 Liangru Guo
Liangru Guo Hengwang He1
Hengwang He1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr. , 11 March 2025
Sec. Social Pediatrics
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1532035
This article is part of the Research Topic Health benefit and promotion of 24-hour movement behaviors in children and adolescents View all 4 articles
Objective: This systematic evaluation and meta-analysis [PROSPERO CRD42024598218] was conducted in order to summarise the effectiveness of a body of school-based behavioural interventions on physical activity (PA) and sedentary behaviour in children and adolescents.
Methods: We conducted a systematic search of the literature up to November 2024 using PubMed, Web of Science and SCOPUS. The methodological quality of the included literature was assessed using the Cochrane Risk Assessment Tool.
Results: Of the 6,071 search records initially identified, 26 studies were considered eligible for systematic evaluation and meta-analysis. School-based behavioural interventions were effective in increasing moderate-intensity physical activity [standardised mean difference (SMD), 0.18 (95% CI, 0.04–0.31), p = 0.01]. School-based behavioural interventions failed to reduce ST (sedentary time) [−0.04 (95% CI, −0.08 to −0.01), p = 0.12] and failed to improve low-intensity PA (LPA) [0.18 (95% CI, −0.07–0.44), p = 0.16]. Subgroup analyses showed that school-based behavioural interventions were more effective in improving moderate-intensity PA in children and adolescents who were in school [0.46 (95% CI, 0.20–0.72), p = 0.02]. School-based behavioral interventions do not differentiate moderate-intensity physical activity among children and adolescents of different ages, [0.18 (95% CI, 0.05–0.31), p = 0.1], nor do they make a difference in moderate-intensity physical activity among children and adolescents in different regions [0.18 (95% CI, 0.04–0.31), p = 0.12].
Conclusion: School-based behavioural interventions are effective in increasing moderate-intensity PA among children and adolescents, particularly those who were in school.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/recorddashboard, PROSPERO [CRD42024598218].
Sedentary behaviours (SB)are typically defined by both low energy expenditure [e.g., resting metabolic rate, typically ≤1.5 metabolic equivalents (METs)] and a sitting or reclining posture (1–3). Sedentary time (ST) is a quantitative indicator of S B and is used to measure the duration of an individual's sitting, reclining, or lying in a low energy expenditure (≤1.5 METs) position (4). Increasing evidence of research demonstrates that both participation in physical activity (PA) and reduction in ST are associated with a number of positive outcomes and benefits to children's health (e.g., self-esteem, well-being, cardiometabolic health, good sleep, etc.) (5). Lack of PA has a significant negative impact on health, contributing to more than 5 million deaths per year globally (6). Excessive ST has been shown to be associated with physical and mental health problems, such as poor body composition, low self-esteem and anti-social behaviours, and reduced academic performance in school-aged children and adolescents (7). Yet globally, more than 85% of children and adolescents do not meet the World Health Organization (WHO) guidelines on PA (8), which suggest that children and adolescents engage in at least 60 min of moderate - to - vigorous - intensity PA (MVPA) daily (8). Additionally, the WHO recommends limiting recreational screen time to no more than 2 h per day to reduce sedentary behaviour and promote healthier lifestyles (9). Therefore, regularly participating in daily MVPA during childhood and adolescence while reducing the chances of ST remains a major challenge in public health (10, 11).
School is an ideal place to promote healthy behaviours in children and adolescents as it is where they spend more than half of their waking hours each day. Children and adolescents have multiple opportunities to be physically active during the last school day, including breaks, sports, physical education classes, and active commuting to and from school. Findings on the impact of school-based interventions on PA levels in children and adolescents have been inconsistent, with school-based PA interventions appearing to have no (12) or only small positive effects (13, 14). Yet other research suggests that interventions targeting these discrete periods of schooling may be effective in increasing children's PA levels (15, 16). Regarding the effectiveness of school-based PA and ST interventions, early studies have mostly relied on self-report measures, which have limited validity and may be differentially biased in subpopulations (17, 18). As research has progressed, more and more studies have begun to use objective measurement tools such as accelerometers to assess PA and ST (1, 19). School-based PA interventions are implemented in a variety of school settings and are often complex, multi-component programmes. It is unclear which school-based strategies are most effective in promoting healthy lifestyles among children and adolescents. Therefore, to fill these gaps in the scientific literature, the present systematic evaluation and meta-analysis aimed to (1) assess the overall effectiveness of school-based interventions (i.e., daily MVPA, ST, and LPA), and (2) investigate the impact of these rates of effectiveness at different ages, in different regions, and during in-school and out-of-school periods.
This systematic review is registered with Prospero, the International Prospective Registry for Systematic Reviews (registration number: CRD42024598218). We conducted this systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
The databases PubMed/MEDLINE, EBSCOhost, Cochrane Library and Web of Science (Core Collection) were consulted for literature from their inception to 11 November 2024. In addition, Scopus has been added to ensure a more comprehensive literature search, as Scopus includes a wider range of journals, particularly in the areas of public health and behavioural sciences. A Medical Subject Headings (MeSH) search was performed to establish all relevant literature about this study. In addition, we conducted a reference tracking of published trials and meta-analysis reviews in the field to ensure inclusion of all relevant studies. Specifically, we used the following MeSH terms including “School-Based Services” or “School Health Promotion”. “exercise” or “physical activity” or “training”, “sedentary” or “sedentary time”, and “school-based services” or “school health promotion”, or “sedentary time” or “sedentary lifestyle”, “child” or “child care”, or “children”, “adolescent” or “adolescents”. Detailed search strategies are shown in Supplementary Table S1.
Inclusion criteria were determined according to the PICOS (Population, Intervention, Comparison, Outcome and Study Design) methodology. Studies were included if the following criteria were met: (1) Type of participants: school-aged children and adolescents (5–18 years old). A study was considered eligible if the average age of the participants falls 5–18 years, regardless of the age range of the study samples. (2) Type of intervention: behavioural intervention in a school setting or school-based behavioural interventions included all types of exercise, such as brisk walking, strength training, and yoga. There were no clear requirements for frequency, intensity, or duration of the intervention. Interventions could be categorised as single or multiple group interventions. (3) Type of control group: the control group does not receive any interventions or non-exercise interventions, or receives routine care not involving medical treatment. (4) Type of outcome: mainly including moderate-intensity PA, SB and low-intensity PA. For types of sedentary behaviour, one or more of the following were included: accelerometer-based total sedentary time (assuming ≤100 activity counts as sedentary), self-reported total sedentary time (total sedentary time was used as a proxy measure for total sedentary time in most self-reported methods), screen time (e.g., watching TV, using a computer), occupationally sedentary behaviour (e.g., attending lectures, private study time), or passive transportation) or passive transport. Sedentary behaviours were reported as summary point estimates (e.g., average minutes/hour per day) or as proportions (e.g., percentage of the sample sitting for more than 6 h per day). (5) Type of study design: we included peer-reviewed and English-written randomized controlled trials (RCTs) non-randomized controlled trials, and quasi-experimental designs. Exclusion criteria: (1) Reviews, letters, editorial comments, case reports, conference abstracts, unpublished articles and non-English articles. (2) Studies whose results were not quantified or lacked appropriate outcome indicators. (3) Literature that was not available in full text through all available channels and methods. (4) Articles with poor research quality and no access to quality information. (5) Literature without a control group.
All retrieved literature was imported into EndNote software for de-duplication, and then the title, abstract, and full text were read independently by two researchers (LRG and HWH) for literature screening. When disagreements arose, the final results were determined by consensus with the two researchers. Based on the literature screening, the two researchers used a Microsoft Excel spreadsheet to extract and code literature information from the trials. The information for each trial included the first author, country, year of publication, study population, intervention content, intervention protocol (single exercise duration, frequency, and intervention period), measurement tools, and outcome indicators. The methods used to extract the data are described below.
(1) We extracted the mean, standard deviation, and sample size reported for each group before and after the intervention. We combined each outcome indicator using pre- and post-intervention differences (M ± SD). The first step was to calculate the mean difference (the raw mean difference between post-intervention and pre-intervention figures for each intervention group) (20):
where, MDdiff is the raw mean difference, Mpost is the reported post-intervention mean, and Mpre is the reported pre-intervention mean (20).
where, CIhigh is the upper limit of the confidence interval, CIlow is the lower limit of the confidence interval, and t is the t-distribution with N - 1 degrees of freedom in the corresponding confidence interval (20).
(2) The standard deviation of the mean difference (SDdiff) (20) is calculated as follows:
The Cochrane Risk of Bias Tool is used to assess the quality of eligible trials. The focus was on: (1) whether random sequence was generated; (2) whether the allocation protocol was hidden; (3) whether subjects and staff were blinded; (4) whether the assessment of outcome data was blinded; (5) completeness of outcome data; (6) selective reporting of study results; and (7) other sources of bias. Each item was assessed on a three-tiered scale of bias risk, i.e., low risk of bias, unclear risk of bias, and high risk of bias. Each study was assessed as a whole based on the indicators of the 6 items, which were rated on a three-tiered scale of bias risk, i.e., low risk of bias, moderate risk of bias and high risk of bias, and the risk of bias map was generated by the software Review Manager 5.3. Quality assessment was carried out independently by two researchers, and any disagreements were resolved through discussion with a third person.
Evidence synthesis was performed in Review Manager 5.3 (Cochrane Collaboration, Oxford, U.K.). MVPA, LPA, and ST were analysed using continuous variables. All indicators were reported with 95% confidence intervals (CI). Heterogeneity in the study was assessed by the chi-square (χ2) test (Cochran's Q) and the index of inconsistency (I2) (21, 22). χ2 p < 0.05 or I2 > 50% was considered significant heterogeneity. When significant heterogeneity was detected, a random-effects model was used. Otherwise, a fixed-effects model was applied. Funnel plots were created by Review Manager 5.3 (Cochrane Collaboration, Oxford, UK). Their outcomes were assessed in at least two included RCTs. Sensitivity analyses were applied to the literature of the included studies to test the reliability of the findings. The presence of a significant effect of each article on the combined effect was tested by removing one article at a time.
A total of 6,701 studies were identified from the three databases searched. After 3,577 duplicates were removed, 102 full-text manuscripts were identified by screening titles and abstracts. After evaluation of the full text, 76 articles were excluded. Finally 26 articles met the criteria and were included in our systematic review and meta-analysis (Figure 1).
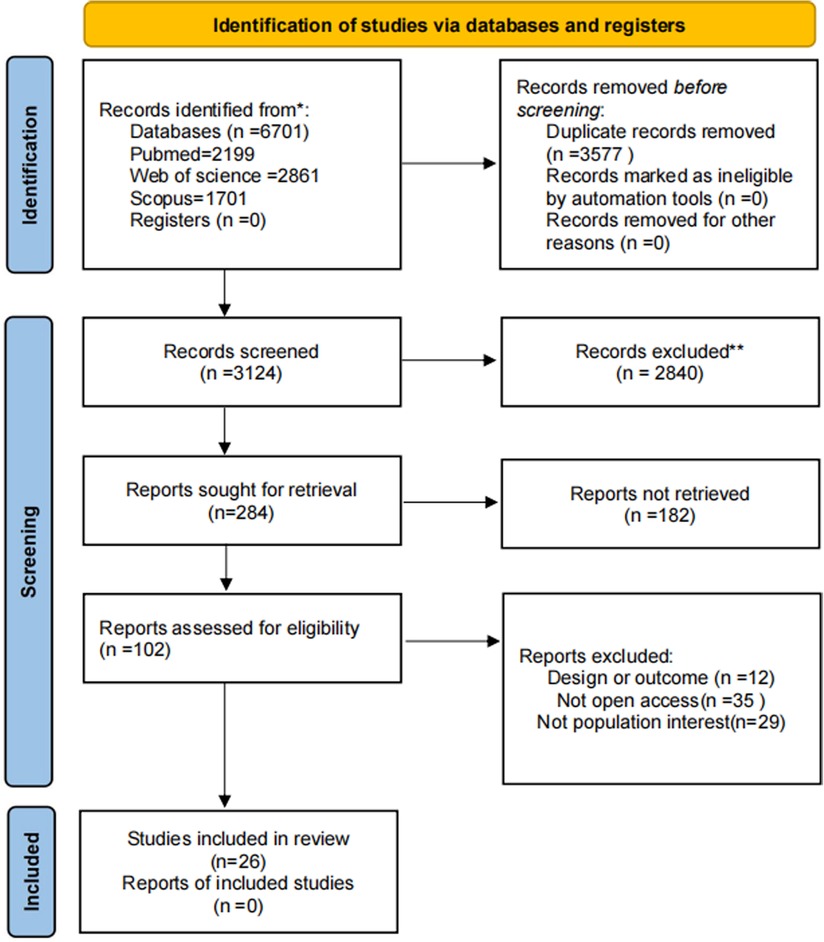
Figure 1. PRISMA 2020 flowchart.
The main characteristics of the participants and interventions are shown in (Table 1). Studies were published between 2005 and 2021, involving 10 RCTs, 4 cluster randomised controlled trials, 2 randomised pilot studies, 2 studies whose types were unclear, 1 pragmatic non-randomized trial, 1 quasi-experimental study, 1 pre-test-post-test design, 1 descriptive study, 1 non-RCT, 1 pilot study, 1 three-arm cluster RCT, and 1 pilot and feasibility study.
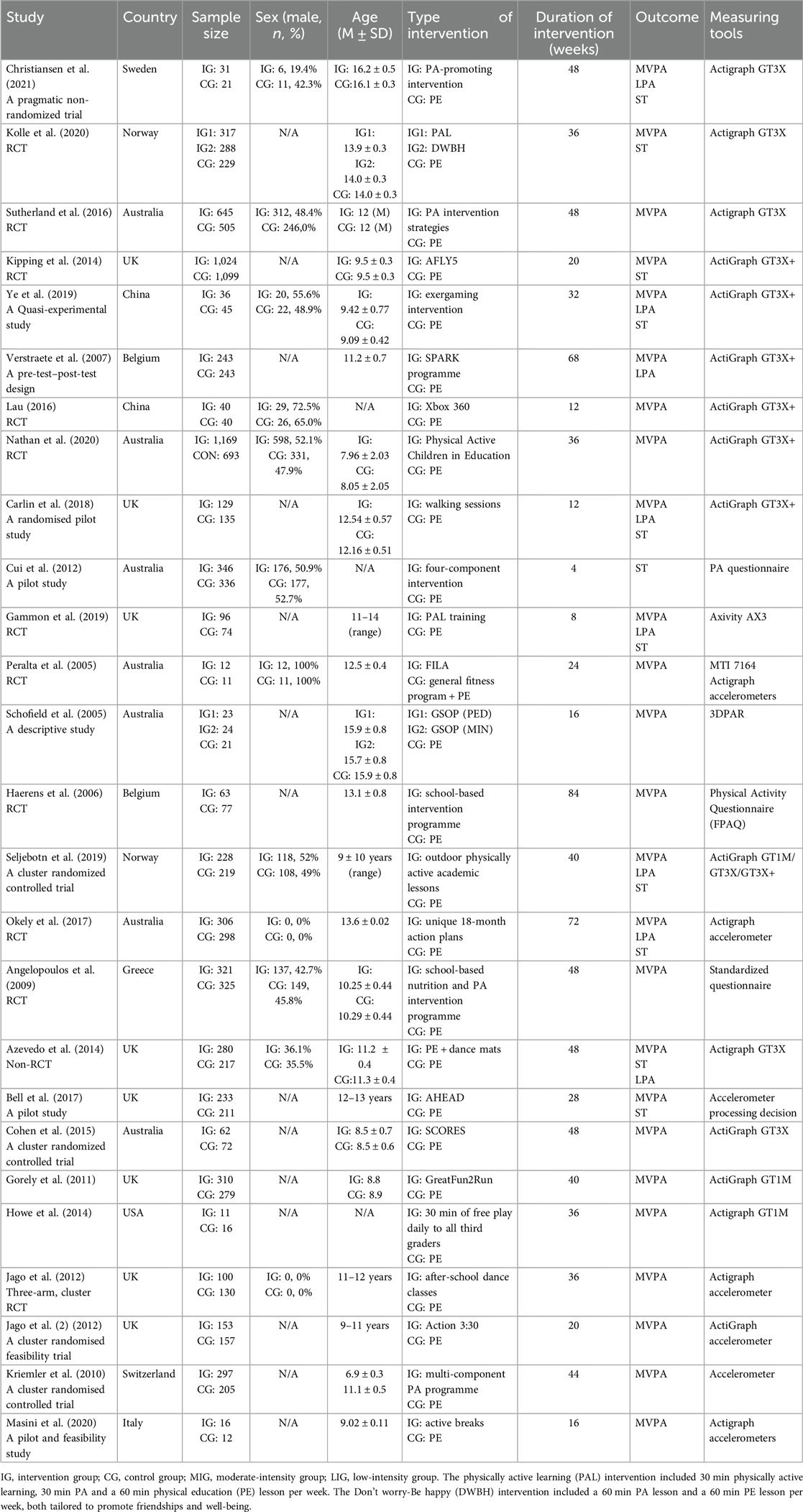
Table 1. Characteristics of studies included in this meta-analysis.
The 26 studies were conducted in 9 countries, including 7 (26.9%) in Australia (23–29), 8 (30.8%) in UK (30–37), 2 (7.7%) in China (38, 39), 2 (7.7%) in Belgium (40, 41), 2 (7.7%) in Norway (22, 42), 1 (3.8%) in Sweden (43), 1 (3.8%) in Greece (44), 1 (3.8%) in Switzerland (45), 1 (3.8%) in USA (46) and 1 (3.8%) in Italy (47). A total of 12,464 individuals were included in the studies. A detailed description of the study participants is given in Table 1. The interventions were all school-based behavioural interventions whose durations ranged from 4 weeks (25) to 84 weeks (25). Regarding the types of intervention outcomes, 25 (96.2%) studies reported MVPA (22–24, 26–47), 13 (50%) studies reported ST (22, 24, 25, 28, 30–34, 39, 41–43), and 9 (56.3%) studies reported LPA (28, 31–33, 39–43).
Figure 2 summarises the risk of bias. Overall, the risk of bias for the 26 trials included in the review was within acceptable limits. Seventeen (65.4%) trials had adequately determined random sequences, and thirteen (50%) adequately implemented allocation concealment. Thirteen (50%) trials blinded participants and staff while 14 (83.8%) were blinded to outcome assessors, and the risk of bias for these trials was judged to be low. In 26 (100%) trials, there were no drop-outs or selectivity reported. Therefore, the risk of bias for these trials was judged to be low.
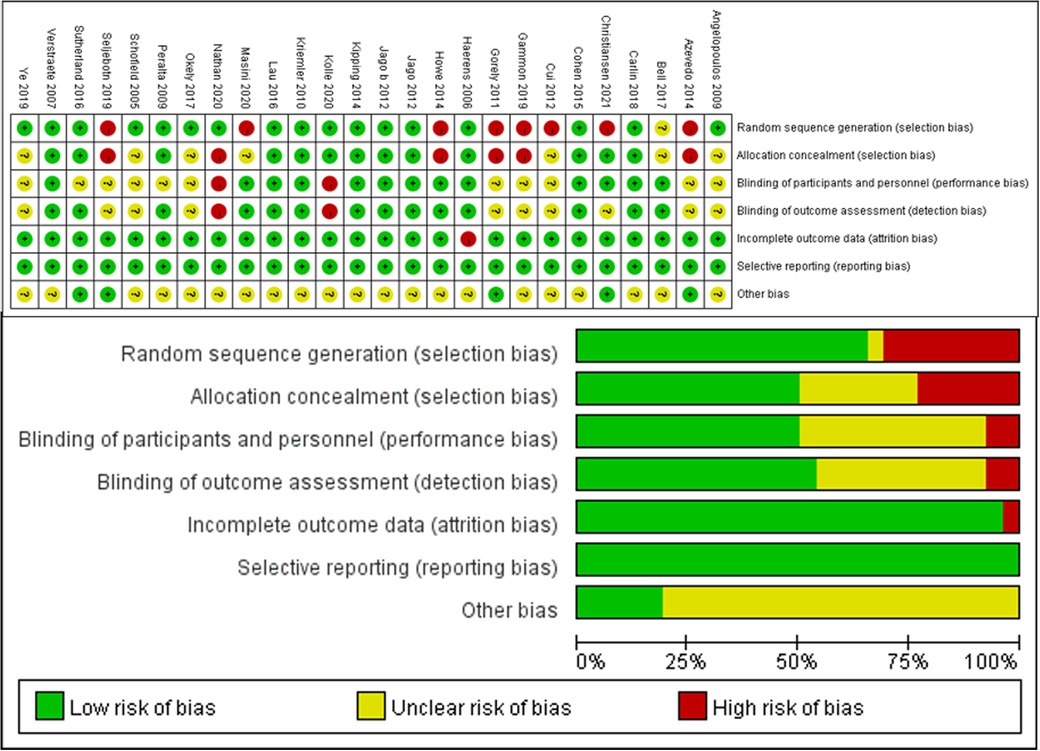
Figure 2. Summary of risk of bias. Risk of bias summary: Review authors’ judgement of risk of bias items for each included study. Below: Risk of bias graph: Review authors’ judgement of each risk of bias item, expressed as a percentage of all included studies.
In the included trials, school-based behavioural interventions for PA levels and sedentary behaviour outcomes of children and adolescents were assessed using a variety of tools. In our review, a meta-analysis was conducted focusing on ST, moderate-intensity PA, and low-intensity PA. Change scores from baseline to final values were used in our final efficacy analyses. The results of our analyses for each outcome are presented below.
Thirteen (22, 24, 25, 28, 30–34, 39, 41–43) studies reported ST and included 6,765 subjects. One study (22) divided the intervention group into two subgroups with different interventions, and one study (41) divided the subjects into two different groups by gender. Fifteen were therefore included in the meta-analysis, and a fixed-effects model was used due to the small heterogeneity present in this review (I2 = 22%). The results showed a combined sample size of 7,053 and a non-significant level of ST for the school-based exercise intervention compared to the control group [SMD = −0.04, 95% CI = (−0.08, 0.01), p = 0.12] (Figure 3).
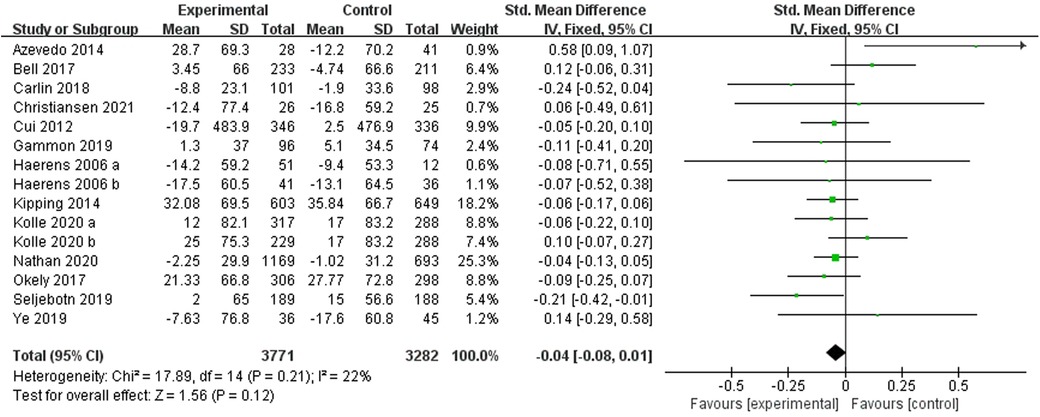
Figure 3. Forest plot of the effect of school-based exercise on ST. CI, confidence interval.
Twenty-two (22–24, 26–35, 38–45, 47) studies reported moderate-intensity PA and included 10,171 subjects. Two studies (22, 27) divided the intervention group into two subgroups with different interventions, and one study (41) divided the subjects into two different groups by gender. Therefore 25 studies were included in the meta-analysis and a random-effects model was used due to the high heterogeneity present in this review (I2 = 89%, p < 0.00001). The results showed a combined sample size of 10,483 and evidence of a significant level of exercise intervention (moderate-intensity PA) compared to the control group [SMD = 0.18, 95% CI = (0.04, 0.31), p = 0.01] (Figure 4). We further conducted subgroup analyses (Table 2). School-based behavioural interventions were found to be more effective in improving moderate-intensity PA in children and adolescents who were in school compared with those who were not in school. No significant differences were found between age subgroups and between study locations.
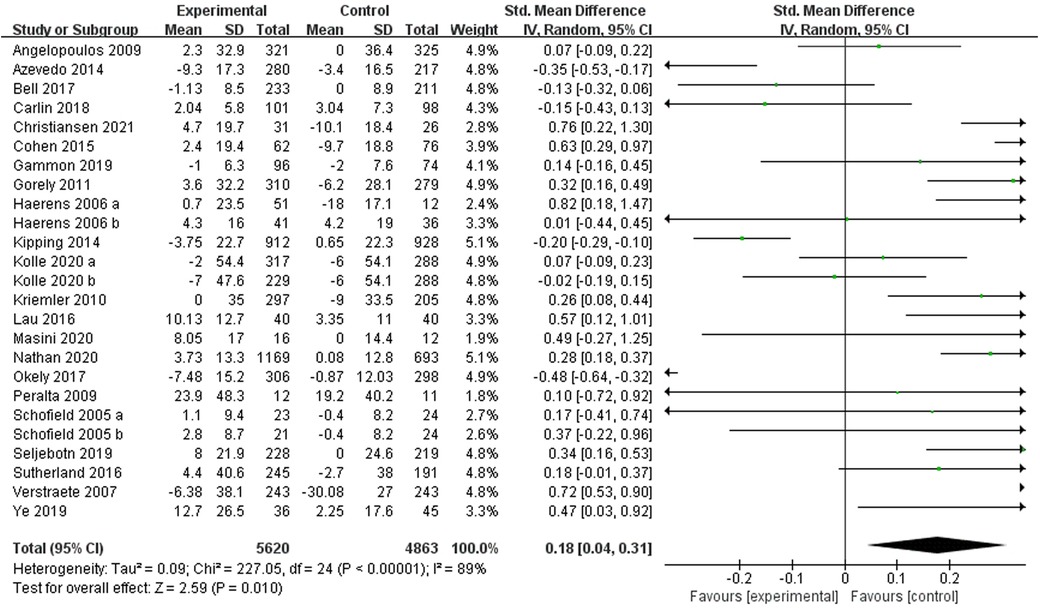
Figure 4. Forest plot of the effect of school-based exercise on moderate-intensity PA. CI, confidence interval.

Table 2. Results of subgroup analysis.
Nine studies (28, 31–33, 39–43) reported low-intensity PA and included 2,179 subjects. One study (41) divided subjects into two different groups by gender. Therefore 10 were included in the meta-analysis and a random-effects model was used due to the high heterogeneity present in this review (I2 = 86%, p < 0.00001). The results showed no evidence of a significant exercise intervention (low-intensity PA) compared to the control group [SMD = 0.18, 95% CI = (−0.07, 0.44), p = 0.16] (Figure 5).
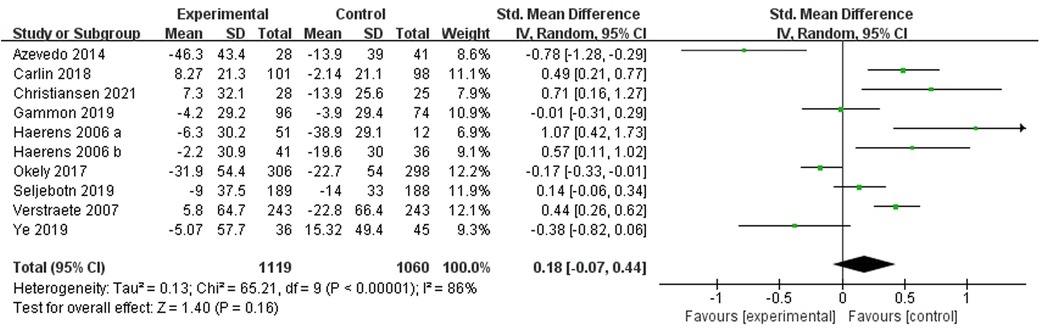
Figure 5. Forest plot of the effect of school-based exercise on low-intensity PA. CI, confidence interval.
Sensitivity analyses were conducted to assess the effect of school-based behavioural interventions on MVPA, ST and LPA in children and adolescents in each study. Figure 6A: The results of the meta-analysis of school-based behavioural interventions on MVPA in children and adolescents were statistically significant, OR (95% CI) = 0.18 (0.04, 0.32). Figure 6B: The results of the meta-analysis of school-based behavioural interventions on ST in children and adolescents were statistically significant, OR (95% CI) = −0.03 (−0.08, 0.02). Figure 6C: The results of the meta-analysis of school-based behavioural interventions on LPA in children and adolescents were statistically significant, OR (95% CI) = 0.18 (−0.07, 0.44). Sensitivity analyses showed good robustness of the results of school-based behavioural interventions on MVPA, ST and LPA in children and adolescents after any separate studies are excluded.
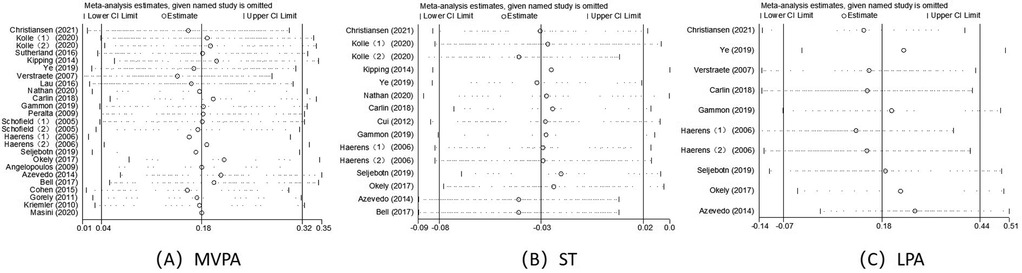
Figure 6. Sensitivity analysis of (A) MVPA, (B) ST, (C) LPA.
According to the funnel plots of school-based behavioural interventions on MVPA, ST and LPA for children and adolescents (Figure 7), the left and right sides of the funnel plots for ST and LPA are largely symmetrical, with less publication bias, the funnel plots for MVPA are less symmetrical, and therefore Egger's and Begg's tests were performed to further test for publication bias.
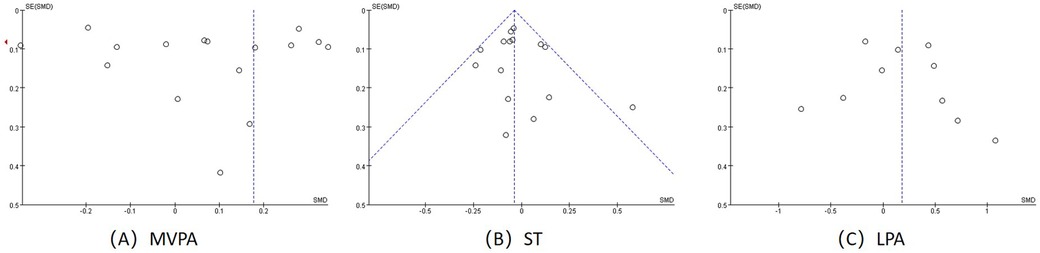
Figure 7. Funnel plots; (A) funnel plot for MVPA (B) funnel plot for ST (C) funnel plot for LPA.
We used Egger's and Begg's linear regression tests to examine publication bias (Table 3) (Supplementary Table S1). MVPA (t = 1.34, P = 0.194), ST (t = 0.11, P = 0.914) and LPA (t = 0.48, P = 0.645) were obtained by Egger's linear regression test. The data obtained by Egger's linear regression test met the criterion when there was no publication bias. By Begg's linear regression tset, MVPA (z = 0.7, Pr = 0.46), ST (z = 0.45, Pr = 0.65) and LPA (z = 0.36, Pr = 0.72) were significantly different. The data obtained by Begg's linear regression test all met the criteria when there was no publication bias. Therefore, there was no publication bias in MVPA, ST, and LPA.
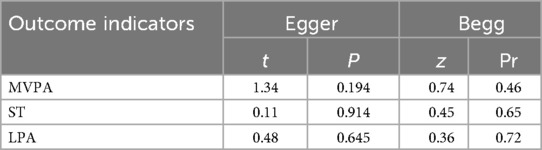
Table 3. Analysis of bias.
Twenty-six studies assessing the impact of school-based behavioural interventions to improve PA and sedentary behaviour in children and adolescents were considered eligible for our systematic evaluation and meta-analysis. We systematically evaluated the available studies and extracted information on sample characteristics, study design, key methodological features, PA and sedentariness. However, most of the included studies were RCTs on exercise interventions and could not be fully blinded. Previous studies have shown that the results of trials using optimal methods may still be at risk of bias. However, it is not reasonable to regard trials as low quality because they were not blinded. During the quality assessment process, we employed the Cochrane Risk of Bias tool (version 1.0) to evaluate the methodological quality of the included studies. This tool was chosen due to its suitability for behavioural intervention research. We did not utilise the GRADE system as our focus was on synthesising effect sizes rather than grading the quality of evidence. The assessment results indicated that 26 studies were deemed to be of high quality, which significantly enhances the credibility and validity of our research, thereby rendering the obtained results and conclusions more accurate and reliable. In order to synthesise the findings on whether school-based behavioural interventions were effective in improving PA and sedentary behaviours in children and adolescents, a meta-analysis of MVPA, ST and LPA was conducted in this study. This meta-analysis provided evidence that school-based behavioural interventions were able to have a smaller but statistically significant impact on moderate-intensity PA in children and adolescents compared to the control group. Subgroup analyses of MVPA, an outcome indicator, by age of the participants, region of study, and time (in or out of school) showed that interventions were more effective in increasing MVPA in children and adolescents during their time in school, with no differences by age or region. School-based behavioural interventions did not improve ST and LPA in children and adolescents.
The school setting has long been defined as the ideal environment for PA promotion interventions. Because children and adolescents spend the majority of their waking hours in the school setting, school-based interventions may be necessary to promote PA in children and adolescents. Our findings update the systematic evaluation of school-based behavioural interventions on PA and sedentary behaviours in children and adolescents. The results of this study suggest that school-based behavioural interventions increased MVPA but had no significant effect on ST and LPA in children and adolescents. This is consistent with the results obtained from a number of previous systematic evaluations, where school-based behavioural interventions have been able to improve PA (48), particularly in urban/suburban schools (49), as well as increase LPA levels and decrease ST in children and adolescents (48, 50). In contrast, some studies have produced opposite findings that school-based behavioral interventions did not improve MVPA (12, 50, 51) and did not improve LPA and ST (51). The inconsistency of the findings is on the one hand attributable to the different results from the included studies. On the other hand, it may be attributed to the different ways (objective accelerometer measurements vs. subjective questionnaires) of assessing PA and ST. Although they have been shown to be valid and reliable in estimating children's PA, accelerometers have the inherent limitation of not being able to take measurements in large numbers, limiting the coverage of whole cohort surveys (52). Moreover, the ability to detect only certain activities and upper body movements, cycling or resistance training may be underestimated (53). In turn, the validity and reliability of questionnaires are relatively weak (54). In addition, these are also sources of potential heterogeneity in the articles and also include differences in intervention design (e.g., duration, intensity, and method of delivery), physical activity, and different characteristics of the study population (e.g., age, gender, and cultural background).
First, the effect of participants' age differences on PA in children and adolescents was assessed. This study involved two subgroups of children (6–12 years old) and adolescents (12–18 years old). The results showed that there were no significant differences between the two subgroups, thus demonstrating that the age of the participants was not a significant factor influencing the effectiveness of school-based behavioural interventions. A meta-analysis concluded that the effects of school-based interventions on PA in older adolescents were usually small and short-term (55). In a specific study that yielded results inconsistent with the present study, the effect size of school-based behavioural interventions increased significantly with the age of the students, with the greatest improvement in the oldest group (Grade 6 students) (24). And a meta-analysis also noted that multiple school-based behavioural interventions were effective in increasing self-reported PA in trials of students aged 13 years or older (48). Given the differences between primary and secondary education, for example, in terms of teaching provision and flexibility of the school day, the resulting studies differed, but the impact of school-based behavioural interventions on PA of children and adolescents was undisputed.
Second, the effect of the region of study on PA of children and adolescents was examined. This study involved three subgroups by the region of study: Europe, Asia and Australia. The results showed no significant differences between the three subgroups, thus demonstrating that the region of study was not an important factor influencing the effectiveness of school-based behavioural interventions. In one study it was noted that a much higher proportion of studies on this topic were conducted in Europe (56). The results of one of these studies suggest that the implementation of interventions in schools in deprived areas has the potential to reduce the decline in PA among adolescents (23). In a study conducted in China, it was noted that Chinese high school students have long school hours (5.4 days of school per week, 7.6 lessons per day 28) and high academic stress (2 h per day for homework) (57). The situation of children and adolescents varies from region to region, but the results of the subgroup analyses show that region does not influence the effectiveness of school-based behavioural interventions.
Thirdly, the impact on PA of children and adolescents in and out of school was examined. The results indicate that the impact on PA was much greater when the participants were in school than that when they were out of school, thus demonstrating that school-based behavioural interventions were an important factor in influencing the PA of children and adolescents in school. No meta-analysis has been conducted to identify the effects of participants on PA when they were in and out of school. The results from one study demonstrated a positive and stronger effect of interventions on PA levels observed during school hours (22). A 10-min increase in MVPA per weekday was equivalent to a 50-min increase in MVPA per week, representing an increase of approximately 30% in PA at baseline (36). School-based interventions were effective in increasing PA levels in children and adolescents.
This systematic evaluation and meta-analysis also had several limitations. First, most of the included studies were randomised controlled trials on exercise interventions and could not be fully blinded. Therefore, subjective factors could cause some degree of bias in the quality assessment process. Second, most studies used accelerometers to assess PA and sedentary behaviour, but a small number of studies used subjective questionnaires for assessment, resulting in high heterogeneity. Third, we combined pre- and post-intervention differential effect sizes and did not consider the long-term impact of the intervention, as only a few of the included studies reported follow-up data in the meta-analysis. This study also has several strengths. First, it is an innovative study since there has not been a systematic evaluation and meta-analysis on the impact of school-based behavioural interventions on PA and sedentary behaviour in children and adolescents, particularly sedentary behaviour. Second, this review employed a rigorous systematic review methodology in accordance with PRISMA guidelines to ensure that relevant literature was identified and assessed with the highest possible scientific rigour. Third, this review provides an a priori design for registration in the Prospero database. Therefore, research questions and inclusion criteria were established prior to conducting this review. Fourth, three electronic sources were searched, as reported above. And, we detailed the search strategy in the electronic Supplementary Table S1. In addition, the quality of the included studies was examined, and the conclusions drawn from this review were strengthened through the use of a quality assessment tool. Fifth, the subgroup analyses conducted in the study are representative, and a distinctive viewpoint can be seen from the study. Our data are able to provide support for policy makers and, in real time, initiatives to improve PA and increase positive health outcomes in children and adolescents.
The present systematic evaluation and meta-analysis suggest that school-based interventions are effective in increasing moderate-intensity PA among children and adolescents, especially during the school days. In future studies, firstly, it is necessary to expand the sample size, standardise the tools for evaluating PA and ST and extend the exercise cycle so that the results of the meta-analysis can be as comprehensive as possible. Secondly, more rigorous and more scientific methods are expected so as to improve the quality of RCTs and draw more rigorous conclusions as much as possible, thus providing better references for relevant medical practitioners as well as physical education teachers.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
LG: Conceptualization, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing. HH: Data curation, Methodology, Software, Writing – original draft. CW: Methodology, Software, Validation, Writing – original draft.
The author(s) declare financial support was received for the research and/or publication of this article. This study was funded by the Annual General Project of the Hunan Provincial Social Science Foundation (Proiect No.23YBA191).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1532035/full#supplementary-material
1. Tassitano RM, Weaver RG, Tenorio MCM, Brazendale K, Beets MW. Physical activity and sedentary time of youth in structured settings: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. (2020) 17(1):160. doi: 10.1186/s12966-020-01054-y
2. Pate RR, O'Neill JR, Lobelo F. The evolving definition of “sedentary”. Exerc Sport Sci Rev. (2008) 36(4):173–8. doi: 10.1097/JES.0b013e3181877d1a
3. Owen N, Healy GN, Matthews CE, Dunstan DW. Too much sitting. Exerc Sport Sci Rev. (2010) 38(3):105–13. doi: 10.1097/JES.0b013e3181e373a2
4. Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, et al. Sedentary behavior research network (SBRN) – terminology consensus project process and outcome. Int J Behav Nutr Phys Act. (2017) 14(1):75. doi: 10.1186/s12966-017-0525-8
5. Carson V, Hunter S, Kuzik N, Gray CE, Poitras VJ, Chaput JP, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Appl Physiol Nutr Metab. (2016) 41(6 Suppl 3):S240–65. doi: 10.1139/apnm-2015-0630
6. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. (2012) 380(9838):219–29. doi: 10.1016/S0140-6736(12)61031-9
7. Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. (2011) 8:98. doi: 10.1186/1479-5868-8-98
8. Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child Adolesc Health. (2020) 4(1):23–35. doi: 10.1016/S2352-4642(19)30323-2
9. Committee on Public Education. Children, adolescents, and television. Pediatrics. (2001) 107(2):423–6. doi: 10.1542/peds.107.2.423
10. Jones M, Defever E, Letsinger A, Steele J, Mackintosh KA. A mixed-studies systematic review and meta-analysis of school-based interventions to promote physical activity and/or reduce sedentary time in children. J Sport Health Sci. (2020) 9(1):3–17. doi: 10.1016/j.jshs.2019.06.009
11. Engelen L, Bundy AC, Naughton G, Simpson JM, Bauman A, Ragen J, et al. Increasing physical activity in young primary school children–it’s child’s play: a cluster randomised controlled trial. Prev Med. (2013) 56(5):319–25. doi: 10.1016/j.ypmed.2013.02.007
12. Love R, Adams J, van Sluijs EMF. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes Rev. (2019) 20(6):859–70. doi: 10.1111/obr.12823
13. Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of children: systematic review and meta-analysis of controlled trials with objectively measured outcomes (earlybird 54). BMJ (Clinical Research ed). (2012) 345:e5888. doi: 10.1136/bmj.e5888
14. Nally S, Carlin A, Blackburn NE, Baird JS, Salmon J, Murphy MH, et al. The effectiveness of school-based interventions on obesity-related behaviours in primary school children: a systematic review and meta-analysis of randomised controlled trials. Children (Basel). (2021) 8(6):489. doi: 10.3390/children8060489
15. Sallis JF, McKenzie TL, Alcaraz JE, Kolody B, Faucette N, Hovell MF. The effects of a 2-year physical education program (spark) on physical activity and fitness in elementary school students. Sports, play and active recreation for kids. Am J Public Health. (1997) 87(8):1328–34. doi: 10.2105/ajph.87.8.1328
16. Ridgers ND, Stratton G, Fairclough SJ, Twisk JW. Long-term effects of a playground markings and physical structures on children’s recess physical activity levels. Prev Med. (2007) 44(5):393–7. doi: 10.1016/j.ypmed.2007.01.009
17. van Sluijs EM, McMinn AM, Griffin SJ. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ. (2007) 335(7622):703. doi: 10.1136/bmj.39320.843947.BE
18. Dobbins M, Husson H, DeCorby K, LaRocca RL. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6–18. Cochrane Database Syst Rev. (2013) 2013(2):CD007651. doi: 10.1002/14651858.CD007651.pub2
19. DiPietro L, Al-Ansari SS, Biddle SJH, Borodulin K, Bull FC, Buman MP, et al. Advancing the global physical activity agenda: recommendations for future research by the 2020 who physical activity and sedentary behavior guidelines development group. Int J Behav Nutr Phys Act. (2020) 17(1):143. doi: 10.1186/s12966-020-01042-2
20. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10(10):ED000142. doi: 10.1002/14651858.ED000142
21. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21(11):1539–58. doi: 10.1002/sim.1186
22. Kolle E, Solberg RB, Safvenbom R, Dyrstad SM, Berntsen S, Resaland GK, et al. The effect of a school-based intervention on physical activity, cardiorespiratory fitness and muscle strength: the school in motion cluster randomized trial. Int J Behav Nutr Phys Act. (2020) 17(1):154. doi: 10.1186/s12966-020-01060-0
23. Sutherland RL, Campbell EM, Lubans DR, Morgan PJ, Nathan NK, Wolfenden L, et al. The physical activity 4 everyone cluster randomized trial: 2-year outcomes of a school physical activity intervention among adolescents. Am J Prev Med. (2016) 51(2):195–205. doi: 10.1016/j.amepre.2016.02.020
24. Nathan NK, Sutherland RL, Hope K, McCarthy NJ, Pettett M, Elton B, et al. Implementation of a school physical activity policy improves student physical activity levels: outcomes of a cluster-randomized controlled trial. J Phys Act Health. (2020) 17(10):1009–18. doi: 10.1123/jpah.2019-0595
25. Cui Z, Shah S, Yan L, Pan Y, Gao A, Shi X, et al. Effect of a school-based peer education intervention on physical activity and sedentary behaviour in Chinese adolescents: a pilot study. BMJ Open. (2012) 2(3):e000721. doi: 10.1136/bmjopen-2011-000721
26. Peralta LR, Jones RA, Okely AD. Promoting healthy lifestyles among adolescent boys: the fitness improvement and lifestyle awareness program rct. Prev Med. (2009) 48(6):537–42. doi: 10.1016/j.ypmed.2009.04.007
27. Schofield L, Mummery WK, Schofield G. Effects of a controlled pedometer-intervention trial for low-active adolescent girls. Med Sci Sports Exerc. (2005) 37(8):1414–20. doi: 10.1249/01.mss.0000174889.89600.e3
28. Okely AD, Lubans DR, Morgan PJ, Cotton W, Peralta L, Miller J, et al. Promoting physical activity among adolescent girls: the girls in sport group randomized trial. Int J Behav Nutr Phys Act. (2017) 14(1):81. doi: 10.1186/s12966-017-0535-6
29. Cohen KE, Morgan PJ, Plotnikoff RC, Callister R, Lubans DR. Physical activity and skills intervention: scores cluster randomized controlled trial. Med Sci Sports Exerc. (2015) 47(4):765–74. doi: 10.1249/MSS.0000000000000452
30. Kipping RR, Howe LD, Jago R, Campbell R, Wells S, Chittleborough CR, et al. Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: active for life year 5 (Afly5) school based cluster randomised controlled trial. BMJ. (2014) 348:g3256. doi: 10.1136/bmj.g3256
31. Carlin A, Murphy MH, Nevill A, Gallagher AM. Effects of a peer-led walking in schools intervention (the wish study) on physical activity levels of adolescent girls: a cluster randomised pilot study. Trials. (2018) 19(1):31. doi: 10.1186/s13063-017-2415-4
32. Gammon C, Morton K, Atkin A, Corder K, Daly-Smith A, Quarmby T, et al. Introducing physically active lessons in UK secondary schools: feasibility study and pilot cluster-randomised controlled trial. BMJ Open. (2019) 9(5):e025080. doi: 10.1136/bmjopen-2018-025080
33. Azevedo LB, Burges Watson D, Haighton C, Adams J. The effect of dance mat exergaming systems on physical activity and health-related outcomes in secondary schools: results from a natural experiment. BMC Public Health. (2014) 14:951. doi: 10.1186/1471-2458-14-951
34. Bell SL, Audrey S, Cooper AR, Noble S, Campbell R. Lessons from a peer-led obesity prevention programme in English schools. Health Promot Int. (2017) 32(2):250–9. doi: 10.1093/heapro/dau008
35. Gorely T, Morris JG, Musson H, Brown S, Nevill A, Nevill ME. Physical activity and body composition outcomes of the Greatfun2run intervention at 20 month follow-up. Int J Behav Nutr Phys Act. (2011) 8:74. doi: 10.1186/1479-5868-8-74
36. Jago R, Sebire SJ, Cooper AR, Haase AM, Powell J, Davis L, et al. Bristol girls dance project feasibility trial: outcome and process evaluation results. Int J Behav Nutr Phys Act. (2012) 9:83. doi: 10.1186/1479-5868-9-83
37. Jago R, Sebire SJ, Davies B, Wood L, Edwards MJ, Banfield K, et al. Randomised feasibility trial of a teaching assistant led extracurricular physical activity intervention for 9–11 year olds: action 3:30. Int J Behav Nutr Phys Act. (2014) 11:114. doi: 10.1186/s12966-014-0114-z
38. Lau PW, Wang JJ, Maddison R. A randomized-controlled trial of school-based active videogame intervention on Chinese children’s aerobic fitness, physical activity level, and psychological correlates. Games Health J. (2016) 5(6):405–12. doi: 10.1089/g4h.2016.0057
39. Ye S, Pope ZC, Lee JE, Gao Z. Effects of school-based exergaming on urban children’s physical activity and cardiorespiratory fitness: a quasi-experimental study. Int J Environ Res Public Health. (2019) 16(21):4080. doi: 10.3390/ijerph16214080
40. Verstraete SJ, Cardon GM, De Clercq DL, De Bourdeaudhuij IM. A comprehensive physical activity promotion programme at elementary school: the effects on physical activity, physical fitness and psychosocial correlates of physical activity. Public Health Nutr. (2007) 10(5):477–84. doi: 10.1017/S1368980007223900
41. Haerens L, Deforche B, Maes L, Cardon G, Stevens V, De Bourdeaudhuij I. Evaluation of a 2-year physical activity and healthy eating intervention in middle school children. Health Educ Res. (2006) 21(6):911–21. doi: 10.1093/her/cyl115
42. Seljebotn PH, Skage I, Riskedal A, Olsen M, Kvalo SE, Dyrstad SM. Physically active academic lessons and effect on physical activity and aerobic fitness. The active school study: a cluster randomized controlled trial. Prev Med Rep. (2019) 13:183–8. doi: 10.1016/j.pmedr.2018.12.009
43. Christiansen F, Ahlqvist VH, Nyroos M, Lofgren H, Berglind D. Physical activity through a classroom-based intervention: a pragmatic non-randomized trial among Swedish adolescents in an upper secondary school. Int J Environ Res Public Health. (2021) 18(21):11041. doi: 10.3390/ijerph182111041
44. Angelopoulos PD, Milionis HJ, Grammatikaki E, Moschonis G, Manios Y. Changes in BMI and blood pressure after a school based intervention: the children study. Eur J Public Health. (2009) 19(3):319–25. doi: 10.1093/eurpub/ckp004
45. Kriemler S, Zahner L, Schindler C, Meyer U, Hartmann T, Hebestreit H, et al. Effect of school based physical activity programme (kiss) on fitness and adiposity in primary schoolchildren: cluster randomised controlled trial. BMJ. (2010) 340:c785. doi: 10.1136/bmj.c785
46. Howe CA, Freedson PS, Alhassan S, Feldman HA, Osganian SK. A recess intervention to promote moderate-to-vigorous physical activity. Pediatr Obes. (2012) 7(1):82–8. doi: 10.1111/j.2047-6310.2011.00007.x
47. Masini A, Marini S, Leoni E, Lorusso G, Toselli S, Tessari A, et al. Active breaks: a pilot and feasibility study to evaluate the effectiveness of physical activity levels in a school based intervention in an Italian primary school. Int J Environ Res Public Health. (2020) 17(12):4351. doi: 10.3390/ijerph17124351
48. Champion KE, Parmenter B, McGowan C, Spring B, Wafford QE, Gardner LA, et al. Effectiveness of school-based ehealth interventions to prevent multiple lifestyle risk behaviours among adolescents: a systematic review and meta-analysis. Lancet Digit Health. (2019) 1(5):e206–21. doi: 10.1016/S2589-7500(19)30088-3
49. Pfledderer CD, Burns RD, Byun W, Carson RL, Welk GJ, Brusseau TA. School-based physical activity interventions in rural and urban/suburban communities: a systematic review and meta-analysis. Obes Rev. (2021) 22(9):e13265. doi: 10.1111/obr.13265
50. Rodrigo-Sanjoaquin J, Corral-Abos A, Aibar Solana A, Zaragoza Casterad J, Lhuisset L, Bois JE. Effectiveness of school-based interventions targeting physical activity and sedentary time among children: a systematic review and meta-analysis of accelerometer-assessed controlled trials. Public Health. (2022) 213:147–56. doi: 10.1016/j.puhe.2022.10.004
51. Neil-Sztramko SE, Caldwell H, Dobbins M. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6–18. Cochrane Database Syst Rev. (2021) 9(9):CD007651. doi: 10.1002/14651858.CD007651.pub3
52. Swain DP, Franklin BA. Comparison of cardioprotective benefits of vigorous versus moderate intensity aerobic exercise. Am J Cardiol. (2006) 97(1):141–7. doi: 10.1016/j.amjcard.2005.07.130
53. Trost SG. Objective measurement of physical activity in youth: current issues, future directions. Exerc Sport Sci Rev. (2001) 29(1):32–6. doi: 10.1097/00003677-200101000-00007
54. Borde R, Smith JJ, Sutherland R, Nathan N, Lubans DR. Methodological considerations and impact of school-based interventions on objectively measured physical activity in adolescents: a systematic review and meta-analysis. Obes Rev. (2017) 18(4):476–90. doi: 10.1111/obr.12517
55. Hynynen ST, van Stralen MM, Sniehotta FF, Araujo-Soares V, Hardeman W, Chinapaw MJ, et al. A systematic review of school-based interventions targeting physical activity and sedentary behaviour among older adolescents. Int Rev Sport Exerc Psychol. (2016) 9(1):22–44. doi: 10.1080/1750984X.2015.1081706
56. Kriemler S, Meyer U, Martin E, van Sluijs EM, Andersen LB, Martin BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. (2011) 45(11):923–30. doi: 10.1136/bjsports-2011-090186
Keywords: school-based behavioural intervention, children and adolescents, physical activity, sedentary behaviour, 24-h movement behaviour
Citation: Guo L, He H and Wang C (2025) Are school-based behavioural interventions an effective strategy for improving physical activity and sedentary behaviour in children and adolescents? A meta-analysis. Front. Pediatr. 13:1532035. doi: 10.3389/fped.2025.1532035
Received: 21 November 2024; Accepted: 26 February 2025;
Published: 11 March 2025.
Edited by:
Yi Sun, Ludong University, ChinaReviewed by:
Sara Górna, Poznan University of Physical Education, PolandCopyright: © 2025 Guo, He and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liangru Guo, Z3VvbGlhbmdydTk1MjcyM0BoeW51LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.