 Anfeng Lu
Anfeng Lu Peilu Huang1
Peilu Huang1 Zhangbin Yu
Zhangbin Yu Hong Tang
Hong Tang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 20 March 2025
Sec. Neonatology
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1534773
This article is part of the Research Topic Maternal and Infant Nutrition: Impact on Breast Milk, Infant Gut Microbiota and Health Development View all 7 articles
Background: Very preterm infants are highly vulnerable to complications, imposing a significant economic burden on healthcare systems. Human milk has protective effects on these infants, but there is no systematic review on its economic impact.
Objective: We conducted a comprehensive review of studies assessing the economic evaluations of human milk for very preterm infants.
Methods: Our literature search covered PubMed, Embase, the Cochrane Library, and Web of Science. Two reviewers independently extracted data on economic evaluations and assessed study quality using the Pediatric Quality Appraisal Questionnaire (PQAQ).
Results: Fourteen studies of moderate quality, conducted in the United States, Germany, and Canada, met the inclusion criteria. However, the studies analyzed had notable variations and shortcomings. The majority of these studies (n = 11) performed economic evaluations from a healthcare system perspective, utilizing cost-consequence analysis (n = 6) up to the point of neonatal discharge (n = 11). All human milk interventions indicated cost-effective or cost saving results; only a minority included discounting (n = 2).
Conclusion: This systematic review suggests that economic evaluation of human milk for very preterm infants is an expanding area of research. Human milk for very preterm infants offers substantial economic advantages during neonatal intensive care unit hospitalization. Standardized and high-quality studies are needed to determine the cost-effectiveness of human milk for very preterm infants in the future.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO, identifier (CRD42024539574).
Worldwide from 2010 to 2020, approximately 15% of all preterm births occurred at less 32 weeks of gestation (1). They have a substantial economic impact on healthcare systems, largely due to the cost of initial hospitalization (2). There is a negative correlation between gestational age and the median cost of neonatal intensive care unit (NICU) hospitalization (3). Though very preterm infants (VPIs, gestational age < 32 weeks) make up only 1.4% of total births, they account for 36.5% of newborn care costs, making them among the most expensive hospitalized patients (4). VPIs also are particularly susceptible to developing serious morbidities associated with prematurity, such as bronchopulmonary dysplasia (BPD), necrotizing enterocolitis (NEC), late-onset sepsis (LOS), retinopathy of prematurity (ROP), intraventricular hemorrhage (IVH), and periventricular leukomalacia (PVL) (5, 6), and having substantially higher risks of adverse outcomes. Meanwhile, these morbidities significantly increase the risk of mortality in those infants, imposing a significant burden on families, healthcare programs, and educational systems throughout childhood (7). Therefore, strategies aimed at reducing the incidence, severity, and risk of these preventable morbidities during initial NICU hospitalization are crucial from both clinical and economic perspectives.
Human milk (HM) is abundant in nutrients and protective immunomodulatory components (e.g., bioactive enzymes and immune cells) and is the “gold standard” for preterm infant nutrition. It adapts dynamically to preterm infant needs to fully support healthy infant development for the first six months of life, and has the dynamic ability to be optimally matched to the evolving stages of preterm infants' immune system development (8). Multiple studies have demonstrated the effectiveness of HM in reducing the incidence, severity, and/or risk of prematurity-related morbidities, including NEC (9, 10), LOS (9, 11), BPD (12, 13) and ROP (14) during the NICU hospitalization at critical post-birth exposure periods, and the impact on these neonatal complications in a dose-dependent manner (15, 16). Accordingly, the American Academy of Pediatrics has released a statement on breastfeeding and has recommended all preterm infants should receive HM (17). However, current breastfeeding rates among VPIs for exclusive mother's own milk (MOM) at discharge is still far from satisfactory, ranging from 41.18% to 52% (1, 18). It is a priority for global health policy to increase very preterm infants' breastfeeding rates in NICU.
However, HM feeding in the NICU incurs costs because it requires an infrastructure within each NICU focused on acquiring and feeding HM. Meanwhile, the healthcare system has limited resources and must allocate them cost-effectively. Economic evaluations compare the costs and benefits of different feeding strategies to estimate which is more likely to be cost-effective (i.e., the lowest cost per unit of benefit) in the NICU. This can provide evidence for policymakers to allocate these limited resources and inform their decisions. By identifying preventable morbidities that are costly and have long-term health consequences for VPIs, society can prioritize interventions based on their impact on reducing the incidence and severity of these morbidities, giving the highest priority to those with the greatest benefit relative to cost.
Prior research has estimated the cost savings associated with feeding HM to VPIs by reducing the incidence of prematurity-related complications (19, 20). Johnson et al. (19–21) and Patel et al. (15, 16) have conducted extensive research on the cost-effectiveness of HM for VPIs. Although there is increasing research exploring the economic analysis of HM for VPIs, there is no systematic review. The aim of this systematic review is to identify, consolidate, and critically appraise published evidence on the economic evaluations of HM for VPIs, to enhance breastfeeding rates among VPIs in the NICU and improve health outcomes for this population.
This systematic review was reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 checklist PRISMA guidelines (22). A comprehensive review protocol, which includes objectives, eligibility criteria, information sources, and search strategies, has been registered with the International Prospective Register of Systematic Reviews (registration number: CRD42024539574). As a systematic review of published studies, ethical approval was not required nor sought.
We included cohort, randomized controlled trials, and case-control studies that examined economic evaluations of HM for VPIs. We excluded reviews, case reports, protocols, comments, case series, expert opinion and editorials. We reviewed the reference lists of the included studies to identify additional studies. The participants, interventions, comparison, outcomes and study design (PICOS) of our studies are listed below.
Participants (P): We included preterm infants born with a gestational age of less than 32 weeks and/or birth weight less than 1,500 g who were admitted to the neonatal ward. We excluded all infants known to have congenital malformations or chromosomal disorders.
Intervention (I): VPIs were fed with HM (mother's own milk, donor milk).
Comparator (s)/control (C): no restrictions on comparator (s). All alternative infant feeding options.
Outcomes (O): Our study examined clinical outcomes related to preterm birth, including NEC, BPD, LOS, ROP, and length of hospital stay. Additionally, we investigated health economic outcomes, including the initial hospitalization cost and the additional cost associated with prematurity-related complications like NEC, LOS, BPD, and ROP. This analysis included cost savings, incremental cost-effectiveness ratio (ICER), Life-Year-Gained, and the additional benefits and costs of interventions aimed at reducing the occurrence and severity of these complications.
Study design (S): Studies have reported various forms of economic evaluation concerning the use of HM to reduce complications in VPIs, including cost analyses, cost-effectiveness analyses (CEA), cost-utility analyses (CUA), cost-benefit analyses (CBA), cost-consequence analysis (CCA), and decision analytic models. CEA compares the costs and outcomes of two or more interventions, where outcomes are measured in natural units (e.g., life-years gained, cases prevented). Its results are often expressed as an ICER, which quantifies the additional cost per additional unit of effect. CUA is a specialized form of CEA that incorporates both the quantity and quality of life into its outcome measurement. Outcomes are typically expressed in quality-adjusted life years (QALYs) or disability-adjusted life years (DALYs), allowing for the comparison of interventions across different health conditions. CBA evaluates interventions by converting both their costs and benefits into monetary terms. This method facilitates a direct comparison of costs and benefits, enabling the calculation of net benefits or benefit-cost ratios to determine whether an intervention's benefits outweigh its costs. CCA presents costs and a variety of outcomes (or consequences) separately, without aggregating them into a single metric. This approach provides a detailed breakdown of different impacts, allowing decision-makers to weigh each outcome according to their own priorities and preferences.
Eligible studies were identified from the following databases: PubMed, Embase, the Cochrane Library, and Web of Science from data inception to April 1, 2024. The databases were searched using key words and Medical Subject Headings (ie, MeSH). Only English-language publications were considered. We manually checked references in the included studies.
The search strategies for the above four databases were developed by the reviewer (A.L.) and reviewed by other reviewers (P.H. and Z.Y.). The full search strategies are detailed in Supplementary File S1.
Two reviewers (A.L. and P.H.) independently screened titles and abstracts against the eligibility criteria. They then obtained the full texts of all potentially relevant publications and reviewed them to assess their compliance with the inclusion criteria. Any discrepancies were resolved through discussion.
The quality of the included studies was evaluated using the Pediatric Quality Appraisal Questionnaire (PQAQ), a comprehensive tool validated for face and content validity, with strong interrater and test–retest reliability for assessing pediatric economic evaluations (23). The PQAQ comprises 57 items across 14 domains: (1) Economic evaluation, (2) Comparators, (3) Target population, (4) Time horizon, (5) Perspective, (6) Costs and resource use, (7) Outcomes, (8) Quality of life, (9) Analysis, (10) Discounting, (11) Incremental analysis, (12) Sensitivity analysis, (13) Conflict of interest, and (14) Conclusions. Of these, 46 items contribute to the study quality rating, with individual item scores assigned between 0 and 1. Based on the PQAQ score, studies were classified into three quality categories with a maximum score of 46: high (>75%), moderate (50%–74%), and low (<50%), as adopted by Sebastian et al. (24). Two authors conducted quality assessments independently, resolving any disagreements through discussion or by consulting a third author.
For each eligible study, two reviewers (A.L. and P.H.) independently extracted data by manually reviewing the included articles using a data extraction form. Z.Y. reviewed the data collected by the two reviewers to rule out any human error. In case of disagreement, a third author (Z.Y.) mediated discussions to reach a consensus. A list of all data entries collected is detailed in Supplementary File S2. Significant heterogeneity was observed among the included studies with respect to interventions, control groups, data sources, types of economic evaluations, study perspectives, price year, and currency. Consequently, a quantitative synthesis was not carried out.
A total of 910 citations were identified through primary literature searches (Supplementary File S1). After removing 253 duplicates, 657 unique citations remained for further screening. Ultimately, 14 studies met the criteria for inclusion in the systematic review. The PRISMA flowchart illustrating the search and screening process is presented in Figure 1, while Table 1 provides a summary of the included studies along with their baseline characteristics (15, 16, 19–21, 25–33). Excluded studies and the reasons for their exclusion are shown in Supplementary File S3. The reviewed studies covered the period from 2012 to 2024 (Table 1). These studies were predominantly conducted in three countries worldwide, with the United States serving as the primary study site, where 85.7% (12/14) of the studies were conducted (Table 1). In terms of study setting, all took place in NICU settings. More than half of the economic evaluations (n = 10) were based on observational studies, whereas four studies (27, 28, 32, 33) employed model-based evaluations. The number of participants in each study varied substantially. For observational studies, this ranged from 64 (25) to 430 (19), while model-based studies included between 207 (32) and 1,000 participants (28).
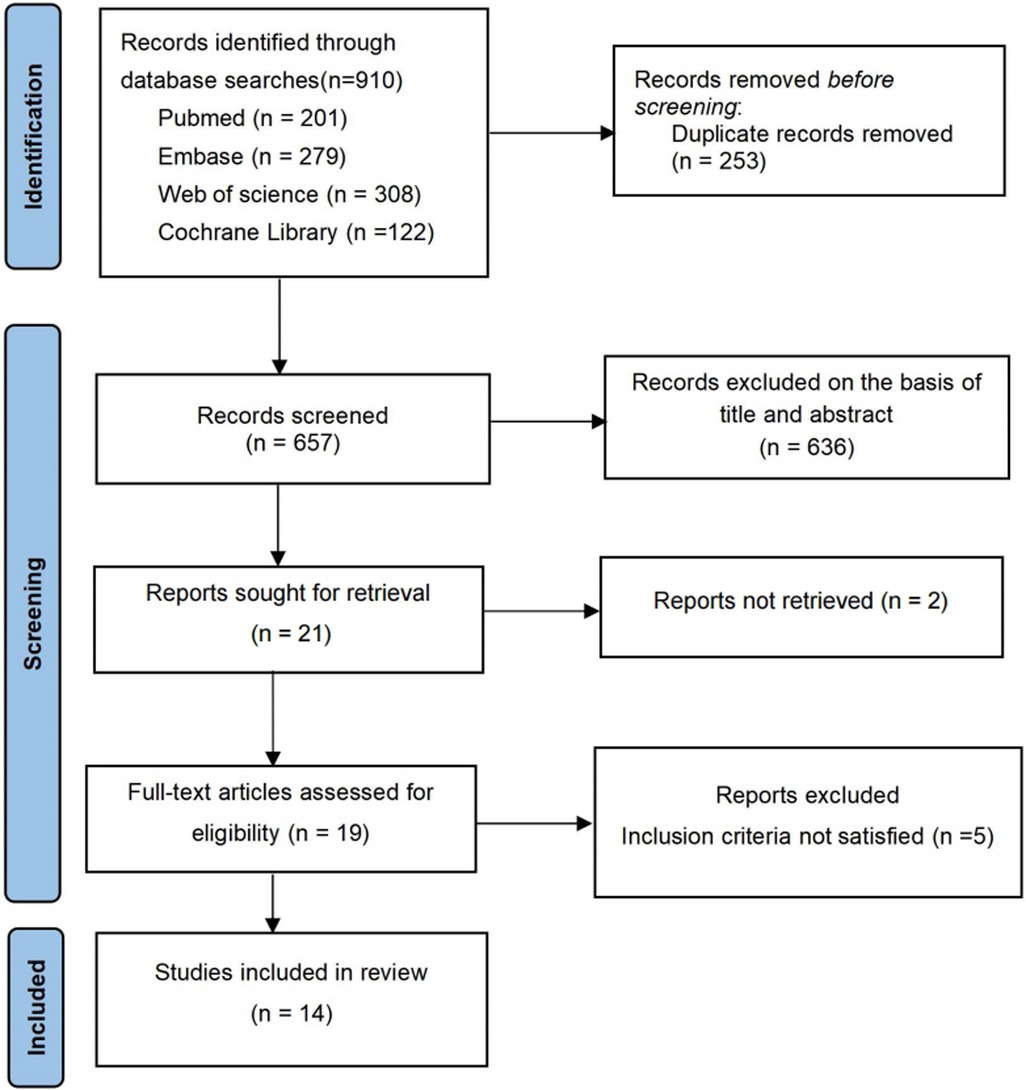
Figure 1. PRISMA flowchart shows the systematic search of the literature.
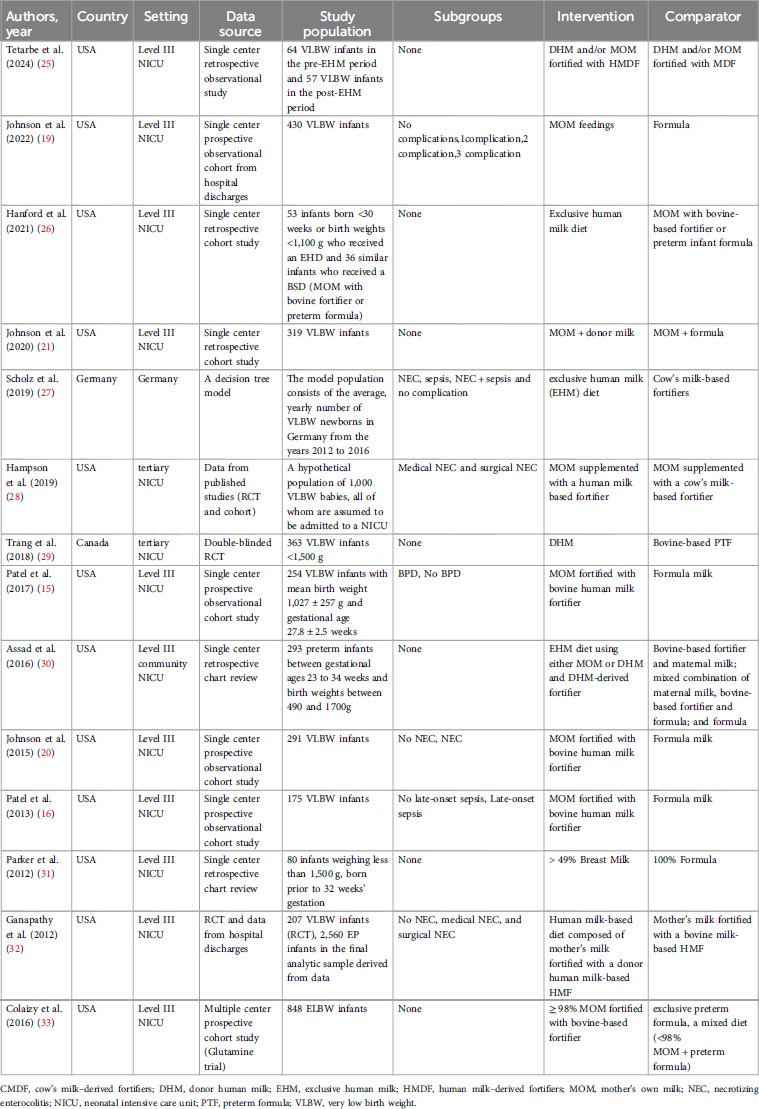
Table 1. Summary of general characteristics of the studies.
One study (29) was evaluated as high quality, while the remaining studies (15, 16, 19–21, 25–28, 30–33) were classified as moderate quality. Further details are provided in Supplementary File S4.
1. NEC: Seven studies (21, 25, 26, 29–31, 33) successfully reported the incidence of NEC in both the intervention and control groups (Table 3). Four studies (21, 29, 30, 33) found a significantly lower incidence of NEC in the intervention group compared to the control group. Johnson et al. (21) reported a significantly lower incidence of NEC during the era of mother's own milk plus donor milk compared to the era of mother's own milk plus formula (1.8% vs. 6.0%, P = 0.048), with fewer infants requiring surgical treatment for NEC in the former. Similarly, Trang et al. (29) observed incidence of NEC stage ≥ I was significantly lower in the DHM group (3.9%) compared to the preterm formula (PTF) group (11.0%). Assad et al. (30) found a lower incidence of NEC in infants fed an exclusively human milk (EHM) diet compared to other groups. Colaizy et al. (33) reported an increased risk of NEC associated with exclusive preterm formula (aOR = 12.1, 95% CI 1.5, 94.2), or a mixed diet (aOR 8.7, 95% CI 1.2–65.2).
2. LOS: Seven studies (16, 21, 25, 26, 29–31) successfully reported the incidence of LOS in both the intervention and control groups (Table 3). Two studies (16, 26) reported a significantly lower incidence of LOS in the intervention group compared to the control group. Hanford et al. (26) found that infants fed an exclusive human diet (EHD) experienced a significant reduction in the rate of late-onset sepsis [7.55% in EHD to 22.22% in the bovine-based standard diet (BSD) group, p = 0.023]. Moreover, an EHD significantly reduced the odds of late-onset sepsis [adjusted odds ratio = 0.323; 95% CI (0.123, 0.768); p = 0.014]. Assad et al. (16) revealed that the increasing the average daily dose of HM (ADDHM) for the first 28 days post birth (ADDHM - Days 1–28) was associated with lower odds of sepsis [odds ratio 0.981, 95% CI (0.967–0.995), P = 0.008].
3. BPD: Five studies (15, 21, 25, 26, 30) documented the incidence of BPD in both the intervention and control groups (Table 3). Among these, one study (15) demonstrated a significantly lower incidence of BPD in the intervention group compared to the control. Patel et al. (15) found a 9.5% reduction in the odds of BPD for every 10% increase in the dose of MOM.
4. ROP: Five studies (21, 25, 26, 29, 30) documented the incidence of ROP in both the intervention and control groups (Table 3). Among these, one study demonstrated a significantly lower incidence of ROP in the intervention group compared to the control group. Hanford et al. (26) found that infants fed an EHD had a significantly reduced rate of severe ROP.
5. NICU length of stay: Eight studies (20, 21, 25, 26, 29–32) have examined the influence of human milk on the duration of hospitalization (Table 3). Of these, five studies (20, 21, 25, 30, 32) suggest that human milk can reduce the length of hospital stay, with reductions ranging from 3.9 days (32) to 6.3 days (25). Nevertheless, three studies (26, 29, 31) found no statistically significant difference in the length of hospital stay between the two groups.
1. Study Design: Six studies (15, 28, 30–33) utilized cost-consequence analysis (CCA), and five studies (19–21, 26, 29) applied cost-effectiveness analysis (CEA), while two studies (16, 25) utilized cost-benefit analysis (CBA). One study (27) utilized cost-utility analysis (CUA). With respect to modelling, one study (32) used a single cost-effectiveness model (assumed to be a decision model); two studies (27, 28) employed a decision tree model; and the fourth used Monte Carlo simulation (33). Studies by Scholz et al. (27), Hampson et al. (28), and Colaizy et al. (33) justified their model choice. The remaining model-based study did not provide any justification for its model choice (32) (Table 2).
2. Analytical Perspectives: All studies clearly reported their study perspective. Eleven studies (15, 16, 19–21, 25, 26, 30–33) evaluated costs solely from the healthcare system perspective. One study evaluated costs solely from a societal perspective (28). Scholz and Greiner (27) evaluated costs from both third-party payer and societal perspectives, while Trang et al. (29) analyzed costs from both the healthcare system and societal perspectives (Table 2).
3. Time Horizon: Among these, eleven studies (15, 16, 19–21, 26, 28, 30–33) adopted a short-term time horizon for evaluating costs and outcomes, extending until neonatal discharge from the hospital. One study (25) spanned a two-year period, one (27) followed a lifelong approach, tracking all costs and outcomes until the death of the cohort entering the model. In addition, Trang et al. (29) focused on the period from birth to 18 months of corrected age. None of these studies justified their choice of time horizon. Thirteen (93%) studies (15, 16, 19–21, 25–27, 29–33) stated the enrolment time frame for the infants (Table 2).
4. Price year/currency: Twelve (15, 16, 19–21, 25–29, 32, 33) (86%) studies specified their price year, while two studies (14%) (30, 31) did not specify a price year. All studies reported their currency.
5. Discount Rate: Twelve (86%) studies did not state a discount rate (15, 16, 19–21, 25, 26, 29–33), whereas two (27, 28) reported using an annual discount rate of 3%, for both costs and benefits as recommended by the US Second Panel on Cost-Effectiveness in Health and Medicine (34) (Table 2).
6. Resource use and costs: The choice of inclusion of a particular type of resource use and cost varied according to the study purpose, perspective, time horizon and the nature of the intervention/comparator being evaluated. Costs tended to be categorized into direct medical care costs [e.g., NICU, NEC treatment (medical and surgical), sepsis and hospitalization costs] (28–30, 32); informal and non-medical care costs (e.g., caregiver transportation and labor market earnings lost) (29, 33); indirect costs incurred by institutions (e.g., administration, human resources and plant operations) (29); societal costs (27–29); enteral feeding costs (29); parenteral feeding costs (25, 26); and resource use and costs of the DHM/other diet provision such as formula milk (detailed information is presented in Table 2) (26, 28, 30, 32).
7. Sensitivity Analysis: Sensitivity analyses were performed in six papers (21, 26–29, 32). Two studies (27, 29) employed deterministic sensitivity analyses, while one study (32) applied one-way and two-way parameter percentage changes to construct an expected cost calculator. Further details are provided in Table 3.
8. Narrative synthesis of economic evaluations: We cannot compare results of economic evaluations that assess health care interventions, which have been conducted in different regions/settings and times. This is due to notable differences in the funding of health care systems, the treatments and care pathways, and baseline population and demographic characteristics around the world. Despite the heterogenous methods of economic evaluations used prohibiting direct comparison between studies, all human milk interventions indicated cost-effective or cost saving results.
Four studies (20, 21, 25, 28) reported cost savings in NICU hospitalizations. Tetarbe et al. (25) reported that EHM feeding led to a cost saving of $1,813,444. Johnson et al. (21) reported that MOM combined with donor milk was associated with $15,555 lower costs per infant (P = 0.045) and saved $1,812 per percentage point decrease in NEC incidence. Hampson et al. (28) demonstrated that EHM diet generated substantial cost savings of $16,309 per infant by reducing adverse clinical events. Johnson et al. (20) indicated that each additional ml (kg. day) of HM during Days 1–14 decreased non-NEC-related NICU costs by $534 (p < 0.001).
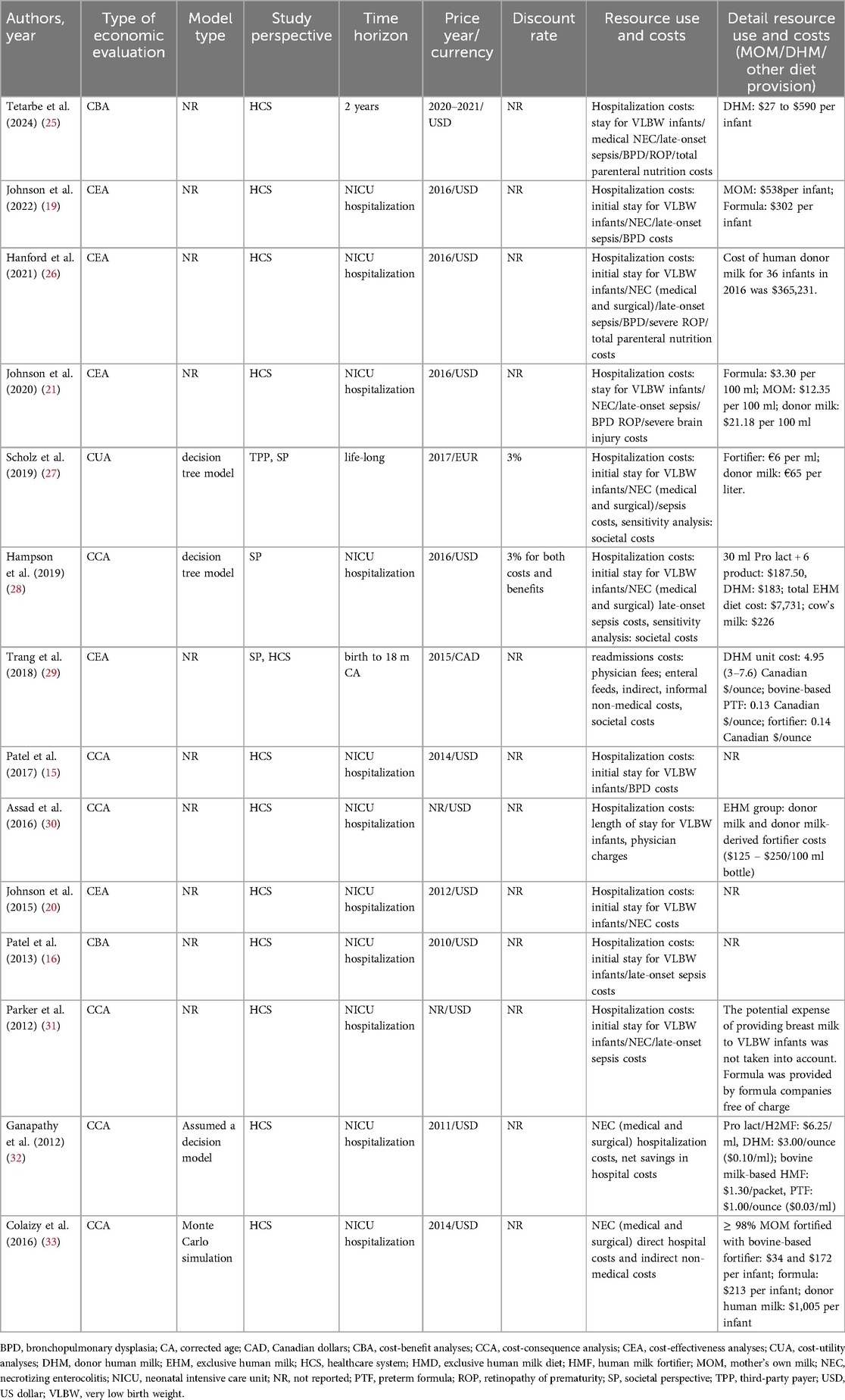
Table 2. Detailed account of the economic evaluation methods — part 1.
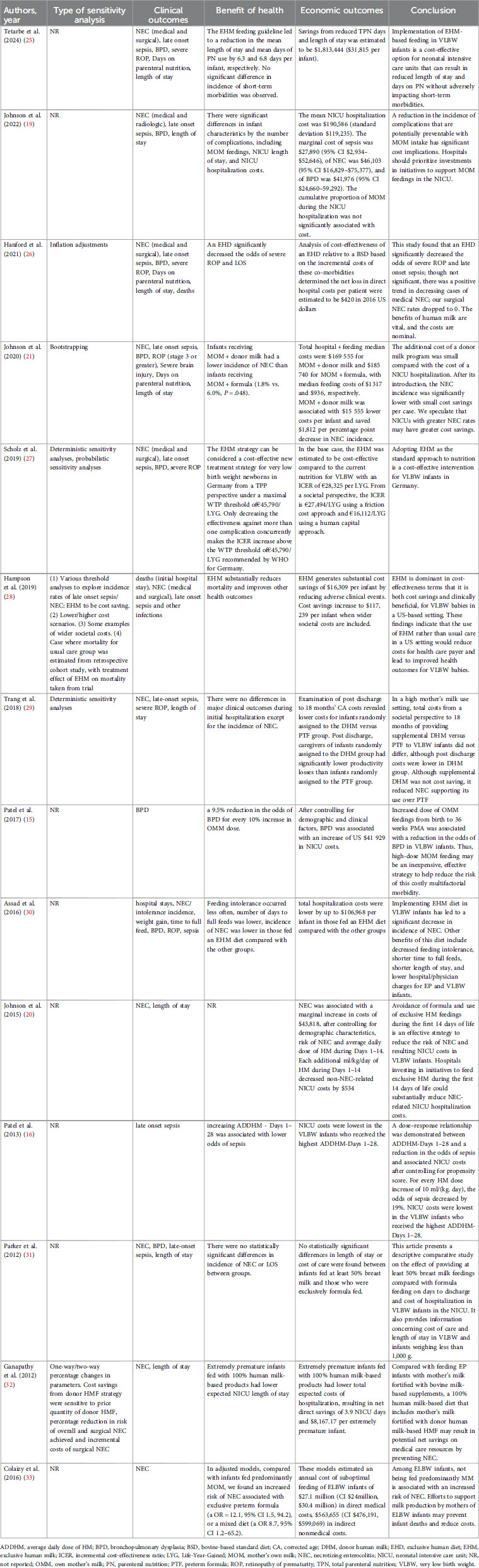
Table 3. Detailed account of the economic evaluation methods — part 2.
Two studies provided marginal costs (19, 20). Johnson et al. (19) reported that the marginal cost of sepsis was $27,890 (95% CI $2,934–$52,646), of NEC was $46,103 (95% CI $16,829–$75,377), and of BPD was $41,976 (95% CI $24,660–59,292). Johnson et al. (20) reported that NEC was associated with a marginal increase in costs of $43,818.
Four studies provided incremental costs (15, 16, 21, 32). Johnson et al. (21) found that NEC was associated with $66,015 greater costs per infant (P < 0.001), and BPD was associated with $74,084 greater costs per infant (P < 0.001). Patel et al. (15) indicated that BPD was associated with an increase of US $41,929 in NICU costs. Patel et al. (16) reported that increasing ADDHM -Days 1–28 was associated with significantly lower NICU costs. Average costs were $31 514 lower for infants with ADDHM-Days 1–28 ≥ 50 ml (kg. day) and $20 384 lower for infants with ADDHM-Days 1–28 25–49.99 ml (kg. day), when compared with infants with ADDHM-Days 1–28 less than 25 ml (kg. day). Ganapathy et al. (32) indicated that the adjusted incremental costs of medical NEC and surgical NEC, over and above the average costs incurred for extremely premature infants without NEC, in 2011 US$, were $74,004 (95%CI, $47,051-$100,957) and $198,040 (95%CI, $159,261-$236,819) per infant, respectively.
Two study offered ICER (27, 29). Scholz et al. (27) found that in the base case, the EHM diet was estimated to be cost-effective compared to the current nutrition for VLBW newborns, with an incremental ICER of €28,325 per Life-Year-Gained. Trang et al. (33) indicated DHM cost an additional $5,328 per case of averted NEC (ICER: $5,328 per case of averted NEC).
9. Generalizability: Four (29%) of the studies reported information regarding the generalizability of their results (15, 16, 28, 29). These studies presented differing perspectives on the generalizability of their findings. Hampson et al. (28) indicated that since the clinical and resource use data are specific to the United States, no strong conclusions on the applicability of their findings to other contexts can be made. However, the cost-saving potential identified in their analysis suggests that further investigation into the cost-effectiveness of an EHM diet in different settings may be warranted. Trang et al. (29) noted that their study, conducted in a single Canadian urban area, may have limited generalizability due to potential variations in maternal milk feeding practices or associated costs in other regions. Similarly, Patel et al. (15) highlighted that their data from a single institution may restrict generalizability, and Patel et al. (16) acknowledged that their single-center study also potentially limits the broader applicability of their findings.
This systematic review is the first to explore the economic evaluations of human milk for VPIs. Fourteen studies from three high-income countries were included. We found that, among the economic evaluations, all HM interventions demonstrated cost-effective or cost saving outcomes. Research indicates a dose-response relationship between HM consumption and the reduction of morbidities, with higher doses leading to greater risk reduction (13, 15, 16). Critical periods during NICU hospitalization, such as the first 10 or 28 days of life, are vital for VPIs to receive high doses of HM (13, 16, 35). Xu et al. found that a daily threshold of ≥50 ml (kg. day) of HM in the first 4 weeks of life was linked to lower incidence of various complications in very low birth weight (VLBW) infants, including BPD, NEC, LOS, and extrauterine growth restriction (13). HM is recommended as the primary nutritional source for NICU patients, particularly VLBW infants at high risk for complications (36). Promoting breastfeeding in critical care settings is associated with greater health benefits and lower costs compared to preterm infant formula, suggesting potential cost-effectiveness (37).
Johnson et al. (38) highlighted the economic benefits of HM feeding during NICU hospitalization; however, they did not perform a systematic evaluation. Buckle et al. (39) reviewed the cost and cost-effectiveness of donor human milk (DHM) specifically for the prevention of necrotizing enterocolitis (NEC), concentrating primarily on this single outcome. Their findings suggested that DHM use is likely cost-effective; nonetheless, they recommended that comprehensive economic evaluations comparing DHM with standard feeding protocols in infants are necessary to strengthen the evidence base. Similarly, Zanganeh et al. (40) conducted a systematic review of economic evaluations regarding DHM vs. standard feeding in infants, focusing exclusively on DHM. They reported that DHM interventions consistently yielded cost-effective or cost-saving results and proposed that future studies should provide more detailed insights into the long-term costs and outcomes associated with DHM. In contrast, our review examines the association between HM feeding and very preterm infants from both clinical and health economics perspectives.
NEC is a severe, inflammation-related morbidity affecting approximately 7% of VLBW infants (41). NEC not only prolongs NICU hospitalization but also raises daily NICU costs due to the utilization of expensive pharmaceutical products, therapies, surgeries, and other services, resulting in an additional cost of $66,015 per infant (21). The incremental cost of NEC varies from $43,818 (20) to $46,103 (19) per infant and $223 per day (95% CI: $100–$346) (19). Evidence indicates that HM may be cost-saving or cost-effective in the context of NEC among preterm infants, although the economic impact may differ across settings (21, 29, 30). The use of donor milk was associated with a saving of $1,812 per percentage point reduction in NEC incidence (21), while DHM incurred an additional cost of $5,328 per averted NEC case (29).
NICU hospitalization costs attributable to LOS range from $17,822 to $27,890 (in 2016 US$) (19, 26). One study demonstrated a strong causal relationship between LOS and MOM feedings (19). Higher doses and longer durations of MOM during NICU hospitalization are associated with reduced risks of sepsis (16) and significant cost savings with institutional investments in MOM feedings (19). A 19% reduction in the odds of developing sepsis is observed for every 10 ml (kg. day) increase in the average daily dose of HM during Days 1–28 (16).
Both HM and DHM significantly decrease the incidence of BPD compared to preterm formula (30, 42). Even when the amount of HM is insufficient, feeding more than 50% of the total volume still offers protective effects against BPD. There is a dose-dependent relationship between MOM consumed in the NICU and BPD occurrence, influencing associated healthcare costs (13). For every 10% increase in the proportion of MOM, the odds of BPD were reduced by 9.5% (15).
The incremental cost associated with severe ROP was $39,344 for an infant born at 27 weeks' gestational age (26). After adjusting for sex, race, gestational age, and birth weight, infants who received EHD demonstrated a significant 65.1% decrease in the odds of severe ROP compared to those fed a bovine-based standard diet (30).
Our study focused on research that addressed both preterm-related complications and health economics, excluding studies that solely examined the relationship between HM and preterm-related complications. Limited data is available on the positive effects of HM feeding on these conditions.
NICU hospitalization costs include physician costs, nursing costs, respiratory costs, transfusion costs, and procedure costs, among others (3). Rios et al. (3) obtained patient resource use data from the Canadian Neonatal Network database. Cost estimates were generated by matching patient resource use data to the appropriate unit costs. All cost estimates were calculated from the perspective of a provincial public payer. The median cost of NICU hospitalization was estimated at $30,572 ($16,597-$51,857) (in 2017 Canadian dollars) for infants with a gestational age of 29–32 weeks and $100,440 ($56,858-$159,386) (in 2017 Canadian dollars) for those with a gestational age of less than 29 weeks. Johnson et al. (19) reported that the mean NICU hospitalization cost of VPIs was $190,586 (in 2016 US$).
Most included studies suggest that human milk feedings can decrease NICU hospitalization costs for VPIs. HM feedings are cost-effective, although different studies have yielded varied conclusions regarding the incidence rates of various complications in preterm infants. HM feedings may also have a direct impact on healthcare costs independent of their association with morbidities such as LOS, NEC, BPD, and ROP. One study evaluated the direct relationship between the dose of HM and healthcare costs, after controlling for the presence of one or more morbidities (16). The study found significantly lower NICU hospitalization costs with higher doses of HM, defined as ml (kg. day), in the first 28 days post-birth.
To ensure an adequate milk supply, NICUs must bear the cost of acquiring HM. Johnson et al. (21) found that the mean cost per 100 ml was $3.30 for formula, $12.35 for MOM, and $21.18 for donor milk (in 2016 US dollars). However, the subsequent direct and indirect cost savings from HM feedings likely far outweigh the hospital's expenses for acquiring HM in most instances. Scholz et al. (27) used a decision tree model to calculate the cost-effectiveness of the EHM diet and found that adopting EHM diet as the standard approach to nutrition is a cost-effective intervention for VLBW newborns in Germany. Hampson et al. (28) conducted an economic analysis of EHM diet compared to cow's milk among VLBW babies in the US and found that an EHM diet is dominant in cost-effectiveness terms; it is both cost-saving and clinically beneficial for VLBW babies in a US-based setting.
The majority of the studies reported clinical outcome measures (e.g., incidence of NEC). Only one of the fourteen studies (27) reported health-related outcome measures (e.g., Life-Year-Gained) commonly used in economic evaluations. Six studies (15, 28, 30–33) applied a CCA approach with costs savings as an outcome; this approach is considered a type of cost-benefit analysis. Consideration of a broader range of outcomes beyond the health sector allows for inclusion of benefits and costs from multiple sectors.
Model-based evaluations offer the opportunity to improve the generalizability of findings and evaluate the longer-term costs and benefits of HM. These evaluations are critical as policy-making tools, often informing resource allocation decisions. One of the model-based studies provided data over a longer time horizon (27). However, one study did not explicitly mention procedures for model validation (32). Moreover, the clinical and resource utilization data are specific to a single country. Therefore, the applicability of findings to other settings, particularly from high-income to low-income countries, may be limited.
Many evaluations in this review lacked the application of a discount rate. The majority of studies utilized a short-term horizon to evaluate costs and outcomes, extending until neonatal discharge from the hospital, and thus may not accurately reflect longer term health effects or consider all aspects of economic evaluations. The methods for collecting resource utilization and types of costs included varied across studies. The majority of the studies did not report which cost components were excluded from their analyses. Future studies should clearly specify which costs are included and excluded. Four studies (27–29, 33) included informal and non-medical care costs, as well as indirect and societal costs. It is considered good practice to report findings both including and excluding informal and indirect costs. Incorporating these types of costs (e.g., costs incurred by families) may influence management recommendations. To determine the macroeconomic benefits of HM in reducing the incidence of NEC, BPD and LOS, an analysis of lifetime costs would be useful. However, a lifetime model comparing the economic impact of HM to formula feeding would require significant assumptions, potentially introducing high uncertainty. Establishing causality in this area is particularly challenging and requires substantial data, which may not be available.
Economic evaluations inherently contain some degree of uncertainty. To assess this uncertainty, various sensitivity analyses can be applied to evaluate how sensitive results are to uncertain parameters. The selection of sensitivity analysis method may depend on the methodology, type of economic evaluation (trial-based or model-based), or the intervention's setting. Notably, six studies (21, 26–29, 32) conducted sensitivity analyses to assess the robustness of their results.
While all HM interventions reviewed appear cost-effective or even cost-saving, variation exists based on intervention design. The narrative synthesis of economic evaluations, including appraisal of applied methods and assessment of study quality, provides valuable insights for health economists, modelers, and future research directions in this field.
Our systematic review has several strengths. Firstly, it is the first comprehensive analysis of economic evaluations of HM for VPIs. Secondly, we employed a thorough search strategy that spanned multiple databases and included additional reference checks to encompass a wide range of relevant published studies. Thirdly, we strictly followed PRISMA guidelines for duplicate screening, data extraction, and quality assessment.
Despite the use of scientific and systematic methods to minimize deviations, it is important to acknowledge several limitations in this study. Firstly, quantitative synthesis was not carried out due to significant heterogeneity across studies. While most studies focused on medical costs, some provided detailed cost breakdowns while others did not, limiting quantitative analysis and horizontal comparison. The definitions of complications associated with preterm infants are not standardized. For example, in the case of NEC, most studies (19, 21, 25) use Bell stage II or higher, some use medical and surgical classifications (26), and others use ICD codes (27). Most included studies do not provide detailed information on the dosage, proportion, and duration of maternal or donor breast milk, making cross-study comparisons infeasible. Therefore, a qualitative summary of evidence was conducted with cautious interpretation of outcomes. However, current published studies are informative and provide the basis for further research on economic evaluations of human milk for very preterm infants. Furthermore, all included studies only considered medical costs, neglecting maternal opportunity costs due to time spent pumping and other costs incurred by the mother. Future research should explore economic evaluations from a societal perspective. Additionally, it is important to note that the included studies were conducted in countries with ample medical resources, so generalizing these findings to countries with limited resources should be done cautiously, as costs and payer arrangements may vary across different economic levels.
This study represents the first systematic review on the economic evaluations of human milk for very preterm infants. This systematic review suggests that economic evaluation of HM for VPIs is an expanding area of research, and current economic evaluations are mainly set in developed countries. The findings suggest that human milk for very preterm infants yield significant economic benefits during critical periods of NICU hospitalization. Optimizing human milk feedings in the NICU emerges as a cost-effective strategy for enhancing infant health outcomes in this highly vulnerable patient population. There was considerable heterogeneity and deficiencies in the included studies. Standardized and high-quality studies are needed to determine the cost-effectiveness of human milk for very preterm infants in the future.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
AL: Data curation, Writing – original draft, Writing – review & editing, Conceptualization. PH: Data curation, Formal analysis, Methodology, Writing – review & editing. XG: Data curation, Formal analysis, Methodology, Writing – review & editing. LZ: Data curation, Formal analysis, Methodology, Writing – review & editing. LB: Data curation, Methodology, Validation, Writing – review & editing. RX: Data curation, Methodology, Validation, Writing – review & editing. ZY: Conceptualization, Supervision, Validation, Writing – review & editing. HT: Conceptualization, Supervision, Validation, Writing – review & editing. GH: Conceptualization, Supervision, Validation, Writing – review & editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
We thank the Shenzhen Neonatal Data Network (SNDN) for providing a learning and working platform for producing this review. And we thank all the authors whose studies were included in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1534773/full#supplementary-material
1. Ohuma EO, Moller AB, Bradley E, Chakwera S, Hussain-Alkhateeb L, Lewin A, et al. National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis. Lancet. (2023) 402:1261–71. doi: 10.1016/S0140-6736(23)00878-4
2. Waitzman NJ, Jalali A, Grosse SD. Preterm birth lifetime costs in the United States in 2016: an update. Semin Perinatol. (2021) 45:151390. doi: 10.1016/j.semperi.2021.151390
3. Rios JD, Shah PS, Beltempo M, Louis D, Mukerji A, Premji S, et al. Costs of neonatal intensive care for Canadian infants with preterm birth. J Pediatr. (2021) 229:161–167.e12. doi: 10.1016/j.jpeds.2020.09.045
4. Phibbs CS, Schmitt SK, Cooper M, Gould JB, Lee HC, Profit J, et al. Birth hospitalization costs and days of care for mothers and neonates in California, 2009–2011. J Pediatr. (2019) 204:118–125.e14. doi: 10.1016/j.jpeds.2018.08.041
5. Bell EF, Hintz SR, Hansen NI, Bann CM, Wyckoff MH, DeMauro SB, et al. Mortality, in-hospital morbidity, care practices, and 2-year outcomes for extremely preterm infants in the US, 2013–2018. JAMA. (2022) 327:248–63. doi: 10.1001/jama.2021.23580
6. Cao Y, Jiang S, Sun J, Hei M, Wang L, Zhang H, et al. Assessment of neonatal intensive care unit practices, morbidity, and mortality among very preterm infants in China. JAMA Netw Open. (2021) 4:e2118904. doi: 10.1001/jamanetworkopen.2021.18904
7. Hebballi NB, Avritscher EB, Garcia E, Bain A, Bartz-Kurycki MA, Tsao K, et al. Healthcare utilization among infants discharged from the neonatal intensive care unit: a descriptive cost analysis. Health Serv Insights. (2023) 16:11786329231169604. doi: 10.1177/11786329231169604
8. Ames SR, Lotoski LC, Azad MB. Comparing early life nutritional sources and human milk feeding practices: personalized and dynamic nutrition supports infant gut microbiome development and immune system maturation. Gut Microbes. (2023) 15:2190305. doi: 10.1080/19490976.2023.2190305
9. Peng W, Han J, Li S, Zhang L, Yang C, Guo J, et al. The association of human milk feeding with short-term health outcomes among Chinese very/extremely low birth weight infants. J Hum Lact. (2022) 38:670–7. doi: 10.1177/08903344221078237
10. Xiong X, Wang Y, Chen X, Lin B, Zhuang Y, Luo L, et al. Mixed feedings and necrotizing enterocolitis: the proportion of human milk matters. Breastfeed Med. (2023) 18:469–74. doi: 10.1089/bfm.2022.0268
11. Thatrimontrichai A, Surachat K, Singkhamanan K, Thongsuksai P. Long duration of oral care using mother’s own milk influences oral Microbiota and clinical outcomes in very-low-birthweight infants: randomized controlled trial. Pediatr Infect Dis J. (2023) 42:804–10. doi: 10.1097/INF.0000000000004002
12. Verd S, Porta R, Ginovart G, Avila-Alvarez A, García-Muñoz RF, Izquierdo RM, et al. Human milk feeding is associated with decreased incidence of moderate-severe bronchopulmonary dysplasia in extremely preterm infants. Children (Basel). (2023) 10:1267. doi: 10.3390/children10071267
13. Xu Y, Yu Z, Li Q, Zhou J, Yin X, Ma Y, et al. Dose-dependent effect of human milk on bronchopulmonary dysplasia in very low birth weight infants. BMC Pediatr. (2020) 20:522. doi: 10.1186/s12887-020-02394-1
14. Zhou J, Shukla VV, John D, Chen C. Human milk feeding as a protective factor for retinopathy of prematurity: a meta-analysis. Pediatrics. (2015) 136:e1576–86. doi: 10.1542/peds.2015-2372
15. Patel AL, Johnson TJ, Robin B, Bigger HR, Buchanan A, Christian E, et al. Influence of own mother’s milk on bronchopulmonary dysplasia and costs. Arch Dis Child Fetal. (2017) 102:F256–61. doi: 10.1136/archdischild-2016-310898
16. Patel AL, Johnson TJ, Engstrom JL, Fogg LF, Jegier BJ, Bigger HR, et al. Impact of early human milk on sepsis and health-care costs in very low birth weight infants. J Perinatol. (2013) 33:514–9. doi: 10.1038/jp.2013.2
17. Parker MG, Stellwagen LM, Noble L, Kim JH, Poindexter BB, Puopolo KM. Promoting human milk and breastfeeding for the very low birth weight infant. Pediatrics. (2021) 148(5):e2021054272. doi: 10.1542/peds.2021-054272
18. Parker MG, Greenberg LT, Edwards EM, Ehret D, Belfort MB, Horbar JD. National trends in the provision of human milk at hospital discharge among very low-birth-weight infants. JAMA Pediatr. (2019) 173:961–8. doi: 10.1001/jamapediatrics.2019.2645
19. Johnson TJ, Patel AL, Schoeny ME, Meier PP. Cost savings of mother’s own milk for very low birth weight infants in the neonatal intensive care unit. Pharmacoecon Open. (2022) 6:451–60. doi: 10.1007/s41669-022-00324-8
20. Johnson TJ, Patel AL, Bigger HR, Engstrom JL, Meier PP. Cost savings of human milk as a strategy to reduce the incidence of necrotizing enterocolitis in very low birth weight infants. Neonatology. (2015) 107:271–6. doi: 10.1159/000370058
21. Johnson TJ, Berenz A, Wicks J, Esquerra-Zwiers A, Sulo KS, Gross ME, et al. The economic impact of donor milk in the neonatal intensive care unit. J Pediatr. (2020) 224:57–65. e4. doi: 10.1016/j.jpeds.2020.04.044
22. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ Brit Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
23. Ungar WJ, Santos MT. The pediatric quality appraisal questionnaire: an instrument for evaluation of the pediatric health economics literature. Value Health. (2003) 6:584–94. doi: 10.1046/j.1524-4733.2003.65253.x
24. Sebastian E, Bykersma C, Eggleston A, Eddy KE, Chim ST, Zahroh RI, et al. Cost-effectiveness of antenatal corticosteroids and tocolytic agents in the management of preterm birth: a systematic review. EClinicalMedicine. (2022) 49:101496. doi: 10.1016/j.eclinm.2022.101496
25. Tetarbe M, Chang MR, Barton L, Cayabyab R, Ramanathan R. Economic and clinical impact of using human milk-derived fortifier in very low birth weight infants. Breastfeed Med. (2024) 19:114–9. doi: 10.1089/bfm.2023.0163
26. Hanford J, Mannebach K, Ohler A, Patten M, Pardalos J. Rates of comorbidities in very low birth weight infants fed an exclusive human milk diet versus a bovine supplemented diet. Breastfeed Med. (2021) 16:814–20. doi: 10.1089/bfm.2020.0345
27. Scholz SM, Greiner W. An exclusive human milk diet for very low birth weight newborns-A cost-effectiveness and EVPI study for Germany. PLoS One. (2019) 14:e0226496. doi: 10.1371/journal.pone.0226496
28. Hampson G, Roberts S, Lucas A, Parkin D. An economic analysis of human milk supplementation for very low birth weight babies in the USA. BMC Pediatr. (2019) 19:337. doi: 10.1186/s12887-019-1691-4
29. Trang S, Zupancic J, Unger S, Kiss A, Bando N, Wong S, et al. Cost-effectiveness of supplemental donor milk versus formula for very low birth weight infants. Pediatrics. (2018) 141(3):e20170737. doi: 10.1542/peds.2017-0737
30. Assad M, Elliott MJ, Abraham JH. Decreased cost and improved feeding tolerance in VLBW infants fed an exclusive human milk diet. J Perinatol. (2016) 36:216–20. doi: 10.1038/jp.2015.168
31. Parker LA, Krueger C, Sullivan S, Kelechi T, Mueller M. Effect of breast milk on hospital costs and length of stay among very low-birth-weight infants in the NICU. Adv Neonat Care. (2012) 12:254–9. doi: 10.1097/ANC.0b013e318260921a
32. Ganapathy V, Hay JW, Kim JH. Costs of necrotizing enterocolitis and cost-effectiveness of exclusively human milk-based products in feeding extremely premature infants. Breastfeed Med. (2012) 7:29–37. doi: 10.1089/bfm.2011.0002
33. Colaizy TT, Bartick MC, Jegier BJ, Green BD, Reinhold AG, Schaefer AJ, et al. Impact of optimized breastfeeding on the costs of necrotizing enterocolitis in extremely low birthweight infants. J Pediatr. (2016) 175:100–105.e2. doi: 10.1016/j.jpeds.2016.03.040
34. Sanders GD, Neumann PJ, Basu A, Brock DW, Feeny D, Krahn M, et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA. (2016) 316:1093–103. doi: 10.1001/jama.2016.12195
35. Corpeleijn WE, Kouwenhoven SM, Paap MC, van Vliet I, Scheerder I, Muizer Y, et al. Intake of own mother’s milk during the first days of life is associated with decreased morbidity and mortality in very low birth weight infants during the first 60 days of life. Neonatology. (2012) 102:276–81. doi: 10.1159/000341335
36. Santacruz-Salas E, Aranda-Reneo I, Hidalgo-Vega Á, Blanco-Rodriguez JM, Segura-Fragoso A. The economic influence of breastfeeding on the health cost of newborns. J Hum Lact. (2019) 35:340–8. doi: 10.1177/0890334418812026
37. Camacho EM, Hussain H. Cost-effectiveness evidence for strategies to promote or support breastfeeding: a systematic search and narrative literature review. BMC Pregnancy Childb. (2020) 20:757. doi: 10.1186/s12884-020-03460-3
38. Johnson TJ, Patel AL, Bigger HR, Engstrom JL, Meier PP. Economic benefits and costs of human milk feedings: a strategy to reduce the risk of prematurity-related morbidities in very-low-birth-weight infants. Adv Nutr. (2014) 5:207–12. doi: 10.3945/an.113.004788
39. Buckle A, Taylor C. Cost and cost-effectiveness of donor human milk to prevent necrotizing enterocolitis: systematic review. Breastfeed Med. (2017) 12:528–36. doi: 10.1089/bfm.2017.0057
40. Zanganeh M, Jordan M, Mistry H. A systematic review of economic evaluations for donor human milk versus standard feeding in infants. Matern Child Nutr. (2021) 17:e13151. doi: 10.1111/mcn.13151
41. Alsaied A, Islam N, Thalib L. Global incidence of necrotizing enterocolitis: a systematic review and meta-analysis. BMC Pediatr. (2020) 20:344. doi: 10.1186/s12887-020-02231-5
Keywords: human milk, preterm infants, cost-effectiveness, economic evaluation, health outcomes
Citation: Lu A, Huang P, Guo X, Zhu L, Bi L, Xing R, Yu Z, Tang H and Huang G (2025) Economic evaluations of human milk for very preterm infants: a systematic review. Front. Pediatr. 13:1534773. doi: 10.3389/fped.2025.1534773
Received: 26 November 2024; Accepted: 10 March 2025;
Published: 20 March 2025.
Edited by:
Valeria Calcaterra, University of Pavia, ItalyReviewed by:
Adora Okogbule-Wonodi, Howard University, United StatesCopyright: © 2025 Lu, Huang, Guo, Zhu, Bi, Xing, Yu, Tang and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guosheng Huang, aHVhbmcyNDU2NzlAc2luYS5jb20=; Hong Tang, c3VwZXJ5aWN0QDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.