
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pediatr., 15 April 2025
Sec. Pediatric Critical Care
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1544404
This article is part of the Research TopicAdvances in Pediatric Rehabilitation Clinical Trials: Design, Methods, and AnalysisView all 8 articles
 Lexi Petruccelli1
Lexi Petruccelli1 Kristen R. Miller2
Kristen R. Miller2 Rachel Greer1Heidi Sauceda1R. Scott Watson3,4Peter M. Mourani5
Rachel Greer1Heidi Sauceda1R. Scott Watson3,4Peter M. Mourani5 Aline B. Maddux6,7*
Aline B. Maddux6,7*
Introduction: Mobile monitoring devices offer an opportunity to characterize physical health recovery in children who survive critical illness.
Methods: To validate the BioIntelliSense BioButton® as a pediatric activity monitor, we studied healthy children (2–17 years-old) who wore the BioButton® device and an ActiGraph wGT3X-BT accelerometer, and a study team member documented activity in 1 min intervals (gold standard) during 45 min of scripted activities. In two-thirds of the cohort (derivation cohort), we identified BioButton activity count thresholds to differentiate activity levels based on highest Youden indices. Thresholds were applied to the remainder of the cohort (validation cohort) to determine sensitivity and specificity [95% confidence interval (CI)]. We also evaluated BioButton activity designations compared with accelerometer designations and calculated agreement between BioButton-measured body position and the activity log.
Results: Forty-five participants provided a median 43 (IQR 41, 44) analyzable minutes. Sensitivity and specificity of derived BioButton thresholds were 0.78 (95% CI: 0.69, 0.88) and 0.95 (95% CI: 0.90, 0.97) to identify moderate or vigorous activity (MVPA) and 0.91 (95% CI: 0.87, 0.95) and 0.98 (95% CI: 0.98, 0.98) to identify sedentary behavior. Sensitivity and specificity compared with the accelerometer were 0.52 (95% CI: 0.45–0.60) and 0.88 (95% CI: (95% CI: 0.84, 0.93) to identify MVPA and 0.92 (95% CI: 0.89–0.96) and 0.70 (95% CI: 0.67, 0.73) to identify sedentary behavior. The BioButton accurately identified position during 1,125 of 1,432 (78.6%) minutes.
Discussion: The BioButton device accurately identified physical activity and body position in children and may be a useful tool to quantify physical activity as an outcome in future trials.
In 2019, an estimated 239,000 U.S. children were admitted to an intensive care unit (1). Although more than 97% of children survived, there is growing recognition that survivors of critical illness can suffer from long-lasting impairments associated with their critical illness (2). Notably, critical illness puts children at risk of prolonged impairments in physical functioning. In a prospective study of 144 children who were mechanically ventilated for at least 3 days, one in five children had persistently worse physical health-related quality of life (HRQL) relative to their pre-admission state that persisted for at least one year after discharge (3). Other studies demonstrated similar or higher rates of physical impairments after pediatric critical illness (4–6). Impairments in physical activity are critically important because prolonged impairment in physical functioning may limit a child's ability to participate in activities that foster physical, social, and cognitive development, decreasing the likelihood of maintaining a healthy lifestyle in adulthood.
As the focus on survivorship has increased, core outcome sets were developed to guide evaluation of critically ill children. Across all outcome sets, physical activity is identified as a critically important outcome (7–9). The measures used to evaluate physical activity are primarily survey-based and, while patient- and proxy-reported outcomes such as HRQL offer valuable insight into a patient's or caregiver's perception of their or their child's health, direct measurements offer complimentary information, providing a more comprehensive understanding of a patient's recovery (10–12). Additionally, in contrast to direct measurements of functional abilities that can be measured in the clinic setting (e.g., six-minute walk test), functional outcomes such as physical activity are best evaluated in a child's natural setting to incorporate the context of everyday living.
The rapid development of mobile technologies provides an opportunity to augment measurement of physical health outcomes in children (13–15). Activity monitors have been used in other domains of pediatric research to evaluate physical health (16–18), but their use to measure physical recovery after a critical illness is limited (19). To ensure feasibility for use in studies evaluating children who survive a critical illness, the activity monitor must be acceptable to wear, and participation should be facilitated remotely given the challenges of in-person contact with study participants after discharge. We previously used the ActiGraph accelerometer (Pensacola, Florida USA), worn on hip (<6 years old) and wrist (≥6 years old), to evaluate physical activity in children who survived an episode of acute respiratory failure (19). The study's impact was limited by missing data because of reluctance to wear the monitor due to discomfort and visibility. In this study, we assessed the BioIntelliSense BioButton® (Golden, Colorado USA) as an alternative device to measure activity in children. The BioButton® is a 1.5 inch-diameter device that is worn directly on the skin and uses accelerometer technology to measure activity. The BioButton received 510(k) clearance by the U.S. Food and Drug Administration (FDA) in December of 2022 and is available for use in pediatric research as a non-significant risk device (20). It has been used to monitor adults during and after hospitalization but has not been used clinically in children (21). The primary objective of this study was to evaluate the accuracy of the BioIntelliSense BioButton® device to characterize physical activity in children relative to direct observation and, as a secondary objective, we compared physical activity level as characterized by the BioButton to the ActiGraph wGT3X-BT accelerometer. We hypothesized that the BioIntelliSense BioButton® device accurately characterizes moderate or vigorous physical activity (MVPA) and sedentary behavior.
This study was approved by the Colorado Multiple Institutional Review Board (Protocol: #22-2214, Physical Activity Monitor Validation) on February 06, 2023, and the study was conducted in accordance with institutional standards and the 1975 Helsinki Declaration. Consent was obtained from each participant's legal guardian, and child assent was obtained in children 7 years and older. Participants were healthy volunteers recruited through advertisements in Children's Hospital Colorado research newsletters. We included children (age 2 to 17) who were ambulatory (defined as able to walk and run independently) and able to engage in age-appropriate activities. We excluded children with chest burns or wounds that would preclude placement of the BioButton device, those who were in state custody, or if they resided in juvenile detention or jail. Enrollment was stratified by age group [>2 to <6 years-old [early childhood], ≥6 to <12 years-old [middle childhood], and ≥12 to <17 years-old [adolescence]]. We enrolled healthy participants to facilitate the ability to directly monitor activity in a prescribed setting which would not have been feasible if we enrolled children who had survived critical illness and, although the amount of activity may differ, we anticipated activity monitors would perform similarly in healthy children and those surviving critical illness. We evaluated for eligibility using a pre-eligibility survey administered by telephone to the participants' parent or legal guardian.
Study participants engaged in directed activities including sedentary behavior and light, moderate, or vigorous activity for a total duration of approximately 45 min (Supplementary eTable S1) (22). During the activities, each participant wore the BioIntelliSense BioButton device, adhered to the left side of their chest, and the ActiGraph accelerometer on their waist (<6-years-old) or wrist (≥6-years-old) (23, 24). In older children, wrist-worn accelerometers provide comparable data and increase wear time as compared to hip accelerometers (25–28). In younger children, hip worn accelerometers are shown to be well tolerated (29). We used previously reported thresholds to characterize activity as sedentary behavior or light, moderate, or vigorous activity based on vector magnitude data reported by the ActiGraph wGT3X-BT accelerometer (23, 24). The BioButton and ActiGraph accelerometer use triaxial accelerometer technology to measure activity defined as activity counts for the BioButton and vector magnitudes for the ActiGraph accelerometer. The BioButton also detects body position and classifies it as supine, prone, lateral, or upright (sitting or standing). A study team member assigned to each participant documented activity, activity level, and position in 1 min intervals in the participant's activity log. At the end of the 45 min activity period, surveys were distributed to families to evaluate receptivity of participants in using the devices (Supplementary eTable S2). The study was conducted at a local park over the course of five days during the summer months under similar weather conditions.
Variables were summarized as median and interquartile range (IQR) or frequency and percentage. To determine BioButton thresholds to characterize activity level in children, the cohort was divided into derivation and validation cohorts. Data from the derivation cohort identified optimal BioButton activity count thresholds to differentiate between the four different levels of activity (sedentary, light, moderate, and vigorous) as compared with the activity log, considered to be the gold standard. Receiver operating characteristic (ROC) curves were created for each pairwise activity level, as recorded by the activity log: (1) sedentary vs. light, (2) light vs. moderate, (3) moderate vs. vigorous. The optimal cutpoint between each level was chosen as the activity count with the highest Youden index (sensitivity + specificity −1) to optimize sensitivity and specificity. We calculated sensitivity and specificity of the thresholds to identify MVPA and sedentary behavior across the derivation cohort and validation cohort, using the activity log as the gold standard. This was repeated within each age group. Due to the clustered nature of the repeated measures on a single child, the ratio estimator for the variance of clustered binary data was used to calculate the confidence intervals of sensitivity and specificity (30, 31). As a secondary comparison, we evaluated the BioButton-derived activity level with the activity level characterized by the ActiGraph accelerometer in the full study cohort. To evaluate accuracy of the BioButton device to characterize body position, data from all participants were used to assess the percent agreement between body position designations by the BioButton device and the activity log. Sensitivity and specificity for correctly identifying body position were also reported. Missing data were not imputed. Statistical analyses were conducting using R version 4.2.2 (Vienna, Austria).
We enrolled 45 children, 28 in the derivation cohort and 17 in the validation cohort. Participants were divided into the validation and derivation cohorts based on timing of participation in the study. Patient characteristics were similar between the derivation and validation cohorts, and there were at least 5 participants evaluated in each age group in both the derivation and validation cohorts (Table 1). Study activities were conducted outdoors over 5 days between July and September of 2023. On the study days, daily high temperatures ranged from 80 to 88 degrees Fahrenheit. Participants engaged in study activities for a median of 46 min (IQR 45, 49) and participants had a median of 43 (IQR 41, 44) analyzable minutes with BioButton, ActiGraph accelerometer, and activity log information.
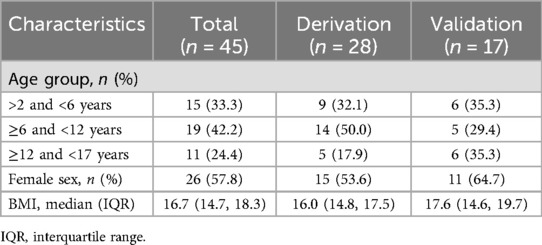
Table 1. Study cohort.
We used data from the derivation cohort to identify optimal activity count thresholds measured by the BioButton to identify sedentary behavior and light, moderate, and vigorous activity based on activity log data (Supplementary eTable S3). In the derivation subset of the cohort, sensitivity for identifying MVPA was 0.76 (95% CI: 0.69, 0.82) and specificity was 0.91 (95% CI: 0.89, 0.94) (Table 2). Across the three age groups, sensitivity values were greater than 0.75 with exception of the ≥12 year-old age group [0.63 (95% CI: 0.45, 0.80)], and specificities were greater than 0.9. Sensitivity of the BioButton device for identifying sedentary behavior was 0.88 (95% CI: 0.85, 0.91), and specificity was 0.93 (95% CI: 0.91, 0.95). Subsequently, we tested these thresholds in the validation cohort. Sensitivity for identifying MVPA was 0.78 (95% CI: 0.69, 0.88), and specificity was 0.95 (95% CI: 0.90, 0.97). Similar sensitivities and specificities were demonstrated across the three age groups (Table 3). Sensitivity of the BioButton for identifying sedentary behavior was 0.91 (95% CI: 0.87, 0.95) and specificity was 0.98 (95% CI: 0.98, 0.98) with similar performance across the three age groups (Table 2).
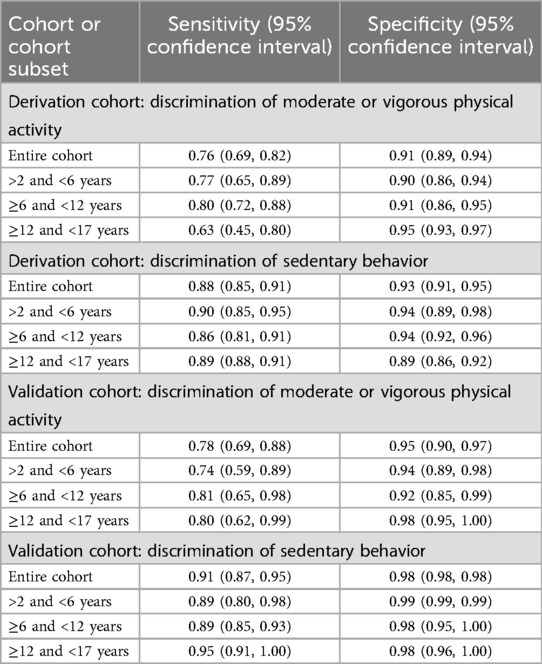
Table 2. Discrimination values of the bioButton compared with the activity Log: derivation cohort.
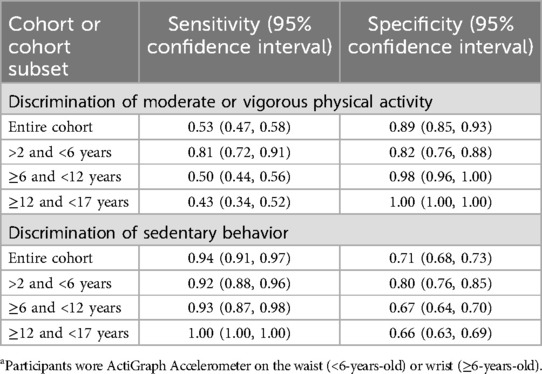
Table 3. Discrimination values of the bioButton compared with the actiGraph accelerometera.
We compared the activity level identified by the BioButton with the activity level identified by the ActiGraph accelerometer as a secondary gold standard (Table 3). Compared with the ActiGraph accelerometer, the BioButton demonstrated a sensitivity of 0.52 (95% CI: 0.45, 0.60) and specificity of 0.88 (95% CI: 0.84, 0.93) in identifying MVPA. Sensitivities were lower in older age groups, but specificities were similar. Compared with the ActiGraph accelerometer, the BioButton demonstrated a sensitivity of 0.92 (95% CI: 0.89, 0.96) and specificity of 0.70 (95% CI: 0.67, 0.73) in identifying sedentary behavior. Performance was similar across the three age groups.
To evaluate accuracy of the BioButton to identify body position, we analyzed 1,432 min. Of these 1,432 min, the device accurately identified participant position during 1,125 (78.6%) minutes (Supplementary eTable S4). Of the 947 min of upright positioning (sitting and standing), the BioButton device accurately identified 861 (90.9%) minutes as upright (Supplementary eTable S4). Sensitivity for identifying upright position was 0.91 (95% CI: 0.88, 0.94) and specificity was 0.76 (95% CI: 0.69, 0.83) (Supplementary eTable S5). Of the 485 min of recumbent positioning, the device accurately identified 317 (72.9%). For the recumbent positions, sensitivity was 0.76 (95% CI: 0.69, 0.83) and specificity was 0.91 (95% CI: 0.88, 0.94). Notably, supine position was most often categorized as upright (Supplementary eTable S6).
Surveys completed at the end of the participation period demonstrated that nearly all participants agreed or strongly agreed that the devices were comfortable to wear and easy to place and remove, and they would agree to wear the devices for the conduct of a study (Figure 1). There was no difference in survey responses based on age <6 and ≥6 years-old (data not shown). As noted by two participants in our study, the BioButton device adhesive was less effective when placed on moist skin such as would occur if placement occurred during activity causing extreme perspiration. If the adhesive was placed prior to sweating, it was more effective.
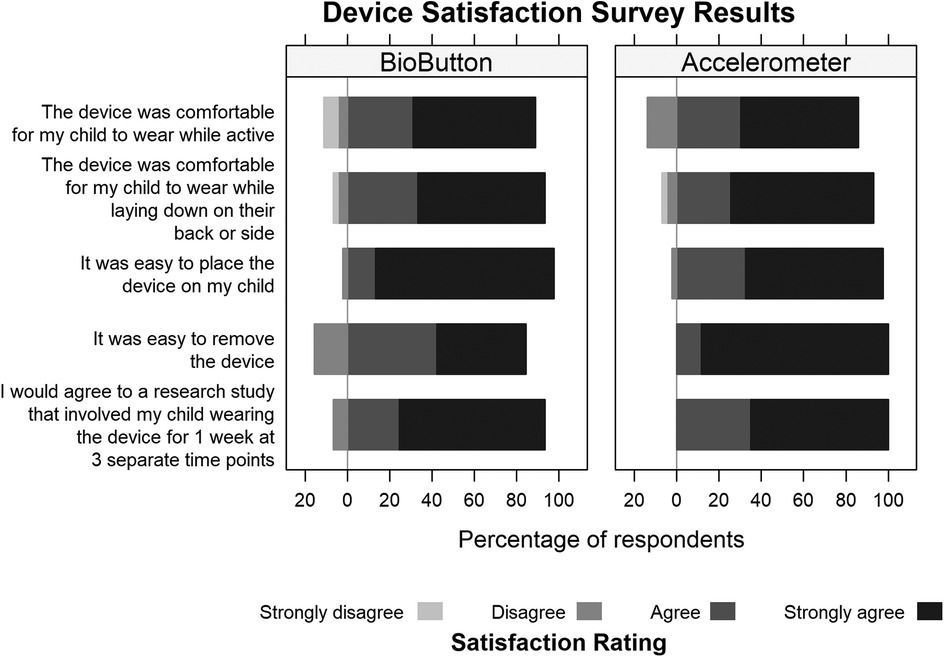
Figure 1. Satisfaction survey results.
In this cohort of healthy, typically developing children, we identified that the BioButton device was able to differentiate MVPA from sedentary and other lesser activity and identify sedentary behavior. In addition to activity monitoring, the BioButton device was also able to differentiate upright vs. recumbent positioning, which may be relevant to children with mobility and activity limitations. Physical activity represents an important outcome domain for children who have experienced critical illness, and the ability to measure activity in free-living conditions is an important complementary evaluation to survey data, which is currently the most common method of assessment of physical outcomes after critical illness. The BioButton device can serve as an alternative option to measure physical recovery longitudinally and could provide a method to identify patients who require further interventions after critical illness.
Core outcome sets developed for critically ill children and adults highlight the importance of physical recovery (7–9, 32, 33). In core outcome sets for adults, surveys are most commonly used for physical activity assessment, but there are objective measures also including the 6 min walk test, short physical performance battery; and 30 s sit to stand test (7, 34–36). In core outcome sets for children who have survived an episode of critical illness, physical activity measurements are limited to survey-based tools (8, 37). Commonly used measures to evaluate physical functioning are the Functional Independence Measure including the pediatric version, WeeFIM, the Functional Status Scale (FSS) score, the PedsQL Physical Health Summary Score, which is a HRQL measure, and the Pediatric Evaluation of Disability Inventory Computer Adaptive Test (PEDICat) (2, 4, 38–41). These measures can reflect change in function over time but are limited by subjectivity. Researchers evaluating physical health recovery after critical illness could add objective physical health data using mobile monitoring devices. As demonstrated by the survey data collected at the end of the wear period of our study, the BioButton may be an acceptable device for this use due to the simplicity of placement and removal as well as the discrete design.
The remote set-up and monitoring capabilities provided by the BioButton and ActiGraph accelerometer may reduce disparities in measuring physical health outcomes by eliminating the need to return to a hospital or clinic for direct evaluation. Removing this barrier may increase participation of socially vulnerable populations who are underrepresented in research but overrepresented in PICU patients (42, 43). Adoption of these methods in critical care research as well as other domains of pediatric research may provide more robust trial outcomes and improve research access for underrepresented populations. Additionally, BioButton users can access their data through a smartphone and data transmission through cellular networks allows for data collection even if the device is not returned. The single-use and relatively low cost of the BioButton, currently one-fifth the cost of the ActiGraph accelerometer, are also attractive features. Additionally, there may be opportunities to pair BioButton monitoring with electronic ecological momentary assessments to understand the social and environmental contexts associated with more sedentary or more active periods (44–47). However, there are important limitations of this technology to quantify physical activity outcomes. The lack of pre-illness baseline measurements poses a challenge to evaluating the impact of critical illness on objectively measured physical outcomes. Additionally, use of the BioButton device requires connection to the downloadable BioMobile™ application by a smart phone or connection to a separate BioHub™ device for wireless data transmission. Notably, BioButton users can access their information through the BioMobile™ application, which could influence their overall physical activity. This would be important to consider if used as a trial outcome. Lastly, the BioButton smartphone application, user guides, and related resources are currently only available in English.
In addition to measuring physical activity, the BioButton device's ability to characterize body position may provide a valuable measure of physical outcomes in children with mobility restrictions. A recent epidemiologic study of critically ill children identified that nearly 60% of children have a pre-existing comorbidity including one in four with technology dependence and one in five with a neuromuscular comorbidity (1). These patients frequently have mobility limitations, but their physical functioning outcomes could be readily quantified by positioning including time in the upright position. The BioButton device's ability to differentiate position offers a unique opportunity to quantify this physical outcome for children with limited mobility.
This study has important limitations. Although we attempted to capture activity and positioning data at the minute-level using direct observation, start and stop times of activity may not have been exact, particularly due to the need for water breaks and brief rests during significant heat on some study days. Due to study location, we were unable to use a gold-standard method to evaluate exercise intensity (e.g., indirect calorimetry). Comparison with the ActiGraph accelerometer demonstrated acceptable specificity to discriminate accelerometer-identified MVPA, even though sensitivity was lower in the older age groups. This may be due to the wrist-worn location for the ActiGraph accelerometer in older participants relative to the similarity of truncal locations between the ActiGraph accelerometer in younger patients (hip) and the BioButton (chest). Discrimination of accelerometer-identified sedentary behavior based on BioButton thresholds was good. Our study population was limited to healthy, typically developing children, which may limit generalizability to children with physical or cognitive impairments. Lastly, the variability in exertion by study participants who completed the same type of activity may also have affected our study's internal validity when comparing measured to documented activity. We attempted to mitigate this with direct one-on-one interaction with the children to encourage participation at the appropriate activity level and note when the activity level was not reached but some participants struggled to maintain specific activity levels for prolonged periods of time.
The BioIntelliSense BioButton® device is a promising new technology that may serve as an accurate, objective, and feasible method to measure physical outcomes in children. This device or devices with similar characteristics may serve as a method to measure objective, patient-centered outcomes for future clinical trials to complement patient-reported outcome measures. Future studies are needed to evaluate tolerance and accuracy of prolonged monitoring periods.
The raw data supporting the conclusions of this article will be made available by the authors with appropriate approvals, without undue reservation.
The studies involving humans were approved by Colorado Multiple Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
LP: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. KM: Conceptualization, Formal analysis, Visualization, Writing – review & editing. RG: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. HS: Investigation, Writing – original draft, Writing – review & editing. RW: Supervision, Writing – review & editing. PM: Conceptualization, Supervision, Writing – review & editing. AM: Conceptualization, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by an award from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Maddux, K23HD096018) and an award from the University of Colorado School of Medicine.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1544404/full#supplementary-material
1. Killien EY, Keller MR, Watson RS, Hartman ME. Epidemiology of intensive care admissions for children in the US from 2001 to 2019. JAMA Pediatr. (2023) 177(5):506–15. doi: 10.1001/jamapediatrics.2023.0184
2. Maddux AB, Pinto N, Fink EL, Hartman ME, Nett S, Biagas K, et al. Postdischarge outcome domains in pediatric critical care and the instruments used to evaluate them: a scoping review. Crit Care Med. (2020) 48(12):e1313–e21. doi: 10.1097/CCM.0000000000004595
3. Maddux AB, Miller KR, Sierra YL, Bennett TD, Watson RS, Spear M, et al. Recovery trajectories in children requiring 3 or more days of invasive ventilation. Crit Care Med. (2024) 52(5):798–10. doi: 10.1097/CCM.0000000000006187
4. Choong K, Al-Harbi S, Siu K, Wong K, Cheng J, Baird B, et al. Functional recovery following critical illness in children: the “wee-cover” pilot study. Pediatr Crit Care Med. (2015) 16(4):310–8. doi: 10.1097/PCC.0000000000000362
5. Pinto NP, Rhinesmith EW, Kim TY, Ladner PH, Pollack MM. Long-term function after pediatric critical illness: results from the survivor outcomes study. Pediatr Crit Care Med. (2017) 18(3):e122–e30. doi: 10.1097/PCC.0000000000001070
6. Watson RS, Asaro LA, Hertzog JH, Sorce LR, Kachmar AG, Dervan LA, et al. Long-term outcomes after protocolized sedation versus usual care in ventilated pediatric patients. Am J Respir Crit Care Med. (2018) 197(11):1457–67. doi: 10.1164/rccm.201708-1768OC
7. Hodgson CL, Fulcher B, Mariajoseph FP, Burrell AJC, Pellegrino V, Brodie D, et al. A core outcome set for research in patients on extracorporeal membrane oxygenation. Crit Care Med. (2021) 49(12):e1252–e4. doi: 10.1097/CCM.0000000000005110
8. Topjian AA, Scholefield BR, Pinto NP, Fink EL, Buysse CMP, Haywood K, et al. P-COSCA (pediatric core outcome set for cardiac arrest) in children: an advisory statement from the international liaison committee on resuscitation. Resuscitation. (2021) 162:351–64. doi: 10.1016/j.resuscitation.2021.01.023
9. Fink EL, Maddux AB, Pinto N, Sorenson S, Notterman D, Dean JM, et al. A core outcome set for pediatric critical care. Crit Care Med. (2020) 48(12):1819–28. doi: 10.1097/CCM.0000000000004660
10. Lo DK, Beardsmore CS, Roland D, Richardson M, Yang Y, Danvers L, et al. Lung function and asthma control in school-age children managed in UK primary care: a cohort study. Thorax. (2020) 75(2):101–7. doi: 10.1136/thoraxjnl-2019-213068
11. Nawaz SF, Ravindrarn M, Kuruvilla ME. Asthma diagnosis using patient-reported outcome measures and objective diagnostic tests: now and into the future. Curr Opin Pulm Med. (2022) 28(3):251–7. doi: 10.1097/MCP.0000000000000871
12. Rhee H, Love T, Mammen J. Comparing asthma control questionnaire (ACQ) and national asthma education and prevention program (NAEPP) asthma control criteria. Ann Allergy Asthma Immunol. (2019) 122(1):58–64. doi: 10.1016/j.anai.2018.09.448
13. Chiang JL, Maahs DM, Garvey KC, Hood KK, Laffel LM, Weinzimer SA, et al. Type 1 diabetes in children and adolescents: a position statement by the American diabetes association. Diabetes Care. (2018) 41(9):2026–44. doi: 10.2337/dci18-0023
14. Foster C, Schinasi D, Kan K, Macy M, Wheeler D, Curfman A. Remote monitoring of patient- and family-generated health data in pediatrics. Pediatrics. (2022) 149(2):e2021054137. doi: 10.1542/peds.2021-054137
15. Rudd NA, Ghanayem NS, Hill GD, Lambert LM, Mussatto KA, Nieves JA, et al. Interstage home monitoring for infants with single ventricle heart disease: education and management: a scientific statement from the American heart association. J Am Heart Assoc. (2020) 9(16):e014548. doi: 10.1161/JAHA.119.014548
16. Chong KH, Suesse T, Cross PL, Ryan ST, Aadland E, Aoko O, et al. Pooled analysis of physical activity, sedentary behavior, and sleep among children from 33 countries. JAMA Pediatr. (2024) 178(11):1199–207. doi: 10.1001/jamapediatrics.2024.3330
17. Neville RD, Lakes KD, Hopkins WG, Tarantino G, Draper CE, Beck R, et al. Global changes in child and adolescent physical activity during the COVID-19 pandemic: a systematic review and meta-analysis. JAMA Pediatr. (2022) 176(9):886–94. doi: 10.1001/jamapediatrics.2022.2313
18. Casado-Robles C, Viciana J, Guijarro-Romero S, Mayorga-Vega D. Effects of consumer-wearable activity tracker-based programs on objectively measured daily physical activity and sedentary behavior among school-aged children: a systematic review and meta-analysis. Sports Med Open. (2022) 8(1):18. doi: 10.1186/s40798-021-00407-6
19. Maddux AB, Miller KR, Sierra YL, Bennett TD, Watson RS, Spear M, et al. Physical activity monitoring as a measure of post-ICU physical recovery in children in the 1-year after surviving an episode of at least 3 or more days of of invasive ventilation: a pilot feasibility study using accelerometers. Pediatr Crit Care Med. (2025) 26(3):e324–33. doi: 10.1097/PCC.0000000000003657
20. 510(k) Premarket Notification Silver Spring, MD: U.S. Food and Drug Administration. Available online at: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K212957 (updated July 3, 2023).
21. Cora TM, Doerner ME, Connerton CS. Enhancing oncology Side effect management using a remote monitoring system. Clin J Oncol Nurs. (2023) 27(5):491–5. doi: 10.1188/23.CJON.491-495
22. Trost SG, Loprinzi PD, Moore R, Pfeiffer KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc. (2011) 43(7):1360–8. doi: 10.1249/MSS.0b013e318206476e
23. Chandler JL, Brazendale K, Beets MW, Mealing BA. Classification of physical activity intensities using a wrist-worn accelerometer in 8–12-year-old children. Pediatr Obes. (2016) 11(2):120–7. doi: 10.1111/ijpo.12033
24. Butte NF, Wong WW, Lee JS, Adolph AL, Puyau MR, Zakeri IF. Prediction of energy expenditure and physical activity in preschoolers. Med Sci Sports Exerc. (2014) 46(6):1216–26. doi: 10.1249/MSS.0000000000000209
25. Mannini A, Intille SS, Rosenberger M, Sabatini AM, Haskell W. Activity recognition using a single accelerometer placed at the wrist or ankle. Med Sci Sports Exercise. (2013) 45(11):2193–203. doi: 10.1249/MSS.0b013e31829736d6
26. RT, JMC. Objective measures of physical activity, sleep, and strenght in U.S. National health and nutrition examination survey (NHANES) 2011-20142012; Rome, Italy. Proceedings of the 8th International Conference on Diet and Activity Methods.
27. UBCC. Category 2 Enhanced Phenotyping at Baseline Assessment Visit in Last 100–150,000 Participants. Stockport Cheshire: UK Biobank Coordinating Centre (2009).
28. Fairclough SJ, Noonan R, Rowlands AV, Van Hees V, Knowles Z, Boddy LM. Wear compliance and activity in children wearing wrist- and hip-mounted accelerometers. Med Sci Sports Exercise. (2016) 48(2):245–53. doi: 10.1249/MSS.0000000000000771
29. Barkin SL, Heerman WJ, Sommer EC, Martin NC, Buchowski MS, Schlundt D, et al. Effect of a behavioral intervention for underserved preschool-age children on change in body mass index: a randomized clinical trial. JAMA. (2018) 320(5):450–60. doi: 10.1001/jama.2018.9128
31. Rao JN, Scott AJ. A simple method for the analysis of clustered binary data. Biometrics. (1992) 48:577–85. doi: 10.2307/2532311
32. Munblit D, Nicholson T, Akrami A, Apfelbacher C, Chen J, De Groote W, et al. A core outcome set for post-COVID-19 condition in adults for use in clinical practice and research: an international Delphi consensus study. Lancet Respir Med. (2022) 10(7):715–24. doi: 10.1016/S2213-2600(22)00169-2
33. Needham DM, Sepulveda KA, Dinglas VD, Chessare CM, Friedman LA, Bingham CO 3rd, et al. Core outcome measures for clinical research in acute respiratory failure survivors. An international modified delphi consensus study. Am J Respir Crit Care Med. (2017) 196(9):1122–30. doi: 10.1164/rccm.201702-0372OC
34. Gorst SL, Seylanova N, Dodd SR, Harman NL, O'Hara M, Terwee CB, et al. Core outcome measurement instruments for use in clinical and research settings for adults with post-COVID-19 condition: an international Delphi consensus study. Lancet Respir Med. (2023) 11(12):1101–14. doi: 10.1016/S2213-2600(23)00370-3
35. Turnbull AE, Sepulveda KA, Dinglas VD, Chessare CM, Bingham CO 3rd, Needham DM. Core domains for clinical research in acute respiratory failure survivors: an international modified Delphi consensus study. Crit Care Med. (2017) 45(6):1001–10. doi: 10.1097/CCM.0000000000002435
36. Davies TW, van Gassel RJJ, van de Poll M, Gunst J, Casaer MP, Christopher KB, et al. Core outcome measures for clinical effectiveness trials of nutritional and metabolic interventions in critical illness: an international modified Delphi consensus study evaluation (CONCISE). Crit Care. (2022) 26(1):240. doi: 10.1186/s13054-022-04113-x
37. Pinto NP, Maddux AB, Dervan LA, Woodruff AG, Jarvis JM, Nett S, et al. A core outcome measurement set for pediatric critical care. Pediatr Crit Care Med. (2022) 23(11):893–907. doi: 10.1097/PCC.0000000000003055
38. ARDS in Children and ECMO Initiation Strategies Impact on Neurodevelopment (ASCEND). NIH Reporter. Available online at: https://www.clinicaltrials.gov/study/NCT05388708?term=ECMO;%20pediatric&rank=5&tab=table (cited January 25, 2024).
39. GM-CSF for Reversal of Immunoparalysis in Pediatric Sepsis-induced MODS (GRACE-2). NIH Reporter. (2023). Available online at: https://www.clinicaltrials.gov/study/NCT05266001?cond=sepsis;%20pediatric%20&page=3&rank=27&tab=table (cited January 25, 2024).
40. Targeted Reversal of Inflammation in Pediatric Sepsis-induced MODS (TRIPS) [Internet]. NIH Reporter. Available online at: https://www.clinicaltrials.gov/study/NCT05267821?cond=sepsis;%20pediatric%20&limit=100&aggFilters=status:rec&rank=6 (cited January 25, 2024).
41. Stress Hydrocortisone In Pediatric Septic Shock (SHIPSS) [Internet]. NIH Reporter. Available online at: https://www.clinicaltrials.gov/study/NCT03401398?cond=sepsis;%20pediatric%20&limit=100&aggFilters=status:rec&rank=11 (cited January 25, 2024).
42. Najjar N, Opolka C, Fitzpatrick AM, Grunwell JR. Geospatial analysis of social determinants of health identifies neighborhood hot spots associated with pediatric intensive care use for acute respiratory failure requiring mechanical ventilation. Pediatr Crit Care Med. (2022) 23(8):606–17. doi: 10.1097/PCC.0000000000002986
43. McCrory MC, Akande M, Slain KN, Kennedy CE, Winter MC, Stottlemyre MG, et al. Child opportunity Index and pediatric intensive care outcomes: a multicenter retrospective study in the United States. Pediatr Crit Care Med. (2024) 25(4):323–34. doi: 10.1097/PCC.0000000000003427
44. Kuhn A, Wang Y, Deitch R, Zemanick A, Dunton G, Turner L, et al. Ecological momentary assessment of momentary associations between availability of physical activity space and physical activity opportunities among children from Rural, Urban, and Suburban locales. Int J Environ Res Public Health. (2024) 21(12):1586. doi: 10.3390/ijerph21121586
45. Liao Y, Intille SS, Dunton GF. Using ecological momentary assessment to understand where and with whom adults’ physical and sedentary activity occur. Int J Behav Med. (2015) 22(1):51–61. doi: 10.1007/s12529-014-9400-z
46. Pickering TA, Huh J, Intille S, Liao Y, Pentz MA, Dunton GF. Physical activity and variation in momentary behavioral cognitions: an ecological momentary assessment study. J Phys Act Health. (2016) 13(3):344–51. doi: 10.1123/jpah.2014-0547
Keywords: exercise, sedentary behavior, patient outcome assessment (MeSH), pediatrics—children, critical care outcomes
Citation: Petruccelli L, Miller KR, Greer R, Sauceda H, Watson RS, Mourani PM and Maddux AB (2025) Validation of the BioIntelliSense BioButton® device for physical activity monitoring in children and future application as a physical health outcome for critically Ill children. Front. Pediatr. 13:1544404. doi: 10.3389/fped.2025.1544404
Received: 12 December 2024; Accepted: 13 March 2025;
Published: 15 April 2025.
Edited by:
Stephanie C. DeLuca, Virginia Tech, United StatesReviewed by:
Laura Nabors, University of Cincinnati, United StatesCopyright: © 2025 Petruccelli, Miller, Greer, Sauceda, Watson, Mourani and Maddux. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aline B. Maddux, YWxpbmUubWFkZHV4QGNoaWxkcmVuc2NvbG9yYWRvLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.