
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 09 April 2025
Sec. Pediatric Gastroenterology, Hepatology and Nutrition
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1568174
This article is part of the Research TopicCeliac Disease In ChildrenView all 4 articles
 Duygu Demirtaş Güner1*†,‡
Duygu Demirtaş Güner1*†,‡ Kübra Baskın2,†,‡
Kübra Baskın2,†,‡
Introduction: Celiac disease (CD) and allergic diseases are immune-mediated disorders with overlapping clinical and immunologic features. The association between CD and selective immunoglobulin (Ig) A deficiency (sIgAD) is well-established, but limited data exist on the relationship between CD, other antibody deficiencies, and allergic diseases in children. This study aimed to evaluate the prevalence of allergic manifestations and immunologic abnormalities in children with CD.
Methods: This prospective study included children with biopsy-confirmed CD, followed at a gastroenterology clinic from August 2022 to February 2023. Participants underwent comprehensive immunologic and allergic evaluation, including serum immunoglobulin levels, vaccine antibody responses, lymphocyte subgroup analysis, and allergy testing as clinically indicated.
Results: The cohort included 76 patients with a median age of 11 years and a median age at CD diagnosis of 5.8 years. Allergic manifestations included aeroallergen sensitivity (22.4%), allergic rhinitis (15.8%), allergic conjunctivitis (13.2%), food allergy (5.3%), and asthma and eczema (3.9% each). Immunologic evaluations revealed normal profiles in 69.7% of patients, while abnormalities included partial IgM deficiency (6.6%), unclassified hypogammaglobulinemia (5.3%), sIgAD (2.6%), and transient hypogammaglobulinemia of infancy (2.6%). Elevated IgE levels were observed in 13.2% of patients.
Conclusion: This study highlighted a significant prevalence of allergic diseases and immunologic abnormalities in children with CD, extending beyond the commonly recognized association with sIgAD. These findings underscore the importance of comprehensive immunologic and allergic evaluation in children with CD.
Celiac disease (CD) is an immune-mediated enteropathy triggered by dietary gluten in genetically predisposed individuals. It affects 0.7%–1.4% of the population worldwide, with a higher prevalence in pediatric populations compared to adults (1).
The cornerstone of CD diagnosis relies on tissue transglutaminase immunoglobulin (Ig) A (TGA-IgA) testing, typically accompanied by total IgA measurement to identify selective IgA deficiency (sIgAD). This practice emerged from the well-documented association between CD and sIgAD, which occurs more frequently in patients with CD than in the general population (2–4). As a result, TGA-IgA levels may be low in patients with CD who also have sIgAD, which can complicate diagnosis. In cases of sIgAD, alternative testing using IgG-based assays becomes essential for accurate diagnosis. It is recommended to check for deamidated gliadin peptide IgG, tissue transglutaminase IgG, or anti-endomysial IgG in children with low total IgA levels (2).
Consequently, pediatric gastroenterologists routinely measure total IgA levels alongside TGA-IgA during screening or in suspected CD cases. However, other immunoglobulin levels are often overlooked, potentially leaving immunodeficiencies undiagnosed. For instance, common variable immunodeficiency (CVID) can present with gastrointestinal manifestations mimicking CD, including villous atrophy. Without comprehensive immunoglobulin evaluation, such cases might be misdiagnosed as seronegative CD (5, 6).
Beyond immunodeficiencies, recent evidence suggests that allergic conditions, including atopic dermatitis, allergic rhinitis, asthma, and food allergies, have an increased prevalence in patients with CD. This association suggests shared immune dysregulation mechanisms in CD and allergic diseases (7–10).
There is growing interest in understanding the potential relationships between CD, immunodeficiencies, and allergic diseases. While early identification of coexisting conditions can guide comprehensive management strategies, further studies are needed to clarify these associations (5, 9, 11).
This study aimed to characterize the immunologic and allergic profiles of children with CD, with particular attention to immunoglobulin levels, allergic sensitization, and immunodeficiencies beyond sIgAD.
This prospective cohort study was conducted at the pediatric gastroenterology clinic of Van Training and Research Hospital between August 21, 2022, and February 21, 2023. Children with biopsy-confirmed CD, diagnosed according to the Marsh-Oberhuber classification criteria, were enrolled.
Inclusion criteria were as follows: (a) Children aged 2–18 years. (b) Biopsy-confirmed CD diagnosis. (c) Informed consent obtained from parents/guardians.
Exclusion criteria were as follows: (a) Patients undergoing immunosuppressive therapy. (b) Patients with incomplete clinical or laboratory data. (c) Presence of other chronic diseases affecting immune function (e.g., primary immunodeficiencies). (d) Inability to complete study procedures.
Patients were referred to the pediatric allergy and immunology clinic for a comprehensive evaluation as part of the study protocol. Serum immunoglobulin levels (IgA, IgM, IgG, IgE) were measured using turbidimetric methods, with age-specific reference ranges applied. For patients with low immunoglobulin levels, a second measurement was performed at least one month later to confirm the diagnosis before classification. Patients with persistently low or abnormal immunoglobulin levels underwent further immunologic evaluation, including lymphocyte subset analysis (CD3+, CD4+, CD8+, CD19+, and CD16+/56+) (12). Vaccine antibody responses (anti-HBs and anti-rubella IgG) were assessed to evaluate immune function.
Patients were evaluated for gastrointestinal and allergic symptoms, including dysphagia and food impaction. However, routine endoscopic screening for eosinophilic esophagitis (EoE) was not performed.
Allergy testing included skin prick tests (SPTs) for common aeroallergens (e.g., pollen, house dust mites, grass pollens, molds, animal dander) and food allergens (e.g., milk, eggs, wheat). SPTs were performed using standardized allergen extracts, and a wheal diameter ≥3 mm greater than that of the negative control was considered positive. Respiratory function testing was performed for patients with respiratory symptoms.
Data were analyzed using SPSS for Windows, version 22.0. Continuous variables were expressed as medians with interquartile ranges (IQR), and categorical variables as counts and percentages. The normality of continuous variables was assessed using the Shapiro–Wilk test. Based on this assessment, appropriate statistical methods were applied: normally distributed data were analyzed using the Student's t-test, while non-normally distributed data were analyzed using the Mann–Whitney U-test. A p-value < 0.05 was considered statistically significant.
The study was approved by the Institutional Review Board of Van Training and Research Hospital (decision number: 2023/13–06), and written informed consent was obtained from all participants’ parents.
The study included 76 children diagnosed with CD [52 females (68.4%), 24 males (31.6%)], with a median age of 11 years (IQR 7.2–14.3) and a median age at diagnosis of 5.8 years (IQR 3.8–9.8). Parental consanguinity was present in 24 patients (31.6%), and 13 patients (17.1%) reported family history of atopy. During the study, 27 patients (35.5%) had negative TGA-IgA results, indicating that these patients had been adhering to a gluten-free diet (GFD), leading to serological normalization. In 28 patients (36.8%), TGA-IgA was positive but less than 10 times the upper limit of normal (ULN). In 19 patients (25%), TGA-IgA was greater than 10 times the ULN (≥200 RU/ml). Tissue transglutaminase IgA levels were missing in two patients.
None of the patients had symptoms suggestive of EoE, such as dysphagia or food impaction. Therefore, no additional endoscopic evaluation for EoE was performed. However, asymptomatic cases of EoE may have gone undetected.
Allergic diseases were prevalent among the patients. Allergic rhinitis was diagnosed in 15.8% of the cohort, while allergic conjunctivitis was observed in 13.2%. Food allergy or a history of food allergy was present in 5.3% of the patients, and asthma and eczema were diagnosed in 3.9% of the patients each. These findings are summarized in Table 1. Of the four patients with food allergy, one was allergic to milk, eggs, walnuts, and sesame; another had a history of egg and lamb allergy; a third had a history of milk and egg allergy; and the last patient had a history of peanut allergy.
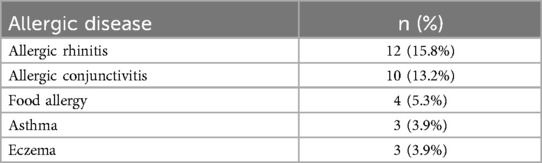
Table 1. Prevalence of allergic diseases accompanying celiac disease.
None of the patients had neutropenia or lymphopenia. Normal immunoglobulin levels and antibody responses were observed in 69.7% of the patients, while immunological abnormalities were identified in 30.3%. The most common abnormality was partial IgM deficiency, followed by unclassified hypogammaglobulinemia, sIgA deficiency, and a preliminary diagnosis of transient hypogammaglobulinemia of infancy. The latter was diagnosed in two patients (aged 2 and 4 years) based on low IgG levels, normal vaccine responses, absence of growth failure, and no evidence of T-cell defects, according to the clinical criteria of the European Society for Immunodeficiencies (ESID) Registry (13). None of the patients had a history of frequent infections. Elevated total IgE levels were observed in 13.2% of the patients.
Further details on the distribution of immunological abnormalities are summarized in Figure 1.
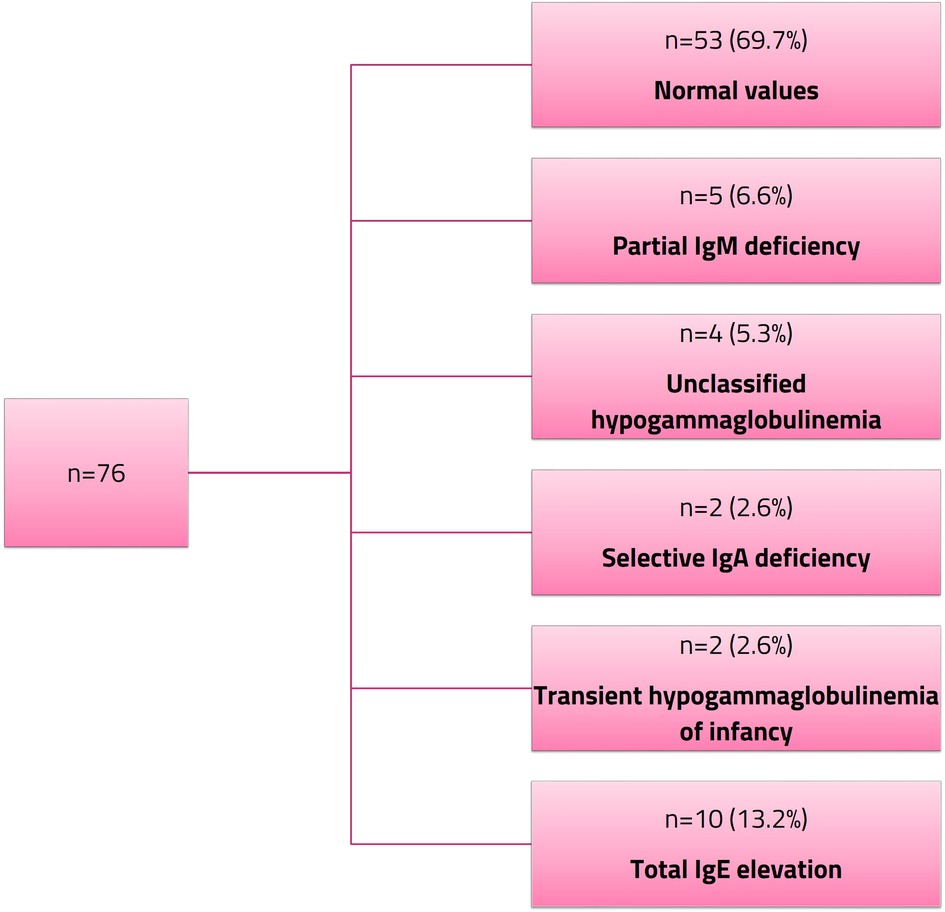
Figure 1. Immunological abnormalities in pediatric celiac disease.
The four patients with unclassified hypogammaglobulinemia underwent immunologic evaluation with simultaneous measurement of TGA-IgA levels at a median of 5.6 years after CD diagnosis. Two of these patients had negative TGA-IgA levels and were adherent to a GFD, while the other two had persistently elevated TGA-IgA levels due to nonadherence. Similarly, among patients with partial IgM deficiency, three had elevated TGA-IgA levels due to nonadherence to a GFD.
Our study highlights the association between CD, allergic diseases, and immunologic abnormalities in children. We identified allergic diseases such as allergic rhinitis, allergic conjunctivitis, food allergy, asthma, along with immunologic abnormalities including partial IgM deficiency, unclassified hypogammaglobulinemia, sIgAD, and a preliminary diagnosis of transient hypogammaglobulinemia of infancy. Importantly, these immunologic abnormalities extend beyond the commonly recognized sIgAD associated with CD, suggesting a broader spectrum of immune dysregulation may coexist with CD and contribute to immune dysfunction.
The link between CD and allergic diseases has been increasingly recognized, with studies suggesting that children with allergic rhinitis, allergic conjunctivitis, asthma, and atopic eczema have a higher risk of developing CD compared to the general population. One study demonstrated adjusted incidence rate ratios of 1.39 for allergic rhinitis/conjunctivitis, 1.44 for atopic eczema, and 1.41 for asthma in adults, highlighting the importance of considering CD screening in patients presenting with allergic symptoms (14). Our findings are consistent with previous studies and further support the clinical association between CD and allergic diseases. In our cohort, 22.4% of patients exhibited aeroallergen sensitivity, 15.8% had allergic rhinitis, 13.2% had allergic conjunctivitis, 3.9% had asthma, and 3.9% had eczema. Additionally, elevated IgE levels were observed in 13.2% of our patients, particularly among those with allergic conditions such as eczema and asthma, supporting the hypothesis of immune dysregulation in CD. A study involving 2,297 individuals found a higher prevalence of IgE sensitization to specific allergens such as wheat, house dust mites, and food allergens in patients with CD (9).
IgE-mediated food hypersensitivity is relatively common among children with CD. One study reported that 50% of children with CD had a positive SPT for at least one food allergen, with peanuts being the most commonly identified sensitization (8). In our cohort, food allergy was documented in 5.3% of patients, with allergen profiles indicating sensitivity to milk, egg, nuts, sesame, and meat (lamb).
The relationship between CD and severe food allergy, defined as high IgE levels combined with a history of severe allergic reactions, has been investigated. One study found that children with severe food allergy had a higher prevalence of CD compared to those with mild allergy or the general population, particularly in the presence of elevated IgE levels (15). Although severe food allergy was not identified in our study, the elevated IgE levels in patients with allergic diseases underscores the complex interplay between CD and allergic sensitization. These findings highlight the importance of screening for CD in children with allergic profiles, even in the absence of severe food allergies. Similarly, screening for allergies in children diagnosed with CD is essential to ensure comprehensive management and address any coexisting allergic conditions.
Increased intestinal permeability in CD, which may increase antigen exposure and promote subsequent allergic sensitization, has been proposed as a potential mechanism underlying the overlap between celiac disease and allergic diseases (9, 15). Additionally, mast cells have been implicated in CD pathogenesis, suggesting another potential mechanism that warrants further investigation (16). Although our study did not directly evaluate these mechanisms, future research is needed to better understand the immunologic interplay between CD and allergic diseases.
It is important to note that immunodeficiencies such as CVID, sIgAD, and IgM deficiencies can present with gastrointestinal symptoms that mimic those of CD, thereby complicating its diagnosis. When coexisting with CD, these immunodeficiencies may lead to false-negative serological results due to insufficient immunoglobulin production (5). This underscores the need for pediatric gastroenterologists to extend their immunological assessments beyond IgA levels, particularly in patients with refractory symptoms despite adherence to a GFD.
Adherence to a GFD is crucial for intestinal mucosal healing, which facilitates the normalization of immunoglobulin levels by improving nutrient absorption and supporting immune function (17, 18). However, persistent immunoglobulin abnormalities despite strict GFD adherence may indicate the presence of primary immunodeficiencies, such as selective IgM deficiency (sIgMD), which require ongoing monitoring and treatment (19).
In our study, partial IgM deficiency and unclassified hypogammaglobulinemia were identified in 11.8% of patients, suggesting a potential role in immune dysregulation in CD. Notably, these abnormalities were observed in both GFD-adherent and non-adherent patients, suggesting that immune dysfunction in CD may not be solely attributed to gluten exposure or intestinal inflammation but may also involve an underlying immunologic component. Non-adherent patients with persistently elevated TGA-IgA levels may develop secondary hypogammaglobulinemia due to ongoing intestinal inflammation. However, the persistence of immunoglobulin deficiencies despite strict dietary adherence suggests an underlying primary immunodeficiency, warranting further investigation. Regular monitoring of dietary adherence is essential in patients with CD, particularly those with coexisting immunologic abnormalities, as continued gluten exposure may exacerbate both gastrointestinal symptoms and immune dysfunction.
Even with strict adherence to a GFD, some patients with CD may continue to experience gastrointestinal symptoms due to coexisting food allergies. For instance, a case report described a 13.5-year-old girl with persistent symptoms despite strict GFD adherence who was diagnosed with a non-IgE-mediated soy allergy that resolved following soy elimination (20). This case highlights the need to consider additional food allergies in children with CD who have refractory symptoms. In our cohort, 5.3% of patients had documented food allergies, emphasizing the necessity of comprehensive allergen screening and management to optimize outcomes.
This study had several strengths that enhance the validity and reliability of our findings. First, its prospective design enabled systematic and standardized data collection. Second, the inclusion of only biopsy-confirmed CD cases ensured diagnostic accuracy. Third, the comprehensive immunological evaluation, including the assessment of all immunoglobulin classes and vaccine responses, provides novel insights beyond the typical focus on IgA levels. Additionally, the use of both clinical assessments and objective testing for allergic conditions strengthens the reliability of our findings.
Despite some limitations, including being conducted at a single center with a relatively small sample size, our results may have limited generalizability to the broader pediatric CD population. Moreover, the absence of a control group restricted our ability to compare the prevalence of immunologic and allergic abnormalities with the general population. Additionally, due to the short study duration, we were unable to reassess immunoglobulin levels after TGA-IgA normalization in some patients, leaving uncertainty about whether these abnormalities resolve with strict dietary adherence.
In conclusion, our findings suggested that CD may be part of a broader spectrum of immune dysregulation, encompassing allergic and immunologic components. The overlap between CD, allergic diseases, and immunologic abnormalities highlighted the importance of comprehensive immunological and allergic evaluations in children with CD, ensuring early detection and management to optimize care and improve outcomes.
Our study underscored the need for an integrated, multidisciplinary approach to managing children with CD, addressing the complex interplay of immune dysregulation and allergic manifestations associated with this condition.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Committee of Van Training and Research Hospital (2023/13-06). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
DD: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. KB: Investigation, Methodology, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that Generative AI was used in the creation of this manuscript. The authors used ChatGPT (OpenAI, GPT-4, January 2025 version) for language editing and improving the clarity of the manuscript. The authors are fully responsible for the accuracy of the content.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Singh P, Arora A, Strand TA, Leffler DA, Catassi C, Green PH, et al. Global prevalence of celiac disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol. (2018) 16(6):823–36.e2. doi: 10.1016/j.cgh.2017.06.037
2. Husby S, Koletzko S, Korponay-Szabó I, Kurppa K, Mearin ML, Ribes-Koninckx C, et al. European Society paediatric gastroenterology, hepatology and nutrition guidelines for diagnosing coeliac disease 2020. J Pediatr Gastroenterol Nutr. (2020) 70(1):141–56. doi: 10.1097/MPG.0000000000002497
3. Mearin ML, Agardh D, Antunes H, Al-Toma A, Auricchio R, Castillejo G, et al. ESPGHAN Position paper on management and follow-up of children and adolescents with celiac disease. J Pediatr Gastroenterol Nutr. (2022) 75(3):369–86. doi: 10.1097/MPG.0000000000003540
4. Wang N, Shen N, Vyse TJ, Anand V, Gunnarson I, Sturfelt G, et al. Selective IgA deficiency in autoimmune diseases. Mol Med. (2011) 17(11-12):1383–96. doi: 10.2119/molmed.2011.00195
5. Giorgio F, Principi M, Losurdo G, Piscitelli D, Iannone A, Barone M, et al. Seronegative celiac disease and immunoglobulin deficiency: where to Look in the submerged iceberg? Nutrients. (2015) 7(9):7486–504. doi: 10.3390/nu7095350
6. Jørgensen SF, Reims HM, Frydenlund D, Holm K, Paulsen V, Michelsen AE, et al. A cross-sectional study of the prevalence of gastrointestinal symptoms and pathology in patients with common variable immunodeficiency. Am J Gastroenterol. (2016) 111(10):1467–75. doi: 10.1038/ajg.2016.329
7. Cudowska B, Lebensztejn DM. Immunogloboulin E-mediated food sensitization in children with celiac disease: a single-center experience. Pediatr Gastroenterol Hepatol Nutr. (2021) 24(5):492–9. doi: 10.5223/pghn.2021.24.5.492
8. Jafari A, Kayvanloo S, Moazzen N, Motevalli Haghi N, Sedghi N, Khoshkhui M, et al. Prevalence of IgE-mediated food hypersensitivity to cereals and beans based on skin prick test in children with celiac disease. Middle East J Dig Dis. (2021) 13(4):339–42. doi: 10.34172/mejdd.2021.244
9. Kårhus LL, Skaaby T, Madsen AL, Thuesen BH, Schwarz P, Rumessen JJ, et al. The association of celiac disease and allergic disease in a general adult population. United European Gastroenterol J. (2019) 7(1):78–89. doi: 10.1177/2050640618811485
10. Khalighi M, Javaherizadeh H, Hakimzadeh M, Ahmadi M, Torabizadeh M, Fayezi A. Ige to wheat, prick test, and patch test among children with celiac disease. BMC Pediatr. (2024) 24(1):367. doi: 10.1186/s12887-024-04844-6
11. Sahin Y. Celiac disease in children: a review of the literature. World J Clin Pediatr. (2021) 10(4):53–71. doi: 10.5409/wjcp.v10.i4.53
12. Tezcan I, Berkel AI, Ersoy F, Sanal O. Sağlıklı Türk çocukları ve erişkinlerde turbidimetrik yöntemle bakılan serum immunoglobulin düzeyleri. Çocuk Sağlığı ve Hastalıkları Dergisi. (1996) 39:649–56.
13. Seidel MG, Kindle G, Gathmann B, Quinti I, Buckland M, van Montfrans J, et al. The European Society for Immunodeficiencies (ESID) registry working definitions for the clinical diagnosis of inborn errors of immunity. J Allergy Clin Immunol Pract. (2019) 7(6):1763–70. doi: 10.1016/j.jaip.2019.02.004
14. Krishna MT, Subramanian A, Adderley NJ, Zemedikun DT, Gkoutos GV, Nirantharakumar K. Allergic diseases and long-term risk of autoimmune disorders: longitudinal cohort study and cluster analysis. Eur Respir J. (2019) 54(5):1900476. doi: 10.1183/13993003.00476-2019
15. Pillon R, Ziberna F, Badina L, Ventura A, Longo G, Quaglia S, et al. Prevalence of celiac disease in patients with severe food allergy. Allergy. (2015) 70(10):1346–9. doi: 10.1111/all.12692
16. Struffert M, Maier C, Neid M, Schäfer HL, Tannapfel A, Schmidt-Choudhury A. Duodenal mast cells and eosinophils in children with celiac disease: occurrence and distribution pattern. Scand J Gastroenterol. (2022) 57(1):22–30. doi: 10.1080/00365521.2021.1985601
17. Magen E, Feldman V, Joseph M, Israel H. Symptomatic secondary selective IgM immunodeficiency in adult man with undiagnosed celiac disease. Case Reports Immunol. (2012) 2012:684247. doi: 10.1155/2012/684247
18. Montenegro L, Piscitelli D, Giorgio F, Covelli C, Fiore MG, Losurdo G, et al. Reversal of IgM deficiency following a gluten-free diet in seronegative celiac disease. World J Gastroenterol. (2014) 20(46):17686–9. doi: 10.3748/wjg.v20.i46.17686
19. Arani MH, Razavizadeh M, ArefNezhad R, Motedayyen H. Selective immunoglobulin M deficiency in a patient with celiac disease and recurrent pneumonia. Clin Case Rep. (2021) 9(1):158–63. doi: 10.1002/ccr3.3489
Keywords: allergy, antibody deficiency, celiac disease, children, immunodeficiency, immune dysregulation
Citation: Demirtaş Güner D and Baskın K (2025) Allergic and immunologic evaluation of children with celiac disease. Front. Pediatr. 13:1568174. doi: 10.3389/fped.2025.1568174
Received: 28 January 2025; Accepted: 24 March 2025;
Published: 9 April 2025.
Edited by:
Yasin Sahin, Gaziantep Islam Science and Technology University, TürkiyeReviewed by:
Marisa Gallant Stahl, University of Colorado, United StatesCopyright: © 2025 Demirtaş Güner and Baskın. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Duygu Demirtaş Güner, ZHV5Z3VkZW1pcnRhc0BnbWFpbC5jb20=
†Present Addresses: Duygu Demirtaş Güner, Department of Pediatric Gastroenterology, Hepatology and Nutrition, Dr. Behçet Uz Children's Hospital, Izmir, Türkiye
Kübra Baskın, Department of Pediatric Allergy and Immunology, Gazi University, Ankara, Türkiye
‡ORCID:
Duygu Demirtaş Güner
orcid.org/0000-0002-3662-4355
Kübra Baskın
orcid.org/0000-0002-4294-7492
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.