
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr., 10 March 2025
Sec. General Pediatrics and Pediatric Emergency Care
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1536571
 Pankaj Soni1,2*†
Pankaj Soni1,2*† Jenny Cheriathu3
Jenny Cheriathu3
Introduction: This systematic review assessed the long-term psychological effects of severe respiratory infections—namely, bronchiolitis and influenza—in school-aged children (5–12 years).
Methods: PubMed, EMBASE, and the Cochrane Library were searched for randomized controlled trials, cohort and longitudinal studies on school-aged children (5–12 years) with a history of bronchiolitis or influenza infection in early childhood published between 2014 and 2022. Studies evaluating long-term psychological outcomes at least 6 months post-infection were included.
Results: Several studies that were included in this review reported increased risks of anxiety disorders, depression, and attention deficit among those with severe respiratory infections in early childhood. Additionally, studies with prolonged follow-up periods often reported a higher incidence of psychological morbidity in children. However, some studies did not detect significant long-term adverse effects, implying that timely interventions and supportive care may minimize negative psychological outcomes. This review underscores the necessity of mental health support following respiratory infections in children, highlights the need for further research on the biological and psychosocial pathways linking respiratory illnesses to psychological outcomes, and emphasizes the value of multidisciplinary treatment strategies for children with such comorbidities.
Conclusions: The findings of this review provide insights for healthcare practitioners, policymakers, and researchers to consider strategies aimed at improving the outcomes of respiratory illnesses in affected children.
Influenza and bronchiolitis are two of the most significant respiratory illnesses affecting children, with onset often occurring in infancy (1). Bronchiolitis, usually triggered by the respiratory syncytial virus, causes inflammation in the small airways of the lungs and may precipitate severe complications, including pneumonia (2, 3). Although short-term complications of respiratory illnesses are well documented, it is important to consider the long-term psychological impact on school-aged children who may have encountered respiratory illnesses during their infancy or toddler years (4, 5).
Recent epidemiological trends underscore the need for increased surveillance and scientific research. Notably, the characteristics of bronchiolitis infections may have changed post-COVID-19 pandemic, as highlighted in recent studies on bronchiolitis during the 2021–2023 epidemic seasons (6). Factors such as public health measures, competition among virus variants, and heightened awareness of respiratory illnesses have influenced both the severity and infection rates of bronchiolitis. Furthermore, new preventive strategies, such as nirsevimab (a monoclonal antibody targeting RSV), could alter future hospitalization rates and help prevent long-term sequelae (7).
The school-going age (5–12 years) is a developmental window characterized by rapid cognitive, emotional, and social growth. Children with chronic illnesses are at higher risk of psychological problems, such as anxiety, depression, and behavioral disorders (8). Although the physical consequences of bronchiolitis and influenza are well-studied, few studies examined their long-term psychological impact on children (9, 10). This knowledge gap is crucial, given that early-life respiratory diseases can influence developmental and psychosocial challenges later in life.
The current systematic review aims to summarize the evidence regarding the long-term psychological consequences of bronchiolitis and influenza in school-aged children. The core research questions include the following: (1) What psychological outcomes (e.g., anxiety, depression, behavioral, or cognitive problems) are associated with early-life bronchiolitis or influenza? (2) Are there specific socioeconomic or demographic factors (e.g., gender, household income, or maternal education) that modify these long-term psychological sequelae? (3) What preventive and clinical management policies can be implemented to provide holistic care interventions addressing both health and psychological issues in children with respiratory complaints?
Several studies have examined post-bronchiolitis psychological outcomes in school-aged children. Martimbianco et al. (11) investigated the pulmonary and neurocognitive impact of severe bronchiolitis on children requiring mechanical ventilation. Their findings showed that survivors face intellectual and neurodevelopmental challenges later in life, including memory and attention deficits. Similarly, Freeman et al. (12) linked severe bronchiolitis to a higher risk of developing asthma and subsequent psychosocial stress. Contrarily, the findings of Wrotek et al. (13) showed no significant long-term psychological impact, such as depression and disruptive behavior, in most children hospitalized for bronchiolitis. This disparity between results could indicate variations in the severity of bronchiolitis, coping mechanisms, or socioeconomic and environmental factors across study populations.
Influenza may also lead to various long-term psychological effects among children. Research conducted on adolescents with physical health issues, such as those who were discharged from medical facilities following influenza infection, demonstrated the occurrence of psychological distress and reduced cognitive performance (2). Endo et al. (14) studied classroom transmission of influenza in Japanese primary schools, observing disruptions in learning and social interactions due to school absenteeism. Moreover, a prospective observational study by Hoy et al. (15) demonstrated that annual influenza vaccination effectively minimized the severity of flu-related symptoms without showing any significant positive effects on long-term cognitive or psychological outcomes in school-aged children. Collectively, the findings of these studies suggest that although physical health might be acutely affected by influenza, residual psychological impacts can be subtle and may depend on vaccination coverage, timely treatment, and baseline health status.
Literature underscores the importance of psychological interventions in children with respiratory conditions including bronchiolitis and influenza. Szakács et al. (9) described psychiatric comorbidities in children with post-H1N1 narcolepsy, emphasizing that early psychological support can forestall or mitigate further psychopathological developments. Similarly, Stevens and Kelsall-Knight (16) noted that children with asthma benefit from counseling, demonstrating reduced anxiety levels and improved quality of life. Not all studies, however, document robust integration of mental health services. Freeman et al. (12) highlighted that psychological symptoms are often neglected in children with severe respiratory infections, especially in developing countries. This underscores the importance of comprehensive care that acknowledges both physical and mental health components for pediatric patients.
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The literature search was conducted using PubMed, EMBASE, and the Cochrane Library. Reference lists of relevant articles were also examined. The review included randomized controlled trials (RCTs) and cohort and longitudinal studies on school-aged children (5–12 years) with a documented history of bronchiolitis or influenza infection in early childhood. Only studies evaluating long-term psychological outcomes—including anxiety, depression, cognitive function, or behavioral changes—at least 6 months post-infection were included. The search covered articles published between 2014 and 2022, without language restriction. Case reports, editorials, opinion pieces, or studies lacking explicit psychological or mental health outcomes, studies with follow-up periods of <6 months, and non-randomized trials were excluded. The keywords and search strings are presented in Table 1; study inclusion and exclusion criteria are listed in Table 2.

Table 1. Keywords and search strings.
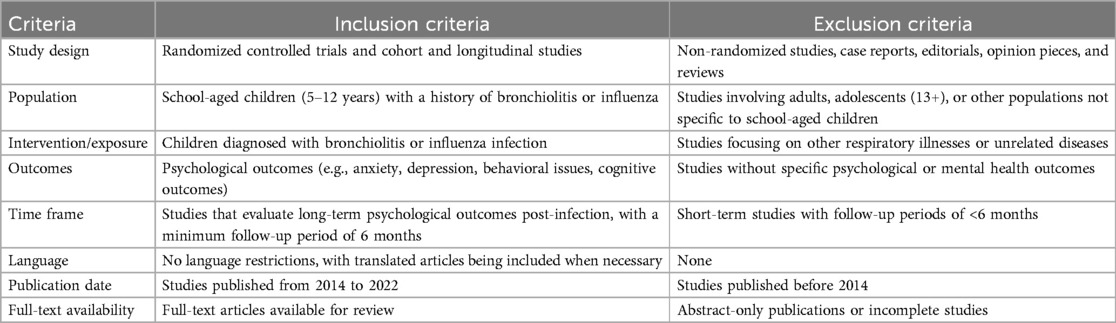
Table 2. Study eligibility criteria.
All references were imported into EndNote (Clarivate Analytics) for deduplication. Two independent reviewers (PS and JC) screened the titles and abstracts using Rayyan, a web-based screening tool. Full texts of potentially relevant studies were retrieved and reviewed thoroughly. Discrepancies were resolved through discussion until a consensus was reached. The final set of included studies was confirmed by both authors.
For data extraction, all identified abstracts and article citations were first reviewed for inclusion in this systematic review. A standardized MS Excel spreadsheet was created to capture relevant data from each included article, such as study characteristics (author, year of publication, design, and location), population details (participant age, sample size, and inclusion/exclusion criteria), exposure details (severity and timing of bronchiolitis or influenza infection), psychological outcomes (anxiety, depression, cognitive function, and behavioral impacts), follow-up duration, and key findings related to long-term mental health. All extracted data were checked for consistency and accuracy by both authors. This was supplemented with a careful analysis of the full text of each article to optimize the identification of all necessary data. PS performed the initial data extraction, which was independently validated by JC for accuracy. Any disagreements were reconciled through discussion. A PRISMA flowchart was developed to depict the selection process of studies included or excluded and the number of articles screened and included, along with the reasons for exclusions at each stage.
We employed the Cochrane risk of bias tool for RCTs and the Newcastle–Ottawa scale for observational studies, evaluating domains such as selection, performance, detection, and attrition bias. Studies were categorized as having a low, moderate, or high risk of bias.
A total of 464 articles were retrieved from the initial database search. After removing duplicates and articles that did not meet the initial screening criteria, 310 articles remained. Of these, 160 were excluded for being published outside the 2014–2022 timeframe or for lacking relevance to the study objectives. The full texts of the remaining 150 articles were reviewed against the inclusion and exclusion criteria, yielding 40 articles selected for detailed evaluation. Finally, 10 articles met all the eligibility criteria and were included in the qualitative synthesis (Figure 1).
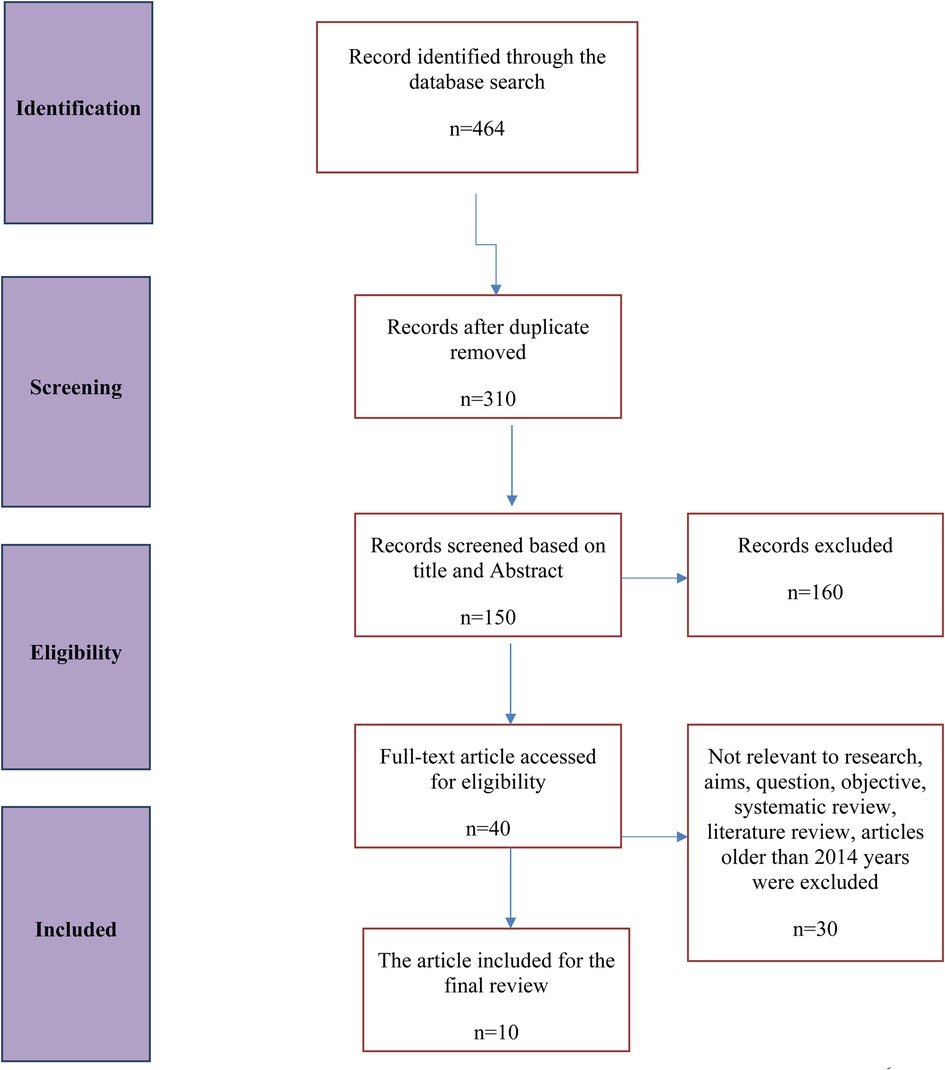
Figure 1. Flow chart of systematic literature search and article selection process.
The Cochrane risk of bias tool was used to assess the risk of bias and the quality of studies (11). The analysis revealed considerable variation in bias risk, necessitating careful interpretation of results. Most studies demonstrated low to moderate selection bias due to the use of matched cohorts and rigorous recruitment methods aimed at reducing confounding variables (14, 17). However, some studies relied on hospital-based samples, introducing a higher risk of selection bias and limiting the generalizability of findings (4). The risk of performance and detection biases was low for most studies, reflecting standardized treatment protocols and objective assessments (Table 3). However, some studies (18) were categorized as having higher risks due to non-blinded machine learning evaluations. Furthermore, attrition bias remained a concern in several studies where dropout rates and participant retention strategies were inadequately described (2, 19). Overall, although most studies provide valuable information, the presence of potential biases raises questions about the general and specific implications of the findings, emphasizing the need for further research to replicate conclusions in diverse samples.
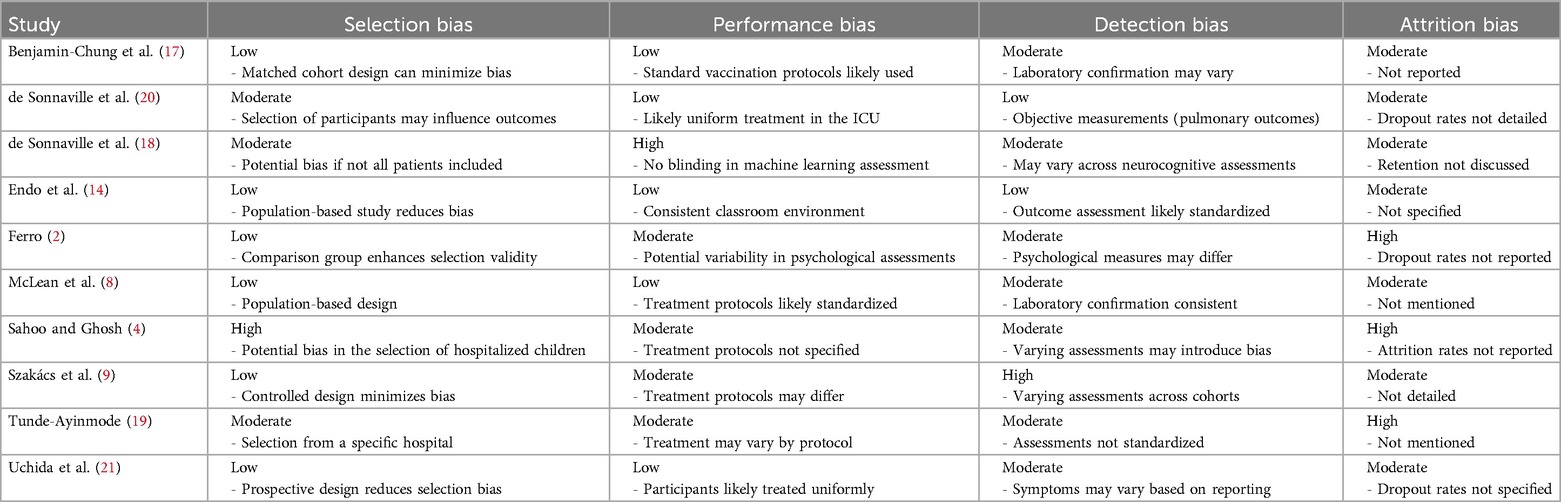
Table 3. Cochrane risk of bias tool for quality appraisal.
Anxiety is the main psychological outcome in children experiencing respiratory infections and those receiving care in the ICU (22). Sahoo and Ghosh (4) conducted a cross-sectional study on children with severe lower respiratory tract infections (LRTIs) in a tertiary care hospital in Eastern India. They found that 78.5% of children experienced delays in receiving medical attention. The delay was more pronounced in children of illiterate mothers compared to those of literate mothers. This delay acts as a stressor for both children and their caregivers due to the unpredictability of the child's condition or worsening of symptoms. Additionally, 67% of families belonged to the lowest socioeconomic strata, a factor that likely heightened anxiety due to financial constraints and inadequate access to healthcare (Table 4).
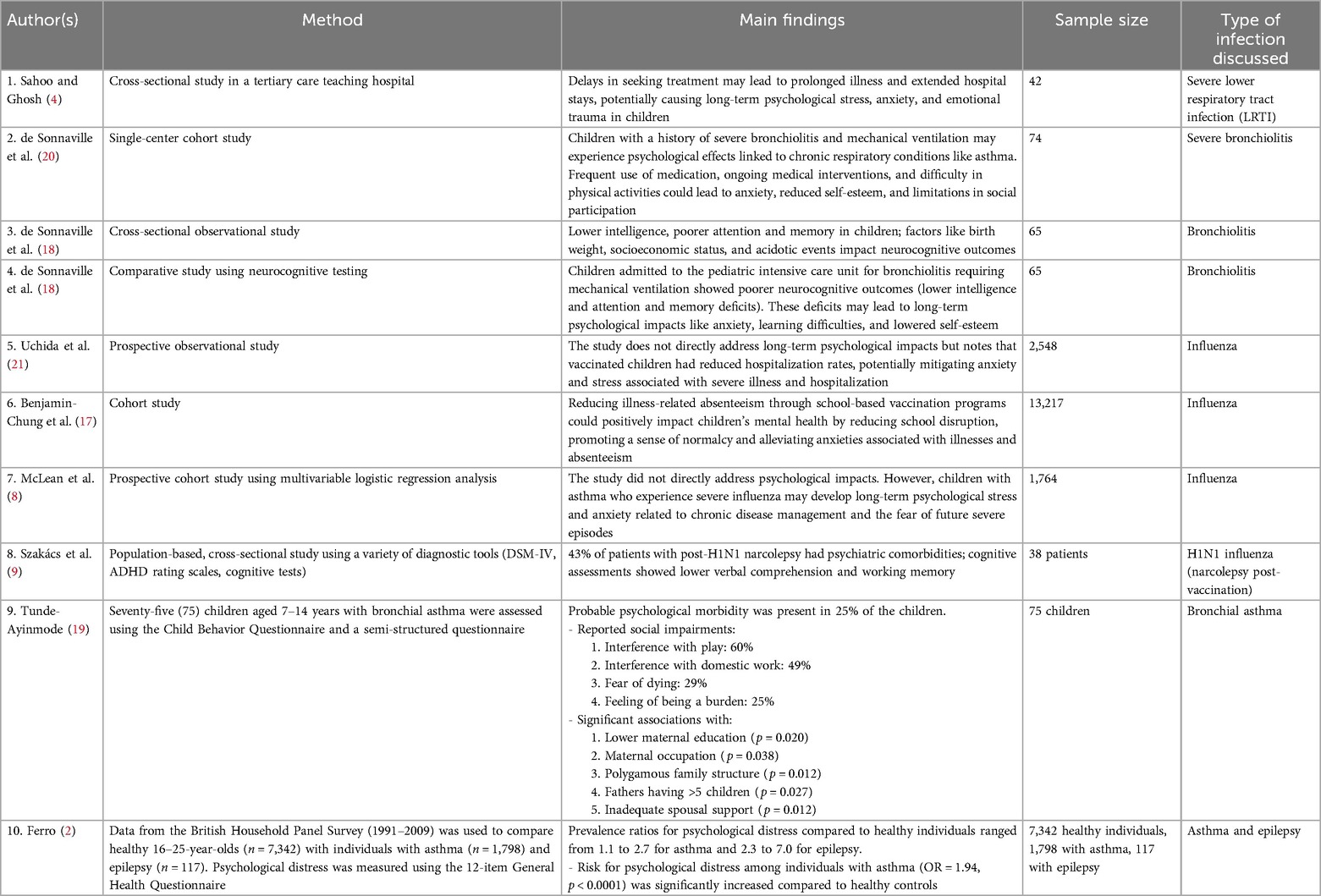
Table 4. Summary of main findings.
Furthermore, children with a history of respiratory infections, particularly those requiring intensive care may experience long-term effects that further contribute to anxiety. In a single-center cohort study, de Sonnaville et al. (20) examined children aged 6–12 years who had undergone invasive mechanical ventilation for bronchiolitis. Of the 74 children treated, 26% had adverse long-term pulmonary outcomes, including asthma in 19% of patients (Table 4). A family history of atopic diseases increased the risk of asthma by approximately 6.4-fold, while prolonged mechanical ventilation was associated with worsened pulmonary outcomes. These long-term health concerns heighten parental stress, particularly regarding their child’s future health, physical activity limitations, and academic performance (23).
Another factor that explains the anxiety of affected families is the interaction between respiratory disorders and neurocognitive outcomes. de Sonnaville et al. (18) found that children with bronchiolitis requiring admission to the pediatric intensive care unit showed lower intelligence quotient (IQ) and poorer neurodevelopment than their healthy peers. These children also demonstrated deficits in attention and processing speed (MA = 54, p = 0.03). Additionally, lower birth weight and socioeconomic disadvantage were associated with reduced cognitive function, intensifying parental concerns about their child's educational and social prospects. Further research is necessary to explore the correlation between respiratory health, the emotional state of children and caregivers, and long-term psychological effects on children.
Bronchiolitis, as a respiratory infection, has been associated with psychological consequences, including depression and anxiety (24). A study conducted by Uchida et al. (21) examined the impact of influenza vaccination on symptom severity in children diagnosed with influenza and explored the broader mental health effects of respiratory diseases. This study included data from 13,217 children from elementary schools, of whom, 2,548 had influenza, 1,122 were vaccinated, and 1,426 were not (Table 4). Although both groups exhibited similar symptom frequency and fever duration, vaccinated children had significantly lower hospitalization rates, suggesting that vaccination may mitigate the severity of influenza-related symptoms. The study also calls for addressing both the physical and psychological health implications of respiratory infections.
Moreover, Benjamin-Chung et al. (17) discussed the effectiveness of a school-based influenza vaccination program in Oakland, California, assessing vaccination uptake, school absenteeism, and laboratory-confirmed influenza cases. Approximately, 7,502–10,006 (22%–28%) students were vaccinated annually. During the two subsequent influenza seasons 2016–2017 and 2017–2018, the intervention school group demonstrated increased vaccination coverage compared to the control group, which translated to a reduced hospitalization rate among vaccinated students. The intervention group demonstrated increased vaccination coverage compared to control schools, which translated to a reduced hospitalization rate among vaccinated students (Table 4).
Ferro (2) conducted a cross-sectional comparative study on psychological distress among adolescents and young adults with physical illnesses, such as asthma or epilepsy. This study compared data from 7,342 healthy adults with data from 1,798 with asthma and 117 with epilepsy. Both patient categories had a higher risk of psychological distress. People with asthma experienced 1.94 times higher odds of psychological distress than those without asthma (p < 0.0001) (Table 4).
These studies show that respiratory infections impact physical and mental health, with high rates of clinically diagnosed depression and anxiety observed in affected populations. Implementing preventive measures such as vaccination and early intervention could significantly mitigate the psychological impact associated with these respiratory diseases (25).
Medical interventions, including vaccines, may be associated with psychiatric conditions such as attention deficit hyperactivity disorder (ADHD) (26). A study conducted by Szakács et al. (9) enrolled patients with narcolepsy, which developed in a few people after H1N1 vaccination. Of the 38 patients evaluated, 43% in the vaccinated group had psychiatric comorbidities, including 29% with ADHD (inattentive type); 20% with mood disorders, particularly major depressive disorder; and 10% with general anxiety disorder. Furthermore, temper tantrums were noted at a high frequency (94%) in the vaccinated group (Table 4).
Although mean full-scale IQ scores remained within the normal range for both vaccinated and unvaccinated groups, individuals with psychiatric comorbidities demonstrated lower IQ scores than those without such conditions (9). This indicates that despite the absence of apparent cognitive decline in some patients, active psychiatric disorders can negatively impact cognitive functioning, including verbal comprehension and working memory. This impairment may be influenced by specific medical interventions, including vaccinations.
McLean et al. (8) compared the severity of confirmed laboratory cases of influenza infection among school-aged children with and without asthma. Among 1,764 children with medically attended influenza, 287 (16%) had confirmed asthma (Table 4). The study also concluded that the incidence rate of severe complications from influenza was the same for children with and without asthma. Children with asthma were 1.35 times more likely to be hospitalized or suffer from pneumonia than children without asthma (AOR 1.35). However, children with respiratory disorders should not be automatically assumed to be at greater risk of severe influenza and its complications. Additionally, their mental health should be monitored as they cope with chronic diseases.
Tunde-Ayinmode (19) conducted a study involving 75 children aged 7–14 years diagnosed with bronchial asthma attending clinics at the University of Ilorin Teaching Hospital in Nigeria. The assessment included the Child Behavior Questionnaire and a semi-structured questionnaire to determine psychological and social factors associated with asthma. The findings showed that 25% of children presented with probable psychological morbidity. The study also established that asthma had the following social impact: limitation in play (60% of respondents), disruption of domestic work (49%), fear of dying (29%), and feeling like a burden to the family (25%). Moreover, psychological morbidity was associated with maternal education (p = 0.020), maternal occupation (p = 0.038), polygamy (p = 0.012), and spousal support (p = 0.012). Logistic regression analysis revealed that perceived inadequate spousal support and low maternal occupational levels were additional predisposing factors for psychological morbidity in these children (Table 4).
The analyzed studies indicate a potential connection between severe respiratory infections in early childhood and higher risks of mental health disturbances among school-aged children, such as anxiety, depression, and behavioral problems. Despite varied evidence, the literature consistently suggested a complex interplay involving pathophysiological and psychosocial factors. Systemic inflammation due to severe bronchiolitis or influenza infection may affect the developing central nervous system, leading to further consequences (8, 10). Factors like prolonged hospital stay, school absenteeism, and stress of parents may significantly influence a child's emotional and behavioral development (14).
According to Minotti et al. (27), despite being a pediatric health problem, bronchial asthma has a strong impact on psychosocial concerns, including perceiving life as a burden to the family and hindering daily activities. Similar to our findings, Ferro (2) found that adolescents with asthma have higher levels of psychological issues than their healthy peers. This highlights the need for both physical and mental evaluations of children with asthma, thereby guiding consensus on treatment and support interventions (28). The negative impact of low maternal education and occupational status on the psychological morbidity of children with asthma underscores the critical role of socioeconomic factors on health (29). Families with lower educational levels may be unaware of available health information and services that could help manage the psychological aspects of the disease (30). Hence, measures to ensure higher education for mothers and support structures could significantly reduce these psychological effects and improve the quality of life of children with asthma. Furthermore, self-reported social impairments emphasize the public sector consequences of providing care to children with chronic illnesses, thereby presenting comprehensive, family-focused community and policy solutions.
Moreover, the analysis reveals school absence resulting from respiratory ailments, highlighted in several studies (17, 21), necessitating preventive measures such as vaccination. Vaccination reduces hospitalization rates and ensures that children attend school and develop socially (31). Such impact of school absenteeism on quality of life and education further supports health promotion policies (32, 33).
Our findings have various implications for clinical practice and policy. For instance, integrating mental health screenings using standardized anxiety or depression scales during routine pediatric respiratory follow-ups may facilitate timely psychological evaluation (16). Other community-level interventions could also mitigate the negative impacts of illness on a child's academic and social well-being by strengthening family education and enhancing primary care resources. Furthermore, the standardization of outcome measures in longitudinal studies will provide clear insight into long-term effects and identify modifiable risk factors (9). All these coordinated efforts may lead to an integrated approach to addressing the problems prevalent among children with asthma and other chronic diseases, thus enhancing their quality of life and social inclusion.
This review reveals that bronchiolitis and influenza infection in early childhood can lead to long-lasting psychological impacts, including anxiety, depression, and attention deficits. However, timely interventions—such as vaccination—may offer significant protective benefits. Moreover, socioeconomic and demographic variables (e.g., maternal education and family structure) play a critical role. Additionally, the delayed or limited availability of psychological care—especially in resource-limited settings—underscores the importance of implementing interventions focused on the mental health of children. In conclusion, this literature review highlights that to optimize care for children recovering from respiratory illnesses, clinicians, policymakers, and educators must work together to develop comprehensive, multidisciplinary strategies that address the entire spectrum of health needs: physical, psychological, and social.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author.
PS: Writing – original draft, Writing – review & editing, Validation. JC: Formal analysis, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generativ AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Nathanielsz J, Toh ZQ, Do LAH, Mulholland K, Licciardi PV. SARS-CoV-2 infection in children and implications for vaccination. Pediatr Res. (2023) 93:1177–87. doi: 10.1038/s41390-022-02254-x
2. Ferro MA. Adolescents and young adults with physical illness: a comparative study of psychological distress. Acta Paediatr. (2014) 103:32–e37. doi: 10.1111/apa.12429
3. Zheng K, Tang L, Wang X, Chen L, Zhao Y, Chen X. The risk factors for chronic cough in children: a meta-analysis covering five continents. Resp Med. (2024) 232:107752. doi: 10.1016/j.rmed.2024.107752
4. Sahoo I, Ghosh S. Missed opportunities for earlier treatment of children admitted with severe lower respiratory tract infections in a tertiary care hospital. J Pediatr Pulmonol. (2022) 1:50. doi: 10.4103/jopp.jopp_25_22
5. Fitzpatrick T, McNally JD, Stukel TA, Lu H, Fisman D, Kwong JC, et al. Family and child risk factors for early-life RSV illness. Pediatrics. (2021) 147(4):e2020029090. doi: 10.1542/peds.2020-029090
6. Curatola A, Di Sarno L, Barbato M, Gatto A, Cultrera Di Montesano E, Chiaretti A. Epidemiological and clinical features of bronchiolitis after the COVID-19 outbreak: comparison of two epidemic seasons. Minerva Pediatrics (Torino). (2024). doi: 10.23736/S2724-5276.24.07510-4
7. Griffin MP, Yuan Y, Takas T, Domachowske JB, Madhi SA, Manzoni P, et al. Single-dose nirsevimab for prevention of RSV in preterm infants. N Engl J Med. (2020) 383:415–25. doi: 10.1056/NEJMoa1913556
8. McLean HQ, Hanson KE, Foster AD, Olson SC, Kemble SK, Belongia EA. Serious outcomes of medically attended, laboratory-confirmed influenza illness among school-aged children with and without asthma, 2007-2018. Influenza Other Resp. (2007) 14:173–81. doi: 10.1111/irv.12710
9. Szakács A, Hallböök T, Tideman P, Darin N, Wentz E. Psychiatric comorbidity and cognitive profile in children with narcolepsy with or without association to the H1N1 influenza vaccination. Sleep. (2015) 38:615–21. doi: 10.5665/sleep.4582
10. Munblit D, Greenhawt M, Brough HA, Pushkareva A, Karimova D, Demidova A, et al. Allergic diseases and immunodeficiencies in children, lessons learnt from COVID-19 pandemic by 2022: a statement from the EAACI-section on pediatrics. Pediatr Allergy Immu. (2022) 33:e13851. doi: 10.1111/pai.13851
11. Martimbianco ALC, Sá KMM, Santos GM, Santos EM, Pacheco RL, Riera R. Most Cochrane systematic reviews and protocols did not adhere to the Cochrane’s risk of bias 2.0 tool. Rev Assoc Med Bras. (2023) 69:469–72. doi: 10.1590/1806-9282.20221593
12. Freeman RE, Qi Y, Geller RJ, Cohen AR, Iyer SS, Waynik IY, et al. Parental mental health and childhood respiratory outcomes in a severe bronchiolitis cohort. Clin Pediatr. (2023) 62:1067–79. doi: 10.1177/00099228221150608
13. Wrotek A, Wrotek O, Jackowska T. The impact of RSV hospitalization on children’s quality of life. Diseases. (2023) 11:111. doi: 10.3390/diseases11030111
14. Endo A, Uchida M, Hayashi N, Liu Y, Atkins KE, Kucharski AJ, et al. Within and between classroom transmission patterns of seasonal influenza among primary school students in Matsumoto city, Japan. Proc Natl Acad Sci U S A. (2021) 118:e2112605118. doi: 10.1073/pnas.2112605118
15. Hoy G, Kuan G, López R, Sánchez N, López B, Ojeda S, et al. The spectrum of influenza in children. Clin Infect Dis. (2023) 76:e1012–20. doi: 10.1093/cid/ciac734
16. Stevens R, Kelsall-Knight L. Clinical assessment and management of children with bronchiolitis. Nurs Child Young People. (2024) 34:13–21. doi: 10.7748/ncyp.2022.e1430
17. Benjamin-Chung J, Arnold BF, Kennedy CJ, Mishra K, Pokpongkiat N, Nguyen A, et al. Evaluation of a city-wide school-located influenza vaccination program in Oakland, California, with respect to vaccination coverage, school absences, and laboratory-confirmed influenza: a matched cohort study. PLoS Med. (2020) 17:e1003238. doi: 10.1371/journal.pmed.1003238
18. de Sonnaville ESV, Vermeule J, Oostra K, Knoester H, van Woensel JBM, Allouch SB, et al. Predicting long-term neurocognitive outcome after pediatric intensive care unit admission for bronchiolitis—preliminary exploration of the potential of machine learning. Eur J Pediatr. (2024) 183:471–82. doi: 10.1007/s00431-023-05307-3
19. Tunde-Ayinmode M. Children with bronchial asthma assessed for psychosocial problems in a teaching hospital in Nigeria. Afr H Sci. (2015) 15:690. doi: 10.4314/ahs.v15i2.49
20. de Sonnaville ESV, Knoester H, Terheggen-Lagro SWJ, Königs M, Oosterlaan J, van Woensel JBM. Long-term pulmonary outcomes in children mechanically ventilated for severe bronchiolitis. Pediatr Crit Care Me. (2022) 23:801–11. doi: 10.1097/PCC.0000000000003022
21. Uchida M, Takeuchi S, Saito M-M, Koyama H. Effects of influenza vaccination on seasonal influenza symptoms: a prospective observational study in elementary schoolchildren in Japan. Heliyon. (2020) 6:e03385. doi: 10.1016/j.heliyon.2020.e03385
22. Backes EP, Gootman JA, Coker TR, National Academies of Sciences, Engineering, and Medicine. Health effects. In Addressing the Long-Term Effects of the COVID-19 Pandemic on Children and Families. US: National Academies Press (2023).
23. Sanghavi B, Sugapradha GR, Premkumar B, Elizabeth J, Premkumar B Sr, Elizabeth J Jr. Clinical profile and outcome of bronchiolitis in children with 1–24 months of age. Cureus. (2024) 16(9):e69640. doi: 10.7759/cureus.69640
24. Cadotte N, Moore H, Stone BL, Pershing NL, Ampofo K, Ou Z, et al. Prevalence of and risks for bacterial infections in hospitalized children with bronchiolitis. Hosp Pediatr. (2024) 14:603–11. doi: 10.1542/hpeds.2023-007549
25. Venkatesan P. Advances in preventing RSV in children. The Lancet Microbe. (2024) 5:e421. doi: 10.1016/S2666-5247(24)00043-0
26. Walsh PS, Wendt W-J, Lipshaw MJ. Asthmalitis? Diagnostic variability of asthma and bronchiolitis in children <24 months. Hosp Pediatr. (2024) 14:59–66. doi: 10.1542/hpeds.2023-007359
27. Minotti C, McKenzie C, Dewandel I, Bekker C, Sturniolo G, Doni D, et al. How does post COVID differ from other post-viral conditions in childhood and adolescence (0–20 years old)? A systematic review. eClinicalMedicine. (2024) 68:102436. doi: 10.1016/j.eclinm.2024.102436
28. Li Q, Song M, Hu Z, Ding Y, Huang C, Liu J. Pediatric respiratory pathogen dynamics in Southern Sichuan, China: a retrospective analysis of gender, age, and seasonal trends. Front Pediatr. (2024) 12:1374571. doi: 10.3389/fped.2024.1374571
29. Perofsky AC, Hansen CL, Burstein R, Boyle S, Prentice R, Marshall C, et al. Impacts of human mobility on the citywide transmission dynamics of 18 respiratory viruses in pre- and post-COVID-19 pandemic years. Nat Commun. (2024) 15:4164. doi: 10.1038/s41467-024-48528-2
30. Davidson AM, Burns S, White LA, Perlman M. “I shall not poison my child with your human experiment”: investigating predictors of parents’ hesitancy about vaccinating younger children (<12) in Canada. Vaccine. (2024) 42:505–11. doi: 10.1016/j.vaccine.2023.12.073
31. Siewert B, Kozajda A, Jaskulak M, Zorena K. Examining the link between air quality (PM, SO2, NO2, PAHs) and childhood obesity: a systematic review. JCM. (2024) 13:5605. doi: 10.3390/jcm13185605
32. Orr C, Kelty E, Belinelo P, Fisher C, Glauert AR, O’Donnell M, et al. Exposure to family and domestic violence in the prenatal period is associated with an increased risk of hospitalization for bronchiolitis in children under 2 years. J Public Health. (2024) 46:e448–57. doi: 10.1093/pubmed/fdae120
Keywords: bronchiolitis, influenza, mental health, psychological effects, school-aged children
Citation: Soni P and Cheriathu J (2025) Exploring long-term psychological effects of bronchiolitis and influenza in school-aged children. Front. Pediatr. 13:1536571. doi: 10.3389/fped.2025.1536571
Received: 29 November 2024; Accepted: 11 February 2025;
Published: 10 March 2025.
Edited by:
Anna Maria Musolino, Bambino Gesù Children's Hospital (IRCCS), ItalyReviewed by:
Varalakshmi Chandra Sekaran, Manipal Academy of Higher Education, IndiaCopyright: © 2025 Soni and Cheriathu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pankaj Soni, cHMzODU4QGdtYWlsLmNvbQ==
†ORCID:
Pankaj Soni
orcid.org/0009-0005-7245-5340
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.