
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 20 March 2025
Sec. Pediatric Hematology and Hematological Malignancies
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1573334
This article is part of the Research TopicDiagnosis and Therapy Pediatric Hematological Malignancies - Recent Progress - Volume IIView all 3 articles
 Polliany Roberta Dorini Pelegrina1,2*
Polliany Roberta Dorini Pelegrina1,2* Rita de Cassia Barbosa Tavares3Adriana Mello Rodrigues1,2,4Gisele Loth1,2,4Samantha Nichele4,5Cilmara Kuwahara2Fernanda Moreira de Lara Benini2Carolina Martins de Almeida Peixoto2Juliana Bach1,2Joanna Trennepohl4Lara Maria Miranda de Gouvea4,5Rafaella Muratori5Adriana Koliski4Rebeca Toassa Gomes4Marcia Quiroga2,4Simone Pereira Lermontov3Valeria Gonçalves da Silva3Ana Paula de Azambuja4Margareth Kleina Feitosa2,4
Rita de Cassia Barbosa Tavares3Adriana Mello Rodrigues1,2,4Gisele Loth1,2,4Samantha Nichele4,5Cilmara Kuwahara2Fernanda Moreira de Lara Benini2Carolina Martins de Almeida Peixoto2Juliana Bach1,2Joanna Trennepohl4Lara Maria Miranda de Gouvea4,5Rafaella Muratori5Adriana Koliski4Rebeca Toassa Gomes4Marcia Quiroga2,4Simone Pereira Lermontov3Valeria Gonçalves da Silva3Ana Paula de Azambuja4Margareth Kleina Feitosa2,4 Alberto Cardoso Martins Lima4Carmem Bonfim1,2
Alberto Cardoso Martins Lima4Carmem Bonfim1,2
Background: Hematopoietic cell transplantation (HCT) represents a well-established therapeutic strategy for high-risk leukemia, though post-transplant relapse remains a significant challenge, particularly in resource-limited settings
Procedure: In this retrospective study, we analyzed medical records of 310 pediatric patients (age < 18 years) who underwent HCT for acute leukemias at four Brazilian institutions between 2010 and 2019.
Results: The cohort included patients with acute lymphoblastic leukemia (ALL; 74.2%) and acute myeloid leukemia (AML; 25.8%). The median age was 9.52 years (range: 0.25–17.97), with male predominance (68.3%). Total body irradiation (TBI)-based conditioning was utilized in 72.6% of cases, and bone marrow served as the predominant graft source (74.5%). Prior to transplantation, 46.5% of patients were in first complete remission. Post-transplant relapse occurred in 36.7% of patients at a median of 245 days (range: 38–2,505). With a median follow-up of 2,019 days (5.5 years), overall survival was 69.3% at one year, declining to 62.4% at two years. The cumulative incidence of relapse was 12.6%, 28.8%, and 33.4% at 100 days, one year, and two years post-HCT, respectively. Adjusted analysis revealed increased relapse risk in patients with mixed donor chimerism, positive minimal residual disease (MRD) status before HCT, and disease status beyond first complete remission (including CR2, advanced disease, and refractory disease).
Conclusion(s): These findings underscore the elevated relapse risk associated with advanced disease status, positive pre-HCT MRD, and mixed donor chimerism post-transplant. Future interventions should prioritize improving diagnostic capabilities, expanding access to modern treatment protocols, and facilitating early referral to transplant centers, particularly for aggressive disease presentations.
Hematopoietic cell transplantation (HCT) has emerged as a well-established therapeutic modality for diverse malignant and nonmalignant disorders. Recent decades have witnessed remarkable improvements in post-HCT outcomes, primarily attributed to advances in supportive care, high-resolution HLA typing technologies, and the expansion of stem cell donor registries. Despite its proven efficacy in enhancing cure rates for high-risk leukemia patients, achieving sustained remission remains challenging, particularly for those who experience disease recurrence within the first year post-transplantation (1, 2).
In high-income nations, post-HCT relapse represents the predominant cause of treatment failure and mortality, with cumulative incidence rates reaching 20% and 35% for Acute Lymphoblastic Leukemia (ALL) and Acute Myeloid Leukemia (AML), respectively (3). The prognosis following post-HCT disease progression remains poor, as evidenced by a comprehensive study of 279 pediatric cases revealing a median survival of merely 149 days (4). These findings underscore the critical need for effective relapse prevention and management strategies in high-risk populations. Notably, data from the Brazilian registry, encompassing over 5,000 patients with malignant diseases, presents a contrasting perspective to the Center for International Blood and Marrow Transplant Research (CIBMTR) findings (5). In the Brazilian context, infections, rather than relapse or organ failure, emerge as the primary cause of mortality within the initial 100 days post-HCT, highlighting the importance of considering regional healthcare disparities when analyzing post-transplant outcomes (6).
Currently, there is no standard recommendation for managing post-HCT relapse (7). This challenge is particularly pronounced in developing nations, where resource constraints often preclude access to innovative therapeutic options readily available in high-income countries. Such interventions include novel targeted agents like blinatumomab and inotuzumab, as well as advanced cellular therapies such as CAR T-cells, which could potentially serve as bridge-to-transplant strategies (8, 9) Understanding the characteristics associated with post-HCT relapse in resource-limited settings and identifying shared healthcare challenges becomes crucial for improving outcomes to match those observed in more developed nations.
Our investigation evaluated outcomes of hematopoietic cell transplantation in pediatric acute leukemia patients in Brazil's resource-constrained setting, especially regarding relapse patterns and risk factors. By identifying key predictors of transplant outcomes, we aim to develop strategies to improve long-term survival in this population.
We analyzed the medical records of patients who underwent HCT for acute leukemias at four Brazilian institutions (Hospital Pequeno Príncipe, Hospital de Clínicas da UFPR, Hospital Nossa Senhora das Graças e Instituto Nacional do Câncer), between 2010 and 2019. All patients were younger than 18 years-old, and the diagnosis of the malignancy was established at the referring institution. The remission status was determined based on the latest available bone marrow evaluation before HCT. Patients were in remission if they had normal marrow cellularity and fewer than <5% blasts in the bone marrow, while those with ≥5% marrow blasts were classified as being in relapse. Measurable residual disease (MRD) was defined as any level of leukemic marrow blasts detected by available technology, including cytogenetics, molecular analysis, or multiparameter flow cytometry. Disease phase was categorized according to the number of medullary remission or relapse events prior to hematopoietic cell transplantation (HCT). Advanced disease was defined as patients who had achieved third or subsequent complete remission (≥CR3). For full compatibility: we consider 10/10 bone marrow and peripheral blood donors compatible, and 6/6 for cord blood. Prior to HCT, patients were treated according to standard protocols at each respective institution. Post-HCT relapse was defined as any morphologic, cytogenetic, or flow cytometry evidence of disease, at any detectable level in the bone marrow or at extra-medullary sites. A second hematologic malignancy without evidence of the original leukemia was not counted as a relapse. Neutrophil recovery was defined as the first of 3 consecutive days with an absolute neutrophil count (ANC) ≥ 0.5 × 109/L. Platelet recovery was defined by a count of at least 20 × 109/L, unsupported by transfusions, for seven days. Graft failure (GF) was defined as the failure to achieve an ANC of 0.5 × 109/L by day 28 and absence of donor-derived hematopoiesis (<5% donor cells). Complete donor chimerism was defined as the presence of over 95% donor-originated cells, and mixed chimerism as the detection of 5%–95% donor-derived cells. Acute and chronic graft vs. host disease (GvHD) were scored according to previous published criteria (10, 11). Cytomegalovirus (CMV) reactivation was diagnosed by viral PCR or antigenemia, depending on the available diagnostic methods at each institution. Patients who were at risk of CMV reactivation included those in whom either the patient or donor, or both, had tested positive for CMV IgG. Haploidentical transplantation was performed using the post-transplant cyclophosphamide platform.
The median follow-up time was calculated using the reverse Kaplan–Meier method. Estimates of neutrophil and platelet recovery and GF were calculated using cumulative incidence curves to accommodate competing risks. Death without hematological recovery was considered a competing risk for neutrophil and platelet recovery, whereas death with sustained engraftment was a competing risk for GF. Relapse and NRM, which are both competing risks, were evaluated by the Gray Test and Fine-Gray competing risk regression. The Gray test was used for univariable comparisons of cumulative incidence curves. The following covariates were considered for univariable analysis: age, gender, year of transplant, ABO incompatibility, type of leukemia, disease status, MRD pre HCT, donor age, donor type, stem cell source, conditioning, use of serotherapy (ATG or campath), gender mismatch, GVHD prophylaxis, CMV reactivation, and donor chimerism. The overall survival (OS) was calculated from the day of the transplant until the date of death or the last contact with the patient, and the disease-free survival (DFS) was calculated from the day of the transplant until the day of relapse or death in remission. The probabilities of disease-free survival (DFS) and overall survival (OS) were estimated using the Kaplan–Meier method and compared between groups using the log-rank test. Multivariable analyses for neutrophil and platelet recovery and GF were performed using Fine-Gray sub distribution hazard models, whereas multivariable analyses for DFS and OS were performed using Cox proportional hazards regression models. Covariates that reached a P value ≤ 0.1 in the univariable analyses were included in the initial multivariable models and were eliminated one at a time using the backward stepwise method. Only covariates that attained a P value ≤ 0.05 (Wald test) were held in the final adjusted models. Results are expressed as the hazard ratio (HR) or sub distribution hazard ratio (SHR) with a 95% confidence interval (95% CI). A 2-sided P value ≤ 0.05 was considered statistically significant. Statistical analysis was performed using EZR version 1.53 (Saitama Medical Centre, Jichi Medical University, Saitama, Japan (12).
Table 1 summarizes patients' and transplantation characteristics. Between January 2010 and December 2019, we analyzed 310 pediatric patients who underwent their first hematopoietic cell transplantation (HCT) for acute leukemia. Acute lymphoblastic leukemia (ALL) represented the primary indication (74.2%), followed by acute myeloid leukemia (AML; 25.8%). The study population had a median age of 9.52 years (range: 0.25–17.97), with male predominance (68.3%).
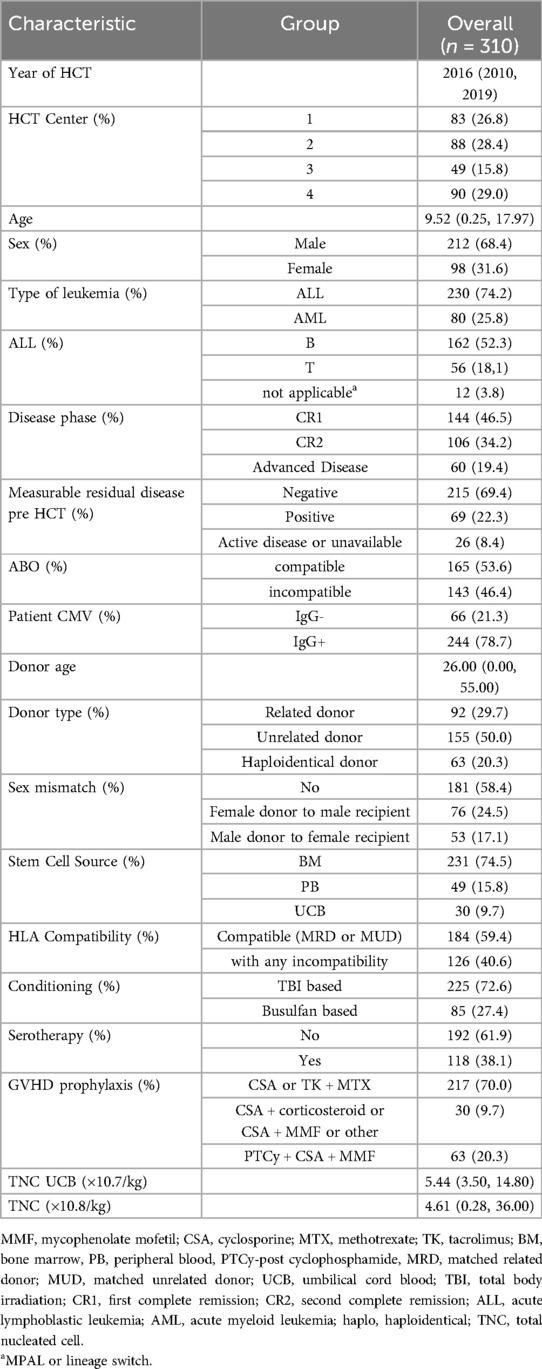
Table 1. Patients' and transplant characteristics.
Alternative donors were utilized in the majority of transplants (70.3%), with HLA compatibility achieved in 59.4% of cases. Bone marrow served as the predominant stem cell source (74.5%). Most recipients (94.8%; n = 294) were at risk for cytomegalovirus reactivation. The conditioning regimen consisted primarily of total body irradiation-based protocols (72.6%, TBI doses 1,200–1,440 rads), while busulfan-based regimens (doses 13–23 mg/kg) were used in the remaining patients (27.4%). Patients under 2 years of age (infant leukemia) received a modified conditioning regimen consisting of busulfan, fludarabine, and thiotepa, avoiding total body irradiation due to age-specific developmental considerations. Graft-vs.-host disease prophylaxis typically included a calcineurin inhibitor (cyclosporine or tacrolimus) combined with methotrexate (70%).
Regarding transplantation status, 46.5% of patients underwent the procedure while in first complete remission (CR1), and 69.4% had negative measurable residual disease analysis prior to HCT. Transplantation in CR1 was conducted in accordance with institutional protocols. Indications for CR1 transplantation were based on established high-risk features, including primary induction failure and adverse cytogenetic characteristics. Post-transplant relapse occurred in 36.7% of patients at a median of 245 days (range: 38–2,505). With a median follow-up of 2,019 days (5.5 years; 95% CI: 1,836–2,352), this cohort represents substantial longitudinal observation.
The cumulative incidence of relapse was 12.6% (95% CI: 9.2–16.5) at 100 days, increasing to 28.8% (95% CI: 23.8–33.9) at one year and 33.4% (95% CI: 28.2–38.7) at two years post-HCT. Time to relapse differed between acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML) patients, with median times of 167 days (range: 22–2,504) and 100 days (range: 16–1,428), respectively.
Univariate analysis (UVA) identified several factors associated with increased relapse risk: acute myeloid leukemia diagnosis, disease beyond first complete remission, positive minimal residual disease pre-HCT, and mixed donor chimerism at day +30 (Table 2). In multivariate analysis (MVA), mixed donor chimerism (HR 2.86, p = 0.047) and positive pre-HCT minimal residual disease (HR 2.26, p = 0.003) emerged as independent risk factors. Disease status beyond first complete remission showed a progressive increase in relapse risk, with hazard ratios of 2.39 (p = 0.0013) for second complete remission, 2.34 (p = 0.0026) for advanced disease, and 3.11 (p = 0.0006) for refractory disease (Table 3, Figure 1C).

Table 2. 1-year overall survival, disease-free survival, and relapse—univariate analysis.
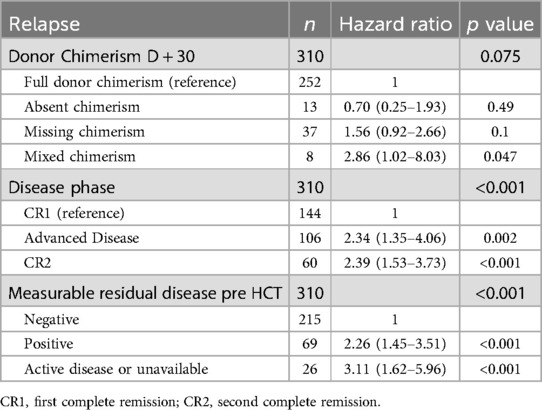
Table 3. Relapse—multivariate analyses.
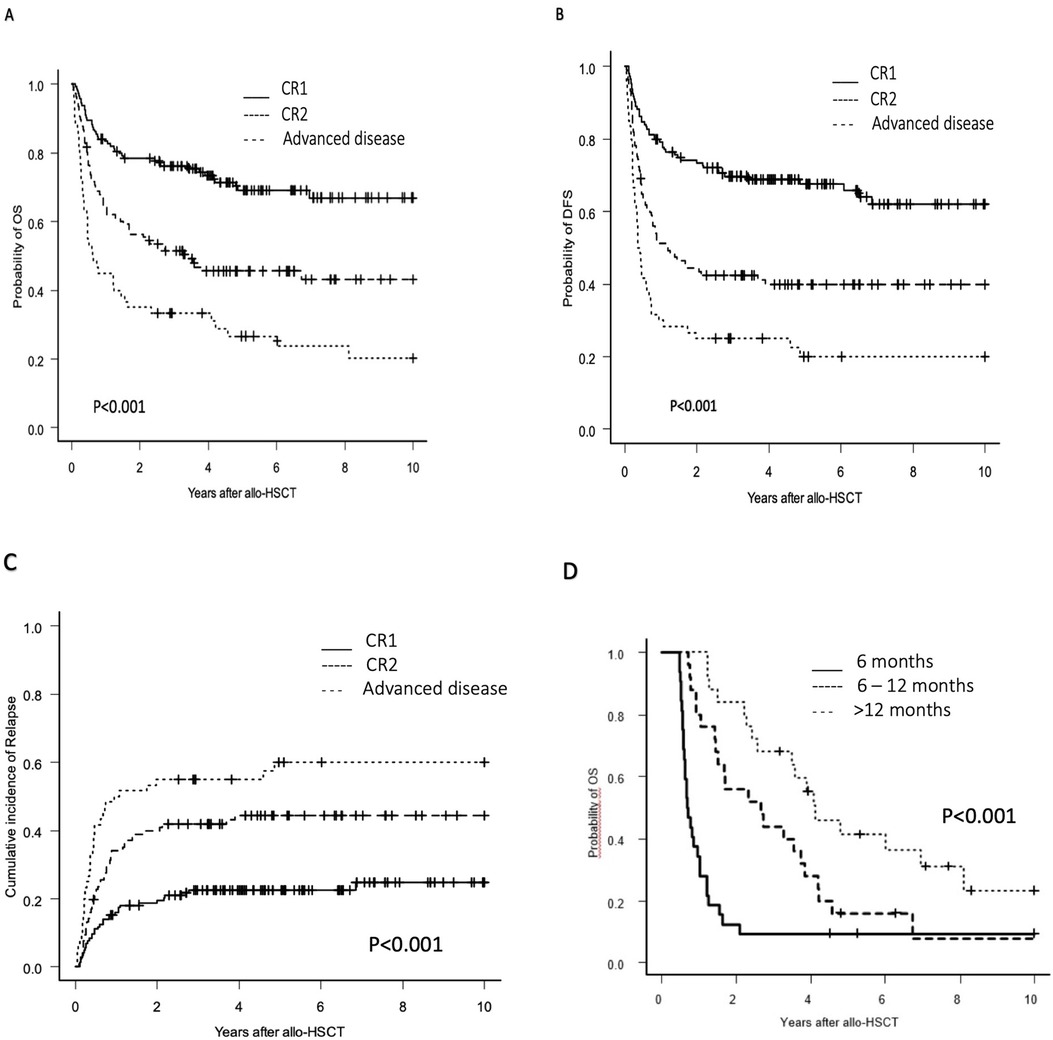
Figure 1. Overall survival, disease-free survival after HCT for pediatric patients with acute leukemias and incidence of relapse after HCT according to the disease phase and overall survival according to and time to relapse after transplant. (A) Probability of OS by disease phase, (B) Probability of DFS by disease phase, (C) Incidence of relapse by disease phase, (D) Probability of OS by time to relapse.
Treatment strategies for post-transplant relapse included chemotherapy and immunosuppression withdrawal, frequently combined with donor lymphocyte infusions or second transplantation. In our cohort of 29 patients who underwent second transplantation, 19 received the procedure specifically for relapse management, with a median interval of one year between transplants. Only 3 of the 19 patients transplanted for relapse achieved sustained remission and survival.
The estimated overall survival was 69.3% (95% CI: 63.8–74.1) at one year, 62.4% (95% CI: 56.7–67.5) at two years, and 52.7% (95% CI: 46.7–58.3) at five years post-HCT. UVA identified several favorable prognostic factors: first complete remission, negative minimal residual disease pre-HCT, ABO compatibility, bone marrow as stem cell source, and complete donor chimerism at day +30 (Table 2).
Due to violation of the proportional hazard assumption in the MVA, we performed a time-stratified analysis using a 365-day cutoff based on Schoenfeld residual assessment. In the early period (≤365 days), stem cell source emerged as the primary predictor of survival, with both peripheral blood (HR 2.23) and umbilical cord blood (HR 2.26) associated with increased mortality compared to bone marrow. Beyond 365 days, disease-related factors became predominant predictors of survival: second complete remission (HR 1.97), advanced disease (HR 3.18), and positive minimal residual disease pre-HCT (HR 3.12) were significantly associated with inferior outcomes (Table 4, Figures 1A,D).

Table 4. Overall survival before and after 365 days—multivariate analysis.
The cumulative incidence of graft failure remained stable at 4.8% (95% CI: 2.8%–7.6%) from 100 days through one year post-transplantation. Although initial analysis suggested higher rejection rates in patients with busulfan-based conditioning, umbilical cord blood transplantation, and acute myeloid leukemia diagnosis, MVA identified only two independent risk factors: busulfan-based conditioning (HR 4.64, p = 0.005) and umbilical cord blood as stem cell source (HR 13.47, p = 0.000005).
Disease-free survival demonstrated a gradual decline over time, with rates of 60.1% (95% CI: 54.4–65.3) at one year, 54.2% (95% CI: 48.4–59.5) at two years, and 48.8% (95% CI: 42.9–54.4) at five years post-transplantation. UVA identified several favorable prognostic factors (Table 2): first complete remission status (46% of patients), negative minimal residual disease pre-HCT (69.3% of patients), bone marrow as cell source (74.4% of patients), and complete donor chimerism (81.2% of patients). In MVA, mixed donor chimerism emerged as a significant risk factor for inferior disease-free survival (HR 2.73, p = 0.019) compared to complete donor chimerism. Additionally, disease status beyond first complete remission significantly impacted outcomes, with both second complete remission (HR 2.52, p < 0.0001) and advanced disease (HR 3.58, p < 0.0001) associated with lower disease-free survival rates (Figure 1B).
The cumulative incidence of acute graft-vs.-host disease (aGVHD) at day +100 was 35.0% (95% CI: 29.7%–40.3%) for grades II-IV and 14.3% (95% CI: 10.4%–18.9%) for grades III-IV. MVA identified unrelated donor transplantation as a significant risk factor, with 50% of these patients developing aGVHD (p = 0.0061).
The 2-year incidence of chronic GVHD was 23.0% (CI: 18,4%–27,8%), with severe cases accounting for only 5.4% (CI: 3.1%–8.7%). In the MVA, only age >10 years when compared to age <10 years, was a risk factor (47% of patients p 0.00007) for chronic GvHD.
The study recorded 145 deaths at a median of 105 days post-HCT (range: 16–1,778). Relapse constituted the predominant cause of mortality (n = 102). Among the 43 patients who died in remission, infection was the primary cause in 90.6% of cases, with 11 of these patients having concurrent chronic GVHD. Temporal analysis of mortality patterns revealed distinct trends: infection dominated early deaths (58% within first 100 days), while relapse emerged as the leading cause thereafter (65% beyond day 100).
The cumulative incidence of non-relapse mortality (NRM) showed a progressive increase from 6.8% (95% CI: 4.3–9.9) at 100 days to 11.9% (95% CI: 8.6–15.8) at one year, reaching 13.0% (95% CI: 9.8–17.3) at two years post-transplantation. UVA identified primary graft failure at day +30 (0.05% of patients, p = 0.003), haploidentical donors (20% of patients, p = 0.01), and umbilical cord blood as stem cell source (10% of patients, p = 0.001) as risk factors for increased NRM. MVA confirmed the independent impact of donor type and stem cell source on NRM: haploidentical donors (HR 4.00, p = 0.015), unrelated donors (HR 2.91, p = 0.026), and umbilical cord blood grafts (HR 3.5, p = 0.0012) were associated with significantly higher NRM rates.
Post-hematopoietic cell transplantation (HCT) relapse remains a significant challenge in pediatric acute leukemia treatment. Our study analyzed relapse rates and outcomes in a substantial cohort of pediatric patients, with particular emphasis on identifying critical factors that influence post-transplant success in resource-constrained settings. While post-HCT relapse is a global concern, data from Latin America and similar regions remain limited, creating a significant knowledge gap in understanding region-specific challenges and outcomes.
The relevance of this research is underscored by the high prevalence of acute leukemia in the pediatric population, with Brazil alone expecting approximately 11,000 new cases between 2023 and 2025. Understanding the patterns of post-HCT relapse and identifying both risk and protective factors is crucial for developing practical, resource-appropriate strategies for relapse prevention and management. This knowledge becomes particularly valuable for healthcare systems facing similar resource constraints, where optimizing available interventions can significantly impact patient outcomes (13).
In pediatric leukemia, post-HCT relapse rates demonstrate a strong correlation with disease status at the time of transplantation. While patients transplanted during first or second remission typically show more favorable outcomes, with reported rates between 23% and 30%, those undergoing transplantation with active disease face significantly poorer prognosis. Our findings align with these published data, underscoring the critical importance of achieving disease control prior to HCT (1, 2, 14–16).
The predictive value of minimal residual disease (MRD) for post-transplant relapse is well-documented (14, 17–19). Our findings reinforce the fundamental importance of achieving disease control before proceeding with HCT and highlight the need for standardized MRD assessment protocols (14, 20). A particular challenge emerges in resource-constrained healthcare systems where access to novel therapeutic agents that effectively achieve MRD negativity, such as blinatumomab and inotuzumab ozogamicin, remains restricted. In Brazil's public healthcare system (Sistema Único de Saúde, SUS), these agents are not currently available, and access is limited to patients with private health insurance coverage, who represent a minority of the Brazilian population. This disparity in access to novel therapies potentially compromises pre-transplant disease control for the majority of patients who rely on the public healthcare system (17).
Early withdrawal of immunosuppression (EWI) and donor lymphocyte infusions (DLI) were implemented as preventive strategies to enhance the graft-vs.-leukemia effect. While EWI was utilized in 58 patients, the concurrent use of multiple interventions and the retrospective nature of our study limited our ability to assess the individual effectiveness of these approaches. Although these strategies theoretically benefit patients with minimal disease burden, the optimal timing, dosing, and patient selection criteria remain challenging to establish. Furthermore, the potential benefits must be balanced against the risk of graft-vs.-host disease (4, 21).
Multiple studies have demonstrated varying outcomes with second hematopoietic cell transplantation as a therapeutic strategy for post-transplant relapse. While some reports show encouraging results, our experience aligns with retrospective studies showing more modest outcomes. The efficacy of this approach depends heavily on factors such as disease status at second transplant, time from first transplant to relapse, and donor availability, emphasizing the importance of careful patient selection (1, 22–24).
Our analysis demonstrates favorable post-transplant overall survival outcomes, aligned with contemporary literature. These results are comparable to those reported by Crotta, who observed rates of 77% and 60% at one and five years, respectively, and to Hoel's excellent outcomes for patients transplanted in complete remission (2, 7). Our findings also indicate significant progress in Brazilian transplant care when compared to the 45% three-year overall survival previously documented by Morando in 2010, likely reflecting improvements in supportive care and patient selection strategies (13) Disease status at transplantation and stem cell source emerged as critical determinants of outcomes. Our observation regarding the superiority of bone marrow transplantation, particularly within the first year post-transplant, corroborates Keesler's findings of improved outcomes with bone marrow grafts after six months post-procedure (25).
Disease-free survival analysis in our cohort identified mixed chimerism and primary graft failure as significant independent risk factors for inferior outcomes. Disease characteristics, including advanced disease status, second complete remission, and positive minimal residual disease pre-transplantation, demonstrated substantial impact on survival and relapse risk. These findings regarding disease-free survival align with previously published data in comparable populations, reinforcing the critical importance of disease control and successful engraftment in determining transplant outcomes (26, 27).
Non-relapse mortality in our cohort demonstrated favorable outcomes when compared to Wang and colleagues' findings (27). Our analysis identified donor type and stem cell source as significant determinants of transplant-related mortality. Specifically, haploidentical and unrelated donor transplants, as well as cord blood as a stem cell source, were associated with increased mortality risk. The higher mortality observed with cord blood transplantation may be attributed to an increased incidence of early rejection, potentially leading to greater susceptibility to infectious complications.
Our study's limitations stem from both methodological aspects and the complex healthcare landscape in Brazil. The country's continental dimensions and heterogeneous healthcare infrastructure create significant variability across leukemia treatment centers regarding diagnostic capabilities, treatment protocols, and timing of transplant referrals. This heterogeneity extends to transplant centers, where treatment options vary considerably between public and private healthcare systems, potentially influencing both pre- and post-transplantation care.
Additional limitations include the retrospective nature of our analysis, which inherently introduces potential biases in data collection and interpretation. The long study period may have encompassed evolution in supportive care practices and treatment strategies, potentially affecting outcomes across different time points. Furthermore, the assessment of minimal residual disease lacked standardization across centers, both in methodology and timing, which may impact the interpretation of this crucial prognostic factor. The evaluation of specific interventions, such as DLI and EWI, was challenging due to the variability in timing and dosing, as well as the concurrent use of multiple strategies. Additionally, our study's single-country focus, while providing valuable regional data, may limit the generalizability of findings to other healthcare settings with different resources and population characteristics.
Our study corroborates established risk factors for post-transplant relapse in pediatric acute leukemia while providing crucial data from the Brazilian healthcare context. Despite identifying previously known risk factors—advanced disease status, positive minimal residual disease pre-transplantation, and mixed donor chimerism—this analysis fills a significant knowledge gap regarding transplant outcomes in Latin American pediatric populations, where published data remains scarce. This regional perspective is particularly valuable given the unique challenges faced by emerging healthcare systems, including variable access to novel therapies and diagnostic tools.
The challenge of post-transplant relapse in resource-constrained settings highlights the importance of expanding access to novel therapies. While CAR-T cell therapy has emerged as a promising intervention for B-cell ALL relapse, its availability remains largely limited to the private healthcare sector in Brazil. Given the poor outcomes observed with second transplantation, developing academic CAR-T cell programs within the public healthcare system becomes imperative. Additionally, broader access to pre-transplant novel agents such as blinatumomab and inotuzumab could significantly improve disease control before transplantation.
Early infection-related mortality also warrants attention, particularly given the limited access to advanced antiviral medications like foscarnet and cidofovir in the public healthcare system. However, the primary focus remains on relapse prevention through improved early disease detection, timely transplant referral, and enhanced access to modern therapeutic protocols. These strategies, combined with standardized monitoring of minimal residual disease and chimerism, offer the most promising path toward improving long-term survival in pediatric acute leukemia patients undergoing transplantation.
Understanding transplant outcomes in our specific healthcare environment provides valuable insights for other regions facing similar resource constraints. This knowledge can guide the development of locally adapted strategies for relapse prevention and management, ultimately contributing to improved pediatric transplant outcomes across Latin America and other emerging healthcare systems.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was approved by the Institutional Review Boards of all participating centers. The requirement for informed consent was waived by the Ethics Committees of all participating institutions due to the retrospective nature of the study.
PP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. RT: Data curation, Formal analysis, Validation, Visualization, Writing – review & editing. AR: Formal analysis, Investigation, Writing – review & editing. GL: Conceptualization, Investigation, Validation, Visualization, Writing – review & editing. SN: Data curation, Validation, Writing – review & editing. CK: Conceptualization, Investigation, Validation, Visualization, Writing – review & editing. FB: Conceptualization, Investigation, Validation, Writing – review & editing. CP: Conceptualization, Formal analysis, Validation, Writing – review & editing. JB: Conceptualization, Investigation, Visualization, Writing – review & editing. JT: Conceptualization, Investigation, Validation, Writing – review & editing. LG: Conceptualization, Data curation, Investigation, Writing – review & editing. RM: Writing – review & editing. AK: Conceptualization, Data curation, Writing – review & editing. RG: Data curation, Writing – review & editing. MQ: Data curation, Writing – review & editing. SL: Data curation, Writing – review & editing. Vd: Data curation, Writing – review & editing. AA: Investigation, Validation, Writing – review & editing. MF: Conceptualization, Writing – review & editing. AL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors would like to thank all the nurses, physicians, and multidisciplinary staff at the participating centers. The authors also thank all oncologists and hematologists who collaborated with the transplant centers to provide the best possible treatment for each patient.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Dahlberg A, Leisenring W, Bleakley M, Meshinchi S, Baker KS, Summers C, et al. Prognosis of relapse after hematopoietic cell transplant (HCT) for treatment of leukemia or myelodysplastic syndrome (MDS) in children. Bone Marrow Transplant. (2019) 54(8):1337–45. doi: 10.1038/s41409-019-0438-z
2. Crotta A, Zhang J, Keir C. Survival after stem-cell transplant in pediatric and young-adult patients with relapsed and refractory B-cell acute lymphoblastic leukemia. Curr Med Res Opin. (2018) 34(3):435–40. doi: 10.1080/03007995.2017.1384373
3. Haugaard AK, Madsen HO, Marquart HV, Rosthøj S, Masmas TN, Heilmann C, et al. Highly sensitive chimerism detection in blood is associated with increased risk of relapse after allogeneic hematopoietic cell transplantation in childhood leukemia. Pediatr Transplant. (2019) 23(7):e13549. doi: 10.1111/petr.13549
4. Roux C, Tifratene K, Socie G, Galambrun C, Bertrand Y, Rialland F, et al. Outcome after failure of allogeneic hematopoietic stem cell transplantation in children with acute leukemia: a study by the société Francophone de greffe de moelle et de thérapie cellulaire (SFGM-TC). Bone Marrow Transplant. (2017) 52(5):678–82. doi: 10.1038/bmt.2016.360
5. Cusatis R, Litovich C, Feng Z, Allbee-Johnson M, Kapfhammer M, Mattila D, et al. Current trends and outcomes in cellular therapy activity in the United States, including prospective patient-reported outcomes data collection in the center for international blood and marrow transplant research registry. Transplant Cell Ther. (2024) 30(9):917.e1–917.e12. doi: 10.1016/j.jtct.2024.06.021
6. Simione AJ, da Silva CC, da Silva Sabaini PM, Macedo AV, das Neves HR, Geraldo BL, et al. Current use and outcomes of hematopoietic stem cell transplantation: Brazilian summary slides—2023. J Bone Marrow Transplant Cell Ther. (2023) 4(2):200. doi: 10.46765/2675-374X.2023v4n2p200
7. Hoell JI, Ginzel S, Kuhlen M, Kloetgen A, Gombert M, Fischer U, et al. Pediatric ALL relapses after allo-SCT show high individuality, clonal dynamics, selective pressure, and druggable targets. Blood Adv. (2019) 3(20):3143–56. doi: 10.1182/bloodadvances.2019000051
8. Puls ML, Silva RL, Fernandes PA, Leite LAC, Fabbron GG, Cavalcante JN, et al. Blinatumomab na leucemia linfoide aguda-b em contexto de pós-transplante de células tronco hematopoiéticas: experiência de dois serviços de referência. Hematol Transfus Cell Ther. (2022) 44:S193–4. doi: 10.1016/j.htct.2022.09.326
9. Pennesi E, Michels N, Brivio E, van der Velden VH, Jiang Y, Thano A, et al. Inotuzumab ozogamicin as single agent in pediatric patients with relapsed and refractory acute lymphoblastic leukemia: results from a phase II trial. Leukemia. (2022) 36(6):1516–24. doi: 10.1038/s41375-022-01576-3
10. Kitko CL, Pidala J, Schoemans HM, Lawitschka A, Flowers ME, Cowen EW, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: IIa. The 2020 clinical implementation and early diagnosis working group report. Transplant Cell Ther. (2021) 27(7):545–57. doi: 10.1016/j.jtct.2021.03.033
11. Jagasia MH, Greinix HT, Arora M, Williams KM, Wolff D, Cowen EW, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. The 2014 diagnosis and staging working group report. Biol Blood Marrow Transplant. (2015) 21(3):389–401.e1. doi: 10.1016/j.bbmt.2014.12.001
12. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. (2013) 48(3):452–8. doi: 10.1038/bmt.2012.244
13. Santos MDO, Lima FCDSD, Martins LFL, Oliveira JFP, Almeida LMD, Cancela MDC. Estimativa de incidência de câncer no Brasil, 2023-2025. Rev Bras Cancerol. (2023) 69(1):e-213700. Avaible at: https://rbc.inca.gov.br/index.php/revista/article/view/3700 (Accessed March 12, 2025)
14. Bar M, Wood BL, Radich JP, Doney KC, Woolfrey AE, Delaney C, et al. Impact of minimal residual disease, detected by flow cytometry, on outcome of myeloablative hematopoietic cell transplantation for acute lymphoblastic leukemia. Leuk Res Treat. (2014) 2014:1–9. doi: 10.1155/2014/421723
15. Willasch AM, Salzmann-Manrique E, Krenn T, Duerken M, Faber J, Opper J, et al. Treatment of relapse after allogeneic stem cell transplantation in children and adolescents with ALL: the Frankfurt experience. Bone Marrow Transplant. (2017) 52(2):201–8. doi: 10.1038/bmt.2016.224
16. Tavares RD, Bonfim CS, Seber A, Pereira Lermontov S, Coulturato V, Zecchin VG, et al. Hematopoietic cell transplantation in pediatric patients with acute leukemias or myelodysplastic syndrome using unrelated adult or umbilical cord blood donors in Brazil. Pediatr Transplant. (2020) 24(7):e13789. doi: 10.1111/petr.13789
17. Komitopoulou A, Baltadakis I, Peristeri I, Goussetis E. Immunotherapy and allogeneic bone marrow transplantation in B acute lymphoblastic leukemia: how to sequence? Clin Hematol Int. (2022) 4(1-2):11–20. doi: 10.1007/s44228-022-00006-6
18. Sutton R, Shaw PJ, Venn NC, Law T, Dissanayake A, Kilo T, et al. Persistent MRD before and after allogeneic BMT predicts relapse in children with acute lymphoblastic leukaemia. Br J Haematol. (2015) 168(3):395–404. doi: 10.1111/bjh.13142
19. Lamble A, Phelan R, Burke M. When less is good, is none better? The prognostic and therapeutic significance of peri-transplant minimal residual disease assessment in pediatric acute lymphoblastic leukemia. J Clin Med. (2017) 6(7):66. doi: 10.3390/jcm6070066
20. Ikoma-Colturato MR, Beltrame MP, Furtado FM, Pimenta G, Costa ESD, Azambuja AP, et al. Minimal residual disease assessment in acute lymphoblastic leukemia by 4-color flow cytometry: recommendations from the MRD working group of the Brazilian society of bone marrow transplantation. Hematol Transfus Cell Ther. (2021) 43(3):332–40. doi: 10.1016/j.htct.2020.09.148
21. Dominietto A, Piaggio G, Pozzi S, Bertolotti F, Colombo N, Grasso R, et al. Treatment of minimal residual disease (MRD) with donor lymphocyte infusions (DLI) in acute leukemia patients undergoing an allogeneic hemopoietic stem cell transplants (HSCT). Blood. (2005) 106(11):2012–2012. doi: 10.1182/blood.V106.11.2012.2012
22. Menon NN, Jenkins LM, Cui H, Jenkins C, Anwer F, Yeager AM, et al. Factors associated with improved outcomes after second allogeneic hematopoietic cell transplantation for relapsed pediatric leukemia. Ann Hematol. (2016) 95(4):637–44. doi: 10.1007/s00277-016-2599-9
23. Kishi K, Takahashi S, Gondo H, Shiobara S, Kanamaru A, Kato S, et al. Second allogeneic bone marrow transplantation for post-transplant leukemia relapse: results of a survey of 66 cases in 24 Japanese institutes. Bone Marrow Transplant. (1997) 19(5):461–6. doi: 10.1038/sj.bmt.1700680
24. Michallet M, Tanguy ML, Socié G, Thiébaut A, Belhabri A, Milpied N, et al. Second allogeneic haematopoietic stem cell transplantation in relapsed acute and chronic leukaemias for patients who underwent a first allogeneic bone marrow transplantation: a survey of the société française de greffe de moelle (SFGM): second allogeneic HSCT in relapsed acute and chronic leukaemias. Br J Haematol. (2000) 108(2):400–7. doi: 10.1046/j.1365-2141.2000.01851.x
25. Keesler DA, Martin A, Bonfim C, Seber A, Zhang MJ, Eapen M. Bone marrow versus peripheral blood from unrelated donors for children and adolescents with acute leukemia. Biol Blood Marrow Transplant. (2018) 24(12):2487–92. doi: 10.1016/j.bbmt.2018.08.010
26. Dalle JH, Balduzzi A, Bader P, Pieczonka A, Yaniv I, Lankester A, et al. The impact of donor type on the outcome of pediatric patients with very high risk acute lymphoblastic leukemia. A study of the ALL SCT 2003 BFM-SG and 2007-BFM-international SG. Bone Marrow Transplant. (2021) 56(1):257–66. doi: 10.1038/s41409-020-01014-x
Keywords: pediatric, ALL, AML, BMT, relapse
Citation: Pelegrina PRD, Tavares RdCB, Rodrigues AM, Loth G, Nichele S, Kuwahara C, Benini FMdeL, Peixoto CMA, Bach J, Trennepohl J, de Gouvea LMM, Muratori R, Koliski A, Gomes RT, Quiroga M, Lermontov SP, da Silva VG, de Azambuja AP, Feitosa MK, Lima ACM and Bonfim C (2025) Clinical outcomes and relapse patterns in pediatric acute leukemia patients undergoing hematopoietic cell transplantation: a multicenter Brazilian experience. Front. Pediatr. 13:1573334. doi: 10.3389/fped.2025.1573334
Received: 8 February 2025; Accepted: 6 March 2025;
Published: 20 March 2025.
Edited by:
Joanna Zawitkowska, Medical University of Lublin, PolandReviewed by:
Baheyeldin Salem, Baylor College of Medicine, United StatesCopyright: © 2025 Pelegrina, Tavares, Rodrigues, Loth, Nichele, Kuwahara, Benini, Peixoto, Bach, Trennepohl, de Gouvea, Muratori, Koliski, Gomes, Quiroga, Lermontov, da Silva, de Azambuja, Feitosa, Lima and Bonfim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Polliany Roberta Dorini Pelegrina, cG9sbGlhbnkucGVsZWdyaW5hQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.