined by Merriam-Webster dictionary as “the technology involving the development, maintenance, and use of computer systems, software and networks for the processing and distribution of data “ (Merriam Webster Dictionary, 2018). A variety of technologies and approaches has been published for the detection of falsified and substandard medicines in LMIC and resource limited settings (Kaur et al., 2010; Glass, 2014; Kovacs et al., 2014; Höllein et al., 2016) which have also been compared with regard to costs, simplicity, and performance (Glass, 2014; Kovacs et al., 2014; Batson et al., 2016). In general, they are easy to operate and access, exhibit low costs, and are very user-friendly (Kovacs et al., 2014). The methods are used for initial identification, quality evaluation, as well as an efficient dissemination of information on SF medicines. The WHO proposed a three-pronged approach of prevention, detection, and response in order to tackle the menace of SF medical products (World Health Organization, 2017c). This review substantiates the above mentioned WHO approach and covers information technology tools including Medicines Authentication Tools (MAT) as mobile apps and messaging service, 2D barcoding linked MAT with drug safety alert systems, web based drug safety alerts, Radio Frequency Identification Tagging (RFID) for product tracking, databases for identification of medicinal products to aid visual inspection, digital aids to enhance performance of quality evaluation kits, reference libraries for identification of falsified and substandard medicines employing various analytical techniques, as well as quality evaluation kits based on machine learning for cheap and convenient field testing.
All identified information technology tools were classified into five categories based on their field of application (Table 1). The type of tool (mobile application, database, software, or field testing kit), respective examples, its role, and the relevance for the end user are incorporated against each application category (Table 1).
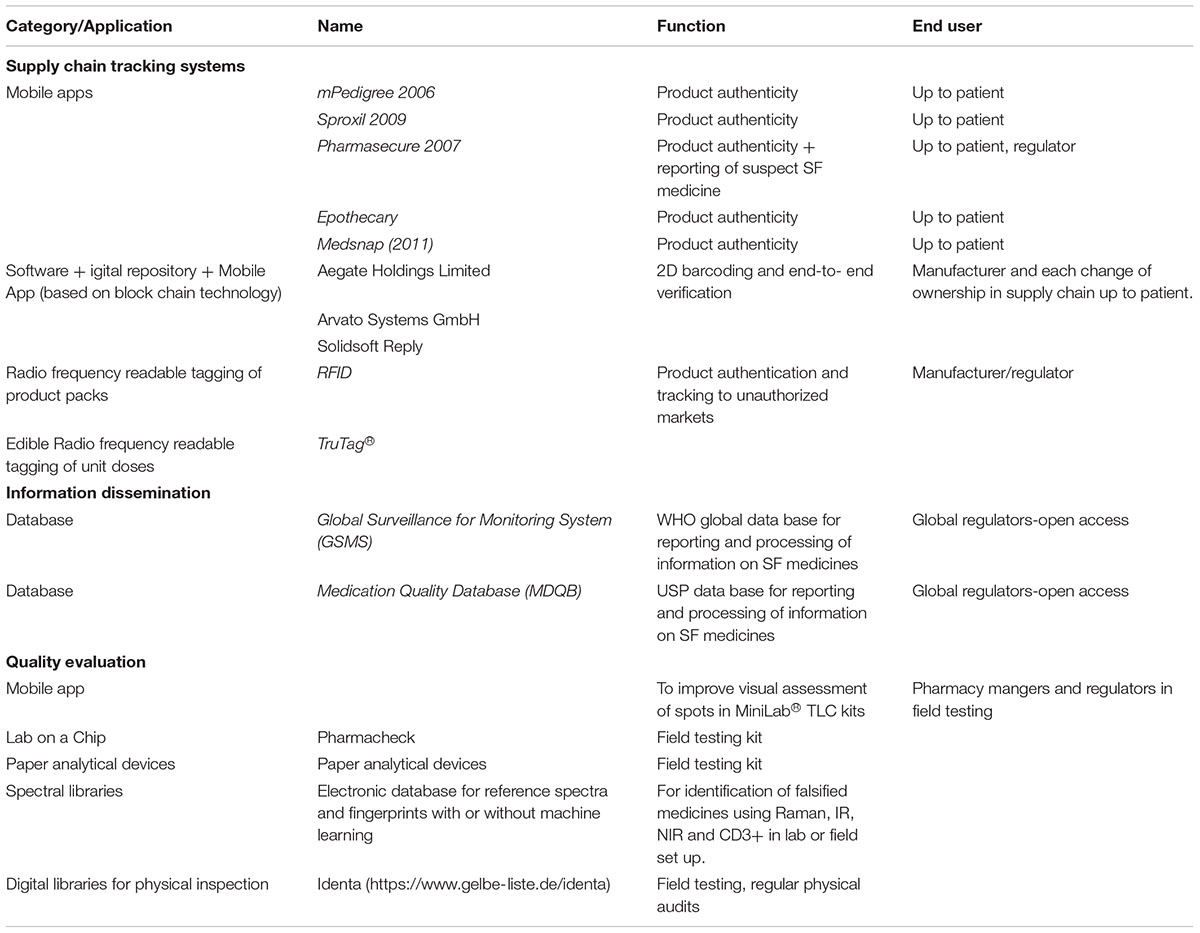
TABLE 1. Information technology tools used for the identification and control of falsified and substandard medicines and medicinal products.
These are mainly information technology-based solutions used for examining the intact packages at various points within the supply chain up to the consumer level. The concept of end-to-end verification and “Track and Trace” is characteristic for all these services, forming the fundamental basis of a traceable supply chain surveillance. Such systems gain more and more global attention.
Medicines are coded using a unique 12-digit serialization and a 2D barcode system with an end-to-end “Track and Trace” process comprising of the following steps (Naughton et al., 2017):
(a) Systematic serialization of the products at the manufacturing site. The serialization code uses block chain technology to enable end-to-end decryption (manufacturer to each user in supply chain) offering retrieval of information by an ePedigree-based digital ledger (Mackey and Nayyar, 2017). The individual coding applies to both raw materials and finished pharmaceutical products and allows multiple participants to update tracking information, to authenticate, and also to share information using integrated anticounterfeit devices (Mackey and Nayyar, 2017).
(b) Authentication, i.e., verification of the product authenticity, by scanning the imprinted codes reveals the “authenticity status” and may include additional information, e.g., whether the product is expired, recalled or falsified. The European Union Falsified Medicines Directive (EU-FMD) requires this authentication to be carried out at the point of supply, whereas the United States Drug Supply Chain Security Act (DSCSA) demands a verification on each change of ownership during the medicine supply and distribution process, respectively.
(c) Decommissioning of the product, if applicable, is required at the final point of supply to the patient in accordance with EU-FMD.
As soon as a product has been scanned for verification, a color-coded pop-up message appears, guiding the user to take appropriate action, e.g., whether a product must be quarantined or can be handed to the patient, respectively. Such warnings and alerts may also be implemented during stocking, dispensing, and supply of medicines, facilitating the identification of suspected or faulty stocks.
The effectiveness of the system is based upon the practice of the end users, i.e., all medicines requiring authentication must be authenticated eventually and a respective action must be taken, accordingly (Naughton et al., 2017). Examples for technology providers are Aegate Holdings Limited, Arvato Systems GmbH, and Solidsoft Reply; they have been assigned by The European Medicines Verification Organization for the provision of medication authentication technology within the European Union (Naughton et al., 2017).
“Track and Trace” systems using 2D or data matrix bar coding are gaining world-wide acceptance. Table 2 summarizes the implementation status in different countries. In January 2012, Turkey became the very first country to implement a fully mobile app based verification system (Taylor, 2015). SecurPharm, a consortium of the Federal Union of German Association of Pharmacists (ABDA) and other professional organizations, launched its pilot project in 2013 involving pharmaceutical manufacturers, wholesalers, and about 400 pharmacies (securPharm e.V, 2012, 2016, 2018). The EU-FMD marks 9th February 2019 as deadline for adopting this technology on all prescription medicines throughout all member states (European Medicines Agency, 2017).
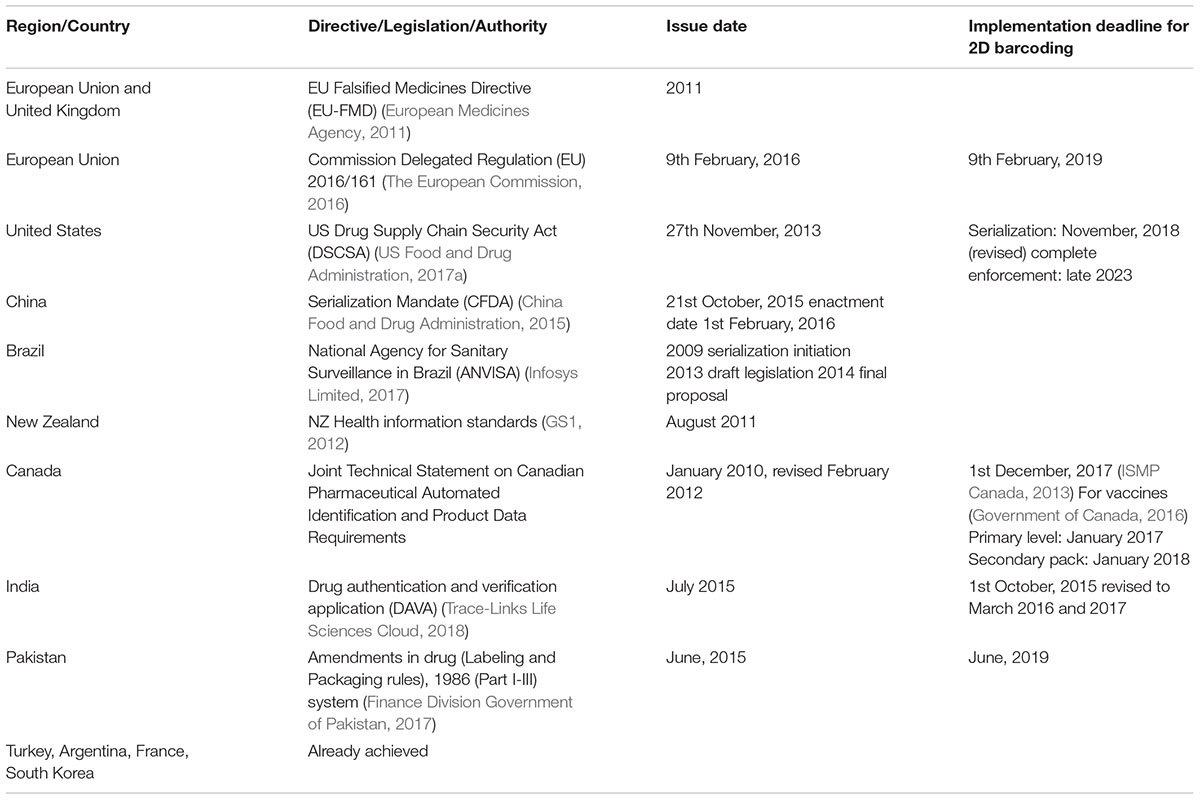
TABLE 2. Implementation status for 2D bar coding of medicines in different countries.
Mobile applications for medication authentication are accessible for large parts of the population, thus directly reaching the patient. Mobile apps and SMS based medicine authentication tools for detecting falsified medicines were pioneered by mPedigree (Nigeria) in 2006 (Wall, 2017), Sproxil (Nigeria) in 2009 (Wall, 2017), İlaç Takip Sistemi (Turkey) in 2010, and Pharmsecure (Nigeria and India) in 2012. These MATs involve the use of a visible or scratchable code which has been printed on the product package by the manufacturer. The patient sends this code to the respective authentication databases using SMS. In reply, a message is received stating whether the stocks inquired are tagged genuine or fake; scannable bar codes are also provided. In Pharmsecure, customers can also capture a photograph of the suspected medicine and send it to the database administrators. Evidence is subsequently transferred to the manufacturer for further investigation. Hence, an early detection of SF medicines is possible, facilitating a rapid response.
The mobile App MyDawa from Ion Kenya, Inc. also uses scratchable codes and can be used for verifying the authenticity of medicines and related medicinal supplies delivered to the Nigerian market. More than 70 international pharmaceutical companies are using the services of Sproxil in Kenya, Ghana, Nigeria, South Africa, and Mali (Wall, 2017). The mPedigree startup was initiated in Nigeria and is now operational in 12 countries across Asia and Africa.
Physicochemical identifiers are a form of authentication token using invisible imprints on a distinct product unit (Wall, 2017). For example, the TruTag® technology employs edible micro-tagging of tablets using high purity silica which offers low costs and reliable solutions for improved security measures for products and/or medicines prone to falsification and illegal trafficking (TruTag Technologies Inc., 2017). The product information can be retrieved anywhere using portable TruTag® optical scanners (TruTag Technologies Inc., 2017).
RFID tags are applicable to products and respective packages using active or passive chips being able to deliver a small set of information, e.g., regarding the origin of a particular product (ISMP Canada, 2013). Usually, such systems consist of a transponder or a tag affixed to or carried in the product, transmitting various information to the interrogator or the reader in form of radio waves or wireless signals, respectively. All fields of logistics can benefit from this technique; commonly, passive tags are used which transmit data only when irradiated with a radio signal from an RFID reader in close proximity, thus not requiring any power supply. Modern hardware is designed in a very inconspicuous manner and is mostly constructed as thin labels or small microchips which can be placed inside a product packaging, thus being invisible at first glance but readable from outside.
Although using this technology is recommended by the U.S. Food and Drug Administration, the individual costs per unit are quite high when compared to optical coding techniques. However, particularly in the field of monitoring temperature sensitive medicines, active chips are utilized to constantly record the surrounding temperature and thus, to provide a detailed log at any time during and after transport as well as storage.
The use of drug safety databases and alerts regarding SF medicines has become an essential tool for an efficient and reliable dissemination of information and control of poor-quality medicines in the global medicine supply chains. A remarkable breakthrough in this context is the establishment of the Global Surveillance and Monitoring System (GSMS) by the WHO in 2013. Recent landmark reports on SF medicinal products conducted by the WHO presented a literature review of 100 publications with major data contributed from the Medicines Quality Database (MQDB) and the GSMS (World Health Organization, 2017a).
Routine quality evaluation procedures require a sophisticated and expensive infrastructure which prove to be a limitation for LMICs (Höllein et al., 2016). A few novel approaches of developing mobile, convenient, and affordable field kits using machine learning to identify and quantify a medicine based upon its chemical nature (Mackey and Nayyar, 2017) or a unique finger print derived from drug interaction analysis are under development (Redaktion Gelbe Liste, 2013; Weinstein and Zaman, 2017).
The GPHF MiniLab® tool kit, established in the 1980’s by the Global Pharma Health Fund, pioneers the concept of field testing for detection of counterfeit and substandard medicines. It has been operating in 95 countries across the world. The current edition of the MiniLab® manual covers more than 90 active compounds including essential antibacterial and antituberculotic drugs. The kit employs thin layer chromatography with visual evaluation of the respective chromatograms as main analytical technique. Of note, the tests are semiquantitative and thus not suitable for analyzing the content of compounds where the exact dosage is critical, e.g., in the case of antibiotics. However, the limitation of visual evaluation has recently been overcome by introducing a mobile phone application for measuring and comparing the spot intensity (Fadeyi et al., 2015). In addition, it was shown that during analysis and evaluation, significant deviations from the true content might occur (World Health Organization, 2011; Höllein and Holzgrabe, 2014).
The project aims to deliver a “lab on a chip” concept that can give results by color indicators in the field (Beltman et al., 2013; Weinstein and Zaman, 2017). Interaction analysis was performed using E. coli to develop fingerprint results for 27 antibiotics. The project is in its developmental stage and aims to provide a fast, low cost, and portable technology that is applicable to the most remote settings. No sample preparation, electric supply, and only minimal training is required (Kovacs et al., 2014).
Spectroscopic libraries are required in Raman and near infra-red (NIR) spectroscopy as well as in newer technologies like the CD3+ counterfeit device approved by the U.S. Food and Drug Administration or Paper Analytical Devices. These techniques may or may not be linked to machine learning tools for the identification of SF medicines (Kovacs et al., 2014; Batson et al., 2016; Mackey and Nayyar, 2017), exhibiting low to medium costs and representing valuable tools for detecting SF medicines (Kovacs et al., 2014; Batson et al., 2016; Mackey and Nayyar, 2017).
Visual inspection of the primary and secondary product packages as well as the respective dosage forms holds a key position in immediate identification of falsified medicines. A respective scheme is offered within a WHO guideline (World Health Organization, 1999; Kaur et al., 2010). In Germany, registered pharmacists and practitioners have access to the online software identa1 for physical identification of medicaments, thus facilitating an early identification and reporting of suspicious medicines. The recall of falsified Pegasys® injection in Germany in 2013, identified during the routine internal audit process, is a prominent example of unraveling falsified medicines using this tool (Redaktion Gelbe Liste, 2013; Roche Pharma AG, 2017).
The constant rise of various types of falsified and substandard medicines demand the incorporation of a fast and effective identification of poor-quality medicines throughout the global supply chain. Efficient and reliable processing of information as well as dissemination of alerts is warranted to minimize the damage caused by the administration of any faulty medicines. Information technology has placed a significant role in providing solutions to both these needs. The majority of currently available applications comprise of medicine authentication tools involving verification of the product packaging. Identification of falsified medicines based upon their active pharmaceutical ingredient (API) content is also anticipated. However, very few applications claim to inform on the amount and purity of the API and innovative approaches are needed to offer accessible solutions in this regard.
Implementing 2D and data matrix barcoding has come up as a unified global strategy. Countries have placed this global intervention program within their respective health system at varying pace. Phase wise realization is seen, with the first step being verifying the serialization and data banking at a local repository (fixed data), proceeding to the second level of enabling data access using a cloud-based repository accessible by multiple users to receive, share, and update information. Equipping pharmacies with the respective soft- and hardware devices including barcode scanners is also a major part of this process. The final stage of the “Track and Trace” process enables a proactive bidirectional system of sending alerts and product warnings that could be linked to electronic prescribing portals to ensure maximum patient safety. However, costs and lack of awareness about the barcoding system had been the major impeding factors in its implementation process. The United States have postponed (US Food and Drug Administration, 2017b) the process to several deadlines and so is the case with Pakistan, where a large manufacturing industry exists. It is yet to achieve the first milestone of elevating a Global Trade Identification Number (GTIN) and serialization to the level of primary packaging by all manufacturers.
India and China are the two main global suppliers of raw materials and finished pharmaceuticals, and their compliance with the implementation of GS1 standards using barcoding holds crucial importance in the success of an end-to-end “Track and Trace” process. The Indian Drug Authentication and Verification Application (DAVA) introduced in 2012 was an award-winning project (GS1 India, 2017). Contrary to that, China has not yet adopted the global concept of serialization and a separate China National Drug Code with serial numbers is issued through its own Product Identification, Authentication and Tracking System (PIATS) (Infosys Limited, 2017).
Implementation of product serialization and barcoding enables end users, including patients, to identify the authenticity of a product, e.g., through mobile phones equipped with a suitable application for reading the barcodes. This broader accessibility of product identification tools down to the patient level will create more public awareness and a participatory approach for the identification of poor-quality medicines in the supply chain. Increased sensitivity at the consumer level and their engagement in implementing a collective scrutiny solution regarding falsified medicines (Mackey and Nayyar, 2017) is particularly important for LMICs where most of the health expenditure is covered by out-of-pocket expense.
“Track and Trace” is a proactive system that updates consumer on the product safety and authenticity at each stage of usage. The collaboration of several systems (e.g., GSMS, Vigibase, and “Track and Trace”) will provide a major impact in the delivery of safe and efficacious medicines worldwide. GSMS and Vigibase are two major global data bases, with GSMS targeting only registration of SF medicines, whereas Vigibase is based upon pharmacovigilance. Currently, LMICs are only minor contributors to the global data base on pharmacovigilance. The implementation of GSMS in the WHO member states will increase the sensitization of authorities and masses over drug safety issues.
Certain regions and countries face poor access to medicines due to failure of registration status, unavailability of particular products, high potentials for drug abuse, corruption or pricing issues, all of them representing predisposing factors to illegal medicine trade and diversion (World Health Organization, 2017a). Tracking is inevitable to ensure that funded and/or donated supplies reach their intended destinations, of note particularly including conflict and disaster-ridden regions. RFID is the best resource for tracking any unauthorized movement of medicines because of the unique technology design and the possibility to extract and store the respective information in web-based portals or server systems at any time (Mackey and Nayyar, 2017). In contrast to 2D barcoding, RFID technologies can be used to identify a product even if it is not in the line-of-sight of the scanner and is detected automatically when in range of the receiver (ISMP Canada, 2013). Readers can be portable, mounted on a post or over head or built in the construction of storage space or buildings, (US Food and Drug Administration, 2017c) thereby increasing the chances of detection of unauthorized movement of the product or consignment. Moreover, radiowaves can penetrate several layers of packaging and allow batch reading of multiple items at a time (ISMP Canada, 2013).
The availability of digital product identification catalogs like “identa” for making regular internal audits for stocked medicines invites retail pharmacist to share the role of a regulator in identification of falsified medicines (Gelbe Liste, 2018). This cost-effective, proactive, and participatory model of fighting against SF medicines practiced in Germany can prove to be effective in LMICs. Availability of such software to health care professionals through mobile applications can make it more user friendly and applicable in remote settings. Training of the field regulatory inspectors on use of such aids can enhance the impact of the intervention. Information technology and digital aids are having a profound impact in the fight against SF medicines and constitute a promising area offering cheap and broadly accessible solutions.
HR conceived, designed the review, and wrote first draft of the manuscript. LH and UH refined the draft, and provided intellectual input. All authors contributed to manuscript revision, read, and approved the submitted version.
Authors are thankful to the Higher Education Commission (HEC), Pakistan (Scholarship Reference No.:1-1/PM/OSS-II/Batch-4/Germany/2012/9493) and the University of Veterinary and Animal Sciences, Lahore, Pakistan (paid study leave) for financially supporting HR for her doctoral studies. Gratitude is also conveyed to German Academic Exchange Service (DAAD), Germany for provision of their administrative support for the scholarship program of HR. This publication was funded by the German Research Foundation (DFG) and the University of Wuerzburg in the funding programme “Open Access Publishing” along with partial support from the University of Veterinary and Animal Sciences, Lahore, Pakistan.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Special thanks extended to Dr. Jens Schmitz, Academic Counselor at Institute of Pharmacy and Food Chemistry, University of Wuerzburg, Germany for sharing the experience of German pharmacy systems with HR.
Batson, J. S., Bempong, D. K., Lukulay, P. H., Ranieri, N., Satzger, R. D., and Verbois, L. (2016). Assessment of the effectiveness of the CD3+ tool to detect counterfeit and substandard anti-malarials. Malar. J. 15:119. doi: 10.1186/s12936-016-1180-2
Beltman, J. J., van den Akker, T., Bwirire, D., Korevaar, A., Chidakwani, R., van Lonkhuijzen, L., et al. (2013). Local health workers’ perceptions of substandard care in the management of obstetric hemorrhage in rural Malawi. BMC Pregnancy Childbirth 13:39. doi: 10.1186/1471-2393-13-39
China Food and Drug Administration (2015). CFDA Issues Administrative Measures for Quality Supervision on the Use of Medical Devices. Available at: http://eng.sfda.gov.cn/WS03/CL0757/133461.html [accessed June 27, 2018].
European Medicines Agency (2011). Directive 2011/62/EU of The European Parliament and of the Council of 8 June 2011 Amending Directive 2001/83/EC on the Community Code Relating to Medicinal Products for Human Use, as Regards the Prevention of the Entry into the Legal Supply Chain of Falsified Medicinal Products. Available at: https://ec.europa.eu/health/sites/health/files/files/eudralex/vol-1/dir_2011_62/dir_2011_62_en.pdf [accessed June 3, 2018].
European Medicines Agency (2017). EMA/785582/2014 rev.2: Implementation Plan for the Introduction of the Safety Features on the Packaging of Centrally Authorised Medicinal Products for Human Use. Available at: http://www.ema.europa.eu/docs/en_GB/document_library/Other/2016/02/WC500201413.pdf [accessed February 22, 2018].
Fadeyi, I., Lalani, M., Mailk, N., Wyk, A. V., and Kaur, H. (2015). Quality of the antibiotics-amoxicillin and co-trimoxazole from Ghana, Nigeria, and the united kingdom. Am. J. Trop. Med. Hyg. 92, 87–94. doi: 10.4269/ajtmh.14-0539
Finance Division Government of Pakistan (2017). The Economic Survey of Pakistan- Chapter: Health. Available at: http://www.finance.gov.pk/survey/chapters_16/11_Health.pdf [accessed August 12, 2017].
Gelbe Liste (2018). Gelbe Liste Indenta. Available at: https://www.gelbe-liste.de/identa [accessed February 22, 2018].
Glass, B. D. (2014). Counterfeit drugs and medical devices in developing countries. Res. Rep. Trop. Med. 5, 11–22. doi: 10.2147/RRTM.S39354
Government of Canada (2016). Bar Code Standards for Vaccine Products in Canada (Update 2014-2015). Available at: https://www.canada.ca/en/public-health/services/publications/healthy-living/bar-code-standards-vaccine-products-canada-update-2014-2015.html [accessed June 27, 2018].
GS1 (2012). GSI Health Care Newsletter No. 24-Spring/Summer-2012. Available at: https://www.gs1.org/docs/healthcare/GS1_Healthcare_Newsletter_24_Q2_2012.pdf [accessed February 22, 2018].
Höllein, L., and Holzgrabe, U. (2014). Development of simplified HPLC methods for the detection of counterfeit antimalarials in resource-restraint environments. J. Pharm. Biomed. Anal. 98, 434–445. doi: 10.1016/j.jpba.2014.06.013
Höllein, L., Kaale, E., Mwalwisi, Y. H., Schulze, M. H., and Holzgrabe, U. (2016). Routine quality control of medicines in developing countries: analytical challenges, regulatory infrastructures and the prevalence of counterfeit medicines in Tanzania. TrAC Trends Anal. Chem. 76, 60–70. doi: 10.1016/j.trac.2015.11.009
Infosys Limited (2017). Pharmaceutical Serialization and Track and Trace. Available at: https://www.infosys.com/industries/life-sciences/white-papers/documents/pharmaceutical-serialization.pdf [accessed June 27, 2018].
ISMP Canada (2013). Medication Bar Coding System Implementation Planning: A Resource Guide. Available at: https://www.ismp-canada.org/barcoding/download/ResourceGuide/BarCodingResourceGuideFINAL_SectionI.pdf [accessed June 27, 2018].
Kaur, H., Green, M., Hostetler, D., Fernáández, F., and Newton, P. (2010). Antimalarial drug quality: methods to detect suspect drugs. Therapy 7, 49–57. doi: 10.1186/s12936-016-1180-2
Kovacs, S., Hawes, S. E., Maley, S. N., Mosites, E., Wong, L., and Stergachis, A. (2014). Technologies for detecting falsified and substandard drugs in low and middle-income countries. PLoS One 9:e90601. doi: 10.1371/journal.pone.0090601
Mackey, T. K., and Nayyar, G. (2017). A review of existing and emerging digital technologies to combat the global trade in fake medicines. Expert Opin. Drug Saf. 16, 587–602. doi: 10.1080/14740338.2017.1313227
Merriam Webster Dictionary (2018). Definition of Information Technology. Available at: https://www.merriam-webster.com/dictionary/information%20technology [accessed February 21, 2018].
Naughton, B., Roberts, L., Dopson, S., Brindley, D., and Chapman, S. (2017). Medicine authentication technology as a counterfeit medicine-detection tool: a Delphi method study to establish expert opinion on manual medicine authentication technology in secondary care. BMJ Open 7:e013838. doi: 10.1136/bmjopen-2016-013838
Redaktion Gelbe Liste (2013). Rote-Hand-Brief zu Pegasys. Available at: https://www.gelbe-liste.de/rote-hand-briefe/rote-hand-brief-pegasys [accessed February 22, 2018].
Roche Pharma AG (2017). Fälschung von PEGASYS® (Pegyliertes Interferon Alfa-2a),Fertigspritze 180 Mikrogramm/0,5 ml, Chargenbezeichnung B1299B03 EXP 07 2015. Available at: https://www.akdae.de/Arzneimittelsicherheit/RHB/Archiv/2013/20131111.pdf [accessed December 20, 2017].
securPharm e.V (2012). Delegated Act on the Detailed Rules for a Unique Identifier for Medicinal Products for Human use, and its Verification. Available at: https://ec.europa.eu/health/sites/health/files/files/falsified_medicines/2012-06_safety-features/securpharm.pdf [accessed February 22, 2018].
securPharm e.V (2016). Falsified Medicines Directive: New Safety Features to Arive in Three Years. Available at: http://www.securpharm.de/fileadmin/user_upload/2016-02-09_PR_delegated_regultation_published.pdf [accessed June 26, 2018].
securPharm e.V (2018). Status Report 2018- Status of the Project to Implement the Falsified Medicine Directive. Available at: http://www.securpharm.de/fileadmin/pdf/statusbericht/status_report_2018.pdf [accessed June 25, 2018].
Taylor, P. (2015). Turkish Medicines Verification app Taking Off? Available at: https://www.securingindustry.com/pharmaceuticals/turkish-medicines-verification-app-taking-off-/s40/a2284/#.WnbWoqiWbMU [accessed February 4, 2018].
The European Commission (2016). Commission Delegated Regulation (EU) 2016/161 of 2 October 2015 Supplementing Directive 2001/83/EC of the European Parliament and of the Council by Laying Down Detailed Rules for the Safety Features Appearing on the Packaging of Medicinal Products for Human Use OJ L32 59. Available at: https://ec.europa.eu/health/sites/health/files/files/eudralex/vol-1/reg_2016_161/reg_2016_161_en.pdf [accessed June 26, 2018].
Trace-Links Life Sciences Cloud (2018). India’s Track and Trace Regulations Overview. Available at: https://tracelink-quality-portal.com/solutions/india [accessed June 26, 2018].
TruTag Technologies Inc. (2017). Brand Protection for Pharmaceutical + Nutraceutical. Available at: https://www.trutags.com/pharmaceutical-nutraceutical/ [accessed June 27, 2018].
US Food and Drug Administration (2017a). Drug Supply Chain Security Act (DSCSA) Implementation Plan. Available at: https://www.fda.gov/Drugs/DrugSafety/DrugIntegrityandSupplyChainSecurity/DrugSupplyChainSecurityAct/ucm382022.htm [accessed June 27, 2018].
US Food and Drug Administration (2017b). FDA Issues Draft Guidance: Product Identifier Requirements Under the Drug Supply Chain Security Act – Compliance Policy. Available at: https://www.fda.gov/Drugs/DrugSafety/DrugIntegrityandSupplyChainSecurity/DrugSupplyChainSecurityAct/ ucm565358.htm [accessed June 27, 2018].
US Food and Drug Administration (2017c). Radio Frequency Identification (RFID). Available at: https://www.fda.gov/radiation-emittingproducts/radiationsafety/electromagneticcompatibilityemc/ucm116647.htm [accessed July 4, 2018].
Wall, M. (2017). Counterfeit Drugs: People are Dying Every Day. Available at: http://www.bbc.com/news/business-37470667 [accessed August 8, 2017].
Weinstein, Z. B., and Zaman, M. H. (2017). Quantitative bioassay to identify antimicrobial drugs through drug interaction fingerprint analysis. Sci. Rep. 7:42644. doi: 10.1038/srep42644
World Health Organization (1999). WHO/EDM/99.1 Counterfeit Drugs: Guidelines for the Development of Measures to Combat Counterfeit Drugs. Available at: http://apps.who.int/medicinedocs/pdf/h1456e/h1456e.pdf [accessed September 24, 2017].
World Health Organization (2011). WHO/EMP/QSM/2011.1. Survey of the Quality of Selected Antimalarial Medicines Circulating in Six Countries of Sub-Saharan Africa. Available at: http://www.who.int/medicines/publications/WHO_QAMSA_report.pdf [accessed June 24, 2018].
World Health Organization (2017a). A Study on the Public Health and Socioeconomic Impact of Substandard and Falsified Medical Products. Available at: http://www.who.int/medicines/regulation/ssffc/publications/Layout-SEstudy-WEB.pdf?ua=1 [accessed December 10, 2017].
World Health Organization (2017b). Seventieth World Health Assembly. Available at: http://www.who.int/mediacentre/news/releases/2017/dementia-immunization-refuguees/en/ [accessed December 20, 2017].
World Health Organization (2017c). WHO Global Surveillance and Monitoring System for Substandard and Falsified Medical Products. Available at: http://www.who.int/medicines/regulation/ssffc/publications/Layout-SEstudy-WEB.pdf?ua=1 [accessed December 10, 2017].
Keywords: information technology, substandard and falsified medicines, field testing, quality evaluation, mobile apps, medicine authentication tools, Track and Trace
Citation: Rasheed H, Höllein L and Holzgrabe U (2018) Future Information Technology Tools for Fighting Substandard and Falsified Medicines in Low- and Middle-Income Countries. Front. Pharmacol. 9:995. doi: 10.3389/fphar.2018.00995
Received: 09 July 2018; Accepted: 13 August 2018;
Published: 31 August 2018.
Edited by:
Zaheer-Ud-Din Babar, University of Huddersfield, United KingdomReviewed by:
Kurt Neumann, Independent Researcher, Kerékteleki, HungaryCopyright © 2018 Rasheed, Höllein and Holzgrabe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ulrike Holzgrabe, dWxyaWtlLmhvbHpncmFiZUB1bmktd3VlcnpidXJnLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.