 Juan Ma
Juan Ma Long Chen
Long Chen Kaihong Mu2
Kaihong Mu2 Yuan Shi
Yuan Shi
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr., 21 February 2025
Sec. Pediatric Pulmonology
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1528054
Objectives: To assess the effectiveness of early vs. late caffeine therapy for bronchopulmonary dysplasia (BPD) in infants.
Methods: PubMed, Embase, Web of Science, and Cochrane databases were searched up to October 2024. Studies comparing early and late caffeine therapy for BPD in infants were included. The primary outcomes were the incidence of BPD, severe BPD, and mortality.
Results: Eleven studies (1 RCT and 10 cohorts) with 64,749 patients (34,175 early and 30,574 late) were included. Meta-analysis revealed a significantly lower incidence of BPD (OR: 0.67; 95% CI: 0.56, 0.79; P < 0.00001) but higher mortality (OR: 1.20; 95% CI: 1.12, 1.29; P < 0.00001) in the early group. Subgroup analysis showed a significant difference in BPD incidence in retrospective studies (OR: 0.57; 95% CI: 0.44, 0.74; P < 0.0001), but not in prospective studies (OR: 0.84; 95% CI: 0.44, 1.61; P = 0.61). No significant difference was observed in severe BPD incidence (OR: 0.89; 95% CI: 0.34, 2.35; P = 0.81).
Conclusions: Early caffeine therapy may reduce BPD incidence but increase mortality risk in infants. More large-scale, prospective studies are needed to further evaluate the efficacy of early vs. late caffeine therapy for BPD.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=474351, PROSPERO (CRD42023474351).
Bronchopulmonary dysplasia (BPD) is a common respiratory complication in premature infants, particularly those with ultra-low and very low birth weights. Its incidence is inversely correlated with birth weight and gestational age (1). BPD typically arises from deviations in normal lung development, influenced by preterm birth itself as well as various potential interfering factors, including genetic factors (2). Pathological changes associated with BPD include alveolar simplification, reduced alveoli count, abnormal capillary development, and aberrant growth of vascular tissue (3). Preterm infants with BPD often exhibit symptoms such as wheezing, decreased gas exchange capacity and mobility ability, along with diminished quality of life. Mild to moderate respiratory obstruction and airway collapse may occur in children aged 1–2 years. Significant respiratory obstruction and airway hyperresponsiveness can be observed in school-aged children who continue to grow; during adolescence follow-up visits most patients develop chronic obstructive pulmonary disease similar to that seen in adults. After puberty onset the majority of children experience abnormal lung function and emphysema (4–6).
The drug prevention and treatment of BPD involves the administration of glucocorticoids, vitamin A, macrocyclic vinegar, etc. Among these options, glucocorticoids are the most commonly utilized in clinical practice (7). However, due to recent reports of adverse reactions and potential long-term neurodevelopmental outcomes associated with their use, the clinical application of glucocorticoids remains controversial (8). Caffeine has been studied as an adenosine receptor inhibitor since 1977 for its role in premature apnea. It has been found that caffeine can reduce the duration of respiratory support treatment, improve lung function, and to some extent decrease the incidence of BPD later on (9). Nevertheless, there is no consensus regarding the optimal timing for administering caffeine treatment for BPD. Studies have demonstrated that caffeine not only helps prevent neonatal apnea but also shows positive effects in preventing and treating both BPD and patent ductus arteriosus (PDA). Early initiation of caffeine therapy (within three days after birth) significantly reduces the occurrence of BPD (P < 0.01) as well as decreases the need for PDA medication or surgical intervention (P = 0.01) (10–13). However, it should be noted that several studies have indicated that early use of caffeine does not appear to significantly reduce the incidence of BPD in preterm infants (14, 15). Furthermore, two large cohort studies have suggested a potential increase in all-cause mortality among preterm infants who received early caffeine therapy; however, this finding may be influenced by confounding factors (10, 13).
Therefore, the impact of caffeine treatment timing on mortality and the incidence of BPD in preterm infants remains inconclusive. This study aim at conducting a meta-analysis incorporating the latest and most comprehensive clinical data to establish evidence-based findings regarding the association between caffeine administration timing and BPD incidence and mortality.
The present meta-analytic investigation adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines (16) and was prospectively registered in PROSPERO (CRD42023474351). PubMed, Embase, Web of Science, and Cochrane databases use to search literature up to October 2024, to identify studies that evaluated the effectiveness of initiating caffeine therapy at an early stage compared to a later stage for the management of BPD in infants. Searching terms: “Caffeine”, “Methylxanthine”, “Xanthine” and “Bronchopulmonary Dysplasia”. The detailed search strategies in PubMed are as follows: ((((“Caffeine”[Mesh]) OR ((((((((((((No Doz) OR (Caffedrine)) OR (Coffeinum N)) OR (Coffeinum Purrum)) OR (Dexitac)) OR (Durvitan)) OR (Percoffedrinol N)) OR (Vivarin)) OR (Percutaféine)) OR (Quick-Pep)) OR (QuickPep)) OR (Quick Pep))) OR (“methylxanthine” [Supplementary Concept])) OR (“Xanthine”[Mesh])) AND ((“Bronchopulmonary Dysplasia”[Mesh]) OR (BPD)). The detailed information were presented in Supplementary Table S1. Two investigators screened all included RCTs independently, and via discussion to solve the differences.
Inclusion criteria: (1) RCTs, cohort, case-control study; (2) studies in infants; (3) comparison of early (no later than 3 days after birth) vs. late caffeine (no earlier than 1 day after birth) therapy efficacy; (4) evaluation of at least one outcome; (5) sufficient data to analyze odds ratio (OR), weighted mean difference (WMD), or standard mean difference (SMD). Excluded were protocols, unpublished studies, non-original works (letters, comments, abstracts, corrections, and replies), studies lacking sufficient data, reviews, case reports, and studies with low quality. In this meta-analysis, BPD is defined as preterm infants less than 32 weeks of gestational age who require supplemental oxygen for at least 28 days after birth, with mild BPD as oxygen requirement at diagnosis (breathing ambient air), moderate BPD as less than 30% oxygen, and severe BPD as more than 30% oxygen (17, 18).
Two authors extracted data independently, and third author solve disagreement. The following information was collected: first author, publication year, research period, study region, design, population, intervention (early caffeine), control (late caffeine), sample size, gestational age, gender, birth weight, 5-minute Apgar score, incidence of bronchopulmonary dysplasia (BPD), incidence of severe BPD, and mortality. Continuous data presented as median and range or median and interquartile range (IQR) were recalculated to mean ± standard deviation (SD) using methods by Wan et al. and Luo et al. (19, 20).
The quality of RCTs was evaluated according to the Cochrane Handbook for Systematic Reviews of Interventions 5.1.0, covering seven domains: random sequence generation, allocation concealment, participant and personnel blinding, outcome assessor blinding, incomplete outcome data, selective outcome reporting, and other bias sources (21). Each domain was classified as low-risk, high-risk, or unclear-risk, with more “low-risk” ratings indicating higher quality. The Newcastle-Ottawa Scale (NOS) was used to assess cohort study quality (22), with scores of 7–9 points considered high quality (23). Two authors independently assessed the quality, resolving disagreements through discussion and consensus.
Meta-analysis was conducted using Review Manager 5.4.1 software. For continuous data, weighted mean differences (WMDs) or standardized mean differences (SMDs) were used, and odds ratios (ORs) were applied for dichotomous data. Each measure was reported with 95% confidence intervals (CIs). Heterogeneity was assessed using the chi-squared (χ2) test (Cochran's Q) and the inconsistency index (I2) (24). Significant heterogeneity was defined as a χ2 P-value <0.1 or I2 > 50%. In the presence of significant heterogeneity, the random-effects model was employed; otherwise, fixed-effects model used. Subgroup analyses were conducted for outcomes with three or more studies to evaluate potential confounding factors and the source of heterogeneity when data were available. Sensitivity analyses with one-by-one elimination method were conducted to assess the impact of each study on the overall WMD, SMD, or OR and the source of heterogeneity for results involving more than two studies. Publication bias was assessed by generating funnel plots with Review Manager 5.4.1 and performing Egger's regression tests (25) using Stata 15.1 (Stata Corp, College Station, Texas, USA). A P-value <0.05 indicated significant publication bias.
The flowchart of the literature screening process was shown in Figure 1. 1190 studies were identified in PubMed (n = 180), Embase (n = 551), Web of Science (n = 381), and Cochrane (n = 78). After removing duplicates, 799 titles and abstracts remained. Ultimately, 11 studies (1 RCT and 10 cohort studies) involving 64,749 patients (34,175 in the early group and 30,574 in the late group) were included (1, 10–15, 26–29). The characteristics of each eligible study are presented in Table 1. Quality evaluation details for included RCTs are shown in Supplementary Figure S1 and Table S2 presents the quality evaluation for included cohort studies. Birth weight was similar between the two groups (SMD: 0.23; 95% CI: −0.001, 0.46; P = 0.05), as were gender (male) (OR: 1.00; 95% CI: 0.96, 1.04; P = 0.96), gestational age (WMD: 0.29; 95% CI: −0.09, 0.68; P = 0.13), and 5-minute Apgar score (WMD: 0.07; 95% CI: −0.18, 0.32; P = 0.60) (Table 2).
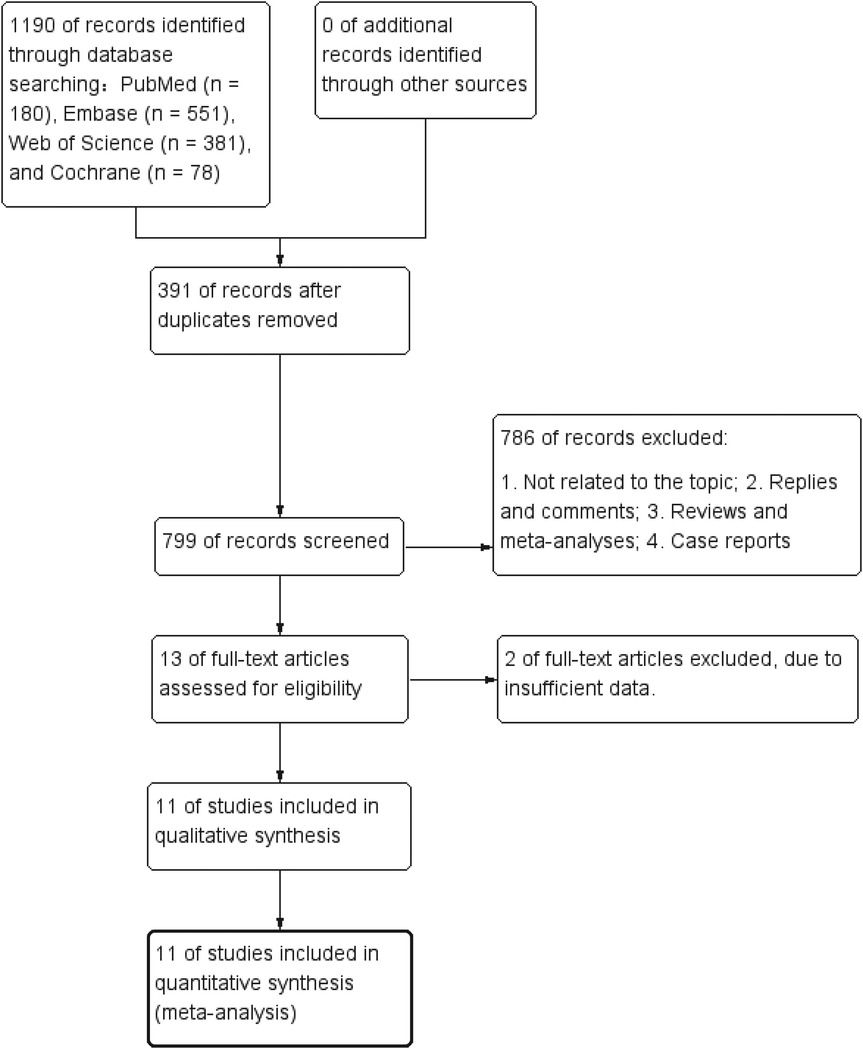
Figure 1. Flowchart of the systematic search and selection process.
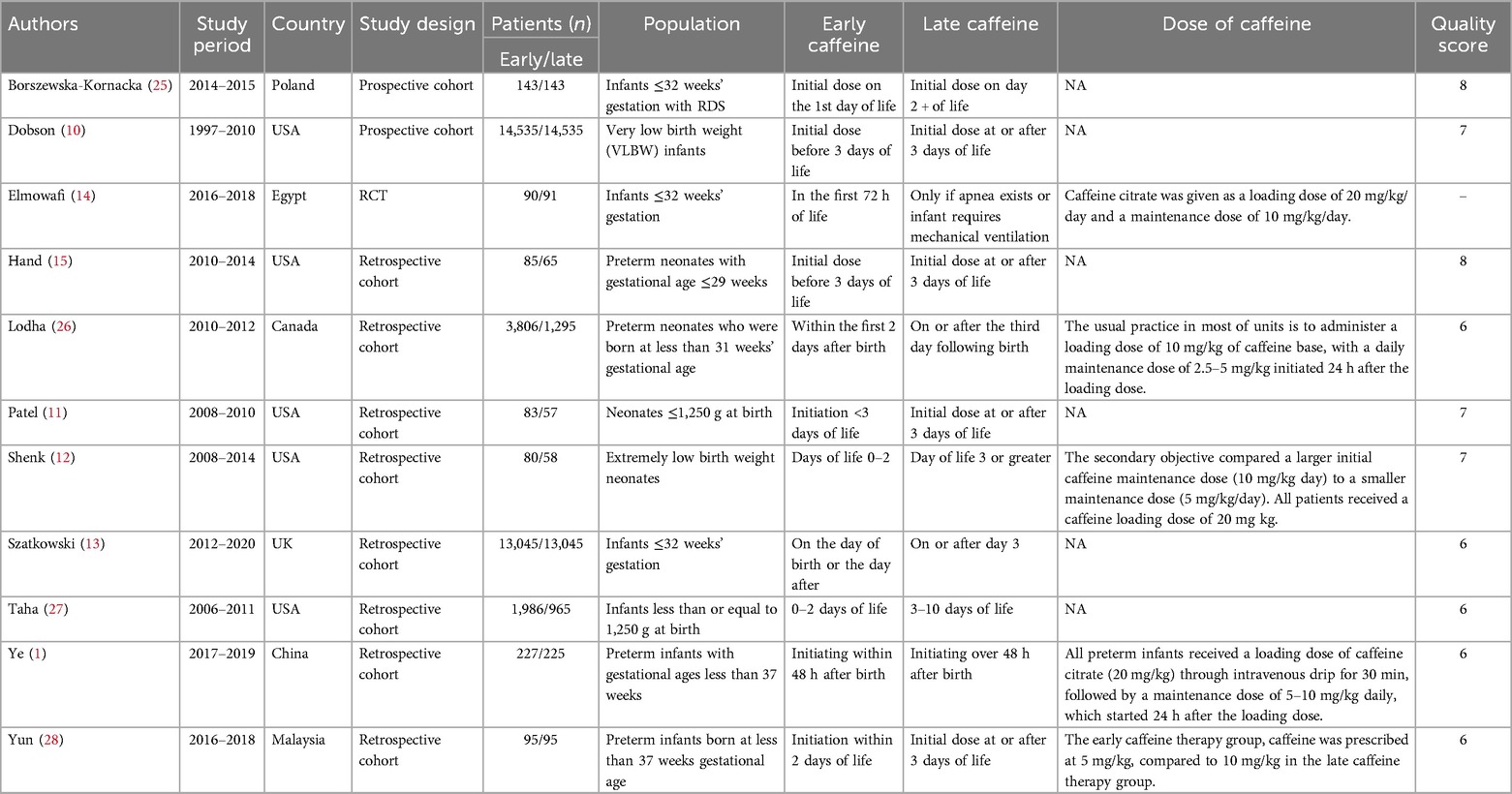
Table 1. Baseline characteristics of include studies and methodological assessment.

Table 2. Demographics and clinical characteristics of included studies.
The incidence of bronchopulmonary dysplasia (BPD) was synthesized from 11 studies, involving 64,749 patients (34,175 in the early group vs. 30,574 in the late group) (1, 10–15, 26–29). Meta-analysis showed a significantly lower incidence of BPD in the early group (OR: 0.67; 95% CI: 0.56, 0.79; P < 0.00001) with considerable heterogeneity (I2 = 90%, P < 0.00001) (Figure 2).
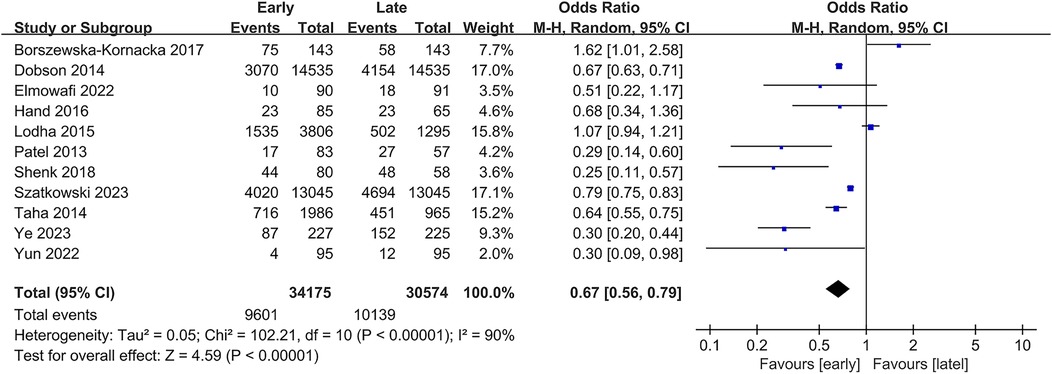
Figure 2. Forest plots of the incidence of BPD.
Subgroup analysis revealed a significant difference in retrospective studies (OR: 0.57; 95% CI: 0.44, 0.74; P < 0.0001) (10, 14, 26), whereas significance disappeared in prospective studies (OR: 0.84; 95% CI: 0.44, 1.61; P = 0.61) (Supplementary Figure S2) (1, 11–13, 15, 27–29).
The incidence of mild and moderate BPD was synthesized from 2 studies involving 467 patients (233 in the early group vs. 234 in the late group) (14, 26). Meta-analysis showed a significantly lower incidence of mild and moderate BPD in the early group (OR: 0.26; 95% CI: 0.16, 0.40; P < 0.00001) without significant heterogeneity (I2 = 0%, P = 0.34) (Figure 3).

Figure 3. Forest plots of the incidence of mild and moderate BPD.
The incidence of severe BPD was synthesized from 2 studies involving 467 patients (233 in the early group vs. 234 in the late group) (14, 26). No significant difference in severe BPD incidence (OR: 0.89; 95% CI: 0.34, 2.35; P = 0.81) (Figure 4).

Figure 4. Forest plots of the incidence of severe BPD.
Mortality data from 8 studies included 61,196 patients (31,877 in the early group vs. 29,319 in the late group) (10–14, 26, 27, 29). This study revealed a significantly higher mortality in the early group (OR: 1.20; 95% CI: 1.12, 1.29; P < 0.00001) with no significant heterogeneity (I2 = 0%, P = 0.80) (Figure 5).
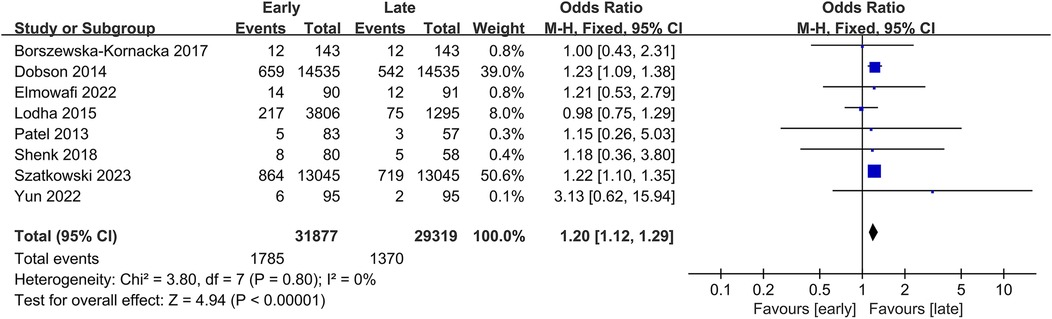
Figure 5. Forest plots of mortality.
Subgroup analysis showed a significant difference in both retrospective studies (OR: 1.19; 95% CI: 1.08, 1.31; P = 0.0004) (11–13, 29) and prospective studies (OR: 1.22; 95% CI: 1.09, 1.37; P = 0.0006) (Supplementary Figure S3) (10, 14, 26).
Sensitivity analyses were conducted to assess the impact of individual studies on the pooled odds ratio (OR) for BPD incidence and mortality, with each eligible study sequentially excluded. The analyses demonstrated consistent and robust ORs following the exclusion of each study, both for BPD incidence (Supplementary Figure S4a) and mortality (Supplementary Figure S4b). Additionally, funnel plots and Egger's regression tests for BPD incidence and mortality, revealing no significant publication bias (Egger's test P = 0.463 for BPD incidence, Supplementary Figure S5a; P = 0.898 for mortality, Supplementary Figure S5b).
Studies have confirmed that BPD is a combination of high oxygen exposure, barometric volume injury and inflammatory factors that lead to impaired lung maturity and abnormal development under the premise of genetic susceptibility, which seriously affects the quality of life of patients in the later period and increases the family economic burden (30, 31). At present, mechanical ventilation and inflammatory response are considered to be the main pathogenic mechanisms of BPD (30). First of all, most children with BPD received respiratory support after birth, which may bring a certain degree of lung damage. Premature lung tissue development was incomplete, which was easy to cause abnormal lung repair and lead to BPD (30). Secondly, inflammatory factors were considered to be the main cause of BPD, and the main pathogenic mechanism was currently believed to be the damage and repair imbalance caused by lung inflammation (32, 33). Studies have shown that inflammation inhibits the secretion of fibroblast growth factor-10 by type I alveolar epithelial cells through the NF-κB pathway, hindering secondary pulmonary segregation and leading to alveolar simplification (34). Therefore, the main factor to prevent the onset of BPD was to withdraw respiratory support as soon as possible to reduce and prevent the occurrence of inflammatory response (31).
Here, the efficacy of early and late caffeine therapy for BPD in infants were assessed. Our study revealed that early administration of caffeine can significantly mitigate the risk of BPD in preterm infants. Caffeine functions as a non-specific antagonist for adenosine receptors, which are present in four forms (A1, A2a, A2b, and A3) throughout the human body (35). Adenosine regulates the concentration of adenylate cyclase by binding to receptors in the body, and is involved in physiological processes such as inflammation, traumatic stress, ischemia reperfusion injury, and vascular dilation, while caffeine mainly acts on the first two receptors (36). Current studies believed that caffeine mainly prevents BPD through the following aspects. First of all, the high concentration of continuous oxygen exposure and the chemotaxis of inflammatory factors after delivery jointly acted on the lungs of newborns, increasing the lung fatigue of newborns and improving their respiratory resistance. Caffeine could improve the outcome of lung development by increasing the sensitivity of respiratory center to carbon dioxide, enhancing respiratory drive, improving lung ventilation, regulating lung vascular development, and inhibiting lung remodeling (37). Secondly, numerous studies have demonstrated that prolonged exposure to high concentrations of oxygen induces neutrophil infiltration into lung tissue and triggers production of inflammatory factors such as neutrophil chemokine-1, tumor necrosis factor-alpha (TNF-α), and interleukin-6 (IL-6). These factors adversely affect alveolar cell development and disrupt pulmonary capillary growth. Caffeine mitigates lung damage by inhibiting the entry of inflammatory factors into lung tissue.
However, we conducted subgroup analysis for the incidence of BPD by study type and found that the significant effect of early application of caffeine in reducing the incidence of BPD disappeared in the prospective study but remained in the retrospective study. Considering that prospective studies (including cohort studies and RCTs) control for the risk of confounders and bias better than retrospective studies, this difference urges caution in interpreting the association between early caffeine use and BPD incidence. Larger, multicenter, well-designed prospective studies are needed to confirm our findings.
On the other hand, infants with early caffeine use had a higher mortality rate. However, this result was somewhat influenced by the two largest cohort studies, both of which reported higher mortality in the early caffeine use group (10, 13), while other studies did not find a significant difference in mortality. Although this finding raises concerns about early caffeine use, higher mortality existed in early caffeine use group may be related to survival bias, as most infant deaths occur in the early years after birth (10). For example, infants who consume caffeine early (0–2 days after birth) are at risk of dying as early as 4 days after birth. In contrast, babies in the late caffeine group who received caffeine on the fifth day of life were apparently less likely to die on the fourth day of life. Further research is needed to confirm whether this conclusion is reliable.
There were several limitations. First of all, most included literatures were retrospective cohort studies, and the number of prospective studies was insufficient, especially RCTs with higher evidence quality, which is also one of the potential reasons leading to significant heterogeneity for the incidence of BPD. However, we did not observe a reduction in heterogeneity after subgroup analysis based on study type, so we speculate that it may be related to caffeine dose, patient sample size, study region and other factors. Secondly, the sample size of the literatures included in this meta-analysis is quite different, resulting in the final result being greatly affected by the large sample size of the studies. However, our sensitivity analysis results did not find instability. Moreover, most literature only reports the relationship between the timing of caffeine use and the mortality and incidence of BPD in the early postnatal period, and its long-term effect lacks effective data, which needs further research to confirm. This meta-analysis presents the latest evidence-based medical evidence and potential confounders for early caffeine use to reduce the incidence of BPD, as well as a potential positive association between early caffeine use and infant mortality, providing a theoretical basis for further prospective clinical studies. More large-scale, multi-center, prospective studies are needed to further confirm our findings.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
JM: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. LC: Data curation, Formal Analysis, Methodology, Software, Writing – original draft, Writing – review & editing. KM: Investigation, Resources, Supervision, Writing – original draft. ST: Formal Analysis, Investigation, Resources, Writing – original draft. YS: Conceptualization, Funding acquisition, Methodology, Project administration, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. 1. National Key R&D Program of China (2022YFC2704800). 2. Technological Innovation and Application of Respiratory Support and Comprehensive Management for Preterm Infants (Chongqing Municipal Bureau of Science and Technology Special Key Project on Technological Innovation and Application Development) (CSTC2021jscx-gksb-N0015). 3. Chongqing Medical Science and Technology Innovation Project (2024MSXM179).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1528054/full#supplementary-material
1. Ye H, Bai L, Yang M, Yang X, Zheng M, Zhong X, et al. A two-center retrospective study: association of early caffeine administration and oxygen radical diseases in neonatology in Chinese preterm neonates. Front Pediatr. (2023) 11:1158286. doi: 10.3389/fped.2023.1158286
2. Wen LS, Manley BJ, Davis PG, Doyle LW. The evolution of modern respiratory care for preterm infants. Lancet. (2017) 389(10079):1649–59. doi: 10.1016/S0140-6736(17)30312-4
3. Jobe AH. What is BPD in 2012 and what will BPD become? Early Hum Dev. (2012) 88:S27–S8. doi: 10.1016/S0378-3782(12)70009-9
4. Vom Hove M, Prenzel F, Uhlig HH, Robel-Tillig E. Pulmonary outcome in former preterm, very low birth weight children with bronchopulmonary dysplasia: a case-control follow-up at school age. J Pediatr. (2014) 164(1):40–45.e4. doi: 10.1016/j.jpeds.2013.07.045
5. Schmalisch G, Wilitzki S, Roehr CC, Proquitté H, Bührer C. Development of lung function in very low birth weight infants with or without bronchopulmonary dysplasia: longitudinal assessment during the first 15 months of corrected age. BMC Pediatr. (2012) 12(1):1–9. doi: 10.1186/1471-2431-12-37
6. Wong PM, Lees AN, Louw J, Lee FY, French N, Gain K, et al. Emphysema in young adult survivors of moderate-to-severe bronchopulmonary dysplasia. Eur Respir J. (2008) 32(2):321–8. doi: 10.1183/09031936.00127107
7. Fike CD, Aschner JL. Pharmacotherapy for pulmonary hypertension in infants with bronchopulmonary dysplasia: past, present, and future. Pharmaceuticals (Basel). (2023) 16(4):503. doi: 10.3390/ph16040503
8. Hysinger EB, Ahlfeld SK. Respiratory support strategies in the prevention and treatment of bronchopulmonary dysplasia. Front Pediatr. (2023) 11:1087857. doi: 10.3389/fped.2023.1087857
9. Lodha A, Entz R, Synnes A, Creighton D, Yusuf K, Lapointe A, et al. Early caffeine administration and neurodevelopmental outcomes in preterm infants. Pediatrics. (2019) 143(1):e20181348. doi: 10.1542/peds.2018-1348
10. Dobson NR, Patel RM, Smith PB, Kuehn DR, Clark J, Vyas-Read S, et al. Trends in caffeine use and association between clinical outcomes and timing of therapy in very low birth weight infants. J Pediatr. (2014) 164(5):992–998.e3. doi: 10.1016/j.jpeds.2013.12.025
11. Patel RM, Leong T, Carlton DP, Vyas-Read S. Early caffeine therapy and clinical outcomes in extremely preterm infants. J Perinatol. (2013) 33(2):134–40. doi: 10.1038/jp.2012.52
12. Shenk EE, Bondi DS, Pellerite MM, Sriram S. Evaluation of timing and dosing of caffeine citrate in preterm neonates for the prevention of bronchopulmonary dysplasia. J Pediatr Pharmacol Ther. (2018) 23(2):139–45. doi: 10.5863/1551-6776-23.2.139
13. Szatkowski L, Fateh S, Abramson J, Kwok TC, Sharkey D, Budge H, et al. Observational cohort study of use of caffeine in preterm infants and association between early caffeine use and neonatal outcomes. Arch Dis Child Fetal Neonatal Ed. (2023) 108(5):505–10. doi: 10.1136/archdischild-2022-324919
14. Elmowafi M, Mohsen N, Nour I, Nasef N. Prophylactic versus therapeutic caffeine for apnea of prematurity: a randomized controlled trial. J Matern Fetal Neonatal Med. (2025) 35(25):6053–61. doi: 10.1080/14767058.2021.1904873
15. Hand I, Zaghloul N, Barash L, Parris R, Aden U, Li HL. Timing of caffeine therapy and neonatal outcomes in preterm infants: a retrospective study. Int J Pediatr. (2016) 2016:9478204. doi: 10.1155/2016/9478204
16. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical Research ed). (2021) 372:n71. doi: 10.1136/bmj.n71
17. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. (2014) 14:135. doi: 10.1186/1471-2288-14-135
18. Katz TA, Bancalari E, Gordijn SJ, Higgins RD, Isayama T, Jensen EA, et al. Towards a harmonized bronchopulmonary dysplasia definition: a study protocol for an international Delphi procedure. BMJ Paediatr Open. (2023) 7(1):e002112. doi: 10.1136/bmjpo-2023-002112
19. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. (2018) 27(6):1785–805. doi: 10.1177/0962280216669183
20. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10:Ed000142. doi: 10.1002/14651858.ED000142
21. Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses (2011). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (cited 2020 12/28).
22. Kim SR, Kim K, Lee SA, Kwon SO, Lee JK, Keum N, et al. Effect of red, processed, and white meat consumption on the risk of gastric cancer: an overall and dose–response meta-analysis. Nutrients. (2019) 11(4):826. doi: 10.3390/nu11040826
23. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21(11):1539–58. doi: 10.1002/sim.1186
24. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ (Clinical Research ed). (1997) 315(7109):629–34. doi: 10.1136/bmj.315.7109.629
25. Borszewska-Kornacka MK, Hożejowski R, Rutkowska M, Lauterbach R. Shifting the boundaries for early caffeine initiation in neonatal practice: results of a prospective, multicenter study on very preterm infants with respiratory distress syndrome. PLoS One. (2017) 12(12):e0189152. doi: 10.1371/journal.pone.0189152
26. Lodha A, Seshia M, McMillan DD, Barrington K, Yang J, Lee SK, et al. Association of early caffeine administration and neonatal outcomes in very preterm neonates. JAMA Pediatr. (2015) 169(1):33–8. doi: 10.1001/jamapediatrics.2014.2223
27. Taha D, Kirkby S, Nawab U, Dysart KC, Genen L, Greenspan JS, et al. Early caffeine therapy for prevention of bronchopulmonary dysplasia in preterm infants. J Matern Fetal Neonatal Med. (2014) 27(16):1698–702. doi: 10.3109/14767058.2014.885941
28. Yun WZ, Kassab YW, Yao LM, Khairuddin N, Ming LC, Hadi MA. Effectiveness and safety of early versus late caffeine therapy in managing apnoea of prematurity among preterm infants: a retrospective cohort study. Int J Clin Pharm. (2022) 44(5):1140–8. doi: 10.1007/s11096-022-01437-0
29. Vento G, Tirone C, Paladini A, Aurilia C, Lio A, Tana M. Weaning from the ventilator in bronchopulmonary dysplasia. Clin Perinatol. (2021) 48(4):895–906. doi: 10.1016/j.clp.2021.08.005
30. Gilfillan M, Bhandari A, Bhandari V. Diagnosis and management of bronchopulmonary dysplasia. BMJ (Clinical Research ed). (2021) 375:n1974. doi: 10.1136/bmj.n1974
31. Perrone S, Manti S, Buttarelli L, Petrolini C, Boscarino G, Filonzi L, et al. Vascular endothelial growth factor as molecular target for bronchopulmonary dysplasia prevention in very low birth weight infants. Int J Mol Sci. (2023) 24(3):2729. doi: 10.3390/ijms24032729
32. Deng X, Bao Z, Yang X, Mei Y, Zhou Q, Chen A, et al. Molecular mechanisms of cell death in bronchopulmonary dysplasia. Apoptosis. (2023) 28(1-2):39–54. doi: 10.1007/s10495-022-01791-4
33. Han T, Chi M, Wang Y, Mei Y, Li Q, Yu M, et al. Therapeutic effects of fibroblast growth factor-10 on hyperoxia-induced bronchopulmonary dysplasia in neonatal mice. Am J Transl Res. (2017) 9(8):3528–40.28861146
34. Jensen EA. What is bronchopulmonary dysplasia and does caffeine prevent it? Semin Fetal Neonatal Med. (2020) 25(6):101176. doi: 10.1016/j.siny.2020.101176
35. Yuan Y, Yang Y, Lei X, Dong W. Caffeine and bronchopulmonary dysplasia: clinical benefits and the mechanisms involved. Pediatr Pulmonol. (2022) 57(6):1392–400. doi: 10.1002/ppul.25898
36. Kumar VHS, Lipshultz SE. Caffeine and clinical outcomes in premature neonates. Children (Basel, Switzerland). (2019) 6(11):118. doi: 10.3390/children6110118
Keywords: caffeine, bronchopulmonary dysplasia, mortality, meta-analysis, BPD
Citation: Ma J, Chen L, Mu K, Tang S and Shi Y (2025) Early caffeine therapy decreases bronchopulmonary dysplasia but might increase mortality in preterm infants? a systematic review and meta-analysis. Front. Pediatr. 13:1528054. doi: 10.3389/fped.2025.1528054
Received: 14 November 2024; Accepted: 7 February 2025;
Published: 21 February 2025.
Edited by:
Albert Martin Li, The Chinese University of Hong Kong, ChinaReviewed by:
Chung-Ming Chen, Taipei Medical University, TaiwanCopyright: © 2025 Ma, Chen, Mu, Tang and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuan Shi, c2hpeXVhbkBob3NwaXRhbC5jcW11LmVkdS5jbg==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.