
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 27 March 2025
Sec. Pediatric Cardiology
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1555982
This article is part of the Research TopicSurgical and Non-Surgical Intervention of Congenital Heart Disease Management in Developing and Developed CountriesView all 10 articles
 Yuxian Xia1,†
Yuxian Xia1,† Rui Yang2,†Yuemeng Zhang2Di Yin2
Rui Yang2,†Yuemeng Zhang2Di Yin2 Wen Zhang1
Wen Zhang1 Qi Jiang1
Qi Jiang1 Yifan Zhu1Haibo Zhang1
Yifan Zhu1Haibo Zhang1 Renjie Hu1*
Renjie Hu1* Wei Dong1*
Wei Dong1*
Background: This study aimed to explore family management style (FMS) after palliative surgery in children with complex congenital heart disease (CCHD) and evaluate its influence on their outcomes.
Methods: A cross-sectional survey was conducted among 252 families of children with CCHD who underwent palliative surgery at our center. The Family Management Measure was used to investigate their FMS, and the outcomes with different FMSs were analyzed. Cluster analysis was employed to classify the FMSs into distinct groups.
Results: The cluster analysis identified four FMSs, namely, the Active and Collaborative (Cluster 1, 29.37%), the Chaotic and Nervous (Cluster 2, 10.71%), the Confident and Caring (Cluster 3, 22.22%), and the Laissez-Faire style (Cluster 4, 37.70%). Children in Cluster 1 demonstrated the highest quality of life, while those in Cluster 2 had the lowest (73.93 ± 12.71 and 59.03 ± 18.70, P < 0.01). The unplanned readmission rates were significantly higher in Clusters 2 and 4 (18.52% and 22.11%) compared to Clusters 1 and 3 (4.05% and 3.57%, P < 0.01).
Conclusion: The findings highlight the significant influence of FMS on the outcomes of children with CCHD following palliative surgery. The children in Cluster 1 exhibited the most favorable quality of life, whereas those in Cluster 2 had the worst. Health professionals should implement interventions to optimize FMS.
Congenital heart disease (CHD) is the most prevalent group of congenital anomalies worldwide, diagnosed in approximately 1% of live births (1). China is no exception, as CHD is the leading cause of neonatal impairment and mortality in the country. Infants with complex defects often require multiple stages of palliative and corrective surgeries early in life, followed by extended hospitalizations in the cardiac intensive care unit (CICU). Children born with complex congenital heart disease (CCHD) are particularly medically fragile and require intensive medical monitoring after discharge. They frequently experience feeding difficulties and growth delays and remain at risk for congestive heart failure (2).
The families of children with CCHD must adapt to postoperative caregiving and manage their children's condition in the long term, as their children often require palliative surgeries to alleviate clinical symptoms and prolong life. Their complex condition cannot be fully corrected anatomically or relieved in a single visit (3). Compared to radical surgery for simple CHD, children undergoing palliative procedures are more prone to unexpected complications due to hemodynamic abnormalities caused by non-anatomical correction (4).
An increasing body of literature indicates that postoperative care for children following palliative surgery for CCHD is suboptimal. Delayed growth and unplanned readmission rates are increasing (5). In addition, mortality rates can reach up to 10%–15% after certain palliative surgeries (4). Moreover, postoperative care for children with CCHD remains a challenging process for most parents, as these families often face significant ongoing pressure in China (6). Therefore, it is essential for healthcare professionals to support these families in developing comprehensive care plans and to help them maintain an active role in the long-term care of their children.
The Family Management Style Framework (FMSF) identifies how families organize, integrate, and carry out family-related tasks when managing chronic health conditions in children (7). A qualitative study explored the potential practical and research implications of the FMSF for children with CHD and demonstrated how family management style (FMS) dynamically influences children's health outcomes over time (8). In addition, their findings suggested that higher survival rates were associated with parents who exhibited a thriving FMS, held more positive attitudes toward their children's condition, and were more confident in managing their children's care regimen (8). Therefore, we aimed to conduct a large-scale quantitative study to quantify the impact of FMS on the outcomes of children with CCHD who underwent palliative surgeries. This study sought to extend our understanding of the application of FMS in this population and provide concrete evidence to inform postoperative care strategies for these children.
The families of children with CCHD who underwent palliative surgeries at Shanghai Children's Medical Center from 1 January 2016 to 31 August 2021 and who signed the consent form to take part in this study were recruited.
Inclusion criteria: (1) the palliative surgeries must have been performed within the last 5 years; (2) the caregivers must be the child's parents; (3) the parents must be able to communicate accurately and freely; (4) the parents must have agreed to participate in the study.
Exclusion criteria: (1) children born prematurely; (2) children with chromosomal abnormalities; (3) children with serious postoperative complications requiring long-term medical intervention.
The general information was collected through surveys. Diagnoses were classified as either single ventricular malformation or biventricular malformation. In addition, data on the children's family location, family economic status, and parents’ education and occupation were collected.
Cardiac function assessment during follow-up was performed on all children using the New York Heart Association (NYHA) cardiac function grade (9), which is divided into grades I–IV.
A nutritional status assessment was conducted using weight-for-age Z-score (WAZ) and body mass index (BMI)-for-age. WAZ was used to evaluate the nutritional status of children younger than 2 years old, with a score of less than -2 indicating a risk of malnutrition. BMI-for-age was utilized to assess the nutritional status of children older than 2 years old, with a BMI percentile less than 5% indicating malnutrition.
The Family Management Measure (FaMM) was initially developed by Knafl in 2006 based on the FMSF (7). The Chinese version of the FaMM was translated by Ying Zhang and her colleagues using the Likert 5-point scale, demonstrating good reliability and validity (10). The scale consists of 53 items across six dimensions. These include three positive dimensions: the Children's Daily Life (CDL) subscale, Condition Management Ability (CMA) subscale, and Parental Mutuality (PM) subscale. Higher scores in these dimensions indicate better family management. In addition, there are three negative dimensions: the View of Condition Impact (VCI) subscale, Family Life Difficulty (FLD) subscale, and Condition Management Effort (CME) subscale. Higher scores in these dimensions indicate poorer family management. The Cronbach’α for each subscale ranges from 0.70 to 0.84, and the content validity index (CVI) is 0.84 (10, 11).
Pediatric Quality of Life (PedsQLMT) is a measurement scale developed by Professor Upton to quantify children's quality of life (12), including two parts, the Child Self-Assessment Questionnaire and the Caregiver Report Questionnaire. This study used a Chinese version of the universal core PedsQLMT4.0 Caregiver Report Questionnaire, which has a reliability ranging from 0.74 to 0.90 (13). The questionnaire includes 23 items across four dimensions: physical functioning, emotional functioning, social functioning, and school functioning. Each item requires participants to recall how often an event occurred in the previous month, and responses are scored using a 5-point Likert scale. A higher score indicates a better quality of life (13).
The socioeconomic status (SES) index was used to measure parents’ occupational prestige and SES. The calculation formula is as follows: SES Index = 11.808 + 3.349 × (average years of education) + 0.573 × (average monthly income in 100 yuan) + 16.075 × (maximum managers) + 11.262 × (middle managers) + 3.738 × (grassroots managers) + 8.942 × (Party and government agencies) + 6.841 × (institutions) − 5.694 × (business units) − 26.655 × (discriminated occupations).
Descriptive statistics were reported as mean (standard deviation) or median [interquartile range (IQR)] for continuous variables and as percentages or frequencies for categorical variables.
A cluster analysis method was employed to identify different family management styles based on the FaMM dimension scores involving three steps. First, a cluster analysis, involving systematic clustering that determined the number of possible clusters according to the pedigree and inter-group connection. Second, K-means cluster, an iterative partitioning method, was performed to identify the best clustering results so that each cluster must contain at least 5% of the entire sample. Third, one-way analysis of variance (ANOVA) and a post-hoc test (Bonferroni test) were then used to test the differences in subscales between each cluster.
Differences in continuous or categorical variables across family management styles were assessed by ANOVA or chi-square tests, and the corresponding X2, F, and P-values are reported in the tables. A P-value <0.05 (two-tailed) was considered statistically significant. All statistical analyses were performed using SPSS 19.0.
A total of 269 families of children with CCHD within 5 years after palliative surgery were followed up in this study, and 252 families completed the questionnaire. The effective response rate was 93.68%, indicating that the results were representative of the target population. The median age of the children at surgery was 2.44 years (IQR: 0.71–6.99 years), the median follow-up age was 4.18 years (IQR: 2.38–8.71 years), the median CICU stay duration was 3.81 days (IQR: 2.00–6.72 days), and the median ventilation time was 26.68 h (IQR: 8.51–79.27 h).
The cluster analysis identified common characteristics within groups by measuring a predefined set of variables (the mean scores of each FaMM subscale). Consequently, the label assigned to each group reflected its typical characteristics. The clustering process was guided by the following principles: appropriate sample size, best interpretability within each cluster, F-values, and one-way ANOVA results. Based on these criteria, the included families were divided into four distinct family management styles (four clusters).
These four clusters were characterized as Active and Collaborative (Cluster 1), Chaotic and Nervous (Cluster 2), Confident and Caring (Cluster 3), and Laissez-Faire style (Cluster 4). Detailed descriptions of these clusters are provided in Table 1.
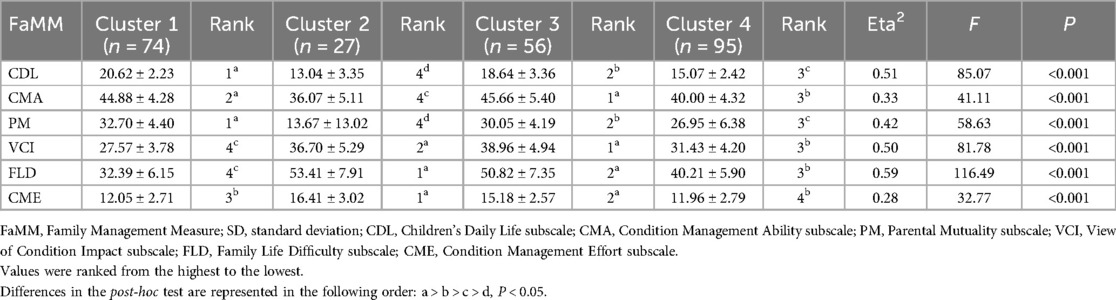
Table 1. Mean scores of six FaMM dimensions in the four clusters (mean ± SD).
This cluster accounted for 29.37% (n = 74) of the sample. In this cluster, the CDL and PM subscales had the highest scores, while the two negative dimensions, VCI and FLD, had the lowest scores. The parents in this cluster demonstrated a natural acceptance of their children's condition. Despite their children having CCHD requiring palliative surgery, they were able to effectively manage both the children and the disease across various aspects of family life.
This cluster accounted for 10.71% (n = 27). In this cluster, the scores for FLD and CME were the highest, while the scores for the three positive dimensions (CDL, CMA, and PM) were the lowest. The parents in this cluster struggled to address their children's conditions calmly and exhibited excessive worry. Most of the parents in this cluster lacked confidence in overcoming challenges and managing their children's conditions, leading to significant consumption of energy and time. In addition, mutual support between the parents was notably lower compared to the other three clusters. Many of the parents in this cluster experienced dissatisfaction or conflict and demonstrated neither the ability nor the intention to understand the medical issues related to their children.
This cluster accounted for 22.22% (n = 56). In this cluster, CMA and VCI scored the highest. The parents in this cluster were capable of caring for their children but expressed concerns about the disease's impact on their children and families.
This cluster accounted for 37.70% (n = 95). In this cluster, the score of CME ranked lowest, while VCI and FLD were also low. Parents in this cluster invested the least amount of energy, and the scores for the three positive dimensions were significantly lower than those in Clusters 1 and 3 (P < 0.05).
There were no significant differences in gender, nutritional status, times of surgery, family location, and paternal SES index distribution among the four clusters (P > 0.05). However, significant differences were observed in the distributions of children's age, cardiac function grade, diagnosis, time from surgery to follow-up, and maternal SES index (all P < 0.05) across the four clusters (Table 2).
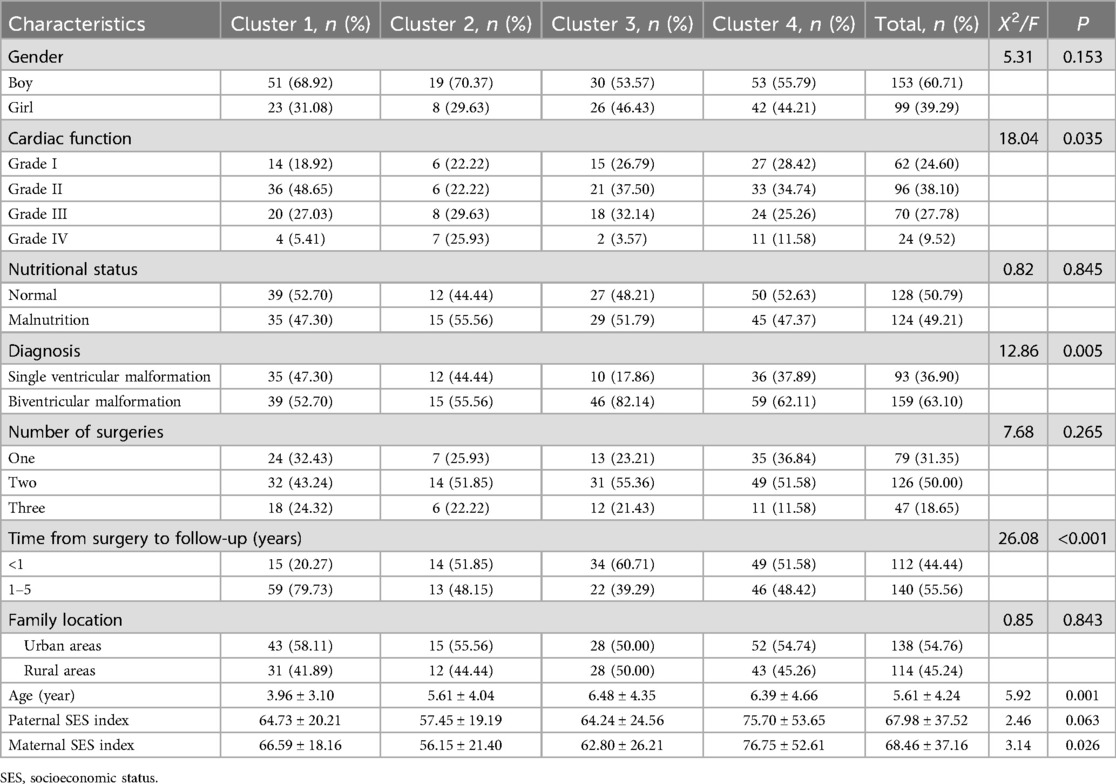
Table 2. The characteristics of the children and families in the four clusters.
In Cluster 1, the children were the youngest, and the proportion of children who were 1–5 years post-surgery was the highest. In Cluster 2, the proportion of children with cardiac function grade IV was the highest (25.93%), and the maternal SES index was the lowest. In Cluster 3, the proportion of children with biventricular malformation was the highest. In Cluster 4, both the paternal and maternal SES indexes were the highest among the clusters.
Table 3 presents the PedsQLMT4.0 scores across the different clusters. Cluster 1 had the highest overall score and Cluster 2 had the lowest overall score. Furthermore, Cluster 2 scored the lowest in all dimensions and was significantly lower than the other three clusters in emotional, social, and school functioning. The differences were statistically significant (P < 0.05).
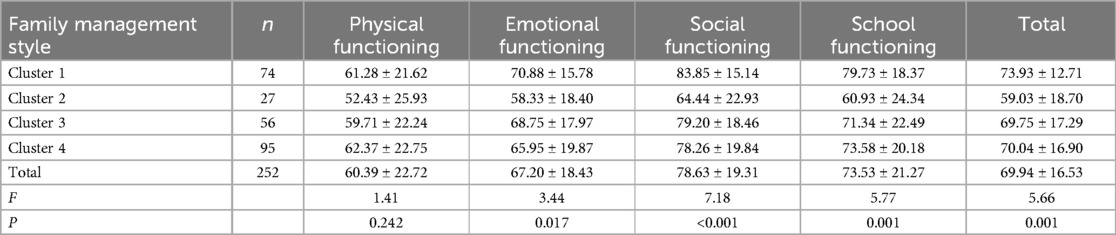
Table 3. Scores of each dimension of PedsQLMT4.0 in the four clusters.
Table 4 presents the unplanned readmission rates of children across the four clusters. The results of this study showed that the children's quality of life in families in Cluster 1 was the best, while that in Cluster 2 was the worst (P = 0.001).
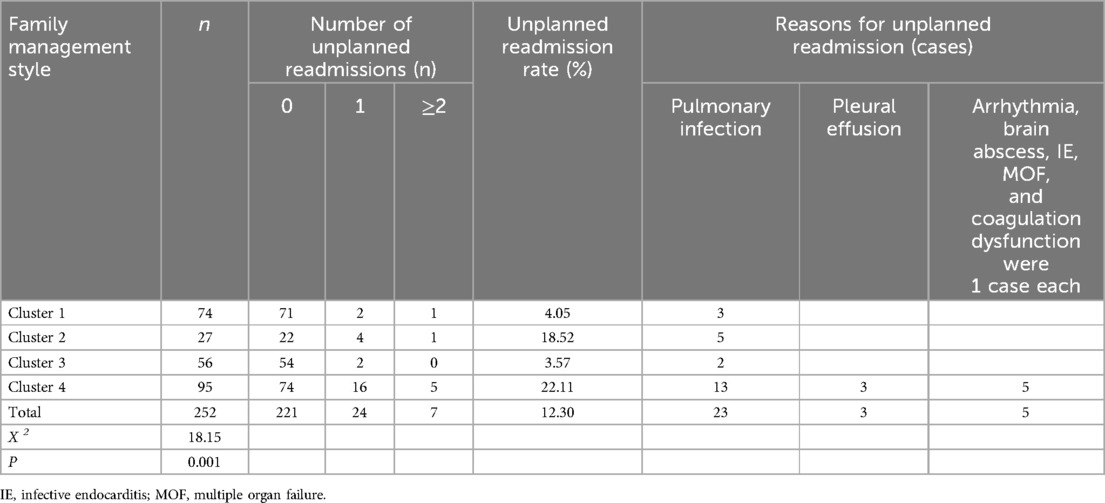
Table 4. Comparison of unplanned readmissions of the children in the four clusters.
In addition, there were five unplanned readmissions (18.52%) in Cluster 2 due to pulmonary infection, and one child (3.70%) was readmitted twice, Furthermore, parents with the Laissez-Faire style (Cluster 4) had the highest rate of unplanned readmissions. Among the 21 unplanned readmissions in Cluster 4, 13 (61.90%) had pulmonary infection, 3 (14.29%) had pleural effusion, and 5 (23.81%) experienced serious complications such as arrhythmia, infectious endocarditis, and multiple organ failure.
Compared with a domestic multi-center study on children with other chronic diseases (urinary system, endocrine system, rheumatic, and genetic diseases) (10) (Table 5), the parents of children with CCHD reported similar levels of difficulty in condition management (P = 0.473). However, they spent less effort on condition management and demonstrated significantly weaker mutual support (P < 0.001).
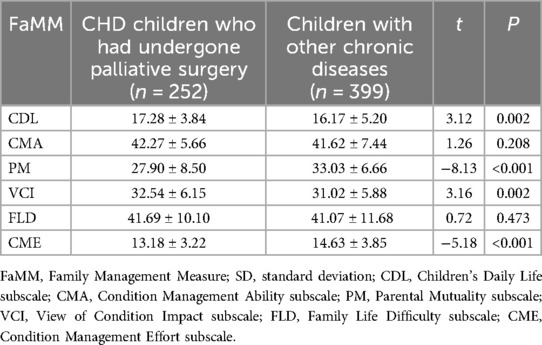
Table 5. Mean scores of the six FaMM subscales in different children (mean ± SD).
This study conducted a questionnaire-based investigation of FMS following palliative surgery in children with CCHD. Through cluster analysis, we identified four distinct FMS subtypes. The results revealed that Cluster 1 exhibited the most favorable quality of life, whereas Cluster 2 had the worst. Notably, Clusters 2 and 4 demonstrated significantly higher rates of unplanned readmissions compared to Clusters 1 and 3. Multivariate analysis revealed several potential determinants influencing FMS patterns, including children's age, cardiac function classification, diagnosis, time from surgery to follow-up, and maternal SES index.
FMS captures the nuances of how parents manage the care of their children, offering medical staff insights into how these care plans are woven into the fabric of daily family life. It also sheds light on parents’ perceptions of their children, their own management abilities, and overall family dynamics. Recognizing the variations in FMS among families of children with CCHD post-palliative surgery is crucial for facilitating effective communication and delivering tailored support and interventions.
Among the four clusters examined, FLD exhibited the highest variability (Eta2 = 0.59), indicating significant differences in how parents care for children with CCHD. It is widely acknowledged that complex congenital heart palliative surgeries carry a more intricate prognosis compared to straightforward corrective surgeries, along with a higher risk of severe complications, such as renal failure, hemothorax, thrombosis, cerebrovascular accident, multiple organ failure, and the need for additional reoperations. Furthermore, frequent clinical interventions and repeated hospitalizations add to the already substantial burden on these families. Over time, as families gain experience in long-term caregiving, many families have progressively enhanced their ability to navigate these challenges. Thus, the proportion of postoperative time between 1 and 5 years in the Active and Collaborative style cluster (Cluster 1) was the highest (59 cases, 79.73%) among the four clusters.
CDL and PM were two significant positive dimensions in determining the classification of the clusters, highlighting that parents held markedly different perspectives on what constitutes a “normal” daily life for their children. Moreover, the level of mutual support between parents in caring for their children with CCHD varied significantly across the four clusters. PM was found to be positively correlated with CDL and CMA (9). This suggested that promoting effective communication and support between parents could positively influence both the child's daily life and the family's ability to manage the condition. Furthermore, enhancing CMA and reducing the level of FLD could also help reduce CME.
In Chaotic and Nervous families (Cluster 2), the SES index of parents was the lowest among the four family types, and the proportion of children with cardiac function grade IV was the highest (seven cases, 25.93%). Children in these families often received fragmented and passive care, with poor care coordination and limited family participation (14). These families frequently faced insurmountable challenges, which eroded the parents’ confidence in managing their children's conditions. Therefore, clinical staff should prioritize support for these families by understanding the difficulties they encounter in home care, regularly tracking and monitoring their disease management progress, and providing timely support and help. For families with a low SES index, clinical staff can facilitate connections to available community health and/or financial support. Currently, our heart center has expanded its network of regional medical centers to better serve economically disadvantaged families of patients with CHD in remote areas, ensuring they receive the care and support they need.
In addition, compared to a cross-sectional study (15.9%) (15), the children in Clusters 2 and 4 had a significantly higher unplanned readmission rate. This underscores the critical impact of insufficient attention to postoperative care, including infection prevention, feeding, and follow-up, which can lead to various adverse outcomes. Therefore, it is important for healthcare workers to provide adequate disease health education and regular assessment of children in the families with Chaotic and Nervous (Cluster 2) and Laissez-Faire styles (Cluster 4).
Last but not least, we compared the families of children with CCHD to those of children with other chronic diseases. Table 5 shows that families of children with CCHD were more concerned about their children's prognosis compared to families of children with other chronic illnesses. Moreover, the level of mutual support among these families was far weaker than in families of children with other chronic illnesses. Therefore, our findings highlight the need for a centered, multi-team intervention approach to enhance mutual support among families of children with CCHD.
First, the FaMM data were collected from only one parent and the results were based on their subjective perceptions. This may cause bias to some extent, as some findings might reflect the perspectives of the adult completing the survey rather than the cardiac problems. Second, this study only conducted a cross-sectional survey of the status of FMS without long-term follow-up. A longitudinal study will be needed to assess the stability of FMS and its relation to readmission and control for confounders, including the severity of disease and success of the surgery. In the future, we will implement an evaluation study to examine different interventions, including the standard of care, and long-term outcomes of children with CCHD.
The novel contribution of the study lies in the different FMSs after palliative surgery in families of children with CCHD. These varying styles reflected diverse care priorities and characteristics across different families. An effective FMS has been shown to positively influence the outcomes of children. Therefore, health managers should implement family-centered interventions and guide families in adopting an effective FMS to improve the outcomes of children with CCHD.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the Ethics Committee of Shanghai Children's Medical Center, School of Medicine, Shanghai Jiao Tong University (Shanghai, China). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
YX: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. RY: Conceptualization, Data curation, Investigation, Writing – original draft. YuZ: Data curation, Methodology, Writing – original draft. DY: Conceptualization, Data curation, Formal analysis, Investigation, Resources, Writing – original draft. WZ: Investigation, Project administration, Resources, Supervision, Writing – review & editing. QJ: Conceptualization, Data curation, Methodology, Project administration, Writing – original draft. YiZ: Investigation, Methodology, Validation, Writing – original draft. HZ: Project administration, Resources, Supervision, Validation, Writing – review & editing. RH: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. WD: Conceptualization, Formal analysis, Project administration, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Key Area Project of the ‘Undergraduate Innovation Training Program’ at Shanghai Jiao Tong University School of Medicine (Grant No. 1824401Z).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sjostrom-Strand A, Terp K. Parents’ experiences of having a baby with a congenital heart defect and the child’s heart surgery. Compr Child Adolesc Nurs. (2019) 42(1):10–23. doi: 10.1080/24694193.2017.1342104
2. Medoff-Cooper B, Naim M, Torowicz D, Mott A. Feeding, growth, and nutrition in children with congenitally malformed hearts. Cardiol Young. (2010) 0(0):149–53. doi: 10.1017/S1047951110001228
3. Tak YR, McCubbin M. Family stress, perceived social support and coping following the diagnosis of a child’s congenital heart disease. J Adv Nurs. (2002) 39(2):190–8. doi: 10.1046/j.1365-2648.2002.02259.x
4. Keizman E, Tejman-Yarden S, Mishali D, Levine S, Borik S, Pollak U, et al. The bilateral bidirectional Glenn operation as a risk factor prior to Fontan completion in complex congenital heart disease patients. World J Pediatr Congenit Heart Surg. (2019) 10(2):174–81. doi: 10.1177/2150135118819997
5. O’Byrne ML, McBride MG, Paridon S, Goldmuntz E. Association of habitual activity and body mass index in survivors of congenital heart surgery: a study of children and adolescents with tetralogy of Fallot, transposition of the great arteries, and Fontan palliation. World J Pediatr Congenit Heart Surg. (2018) 9(2):177–84. doi: 10.1177/2150135117752122
6. Ni ZH, Lv HT, Ding S, Yao WY. Home care experience and nursing needs of caregivers of children undergoing congenital heart disease operations: a qualitative descriptive study. PLoS One. (2019) 14(3):e0213154. doi: 10.1371/journal.pone.0213154
7. Beacham BL, Deatrick JA. Adapting the family management styles framework to include children. J Pediatr Nurs. (2019) 45(0):26–36. doi: 10.1016/j.pedn.2018.12.006
8. Rempel GR, Blythe C, Rogers LG, Ravindran V. The process of family management when a baby is diagnosed with a lethal congenital condition. J Fam Nurs. (2012) 18(1):35–64. doi: 10.1177/1074840711427143
9. Ponikowski P, Voors A, Anker S, Bueno H, Cleland J, Coats A, et al. 2016 Esc Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. (2016) 37:2129–200. doi: 10.1093/eurheartj/ehw128
10. Sheng N, Ma J, Ding W, Zhang Y. Family management affecting transition readiness and quality of life of Chinese children and young people with chronic diseases. J Child Health Care. (2018) 22(3):470–85. doi: 10.1177/1367493517753712
11. Ma J, Yu Q, Zhang T, Zhang Y. Chinese Family care patterns of childhood rheumatic diseases: a cluster analysis. Int J Nurs Sci. (2019) 7(1):41–8. doi: 10.1016/j.ijnss.2019.11.005
12. Upton P, Maddocks A, Eiser C, Barnes P, Williams J. Development of a measure of the health-related quality of life of children in public care. Child Care Health Dev. (2005) 31(4):409–15. doi: 10.1111/j.1365-2214.2005.00520.x
13. Ding Y, Wang J, Zhou Y, et al. Quality of life in children with tuberous sclerosis complex: a pediatric cohort study. CNS Neurosci Ther. (2021) 27(3):280–8. doi: 10.1111/cns.13473
14. Mazwi M L, Henner N, Kirsch R. The role of palliative care in critical congenital heart disease. Semin Perinatol. (2017) 41(2):128–32. doi: 10.1053/j.semperi.2016.11.006
Keywords: congenital heart disease, palliative surgery, family management styles, pediatric quality of life, surgical outcome
Citation: Xia Y, Yang R, Zhang Y, Yin D, Zhang W, Jiang Q, Zhu Y, Zhang H, Hu R and Dong W (2025) Effect of family management styles on the outcomes of children with complex congenital heart disease after palliative surgery. Front. Pediatr. 13:1555982. doi: 10.3389/fped.2025.1555982
Received: 6 January 2025; Accepted: 12 March 2025;
Published: 27 March 2025.
Edited by:
Inga Voges, University Medical Center Schleswig-Holstein, GermanyReviewed by:
Silvio Fabio Torres, Austral University, ArgentinaCopyright: © 2025 Xia, Yang, Zhang, Yin, Zhang, Jiang, Zhu, Zhang, Hu and Dong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Renjie Hu, aHVyZW5qaWUxOTg4QGhvdG1haWwuY29t; Wei Dong, ZHJ3ZWlkb25nQDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.